
Abstract
Background:
Middle childhood and adolescence are critical times for the growth, development, and establishment of healthy eating habits. The Europe and Central Asia (ECA) region has been through economic and nutrition transitions over the past 20 years, which are likely to have affected the nutritional status of this group.
Objective:
This review aimed to collate data on the nutritional status and dietary patterns of school-aged children (SAC) and adolescents (5-19 years) across the ECA region in order to inform policy and programming decisions.
Methods:
A systematic search of the literature in Pubmed, Cochrane, and ScienceDirect databases was conducted (April 2019), complemented by a systematic review of nationally representative surveys. Inclusion criteria were any data on micronutrient deficiencies, overweight, stunting, wasting, thinness, or dietary patterns in SAC and adolescents in the 21 UNICEF-defined countries of ECA, published since the year 2000.
Results:
Results included 134 published papers and 6 sources of survey data. The majority of studies were conducted in Turkey (56%), with all other countries having fewer than 10 studies each; 8 countries in the region having no studies on this age group at all. The most significant nutrition issue was overweight and obesity. Micronutrient deficiencies, particularly anemia, emerge as a further challenge. Dietary patterns were worse in urban areas and boys.
Conclusions:
The findings of this review suggest that there are 3 critical areas that need immediate attention: the promotion of healthy diets and physical activity to address high levels of overweight/obesity, anemia prevention efforts, and addressing the considerable data gaps for SAC and adolescent nutrition.
Introduction
Across the life cycle—from the womb until adulthood—a child’s nutritional needs and the behaviors and influencers on diet evolve and change. While the first 1000 days—from the point of conception to the child’s second birthday—are crucial, middle childhood (age 5-9 years) and subsequent adolescence (defined by the World Health Organization [WHO] as 10-19 years) are also critical times for growth, development, and establishment of healthy eating habits. Middle childhood is marked by continued, steady growth, yet research has shown the potential for children to catch up during this age after early stunting, given the right nutritional environment. 1 Adolescence is a time not only of sexual maturation but also of rapid growth, second only to the first year of life, and therefore also offers a window of opportunity for healthy growth and development with good nutrition. 2 However, it is also a challenging time since rapid physical growth and development during puberty raises nutritional needs, making adolescents especially vulnerable to malnutrition. This is also influenced by increasingly strong gendered cultural norms, which can limit access to nutritious food, education, and economic opportunity, particularly for girls. 3 As reproductive maturity occurs during this critical period, nutrition can also have a profound effect on the health and nutritional status of the next generation. 4
The “Europe and Central Asia” (ECA) region, as defined by UNICEF, is a large and diverse group of 21 countries that have been through economic and nutrition transitions over the past 20 years. 5 This is likely to have affected the nutritional status of adolescents and school-aged children (SAC). The region has exhibited good progress in reducing child stunting, child wasting, and low birth weight in most countries and is on track to meet the 2030 Sustainable Development Goals (SDGs) for these indicators. 6 However, no progress has been made regarding childhood overweight, adult obesity (in all countries in the region), anemia (in all countries of the region), and exclusive breastfeeding (in some countries of the region). 6 More than 55% of adults in the ECA region are overweight or obese, while the number of overweight children younger than 5 years in the region has increased by 80% between 2000 and 2018, from 2.1 to 3.8 million, representing the largest increase globally. 7 Based on these estimates, the number of overweight children is much larger than the number of undernourished children who are stunted or suffer from wasting in all countries. At the same time, millions of children are anemic, or suffer from iodine, zinc, vitamin A, and/or vitamin D deficiencies. 7 These data on younger children and adults provide suggestions regarding the nutritional status of SAC and adolescents in the region.
However, collated evidence on SAC and adolescents in the region is currently lacking. This review aimed to summarize information on the nutritional status (overnutrition and undernutrition and micronutrient deficiencies) and unhealthy dietary patterns of children and adolescents (5-19 years) across the ECA region, in order to assist with evidence-informed advocacy, policy, and programming decisions.
Methods
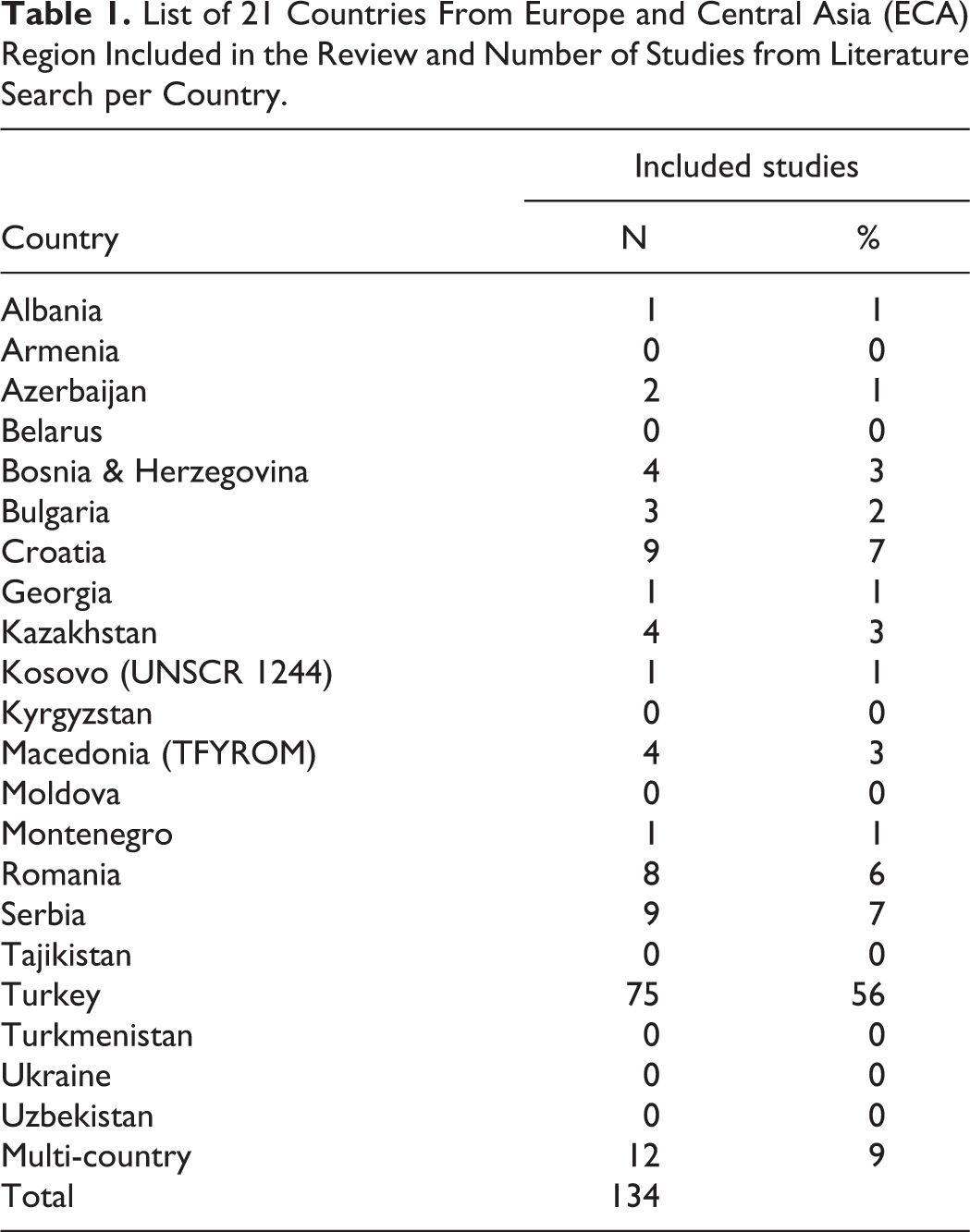
This study consisted of a systematic literature search and a comprehensive review of all publicly available, nationally representative survey data for SAC and adolescents (5-19 years) in the 21 countries in the UNICEF-defined ECA region (Table 1).
List of 21 Countries From Europe and Central Asia (ECA) Region Included in the Review and Number of Studies from Literature Search per Country.
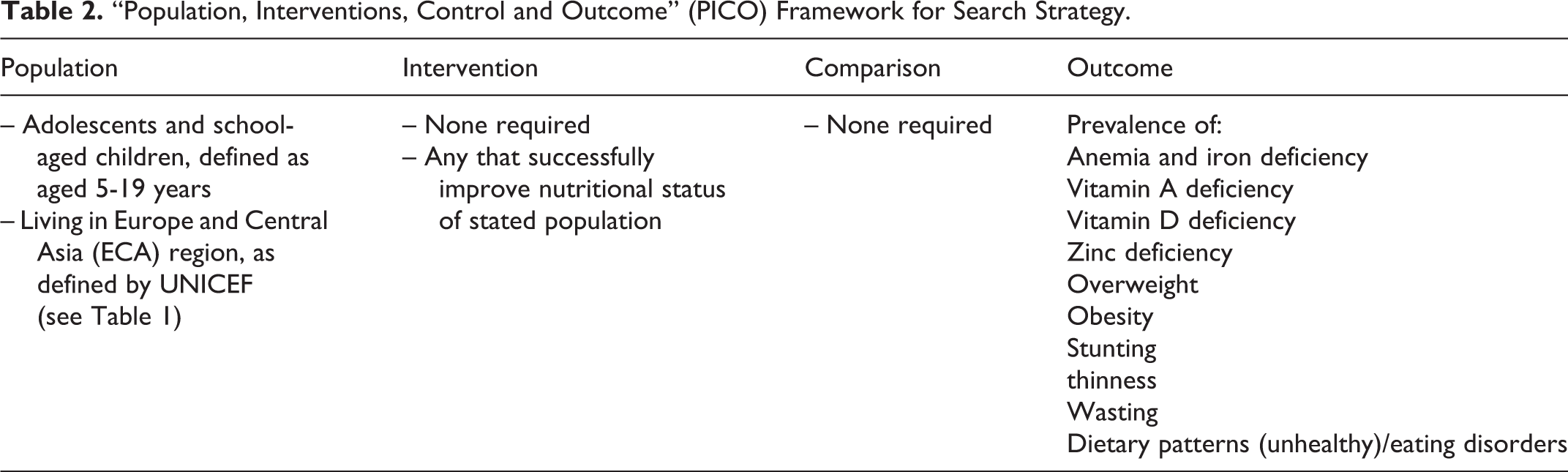
The literature search included Pubmed, Cochrane, and ScienceDirect databases as well as reference lists of eligible publications and expert referrals. The search strategy and eligibility criteria were guided by the “Population, Interventions, Control and Outcome (PICO) framework” presented in Table 2 (exact search terms detailed in Annex 1). Two researchers conducted the screening and study selection process independently (E.M. and N.L.). Gray literature was not eligible for inclusion, nor were papers that focused only on adolescents with diagnosed diseases. Database searches were restricted to “human studies” and studies published since the year 2000; no restriction was placed on study design or language of publication. Data from eligible studies were extracted using a standardized form. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist was followed for reporting results. 8
“Population, Interventions, Control and Outcome” (PICO) Framework for Search Strategy.
The survey review examined nationally representative surveys that included data on nutritional status (overnutrition and undernutrition, micronutrient deficiencies) or dietary patterns of children and adolescents (5-19 years) across the ECA region (n = 21) from 2000 to 2019. Data were not included when it was not nationally representative, or for overnutrition calculated based on adult body mass index (BMI) thresholds (BMI values adjusted for age using global reference data, which is more appropriate, 9 are included). The classifications of anthropometric and micronutrient status used in this study are provided in Box 1. Studies using a variety of references (WHO/International Obesity Task Force [IOTF]/Centers for Disease Prevention and Control [CDC]) for overweight and obesity were included. Due to the heterogeneous coverage of studies and survey data, we have avoided presenting aggregated figures for the region; however, it is important to note that where prevalence data are presented, they are not weighted by sample size.
Classification of Anthropometric and Micronutrient Status.
Undernutrition
Stunted or short stature: height-for-age <−2 SDs below the WHO 2007 Growth Reference median
Thinness: BMI-for-age <−2 SDs below the WHO 2007 Growth Reference median
Overnutrition
WHO 2007
Overweight: BMI-for-age >+1 SD above the WHO 2007 Growth Reference median
Obese: BMI-for-age >+2 SD above the WHO 2007 Growth Reference median
International Obesity Task Force (IOTF)
Overweight: equivalent to BMI ≥25 at 18 years using IOTF sex-specific references
Obese: equivalent to BMI ≥30 at 18 years using IOTF sex-specific references
Centers for Disease Prevention and Control (CDC)
Overweight: BMI-for-age expressed as ≥85th percentile of the CDC growth reference
Obesity: BMI-for-age expressed as ≥95th percentile of the CDC growth reference
Micronutrient status
Anemic
Children aged 10-14 years: hemoglobin concentration <115 g/L; nonpregnant girls aged ≥15 years, <120 g/L
Pregnant girls aged ≥15 years, <110 g/L (WHO, UNICEF, UNU, 2001)
Boys aged ≥15 years, <130 g/L
Iodine
Median urinary iodine concentration:
insufficient <100 µg/L, adequate 100-299 µg/L, and excessive 300 and above µg/L
Vitamin D deficiency
serum 25(OH)D levels at <20 ng/mL
Results
The systematic literature search, conducted on April 25, 2019, screened 4869 titles and abstracts and found 272 potentially eligible full texts (flow diagram in Figure 1). One hundred thirty-four full texts were found to be eligible for inclusion based on our PICO framework (summary data extraction for all text in Annex 2). The majority of studies were conducted in Turkey (56%), with all other countries having fewer than 10 studies each; 8 countries in the region having no studies on this age group at all (Table 1).
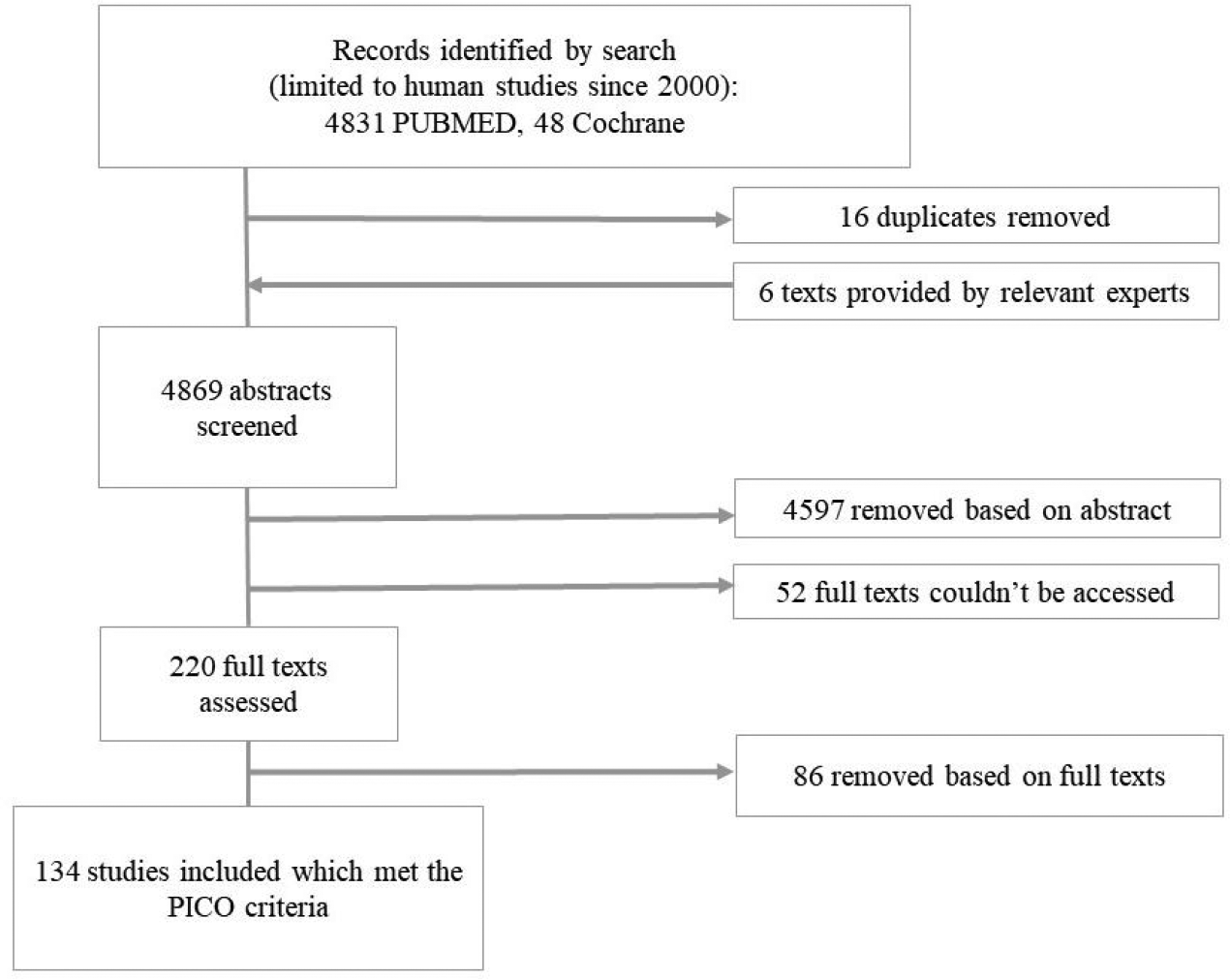
Literature research results flow diagram. PICO indicates population, intervention, control, and outcome.
Summary of Included Data Sources From Survey Review.
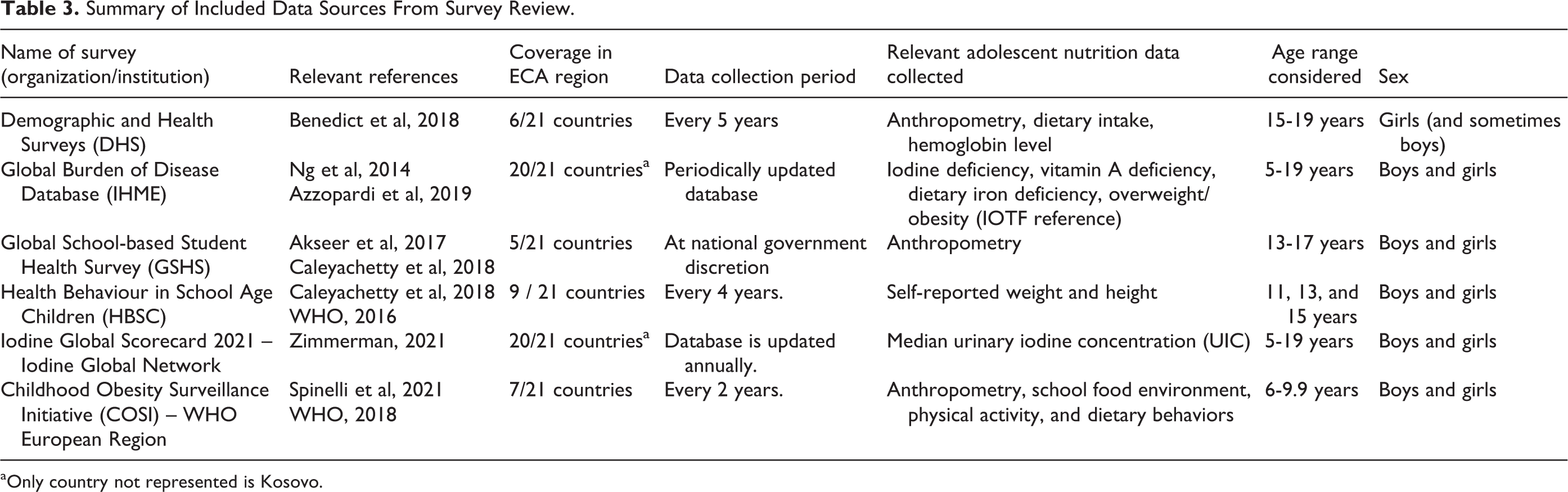
a Only country not represented is Kosovo.
Summary of Surveys Included Detailed by Country, Age, Sex, and Indicator.a
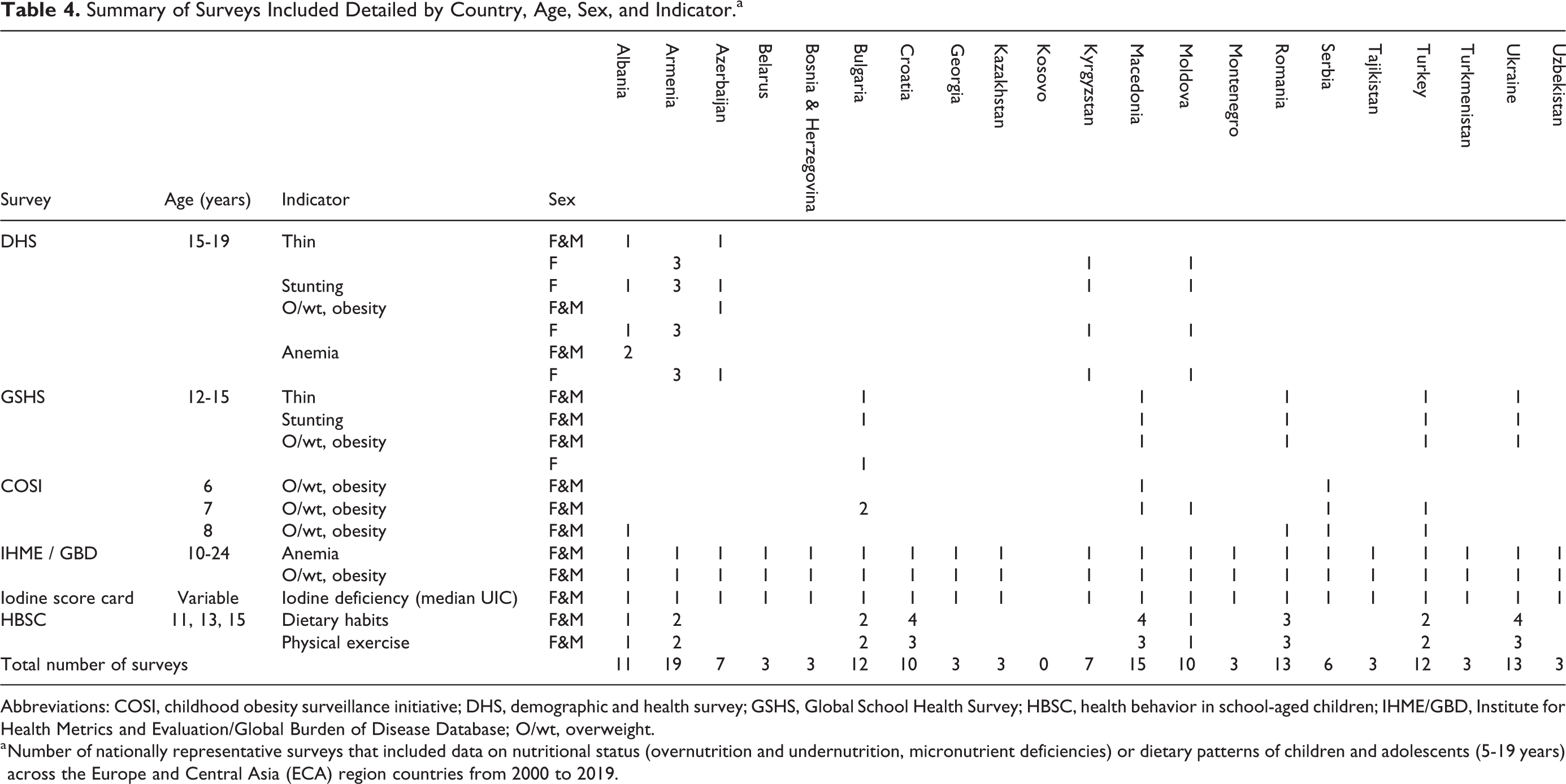
Abbreviations: COSI, childhood obesity surveillance initiative; DHS, demographic and health survey; GSHS, Global School Health Survey; HBSC, health behavior in school-aged children; IHME/GBD, Institute for Health Metrics and Evaluation/Global Burden of Disease Database; O/wt, overweight.
a Number of nationally representative surveys that included data on nutritional status (overnutrition and undernutrition, micronutrient deficiencies) or dietary patterns of children and adolescents (5-19 years) across the Europe and Central Asia (ECA) region countries from 2000 to 2019.
Overweight and Obesity
A summary of the maximum and minimum prevalence values by country, from both the surveys and the literature, is presented in Figure 2. All countries in the region, except Kosovo, had multiple sources of overweight and obesity data. The lowest prevalence estimates were 7.7% in Kyrgyzstan and 7.9% in Ukraine; the highest estimates were 41% in Bulgaria and 52.2% in Macedonia. Boys were generally more overweight or obese than girls across many of the studies reviewed. 10 Some studies, for example, a study of younger children (6-9 years) in Serbia in 2015, found no difference in the prevalence of overweight and obesity between girls and boys, so it is possible that differences in lifestyle, eating habits, and BMI only happen later in adolescence. 11
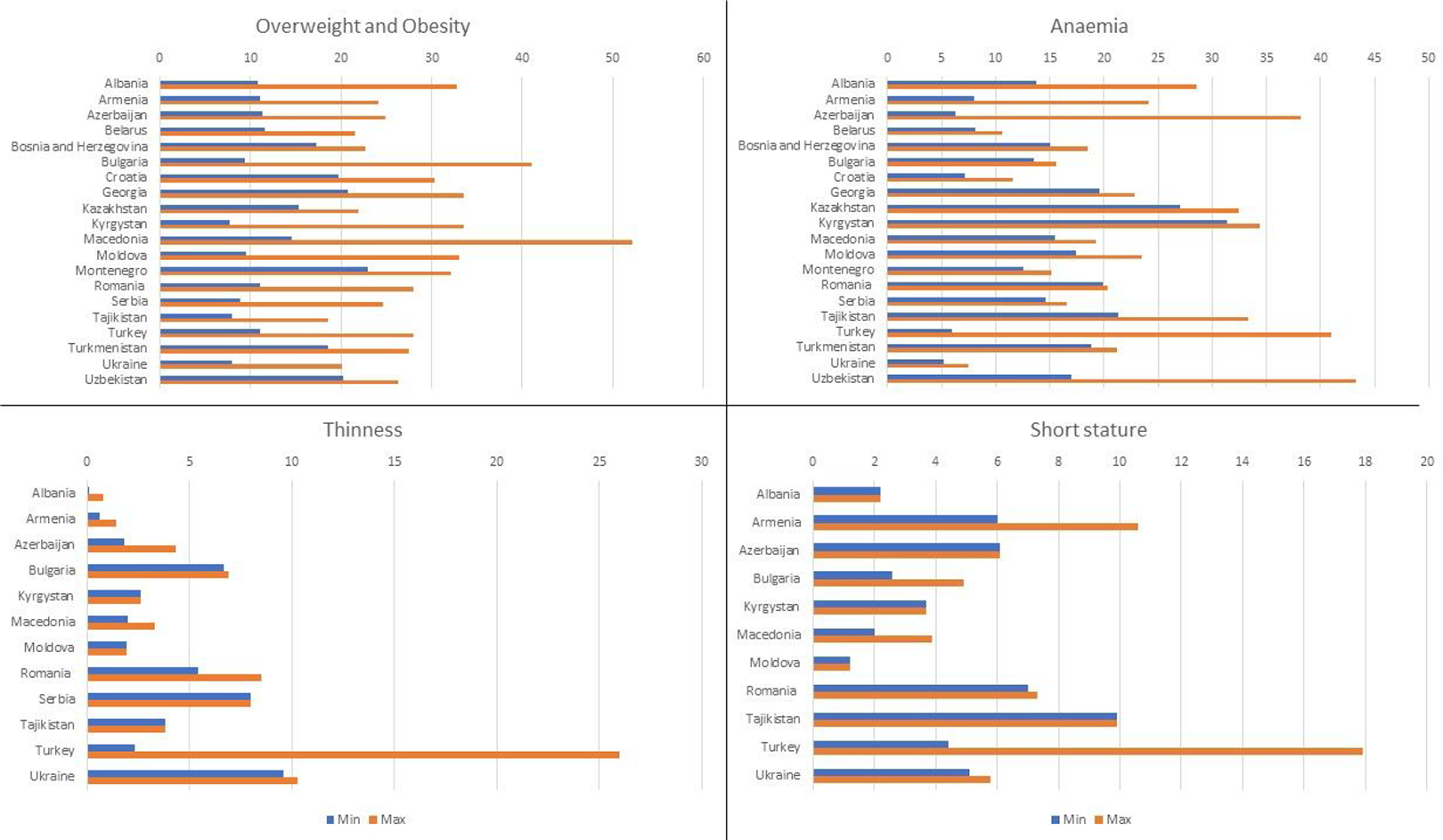
Minimum and maximum prevalence values in the literature for different types of malnutrition per country in the region.
Studies from the region have shown many factors to predict the likelihood of being overweight and obese in childhood and adolescence. These range from the individual level to the family level and larger environmental factors. Being male, being in the younger category of adolescents, and living in an urban area were all found to be predictive of obesity. 12,13 Lifestyle factors such as energy intake and physical activity are already impacting on rising levels of overweight and obesity in children and adolescents. 14 A study in Turkey found that skipping breakfast was associated with a higher risk of obesity. 15 Parental obesity, low socioeconomic status (SES), and having a mother working out of the home have also all been linked to an increased risk of being overweight among SAC and adolescents, especially in contexts of economic transition and increased availability of processed and “junk” foods. 14,16 A multicountry study involving adolescents from Romania, Bulgaria, and Turkey has established a relationship between television viewing time and overweight and obesity. 17 For example, among school children in Turkey, there was greater obesity in those who spent at least 3 hr/d watching television. 18
Stunting/Short Stature
Only 52% (11/21) of countries in the region had 1 or more prevalence estimates for stunting/short stature in SAC and/or adolescents. The prevalence of stunting was less than 10% in 10 of 11 countries in the region where data were available (Figure 2). 19 The highest level was reported in boys in Turkey (17.9%). Data on boys specifically were only available for 5 countries (Macedonia, Tajikistan, Azerbaijan, Armenia, and Turkey). Studies from the region found levels of stunting, underweight, or thinness to be associated with very low SES. 20,21
Micronutrient Status
Data on anemia prevalence was available for all countries in the region, except Kosovo (Table 4). The review found a wide range of anemia prevalence across the region, ranging from 5% in Ukraine to 43% in Uzbekistan (Figure 2). Eight countries reported that, among SAC and adolescents, more than 1 in 5 girls (prevalence of > 20%) were anemic. The prevalence was also high in boys; 6 countries reported more than 1 in 5 boys as being anemic. In Balkan countries, the prevalence of anemia among boys tended to be higher than for girls. Although the reasons for this are not clear, one study from Turkey reported that boys with low SES were more likely to consume iron absorption inhibitors (tea) and less likely to eat iron absorption enhancers (citrus fruits) whereas girls were less likely to consume iron absorption inhibitors. 22
Data were also available for iodine status and vitamin D deficiency for SAC and adolescents in surveys and research in the region. Survey data from the Global Iodine Scorecard showed that all countries in the region had an “adequate” intake of iodine among SAC (age range varies by country; approximately 6-14 years), except for 1 (Ukraine), which was insufficient in 2002 but had no recent survey. While many studies from the region have shown considerable improvements in iodine status with the rollout of salt fortification, 23,24 some studies indicate “pockets” of deficiency in particular locations or demographic groups. 25,26
Vitamin D deficiency was examined by a study in Turkey in 2015 at the end of winter and summer in children and adolescents (3-17 years). The end-of-winter estimates of deficiency was reported to be very high across both sexes at 80%, while the end-of-summer levels of the vitamin were only still low in girls. 27 Sunlight exposure was significantly higher in boys, which may explain some of the difference between the sexes. Those with a sufficient dairy product, consumption had significantly higher vitamin D levels at both the end of summer and the end of winter. Limb pain was frequently reported in children with low vitamin D. Other studies in Romania and Croatia also reported high levels of vitamin D insufficiency and deficiency. 28 Evidence of other micronutrient deficiencies was not found.
Dietary Habits and Physical Exercise
Table 5 provides information from 9 countries that have data on dietary patterns and physical activity from the Health Behavior in School-aged Children (HBSC) survey. 29 Overall levels of physical exercise and daily fruit and vegetable consumption are low for many countries. Less than 25% of girls and less than 35% of boys were achieving the minimum recommended levels of exercise in most countries, and in all countries, fruit and vegetables are consumed daily by less than 50% of the population sampled. Trend data are available for 4 countries (Croatia, Macedonia, Romania, and Ukraine), suggesting that the percentage meeting minimum standards of physical exercise (at least 60 min of moderate exercise daily) has increased between 2002 and 2014 across all 4 countries and in most countries by more than 5% between surveys. There are also some encouraging signs of reductions in daily consumption of sweets and soft drinks and some increasing daily vegetable consumption in Romania and Macedonia. Very broadly, boys appear to eat fewer vegetables than girls and drink more soft drinks, which is noted in some of the literature, 30 but have higher levels of exercise.
Summary Data of the Percentage Meeting Recommended Dietary and Physical Activity Levels Based on HBSC Surveys, 2002-2014.
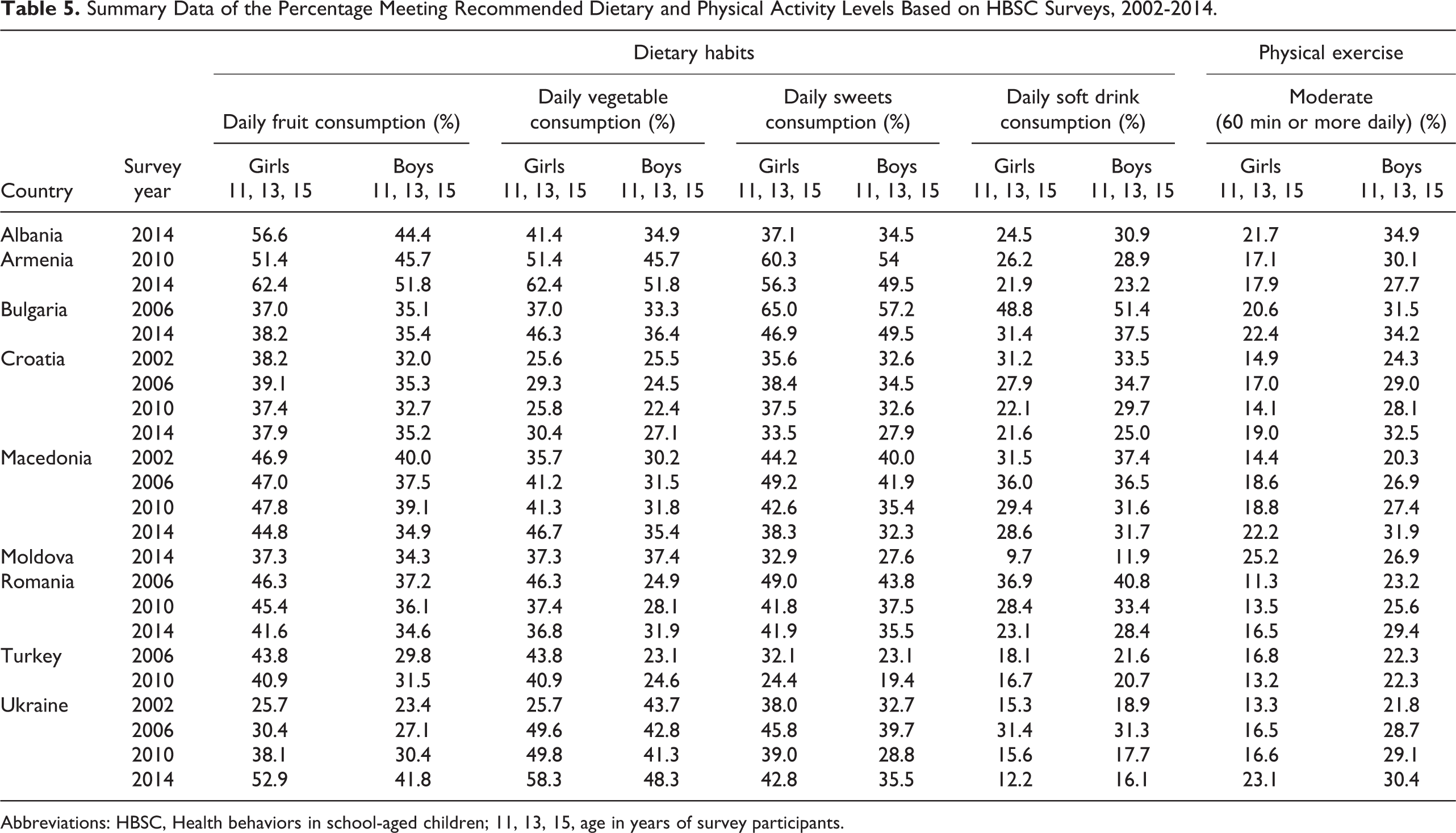
Abbreviations: HBSC, Health behaviors in school-aged children; 11, 13, 15, age in years of survey participants.
Breakfast consumption patterns have also been the focus of many studies in the literature. One multicountry study reported daily breakfast consumption among adolescents to be highest in Ukraine (64.0%), followed by Macedonia (57.3%) and Croatia (55.0%), and was lowest in Hungary (46.0%). Trends of daily breakfast consumption decreased for both boys and girls in all countries between 2002 and 2010, except in Macedonia where there was an increase both for boys and girls. 31
One study reported that television adverts had an important influence on the types of foods adolescents chose in Romania. 32 In a sample of adolescent girls, most of them reported seeing unhealthy food adverts on television (66.0%), while only 48.0% reported seeing healthy adverts. Healthy food advertisement exposure was positively associated with fruit and vegetable consumption, even though perceived levels of “self-control” were also a strong predictor of the consumption of healthy foods. Place of residence also appeared to be associated with eating behaviors; those from urban areas reported less healthy eating behavior, with higher consumption of soft drinks and snacks than those living in rural areas. 33 One school-based intervention involving a small number (139) of 12- to 13-year-olds in Croatia attempted to control eating attitudes in adolescents using education and practical sessions (2 hr/wk). 34 The intervention significantly reduced eating disorder attitudes and dieting behavior, especially in females.
Discussion
Our review highlights the limited availability of nutritional data for this age group and explores the nutritional issues in the ECA region. Survey data are largely available for overweight and obesity, anemia prevalence, and iodine deficiency, but lacking for other indicators of nutrition status such as thinness, stunting, zinc, and vitamin A deficiencies. Published research on the nutritional status of SAC and adolescents varies widely by country with most evidence from the region coming from Turkey. Eight countries in the region have no published studies on this topic at all.
Although the data are complex and, this therefore, presents challenges for assessing trends, the available data suggest that the most significant nutrition issue among SAC and adolescents throughout the region is overweight and obesity. The prevalence of thinness was often not reported in articles and while it is likely to be less prevalent than overweight and obesity, this presents a missed opportunity to estimate trends. Consumption of fast foods, soft drinks and sweets was also notably high in this age group, and levels of breakfast consumption may be decreasing. In addition, the majority of adolescents are not reaching minimum levels of daily physical exercise. Many of the papers reviewed here suggested that children and adolescents living in rural areas had better diets, and boys were more physically active than girls, although girls were more conscious of their weight and eating habits. Greater prevalence of obesity in younger rather than older adolescent ages may reflect changes in behavior as adolescents age or may simply reflect weight gain prior to the adolescent growth spurt. The growth spurt is difficult to accurately reflect in reference data and, therefore, disruptive to accurately assessing adolescent anthropometric indicators. 35
While adolescent overweight and obesity prevalence rates are rising across the region, they are mostly similar to other European countries. 10,36 It may, therefore, be helpful for countries in the ECA region to investigate what measures other European countries are implementing and apply successful strategies to their contexts. A number of initiatives are underway across Europe, including the Physical Activity Strategy for the WHO European Region 2016–2025; the “The Healthy Lifestyle Promotion and Care of Non-Communicable Diseases Act,” which was enacted by the Maltese government in 2016; the introduction of a tax on sugary drinks in England in 2018; and initiatives in Turkey to regulate marketing and TV advertising. Although the literature did not reveal any coordinated strategies across countries, school-based education interventions were the most widespread. Multisectoral strategies to improve nutritional outcomes may include regulation of advertising, enhancing availability/provision of healthy foods at and around schools, and nutrition education through mass public campaigns targeted to school children. 37
Another key nutritional issue in the region is anemia, which remains high in many countries and affects both sexes. The absence of robust national strategies to address anemia, such as flour fortification, in many countries of the region may be among the major factors contributing to the high prevalence. 38,39 Besides anemia and iodine deficiency, data on other micronutrient deficiencies was sparse. Vitamin D deficiency has been noted as a concern in Bosnia and Herzegovina and Turkey, while iodine deficiency prevalence appears to be decreasing as improvements in fortification of salt are realized. However, iodine deficiency still exists in subnational pockets, which highlights the importance of disaggregating data at the subnational level and gathering evidence on minority groups. 40,41 For example, the Roma population are an important minority group living in several countries in Europe; however, there were few studies on SAC and adolescents, specifically focusing on this population. It would be helpful to further examine the nutritional status of marginalized groups, as tailored strategies may be required to address identified deficits.
Limitations
The prevalence of different forms of malnutrition among the adolescent population of the ECA region is difficult to assess. This is because representative and comparable data on the nutritional status of adolescents are severely lacking. Differences between age group categories (for example, see Table 4), reference populations used (IOTF/WHO 2007/CDC), methods of assessment (self-reported anthropometry vs measured), and differences in thresholds for classification limit the comparability and assessment of trends. Research data are lacking from 8 countries in the region, and the majority of the research is from European countries, Turkey in particular, which makes it difficult to draw general conclusions. Central Asian countries are especially under-represented, and the nature of nutrition problems in these countries may be quite different to that of European countries.
Conclusions
Despite the availability of a number of articles and surveys, our review shows a lack of research in a number of countries as well as in minority vulnerable groups. Where data are available, it is difficult to interpret and compare, due to differences between the age groups studied, the use of different reference populations, and differences in the thresholds used to classify malnutrition in children. In order to inform policies and interventions for middle childhood and adolescent nutrition, more robust, standardized data are required. Where studies do exist, they tend to focus on the issue of overweight/obesity and associated risk factors as well as the occurrence of some micronutrient deficiencies—mainly iron, iodine, and vitamin D. Data on thinness, underweight, and other micronutrient deficiencies are lacking. The findings of this review suggest that there are 3 critical areas requiring immediate attention in the region: the promotion of healthy diets and physical activity to address high levels of overweight/obesity and micronutrient deficiencies, scale-up of anemia prevention efforts, and measures to address the considerable data gaps and challenges in assessing nutrition in SAC and adolescents.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721231163021 - Nutrition of School-Aged Children and Adolescents in Europe and Central Asia Region: A Literature and Survey Review
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721231163021 for Nutrition of School-Aged Children and Adolescents in Europe and Central Asia Region: A Literature and Survey Review by Emily Mates, Natasha Lelijveld, Zakari Ali, Kate Sadler, Amirhossein Yarparvar, Tamsin Walters, Rebecca Brown and Basil Rodriques in Food and Nutrition Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: The work (research and support for publication) was funded by UNICEF.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.