
Abstract
Background:
An optimal cobalamin status is necessary for normal neurodevelopment.
Objective:
To give a description of the epidemiology, pathophysiology and diagnostic challenges related to cobalamin insufficiency in neonates and infants in order to prevent its occurence.
Results:
Inadequate cobalamin status is prevalent among neonates and young infants, due to a high prevalence of maternal cobalamin deficiency, exclusive breastfeeding for extended periods and late introduction of animal food. Cobalamin insufficiency is associated with delayed neurodevelopment and subtle clinical symptoms like feeding difficulties, regurgitations and constipation in young infants. Early diagnosis and treatment of impaired cobalamin status is important to prevent neurologic damage.
Conclusion:
Clinical suspicion of cobalamin insufficiency in infants should infer immediate biochemical testing and a plasma total homocysteine > 5.0 µmol/L indicate cobalamin insufficiency in need of intramuscular treatment with hydroxycobalamin, followed by introduction of animal food after 4 months of age.
Plain language title
Vitamin B12 Is Important for Normal Development in Young Children
Plain language summary
Vitamin B12, also called cobalamin, is found only in animal-sourced food. As low-meat, vegetarian, and vegan diets are increasingly popular in Western countries, vitamin B12 deficiency has become common, also in pregnant women and babies. Vitamin B12 status is essential for normal development and adequate levels of this vitamin is particularly important during pregnancy and the first years of life. In pregnancy, vitamin B12 is transferred from the mother to the fetus, so the baby has a store of this vitamin at birth. However, if the mother has vitamin B12 deficiency or the baby is born premature or with a low birth weight, the vitamin store may be insufficient and the baby may develop vitamin B12 deficiency. Maternal vitamin B12 status is important as long as the baby is exclusively breastfed. Breast milk contains vitamin B12, but the concentration decreases after 4 to 6 weeks and may be too low to support the baby until animal-sourced foods are introduced. The vitamin B12 content in formula milk is higher than in breast milk, and vitamin B12 deficiency is more common in exclusively breastfed babies. Vitamin B12 deficiency is associated with diffuse symptoms in small babies and may be difficult to detect, and the diagnosis have a mean delay of 4 months in this age-group. Typical symptoms are regurgitations or spitting up, constipation, problems with feeding and swallowing, and delayed psychomotor development. Suspicion of vitamin B12 insufficiency in babies should prompt immediate biochemical testing. Plasma total homocysteine is a metabolic marker of vitamin B12 status and can be measured in a blood sample from the baby. A level >5.0 µmol/L indicates probable vitamin B12 insufficiency and the baby should receive vitamin B12 supplementation, followed by introduction of animal-sourced foods at 3 to 4 months of age.
Introduction
An adequate cobalamin (vitamin B12) status is essential for normal neurodevelopment during fetal life and infancy, as demonstrated by inborn errors of cobalamin metabolism and published case reports. 1 -3 Severe cobalamin deficiency in early life can cause permanent neurological deficits, but even moderate cobalamin deficiency is associated with delayed psychomotor development and clinical symptoms, like tremors, regurgitations, feeding difficulties, and constipation in infants. 4 -6 Intervention studies show that cobalamin supplementation improves psychomotor development and symptoms in infants with cobalamin insufficiency, 7,8 confirming the importance of an optimal cobalamin status in infancy. Early treatment is essential to ensure optimal neurodevelopment and prevent irreversible neurologic damage, but the challenge lies in diagnosing the patients.
Factors Determining Cobalamin Status in Neonates and Infants
The cobalamin status of a neonate depends on maternal cobalamin status during pregnancy, placental function, and gestational age at birth. 4 There is a strong dose–response relation between markers of maternal cobalamin status in pregnancy week 18 and infants at 6 months of age. 9 A maternal serum cobalamin concentration >275 pmol/L measured by routine laboratory methods at week 18 of pregnancy is reported to secure an optimal infant cobalamin status during the first 6 months of life. 9,10 Maternal cobalamin deficiency, prematurity, and low birth weight are all associated with lower fetal cobalamin stores and risk of deficiency, particularly if the infant is exclusively breastfed. 8,11,12 In recent years, vegetarian and vegan diets have become increasingly popular in Western societies, 13 particularly among young women, 14 imposing a risk for cobalamin deficiency in the infant, even when supplements are used during pregnancy. 2,15,16
As long as the infant is exclusively breastfed, maternal cobalamin status will continue to have an impact. Total cobalamin concentration in human milk falls progressively during the lactation period, 17 and in exclusively breastfed term infants with adequate birth weight, a biochemical profile indicative of impaired cobalamin status is reported to be common from 4 months. 4 As formula is supplemented with several B vitamins, deficiency is uncommon in formula-fed infants. 18
Exclusive breastfeeding for extended periods is associated with short- and long-term feeding difficulties, 19,20 which may postpone weaning, thereby increasing the risk of cobalamin deficiency. Approximately 50% of Norwegian infants start with porridge, fruit, and vegetables between 4 and 6 months of age. The introduction of animal-sourced foods is usually postponed until after 6 months and the portions are initially small, 21 something which increases the risk of cobalamin deficiency during infancy.
Prevalence of Cobalamin Deficiency
Cobalamin deficiency in infants has traditionally been considered to be a problem in countries with endemic cobalamin deficiency, 4 but expanded newborn screening and infant studies have detected a high prevalence of cobalamin deficiency in both Europe and the United States. 22 -27 Depending on the decision limit used, the prevalence of cobalamin deficiency in newborn screening varies from 1:1989 to 1:17 837 27 and in infants from 13% to 66%. 28,29
As serum cobalamin progressively decreases during pregnancy, 9 prevalence data of cobalamin deficiency in pregnant women depend on which pregnancy week the test was applied. Women with a low intake of animal-sourced foods, malabsorption due to disease or bariatric surgery are particularly at risk. 4,16,30 The prevalence of cobalamin deficiency in pregnancy is reported to be high, 16,31 from 72% in Turkey (serum cobalamin <118 pmol/L) 23 to 5% in Canadian women in early pregnancy (<125 pmol/L). 32 Cobalamin deficiency is reported to be prevalent also in lactating mothers. At 5 weeks postpartum (range 0-20 weeks), 41% of German mothers had a serum cobalamin concentration below 160 pmol/L. 33
Clinical Signs of Impaired Cobalamin Status in Infants
The symptoms and signs of cobalamin deficiency in childhood depend on the age of the child and the severity and duration of the deficit. 34 Classical signs are delayed neurodevelopment and neurological symptoms, 35 but severe cobalamin deficiency may be associated with reduced weight, length, and head circumference, 36,37 as well as macrocytic anemia. 37,38 In contrast, moderate deficiency is associated with normal or even increased weight 39 -41 and normal hematological parameters. 40,42,43 Symptoms may appear as early as the second month of life 35,44 and include feeding difficulties, regurgitations, constipation, apathy, irritability, twitching, tremors, myoclonic jerks, and developmental delay with reduced gross motor development, as well as reduced smiling and babbling. 7,35,38,45
Diagnosing cobalamin insufficiency in young infants may be difficult, as there are large variations in normal psychomotor development 46 and minor developmental delays may not be considered abnormal in this age-group. 47 Doctors may be uncertain about the degree of delay that deserves evaluation and may also have concerns about causing parental anxiety. 47
Subtle symptoms associated with infant cobalamin deficiency, like tremors, regurgitations, and feeding difficulties, are very common in young infants. 48 -50 In a population-based study, 55% of the infants suffered from gastrointestinal symptoms, of which regurgitation was the most common, followed by colic, constipation, failure to thrive, vomiting, and diarrhoea. 47 Consequently, cobalamin deficiency may be overlooked in the youngest age groups and cobalamin deficiency has a reported median diagnostic delay of 4 months in infants, 35 which is particularly concerning during a period of rapid brain growth and development. 51
Biochemical Markers of Cobalamin Status in Children
Cobalamin status undergoes marked changes during infancy and childhood. 43,52 During the first weeks of life, serum cobalamin decreases by approximately 30%, and the lowest cobalamin concentrations are seen in exclusively breastfed infants aged 4 to 6 months. 43,53 -57 After the introduction of animal-sourced foods containing cobalamin, which usually happens around 7 to 8 months, 58 serum cobalamin increases and peaks at 3 to 7 years and then gradually decreases to levels seen in adolescents and adults. 43
As serum folate concentrations are very high in infants and young children, plasma total homocysteine (tHcy) is considered the primary metabolic marker of cobalamin status in this age-group. 43 In older children and adults, plasma tHcy becomes more of a metabolic marker of intracellular folate status.
Figure 1 is based on published data from 173 newborns aged 4 days 59 and shows that plasma tHcy progressively changes over what is considered to be a normal cobalamin range (200-500 pmol/L). Plasma tHcy gradually starts to increase when serum cobalamin falls below 700 to 800 pmol/L, with a steeper increase below 300 to 400 pmol/L (Table 1). The same metabolic pattern is seen in older infants and indicates that there is a gradual transition from an optimal to a deficient intracellular cobalamin status below a serum cobalamin concentration of 800 pmol/L.
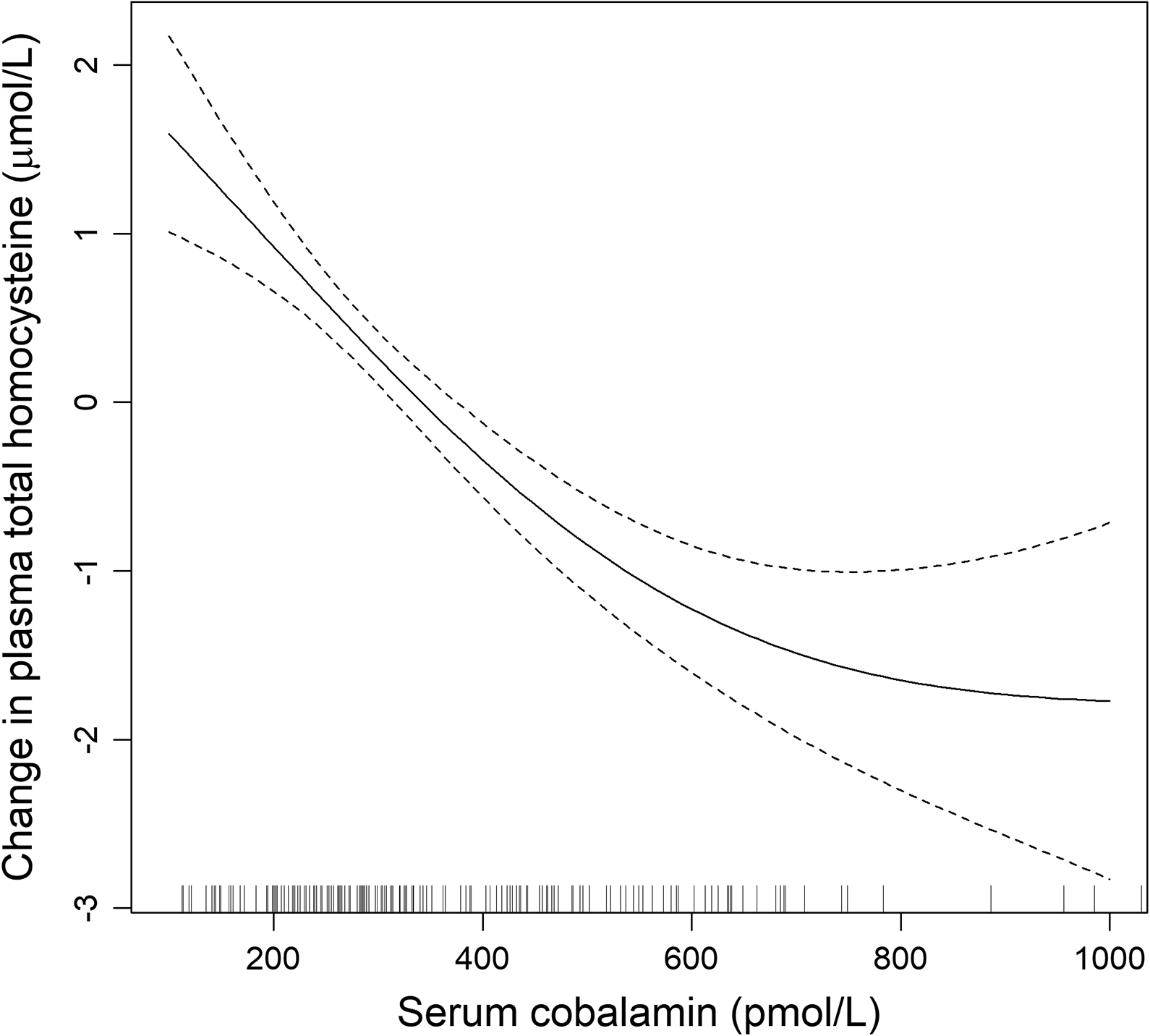
Serum cobalamin concentrations in relation plasma total homocysteine (tHcy) in newborns aged 4 days, by generalized additive models (GAM). The values on the y-axes represent the difference from the mean plasma tHcy concentration.
Plasma Total Homocysteine in Relation to Serum Cobalamin in Newborns Aged 4 Days.a

a N = 173.
b Median, (25th, 75th percentile) compared by Kruskal-Wallis test.
Serum methylmalonic acid (MMA) is inversely related to circulating cobalamin. It is a marker of cobalamin status, but during the first years of life, the MMA concentrations are higher through the whole range of cobalamin concentrations compared to older children and adults. 43 The causes of the higher MMA levels in young children are uncertain, but it may be the result of increased intestinal absorption of propionate and MMA precursors produced by intestinal bacteria or degradation of odd-chain fatty acids present in milk. 43,60
Strategies for Classifying Vitamin Status
Many laboratories use reference values for serum cobalamin, of which the lower 2.5 percentile is often considered a marker for deficiency. 61 However, the reference values for micronutrients vary according to the diet of the population on which the reference range is based and do not tell us whether the status is adequate or not. We should preferably define micronutrient decision limits based on a vitamin-replete status. 61
Traditionally, decision limits for micronutrients have been based on clear signs and symptoms of depleted stores, but there is an increasing awareness that also subclinical deficiencies may have a negative impact on development and health. 62 Decision limits may therefore vary over time depending on the chosen outcome parameter, exemplified by the different decision limits for serum folate published by the World Health Organization (WHO) over the years. In 1968, the decision limit for serum folate was 6.8 nmol/L and based on the presence of megaloblastic anaemia, that is, a severe vitamin deficiency causing clinical disease. 63 In 2005, WHO chose a decision limit of 10 nmol/L for folate deficiency based on changes in the metabolic marker tHcy. 64 In 2015, a decision limit of 25.5 nmol/L in fertile women was chosen for optimal neural tube defects prevention. 65,66 The relation between serum folate and plasma homocysteine in older children and adults resembles the metabolic pattern observed for serum cobalamin and plasma homocysteine in Figure 1. Plasma tHcy starts to increase when serum folate falls below 25 to 27 nmol/L, indicating suboptimal intracellular folate status and increases sharply when serum folate falls below 10 nmol/L, indicating intracellular folate deficiency. 67
What Decision Limits Should Be Used for Cobalamin Status?
There is no clear agreement on what constitutes deficient or optimal cobalamin status in either children or adults. 4 The lower decision limit for cobalamin deficiency (<148 pmol/L) is based on the presence of clinical deficiency symptoms, decision limits in the range of 200 to 250 pmol/L are based on changes in the metabolic markers tHcy and MMA, 4 while molecular studies show that serum cobalamin concentrations need to be >300 pmol/L in order to minimize DNA damage. 68
In newborns aged 4 days, a serum cobalamin cut-point value of 359 (95% CI = 332-391) pmol/L was obtained by segmented regression, with plasma tHcy concentration as the dependent variable (Figure 1). This serum cobalamin concentration might be used as a decision limit for cobalamin deficiency in newborns and infants; however, as the figure shows, plasma tHcy is not stabilized until serum cobalamin is >700 to 800 pmol/L, indicating cobalamin insufficiency and possibly also associated impaired neurodevelopment below these levels.
Plasma tHcy is a suitable marker for cobalamin status in infants. It is possible to reduce tHcy by cobalamin supplementation, implying that high plasma tHcy concentrations in young infants reflect cobalamin insufficiency and not organ immaturity. 7,69 Higher plasma tHcy concentrations are related to impaired neurodevelopment in infants. 5,7,8,53 A dose–response reduction in AIMS score, an observational tool for evaluating gross motor development, 70 with increasing levels of tHcy and MMA were seen in infants at 6 months 8 and an increase in Alberta Infant Motor Scale (AIMS) score with decreased tHcy levels have been confirmed in randomized, controlled cobalamin intervention studies in young infants. 7,8
A plasma tHcy concentration of 6.5 µmol/L has been suggested as a decision limit for impaired cobalamin function in infants. This cutoff represented the 97.5th percentile in 4 months old infants given a single intramuscular dose of 400 µg hydroxycobalamin at 6 weeks and was considered a vitamin-optimized value. 28 However, the chosen plasma tHcy decision limit might be too high. The infants received a moderately low cobalamin supplement dosage and the plasma tHcy 97.5th percentile more than 2 months later might include infants with deficient cobalamin status. In the cobalamin-treated infants, the median plasma tHcy concentration was 4.6 µmol/L (IQR = 4.0-5.1) µmol/L. The same plasma tHcy range is seen in neonates with serum cobalamin concentrations >500 pmol/L (Table 1). A plasma tHcy concentration below 5.0 µmol/L (the 75th percentile) might be a more appropriate decision limit for securing an adequate cobalamin status in neonates and infants.
When defining decision limits for newborn screening of cobalamin status, 27 one has to take into account the expected 30% reduction in serum cobalamin and the increase in plasma tHcy, which appear during the first weeks of life in exclusively breastfed infants. 43 If the decision limit for plasma tHcy level is too high, infants at risk of developing a deficiency in the following weeks might escape attention.
How Much Cobalamin Is Needed in Infants?
Adequate cobalamin intake (AI) for infants aged 0 to 6 months is approximately 0.4 μg/day, based on the assumption that breast milk contains sufficient cobalamin for optimal health during this period of life. 71 The AI is calculated based on an average intake of breast milk of ∼800 mL/d and an average cobalamin concentration in breast milk of ∼0.45 μg/L. Whether this amount of cobalamin is enough will depend on infant cobalamin stores, which will be low in premature and low birthweight infants, and in infants born to cobalamin-deficient mothers.
Only 28% of infants at 6 weeks and 34% at 4 months achieve the recommended intake of 0.4 µg cobalamin per day from breast milk. 9 As cobalamin insufficiency is reported to be common among young infants, the assumption that breast milk contains enough cobalamin for optimal health during the first 6 months of life does not seem to apply to most infants. 28,40,49,65,67
The dosage of 400 µg hydroxycobalamin given intramuscularly in intervention studies in infants represents approximately twice the total amount of cobalamin considered necessary for the first year of life (0.4 µg/d for the first 6 months of life and 0.5 µg/d for the next 6 months). 71 The dosage necessary for treatment of cobalamin deficiency in infants must depend on the severity of deficiency, age, and weight of the patient and might be increased to 1 mg hydroxycobalamin. If the infant has deficiency symptoms, cobalamin should be given as an intramuscular injection for rapid cure. Unless the infant has very low stores and is still exclusively breastfed, it is usually not necessary to repeat the intramuscular treatment. It is advisable to control serum cobalamin and plasma tHcy levels to see whether the patient has achieved and maintains an optimal status and if necessary, cobalamin supplementation should be repeated. There are no known adverse effects of excess cobalamin intake. 72
Implementation of animal-sourced foods should start as soon as possible. Introduction of solid food at age 3 months in breastfed infants do not affect the growth or the duration of breast-feeding and may also reduce food allergy. 73,74
Conclusion
Cobalamin deficiency is prevalent among young infants due to low maternal cobalamin status, exclusive breastfeeding for extended periods and late introduction of animal food. Optimal cobalamin status is essential for normal neurodevelopment, and early diagnosis and treatment of cobalamin insufficiency are vital to prevent irreversible neurologic damage. Clinical diagnosis of cobalamin deficiency is difficult in young infants, and suspicion of cobalamin insufficiency should prompt immediate biochemical testing. A plasma tHcy >5.0 µmol/L indicates cobalamin insufficiency in need of cobalamin supplementation. In infants with clinical symptoms of cobalamin deficiency, an intramuscular injection of 0.4 to 1 mg of hydroxycobalamin, adjusted for deficiency severity, age, and weight, should be promptly given. Decision limits for cobalamin status used in newborn-screening programs must take into account the expected 30% reduction in cobalamin status which occurs during the first weeks of life.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241227782 - Defining Optimal Cobalamin Status for Neonates and Infants
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721241227782 for Defining Optimal Cobalamin Status for Neonates and Infants by Anne-Lise Bjørke-Monsen in Food and Nutrition Bulletin
Footnotes
Acknowledgments
The author thank Paul Kjetil Soldal Lillemoen at Department of Medical Biochemistry and Pharmacology, Haukeland University Hospital, Bergen, Norway, for help preparing the figure.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.