
Abstract
Background:
Livestock-dependent communities in Africa’s drylands disproportionately experience acute malnutrition, especially during drought seasons. We detail the design and implementation of the Livestock for Health (L4H) study aimed at determining the effect of providing livestock feed and nutritional counselling to prevent seasonal spikes of acute malnutrition.
Methods:
The L4H study employed a 3-arm cluster randomized controlled trial to compare households in pastoralist settings in northern Kenya receiving livestock feeds during critical dry periods, with or without nutritional counseling, with control households. Over 4 dry seasons, 2019 to 2021, the study collected data on household milk production, consumption patterns, mothers’/children’s nutritional status, household socioeconomic status, herd dynamics, and human and animal health status every 6 weeks.
Results:
L4H recruited 1734 households, with 639, 585, and 510 households assigned to intervention arms 1 and 2 and control arm 3, respectively. From these households, 1734 women and 1748 children younger than 3 years were recruited. In total, 19 419 household visits were completed, obtaining anthropometric measures 9 times on average for each child and mother. Eighty-one households (5%) were lost from the study due to the mother’s death, child’s death, migration, and withdrawal for other reasons.
Discussion:
L4H’s success in a challenging environment was possible due to strong community engagement, formative studies to inform trial design, collaboration with local authorities, and effective interdisciplinary collaboration. Subsequent manuscripts will report the study findings.
Trial Registration:
The study was registered October 29, 2020, and is online at ClinicalTrials.gov (ID: NCT04608656).
Introduction
Africa’s drylands cover nearly two-thirds of Africa’s land, are home to 268 million pastoralists, and significantly contribute to national economies. 1,2 Communities in Africa’s drylands experience seasonally recurring high rates of global acute malnutrition (GAM <−2 weight-for-height z-scores). 3
The 2014 Kenya Demographic and Health Survey reported the predominantly pastoral region of northern Kenya had a higher proportion of severely wasted children (2.6%) compared to the national level (0.9%). 4 High levels of acute malnutrition among children younger than 5 years have been recorded in nutrition surveys of pastoralist populations, usually during the dry or hunger season. 5 A study of acute malnutrition in 3 dryland regions demonstrates the seasonality of acute malnutrition and their links to climate variability, conflict, and livelihood system. 3
Our previous studies in Kenya showed strong seasonal patterns of acute malnutrition, with the highest levels observed in March and October, before or at the start of the wet seasons, when food is most scarce. 6 There remains a dearth of knowledge on how interventions in agriculture can contribute to improving human nutritional status in such settings. 7
In this short communication, we detail the design, implementation, strengths, and limitations of the Livestock for Health (L4H) study designed to measure the effect of providing livestock feed and nutritional counselling to prevent or reduce seasonal spikes of acute malnutrition in drylands.
Methods
Study Setting
The L4H study was carried out in the Laisamis region of Marsabit County in northern Kenya. The study site was chosen for 3 key factors: high prevalence of undernutrition among children and women; strong dependence on livestock as the main source of livelihood for the Rendille and Samburu pastoralist communities that inhabit the area; and accessibility for field data collection.
Study Design
The study employed a cluster randomized controlled trial design with 2 intervention arms and a control arm. At the start of each dry season, households in intervention arms 1 and 2 received livestock feeds (range cubes) sufficient to sustain 2 tropical livestock units (TLUs) of their milking animals for 90 days. One TLU is the equivalent of either 1 cow, 1 camel, 10 goats, or 10 sheep. The feeds were provided early in the dry season to allow for maintenance of milk production. Additionally, households in intervention arm 2 received enhanced nutritional counseling and education based on the Maternal Infant and Young Child Nutrition programme. 8 This was accompanied by information on benefits of consuming milk, hygienic handling and storage, and milk preservation and preparation, in the form of a milk utilization card codeveloped between the government and partners in the L4H program. The enhanced counseling was offered weekly by trained community health workers drawn from the same study community.
Households in study arm 3 did not receive either intervention during the study period. All households in the study had their animals dewormed annually. At the end of the study, households in arm 3 received livestock feeds to last their milking herd for 1 dry season. The study ran from September 2019 to December 2021, covering 4 dry seasons.
Sample Size, Sampling Strategy, and Data Collection
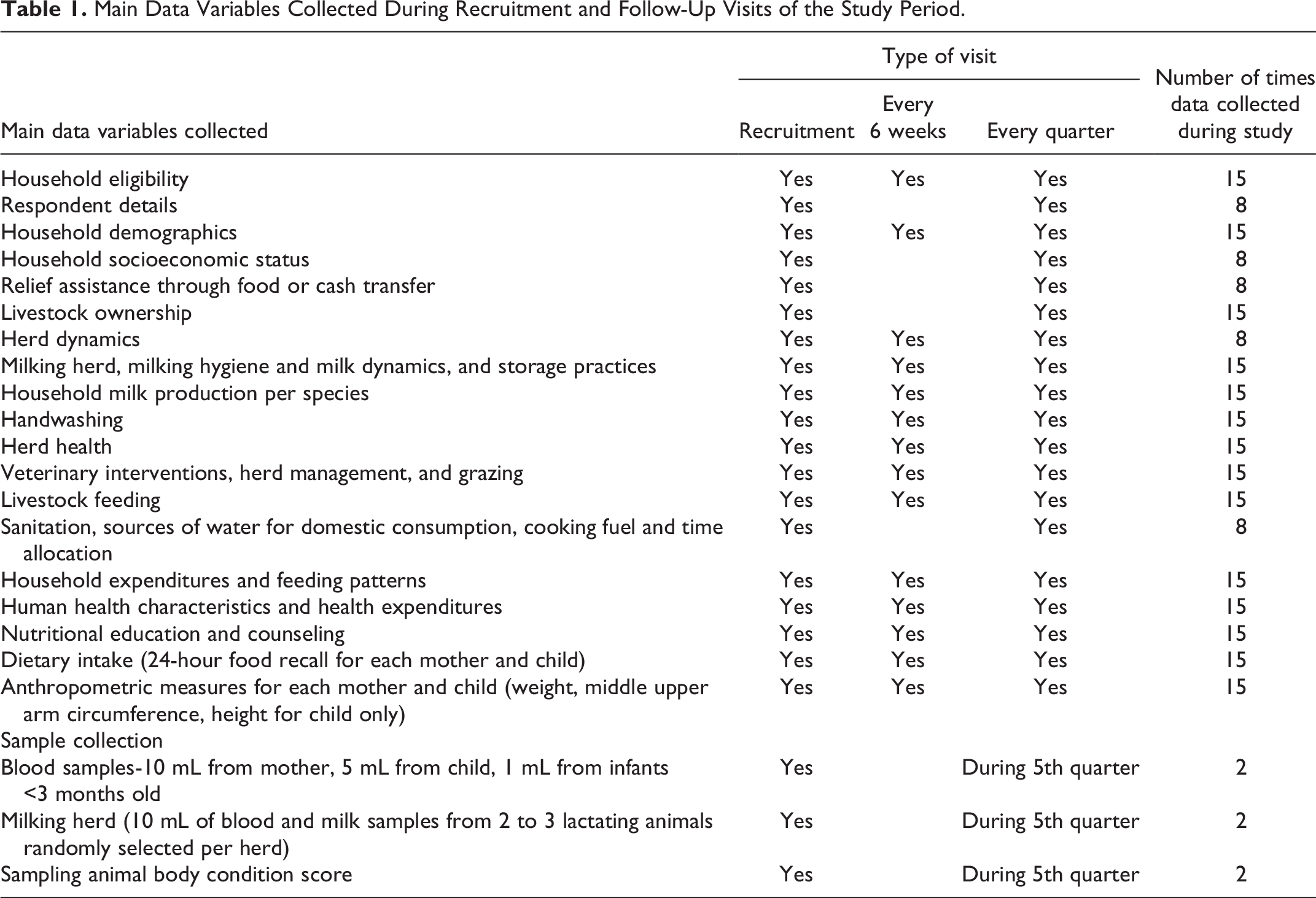
The sample size, 600 households per study arm, was estimated to be sufficient to detect an effect size difference of at least 0.25 points (weight-for-height z-score) between the intervention and control arms. A stratified multistage cluster sampling procedure was used to select the study sublocations, villages, households, and participants. To minimize contamination between intervention arms and control arms, all participating households at any given sublocation were assigned to the same study arm. The household inclusion criteria were presence of a pregnant woman/mother (lactating or not) and a child 3 years and below and ownership of livestock. Households that did not consent to participate or were unwilling to adhere to the study protocol were excluded from the study. Data collected and the frequency of collection are summarized in the Appendix Table 1.
Ethical Considerations
Ethical clearance was obtained from the Kenya Medical Research Institute Scientific and Ethics Review Committee (KEMRI/SERU/CGHR/02-09/3755). The study protocol was registered at https://clinicaltrials.gov (ID: NCT04608656).
Results
In total, 1734 households with 1734 women and 1748 children consented and were recruited into the study. Of these, 639, 585, and 510 households were assigned to study arms 1, 2, and 3, respectively. Study households were visited an average of 9 times (median 10 times) by the research team. In total, 19,419 household visits were made, and 16,015 household questionnaires were completed (see Figure 1). Movement of household members in search of pastures for their animals (transhumance) resulted in some missed questionnaire administration. In total, 81 households could not be followed to the end of the study, for reasons including migration (63%), mother’s death (1%), child’s death (12%), and withdrawal for other reasons (24%).
Information on household, mother and child food consumption patterns, and anthropometric measures of mothers and children were collected for an average of 9 out of 15 planned visits per household (60%).
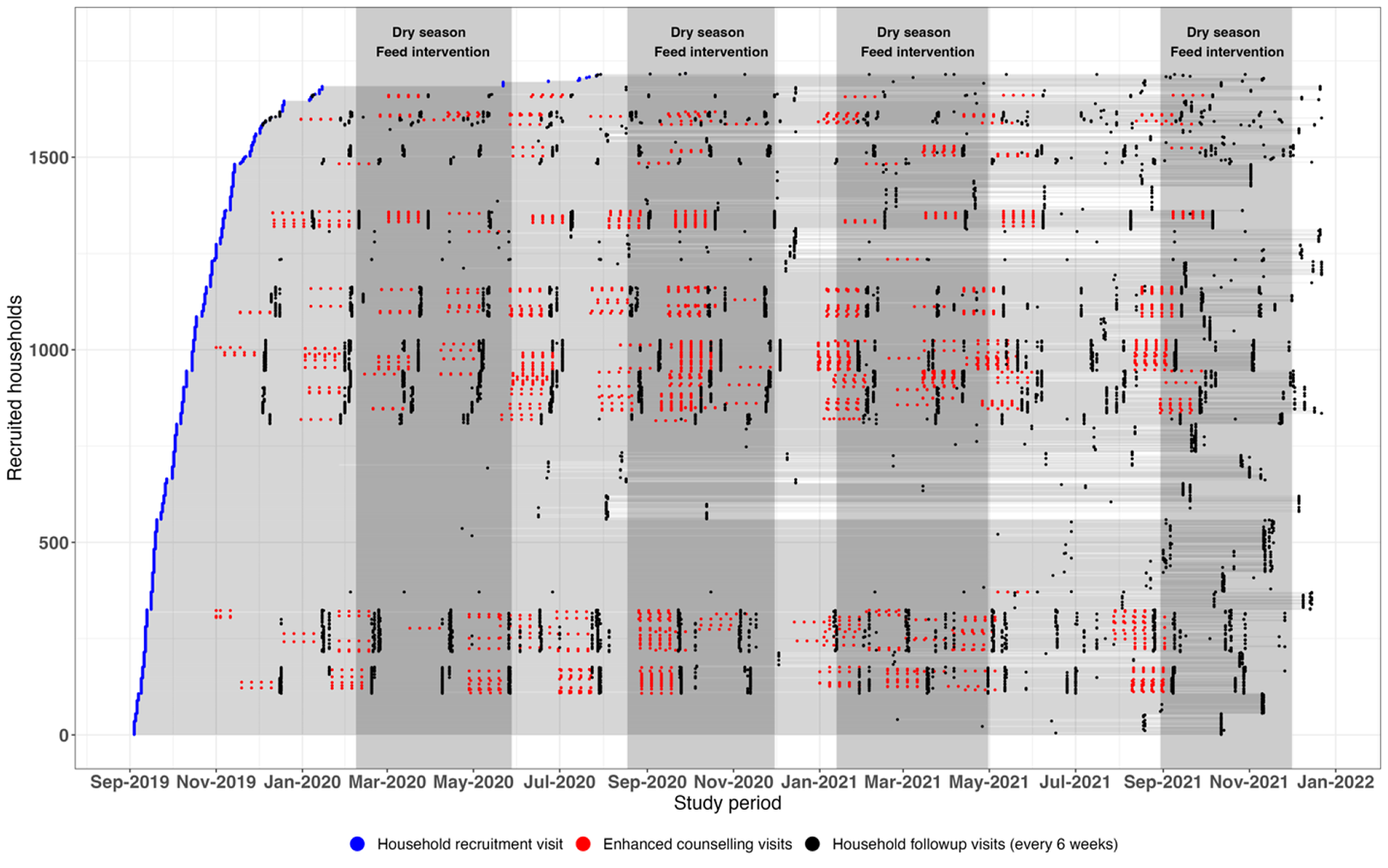
Summary graphic of the Livestock for Health study showing recruitment visits (blue dots), follow-up visits every 6 weeks (black dots), and visits with enhanced counselling for each of the 1734 study households. Gray shading shows dry seasons during the study period when feeds were provided to all eligible households.
To determine exposure to zoonotic pathogens among study participants and milking animals from their herds, we obtained biological samples at the start and end of the study. Samples were obtained at the start and end, respectively, from 1074 and 1052 women, 255 and 311 children, and 61% (n = 1050) and 61% (n = 1052) of households. For animals, 240, 624, and 3597 samples were collected from 3222 camels, 6444 sheep, and 7518 goats, respectively. Results from analysis of these data will be published in upcoming manuscripts.
Discussion
Although there are qualitative and anecdotal data on the benefits of livestock feed provision in addressing spikes of malnutrition during drought, evidence from randomized control field trials is rare. This is partly due to the difficulty and expense of such intensive studies in drylands with challenging landscapes.
L4H study has produced a rich dataset with information on household milk production, consumption patterns, and nutritional status of women and children in a large number of pastoralist households, collected every 6 weeks over a 2-year period covering 4 dry seasons. The study’s success can be attributed to multiple factors, including community involvement in design and selection of study areas and participants; preliminary studies to inform trial design and implementation 6 ; deliberate involvement of local community members in delivery of study interventions and collection of data; close collaboration with local authorities; and a multidisciplinary approach. L4H addressed 2 related priority issues for the community: threat to livestock health and production and spikes of acute malnutrition in women and children during dry seasons. It implemented an appropriate intervention tailored to community livelihood practices (the practice of leaving a few milking animals around the household when the rest of the herd migrates in search of pasture and water).
Randomized control trials are an effective study design to estimate and test the effects of an intervention. Enrolling control groups in trials can be challenging as incentives for participation are less compared to those in the intervention arms. Before the start of the study, several sensitization meetings with the community and local authorities were carried out. Study staff were drawn from the study community, increasing participation and ownership by the community. As a result, the L4H study did not suffer notable declines in participation in any of the study arms.
The L4H project team brought together personnel and institutions with a broad range of expertise. The Food and Agriculture Organization of the United Nations (FAO) led the implementation of the study in collaboration with a local community organization, Pastoralist Community Initiative Development and Assistance. Food and Agriculture Organization supported the delivery of livestock feeds to all eligible households. Nutrition counseling and education, and design and rollout of the milk utilization card, were supported by UNICEF, Concern Worldwide, and FAO in collaboration with the Government of Kenya. Washington State University directed the L4H research design, implementation, and analysis through its global health program based in Kenya and led by local scientists with expertise in conducting field trials for public and animal health. A technical advisory team, drawing participation from relevant institutions such as the National Drought Management Authority, Marsabit County Government, Kenya Medical Research Institute, International Livestock Research Institute, and technical experts from the United States Agency for International Development (USAID), met every 2 months to review the project progress.
The L4H trial design and implementation had limitations. Although villages in intervention arms and those in the control arm were separated geographically, contamination between arms or sharing of livestock feeds with nonstudy households cannot be ruled out. To account for this, participants were asked if they had shared or received livestock feeds from other sources. This self-reported information on feed sharing or study outcomes can be biased. The enumerators were trained on triangulation techniques to minimize these potential self-reporting biases.
Although research on the relationship between agriculture interventions and nutrition has gained much recent interest, empirical evidence to guide malnutrition prevention has remained scarce. Findings from this research should provide important data to support decisions on how best to prevent seasonal spikes in malnutrition in pastoralist communities and, more broadly, on livestock interventions that can help prevent malnutrition among livestock-dependent communities.
Footnotes
Acknowledgments
The authors thank the National government, county government of Marsabit, and the National Drought Management Authority for support during the study. The authors acknowledge support of the L4H study participants and the field research team members: Arbelle Judy, Bonaya Galgallo, Bonaya Ibrae, Boru Galgallo, Bursuna Stephen, Darba Doche, Boranto Rosemary, Emanuel Eisimkorro, Gumatho Ann, Gobanai James, Kato Amos, Kargio Emmanuel, Keriya Sabrina, Lekapana Jacob, Leyamyam Jeremiah, Matini Newton, Ogoti Brian, Parkasio John, and Seree Stephen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Office of Technical and Program Quality, Bureau for Humanitarian Assistance, USAID [720FDA18IO00035]. JM was funded by the Fogarty International Center and the Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Number D43TW011519. The opinions expressed in this manuscript are those of the authors and do not necessarily reflect the views of USAID, National Institutes of Health or the U.S. Government. Laboratory testing for zoonoses was partly supported through the Kenya National Research Fund [BB/S004904/1].
Appendix
Main Data Variables Collected During Recruitment and Follow-Up Visits of the Study Period.
| Main data variables collected | Type of visit | Number of times data collected during study | ||
|---|---|---|---|---|
| Recruitment | Every 6 weeks | Every quarter | ||
| Household eligibility | Yes | Yes | Yes | 15 |
| Respondent details | Yes | Yes | 8 | |
| Household demographics | Yes | Yes | Yes | 15 |
| Household socioeconomic status | Yes | Yes | 8 | |
| Relief assistance through food or cash transfer | Yes | Yes | 8 | |
| Livestock ownership | Yes | Yes | 15 | |
| Herd dynamics | Yes | Yes | Yes | 8 |
| Milking herd, milking hygiene and milk dynamics, and storage practices | Yes | Yes | Yes | 15 |
| Household milk production per species | Yes | Yes | Yes | 15 |
| Handwashing | Yes | Yes | Yes | 15 |
| Herd health | Yes | Yes | Yes | 15 |
| Veterinary interventions, herd management, and grazing | Yes | Yes | Yes | 15 |
| Livestock feeding | Yes | Yes | Yes | 15 |
| Sanitation, sources of water for domestic consumption, cooking fuel and time allocation | Yes | Yes | 8 | |
| Household expenditures and feeding patterns | Yes | Yes | Yes | 15 |
| Human health characteristics and health expenditures | Yes | Yes | Yes | 15 |
| Nutritional education and counseling | Yes | Yes | Yes | 15 |
| Dietary intake (24-hour food recall for each mother and child) | Yes | Yes | Yes | 15 |
| Anthropometric measures for each mother and child (weight, middle upper arm circumference, height for child only) | Yes | Yes | Yes | 15 |
| Sample collection | ||||
| Blood samples-10 mL from mother, 5 mL from child, 1 mL from infants <3 months old | Yes | During 5th quarter | 2 | |
| Milking herd (10 mL of blood and milk samples from 2 to 3 lactating animals randomly selected per herd) | Yes | During 5th quarter | 2 | |
| Sampling animal body condition score | Yes | During 5th quarter | 2 | |