
Abstract
Plant-based diets are increasingly popular worldwide. A well-planned plant-based diet lowers the risk of cardiovascular disease, type 2 diabetes and certain cancers. In contrast, a poorly planned plant-based diet increases the risk of certain micronutrient deficiencies, chiefly, vitamin B12 (B12). Because B12 is not present in plants or in unfortified plant-based foodstuffs, the safest way to prevent its deficiency in plant-based diets is to take an oral B12 supplement. Studies determining the dose and frequency of B12 to be taken by healthy individuals on a plant-based diet to support an adequate B12 status are scarce. Here, we summarize the natural sources, metabolic requirements, biomarker findings with and without supplementation with B12, and current recommendations to help prevent vitamin B12 deficiency in healthy individuals adhering or transitioning to plant-based diets. This review focuses on the prevention of vitamin B12 deficiency in healthy individuals adhering to plant-based diets. The information covered in this review does not apply to individuals suffering from autoimmune-based malabsorption of vitamin B12 resulting from pernicious anemia due to atrophic gastritis, other acquired causes of B12 malabsorption or to those with genetic disorders that impair vitamin B12 absorption, transport and utilization.
Plain language title
Vitamin B12 in Plant-Based Diets
Plain language summary
Plant-based diets are increasingly popular worldwide. Because vitamin B12 is not found in plants, individuals must acquire the micronutrient by consuming fortified foods or by taking an oral vitamin B12 supplement. We review B12 sources, required daily intake, and use of B12 supplements among those on plant-based diets. The safest way to prevent B12 deficiency in individuals adhering to plant-based diets is by using an oral B12 supplement.
Natural Sources and Chemical Forms of Vitamin B12
Vitamin B12 is a water-soluble vitamin synthesized exclusively by a few groups of microorganisms. 1 -6 Omnivores obtain vitamin B12 by consuming animals that are environmentally exposed to vitamin B12 produced by microorganisms. Because B12 is not found in plants, humans adhering to unsupplemented plant-based diets have an increased risk of developing B12 deficiency. Edible mushrooms 7 and commercial sauerkraut 8 have highly variable quantities of B12, therefore they are not a reliable source of the micronutrient. A cultivated aquatic plant has been found to contain bioactive B12 material. 9 Much like humans, certain algae depend on the acquisition of B12 from the environment to support function. Such algae employ specialized transport proteins to acquire the micronutrient from their natural ecosystems. 10 This makes algae a potential source of B12 for individuals adhering to plant-based diets. A recent study that examined 57 nutritional supplements found that certain algae such as Chlorella sp contain vitamin B12 in substantial quantities. 11 However, the same study showed that other types of algae, such as Spirulina sp, 11 contain little to no B12 and instead carry large quantities of the structural analogue pseudo-B12, which does not support function in humans. The effects of B12-analogue consumption in humans, as would possibly occur when using Spirulina sp as the sole source of B12, have not been investigated. Because the presence of B12 analogues in blood has, in a few cases, been correlated with severe neurological impairment, 12 the safest way to secure an adequate intake of B12 in plant-based diets is the use of supplements that contain pure B12. The biologically active forms of vitamin B12 include cyanocobalamin (CNCbl), hydroxocobalamin (HOCbl), methylcobalamin, and adenosylcobalamin. In healthy individuals, all of these chemical forms are absorbed and processed to support physiological needs. The enzyme MMACHC processes all 4 chemical forms of B12 into a common intermediate that can be used by the 2 B12-dependent enzymes, methionine synthase (MS) and methylmalonyl-CoA mutase (MUT). 13 There is no proven superiority of one chemical form of B12 over another to supplement healthy individuals. 14 Most commercial supplements contain CNCbl.
Requirement for Vitamin B12 in Human Physiology
Humans require vitamin B12 to support the activity of the enzymes MS and MUT. Deficiency of vitamin B12 impairs the activity of the 2 vitamin B12-dependent enzymes, which manifests in the elevation of their respective substrates, homocysteine (Hcy) and methylmalonic acid (MMA). 15 Cells that lack vitamin B12 produce larger than normal quantities of Hcy and MMA, which are exported into the extracellular milieu, and can therefore be measured in plasma and urine. The absorption of food B12 and supplemental free B12 is a complex process. Food B12 is mostly bound to proteins (MS, MUT, haptocorrin [HC], and transcobalamin [TC]). Free B12, whether in food or taken in as an oral supplement, will bind to HC in saliva and the stomach. B12 is liberated from proteins by digestion and binds to gastric apo-IF (apo-intrinsic factor) to form holo-IF, which is then largely absorbed by enterocytes in the ileum. 16,17 After release from IF, B12 enters portal circulation and binds to both apo-TC and apo-HC. Only the fraction of B12 bound to TC, known as holo-transcobalamin (holo-TC) is the bioactive fraction of B12 that undergoes uptake by all cells in the body. 18 Apo-HC also binds B12 analogues and is probably involved in their removal from circulation through the enterohepatic circulation of cobalamins. 19,20 Asialo-holo-HC is cleared by the liver. 21 Thus, total plasma vitamin B12 (holo-TC + holo-HC + trace free B12) and specifically holo-TC are 2 biomarkers of vitamin B12 status. In healthy individuals, these 2 biomarkers respond to and reflect the dietary and supplemental intake of vitamin B12. Individuals taking large amounts of supplemental B12 absorb small amounts by passive diffusion along the gastrointestinal (GI) tract. By this nonphysiological process, it is estimated that approximately 1% of a 1000 to 2000 µg dose of CNCbl is absorbed (10-20 µg). 22 Thus, large daily doses of CNCbl have been used to successfully treat subjects with pernicious anemia. 23,24 Absorption by this nonphysiological process appears to occur across the entire length of the GI tract. 25
The Challenge of Acquiring Enough Vitamin B12 in the Era of Sustainability
Humans and other animals are B12-auxotrophs and, therefore, they must acquire B12 from the environment. 26 Omnivores are protected from a low intake of B12 by the consumption of animals or animal-derived products (dairy, eggs) that have previously acquired vitamin B12 from the environment. This mode of acquisition of vitamin B12 is effective in that it supplies sufficient quantities of the micronutrient; however, it is also more environmentally taxing compared to using oral supplementation while on a plant-based diet. Firstly, the consumption of foodstuffs derived from animals contributes significantly to water and land wasting and to greenhouse emissions. 27 -30 Secondly, the upscaling of meat production to satisfy increasing planetary demands has led to live-stock being husbanded under conditions wherein supplementation with either cobalt (to supply rumen microbes with the metal for B12 biosynthesis) or with parenteral vitamin B12 (to treat cobalt deficiency) are necessary for their own health and growth. 31 -34 This requirement appears to be linked to unnatural feeding conditions typical of intensive animal agriculture, as free grazing animals do not have a need for supplementation with vitamin B12. 34 Thirdly, the high demand for meat on the planet does not permit the feeding of all humans with free-ranging grazing animals. Since the transition toward plant-based diets that are devoid of B12 is unavoidable, every effort should be made to prevent B12 deficiency in vegetarians and vegans. Vegetarians obtain vitamin B12 primarily from dairy and eggs, whereas vegans rely on the use of supplements or fortified foods. Two recent studies have identified types of algae (in addition to Chlorella sp) and an aquatic duckweed plant that contain substantial amounts of vitamin B12. 9,10 This presents as a potentially new source of vitamin B12 for human consumption, in particular, ones that are compatible with all diets including vegan.
Intake of Vitamin B12 in Plant-Based Populations
The intake of vitamin B12 decreases proportionally to the greater sustainability of the diet, in rank-order omnivore > flexitarian > vegetarian > vegan. 35 This trend is applicable to all ages, from neonates to the elderly. The European Food Safety Agency (EFSA) recommends a daily intake between 1.5 µg/d (infants 7 to 11 months old) and 4.0 µg/d (children aged 15-17 years and adults), and between 4.5 and 5.0 µg/d for pregnant and lactating women. 36 The National Institutes of Health (NIH, USA) recommend 0.4 to 2.4 µg/d depending on age (adults > 19 years old: 2.4 µg/d), 2.6 µg/d for pregnant women, and 2.8 µg/d for lactating women. 37 The National Health Systems (NHS) in the United Kingdom recommend 1.5 µg/d for adults between 19 and 64 years old. 38 The DACH reference values for nutrient intake are jointly issued by the nutrition societies of Germany, Austria, and Switzerland. 39 The revised values are as follows: a range from 0.5 to 4.0 µg/d for children and adolescents, 4.0 µg/d for adults, 4.5 µg/d for pregnant women, and 5.5 µg/d for lactating women. 39 The Nordic Nutrition Recommendations (NNR) 2023 have increased the recommended intake for B12, in line with the recommendations of EFSA, to 4.0 µg/d for adult males and females. 40 A systematic analysis of vitamin B12 intake with respect to vitamin B12 status in groups vulnerable to B12 deficiency (including 4 studies on vegetarians and vegans) failed to conclude whether habitual B12 intake per the NNR is sufficient to support adequate vitamin B12 status in all vulnerable groups, and strongly encouraged population-based cohort studies. 41 A systematic review of 13 publications determined that the intake of vitamin B12 in children and adolescents following vegetarian and vegan diets does not meet the estimated average requirement. 42 When excluding the use of B12 supplements, the average B12 intakes calculated from 10 independent studies were 3.49, 1.66, and 0.59 µg/d for meat-eaters, vegetarians, and vegans, respectively. 42 This pattern changed when the analysis considered intake including B12 supplements, as follows: 28.8, 5.2, and 116.6 µg/d for meat-eaters, vegetarians, and vegans, respectively. 42 This implies that vegetarians do not consume supplemental B12 as much as do vegans. A study performed in a cohort of Swiss adults who have been omnivore, vegetarian, or vegan for at least 1 year showed a similar pattern of B12 intake. 43 Omnivores, vegetarians, and vegans had an intake of 4.1, 1.6, and 0.2 µg/d, respectively. In this study, both vegetarians and vegans had B12 intakes below the estimated average requirement of 2.0 µg of B12. 43 Two independent cross-sectional studies performed in different regions of Germany showed concurrent data. In a study conducted in northern Germany, the B12 intake of flexitarians (therein defined as consumption of meat and meat products ≤50 g/d; equivalent to ≤350 g/week), vegans and omnivores was 2.12, 1.81, and 3.70 µg/d, respectively. 44 The B12 intake of participants in a study in southern Germany was 0.43, 0.98, and 2.14 µg/d for vegans, lacto-ovo-vegetarians, and omnivores, respectively. 45 Beside children and adults, babies born to mothers whose pregnancy progressed with low or deficient B12 can suffer from vitamin B12 insufficiency or deficiency. Data from a national pilot study on expanded newborn screening (NBS) in Germany involving 176,702 children screened over 27 months detected nutritional B12 deficiency in 33 neonates (incidence 1 in 5355). 46 Homocysteine was the most sensitive biomarker. However, MMA measurement was necessary to identify all 33 children with B12 deficiency. Of the diagnosed children, 84% were treated with oral B12 and remained without clinical symptoms. 46 Interestingly, 89% of the mothers adhered to a balanced omnivore diet. In a NBS project involving 588,793 newborns aimed at capturing propionic acidemia, methylmalonic acidemia, and vitamin B12 deficiency in Spain, 89 cases were due to maternal B12 deficiency (incidence 1 in 6616). 47 Of these cases of maternal B12 deficiency, 5% were vegetarian mothers and 15% were mothers diagnosed with pernicious anemia. 47 These 2 large studies confirm that nutritional B12 deficiency during pregnancy is common among omnivores, and its monitoring should not be exclusively restricted to individuals on plant-based diets. The early diagnosis of B12 deficiency in neonates permitted the rapid initiation of treatment to prevent their health deterioration, with the added benefit of treatment to the undiagnosed mothers.
Biomarkers of Vitamin B12 Status: Which One(s) to Use and Why?
Vitamin B12 status is determined by the use of single or multiple biomarkers, namely, plasma vitamin B12, holo-TC, Hcy, and MMA. 48 The 4 biomarkers of vitamin B12 status constitute an aggregate measurement of the absorption, transport, and cellular utilization of the micronutrient. Plasma vitamin B12 and holo-TC are measured by automated platforms in diagnostic laboratories. Homocysteine and MMA are often determined by liquid chromatography tandem mass spectrometry. Plasma and serum are the primary biofluids employed for the determination of biomarkers of vitamin B12 status. The reference ranges for each biomarker in healthy adults are provided in Table 1.
Reference Ranges for Biomarkers of Vitamin B12 Status in Healthy Adults.
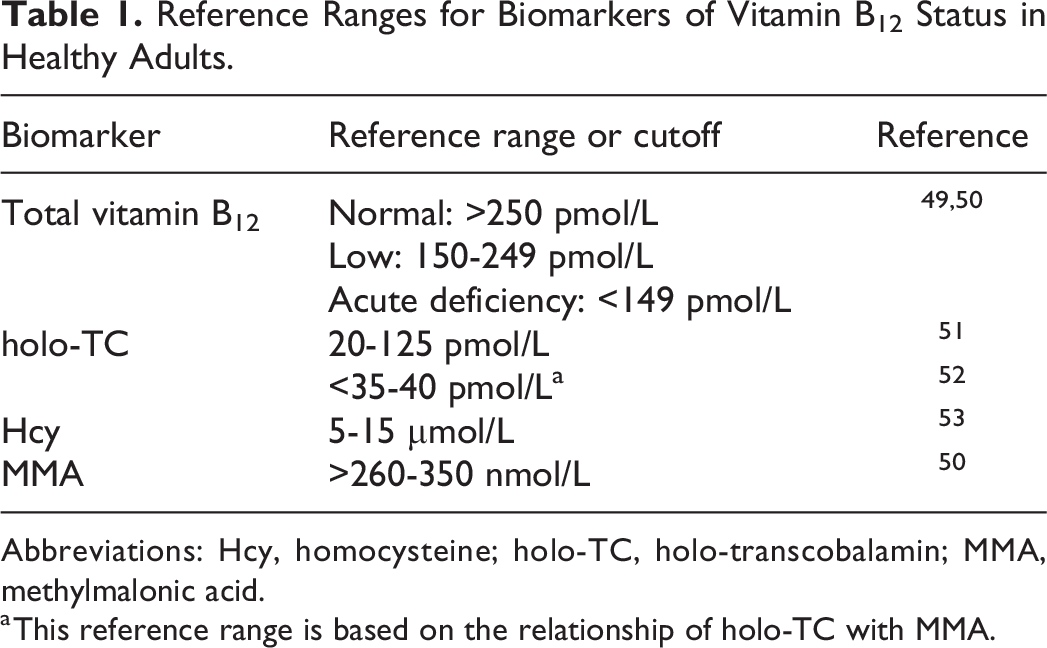
Abbreviations: Hcy, homocysteine; holo-TC, holo-transcobalamin; MMA, methylmalonic acid.
a This reference range is based on the relationship of holo-TC with MMA.
As with all laboratory biomarkers, decisions on B12 adequacy, insufficiency, and deficiency are based on reference ranges determined in a large cohort of healthy individuals, who are predominantly omnivores (>90%). Age- and sex-specific reference ranges have been reported for the assessment of vitamin B12 status. 52,54 - 56 Because none of the individual biomarkers possess sufficient sensitivity and specificity to detect B12 insufficiency and deficiency, a combination of at least 2 biomarkers is recommended. 48 Concurrent measurement of plasma B12, holo-TC, Hcy, MMA, and the 4cB12 index developed by Fedosov 57,58 in a population of 11 833 mixed patients suggested that holo-TC was the better of the 2 direct biomarkers and MMA was the better of the 2 metabolic biomarkers, with holo-TC being the preferable first-line marker for the identification of B12 deficiency. 59
In a controlled trial where healthy omnivores were randomized into either a meat-rich diet or a vegan diet for 4 weeks, both plasma vitamin B12 and holo-TC underwent a significant reduction at the end of the trial in the vegan group, without changes in Hcy or MMA. 60 The concentration of plasma holo-TC decreased by 28% compared to baseline concentrations after only 4-weeks on an unsupplemented vegan diet. 60 This study demonstrated that holo-TC decreases quickly upon reduction of dietary intake after transitioning from omnivore to vegan diets, and thus may serve as the preferable marker to monitor B12 status in healthy individuals on plant-based diets.
Plasma Hcy is the preferred biomarker for the assessment of B12 status in infants and toddlers up to 3 years old, with a cutoff of 6.5 µmol/L. 55,56,61 In older children and adults, Hcy is most responsive to folate status and thus MMA is the preferred biomarker. 15 The biomarkers of B12 status change distinctively during pregnancy due to increased blood volume and maternal-fetal transfer of vitamin B12. 62 -65 Results from an extended NBS in Spain showed that in cases of babies born with B12 deficiency due to maternal B12 deficiency, the mean concentrations of plasma B12 were 187.6 ± 76.9 pg/mL (139 ± 70 pmol/L) and 213.7 ± 95.0 pg/mL (158 ± 57 pmol/L) in babies and mothers, respectively. 47 Thus, pregnant women with a low concentration of plasma B12 (150-249 pmol/L) are a high-risk group for neonatal vitamin B12 deficiency.
In addition to the above reference range considerations that are applicable to healthy individuals irrespective of their dietary pattern, studies performed on healthy vegetarians showed that assessing B12 status in individuals on plant-based diets may require adjusted reference ranges. Analysis of plasma B12, holo-TC, and Hcy in healthy vegetarian Indian graduates showed that when using the reference ranges given in Table 1, 50% were B12 deficient, 70% of males and 50% of females had low concentration of plasma holo-TC, and 92% of males and 50% of females had elevated Hcy. 66 Strikingly, none of the study participants exhibited clinical signs of B12 deficiency. 66 As noted by Carmel, vegetarians and vegans may fall within the category of subclinical B12 deficiency, wherein biomarkers of B12 status are suboptimal yet individuals remain asymptomatic for long periods of time and may not always develop B12 deficiency. 67 Analysis of biomarker relationships by receiver operating characteristic curves led to the suggestion of the use of a combination of biomarkers to define B12 deficiency in healthy vegetarian Indians, with the following adjusted cutoffs: 100 pmol/L for plasma B12, 19.6 pmol/L for holo-TC, 17.6 and 27 μmol/L for plasma Hcy in females and males, respectively. 66 While the use of adjusted reference ranges for individuals on plant-based diets merits consideration, 68 reducing the cutoff for plasma B12 to 100 pmol/L to define deficiency may expose healthy vegetarian women of child-bearing age to a pregnancy that progresses with too low plasma vitamin B12, which per available evidence 47 will lead to neonatal B12 deficiency. A concentration of plasma vitamin B12 >394 pmol/L has been recommended as a target at week 18 of pregnancy. 69 Hence, the status of vitamin B12 should be monitored carefully in prospective mothers and early in pregnancy especially if they adhere to plant-based diets. Likewise, any adjustment to existing reference ranges should consider stages of life where demands for vitamin B12 are high (i.e., child and adolescent development, pregnancy and lactation, elderly).
Vitamin B12 Status in Plant-Based Populations
In the absence of vitamin B12 supplementation or the consumption of foodstuffs fortified with B12, individuals on plant-based diets exhibit a poor status of vitamin B12 and are at risk of developing B12 deficiency. 70,71 A randomized controlled trial with dietary intervention showed that both plasma B12 and holo-TC undergo a significant decrease in individuals transitioning from omnivore to vegan diets, after only 4 weeks. 60
According to survey data and recording of B12 supplement use in cross-sectional studies, the level of awareness concerning the importance of using a B12 supplement while on a vegan diet has risen over the years. A survey designed to assess the level of B12 supplement use among Slovak and Czech vegans showed that in a population of 1337 self-identified vegans, approximately 88% of participants supplemented with B12. 72 The mean weekly B12 intake ranged from 1630.31 ± 1949.27 µg to 2938.34 ± 2566.60 µg in irregularly and regularly supplementing vegans, respectively. 72 These weekly intakes of B12 exceed the recommendations in all available guidelines. A survey examining 1565 vegans from Austria revealed that 92% took B12 supplements and/or fortified foods, and 76% of the participants had their B12 status checked. 73 A survey assessing 1530 Australian vegan women of reproductive age revealed that the use of B12 supplements varied widely. In this study, when the calculated fraction of B12 absorbed was taken into consideration, 39% of participants had an estimated total intake of B12 below the recommended dietary intake (RDI) equivalency, versus 26% being below the RDI when estimations were based exclusively on mean daily intake. 74 Analysis of maternal B12 deficiency detected by NBS in Germany revealed that in a total of 121 mother-infant dyads, 100% of mothers following a vegan diet and most mothers with a vegetarian diet took vitamin preparations during pregnancy, whereas only 55.6% of mothers with an omnivore diet took vitamin supplements. 75
Cross-sectional studies have been also valuable in examining the B12 status of long-term (>1 year on the diet) vegetarians and vegans and their conduct toward the incorporation of B12 supplements. In a cross-sectional study conducted in healthy Germans following flexitarian (therein defined as consumption of meat and meat products ≤50 g/d; equivalent to ≤350 g/week), vegan and omnivore diets, 32%, 82%, and 24% reported using vitamin supplements, respectively. 44 Surprisingly, analysis of B12 status using the 4cB12 index showed that suboptimal B12 status was lowest among vegans (9%), followed by omnivores (10%) and flexitarians (13%). 44 A study conducted in Switzerland comparing omnivores, vegetarians, and vegans showed that despite low intakes of B12 especially in vegans, a normal B12 status was achieved by the use of oral B12 supplements. 43 A study on healthy omnivores and vegans from the Berlin area in Germany showed comparable B12 status in the 2 groups, as determined by the 4cB12 index indicating adequate B12 supply. 76 The adequate B12 status in vegans was attributed to a high rate of supplement use in this group (97.2% of participants). 76 A study performed on healthy young adults from south Germany showed that the B12 status (4cB12 index) of vegans was comparable to that of omnivores, owing to the high rate of B12 supplement use among vegans (90%) compared to lacto-ovo-vegetarians (51%). 45 Vegetarians exhibited the poorest B12 status. 45 Examination of unsupervised supplement use over the course of 1 year showed that a median intake of 250 µg B12/d was sufficient to achieve an adequate status of B12 in vegans. 45 Similarly, a study performed on Czech vegans showed that those using regular supplementation with vitamin B12 had similar plasma concentrations of B12 and holo-TC as omnivores. 70
Clinical trials with B12 interventions in individuals on plant-based diets are few and heterogeneous in design and biomarker readouts. Table 2 summarizes studies with vitamin B12 intervention in groups susceptible to vitamin B12 deficiency with a focus on plant-based diets. Plasma vitamin B12 is the most commonly measured biomarker across different studies and was herein chosen to examine response to various supplementation regimens. The available studies show known trends in vitamin B12 absorption and the relationship between B12 intake and plasma vitamin B12 concentration. These can be summarized as follows: A comparatively greater fraction of B12 is absorbed from low-dose supplements compared to high-dose supplements.
84
The magnitude of change in plasma vitamin B12 in response to oral supplementation depends on the initial status of B12 and the duration of the trial, more so than on the dose alone (see also study by Del Bo et al).
80
Neither chemical form of B12 (CNCbl, HOCbl, or methylcobalamin) exhibits superiority over the others in supporting function in healthy individuals.
14
Response of Plasma Vitamin B12 to Oral Supplementation in Vulnerable Groups of Adults Including Individuals on Plant-Based Diets.
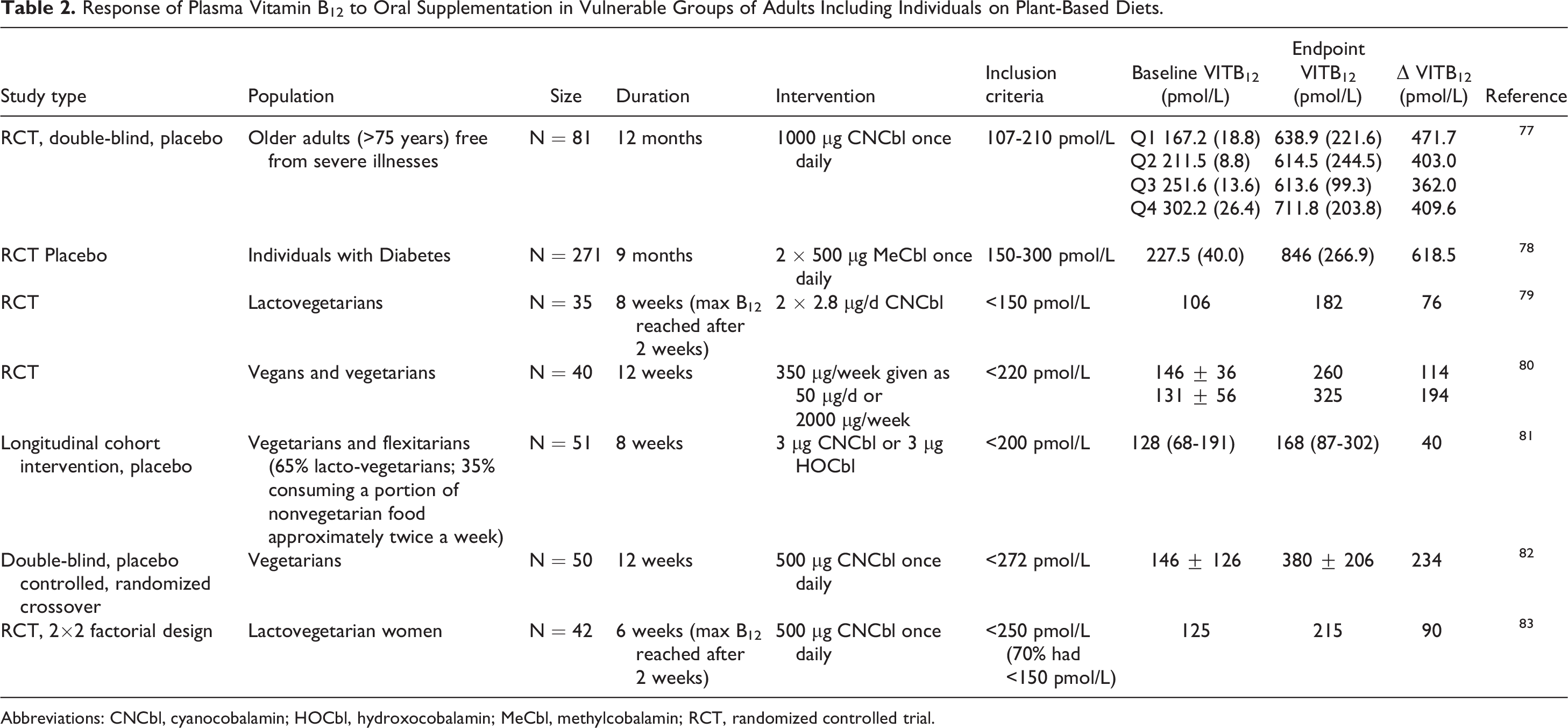
Abbreviations: CNCbl, cyanocobalamin; HOCbl, hydroxocobalamin; MeCbl, methylcobalamin; RCT, randomized controlled trial.
Vitamin B12 Supplementation in Plant-Based Diets
Despite its importance, there is a lack of international consensus on the dose and frequency of vitamin B12 supplementation required to support B12 status adequacy in healthy adults on plant-based diets. Prior estimates include: (1) a daily intake of 50 to 100 µg/d B12 or 2000 µg per week B12 divided into 2 doses 85,86 for healthy vegetarian adults, (2) a daily dose of 50 µg sublingual B12 for vegans and vegetarians with marginally low plasma B12, 87 (3) a daily intake between 50 and 150 µg B12 for healthy asymptomatic individuals without malabsorption (no diet specified), 88 and (4) a daily dose of 500 µg/d B12 to treat individuals with vitamin B12 in the low normal range (no diet specified). 89 Based on the joint consideration of intake, supplement use and plasma biomarkers of B12 status, results from a cross-sectional study comparing long-term omnivores, lacto-ovo-vegetarians, and vegans suggest that a B12 intake of 250 µg/d supports an adequate status of the micronutrient in individuals on plant-based diets. 45 This daily intake was calculated based on unsupervised use of B12 supplements by the study participants. While supplement use by vegans in that study exceeded the daily intake of 4 to 20 µg B12 recommended by an international panel of experts for individuals of all ages, 35 it highlights an increasing awareness and acceptance of the importance of B12 supplementation in plant-based diets. Concerning pediatric and adolescent populations, intervention with B12 in a study performed in Canada showed that a daily consumption of up to 10 µg B12 by children older than 6 years and adolescents, and up to 10-25 µg by older adults led to an improved vitamin B12 status. 90 The NNR suggest a daily intake of 3 to 4.9 µg B12 in children <10 years old, and 5.3 to 10 µg/d for children >10 years old to sustain an adequate B12 status. 55
Conclusions
Unfortified plant-based diets are devoid of vitamin B12. Vitamin B12 intakes in unsupplemented vegetarians and vegans fail to meet the estimated average requirements. The 4 biomarkers of vitamin B12 status respond to changes in dietary intake, albeit differently. A combination of at least 2 biomarkers, ideally holo-TC (direct marker, rapid responder to changes in B12 intake) and MMA (metabolic marker, denotes cellular deficiency) is desirable when monitoring B12 status in individuals on plant-based diets. In studies performed with vegetarians and vegans, plasma biomarkers of vitamin B12 changed markedly before the onset of clinical symptoms. Thus, despite their known shortcomings, 48,91 these biomarkers remain a valuable tool to monitor and to diagnose B12 deficiency in individuals on plant-based diets. Certain types of algae such as Chlorella sp contain substantial quantities of vitamin B12 and carry little quantities of unwanted, nonmetabolizable B12 analogues. However, because the production of algae preparations is not controlled with pharmaceutical quality assurance and controlled dose–response studies with algae preparations in humans are lacking, the safest way to prevent vitamin B12 deficiency in plant-based diets is to use a supplement of B12. Healthy adults on plant-based diets can prevent vitamin B12 deficiency by securing a daily intake of B12 of 4 to 20 µg/d. 35 The recommendation of B12 intake for children younger than 10 years is 3 to 4.9 µg/d, and for those older than 10 years 5.3 to 10 µg/d. 55
Insufficient intake of B12 was documented not only in individuals on a vegan diet but also in vegetarians and flexitarians, the latter two being the fastest growing dietary regimens worldwide. Flexitarians and vegetarians did not use B12 supplements as often as vegans (32%-55% vs 80%-97%), which shows an excessive reliance on food intake as the sole source of B12. Survey data indicate that while the level of awareness regarding the importance of using a B12 supplement when adopting a vegan diet is high, the dose and frequency of B12 supplementation varied widely. The analysis of unsupervised B12 supplement use by vegans in independent cross-sectional studies showed that their daily B12 intake from supplements vastly exceeds the daily intakes recommended by a multitude of regulating authorities including DACH, EFSA, NIH, NHS, and NNR. While there is no toxicity associated with the use of high-doses of oral B12, it is presently unknown whether long-term exposure to high-dose B12 may perturb gut microbiome communities that produce B12 as well as those that synthesize vitamin B12 analogues from B12. Dose-finding studies are urgently needed to determine the physiologically optimal upper limit of B12 supplementation for individuals on plant-based diets.
Footnotes
Author Contributions
Author contributions were as follows: LH planned and wrote a first complete version of the manuscript; AKL, MAS, RH wrote and edited sections of the manuscript focused on plant-based nutrition; DWJ wrote and edited sections of the manuscript focused on vitamin B12 biomarkers and B12 deficiency. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.