
Abstract
Background:
Management of moderate acute malnutrition (MAM) in children needs to improve to reduce the transition from MAM to severe acute malnutrition (SAM).
Objective:
This study aimed to assess barriers to management of MAM among children aged 6 to 59 months in Damot Pulassa, Wolaita, South Ethiopia.
Method:
This descriptive phenomenological design used 6 focus group discussions with mothers or caregivers of children aged 6 to 59 months and 10 in-depth interviews with health service providers. Data were analyzed using Colaizzi’s descriptive phenomenological method.
Result:
Six themes were identified: Possible reasons for MAM; identification of a child with MAM; management services of MAM; maternal-level barriers; service provider-level barriers; and suggestions to improve the service. Shortage of food and money, selling out of self-produced food without having sufficient reserves at home, large household size, shame from having children with malnutrition, occasional house-to-house screening for MAM, family-initiated screening, leaving the management responsibility of children with MAM to the family, no provision of supplementary food, and lack of repeated follow-up visits were the main obstacles for managing MAM.
Conclusion:
Maternal-level barriers and service provider-level barriers affect the management of MAM negatively in Damot Pulassa, Wolaita. Children with MAM living in the area ineligible for food supplementation could deteriorate to SAM. The provision of nutrition counseling to the mothers of children with MAM without food supplementation placed children with MAM at increased risk of negative outcomes. Thus, the government should give more attention and facilitation in promoting supplementary food into the existing management of MAM.
Keywords
Introduction
Worldwide, moderate acute malnutrition (MAM) affects approximately 33 million children below 5 years of age, and these children have a 3 times increased risk of death compared to well-nourished children. 1,2 Moderate acute malnutrition is defined by a weight-for-height z-score between −2 and −3 and/or mid-upper arm circumference (MUAC) of between 11.5 cm and 12.5 cm, without bilateral pitting edema. 3 -5 A large number of guidelines for managing MAM exist. 5 -7 However, there is currently no standardized method for managing MAM. 6,8 If children with MAM do not receive adequate management, they may progress toward severe acute malnutrition (SAM), which could be a life-threatening condition. However, MAM has not received the consideration it deserves and is not frequently seen as of public health importance. 8,9
The supplementary feeding program is one of the recommendations for the management of children with MAM. Supplementary feeding programs are classified as targeted supplementary feeding programs or blanket supplementary feeding programs, depending on the beneficiaries. A blanket method delivers supplemental food to all vulnerable children within a definite population, irrespective of whether or not children are acutely malnourished. This method has been used to treat MAM when prevalence rates are higher than 20%. A targeted approach offers supplemental provisions only for children with MAM. It is frequently chosen when MAM and SAM prevalence rates are from 10% to 14%. 7,8
In conditions where caregivers may have access to affordable food, but the knowledge and practices in how to use it are limited, nutrition counseling has been used as a method for MAM management. Nutrition counseling emphasizes disseminating information on appropriate feeding practices, which can improve dietary diversity and achieve desired nutritional outcomes, as well as progress in hygiene and sanitation practices. 10
Challenges faced in MAM management include the high unit cost of products, having low coverage of programs, focusing on generalized prevalence rates rather than season-specific incidence rates, and frequent high defaulting. Using a variety of definitions and classifications across different MAM management programs is also considered a challenge. This leads to confusion over the inclusion and exclusion criteria for MAM. 6,11
In Ethiopia, the current strategy for managing MAM is to restrict targeted supplementary feeding programs to particular districts of the country defined as chronically food insecure. In areas not selected as chronically food insecure, there are no food supplementation programs. In such areas, the alternative management approach consists of vitamin A supplementation and deworming, water treatment to make appropriate for drinking, enhanced sanitation, and nutrition counseling. 4,12
A key step toward better future programs and policies is to improve our understanding of the community’s and health care workers’ views, experiences, and preferences of maternal and child health care services. Discussion with mothers who are the primary caregiver of a child and service providers provides insight about barriers to management of MAM among children aged 6 to 59 months. Such contextual knowledge contributes to the development of recommendations on the management practice of MAM that could be implemented at the local level and improve existing management guidelines of MAM among children. Little research has been done to assess community perceptions toward barriers of the existing management practices for MAM in Ethiopia, both among the service providers and beneficiaries. There is a high prevalence of malnutrition in the country. This study aimed to explore barriers to management of MAM among children aged 6 to 59 months in Damot Pulassa, Wolaita, South Ethiopia: a phenomenological study of mothers and health service providers.
Methods and Materials
Study Setting and Study Period
This study was conducted in Damot Pulassa district of Wolaita Zone, which is located 328 kilometers south of Addis Ababa. Damot Pulassa is a rural district with an estimated population of 130 515 people, and a population density of 700 people per square kilometer. 4,13 There is a persistent disparity in the land and population balance resulting in endemic food insecurity because the district is characterized by fragmented farm and land ownership. 14 The population is mainly growing maize, beans, and sweet potatoes. Rain failure and pests are persistent problems and frequently drive much of the population into hunger and malnutrition. Damot Pulassa has 5 health centers and 23 health posts. These health posts are led by health extension workers (HEWs) and deliver nutrition-linked services like nutrition education, screening of the nutritional status of young children, and nutritional management of malnourished children. The study was carried out between June and July 2018. In that period, there was no targeted supplementary feeding program in the area.
Study Design
This study used a descriptive phenomenological qualitative design. This design is used to attain an understanding of the right meaning of a phenomenon of interest through engaging detailed descriptions of the mothers or caregivers and service provider’s perception toward barriers during managing acute moderately malnourished children. 15,16 In this approach, the perception of researchers is bracketed or set aside, to acquire the lived experience of the participants. 17
Study Population and Sampling Procedure
In the 6 focus group discussions, 8 to 10 mother or caregiver-child pairs per group were recruited. The total number of mother or caregiver-child pairs who participated in the study was 55. To identify subjects that are especially knowledgeable about or experienced informants toward the existing management practice of MAM and its barriers, the mothers or caregivers were purposively enrolled from the community with the assistance of HEWs who know the local population. The rationale and power of purposeful sampling are found in selected cases with a lot of information to explore in-depth. Information-rich cases are those from which a lot can be learned about topics that are important to the objective of inquiry, hence the term “purposeful sampling.” Studying information-rich cases gives insights and in-depth understanding toward the study topic. 18 The recruitment criteria for mothers or caregivers was that they had a child or children aged 6 to 59 months currently suffering from MAM who had been admitted to the management program for MAM. Ten in-depth interviews were carried out with 4 HEWs and 6 Women’s Development Army workers (WDAs); these are first-level community-based health care volunteers who provide support in the management practices for acute malnutrition. Informants were purposely selected from the HEWs and WDAs based on their relevant experience (i.e., they function in a role detecting and managing children with MAM). None of the potential participants declined to participate.
Research Instrument
Open-ended, semi-structured focus group discussion guides and in-depth interview guides were developed following an extensive review of the relevant literature. The focus group discussion and in-depth interview guides were prepared in English and translated into the local language, Wolaitato. This was followed by a back-translation into English to ensure internal validity. A pilot study comprising one focus group discussion and one in-depth interview was carried out among respondents who were not included in the study samples. The pilot test aimed to determine whether the particular focus group discussion and in-depth interview guides were clear, thus confirming reliability.
Data Collection
The focus group discussions were applied by the first author and research assistants (2 facilitators and one notetaker). The research assistants are trained on study objectives and methodology and were fluent in Wolaitato, the local language spoken by mothers. Before starting the data collection, the participants were informed about the objective and procedure of the study. Participants were then asked about their willingness to continue and to provide oral as well as written informed consent. The focus group discussions were conducted in privacy at sites that were accessible to participants (i.e., health posts and health centers). During focus group discussions, each mother or caregiver had the chance to share her opinions on a question raised before moving to another question in which active participation was ensured. Each focus group discussion lasted between 50 and 70 minutes.
Face-to-face in-depth interviews were the second method of data collection done by the first author using the local languages of HEWs and WDAs, Wolaitato. Probing to get detailed information was done. All the in-depth interviews were performed privately at the workplace of each health worker. Two trained research assistants helped the first author with note-taking and audio recording. Each in-depth interview had an approximate duration of 60 to 80 minutes.
Focus group discussions and in-depth interviews were done until saturation of content was achieved; this occurs when additional interviews do not provide new information to data already collected and they become simply redundant. 19 At the end of focus group discussions and in-depth interviews, the facilitator of focus group discussions and the interviewer of in-depth interviews moderated the scribed content of the notes to define assertion and meaning with mothers to improve face validity. Data collected from focus group discussions and in-depth interviews were audio-recorded with permission from the participants.
Trustworthiness and Quality Assurance
Based on 4 dimension criteria, we kept the data collection scientifically rigorous and trustworthy. 20 Credibility: To accomplish this, we have spent time in the field, done peer debriefing and member check. To obtain an in-depth understanding, it has been kept throughout group discussion and interview. Dependability: With the help of the supervisor, the research team created a data audit to ensure that the data and findings were rich-thick, consistent, and stable over time. Confirmability: We were able to assess the accuracy of the results and the truthfulness of the participants’ perspectives by using data audit and triangulation. Transferability: We have done purposive sampling to get specific data relative to the context. In addition, we provided detailed descriptions to help readers determine whether the findings could be applied to their situation.
Data Analysis and Management
Data collected in the focus group discussions and in-depth interviews were transcribed verbatim (a word-for-word record). Transcription of interviews was assisted by Express Scribe transcription software (Pro v 7.03 NCH Software Pty Ltd). An initial coding framework was generated by the primary researcher and research assistants after manual coding of transcripts independently. Data were analyzed using Colaizzi’s descriptive phenomenological method. Using this approach, there are 7 steps involved in analysis of qualitative data 21 (Figure 1). The data were imported and coded in the computer software of ATLAS.ti 8 and analyzed by the same software (Scientific Software Development GmbH). The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was used to report findings (Supplement 1). 22
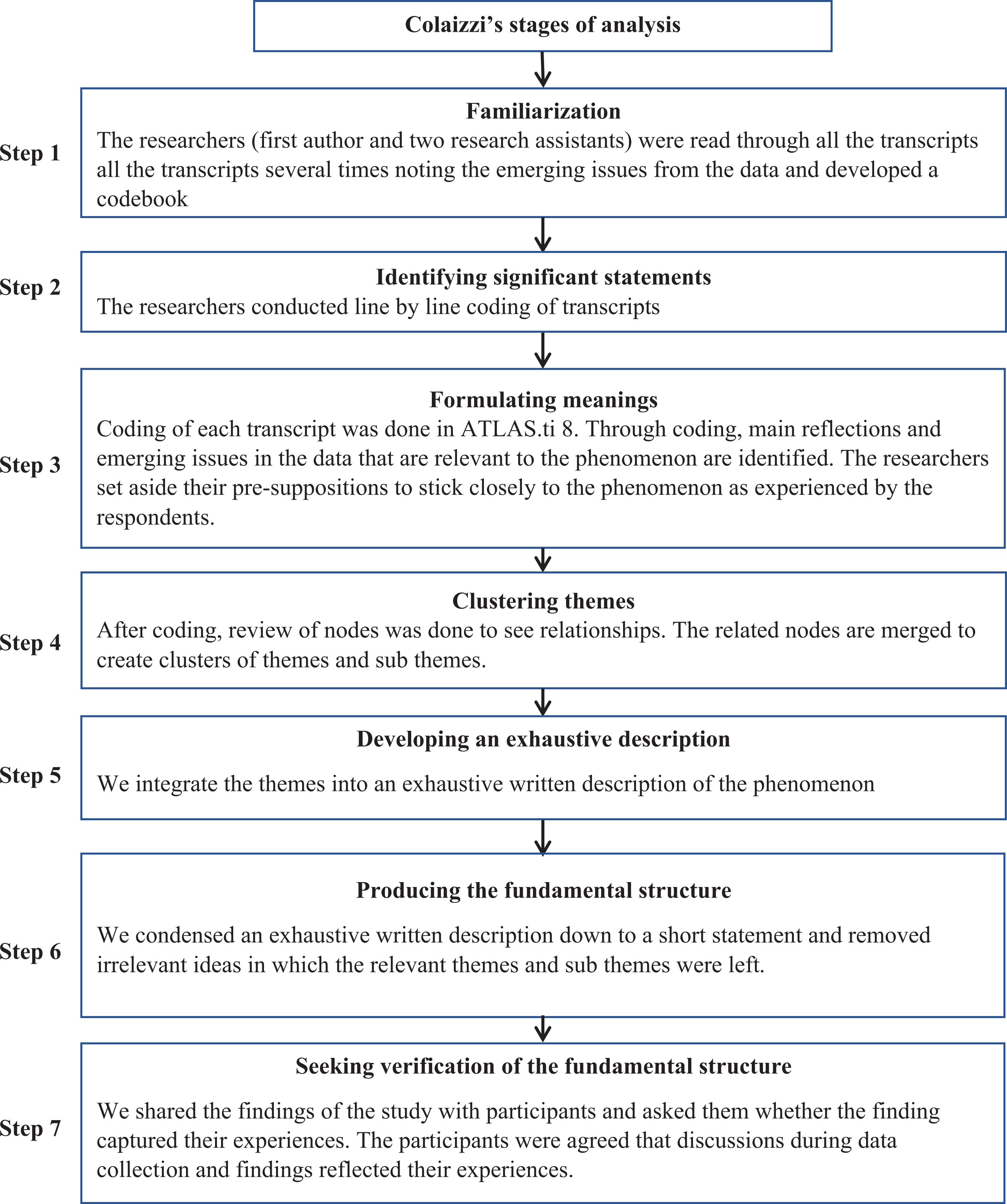
Colaizzi’s stages in descriptive phenomenological analysis and how it was applied in this study.
Ethics Approval and Consent to Participate
The ethical approval for the study was obtained from Hawassa University College of Medicine and Health Sciences Institutional Review Board (IRB/024/10) and regional committees for medical and health research ethics in Norway, 2018/69/REK vest. Verbal as well as written informed consent was obtained from the participants. The confidentiality of the information provided was maintained at all stages of data analysis.
Results
We conducted 6 focus group discussions with 47 mothers and 8 caregivers and 10 in-depth interviews with 4 HEWs and 6 WDA workers. The mothers’ or caregivers’ characteristics are described in Table 1. The mean age of mothers or caregivers was 30 years; most of them were mothers and the rest were grandmothers. Nearly 80% of them were housewives. The majority of mothers or caregivers were married. Nearly half of mothers or caregivers had not attended formal school.
Demographic Characteristics of Focus Group Discussions (FGD) Participants.a
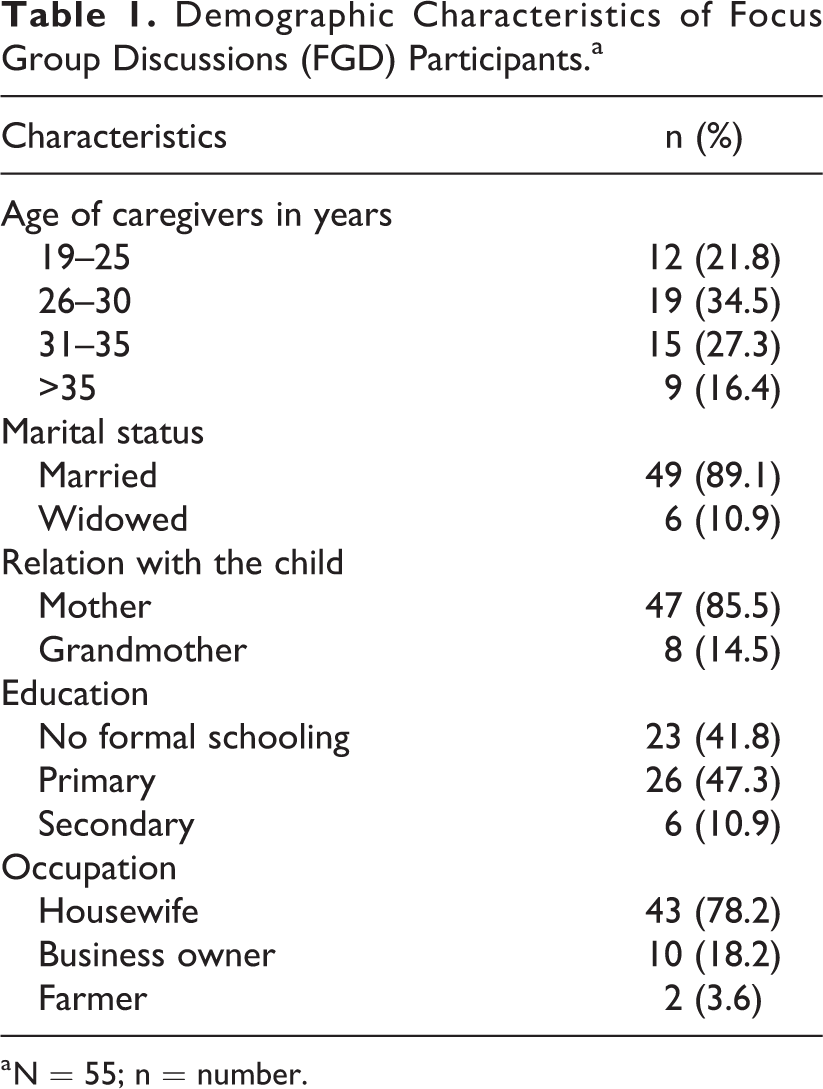
a N = 55; n = number.
The educational status of the HEWs ranged from a diploma and above, whereas the educational status of WDA workers ranged from secondary school completed and above (Table 2).
Demographic Characteristics of Health Service Providers.a
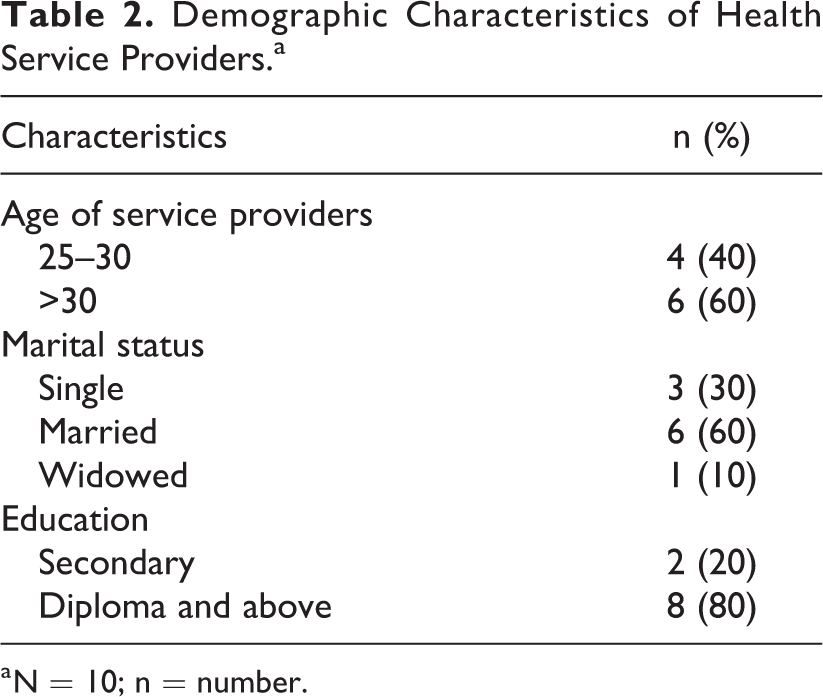
a N = 10; n = number.
Six main themes demonstrate perceptions from mothers and health service providers toward existing management practice of MAM and its barriers experienced: (1) Possible reasons for MAM; (2) Identification of child with MAM; (3) Management services of MAM; (4) Mothers or caregivers-level barriers; (5) Service provider-level barrier, and (6) Suggestions to improve the service (Table 3).
Summary of Themes and Subthemes From the Interview Data.
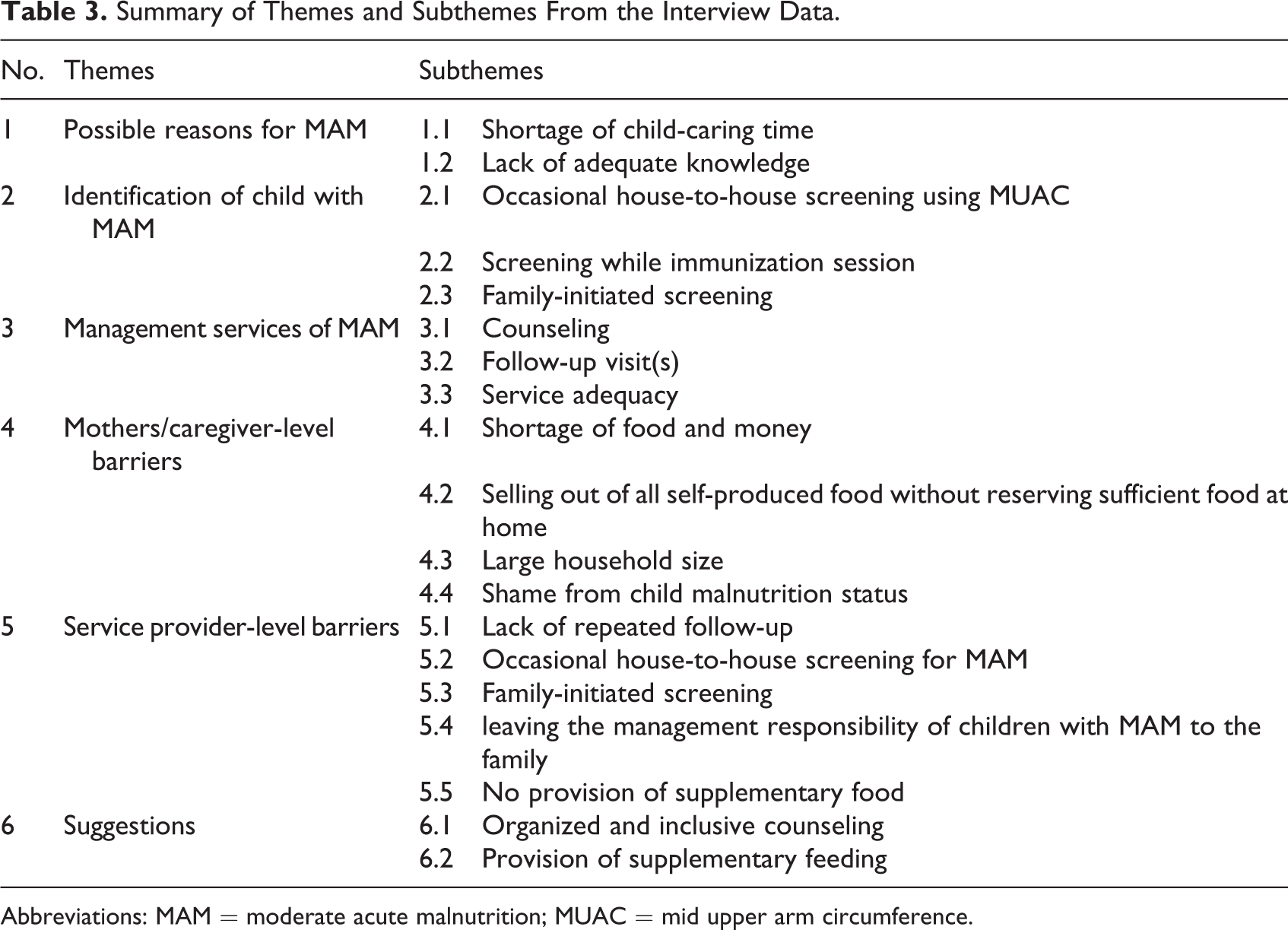
Abbreviations: MAM = moderate acute malnutrition; MUAC = mid upper arm circumference.
Theme 1 Possible Reasons for MAM
We present the possible reasons for MAM in order to give the basis for the management of MAM among children. The possible reasons for MAM may act as a background to understand the context for the barriers toward existing management practice of MAM. Shortage of child-caring time, lack of awareness, a large household size, and maternal malnutrition were mentioned as the possible reasons for MAM.
Shortage of child-caring time
Work overload prevents mothers or caregivers from caring for their children appropriately. In addition to this, small business traders do not have time to see their children. A mother of 31 years old said: “As to me, I have a workload at home. For example, caring for children, cooking for the family, drawing water, preparing firewood, going to the market, and sometimes farming, has made me not feed my child properly. Not only that, it has prevented me from attending the counseling offered by HEWs and WDA workers.” Likewise, a HEW of 28 years old said: “Some of the mothers who have small businesses are unable to practice the nutrition education received from service providers because they have no time to care for their affected child; they are not at home throughout the day.”
Lack of adequate knowledge
Respondents revealed that due to a lack of adequate knowledge toward appropriate childhood feeding practices, some mothers do not feed their baby regularly enough to ensure adequate intake. Instead, they give dry family foods when the child is hungry. As a result, children would often become ill and hence end up with MAM. A mother of 30 years old said: “Lack of knowledge may be the main cause for inappropriate feeding of the child. Some mothers do not feed their children regularly because they have no idea to prepare food for the child. Not only that, some mothers feed their child with easily unchewable food.”
Theme 2 Identification of Children With MAM
Mothers or caregivers who participated in the focus group discussions revealed that their children had been screened for MAM. They mentioned that the process of screening was done by measuring the upper arm of the child with plastic tape. The majority of mothers or caregivers reported that both HEWs and WDA workers were involved in the screening process. In this theme, the perceived barriers mentioned by mothers or caregivers were occasional house-to-house screening of children for MAM and family-initiated screening of children for MAM.
Occasional house-to-house screening using MUAC
One of the obstacle mentioned by the mothers or caregivers was that the screening is sometimes done with occasional household visiting by service providers. A mother of 25 years old said: “The most used way for screening of children is measuring upper arm by plastic tape. Based on the measurement result, they classified children as having low weight or not. The HEWs are doing this service occasionally.” Both mothers or caregivers and service providers mentioned that, sometimes, nongovernmental organizations had done the screening of children below 5 years for MAM but it was not continuous. Women’s Development Army workers of 40 years old said: “Sometimes, nongovernmental organizations has done the screening of children for MAM and support the affected children but the program was not continuous.”
The service providers informed that they have monthly screening programs for identification of children with MAM using the measurement of MUAC, by visiting house to house. They have also mentioned that they visit families who worry about their child’s nutritional status. A 32-year-old HEW said: “I go out and do house-to-house visits every month to screen children for acute malnutrition. Sometimes I visit households with children suspected of MAM based on the report of mothers.”
Screening during immunization session
According to the report of both mothers or caregivers and service providers, children with MAM were identified during the routine vaccination program and vaccination campaign as well. A grandmother of 39 years old said: “We have a commonplace in our area where we meet with the HEWs when there are a vaccination campaign and some other meeting. When the WDA workers inform us to bring our children to the site, we take them and they measure MUAC for all children through the vaccination program and classified children as affected or not.”
Family-initiated screening
The perceived barriers mentioned by the mothers or caregivers were that screening is done either by HEWs or by other medical persons working in health centers (when the family brought their children to visit health institutions for other medical reasons) or at the initiation of mothers or caregivers. Some mothers also mentioned that the screening process started when mothers or caregivers report the condition of their children to the service providers. A mother of 30 years old said: “When we presented with a sick child to the health center, medical persons working in the health center referred our child to HEWs after identifying the child as affected.” A grandmother of 40 years old also said: “As I know, I have brought my child to the health post more than once since she gets thin and has a loss of appetite…The HEW measured my child’s arm with plastic tape and told me as she has a moderate low weight.” Likewise, service providers mentioned that they screen children for MAM when the children are referred from other health facilities and when the mothers report the condition of the children. A 32-year-old HEW said: “I also screen the children, when mothers or caregivers bring their children for other medical reasons, and when they come and report to me, as their children are being thin…”
Theme 3 Management Practices of MAM
More than half of the focus group discussants did not know exactly what MAM was; they described the condition as low weight without body swelling and lost hair, but they knew they would stay in counseling if their child’s upper arm measurement was on the yellow mark on the plastic tape. In addition to this, they often mentioned the provision of Plumpy’nut (a nutritional supplement) for the severe form. Generally, mothers/caregivers and HEWs described similar existing management practices for MAM. These included nutrition counseling and follow-up visit(s). They also mentioned about the inadequacy of existing management service of MAM. In this theme, the perceived barrier mentioned by mothers or caregivers toward existing management practice of MAM were difficulties to implement the counseling advice because of household food shortage, and ignoring management of MAM and leaving the management responsibility to the family. The perceived barrier mentioned by service providers toward existing management practice of MAM was limited or no provision of therapeutic supplement.
Nutrition counseling
The mothers or caregivers said that the existing management service for MAM is primarily counseling. The counseling topics cover healthy complementary feeding practices, types of different food ingredients that the children need, as well as hygiene. These services are mostly given by the HEWs and sometimes by WDA workers. Some of the mothers or caregivers mentioned that they get these services when they bring their child for vaccination. Others informed that they are getting the service every month. A mother of 35 years old said: “As I know, I am getting an education from HEWs on hygiene and demonstration to feed our child with porridge made from different food ingredients like cabbage, potato, carrot, maize, and egg. Sometimes the HEWs visit my home to provide counseling and check my child.” Similarly, service providers (HEWs and WDA workers) mentioned they do home visits, providing monthly counseling on exclusive breastfeeding practices, complementary feeding practice, preparation of porridge from cereals and vegetables, hygiene, family planning, vaccination, and communicable disease control. The perceived barrier toward existing management practice of MAM mentioned by all health service providers was that there is limited or no provision of supplements for MAM. Health extension workers of 30 years old said: “I have advised caregivers by visiting households monthly with different topics like exclusive breastfeeding practices, complementary feeding practice, hygiene, family planning, vaccination, and communicable disease control. Other than the above services, we are not providing any supplements.”
Follow-up visit(s)
Mothers or caregivers mentioned that the HEWs, as well as WDA workers, were visiting their home and checking their child’s status. Almost all service providers agreed on having follow-up visits to check the progress of children with MAM, once the children are identified and registered as such. A 40-years-old HEW said: “I also do follow-up checks for registered MAM cases for their progress and to counsel mothers or caregivers. Similarly, I send WDA workers to do follow-up visits of registered children with MAM by measuring MUAC.”
Adequacy of the service given
According to the mothers or caregivers, they agreed that the management services for MAM are inadequate. The barrier toward management services of MAM perceived by some of mothers or caregivers was that it is difficult to implement the counseling advice because of the shortage of food in their house. They also raised that getting counseling only on feeding practices is not bringing improvement to their children with MAM. A 31-years-old mother said: “I can say that my child with moderate thinness is not improving with the current service. It is my delight if I can implement what I learned about how to feed, but I can’t.” Another barrier mentioned by the mothers or caregivers was that MAM is an ignored condition because the management of it is left to the family; however, the children always develop edema within a short period. A 30-years-old mother said: “The problem is that children with moderate thinness were ignored. The surprise here is caregivers have no option to care for their children other than giving family food and breast milk. The service providers are only providing counseling on feeding practice and advising us to follow-up with our kids at home.”
The perceived barrier mentioned by the health service providers was that nutrition counseling only is not helpful as the children are progressing to the severe form of acute malnutrition; they further pointed to the fact that there is limited or no provision of supplementary food for MAM. A 34-years-old HEW said: “I think the management services for MAM are less appropriate to people who cannot access food according to our advice. Some can be improved through counseling but not satisfied. Mostly, they progress into severe form. So I think it’s better to think about something else.” Likewise, a 31-years-old WDA indicated that the children with MAM are not benefited from the management compared with SAM children. She mentioned: “….We are providing a therapeutic supplement to SAM children but we are not giving a therapeutic supplement to children with MAM, it is because of the management guideline of MAM, so that, they are not getting improved as needed.”
Theme 4 Mothers or Caregiver-Level Barriers
According to mothers or caregivers, the barriers that prevent them from implementing the nutrition counseling were a shortage of food and money, selling-out of self-produced food without reserving sufficient food at home, large household size, and shame from having a child with malnutrition. These were the main obstacles that prevent mothers or caregivers from diversifying the children’s diet.
Shortage of food and money
Most respondents felt that the shortage of food and money at home prevented them to implement what they learned about feeding their children with MAM. A 30-years-old mother said: “To be honest, I have a shortage of food and money in my house. As a result, I was unable to provide my child with better food. My child is a 3-year-old boy; he only eats family food, not baby food. Even if I feed my baby well today, I can’t do it tomorrow. I am sure that there are many mothers like me because we know each other. Health professionals are teaching us, without consideration of our circumstances; that is why the counseling has little importance to our children.” Another mother of 32 years old said: “The problem with us is that we do not feed our children adequately. It is directly linked to our limited economy. We have a noticeable shortage to implement what we know about child feeding.” A 43-years-old grandmother indicated that the counseling service given to the mothers or caregivers of children with MAM is not useful for the poor. She mentioned, “People are offended with the management of MAM like getting only education. I am not interested in education and even not attend the session because it has no help for poor like me.”
Selling out of the self-produced crops without reserving sufficient food at home
Respondents also felt that selling out of all self-produced crops was another obstacle for cash restricted families from having adequate food at home. Even if the farms look green, the families could not be benefited from it. A 35-years-old mother said: “We cannot say that there is no problem with us, because the sale of all crops cultivated at our farm has made our children hungry.” The respondents also mentioned that there is a disagreement between men and women toward the use of cultivated crops. A 40-years-old WDA worker said: “Our area is looking green right? But most families have nothing to feed their children. In our area, there is a disagreement between husband and wife regarding farm crop use. Men sell self-produced crops without reserving sufficient food at home to get money in which the household remained within sufficient food to eat. That is why families are not getting enough food.”
Large household size
In-depth interviews (IDIs) revealed that the large household size is an obstacle negatively affecting children with MAM. A high number of family members may constrain the mother’s capability to monitor her children’s feeding practices because they assume the child has been fed somewhere else. A 31-years-old WDA said: “Despite food shortages and financial difficulties for mothers or caregivers, they have still other gaps. For example, they are giving birth to more children with limited spacing because they are not using contraceptives properly.” Likewise, a mother of 33 years old mentioned that the restricted resources might be stretched to supply unexpected visitors in addition to extended family. She mentioned, “….sometimes you may cook food that is just enough for your family and then the neighbors turn up and you are indebted to feed them too. At that time, your children do not get enough food.”
Shame from child malnutrition status
Our respondents mentioned that shame from the malnutrition status of children is one of the barriers that prevent mothers or caregivers from seeking service. Some of the respondents reported that mothers or caregivers whose children become wasted felt that the community may undermine them. A 28-years-old mother said: “when my child wasted I don’t want to report to HEWs about my child’s case as it is because of food shortage rather I believe and disclose it is because of illness. Otherwise, my neighbors undermine or gossip me as I can’t feed my child.”
Theme 5 Service Provider-Level Barriers
In addition to the barriers mentioned under the themes of identification of children with MAM and management services of MAM (the occasional house-to-house screening of children for MAM, family-initiated screening, ignoring the management of MAM, and leaving the management of MAM responsibility to the family), lack of repeated follow-up by the service providers was mentioned as a service provider-level barrier.
Lack of repeated follow-up
Health service providers stated that they lack repeated follow-up of their children with MAM. Most of the time, they just give nutrition counseling to caregivers of children with MAM at the time of admission. A 40-years-old HEW said: “We provide information to the mothers of children with MAM regarding how to feed their affected child consistently and clearly during admission time but I feel that we are not doing it repeatedly. We need to do a repeated follow-up.”
Theme 6 Perceived Suggestions to Improve the Service
Both mothers or caregivers and service providers considered management of MAM with counseling of appropriate feeding practice, in addition to a therapeutic supplement, to be a positive option through which the children with MAM will improve. However, they also mentioned some concerns and made related suggestions.
Organized and inclusive counseling
Some said that the counseling service given by the service providers is not focused, routine, and inclusive. They have suggested that it needed to be focused, routine, and include all mothers and fathers of children aged below 5 years. A 35-years-old mother said: “Counseling on feeding practice is good but there was no exact time which was known by us and service providers. [It was] not focused and it was not involving all mothers with children under 5 years old. So, it is better to improve in this regard.”
One of the mothers mentioned that where the mothers were not in control of family incomes; thus, they often did not have the authority to implement knowledge of nutritional needs into practices. Even though the mothers provided with nutrition counseling, the husbands were often made the judgment about what food should be bought. Mothers also mentioned since their husbands are not directly involved in nutrition counseling sessions and child feeding, they may not be ready to participate in nutritious food prepared for the children. A 30-years-old mother said: “I am always responsive to my children regarding the preparation of food but I have no economic power to buy nutritious food. I tried to provide nutrition information to my husband that I get from the service providers but he was not being convinced. As to me, it is better to include the husbands in the nutrition counseling session.”
Supplementary feeding
Our respondents mentioned that supplementary feeding is highly needed to manage children with MAM in addition to nutrition counseling. They reported that household food shortages and economical limitations prevented them from implementing nutrition counseling. A 34-years-old-mother said: “feeding children with MAM with supplementary food is the better management option compared to the provision of nutrition counseling only. With nutrition counseling only, most of the children with MAM deteriorate to the severe form.
Discussion
This study attempted to assess barriers to management of MAM among children aged 6 to 59 months in Damot Pulassa, Wolaita, South Ethiopia: a phenomenological study of mothers and health service providers. The findings that emerged from this study were possible reasons for MAM, identification of a child with MAM, types of management services of MAM, mothers or caregivers-level barriers, service provider-level barrier, and suggestions to improve the service.
In this study, shortage of child-caring time and lacks of adequate knowledge were mentioned as the possible reasons for MAM. The time constraints of mothers or caregivers in caring for their children have been perceived as a possible reason of MAM. This is in line with the studies done by Hyder et al and Berhane et al showing how an increased workload for women negatively affects their child’s health status and that, if time is made available, improved child health outcomes can be attained. 23,24 Another study done in Uganda revealed that the heavy workload of the primary caregiver of the child was a major barrier to improving child-feeding practices. 25 However, another study argued that a reduction in the working time of caregivers did not improve their child’s health status or affected it negatively. 12 Similarly, a retrospective study done in rural Ethiopia proposed that labor-saving technology was associated with an increased malnutrition rate since it related to increased fertility in women. 26
Our findings have shown that a lack of adequate knowledge toward appropriate childhood feeding practices due to a lack of formal education of mothers mentioned as another possible reason for MAM. This finding is in line with a study done in Uganda showing a lack of adequate knowledge regarding appropriate childhood feeding practices emerged as a barrier to caring for children. 27 Caregiver’s lack of adequate knowledge has also been found to be related to spending inadequate time to nourish the child and lacking feeding of sufficient amounts of complementary foods to meet the child’s energy and micronutrient requirements. 28 This shows that lack of knowledge may be impacting critical parts of child-feeding and thus, affect child nutritional status negatively.
The findings from this study have shown that occasional house-to-house screening for MAM, screening for MAM through immunization program, and family-initiated screening for MAM were the ways how the health service providers are identifying children with MAM. Occasional house-to-house screening for MAM might not help to identify all children with MAM and reach the marginalized groups. Screening for MAM during the immunization program might be helpful to identify children below 2 years because these children are mostly included under the routine immunization program. Family-initiated screening is always based on either the symptom-based report of mothers or caregivers or referral from other health units. This shows that mothers or caregivers have a role in the screening of children for MAM though it is the role of health service providers. Further, if the mother didn’t report about the status of her child, the child might not be screened for MAM. Thus, occasional house-to-house screening for MAM and family-initiated screening are the service provider-level barriers.
In this study, the screening process was done using only MUAC as a screening tool. There is an increasing understanding that MUAC can be used safely and successfully as the single anthropometric measure for admission, follow-up, and discharge from malnutrition treatment. 29,30 Mid-upper arm circumference is an easy, quick, and powerful screening tool for acute malnutrition at the community level. 31 This is due to the current national guidelines on screening for acute malnutrition. The advantages of MUAC are that it is a better measure to identify children most in need of treatment and it is less prone to mistakes compared to other indices.
The current study has shown that children aged below 5 years who are admitted to the management program of MAM getting nutrition counseling and follow-up visit(s) as management of MAM. Nutrition counseling is perceived as the primary management service for MAM. As stated by Prinzo and Briend, nutrition advice is provided to families on the assumption that they have access to all foodstuffs required for feeding their children but lack the knowledge of how to implement this knowledge. 11
Mothers or caregivers of children with MAM got monthly counseling on exclusive breastfeeding practices, complementary feeding practices, and preparation of porridge from cereals and vegetables, hygiene, family planning, vaccination, and communicable disease controls. This is in agreement with the results of the meta-analysis done by Lenters et al. 8 Only providing counseling as management to MAM may be because the study area is classified as food secure, even though the respondents reported that they had a shortage of food at home. In Ethiopia, the current strategy for the management of MAM is to restrict supplementary feeding programs to selected districts defined as chronically food insecure. However, in areas not considered as chronically food insecure, there are no food supplementation programs, and instead, there is nutrition counseling. 4,12 However, there might be food-insecure households in areas seen as food-secure. 12
Our study showed that, once children below 5 years of age are identified as having MAM, the HEWs or WDA workers do monthly visits, in addition to counseling, to check the children’s progress. To achieve maximum results in the management of MAM, home visiting is one of the recommended techniques. 7 This might help service providers to easily identify whether children with MAM are progressing positively or negatively, and to decide on possible referrals.
In the current study, the respondents claimed that the management service that had been given to their moderately malnourished children is not adequate to treat the condition, since their children have mostly progressed to the severe form of acute malnutrition. Further, as reported by James et al, in an area where supplementary feeding programs are not accessible for the management of MAM, there is an unsatisfactorily high occurrence of SAM and a low recovery rate. 12 Similarly, another study showed that treatment of MAM with food supplements is more effective than counseling only. 10,32 This could probably be due to counseling on feeding practices and the actual household food availability is not balanced.
In this study, ignoring the management of children with MAM and leaving the responsibility of managing children with MAM to the family are the service provider-level barriers mentioned by the mothers or caregivers. This shows that MAM is not getting recognition though it progresses to the severe form of acute malnutrition which is life-threatening condition.
Our finding showed that household food shortage is perceived as a maternal-level obstacle. This may be because the household’s food reserve status is low and the market price of the foods increased. Even if the mothers or caregivers know good feeding practices, they cannot effectively implement nutritional advice because of the shortage of food at home. This finding leads to the idea that, if there was the availability of food at home, nutritional counseling would have improved outcomes. Further, the provision of improved, well-organized, and inclusive counseling may help positively.
Another obstacle perceived by our respondents is their financial limitation. Children who avoided or reduced meals because of lacking money were more likely to be wasted than those who did not. 33 Further, as reported by Abitew, low socioeconomic status or monthly income decreases the household purchasing power and hence reduces access to food. 34 Likewise, another study done in Burkina Faso reported that the higher recovery rate from MAM was where the fair levels of food security, which enabled the effective implementation of nutrition advice at home. 32 The explanation here is that when there is limited access to have nutrient-dense food, the mothers or caregivers cannot feed their child with adequate and diversified food, and thus, the mothers or caregivers can’t implement the nutrition counseling they received. Besides, there might be an imbalance between available farmland and household population size.
In the present study selling out of self-produced food without reserving at home was mentioned as the maternal or caregiver-level barrier that influences the implementation of management practice of MAM. To get money in hand, households are doing inappropriate usage of their farm crops.
Our findings have shown that the large household size was one of the barriers that prevent the implementation of nutrition advice given to mothers or caregivers of children with MAM. The food available to larger families per head was frequently lower than that available to smaller families and this difference was reflected in the growth rate. 33 The explanation here might be the imbalance between available food at home and household population size affect the children negatively.
In this study, the findings revealed that women whose children had MAM were ashamed when seeking care and perceived the condition as a sign of insufficient parental care, such as poor food provisioning. This is in line with a study done in Kenya and Malawi showing that caregivers of children with wasting practice stigmatization, as shown in the emotional state of shame, humiliation, and embarrassment stated in the process of accessing treatment. 35,36 The explanation here might be child wasting is inseparable from hunger and poverty in the rural community.
Our study revealed that lack of repeated follow-up of children with MAM is considered as a service provider-level barrier. The explanation here is that follow-up visit(s) is one of the existing management practices of MAM in which the HEWs or WDA workers can provide nutrition counseling and evaluate the progression of a child with MAM. Thus, a lack of repeated follow-up visits will influence the recovery of children from MAM negatively.
The current study has shown that organized and inclusive counseling and provision of supplementary food were identified as the suggestions to improve the existing management practice of MAM. The respondents revealed that the presence of well-organized and focused counseling for beneficiaries is necessary for the management of MAM. This is in agreement with a study done in Burkina Faso showing that nutrition counseling might demonstrate to be a valuable substitute delivered that presence to a counseling session by caregivers is confirmed. 32 Another study done by Lelijveld et al reported that the standardization of quality and content of nutrition advice interventions needs concern. 37
In the present study, the findings have shown that including mothers and fathers of children aged below 5 years in nutrition counseling sessions would have a positive influence on the management of MAM. Men were often decided on different household activities including what food should be bought from the market. This might be due to men are economically powerful and decisive compared to women in developing countries. According to different studies, husbands are considered as the primary spokespersons for their family, and their say and counsel are also very respected by mothers and children in utilizing health care services. 32,38,39 In sub-Saharan Africa, the restricted participation of men in the day-to-day care of the child, child-feeding, and nutrition activities is common even though the involvements of men have a potential benefit to reduce the burden of work responsibilities faced by caregivers. 40
Our study identified that management of MAM with counseling of appropriate feeding practice in addition to supplementary feeding may have a positive outcome in treating children with MAM. As a study done by Roy et al shows, children with MAM who were receiving intensive nutrition education only had reduced improvement in nutritional status compared to the children with MAM who received both food supplementation and intensive nutrition education. 41 This shows that children with MAM may need to have supplementary feeding in addition to counseling for them to recover from the condition or to prevent progression to SAM.
The study had some limitations. The main one is that there might be social desirability bias because service providers are included as respondents in in-depth interviews. They might answer the interview questions in such a way that might support the existing management practices for MAM. This bias was alleviated by including mothers or caregivers as respondents in the focus group discussions. We tried to keep complete bracketing but challenged with the opinion of putting aside predetermined knowledge to induce a pure description of the participants experiences. In practice, pure bracketing may be difficult. However, we maintained the bracketing approach by separating our personal experiences and knowledge from reflecting on the lived experiences of the respondents as much as possible. This indicates that the interpretation of the research results was not affected by our beliefs or experiences. This bracketing confirms the validity of results.
In our study, we choose to include mothers or caregivers for the focus group discussions and the most grassroots level health service providers, namely the HEW and WDAs for an in-depth interview. Health extension workers and WDAs are the main health service providers in the rural areas assigned to manage acute malnutrition. We could have chosen to include staff in the district health office. This could have added perspectives from Wolaita zone health office staff and enabled a fuller insight into the matter, as well as comparing whether the perception of barriers expressed at the various levels match/differ across the structure within that local context. This is something that can be recommended for a further study of the responsibility levels within the health service system. However, this was seen to go beyond the scope of the present study.
Despite the limitations, the study gives qualitative evidence on the perceptions of mothers/caregivers and service providers on the barriers to existing management practice of MAM among children aged 6 to 59 months. An intense and in-depth understanding of barriers to existing management practice of MAM were identified and showed in the results. It, therefore, provides support for programs that aim to promote or improve management services for MAM in the area.
Conclusion
Moderate acute malnutrition among children aged 6 to 59 months has been managed by counseling or nutrition advice only. The identification of children with MAM was based on the measurement of MUAC. Maternal-level barriers and service provider-level barriers affect the management of MAM negatively. Household food shortages and financial limitations, selling out of self-produced food without reserving sufficient food at home, large household size, and shame from child malnutrition status are maternal-level barriers. Occasional house-to-house screening for MAM, family-initiated screening for MAM, leaving the management responsibility of children with MAM to the family, limited or no provision of therapeutic supplement to children with MAM, and lack of repeated follow-up are service provider-level barriers. These obstacles make the management services for MAM inadequate and lead to progression to SAM. In such situations, the government should consider interventions addressing the food shortage and financial constraints of households, in addition to counseling to improve the management services for MAM.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721221088817 - Barriers to Management of Moderate Acute Malnutrition Among Children Aged 6 to 59 Months in Damot Pulassa, Wolaita, South Ethiopia: A Phenomenological Study of Mothers and Health Service Providers
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721221088817 for Barriers to Management of Moderate Acute Malnutrition Among Children Aged 6 to 59 Months in Damot Pulassa, Wolaita, South Ethiopia: A Phenomenological Study of Mothers and Health Service Providers by Debritu Nane, Anne Hatløy and Bernt Lindtjørn in Food and Nutrition Bulletin
Supplemental Material
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721221088817 - Barriers to Management of Moderate Acute Malnutrition Among Children Aged 6 to 59 Months in Damot Pulassa, Wolaita, South Ethiopia: A Phenomenological Study of Mothers and Health Service Providers
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721221088817 for Barriers to Management of Moderate Acute Malnutrition Among Children Aged 6 to 59 Months in Damot Pulassa, Wolaita, South Ethiopia: A Phenomenological Study of Mothers and Health Service Providers by Debritu Nane, Anne Hatløy and Bernt Lindtjørn in Food and Nutrition Bulletin
Footnotes
Authors’ Note
DN designed the study, analyzed the interview and discussion data, interpreted the result, and drafted the manuscript. AH and BL were responsible for the design of study, assisted to analyze the data, and interpret the results as well as critically reviewed the manuscript. All authors were responsible for drafting and revising the document and approved the final version. The datasets used during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Authors thank the participants who consented to give their time and share their opinions. Authors would like to thank all data collectors and supervisors for their contribution to conducting focus group discussions and for their work on the transcription.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding organization of this research is NORAD (Norwegian Agency for Development Cooperation); through the NORHED program (Norwegian Program for Capacity Development in Higher Education and Research for Development). The funding number is NORHED ETH 13/0025 SENUPH Project.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.