
Abstract
Background:
Beriberi is the clinical manifestation of thiamine deficiency. It is multicausal and typically associated with poverty and food insecurity among vulnerable populations, such as indigenous people.
Objective:
The objective of this study was to carry out a spatial analysis of reported cases of beriberi among indigenous people in Brazil.
Methods:
Cross-sectional study using time series data on suspected cases of beriberi reported to the Ministry of Health via the FormSUS between July 2013 and September 2018. Indigenous villages were georeferenced, and Kernel density estimation was used to identify patterns of the spatial distribution of beriberi cases.
Results:
A total of 414 cases of beriberi were reported in the country of which 210 (50.7%) were indigenous people. All the cases in indigenous people occurred in states located in the Legal Amazon (Maranhão, Roraima, and Tocantins). Kernel density estimation showed high-density areas in Tocantins and Roraima.
Conclusions:
This is the first nationwide study of reported cases of beriberi. The findings can be used to guide actions that contribute to the monitoring and prevention of beriberi among indigenous people.
Background
Beriberi is the clinical manifestation of thiamine (vitamin B1) deficiency which in turn has multiple underlying causes or risk factors. Although easily treatable, if left untreated it can lead to death. 1 The clinical manifestations of thiamine deficiency encompass the nervous, cardiovascular, and gastrointestinal systems. Early signs include anorexia, general malaise, and weakness, and the disease is frequently associated with paresthesia, slight edema, and heart palpitations. The condition can worsen and develop into wet beriberi, characterized by cardiovascular symptoms and edema, or dry beriberi with symptoms of peripheral neuropathy. Wet beriberi may develop abruptly into a more severe form known as Shoshin beriberi, resulting in sudden cardiac arrest associated with lactic acidosis and shock. Another severe form of beriberi is Wernicke encephalopathy, associated with irreversible memory loss and a confabulatory psychosis known as Wernicke-Korsakoff syndrome, typically seen in alcoholic patients. 2 Beriberi is associated with high morbidity and mortality. Misdiagnosis is an important issue that needs to be taken into account in the control and monitoring of the most affected groups. 3
Reports of beriberi in the 20th century were typically outbreaks and cases among susceptible groups characterized by a monotonous diet and heavy physical exertion. 4 After a number of decades without reports of beriberi outbreaks in Brazil, an outbreak was recorded in 2006 in the State of Maranhão involving 434 cases and leading to 40 deaths, probably associated with alcohol abuse and physically demanding labor. 1 In 2008, various cases were reported in the State of Roraima among Indians from various ethnic groups and communities living in poverty and experiencing food insecurity and where excessive intake of alcohol, including a traditional drink called caxiri, was common. 5
Today, most outbreaks in Brazil are associated with poverty, hunger, monotonous diets consisting of excessive consumption of polished rice and other simple carbohydrates, alcohol abuse, and heavy physical activity. 2 The association between the consumption of polished rice and the development of beriberi was discovered by the Dutch physician and pathologist Christiaan Eijkman in 1890 after showing that a paralytic condition resembling beriberi was produced in chickens by feeding them a diet consisting solely of polished rice. 6 However, thiamine deficiency has also been shown to occur in undernourished individuals, people with chronic diseases, patients with anorexia, people who have undergone bariatric surgery (due to changes in nutrient absorption), 7 women with hyperemesis gravidarum, 8 and people with genetic defects related to thiamine metabolism and transport, as described by Ortigoza-Escobar et al. 9 Patients with malnutrition or exposed to nutritional risk are potential candidates for thiamine deficiency, regardless of the causes of malnutrition. 3
Considering that 50.7% of the reported cases of beriberi in Brazil are Indians, this study consisted of a spatial analysis of reported cases of the disease among indigenous peoples.
Method
A cross-sectional study was conducted using time series data on suspected cases of beriberi reported to the Ministry of Health via the FormSUS between July 2013 and September 2018.
The suspected cases were reported by health professionals in accordance with the Ministry of Health definitions. Suspected cases include all individuals in a situation of risk and showing signs and symptoms of beriberi. Situations of risk include heavy physical activity (eg, manual labor), excessive alcohol use, monotonous diet, hyperemesis gravidarum, and diarrhea. Signs and symptoms of beriberi include paresthesia and/or leg pain, partial loss of sensation and reflexes, decreased muscle strength (difficulty walking), sinus tachycardia (palpitations), divergent blood pressure, water hammer pulse, jugular venous distention, systolic heart murmurs, gallop rhythm, dyspnea, leg swelling, sudden cardiac arrest associated with lactic acidosis and shock, ophthalmoparesis, nystagmus, cerebellar ataxia, and memory deficit. 2
Cases of infantile beriberi (infants aged up to 12 months) are reported in accordance with the following Ministry of Health definitions: acute infantile cardiac beriberi (infants aged between 1 and 3 months)—the first symptoms are colic, restlessness, anorexia, and vomiting, progressing to generalized edema, cyanosis, and dyspnea, including signs of heart failure; infantile aphonic beriberi (infants aged 4 to 6 months)—vocal cord paralysis due to neuritis. Without treatment, after a few days, these cases develop into restlessness, edema, and dyspnea, lead to death, and infantile encephalitic or pseudomeningitic beriberi (infants aged 7-9 months). 2
The data were extracted from the FormSUS on November 01, 2018, and entered into an Excel worksheet.
The study variables were month and year of occurrence, municipality and state of residence, race/skin color (self-declared), 10 and, in the case of indigenous people, village, and ethnic group. Statistical analysis was performed using Stata® 14 (Stata Corporation).
The villages were georeferenced for spatial analysis purposes. The geographic coordinates (latitude and longitude) of the villages were obtained from the national indigenous health information system and validated using the ArcGIS 10.4.1 Geocoding tool. Occurrences were then converted into a geographical point database using ArcGIS’s GIS tool. Cases of beriberi in indigenous people were grouped by village and municipality on a map of Brazil obtained from the website of the Brazilian Institute of Geography and Statistics (IBGE, acronym in Portuguese) based on the 2010 municipal grid. The spatial distribution of beriberi cases was analyzed using the Gaussian Kernel density estimate and 1000-meter neighborhood radius, calculated automatically by the software.
The study was conducted in accordance with the norms and standards set out in National Health Council Resolution 466/2012 11 and approved by the Ethics Committee of the Federal University of the State of Maranhão’s University Hospital and the National Research Ethics Committee (code numbers 2.888.343 and CAAE 83673418.7.0000.5086, September 11, 2018, respectively).
Results
A total of 414 beriberi cases were reported in the country between 2013 and 2018, comprising 210 (50.7%) indigenous people, 178 (43.0%) brown people, 16 (3.9%) black people, and 10 (2.4%) whites (data not shown). The age of the cases varied from 0 to 98 years, with a mean ± SD and median age of 43.9 ± 0.7 and 44 years, respectively. There were 7 reported cases of infantile beriberi (data not shown in the table).
Almost all of the cases (407; 98.3%) occurred in 3 states in the Legal Amazon: Maranhão (MA), Tocantins (TO), and Roraima (RR). The frequency of cases was greatest in 2017 (n = 159; 38.4%). RR accounted for 80.0% of cases in 2014 and 61.7% of cases in 2015. In 2016, and each year thereafter, TO accounted for the majority of cases (Table 1).
Distribution of Reported Cases of Beriberi by State and Year of Occurrence. Brazil, 2013 to 2018.a
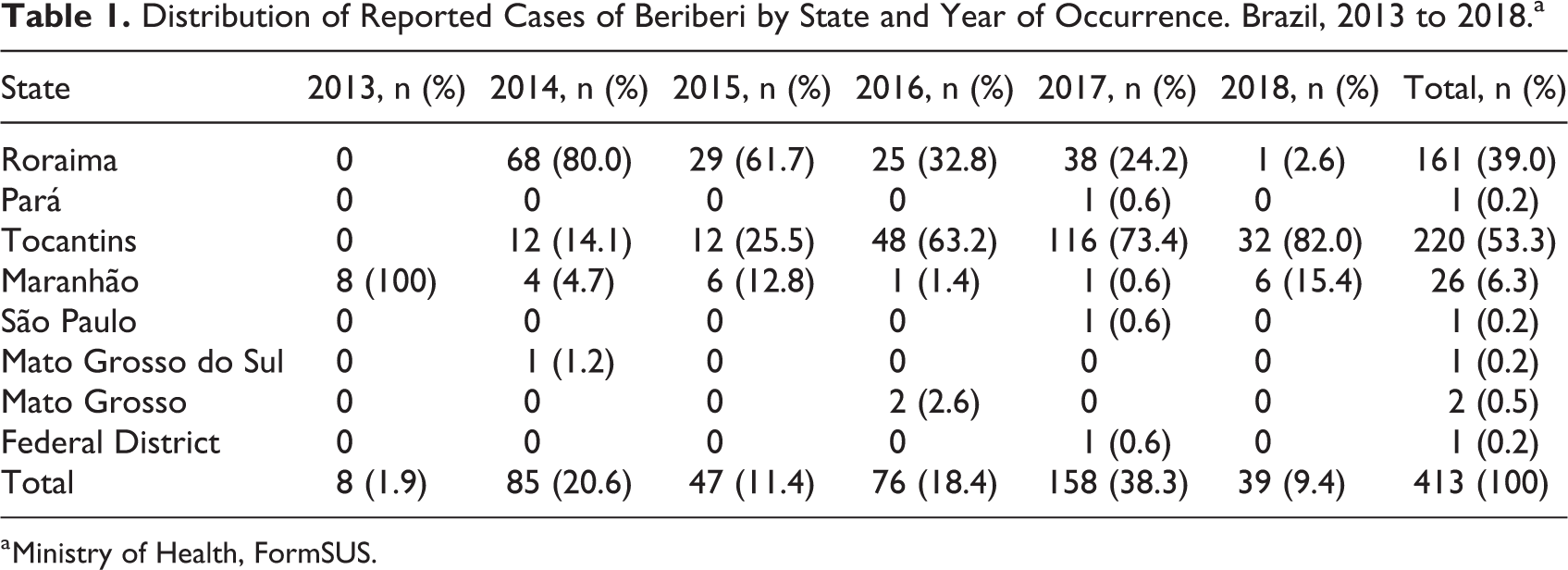
a Ministry of Health, FormSUS.
All cases among indigenous people occurred in states in the Legal Amazon (MA, RR, and TO; Figure 1). In MA, there were 7 cases among indigenous people (26.9% of total cases) occurring in 2 ethnic groups living in the northeast of the state in 3 villages located in 3 different municipalities (Figures 2A and B). In RR, all of the 161 cases were among indigenous people and occurred in 2 ethnic groups living in the north of the state in 47 villages located in four different municipalities; 159 (98.8%) of the cases occurred among the Macuxi people (Figure 2C and D). In TO, there were 42 cases among indigenous people (19.1% of total cases) spread diffusely throughout the state across 8 ethnic groups living in 22 villages in 8 different municipalities (Figure 2E and F).
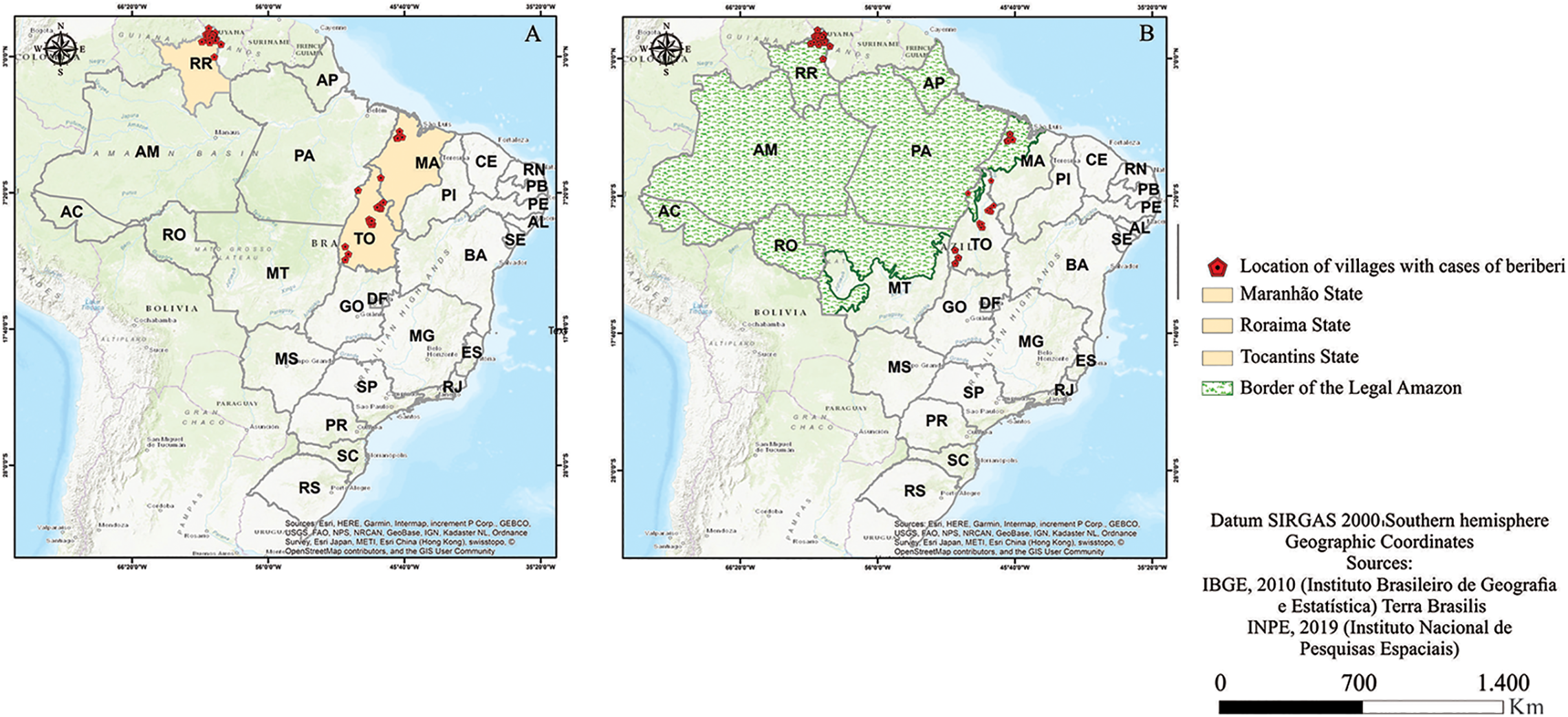
Distribution of reported cases of beriberi among indigenous people in states located in the Legal Amazon. Brazil, 2013-2018. (A) Location of the villages in the 3 states. (B) Overlapping of cases and boundary of the Legal Amazon. This figure is in color in the electronic version.
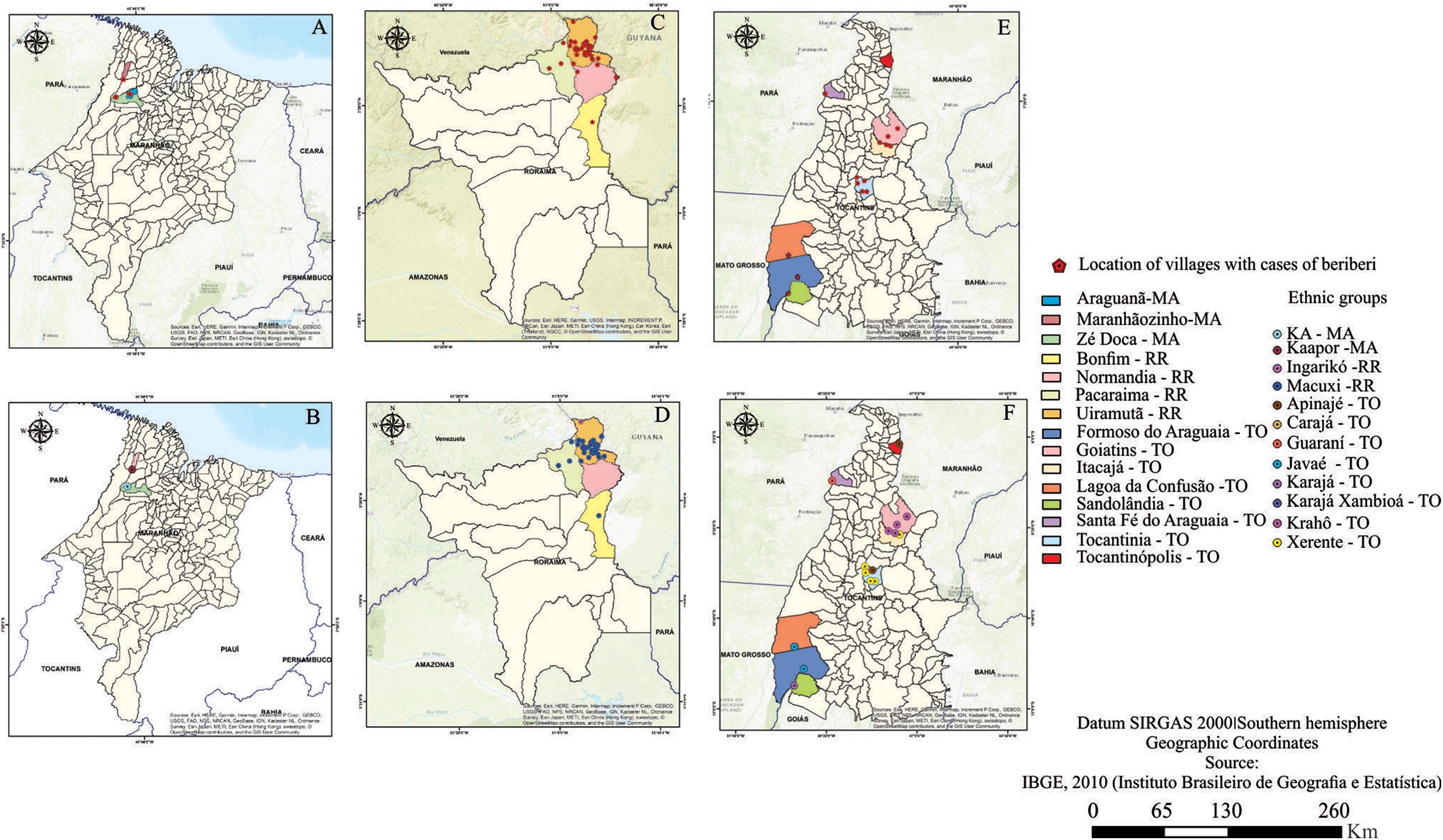
Reported cases of beriberi among indigenous people by state, village, and ethnic group. Brazil, 2013-2018 (A and B) Maranhão. (C and D) Roraima. (E and F) Tocantins. This figure is in color in the electronic version.
With regard to distribution of cases by month of occurrence, 52.0% of the cases among indigenous people occurred in July 2014 and November 2017, while 13.7% of cases in nonindigenous people occurred in March 2017.
Kernel density estimation showed hotspots (high density) in TO and RR, which were also the states with the highest concentration of cases (381; 92.0%; Figure 3).
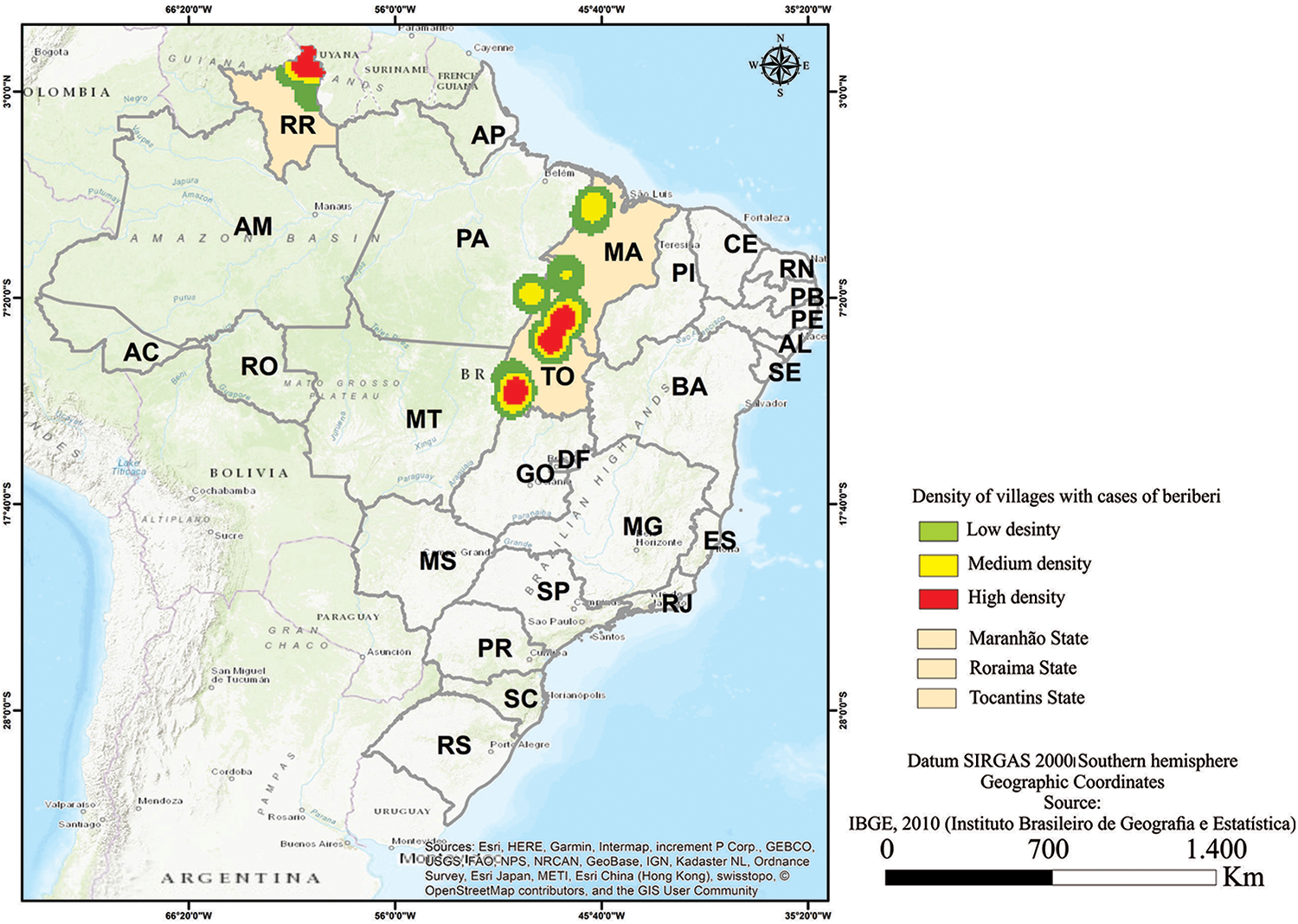
Kernel density of reported cases of beriberi among indigenous people. Brazil, 2013-2018. This figure is in color in the electronic version.
Discussion
The beriberi cases reported among indigenous and nonindigenous people occurred in the Legal Amazon, primarily in the states of Maranhão, Roraima, and Tocantins. Cases were reported in each of the months throughout the study period, with the largest number of cases being reported in 2014 and 2017.
The climate in the Legal Amazon is predominantly equatorial, with rainfall concentrated in a 6-month rainy season. 12 However, some regions have a tropical climate, with rainfall concentrated in the summer months. 13 It is important to highlight that historical reports of cases of beriberi show frequent outbreaks in tropical regions. 5
It is important to mention that ploughing and hunting are physically demanding activities that require high energy expenditure and, consequently, a high intake of thiamine. Likewise, high intakes of carbohydrates and alcohol also lead to an increased demand for this micronutrient, which is already scarce due to a diet that is low in thiamine. 1
Although TO ranked first in the number of cases during the study period, occurrences were not concentrated in specific areas, while in MA and RR cases were concentrated in the northwest and north, respectively. One of the predisposing factors for beriberi in TO is development projects affecting indigenous territories and traditional communities, which result in hunger, disease, and poverty. For example, large-scale hydroelectric projects in the region have jeopardized the traditional livelihood practices of the Xerente people, 14 one of the ethnic groups affected by the disease identified by this study. Indigenous people in Brazil are exposed to various environmental and socioeconomic transformations, leaving them in a situation of food insecurity and nutritional vulnerability. 15
MA ranked third in the number of cases reported during the study period (26 cases). It is interesting to note, however, that there was a sharp drop in the number of cases when compared to the numbers reported by Padilha et al 1 for the period 2006 to 2008 (1207 cases and 40 deaths). This suggests a possible underreporting of cases, given that the state was in the high social vulnerability category in the dimension income and employment from 2016 to 2017. 16 Underreporting may be caused by difficulties in diagnosing vitamin deficiency and misdiagnosis with other conditions such as Guillain-Barré syndrome. 17 Although we identified cases in a specific region of the country, it is highly likely that people in other regions were affected by the disease. Further research is needed in other areas with different populations.
A case–control study conducted in Uiramutã in RR investigating factors associated with beriberi in the Macushi people found that all the controls showed low thiamine levels, indicating that the whole population ran the risk of developing beriberi. 5
The majority of nutritional diseases are associated with poverty and hunger. In this regard, it is notable that the prevalence of undernourishment dropped from 4.6% (8.6 million people) in 2004 to 2006 to under 2.5% (less than 5.2 million people) in 2015 to 2017. 18 It is important to stress, however, that this reduction should not conceal populations living with food insecurity, such as those living in pockets of poverty in the country’s North and Northeast regions, including areas of the semi-arid region, indigenous populations, Quilombolas (descendants of slaves living in rural, suburban or urban communities characterized by subsistence farming and cultural manifestations rooted in the African past), artisanal fishers, and riverine communities.
Another very common practice in subsistence farming is post-harvest storage. One of the main crops stored in the North and Northeast regions is rice, which can be attacked by fungi that produce mycotoxins. Several decades ago, in Japan, Shoshin beriberi was associated with the consumption of yellow rice contaminated with the mycotoxin citreoviridin produced by Penicillium citreonigrum. 19 More recently, P citreonigrum and citreoviridin were found in rice samples during an outbreak of beriberi in MA. 20
Thiamine deficiency testing is rarely available in the region of occurrence of beriberi, and testing is not available on the national health system, 2 making the confirmation of the diagnosis rare among people with limited financial resources. 21 The diagnosis of beriberi relies on a high level of clinical awareness and educated guessing, 22 and empirical treatment with thiamine is used to confirm diagnosis, showing rapid clinical improvement. 2
The Kernel density map shows clusters with a high density of beriberi cases in TO and RR. This pattern may be due to the influence of environmental factors and the social vulnerability of indigenous peoples in these states. This is the first time that this spatial analysis tool has been used in a study of cases of beriberi.
Our attention is focused on malnutrition that arises from the proximity between indigenous people and non-indigenous people, particularly through changes in behavior after contact with another culture and conflicts over lands of which the former are the rightful owners. Indigenous people have had their lands invaded and face the illegal occupation of areas surrounding their villages. As a result, they lack sufficient land to support hunting and fishing, their age-old ways of obtaining food, leaving them no alternative but to seek sub-employment or depend on government programs. Combined with numerous other factors associated with food and nutritional insecurity, this situation jeopardizes the quality and quantity of food. 23
Study limitations are related to the form used to report diseases to the country’s national health information system. The form consists of an Excel worksheet without automated control of data entry errors and missing information and without a function preventing the finalization of completed forms due to inconsistencies.
Despite these limitations, this study makes an important contribution to existing knowledge on this subject and provides important insights into nutritional deficiency among vulnerable populations in Brazil. In this respect, to the best of our knowledge, it is the first nationwide study on reported cases of beriberi among indigenous populations.
Conclusions
The findings show an important pattern in the spatial distribution of reported cases and can be used to guide actions that contribute to the monitoring and prevention of beriberi among indigenous people. It is vital that the government provides adequate care and treatment to people with beriberi in endemic regions, promotes interventions in primary health care to develop and revise beriberi prevention and control strategies directed at these populations, and implements training programs for health staff in prevention and follow-up of patients from at-risk groups.
All people have the legal right to regular and permanent access to quality food in sufficient quantity to satisfy individual nutritional demands. The occurrence of cases of beriberi among vulnerable populations such as indigenous peoples shows disrespect for this human right. The government has the responsibility to guarantee the realization of the human right to adequate food. It is vital to understand the magnitude of this disease in the country in order to take the necessary measures to overcome hunger among affected populations.
Footnotes
Authors’ Note
AKMA participated in the research and design of the article, performed the organization and analysis of the FormSUS data, and participated in all phases until the final writing of the article. MRFCB contributed to the research and design of the article, guided all phases of the research, and participated in all phases until the final writing of the article. TSS, SSBC, JJDJ, VMSS, and ASA performed the analysis of the FormSUS data and contributed to the writing of the article. RCSQ, MTBAF, and AJMC contributed to the final edition of the article. BLCAO contributed to the interpretation of data and writing of the article. AMS contributed to the design of the article and participated in all stages until the final writing of the article. All authors approved the final version sent and are prepared to assume public responsibility for its content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CNPq (National Counsel for Technological and Scientific Development) [Grant No: 408230/2017-7]. We thanks CAPES (Coordination for the Improvement of Higher Education Personnel) [finance code No: 001]. We are grateful to the FAPEMA Foundation (Maranhão State Foundation for Scientific Research and Technological Development) for their support program to article publication. The authors are grateful to FAPEMA Foundation for the fellowship granted PIBIC to TSS and to CAPES for the doctorate research fellowship to SSBC and VMSS.