
Abstract
Background:
Little attention has been given to prenatal cobalamin insufficiency in settings where dietary cobalamin intake is presumed adequate, such as populations with habitual intake of foods from animal sources.
Results:
However, low cobalamin status in women of fertile age has been reported in Europe, United States, and Canada. In India, where cobalamin deficiency is highly prevalent, it has been associated with an increased risk of miscarriage, intrauterine growth retardation, as well as insulin resistance and lower neurodevelopment scores in the offspring. Low cobalamin status in pregnancy has been associated with similar outcomes as those reported in the Indian studies although the evidence is scant and conflicting.
Conclusions:
Consideration should be given to maternal cobalamin status in the context of prevention of adverse pregnancy outcomes as well as cobalamin insufficiency both in the mother and the offspring during lactation. Further attention is now justified with the increasing tendency toward plant-based diets. Reference intervals for cobalamin status during each trimester of pregnancy are needed and further investigation of the long-term conse-quences of low cobalamin status during pregnancy for health and development in the offspring is warranted.
Plain language title
Inadequate cobalamin status during critical periods of growth and development can have negative consequences on maternal and childhood health
Introduction
Cobalamin deficiency in pregnant women has been reported to be highly prevalent studies in India, Nepal, and other parts of Asia. Transgenerational associations between maternal cobalamin insufficiency and adverse health and development outcomes during childhood in the offspring have been reported. This article set out to review cobalamin status during pregnancy and its long-term association with maternal and child health and development, especially outside of the context of the Indian/Asian setting, where there has been less research on this topic. We conducted a PubMed search on May 1st 2023, including all publications from January 1, 1993, and limited to human studies published in English. We manually revised the 947 studies retrieved to include original studies where early pregnancy cobalamin status was the main exposure and childhood health or development was the principal outcome. Intervention trials containing multiple nutrients were excluded.
Cobalamin is essential for fetal growth and development. As a cofactor for methionine synthase, using methyl groups provided by the folate cycle, methylcobalamin participates in the supply of methionine to the fetus as well as in several biological processes, including amino acid and nucleotide synthesis and epigenetic processes. 1 Adenosylcobalamin is a cofactor for methylmalonyl-CoA mutase in the conversion of methylmalonyl-CoA to succinyl-CoA, a central intermediary of the tricarboxylic acid cycle, thus affecting energy production. 2
Cobalamin Status During Pregnancy
Reference intervals are needed for cobalamin status in pregnancy. Cobalamin status varies with time of pregnancy 3 and plasma cobalamin concentrations gradually decline by, on average, 32% from preconception concentrations as normal pregnancy progresses. The physiological demands of pregnancy and the growing fetus play a major role in the drop in plasma cobalamin concentration during pregnancy. Nevertheless, in the Spanish Preconception study of nonvegetarian healthy women, the lowest decile for plasma cobalamin status was below 148 pmol/L from preconception throughout pregnancy. The pattern of pregnancy changes in plasma methylmalonic (MMA), a functional indicator of cobalamin status, and plasma holotranscobalamin (holoTC), the biologically active component of cobalamin, were different to those of plasma total cobalamin, but while plasma MMA gradually increased as pregnancy progressed, holoTC did not fall further for the remainder of pregnancy. These 3 plasma indicators of cobalamin status are susceptible to the same physiological changes during pregnancy and the concentrations of all of them fell in the first trimester. Thereafter, unlike plasma total cobalamin, holoTC concentrations were maintained and MMA concentrations increased in the face of hemodilution and increased renal function that occur during the second and third trimesters of pregnancy. Stratification by preconception holoTC status showed that the pregnancy increase in MMA was greater in the women that started pregnancy with holoTC below the median (67 pmol/L) compared with above the median, suggesting worsening maternal cobalamin status as pregnancy progresses. The same study showed that all plasma indicators of maternal cobalamin status (total cobalamin, holoTC, and MMA) are correlated with cord cobalamin status, and the correlations are more robust in the third trimester and late pregnancy. Cord plasma concentrations of all indicators are higher than in the mother at labor. In the case of fasting plasma total homocysteine (tHcy), however, cord concentrations are lower than in the mother at labor. 4
Results
Maternal Cobalamin Status and Adverse Pregnancy Outcomes
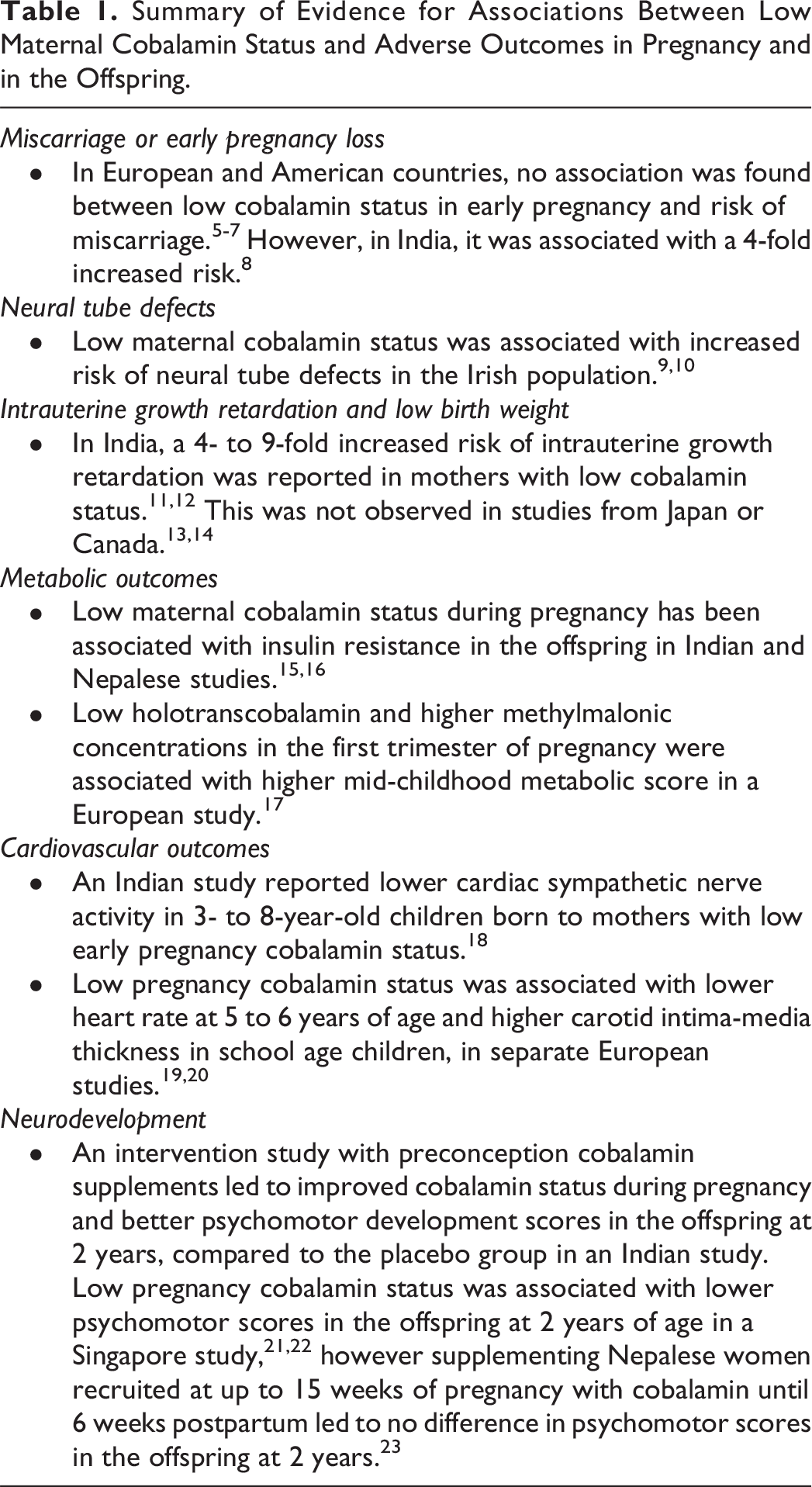
The main conclusions are summarized in Table 1.
Summary of Evidence for Associations Between Low Maternal Cobalamin Status and Adverse Outcomes in Pregnancy and in the Offspring.
Miscarriage or Early Pregnancy Loss
Low cobalamin status has been associated with adverse pregnancy outcomes in some studies but not in others. A German study reported no difference in cobalamin status in women with a history of recurrent miscarriage (range 179-793 pmol/L) compared with controls (range 142-932 pmol/L). 5 A preconception study in Anhui, China, reported low cobalamin status (plasma cobalamin <258 pmol/L) in 18% of the participants but observed no association between cobalamin status and risk of miscarriage. 24 A Brazilian study reported no association between early pregnancy plasma cobalamin and risk of miscarriage but reported a 4-fold increase in risk of miscarriage for every quartile increase in early pregnancy MMA. 6 In the Reus-Tarragona Birth Cohort Study, we reported that elevated early pregnancy tHcy is associated with increased risk of idiopathic early pregnancy miscarriage (RR [95% CI]: 2.5 [1.1, 5.7]). First trimester red blood cell folate status was lower in women who miscarried than those who went on to have a normal pregnancy. Still, there was no difference in cobalamin status between the 2 groups. 7 In an Indian case–control study, 39% of women with early pregnancy loss were cobalamin deficient (plasma cobalamin < 148 pmol/L) compared with 10% of the control group. The OR (95% CI) for early pregnancy loss was 4.83 (1.96-11.98). 8
Neural Tube Defects
With regard to neural tube defects (NTDs), an Irish case–control study derived from a large representative sample of pregnant women reported lower plasma cobalamin status (median 179 pmol/L) in mothers of fetuses with NTDs compared with control mothers (median 218 pmol/L). 9 The highest prevalence of NTDs was observed in mothers with plasma cobalamin status <179 pmol/L, and low plasma cobalamin status was independently associated with NTD risk in the fetus. Stratifying by plasma folate status, the prevalence of NTDs increased with worsening B12 status in every category of folate status. Subsequently, another study confirmed that mothers who gave birth to babies with NTDs had lower cobalamin status during pregnancy and that plasma total cobalamin in the lowest quartile (<184 pmol/L) was associated with triple the risk of having an NTD-affected pregnancy. A preconception plasma cobalamin status of at least 221 pmol/L was recommended to prevent NTDs. 10
Fetal Growth and Birth Weight
An Indian study reported 4- to 9-fold increases in the risk of intrauterine growth retardation in the offspring born to mothers in the lowest and mid-tertiles of plasma cobalamin in any of the trimesters of pregnancy. 11 Another Indian study with a high prevalence of cobalamin deficiency reported that first-trimester cobalamin deficiency was associated with an 8-fold risk of low birth weight in the offspring. 12 On the other hand, a Japanese study observed no association between serum cobalamin at any time of pregnancy with birth weight, length or head circumference in the offspring, 13 and a Canadian study reported no association between early pregnancy cobalamin status and birth weight in the offspring, despite observing cobalamin deficiency (plasma cobalamin <148 pmol/L) in 20% of the women in the first trimester. 14
Metabolic and Cardiovascular Outcomes in the Offspring
Low cobalamin status during pregnancy was originally associated with negative metabolic health outcomes in the offspring in studies in regions renowned for low status. 15,16 The Reus-Tarragona Birth Cohort study, conducted in Spain, investigated the associations between pregnancy tHcy, plasma cobalamin, holoTC, MMA, and mid-childhood metabolic score (MetSco) at 7.5 years in the offspring. 17 Highest versus low-mid tertile maternal tHcy in the first and third trimesters of pregnancy was associated with elevated mid-childhood MetSco in boys but not in girls. This association was confirmed for fat mass index and homeostatic model of insulin resistance z-scores. Although first trimester plasma cobalamin was not associated with child health outcomes, lowest (<47.6 pmol/L) versus mid-high plasma holoTC tertile was associated with higher MetSco (specifically zFMI and zHOMA-IR), and highest (≥0.16 µmol/L) versus low-mid plasma MMA tertile was associated with greater MetSco and dyslipidemia in boys only. These observations were in a study of women with a low prevalence of cobalamin deficiency (2.6% during the first trimester). Further investigation is warranted, but the mechanism may be epigenetic based. Sex differences were also reported in an animal study of 1-carbon nutrient restriction during pregnancy in rat dams. The intervention led to elevated insulin in the male offspring only. 25 Some studies have reported an association between pregnancy cobalamin status and cardiovascular outcomes in the offspring, but the evidence is scant and inconclusive so far. An Indian study reported lower sympathetic nerve activity to the heart in 3- to 8-year-old Indian children born to mothers with first trimester pregnancy serum B12 <114 pmol/L versus ≥ 114 pmol. None of the other heart rate variability parameters were different between the 2 groups. 18 A multi-ethnic Dutch study, reported lower heart rates in the 5- to 6-year-old offspring born to mothers with low serum vitamin B12 status during pregnancy but the results were not significant when restricted to Dutch mother-child dyads. 19 The school age offspring (median 9.7 years) born to mothers with low serum B12 (<145 pmol/L) during pregnancy, in another Dutch study, had higher carotid intima-media thickness compared to those born to mothers with pregnancy serum B12 ≥ 145 pmol. However, the difference was no longer significant following post hoc correction for multiple comparisons. 20
Neurological Development
We previously reported that elevated preconception tHcy is associated with lower scores at 2 stages of development: in psychomotor tests at 4 and 12 months and in intelligence tests, of the same offspring, at 6 years of age. 26 Specifically, regarding studies of maternal cobalamin status, the results are less consistent. Preconception cobalamin supplements in an Indian trial resulted in improved cobalamin status during pregnancy and better psychomotor development outcomes in the offspring at 2 years compared with the placebo group. However, the neurodevelopmental outcomes in the group receiving cobalamin combined with other micronutrients did not differ from the placebo group. 21 A Singapore study reported cobalamin deficiency (<148 pmol/L) in the third trimester of pregnancy in 15% of the mothers and worse scores in neurodevelopment tests at 2 years in their offspring compared with those with cobalamin-replete mothers. 22 This was also true for the offspring of mothers with cobalamin insufficiency (148-221 pmol/L) combined with pyridoxine deficiency. A randomized control trial in Nepal reported no difference in neurodevelopment at 2 years of age in the offspring of mothers who had been recruited at up to 15 gestational weeks and supplemented with 50 µg/d of cobalamin until 6 months postpartum compared with placebo. At baseline, 71% of the mothers had cobalamin insufficiency. 23 Cobalamin status of the mothers was improved by the supplement regime but it cannot be discarded that the lack of difference between the offspring in the treated versus the placebo group is due to the late initiation of the intervention (after neurogenesis onset), especially considering the high prevalence of cobalamin insufficiency during neurogenesis in the fetus. Furthermore, measuring the outcome, at only 2 years of age, limits the aspects of neurological development that can be assessed. The Dutch Generation R study reported no association between pregnancy cobalamin status and neurological development (behaviour or IQ) in the children aged 6. 27 The UK ALSPAC study did not have any measurement of maternal B12 status during pregnancy but reported lower scores in 6 year speech intelligibility and some parameters of mathematic outcomes at 8 years in children born to mothers with the lowest decile of B12 intake during pregnancy (<2.26 µg/d) versus the rest. 28
Global Cobalamin Status and Interactions With Folate Status
Cobalamin deficiency was reported to affect 15.0% to 46.0% of women of fertile age or during pregnancy in studies from India and Nepal, 22,23 areas where dietary cobalamin intake is habitually low for cultural or socioeconomic reasons. But cobalamin deficiency has also been reported to affect 42% of nonvegetarian pregnant women in a Pakistani study (<140 pmol/L) 29 as well as 12.4% and 14% of women in United Kingdom 30 and Canadian studies, 31 respectively. The increasing tendency of change to plant-based diets 32 potentially puts more women at risk of cobalamin insufficiency. 33 Widespread introduction of mandatory fortification of flour with folic acid has been implemented to prevent folate deficiency and prenatal care protocols include recommendations for folic acid supplementation from preconception until the end of the first trimester of pregnancy (at least). No measures have been taken regarding cobalamin intake and generally cobalamin status is not routinely considered in prenatal monitoring.
Imbalance between folate and cobalamin and related metabolites has been reported to be associated in some Indian studies, with adverse maternal and perinatal health outcomes, such as gestational diabetes, 34 small for gestational age, 35 or insulin resistance in the offspring. 15 In the Reus-Tarragona Birth Cohort study, we reported that folate status modified the association between plasma cobalamin and MMA during pregnancy. Of the women with suboptimal first-trimester cobalamin status (≤221 pmol/L) MMA was consistently elevated throughout pregnancy, only in those who had elevated plasma folate status (≥30 nmol/L). 36 The study was limited by low prevalence of suboptimal cobalamin status but further investigation along these lines is warranted because high dose folic acid supplements (1-5 mg) are widely used by pregnant women without knowing their cobalamin status.
Conclusions
Low cobalamin status and adverse outcomes during pregnancy or affecting the offspring in the short- and long-term are not limited to regions of the world with renowned low dietary intake of the vitamin. Plasma cobalamin is susceptible to change during pregnancy and specific reference intervals to pregnancy are needed. Other indicators, such as holoTC and MMA, have revealed some maternal-offspring associations that are missed by measuring plasma cobalamin concentration alone. Studies investigating the association between very early pregnancy cobalamin status and development in the offspring are lacking. Many studies refer to maternal blood samples collected in the second trimester of pregnancy as “early” pregnancy samples. This limitation is also compounded by the lack of pregnancy specific reference ranges for plasma cobalamin and relative lack of studies using alternative indicators of cobalamin status. This review shows that further investigation of the implications of maternal cobalamin status during pregnancy for health and development in the offspring is warranted.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241229502 - Indicators of Cobalamin Status During Pregnancy, Pregnancy Outcome and Long-Term Effects on Offspring Health
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241229502 for Indicators of Cobalamin Status During Pregnancy, Pregnancy Outcome and Long-Term Effects on Offspring Health by Luis Adolfo Santos-Calderón, Alejandra Rojas-Gómez, Carla Ramos-Rodríguez and Michelle M. Murphy in Food and Nutrition Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Reus-Tarragona Birth Cohort study has been supported by grants from The Interministerial Science and Technology Committee (SAF2005-05096); The Carlos III Health Institute, National Scientific Research, Development and Technological Innovation Program Health Investigation Resources, cofinanced by The European Regional Development Fund (FIS10/00335, FIS13/02500, FIS16/00506, FIS19/00844, FIS22/01314); The European Union Horizon 2020 Research and Innovation program (EPIBRAIN project) funded by the Joint Programming Initiative “A Healthy Diet for a Healthy Life” (ERA HDHL), JFA2 Nutrition and the Epigenome, Horizon2020 grant agreement number 696300, with funding provided by The Spanish State Agency for Investigation (PCI2018-093098/AEI). Pere Virgili Health Research Institute (IISPV-2010/21); Biomedical Research Networking Center for the Pathophysiology of Obesity (CIBERobn); Agency for Management of University and Research grants, Generalitat de Catalunya (Support to Research Groups: 2009-1237, 2014-332) and Italfarmaco S.A., Spain. Luis Adolfo Santos-Calderón is a Predoctoral research fellow from the URV Martí-Franques program, Carla Ramos-Rodriguez is a Postdoctoral research fellow from INVESTIGO (AGAUR, Spain), and Alejandra Rojas-Gómez is a Postdoctoral research fellow from the EPIBRAIN project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.