
Abstract
Background:
Integrated school and home garden interventions can improve health outcomes in low-income countries, but rigorous evidence remains scarce, particularly for school-aged children and to reduce anemia.
Objective:
We test if an integrated school and home garden intervention, implemented at pilot stage, improves hemoglobin levels among school children (aged 9-13 years) in a rural district in the mid-hills of Nepal.
Methods:
We use a cluster randomized controlled trial with 15 schools each in the control and treatment groups (n = 680 school children). To test if nutritional improvements translate into a reduction of anemia prevalence, hemoglobin data were collected 6 months after intervention support had ended. Using structural equation modeling, we estimate the direct and indirect effects of the treatment through several pathways, including nutritional knowledge, good food and hygiene practices, and dietary diversity.
Results:
The integrated school and home garden intervention did not lead to a direct significant reduction in anemia. Causal positive changes of the treatment on nutritional outcomes, although significant, are not strong enough to impact hemoglobin levels. The program improved hemoglobin levels indirectly for children below 12 by increasing the use of good food and hygiene practices at home. These practices are associated with higher hemoglobin levels, particularly for girls, young children, and in households where caregivers are literate.
Conclusions:
Even integrated school and home garden interventions are not sufficient to reduce anemia among school children. Incorporating behavioral change components around food and hygiene practices into integrated garden interventions is important to unlocking their health impacts.
Plain language title
Effect of a Joint School and Home Garden Programme on Child Health Among School-Aged Children in Nepal
Plain language summary
The effects of agricultural and nutritional support programs on health are not fully understood. This article looks at school and home gardens, which are gaining attention in the research and development community, but evidence for their effects is limited, particularly for lower-income countries. We examine whether a joint school and home garden program improves blood iron levels among school children (aged 9-13 years) in rural Nepal. Low levels are an indicator for anemia—a common nutritional disorder in South Asia. Our data come from an experiment involving 30 schools and 680 children and was measured via a finger prick method 6 months after program support ended. We also evaluate if the program influenced blood iron levels through the nutritional knowledge of children and their caregivers; through the use of good food and hygiene practices at home and the children’s dietary diversity. Our results indicate that the program did not lead to a direct reduction in anemia. However, for children under the age of 12, the program indirectly improved blood iron levels through behavioral changes in the use of good food and hygiene practices (e.g., washing hands before eating). We therefore argue that including education on nutrition and good food and hygiene practices as part of integrated garden support programs is key to improving children’s health.
Introduction
Iron deficiency is the most common nutritional disorder and accounts for half the cases of anemia globally. 1 Iron deficiency anemia increases mortality, decreases physical strength, and often triggers long-term chronic diseases, which particularly affects children under 5 years and women of reproductive age. 2 Worldwide, 39.8% of children under the age of 5 and 29.9% of women of reproductive age suffered from anemia in 2019. 3 In school children, anemia has strong negative implications on cognitive and learning abilities. 4 However, there is not much data available about anemia prevalence among school children.
Low dietary diversity is associated with iron deficiency and anemia. 5 Hence, improving nutrition is a key pathway to address these disorders. 6,7 Nutrition-sensitive agricultural interventions, including integrated home gardens, are known to improve dietary diversity and encourage healthy diets and eating habits. 8 -14 Therefore, these interventions are expected to reduce iron deficiency and anemia, particularly through the consumption of dark green leafy vegetables rich in iron. 15 The empirical evidence to date is not conclusive, however.
An early study from Cambodia found no evidence for the impact of home gardens on anemia in children below the age of 5. 16 A systematic review on the nutritional benefits of agricultural interventions, including home gardens, on children in low- and middle-income countries demonstrated a positive impact on vitamin A absorption, but not on iron absorption. 17 An integrated home garden intervention in Burkina Faso showed higher hemoglobin levels and reduced anemia for children below the age of 5, 18 which was found to have positive spillover effects in reducing anemia among other children in the same villages. 19 These results are underlined by 2 recent studies in Asia: In Nepal, a home garden intervention reduced anemia among young children and their mothers, 20 while in Cambodia, a home garden intervention reduced the prevalence of anemia among children below the age of 5 but not among nonpregnant women. 21
School garden interventions have the potential to increase the nutritional knowledge of 8- to 15-year-old children and nudge their preferences toward eating more fruit and vegetables, particularly when combined with nutritional and agricultural education. 22 -24 Shrestha et al found through a randomized controlled trial that school gardens coupled with a water, sanitation, and hygiene (WASH) intervention arm reduced the incidence of anemia among school children aged 8 to 17 years in Nepal. 25 The mechanisms driving this overall effect from school gardens to anemia, however, remain largely unconfirmed. To our knowledge, this is the only study assessing the impact of a school gardening on anemia with a focus on school children.
While the literature from low- and middle-income countries demonstrates that home garden interventions can reduce anemia in certain subgroups like women and young children under the age of 5, there remain key knowledge gaps. First, evidence on how gardening interventions impact the prevalence of anemia in school children older than 5 years is scarce, despite the high prevalence of anemia in children and adolescents aged 5 to 19 years. 26 Second, the available evidence for school children in low- and middle-income countries focuses mainly on the impacts of school feeding or fortification programs, 27,28 but none assess impacts of integrated school and home garden interventions. Finally, there is a clear lack of evidence on the extent of how pathways in knowledge and behavior change contributes to improving the nutrition and health of school-aged children.
This article fills these knowledge gaps by analyzing the impact of an integrated school and home garden intervention on the nutritional and health status of preadolescent school children aged 9 to 13 years in Nepal. We build on the design and findings of Schreinemachers et al, who based on a cluster randomized controlled trial from 15 treatment and 15 control schools found that combined school and home garden have positive nutritional effects. 10 More specifically, they found that the intervention increased the production of vegetables at home, improved the nutritional and agricultural knowledge of caregivers, and nudged children’s food preferences toward eating more vegetables. The combination of these effects was found to have a positive impact on the consumption of vegetables among school-aged children. However, the previous study did not assess the effect on the children’s health status such as the prevalence of anemia.
Building on these findings, we examine if school children who took part in the integrated home and school garden program show improved levels of hemoglobin compared to school children who did not receive the intervention. Then, we analyze if key pathways, including nutritional knowledge of both parents and children, good food and hygiene practices (including washing hands before eating), and the children’s dietary diversity contribute to improving hemoglobin levels, both directly and indirectly. Finally, we test the heterogeneous impacts by age, sex, and the literacy of the caregiver.
The remainder of this article is structured as follows. In the second section, we explain the study design, the data collection, and the methods. In third section, we present our results. In fourth section, we discuss our findings in a broader context and fifth section concludes.
Study Design, Data Collection, and Methods
Choice of Study Location
We conducted the study in Nepal. Even though South Asian countries showed progress in reducing child undernutrition and stunting in recent years, the figure remains high, particularly among disadvantaged households. 6 Based on recent WHO data, 44.6% of the Nepalese children under the age of 5 and 35.7% of women in reproductive age are anemic. 3 It has been estimated that among 10- to 19-year-old adolescents in Nepal, 11% of the boys, and 21% of the girls are anemic in 2016. 29 Other studies found a prevalence of anemia between 35% and 38% among children aged 4 to 13 years in the past decade. 30,31 Poor diets are one of the main drivers of anemia among (young) women and children in Nepal. 6 In the Kathmandu Valley, children under the age of 2 get a quarter of their calories from snack foods and beverages with low nutritional value, 32 while only 1.1% of Nepal’s adult population consumes 400 g of fruit and vegetables a day—the amount recommended by the WHO. 33
The study was conducted in Sindhupalchok District, located between Kathmandu and the border with China. We selected this district because it is relatively poor, but reachable from Kathmandu within a day’s drive, which was important for the implementation of the pilot. The district also has enough schools for the sampling. The mountainous terrain and the extreme altitude differences make most areas difficult to reach, which directly impacts food availability and accessibility. 34 The district was severely affected by the Gorkha earthquake in 2015, which contributed to unhealthy food choices among school children. 35
Intervention and Theory of Change
The intervention consisted of 2 components: school gardens coupled with nutrition education aimed at school children, and training of their parents in home gardening and nutrition. The theory of change posits that hands-on gardening experience and complementary lessons at school on the nutritional benefits of vegetables and fruits strengthen children’s knowledge about the importance of healthy and nutritious food. This is coupled with the caregivers receiving a seed package and training in nutrition and gardening. The school garden is expected to create a stronger interest among children and caregivers toward healthy eating while the home gardens increase the household-level availability of vegetables. Combined, these interventions are expected to increase the intake of vegetables, contributing to greater dietary diversity and increased hemoglobin levels. Figure 1 depicts the combined effects of these interventions, highlighting the possible pathways through which integrated home gardens can improve hemoglobin levels. In essence, we theorize that strengthening nutritional and hygienic knowledge and practices for both children and their caregivers improves directly and indirectly (via healthier diets) hemoglobin levels.
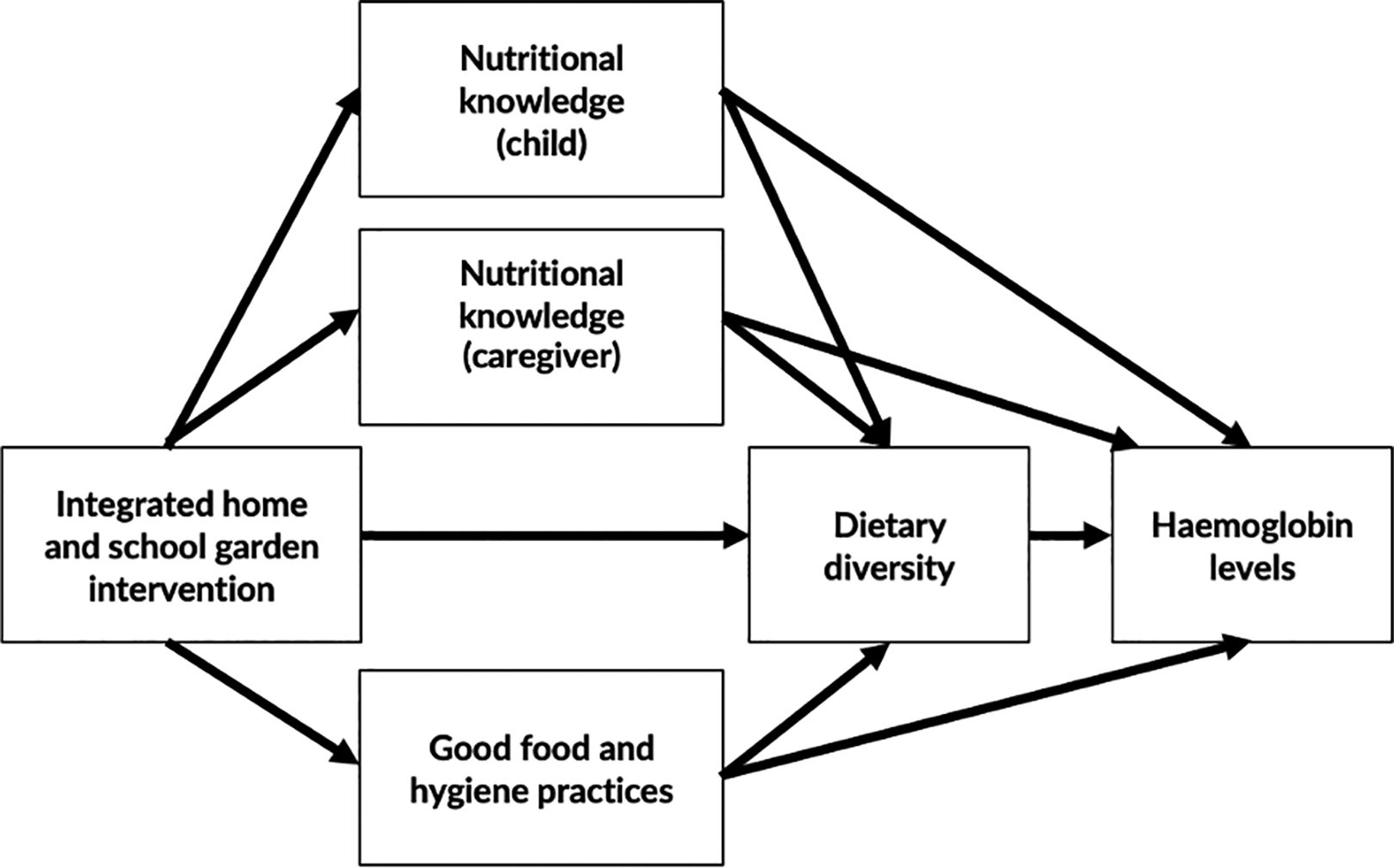
Theory of change.
Following a booklet with 23 weekly learning modules, the school gardens provide the children with hands-on experience and nutritional education. 36 The target group at baseline is children in grades 4 and 5, aged 8 to 12 years. In this age-group, food behavior is expected to be easily influenced, while the children are old enough to do physical garden work and understand the nutrition learning modules. Two teachers per school were trained by project partners in operating the school garden. Schools were provided with financial support to be spent on land preparation, a water tank, garden tools, plastic sheets for making a nursery, and fencing materials. Schools were supplied with seeds of 9 local vegetable species for the winter season and seeds of another 10 species for the summer season.
In the second intervention component, children’s caregivers (mostly their mothers but also fathers and grandmothers) received support to improve their home gardens. The training consisted of 3 sessions on gardening, including topics such as garden establishment, crop rotation, compost making, and pest management, and on nutrition, including topics such as the role of vegetables for family health, the nutritional content of different food items, and cooking methods to preserve the nutritional quality of vegetables. About 80% of the selected caregivers participated in the training. Additionally, the caregivers received the seeds of the same species as provided to the schools. School garden focal teachers provided technical advice to the caregivers and visited their home gardens.
The Nepal Agricultural Research Council implemented the school garden component while the Asia Network for Sustainable Agriculture and Bioresources implemented the home garden component. To assess the program implementation progress, representatives from both organizations conducted 2 monitoring visits. Furthermore, the research team conducted a field visit in December 2018.
Study Design
In our study, we randomly assigned villages (and their respective schools) to either a control group or a treatment group through a cluster-randomized controlled trial (cRCT) design. The treatment group received both the school and home gardens components while the control group received nothing. We assess the intent-to-treat effect which is the same as the “treatment effect on the treated” for the school children since the participation rate is 100%. For caregivers, we rely on intent-to-treat effects since not all of them participated in the training.
Using a minimum detectable difference of 0.2 in terms of vegetable consumption outcomes and intracluster correlation coefficient of 0.025, a sample size consisting of 30 schools with 30 students provided sufficient power at 80% using a 95% confidence interval. 22 However, the original design of the study did not test power for hemoglobin outcomes. Therefore, we calculate the expost power based on the means and standard deviations of the control group taking the cluster size after attrition into account. We find that the minimum detectable effect size of 0.28 is reached at 80% using a 95% confidence interval. An effect of this size is sufficient given that hemoglobin levels exhibit, on average, fluctuations of 0.471 g/dL per day. 37 This implies that a difference of at least 0.5 g/dL between the control and treatment groups is necessary to casually attribute any program effects.
The small cluster size might lead to a lack of balance in outcome variables at baseline. Two instruments were used to reduce this risk at the design stage. First, stricter eligibility criteria were applied to increase the similarity between clusters. We only selected nonboarding government-run schools which have fresh water access. Second, we used altitude (as a proxy of the agroclimatic conditions) and the teacher–student ratio (as a proxy of school quality) as stratification variables in the randomization process to increase the balance between the treatment and control groups. In coordination with the local district education office, 52 schools that met these eligibility criteria were assigned for preselection. These make up 10% of all primary schools in the district, but may not be representative of all schools in the district. From these, 30 schools were then randomly selected to participate in the study taking into account the stratification strategy. From each stratum, we randomly assigned half of the schools to the treatment and the other half to the control. In the next step, we randomly selected 30 school children from each school (15 children each from grades 4 and 5).
Figure 2 shows the sample size in both treatment and control group for the 3-waves of the study. We dropped observations with incomplete data on key outcome variables at the endline. Baseline data were collected in June 2018 from 438 treatment and 436 control children and their caregivers. The endline was administered 1 year later after the end of the intervention in June 2019 from 410 and 419 treatment and control children, respectively. The post-endline data collection, which included mainly taking the blood samples, took place in December 2019, 6 months after the endline data. At post-endline, we collected data from 350 children from the treatment group and 330 children from the control children, but we did not interview the parents as we did in baseline and endline. We reached 80% and 74% of the baseline sample, respectively. In other words, we have an attrition rate at post-endline of 20% in the treatment group and 26% in the control group; 70% of the attrited households migrated, while 30% were temporarily not available.
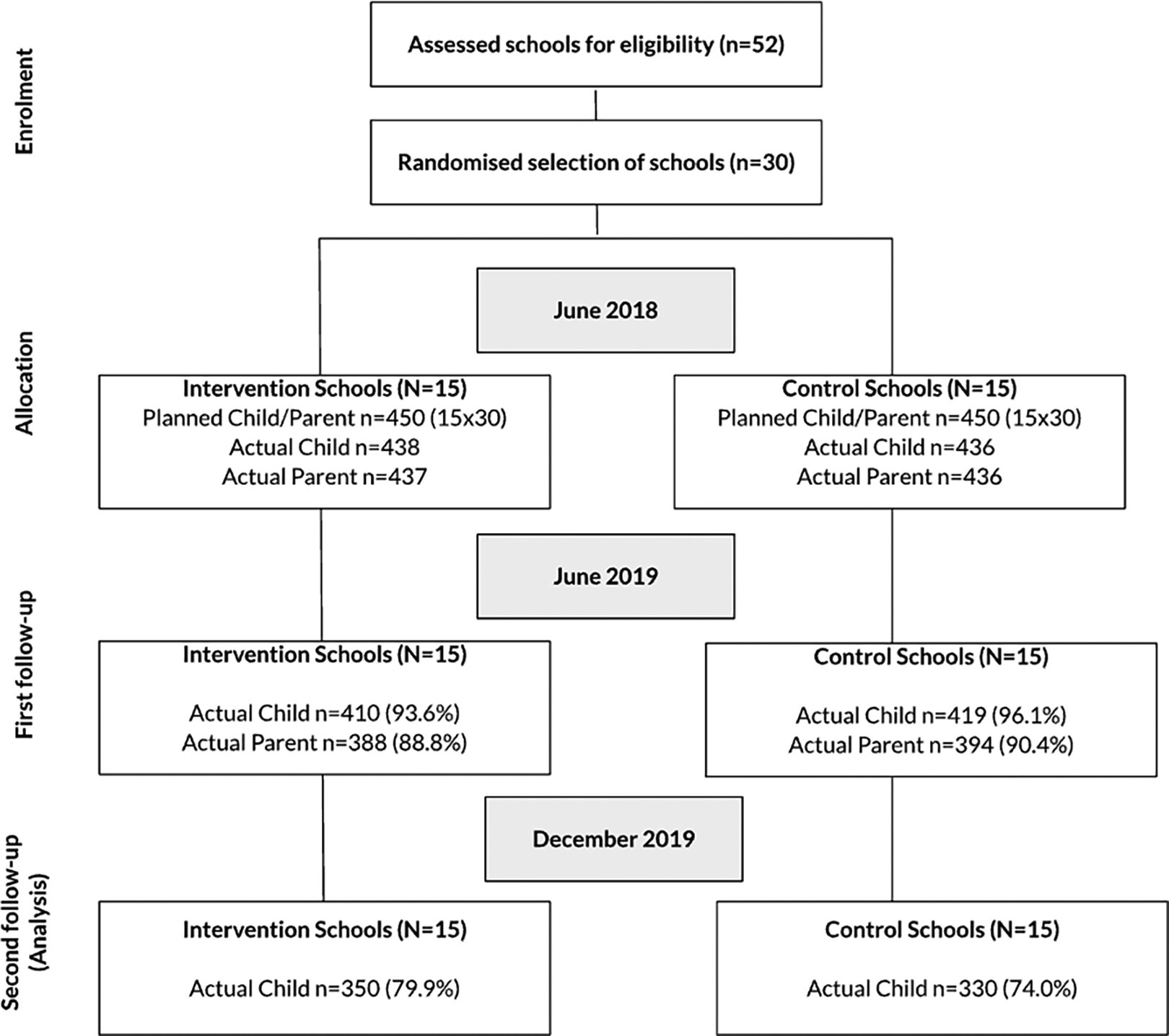
Cluster-randomized controlled trial (cRCT) consort flow diagram. Note: Percentages in parentheses indicate the share of the baseline sample that we reached in the endline and post-endline.
In order to ensure that our random assignment is still valid and that our estimates remain unbiased, it is important that the sample attrition is not systematic between the treatment and control groups. We regress the treatment assignment on attrition while clustering at school levels. We do not find a significant difference in attrition based on treatment assignment. However, regressing key characteristics of the children and caregivers on attrition, we find that children from attrited households are on average older and more likely to be male. Attrited households have a longer distance to school on average and their caregivers are less likely to be literate.
Second, we assess if there are any significant differences in baseline characteristics between the treatment and control groups from our post-endline survey. We additionally test the balance with weighted regressions increasing the weights for households with a higher probability to attrit to simulate a sample without attrition. 38 Any differences we still detect between the 2 groups at post-endline (if any) will be included as control variables in the regression analysis to strengthen the precision of the estimates of the causal effect. 39,40
Data Collection and Ethics
In the post-endline, trained health workers measured the children’s height to the nearest cm using a standard scale, their weight to the nearest 0.1 kg using a digital portable calibrated weighing scale wearing a light uniform with empty pockets and no shoes, and their hemoglobin level through capillary blood samples, using HemoCue digital point-of-care-devices (HemoCue Hb 201 + System). The blood sample was taken through a small finger prick and analyzed directly in a microcuvette via the HemoCue analyzer. Data on anemia is only available in the post-endline wave. Furthermore, the children’s diet was assessed through a 24-hour recall of their consumption of different food groups, including meat, dairy, and vitamin A-rich fruit and vegetables such as pumpkin, carrots, squash or sweet potatoes, dark green vegetables, ripe mangoes, and ripe papayas.
The study was approved by Nepal Health Research Council Ethical Review Board on May 30, 2018 (Reg. No. 222/2018), and on May 15, 2019 (Reg. No. 214/2019). Study participation was voluntary. School principals signed consent to include the schools in the study after selection to receive school gardens, and caregivers signed a written consent form at baseline. Participation in the project bore no risk for caregivers and children while the potential benefits in terms of improved nutrition as a result of the school and home garden intervention were potentially substantial. The results from the hemoglobin tests were shared with the children and their caregivers. To incentivize control schools to participate in the project, we provided them with cash support and teacher training to also establish a school garden after the completion of the endline data collection. However, we did not follow-up with the schools on how they spent the money that we provided. The cash transfers and training took place before the data collection of the post-endline. However, we do not anticipate that these could impact the treatment effect of the program on nutrition and hemoglobin levels, particularly that the caregivers from the control were not provided with additional support. The original trial is included in the Registry for International Development Impact Evaluations (Study ID 5cd93ec673096). Our specific research question on how an integrated school and home garden intervention influences the prevalence of anemia was not included in the initial trial registration.
Main Variables
The independent variable of interest is program participation, which is exogenous as treatment assignment was cluster randomized. We use the childrens’ age, sex, weight and height, distance to school, and their caregiver’s literacy as control variables to isolate the effect more reliably and increase the precision of our estimates. 41
The main continuous outcome of interest is the overall hemoglobin levels of school children, used as a proxy for anemia. We also assess the prevalence and severity of anemia following WHO classification. 42 Children aged 5 to 11 years are diagnosed as not anemic with a hemoglobin level ≥ 11.5 g/dL, mildly anemic with 11.0 to 11.4 g/dL, moderately anemic with 8.0 to 10.9 g/dL, and severely anemic with <8 g/dL. For children aged 12 to 14 years, the thresholds are ≥12 g/dL, 11.0 to 11.9 g/dL, 8.0 to 10.9 g/dL, and <8 g/dL, respectively. 42 For robustness, in addition to hemoglobin levels, we include the binary variable for each anemia level as an outcome.
Furthermore, we assess the children’s food and nutritional intake at post-endline using a dietary diversity score both as an outcome and as a mediator variable for hemoglobin. The dietary diversity score is constructed based on the number of food groups the children consumed on the day before the post-endline data collection out of 14 local food groups including (1) grain products, (2) roots and tubers, (3) legumes and nuts, (4) milk, (5) yoghurt, (6) cheese and other dairy products, (7) organ meat, (8) other meat, (9) dried meat and fish, (10) eggs, (11) yellow and orange vitamin-A-rich vegetables, (12) dark green leafy vegetables, (13) vitamin-A-rich fruits, and (14) other fruits and vegetables.
Additional mediator variables include nutritional knowledge of children and caregivers, and the use of good food and hygiene practices at home. First, nutrition knowledge scores from children and their caregivers were measured using 15 multiple choice questions (each question had 1 correct answer out of 4) on food nutrient composition and healthy diets. Second, a good food and hygiene practices indicator was constructed by aggregating 8 statements answered by caregivers on food and hygiene practices at home, which included, for example, washing hands before eating and not allowing children to regularly consume junk food. The scores are normalized into a range between 0 and 1 by using unity-based normalization ([value-min]/[max-min]). All these indicators were collected 6 months before the blood test during the endline data collection.
Methodological Approach
All data are analyzed using Stata/IC 16.1. We first apply OLS linear regressions to estimate the treatment effect on anaemia and nutrition between the treatment and control groups between the treatment and control groups at the post-endline. Equation 1 displays the main regression where Yik is the outcome variable for each school child i in school k. a is the main coefficient of interest, which is the treatment effect. b captures the association of the control variables with the outcome and uik represents the error term. We cluster standard errors at the school level to allow within-school correlation. 43 We weigh the regression by the inverse probability to attrit using control variables that differed between attrited and nonattrited households. 44

Second, using structural equation modeling (SEM) with a maximum-likelihood estimator, we estimate the effect of the treatment on hemoglobin levels directly and indirectly through mediator variables. These mediators are potential treatment pathways that are expected to drive our main outcome. Structural equation modeling allows estimating the association between endogenous variables. 45 Equations 2 and 3 illustrate the direct and indirect estimation models of the treatment effects.


We assess the mediator effects jointly in one regression since our mediator variables are not independent from one another. 46 The direct effect of treatment on hemoglobin (Hb) controlling for the mediator variables (Mik) is captured with dMHb. The indirect effect through the mediators is depicted in the product of cM and dMHb . The total effect is then the sum of the direct and indirect effects. The error term is captured in uHb ik . The standard errors are derived through cluster bootstrapping. 47 Again, we control for household-specific characteristics.
Finally, we break down the analysis by sex and age of children, as well as by the literacy of the caregiver to explore heterogeneous treatment effects through a moderated mediation analysis. We separate between children above and below the age of 12 since the hemoglobin threshold for anemia changes at this age. 42 We theorize that apart from physical differences between preadolescent girls and boys, there might be behavioral differences that affect treatment outcomes. Likewise, we expect disparities in the outreach of the interventions at home based by the caregivers’ nutritional knowledge. The heterogeneous estimates provide indicative evidence and should be interpreted with caution given the loss of statistical power when including interaction terms.
Results
Sample Balance and Descriptives
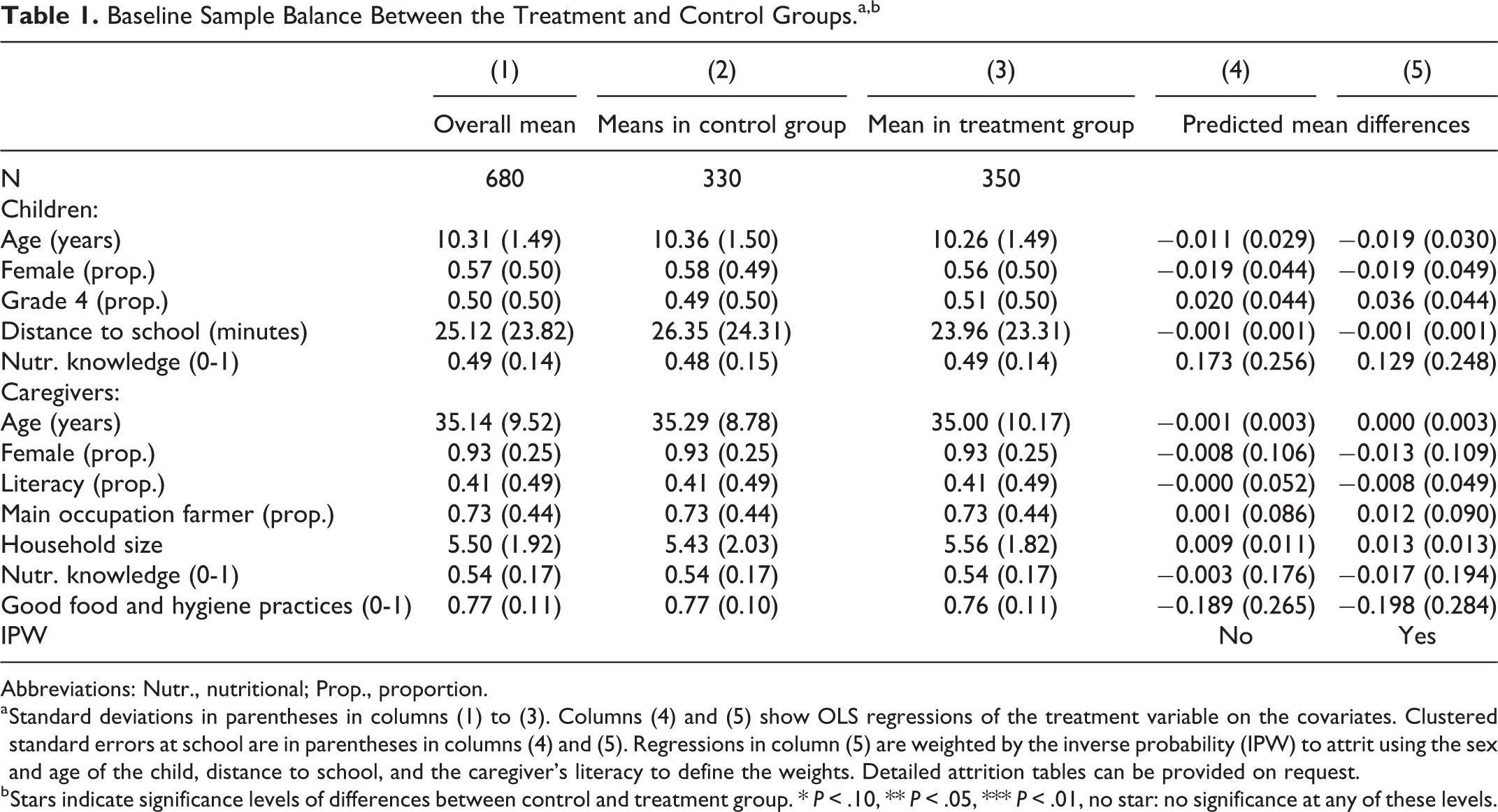
Since the treatment is randomized, there is no need to ensure that the sample at baseline is balanced between the 2 groups. However, given that we have an attrition rate of 22%, we check if the randomization remains valid after attrition. Table 1 compares the baseline mean differences in the characteristics of the children and their caregivers between the treatment and control groups for our post-endline sample (i.e., nonattrited sample). Columns (4) and (5) show OLS regressions of the treatment variable on the covariate. The characteristics do not significantly differ between the 2 groups at both the 5% and 10% levels, which indicates that the sample is balanced.
Baseline Sample Balance Between the Treatment and Control Groups.a,b
Abbreviations: Nutr., nutritional; Prop., proportion.
a Standard deviations in parentheses in columns (1) to (3). Columns (4) and (5) show OLS regressions of the treatment variable on the covariates. Clustered standard errors at school are in parentheses in columns (4) and (5). Regressions in column (5) are weighted by the inverse probability (IPW) to attrit using the sex and age of the child, distance to school, and the caregiver’s literacy to define the weights. Detailed attrition tables can be provided on request.
b Stars indicate significance levels of differences between control and treatment group. * P < .10, ** P < .05, *** P < .01, no star: no significance at any of these levels.
The mean age of the children was 10 years at baseline and 57% were girls. Half of the pupils were in fourth grade. They walk on average 25 minutes to reach their school. They answered, on average, half of the questions on nutritional knowledge correctly. For about 93% of the children, the caregiver is female with a mean age of 35 years; 41% of the caregivers are able to read and write and 73% practice farming. On average, 5 to 6 persons belong to one household. Caregivers responded to 54% of the nutritional knowledge questions correctly. The average score for good food and hygiene practices was 0.77 out of 1 at baseline.
Average Treatment Effect
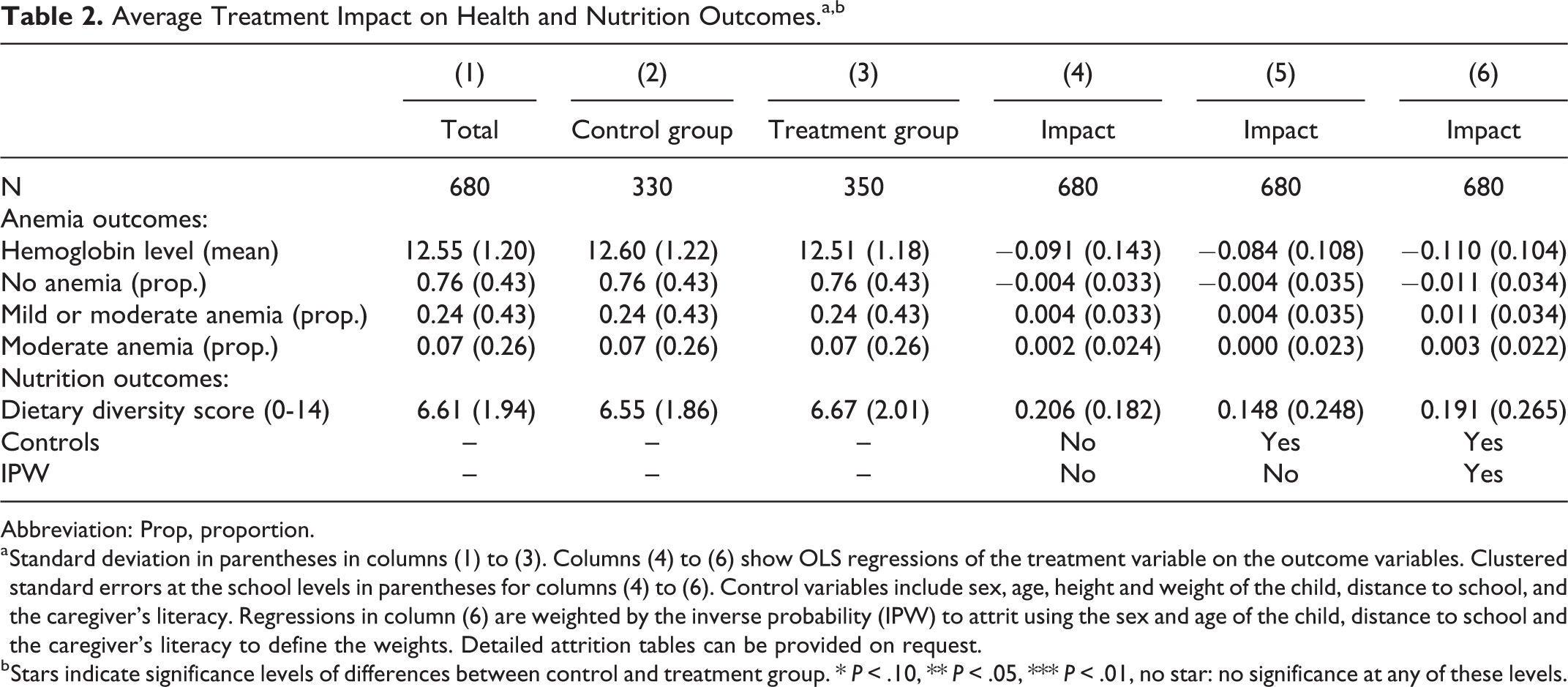
Table 2 shows the treatment effect on anemia and dietary diversity from OLS regressions at post-endline. First, we display the mean values of these outcomes for the overall sample in column (1) and by group in columns (2) and (3). Columns (4) to (6) show the coefficients of the treatment for each of these outcomes without controls, with the inclusion of the control variables, and with controls and inverse probability weighting, respectively.
Average Treatment Impact on Health and Nutrition Outcomes.a,b
Abbreviation: Prop, proportion.
a Standard deviation in parentheses in columns (1) to (3). Columns (4) to (6) show OLS regressions of the treatment variable on the outcome variables. Clustered standard errors at the school levels in parentheses for columns (4) to (6). Control variables include sex, age, height and weight of the child, distance to school, and the caregiver’s literacy. Regressions in column (6) are weighted by the inverse probability (IPW) to attrit using the sex and age of the child, distance to school and the caregiver’s literacy to define the weights. Detailed attrition tables can be provided on request.
b Stars indicate significance levels of differences between control and treatment group. * P < .10, ** P < .05, *** P < .01, no star: no significance at any of these levels.
First, the mean hemoglobin level for the overall sample is 12.55 g/dL; 76% of children are not anemic, 24% are at least mildly anemic, and 7% are moderately anemic. None of the children in our sample are severely anemic. We find no treatment effect on mean hemoglobin levels or anemic status at the 10% significance level. Second, we also find no strong statistical differences on children’s dietary diversity score 6 months after the end of the program, with an overall average score of 6.6 out of 14 points.
In summary, we find that school and home garden interventions did not have any direct causal impact on anemia and dietary diversity 6 months after program support ended. We will interpret further these null findings in the discussion section.
Mechanisms and Heterogeneity
Table 3 displays the findings from our mediation analysis. In line with Schreinemachers et al, 10 we show that the treatment significantly increases the nutritional knowledge of caregivers by 14 % points (P < .01) and good food and hygiene practices used at home by 2 % points (P < .05). Moreover, a better nutritional knowledge of the children and the caregiver is associated with a more diverse diet at post-endline, but this does not drive hemoglobin levels. We do not find a significant indirect effect of the treatment through the mediators. Finally, we find that higher hemoglobin levels are strongly associated with better nutritional knowledge of the children (P < .05). As shown in Table 3, the treatment, however, did not directly impact the nutritional knowledge of children, which partly explains the insignificant total effect of the treatment on hemoglobin.
Direct and Indirect Impacts of the Integrated Home and School Vegetable Garden on School Children’s Hemoglobin Levels.a,b
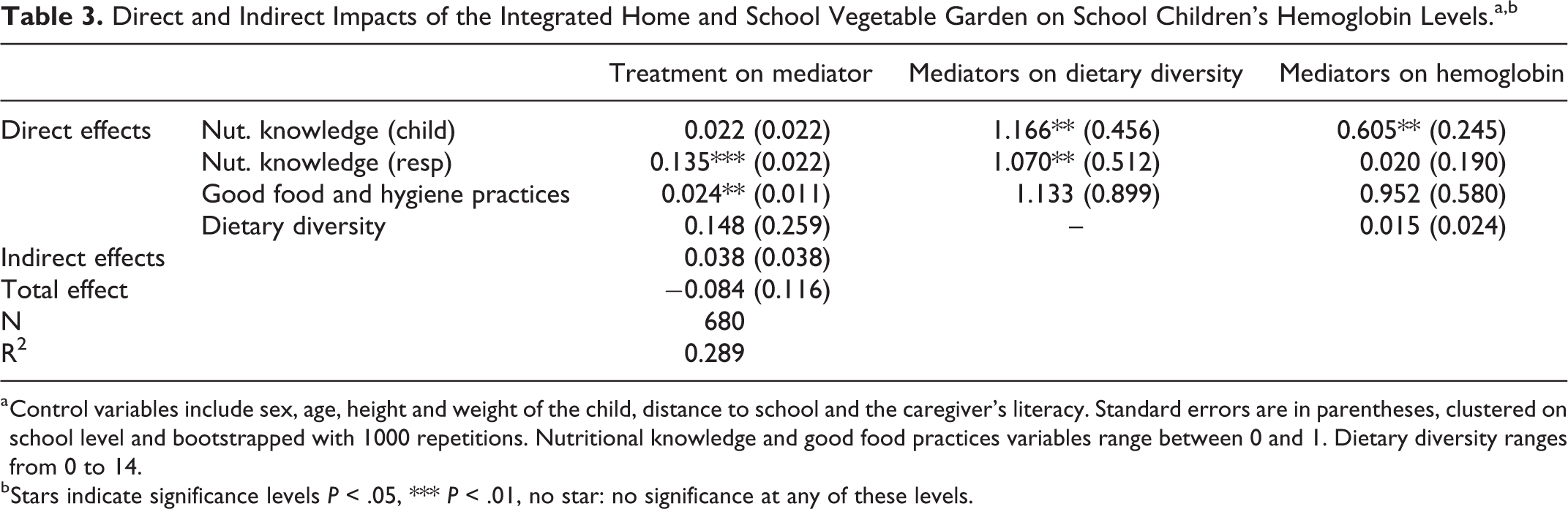
a Control variables include sex, age, height and weight of the child, distance to school and the caregiver’s literacy. Standard errors are in parentheses, clustered on school level and bootstrapped with 1000 repetitions. Nutritional knowledge and good food practices variables range between 0 and 1. Dietary diversity ranges from 0 to 14.
b Stars indicate significance levels P < .05, *** P < .01, no star: no significance at any of these levels.
Table 4 shows the heterogeneous impacts of the mediators on hemoglobin levels for different subgroups: children above and below the age of 12; girls and boys; and children with literate and illiterate caregivers.
Heterogenous Impacts and Pathways of the Integrated Home and School Garden on School Children’s Hemoglobin Levels—Analysis by Age, Sex, and Literacy.
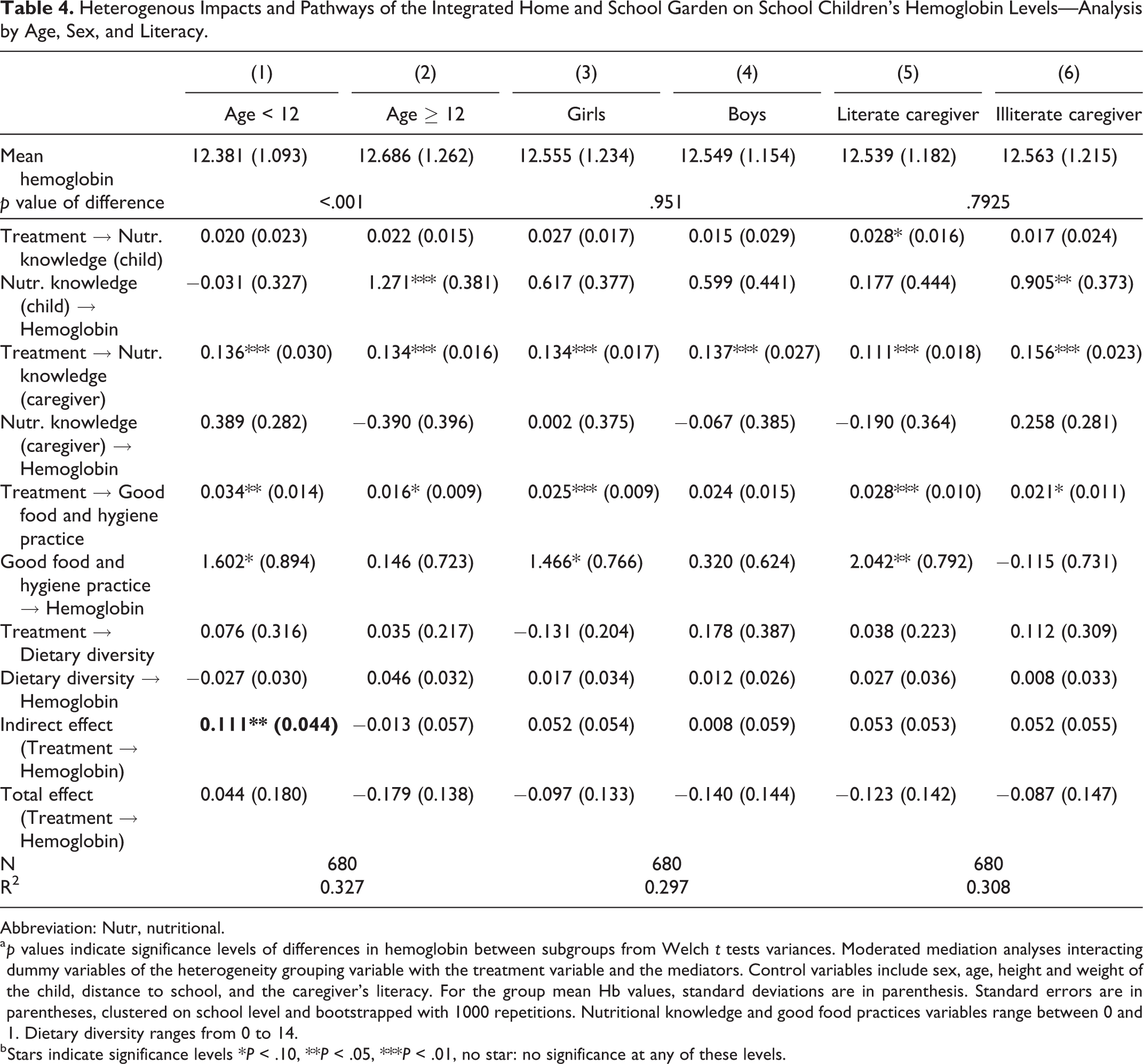
Abbreviation: Nutr, nutritional.
a p values indicate significance levels of differences in hemoglobin between subgroups from Welch t tests variances. Moderated mediation analyses interacting dummy variables of the heterogeneity grouping variable with the treatment variable and the mediators. Control variables include sex, age, height and weight of the child, distance to school, and the caregiver’s literacy. For the group mean Hb values, standard deviations are in parenthesis. Standard errors are in parentheses, clustered on school level and bootstrapped with 1000 repetitions. Nutritional knowledge and good food practices variables range between 0 and 1. Dietary diversity ranges from 0 to 14.
b Stars indicate significance levels *P < .10, **P < .05, ***P < .01, no star: no significance at any of these levels.
The first row in Table 4 shows the average hemoglobin levels for each of these subgroups. We only find significant differences in hemoglobin levels (P < .01) between children older and younger than 12 years, which is expected given changes in hemoglobin levels around the age of 12 years.
Analytically, and in a similar vein to the overall analysis, we do not find any significant direct effects of the treatment on hemoglobin for any subgroup. However, we find a strong positive and significant indirect treatment effect for children under the age of 12 (P < .05) driven through better use of good food and hygiene practices at home (p < 0.01). Despite these positive and notable causal effects. The mediator does not significantly alter the overall effect of the program on hemoglobin. In contrast, for children older than and equal to 12 years, nutritional knowledge of the children is strongly associated with higher hemoglobin levels (P < .01) while food and hygiene practices at home have no effect.
Moreover, we find notable disparities in mediator effects between girls and boys. While for girls, the integrated school and home garden intervention significantly improved good food and hygiene practices (P < .01), there is no such effect for boys. In turn, good food and hygiene practices are also associated with higher hemoglobin levels in girls (P < .1).
Finally, for children whose caregivers are able to read and write, the treatment significantly contributes to better food and hygiene practices at home (P < .01), which are significantly and positively associated with higher hemoglobin levels (P < .5). On the other hand, and in addition to treatment benefits on food and hygiene practices, the nutritional knowledge from the treatment for children living with caregivers who are not able to read and write is strongly associated with higher levels of hemoglobin (P < .05).
Discussion
In this article, we study the impact of an integrated school and home garden intervention on reducing anemia levels in school children aged 9 to 13 from Sindhupalchok in Nepal. We find that 24% of the school children are mildly or moderately anemic. This figure lies within the range of estimates from other studies from Nepal, which found incidences of anemia of 35% among children in the age of 4 to 13 years, 30 38% among children in the age of 6 to 13 years, 31 and 11% to 21% among children and adolescents in the age of 10 to 19 years. 29 In contrast to the latter study, we do not find notable differences between girls and boys, which is attributed to the fact that the majority of our sample is preadolescent.
We build on a previous study in Nepal which found that a combined school and home garden intervention nudged school children to eat more vegetables and their caregivers to include more vegetables in meals and improve overall good food and hygiene practices at home. 10 Despite the potential of this integrated approach in improving overall health beyond the consumption of healthy food, we find no direct evidence of it in reducing anemia (measured through hemoglobin) among preadolescent school children. Previous studies have shown that gardening interventions can have a positive impact on reducing anemia on average. 18,20,25 However, most of the previous studies focus on women of reproductive age and/or children below the age of 5.
One of the main challenges in detecting impact is the difficulty in disentangling the pathways through which combined school and home garden interventions could reduce anemia. Schreinemachers et al emphasize that the combination of increased nutritional knowledge and changing preferences will increase vegetable consumption. 10 This study found a significant improvement in the food preferences and nutritional knowledge of caregivers and a significant increase in children’s preferences for eating vegetables and using healthy food and hygiene practices. Yet, 6 months after the end of the same intervention, we are not able to detect a causal significant impact on improving children’s vegetable consumption or dietary diversity. However, due to the reliance on 24-hour recall for the dietary diversity score, which indicates that 99% of the children ate at least one vegetable in their meals, is not sufficient to capture overall changes in the food behavior toward eating more vegetables. The effect on vegetable consumption detected in the previous study from the same schools used dietary data collected every month in food logbooks.
In comparison to the strong evidence on the role of feeding and fortification programs in reducing anemia among school children, 27,28 the impacts of school and home gardening on anemia are less established for this age-group, and remain empirically unconfirmed. The impacts in reducing prevalence of anemia, found by one other recent study, were only driven by the inclusion of a WASH component to the school garden intervention. Similar to our findings, they do not find a significant impact of the standalone school garden arm on anemia. 25
Moreover, our study shows a strong correlation between good food and hygiene practices at home and higher hemoglobin levels among preadolescent school children. Yet the integrated vegetable garden intervention was not sufficient to drive significantly enough positive changes in these practices to reduce anemia prevalence 6 months after the end of the program. This underscores that treatment strategies for preadolescent children that aim to build on behavioral change around food habits and health are only sustainable if the observed change is long-lasting.
Adding our findings to the meagre existing evidence, we make 2 important observations for future research:
First, components designed to directly improve children’s hygiene practices, like washing their hands before eating meals, are important to decrease the incidence of anemia. We find that good food and hygiene practices explain 7.6% of the variation in hemoglobin levels, and more importantly, they explain the causal impact on the anemia levels of younger cohorts. Particularly for younger school children, good food and hygiene practices clearly explain a detectable causal impacts of the integrated gardens on hemoglobin. What practices are more effective and how these interact with changes in food preferences remain to be established.
Second, school children’s nutritional knowledge is positively associated with stronger hemoglobin levels, which is particularly evident for older cohorts, while good food and hygiene practices work better for younger cohorts. Similar to Schreinemachers et al, we find that the integrated garden intervention did not directly improve children’s nutritional knowledge, 10 which explains part of our null finding. Moreover, caregiver’s literacy and children’s age and gender play an important role in explaining how the mechanisms can drive the overall treatment effect. 15 The disparities between boys and girls around food and hygiene practices is also important for explaining improvements in hemoglobin levels. Future research should carefully assess how food choices and practices at home differ between boys and girls at different ages and how the literacy levels of caregivers shape these differences. For example, are boys allowed to consume more junk food than girls? And if so, what are the reasons for such gendered effect? Answering such questions goes beyond the scope of this study, but the findings reiterate that behavioral measures are key to reduce anemia prevalence, especially for the most vulnerable children.
These 2 observations raise the question if the gardening components are generally necessary to reduce anemia prevalence in school children or if educational and behavioral change tools are more effective. Due to the limitation in scope and design of our study, we are unfortunately not able to disentangle the impacts and mechanisms more clearly, particularly in the absence of preintervention hemoglobin data, and the insufficient information on hygiene practices and exact quantities of food consumed. However, this remains an important question for future research.
Conclusion
Using a cRCT, we show that an integrated school and home garden intervention did not have a direct causal impact on hemoglobin levels among school children in the mid-hills of Nepal 6 months after a year-long intervention. For children under the age of 12, the integrated vegetable gardens intervention improves food and hygiene practices at home (eg, providing less junk food and washing hands before eating), through which the intervention causally and indirectly improves their hemoglobin levels. Improvement in these practices are also notable for girls and children with literate caregivers, but do not mediate the treatment effects on hemoglobin. Moreover, in our moderated mediation analysis using SEM, we find a notable association of the nutritional knowledge of children with hemoglobin levels, particularly for children above the age of 12 years and children with illiterate caregivers. The age and gender difference points at intrahousehold variation in how the treatment works, particularly behavioral changes around the use of good food and hygiene practices, including on whether caregivers apply such practices equally to boys and girls. Our findings indicate that behavioral and educational measures should be a key component of integrated school and home garden interventions to reduce anemia prevalence among school children. More research should be conducted in different settings to confirm the generalizability of these findings for preadolescent school children. Future studies should also assess the effectiveness of multiple behavioral components both jointly and separately to better disentangle the pathways that drive improvements in nutrition and health among school children.
Footnotes
Author Contributions
GB, TB, and PS designed the randomized controlled research study. MS designed the blood sampling and selected blood parameters. RMS collected survey data and AS collected blood sample data. GB and DW merged and analyzed the data and drafted the manuscript. TB, MS, PS, and AS revised and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Drivers of Food Choice (DFC) Competitive Grants Programs, which is funded by the UK Government’s Foreign, Commonwealth and Development Office (FCDO) and the Bill & Melinda Gates Foundation OPP1110043, and managed by the University of South Carolina, Arnold School of Public Health, USA. Additional funding was received from the Leibniz Institute of Vegetable and Ornamental Crops (IGZ).