
Abstract
Vitamin B12 (B12) is essential in activating folate needed in DNA synthesis. Inadequate intake results in the impairment of nerve transmission and inadequate synthesis of erythrocytes and other hematological cells. Two separate mechanisms of B12 absorption exist, a receptor-mediated endocytosis that occurs in the distal ileum and the mass-action pharmacologic mechanism. The recommended dietary allowance for B12 for adults issued by the Institute of Medicine is 2.4 µg/d. B12 is only found in meats and other foods of animal origin. B12 deficiency is widespread. Two main causes of deficiency include inadequate absorption and intake. Elderly and vegetarians are at highest risk for deficiency. Prevalence of deficiency ranges from 7% of the US population 3 years and older to 90% among vegans. The best way to assess deficiency is by using methylmalonic acid. Populations at risk could benefit from using B12 supplements and from fortification of flour.
Introduction
Vitamin B12 (B12) was discovered in 1948 by Smith as an antipernicious factor. 1 B12 has the largest and most complex chemical structure of all vitamins. 2 It has been named cobalamin because it contains the rare element cobalt in its chemical structure. Cobalamin belongs to a group of cobalt-containing compounds known as corrinoids that contain a specific corrin ring. Unlike B12 analogues that are inactive in humans, the active forms of B12 have 3 distinct molecules: aminopropanol, sugar (eg, ribose), and a nucleotide attached to the corrin nuclei. 3 Methylcobalamin and adenosylcobalamin are 2 biologically active forms of B12. Other forms such as hydroxocobalamin (or aquacobalamin) and cyanocobalamin must be metabolized to either of the 2 active forms in order to be used in human cells. A specific R-group attached to the cobalt element is what differentiates these forms of B12 chemically.
B12 is only synthesized by microorganisms. B12 is not found in foods of plant origin.
Function
B12 (methylcobalamin) is a coenzyme involved in the transfer of a methyl group in a methionine synthase-requiring reaction that converts homocysteine to methionine. B12 (adenosylcobalamin) is also essential in converting
Digestion and Absorption
B12 is only synthesized by microorganisms. B12 is not found in foods of plant origin. 3 It is, however, found in meats and foods of animal origin, including dairy products and eggs. In foods, B12 is bound to proteins known as R-proteins or R-binders. For B12 to be absorbed, the peptide bond that binds B12 to the protein carrier has to be broken down. The process of digestion and absorption takes place in a few stages and requires adequate synthesis of hydrochloric acid, proteases and an intrinsic factor (IF), a glycoprotein secreted by the parietal cells of the stomach. B12 is released from the R-binders found in foods by the actions of pepsin, an enzyme secreted in the stomach. This enzyme is secreted as pepsinogen and is activated by hydrochloric acid. Once released, B12 binds with R-binders (also known as haptocorrins) secreted with the saliva. Bound to these R-binders B12 travels into the small intestine wherein pancreatic proteases digest the R-binders, enabling B12 to be taken up by IF, forming IF-B12 (or IF-Cbl) complex. 3
There are 2 separate mechanisms of B12 absorption into the blood stream. The first is a receptor-mediated endocytosis that occurs in the distal ileum. IF-Cbl receptor is only expressed in the distal ileum of the intestines. Once inside the enterocytes B12 is released from the IF and it then binds to holo-transcobalamin II protein (TCII), a protein carrier synthesized in the microvascular endothilium of the ileal villi.5,6 Cell membranes internalize the TCII-Cbl complex by a process known as endocytosis.
The second mechanism of B12 absorption has been referred to as the mass-action pharmacologic mechanism. 3 In the presence of large amounts of B12, such as in the case of ingesting B12 supplements, about 1% or less of free vitamin B12 is absorbed by diffusion across the epithelial ileum. This process does not require IF and bypasses IF-Cbl receptors.
Recommendation
The recommended dietary allowance (RDA) for B12 for adults issued by the Institute of Medicine is 2.4 µg/d. 7 The daily amount that is actually needed to maintain adequate serum level to promote erythropoiesis and other hematological functions is considerably smaller but this recommendation assumes a 50% absorption rate of B12 from the amount ingested with foods. The RDA issued by the Institute of Medicine is consistent with recommendations of other organizations. For example, the World Health Organization recommends an intake of 1.9 µg/d, the European Union, 3 µg/d, and the National Research Council, 2 µg/d.7-9 Intake of relatively high doses of B12 does not appear to be associated with any detrimental health problems. Thus, the Institute of Medicine states that there is no sufficient scientific evidence to set a tolerable upper intake level for B12. 7
Food Sources and Bioavailability of B12
B12 in foods comes in several forms, including adenosylcobalamin, hydroxocobalamin, methylcobalamin, cyanocobalamin, and sulfitocobalamin.2,3 Adenosylcobalamin and hydroxocobalamin are the predominant sources in foods. Hydroxocobalamin and methylcobalamin are better absorbed than the other forms. 10 Although B12 is found naturally only in meats and foods of animal origin, some foods believed to be made exclusively from plant foods (eg, cereal, breads, pies, and even cookies) do contain very small amounts of B12 because of either contamination during processing, adding of small amounts of ingredients derived from products of animal origin such as milk solids, or fortification. 11 However, the amount of B12 in the majority of these foods, except foods fortified with this vitamin, is negligible.
The highest amounts of B12 are found in organ meats such as the liver and in clams. The content of B12 in the liver varies from about 3.3 µg in whole chicken liver to more than 70 µg in 3 oz. of beef liver. Most other meats contain between 1 and 3 µg of B12 per 3 oz. Bioavailability of B12 from meats ranges from 10% from liver to as much as 90% from ground-cooked mutton patties. 2 Bioavailability depends on the quantity of meats ingested. B12 content of fish varies from 3.0 to 8.9 µg/100 g (about 3.5 oz). One of the best fish sources of B12 appears to be the dark muscle of skipjack (159 µg/100 g). 2
Milk contains between 0.3 and 0.4 µg B12/100 g. The absorption rate of B12 from milk is about 65%. B12 can be destroyed by heat. Boiling milk can destroy 30% to 50% of B12 depending on the duration of cooking and pasteurization destroys 5% to 10% of B12. The B12 content of dairy products such as cheese or cottage cheese ranges between 20% and 60% of that of milk. 2
B12 content of whole egg is between 0.9 and 1.4 µg/100 g. 2 Most of the B12 in an egg is found in the yolk. Bioavailability of B12 from eggs depends on the preparation method (eg, scrambled egg, boiled egg) ranging from less than 4% to a little more than 9%.2,11,12
Supplements and Fortified Foods
B12 is widely available as supplements in pharmacies and health food stores alike in the United States, mostly as cyanocobalamin. Other forms of this vitamin such as methylcobalamin and hydroxocobalamin can also be found. The dose of cyanocobalamin in supplements ranges from 100 to 5000 µg.
In the United States, many foods are fortified with B12. This includes cereals such as Kellogg’s Special K, Wheat Bran Flakes, Total, Total Raisin Bran, All Bran Original, soymilk, and soy meat analogues such as MorningstarFarms Burger Crumbles. These foods contain from less than the RDA to more than 200% of the RDA for B12. 3 Additionally, 1 tablespoon of nutritional yeast contains 100% or more of the RDA of B12. 13
Bacteria-Synthesized B12 in the Small Intestine
Although a team of researchers led by Albert 14 found that lactobacilli, streptococci, bacteroides, and other enteral bacteria made some B12, this amount does not seem to be adequate to maintain required B12 status in humans. In addition, these researchers used microbiologic assays in assessment of the B12 synthesis and this method measures both the active B12 and inactive B12 analogues. 3 Thus, it is impossible to know how much of the isolated corrinoids was the active cobalamin.
Algae as a Source of B12
Although in the past algae such as spirulina, nori, or kombu were believed to contain B12, Herbert 3 showed not only that they almost exclusively contain inactive analogues of B12 but also that they may interfere with absorption and metabolism of the active B12 forms and thus, may contribute to the development of B12 deficiency.
Assessment of B12 Status
There are several B12 assessment techniques such as serum or plasma B12, TCII, homocysteine (tHcy), serum or urinary methylmalonic acid (MMA), and mean corpuscular volume (MCV). Each assessment technique has varying levels of accuracy in terms of diagnosing B12 depletion or deficiency. Serum or plasma B12 and TCII are direct measure of B12, and tHcy and MMA are metabolites affected by B12 status. MCV is an assessment of the erythrocytes volume. TCII and MMA are the most accurate, whereas serum or plasma B12 and MCV are believed to be unreliable.3,7 TCII can be used to assess B12 depletion, whereas MMA indicates B12 deficiency. 15 Microbiological assay used to measure serum B12 level, although commonly used, is especially unreliable because it measures both active B12 forms along with inactive B12 analogues.
According to Herbert, 15 low serum B12 is a relatively late indicator of B12 deficiency whereas TCII indicates an early B12 depletion. Serum or plasma B12 level includes a total circulating B12 from all B12 carriers, including TCII and haptocorrin. At any given time, at least 80% of B12 is bound to haptocorrin. Haptocorrin values reflect body stores of B12, including B12 stored in the liver. According to Herbert, 15 all cells have receptors for TCII whereas only the liver has receptors for haptocorrin. Thus, depletion of B12 in some cells may develop before hepatic cells are depleted and before serum B12 level shows a subnormal value. Serum assessment may not show low values until hepatic stores are depleted, which consequently will affect haptocorrin B12 values. Haptocorrin has a half-life of approximately 240 hours whereas TCII only 6 minutes. 15 For the reasons mentioned above, TCII is considered more useful in detecting B12 depletion early. 16 Thus, using TCII instead of serum B12 assessment will help in detecting B12 depletion before stores of B12 from the liver are depleted.
It is generally accepted that a level of serum B12 that is less than 200 pg/mL (150 pmol/L) is considered to be B12 deficiency. However, many people show symptoms of B12 deficiency with higher levels of serum B12. Herbert 15 suggested using <300 pg/mL (222 pmol/L) as the cutoff value for deficiency. A value of <35 pmol/L is most often used when assessing B12 status with TCII.
Methylmalonic acid and tHcy are elevated when B12 status is compromised. Both of these metabolites are considered early signs of biochemical B12 deficiency. 16 Elevated tHcy (>12 µmol/L) may also indicate folate or pyridoxine deficiency. Thus, additional tests have to be done to determine B12 status. MMA is considered one of the most reliable assessments of B12. The Institute of Medicine set the normal urine MMA value as 0.58 to 3.56 µmol/mmol creatinine. 7 Different cutoff values for serum MMA have been used, including 210, 260, 271, 370, and higher. 16 MMA is a especially sensitive marker of B12 deficiency; however, MMA, and to a lesser degree tHcy are affected by the renal function and thus in patients with kidneys insufficiency, using them to assess B12 status may be inaccurate.
Normal MCV is between 80 and 96 fL. Higher values indicate a megaloblastic anemia. MCV is affected not only by B12 level but also iron and folate status. Iron deficiency causes microcytic erythrocytes and thus decreases MCV, whereas folate deficiency causes megaloblastic erythrocytes. This is why assessment of MCV is also not reliable to assess B12 status because it also reflects the status of folate and/or iron. In addition, MCV values may be normal with high folate intake even in the presence of B12 deficiency.
Several researchers suggested using more than one assessment methods such as TCII and MMA or tHcy and MMA to evaluate B12 status. Although MMA is considered the most sensitive marker of B12 status, it is also the most expensive and this makes is less attractive for clinical use than TCII or tHcy. 16
Deficiency
Although once thought that B12 deficiency is rare and unlikely to develop, except in strict vegetarians, studies conducted in the past few decades showed that this view has been based on the incorrect assumption, that it takes many years for the deficiency to develop.17-21 These studies showed that B12 deficiencies are common in both developing and wealthier countries. Deficiency is particularly high among the elderly and vegetarians, but it is also prevalent among pregnant women and children, especially in less developed countries. 17 Studies showed that B12 deficiency is common among people of European and African descents, Indian subcontinent, Central America, and South America. In Asia, B12 deficiency is less prevalent except in vegetarians. 18
B12 deficiency may occur as a result of malabsorption due to a gastrointestinal condition, inadequate intake, lack of synthesis of TCII, a genetic defect of methylmalonyl coenzyme A mutase, or nitrous oxide poisoning. Malabsorption may have 2 primary causes: inadequate or complete inability of synthesis of IF and/or inadequate synthesis of or synthesis of weak hydrochloric acid, essential in activating pepsinogen to pepsin that digests dietary R-proteins. Although malabsorption due to the above-listed conditions is most prevalent among the elderly, it may occur at any age among people who have undergone gastrectomy such as in ulcer disease, gastric bypass for obesity, patients with celiac disease, Crohn’s disease, and those receiving chemotherapy. Deficiency due to inadequate intake has been reported in strict vegetarians, lacto-ovo-vegetarians, people following a macrobiotic diet, those who follow some form of raw food diets, children with regular disturbance in feeding behavior especially coupled with increased metabolic demand, and alcoholics. Also, mild B12 deficiency is common in many countries with relatively low intake of meat and animal products such as Guatemala, Mexico, or Venezuela.19-21
The rate of B12 deficiency reported in studies depends largely on several factors, including the assessment method and cutoff points used. Deficiency prevalence may have been underestimated in studies that used serum B12 assessment for the reason described earlier.
According to the National Health and Nutrition Examination Survey data reported by Pfeiffer et al, 22 7% of the US population 3 years and older has elevated MMA (>370 nmol/L). The rate of B12 deficiency among elderly (>60 years) Latinos from California participating in the SALSA study was 27.6% and an additional 40.3% had marginal B12 status. 23 Twenty-three percent of the elderly from Georgia were diagnosed with B12 deficiency in a study led by Johnson 24 (MMA > 271 nmol/L).
Using MMA as the indicator of B12 status, B12 deficiency has been reported in between 55% to slightly more than 85% in children adhering to macrobiotic diets (deficiency defined as >430 nmol/L), 41% of adolescents formerly on macrobiotic diet (deficiency defined as >290 nmol/L), 31% of adult lacto-ovo- or lacto-vegetarians who were taking supplements (deficiency defined as >260 nmol/L), 47% of Chinese vegetarian women 55 years and older (deficiency defined as >0.4 µmol/L), and 68% among Buddhist and Taoist monks living in Hong Kong (deficiency defined as >0.4 µmol/L).19,20,25,26 Deficiency among lacto-ovo-vegetarians and vegans from Germany and the Netherlands was between 68% and 90%.25-29 B12 deficiency is relatively high among people in the developing world such as countries in South America with relatively low meat and animal products intake. Some studies showed a deficiency rate of 50% or higher.19,20
In rare cases, deficiency may also occur because of lack of or inadequate synthesis of TCII. TCII is the protein carrier of B12 to all cells in the body, including transport of B12 from intestines via the portal vein. Also, in even rarer cases, a genetic defect of methylmalonyl coenzyme A mutase, essential in the breakdown of some amino acids, is a cause of deficiency. In addition, all people who undergo a surgery under anesthesia should be screened for B12 deficiency because nitrous oxide causes irreversible oxidation of cobalt, deactivating B12. 30
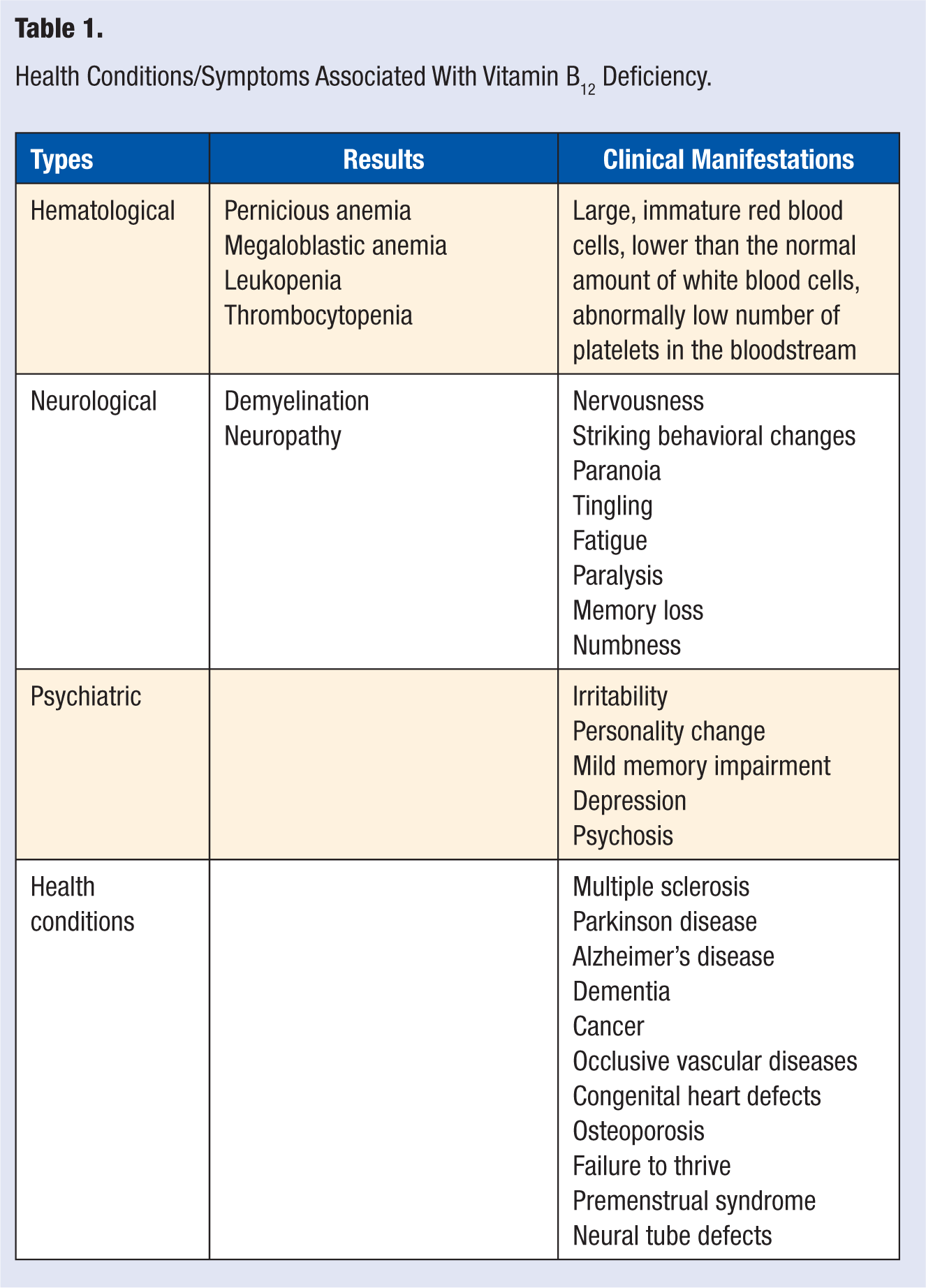
B12 deficiency symptoms can be grouped into several categories, including hematological, neurological, and psychiatric. Specific symptoms of B12 deficiency in each of the above categories are listed in Table 1. Although description of symptoms of B12 deficiency has been widely published, deficiency of B12 is very often misdiagnosed. This is because these symptoms mimic symptoms of other health conditions such as Alzheimer’s disease, spinal cord compression, amyotrophic lateral sclerosis, diabetic peripheral neuropathy, alcoholic peripheral neuropathy, and congestive heart failure.31,32 The classic B12 deficiency symptoms include synthesis of large, immature, oblong-shaped erythrocytes (megaloblasts) and myelin deterioration in both central and peripheral nervous systems. 32 Megaloblastic anemia leads to symptoms such as weakness, fatigue, lightheadedness, tachycardia, angina, and pale skin. 7 However, high intakes of folate and iron-deficiency anemia can mask the megaloblastic symptoms, making assessment of erythrocytes volume an unreliable assessment tool for B12 status. The deterioration of myelin may progress to axonal degeneration and even axonal death, which leads to neuropathy.
Health Conditions/Symptoms Associated With Vitamin B12 Deficiency.
Toxicity
Hydroxocobalamin taken in high dose has been associated with acne-like dermatological effect. 33 Cyanocobalamin does not exhibit similar association. It has been hypothesized that the dermatological effect seen after ingestion of hydroxocobalamin was due to degradation products of hydroxocobalamin rather than hydroxocobalamin itself. 33 A tumor-promoting effect of high doses of B12 has been suggested based on studies on rats. 34 However, neither carcinogenic nor mutagenic effects of B12 were confirmed in human studies even when mega doses of B12 were used for a very long time.35-37 No symptoms of toxicity were reported among patients with pernicious anemia, patients on dialysis, and geriatric patients. Even in studies where a dose of 1000 to 2000 times greater than the RDA for several months to a few years were used, no symptoms of toxicity were reported.35-37 Thus, it is commonly accepted belief that B12 does not appear to have any toxic side effects even when mega doses of B12 are used as supplements, in parenteral administrations, or in injections.7,38
Discussion
B12 deficiency is a prevalent nutrient deficiency resulting from a variety of factors, including inadequate intake and absorption. In the United States, to prevent B12 deficiency, people 50 years and older are recommended to take supplements of this vitamin, as stated in the Dietary Guidelines for Americans document. 39 It is, however, reasonable to assume that the majority of people in this age-group are not aware that they should be taking B12 supplements. Furthermore, although some vegetarians may be aware of the risk, many do not supplement B12 for a variety of reasons, including common misconceptions such as that a deficiency develops only in strict vegetarians after many years of following such a diet. 40 In fact, the popularity of this misconception is not exclusive to some vegetarians. It has been disseminated in some scientific publications and even in a statement published on the National Library of Medicine’s Web site. 41 B12 deficiency is widespread and is associated with many adverse health outcomes from mild, such as forgetfulness and lack of energy, to severe, such as loss of smell, neural tube defects, multiple sclerosis, Alzheimer’s disease, and inability to work.
Although taking a B12 supplement has been shown to be effective in both prevention and treatment of B12 deficiency, there is little effort on the part of public health officials to promote its use. Also, as already indicated, some groups of vegetarians resist taking B12 supplements. Furthermore, the experience with promoting the use of folic acid–containing supplements to prevent neural tube defects has shown that promotion campaigns are largely ineffective. 42 Many years since such recommendation was first issued by the Center for Disease Control and Prevention, women are still unsure of what is the best time to use them, the dose, and the form of folic acid. 42 This experience indicates it may take a very long time to increase awareness of the prevalence of B12 deficiency and any efforts to combat this epidemic may be ineffective.
Some scientists have proposed fortification of flour with B12. 22 Fortification of flour with folic acid contributed to an increase in folic acid content of red blood cells, decreased total homocysteine and consequently, a reduction in rates of neural tube defects. 22 It is reasonable to assume that this preventive measure would have the same effect in terms of reduction in B12 deficiency and its associated symptoms. Oakley and Tulchinsky 43 suggested that B12 deficiency symptoms would disappear if mandatory fortification of flour with B12 was implemented in Europe. However, the benefits of fortifying products such as flour with B12 can only be accomplished if adequate dose of B12 were used. Different doses of B12 fortification have been proposed, including 1, 10, and 20 µg per 100 g of flour.44-46 Although these proposed doses range from about 50% of the US RDA to almost 9 times higher than that RDA, only about 1% of the crystalline form of B12 can absorbed. Carmel 47 suggested that fortification of flour with just 1 to 10 µg will be ineffective in preventing B12 deficiency among the most vulnerable groups such as the elderly. In fact, Carmel suggested that if a total intake of B12 is less than 100 µg in the elderly, it would neither prevent the deficiency nor replenish the body’s stores of B12. Thus, for the best benefit, flour would have to be fortified with a dose of 100 µg or higher per 100 g. Cyanocobalamin is the most stable of all B12 forms and thus it is the best candidate to use in fortification.