
Abstract
Background:
Breastfeeding and Kangaroo Mother Care (KMC) are interventions to reduce neonatal mortality and undernutrition. We investigated the knowledge of allopathic and Ayurvedic, Yoga-naturopathy, Siddha, and Homeopathic (AYUSH) general practitioners in rural western India and identified attributes associated with awareness and knowledge on these topics.
Methods:
This cross-sectional study of general practitioners in the Anand district of Gujarat, India, used an anonymous self-reported survey. Multivariable regression models were used to identify practitioner attributes associated with awareness and knowledge.
Results:
Among the 158 respondents, a quarter (26.0%) were trained in allopathic medicine and 63.0% had practiced for 5 years or more. The average score of breastfeeding knowledge was 8.0 of 13. Most (79.1%) did not have any awareness of KMC. After adjusting for potential confounders, knowledge of breastfeeding practices among AYUSH practitioners was 4-fold greater than that of allopathic practitioners (incidence rate ratio: 3.9; 95% CI: 3.2-4.6). By contrast, AYUSH practitioners had 80% decreased odds of awareness about KMC compared with allopathic practitioners (odds ratio: 0.2; 95% CI: 0.1-0.3).
Discussion:
This study demonstrates distinct knowledge gaps among allopathic and AYUSH general practitioners regarding breastfeeding and KMC. There is a need for tailored continuing medical education among general practitioners to enhance their clinical knowledge of newborn care practices to achieve improvements in neonatal health.
Background
Nearly one-third of the world’s neonatal deaths and undernourished children are in India. 1 Breastfeeding and Kangaroo Mother Care (KMC) are essential interventions to address these public health crises. 2,3 Improvement in these practices requires an informed health care workforce. In rural India, most primary health care is provided by general practitioners who practice allopathic medicine; however, many have received formal training in complementary and alternative medicine including Ayurvedic, Yoga-naturopathy, Siddha, and Homeopathic medicine (AYUSH). 2 We investigated the knowledge of breastfeeding and KMC among general practitioners in rural western India and identified practitioner attributes associated with awareness and knowledge about breastfeeding and KMC.
Methods
This cross-sectional study was conducted in the Anand district of Gujarat, India, between February and May 2017. A total of 190 practitioners were identified using a central directory of general practitioners. They were approached in their outpatient clinic and asked to complete an anonymous self-reported survey. The survey assessed knowledge of appropriate practices and benefits of breastfeeding and KMC based on information published by the Indian Ministry of Health and Family Welfare. 4 Demographic information included practitioners’ medical degree, years of experience, monthly number of patients aged younger than 2 years, and practice type. A multivariable negative binomial regression model was used to assess practitioner knowledge of breastfeeding and account for overdispersion in the underlying data. Because of the low awareness of KMC, we performed multivariable adjusted logistic regression analysis to assess practitioner attributes associated with awareness of KMC.
Results
A total of 158 practitioners completed the survey. Approximately one quarter (26.0%) were trained in allopathic medicine and 63.0% had practiced for 5 years or more. Nearly half (48.7%) reported seeing at least 5 pediatric patients younger than 2 years per month. The average score of breastfeeding knowledge was 8.0 of 13. Prevalence of misinformation about optimal time of initiation, recommended period, and contraindications for breastfeeding were 37.3%, 43.7%, and 78.5%, respectively. Most (79.1%) practitioners did not have any awareness of KMC. Of the 33 practitioners who knew about KMC, the average knowledge score was 6.3 of 11. Table 1 shows the association of practitioners’ attributes with knowledge of breastfeeding practices and awareness of KMC. After adjusting for several confounders, knowledge of breastfeeding practices among AYUSH practitioners was 4-fold greater than that of allopathic practitioners (incidence rate ratio: 3.9; 95% CI: 3.2-4.6). Conversely, AYUSH practitioners had 80% decreased odds of awareness about KMC compared with allopathic practitioners (odds ratio: 0.2; 95% CI: 0.1-0.3).
Factors Associated With Knowledge About Breastfeeding and Awareness of Kangaroo Mother Care Among General Practitioners in the Anand District of Gujarat, India.
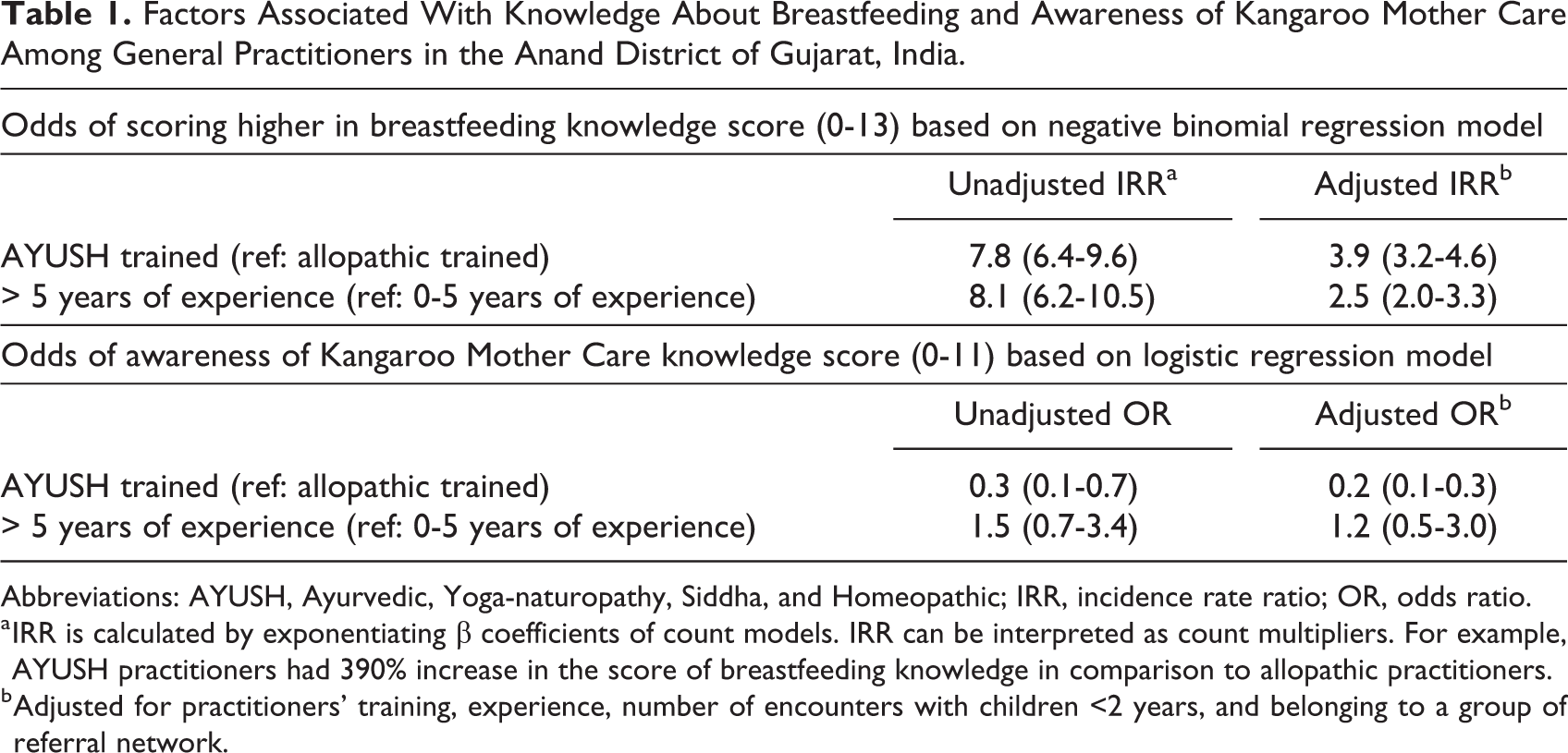
Abbreviations: AYUSH, Ayurvedic, Yoga-naturopathy, Siddha, and Homeopathic; IRR, incidence rate ratio; OR, odds ratio.
a IRR is calculated by exponentiating β coefficients of count models. IRR can be interpreted as count multipliers. For example, AYUSH practitioners had 390% increase in the score of breastfeeding knowledge in comparison to allopathic practitioners.
b Adjusted for practitioners’ training, experience, number of encounters with children <2 years, and belonging to a group of referral network.
Discussion
This study demonstrates overall low knowledge among general practitioners regarding breastfeeding and KMC, 2 essential interventions for newborn health. Breastfeeding knowledge was limited, and most practitioners were not aware of KMC at all. Furthermore, AYUSH practitioners had greater knowledge about breastfeeding practices but less awareness of KMC than their allopathic practitioner counterparts. These distinct knowledge gaps underscore the need for tailored continuing medical education among general practitioners.
The Ministry of Health and Family Welfare of India has emphasized the importance of breastfeeding and KMC to address neonatal mortality and child undernutrition. 2,3 National programs have focused on strengthening infrastructure and surveillance in rural regions by cultivating an expansive workforce of community health workers. 2 These programs are maintained through regular training in prenatal and postpartum counseling. Despite these efforts, the prevalence of neonatal mortality and child undernutrition remains high. 2
One possible explanation for suboptimal outcomes may be inadequate knowledge about newborn care among general practitioners, as demonstrated in our findings, resulting in discordant counseling of families. General practitioners are highly respected and valued members of their communities in India. Their trust and goodwill with the community creates an opportunity for impactful dissemination of newborn care practices. However, this avenue is only as valuable as the knowledge of the general practitioner. Our finding that AYUSH practitioners were relatively more knowledgeable than allopathic practitioners about breastfeeding practices may be due to the supplemental training AYUSH practitioners receive from the government to integrate them into the primary health care workforce of rural regions. Allopathic practitioners lack the opportunities for continuing medical education that are often disseminated by professional medical bodies to their specialist counterparts. Including all general practitioners in the government’s overarching strategy to improve newborn care practices may address these knowledge gaps.
In this study, we identified an overall lack of awareness about KMC with only 20.9% of practitioners having heard of KMC. The concept of KMC is relatively new and active efforts are needed by the Indian government to enhance its awareness and acceptance among the medical community. Previous evidence from this region shows that when practitioners are aware of the benefits of KMC, its practice increases. 5 This encouraging finding may be particularly noteworthy because of recent evidence demonstrating the benefits of community-initiated KMC on neonatal survival. 6
Our study findings should be interpreted in the context of its limitations, most notably the use of self-reported data provided by a nonrandom sample from a single region in India. However, this survey is among the first to assess knowledge of these topics among general practitioners in India and represents the best currently available data. We elected to collect data anonymously to minimize information bias and it is likely that practitioners who felt confident in their knowledge were more likely to respond. Therefore, the results presented here likely represent the upper bound of awareness and knowledge among general practitioners. It is worth noting that these practitioners may not be directly involved in providing breastfeeding and KMC consultation to families; however, we accounted for practitioners’ history of caring for infants.
In conclusion, general practitioners’ knowledge is a key contributor to the health behaviors of their community. Many low- and middle-income countries, including India, have identified breastfeeding and KMC as critical interventions to improve neonatal health and have developed initiatives to increase these practices. The focus on training community health workers is an important component but should not be at the exclusion of general practitioners. Educational opportunities tailored to general practitioners will enhance their clinical knowledge of newborn care practices and generate harmony among the counseling provided to families from community health workers and practitioners, alike.
Footnotes
Authors’ Note
Nisha Fahey, Nitesh Sadhwani, Smit Shethwala, Apurv Soni, Somashekhar Nimbalkar contributed to conception and design. Nisha Fahey, Jeroan Allison, and Apurv Soni contributed to analysis and interpretation. Nisha Fahey and Apurv Soni drafted manuscript. Nitesh Sadhwani and Smit Shethwala contributed to acquisition. Jeroan Allison contributed to conception. Somashekhar Nimbalkar contributed to acquisition, analysis, and interpretation. All authors critically revised manuscript, gave final approval, agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Minority Health and Health Disparities [P60-MD006912-05 to J.A.]; the National Institute of General Medical Science [T32GM107000 to A.S.]; National Center for Advancing Translational Sciences [TL1-TR001454 to A.S.]; and the Eunice Kennedy Shriver National Institute of Child Health and Human Development [1F30HD091975-03 to A.S.].