
Abstract
Background:
Optimal early child development (ECD) is fundamental for every child to achieve their developmental potential and thrive. Household food insecurity (HFI) is a risk factor for suboptimal development, but there is still a need to better understand the pathways that explain this relationship.
Objective:
To evaluate whether maternal mental health and infant’s diet mediate the association between HFI and ECD using structural equation modeling.
Methods:
Cross-sectional study with 474 mother–infant dyads. Mothers answered a questionnaire that evaluated variables through validated instruments. Structural equation modeling analyses were conducted to obtain standardized effects (β) and bias-corrected 95% CI, enabling comparisons between the magnitude of the effects. The following observed variables were included: HFI, ECD, consumption of a healthy and diverse diet, the presence of a partner in the household, wanted pregnancy, and current breastfeeding. Latent variables were included to evaluate mental health, poverty, and neonatal health.
Results:
Poor maternal mental health mediated the relationship between HFI and ECD (β = −.05), but a healthy and diverse diet was not a mediator in this relationship. Poverty was related to lower development scores directly (β = .21) and indirectly (β = .02). Not having a partner (β = .05) and having an unwanted pregnancy (β = .02) predicted indirectly lower development scores.
Conclusions:
Poor maternal mental health mediates the relationship between HFI and ECD, and ECD is influenced by poverty, single motherhood, and unwanted pregnancy through different pathways. Therefore, public policies and interventions that aim to promote an optimal ECD should also approach these aspects.
Keywords
Introduction
Early child development (ECD) is fundamental for every child to achieve their developmental potential and have their right to survive and thrive guaranteed. 1,2 The period of most rapid brain growth occurs from pregnancy to toddlerhood and is considered to be a window of opportunity for optimal ECD. An adverse environment that does not support ECD can impact individual’s future earnings, health, and well-being. 1,3,4 It is estimated that 250 million children younger than 5 years are at risk of poor development in low- and middle-income countries. 3 Poverty, poor caregiver’s mental health, inadequate nutrition, and household food insecurity (HFI) are risk factors for suboptimal ECD. 1,5 -7
Household food insecurity is characterized by the lack of access to nutritious and safe foods in enough amount to lead an active, productive, and healthy life. 2,5,8 -10 Household food insecurity can be manifested in different levels of severity: Mild HFI happens when there is a concern about the availability or access to food in the future and there is a reduction in the quality of food consumed. Moderate or severe HFI occurs when families experience a reduction in the quantity of food, which can in turn lead to overt hunger. 8 In Brazil, in 2013, 22.6% of households experienced HFI, with 7.8% being in moderate or severe levels. 8 The negative association between HFI and ECD has been found in previous studies, most of them conducted in high-income countries. 5,6,11 However, there is still a need to better understand the pathways that explain this relation, especially in low- and middle-income countries.
Peréz-Escamilla and Vianna 5 pointed out 2 pathways that could explain the relation between HFI and ECD. First, HFI can compromise the availability of food in the household, and the nutritional deficiencies caused by the lack of access to a nutritious diet can affect the brain development, leading to ECD delays. 5,12,13 Second, the inability to cope with the psychosocial stress caused by HFI can lead to maternal mental health issues, such as anxiety and depression, which could impact ECD through insufficient caregiver–child interaction, stimulation, and attachment. 5,12 -14 Other factors can also mediate or modify this relation, including poverty, unwanted pregnancy, preterm birth, infant health, and single-parent households, resulting in the need to understand the association between HFI and ECD through more complex models. 1,5,15 -18
To our knowledge, the complex relation and mediation pathways between HFI, maternal mental health, infant’s diet, and ECD have never been studied. Structural equation modeling (SEM) is a statistical tool that has been used to understand complex direct and indirect pathways among multiple factors. 19 Therefore, the present study aimed to evaluate whether maternal mental health and infant’s diet mediate the association between HFI and ECD using an SEM. We hypothesized a priori that both maternal mental health and infant’s diet would mediate the association between HFI and ECD.
Methods
This cross-sectional study was carried out at 20 primary health centers (PHC) in the Federal District, Brazil. It is part of a wider study that aims to evaluate the association between maternal mental health and infant’s nutrition and health. The minimum sample size (461 mother–infant pairs) was estimated to detect associations between maternal depression, HFI, and ECD based on the prevalence of maternal depression (50%), an α of 5%, a CI of 10%, and a loss of up to 20% owing to incomplete questionnaires.
Adult mothers (≥20 years old) whose infants were between the ages of 6 and 12 months were included in the study. The mother responded questions regarding the older infant if she had twins. From the 623 mothers invited to participate in the study, 79 refused to participate and 45 had incomplete questionnaires. Twenty-five pairs were excluded from the sample due to infant’s pathologies that could influence directly or indirectly ECD and/or infant’s diet (eg, meningitis, asthma, bronchitis, syphilis, mononucleosis, cardiopathy, seizures, anemia, G6PD deficiency, phenylketonuria, jaundice). Therefore, the final sample consisted of 474 mother–infants dyads.
All dyads who attended the PHC for either infant’s vaccination or well-child medical visits and fulfilled the study’s inclusion criteria were invited to participate in the study. The questionnaire was applied by trained interviewers, and it was previously tested in a pilot study with 30 mothers in a nonselected PHC. The data collection occurred from March to September 2018. At the end of the research, to guarantee the quality of the study, 5% of the participants were called back by phone for the reapplication of 3 sociodemographic questions. The information was checked with what was answered previously in the questionnaire, and no inconsistency was found.
The research protocol was explained in detail and all mothers signed a written consent form to participate. The study was approved by the research ethics committee of the School of Health Sciences at University of Brasília (protocol number: 67069417.0.0000.0030) and by the research ethics committee of the Foundation of Education and Research in Health Sciences (protocol number: 67069417.0.3001.5553).
Measures
The SEM analyses were based on observed variables that were directly measured and latent variables derived from groups of observed variables, reflecting theoretical constructs. 19 For the construction of the latent variables, only observed variables with a significant factorial load higher than 0.3 were included.
Observed Variables
Household food insecurity was assessed with the extensively validated Brazilian Food Insecurity Measurement Scale (Escala Brasileira de Insegurança Alimentar [EBIA]). 20 The EBIA is a 14-item scale adapted from the US Household Food Security Survey Module that can be used to classify the households as food secure (0 points), mild food insecure (1-5 points), or moderate or severe food insecure (6-14 points). 8,21,22 In our analyses, HFI was classified in 3 levels of severity (0 = food security, 1 = mild HFI, 2 = moderate or severe HFI).
Early child development was measured using the Brazilian Early Childhood for Healthy Adults Questionnaire (PIPAS), which was developed for Brazilian children and has been shown to have adequate reliability and validity. 23,24 The PIPAS is a population assessment instrument that evaluates, based on the primary caregiver’s self-report, the overall development of children until 5 years old across the motor, language, cognition, and socioemotional domains. It has different number of questions according to the infant’s age: birth to 6 months (9 questions), 7 to 9 months (9 questions), and 10 to 12 months (12 questions). The final score is calculated by adding the number of items achieved by the children and reflects the overall child’s development. In order to be comparable between different ages, the score was standardized in a percentage basis. The ECD overall scores were used as a continuous variable, ranging from 0% to 100%, with higher score percentages indicating better development. 23
The consumption of a healthy and diverse diet by the infant was assessed using a Food Frequency Questionnaire (FFQ) previously used in the Brazilian Demography Health Survey. 25 The FFQ evaluated the intake of different food groups during the last week (no intake; 1 d/wk; 2-3 d/wk; 4-6 d/wk; every day of the week). The infant had a healthy and diverse diet in the previous week if he or she consumed the following groups in most days (at least 4 times per week): (1) fruits, vegetables, or leafy greens; (2) chicken, beef, or pork; (3) beans; and (4) cereals or tubers; consumed fish, liver, or egg at least once; and did not consume candies, soft drinks, processed snacks, or fried foods. The consumption of a healthy and diverse diet was classified in 2 categories (0 = no, yes = 1). 26
Other variables included were the presence of a partner in the household, wanted pregnancy, and current breastfeeding, all classified as 0 = no and yes = 1. According to the recommendations of the World Health Organization, the infant was considered currently breastfed if the mothers reported breastfeeding on the day before the interview. 27
Latent Variables
The mental health latent variable was created from 3 continuous observed variables: maternal depression, maternal trait anxiety, and maternal state anxiety. Maternal depression was measured using Beck Depression Inventory-II, a self-administered 21-item questionnaire, that evaluates the presence and intensity of depression symptoms and that had been previously validated in Brazil. 28,29 The final score ranges from 0 to 63 points and a greater score reflects a higher risk of depression. The State-Trait Anxiety Inventory (STAI), which has been previously validated in Brazil, 30,31 assessed both trait and state anxiety. 32 Each STAI scale (anxiety-trait and anxiety-state) includes 20 items with a 4-point Likert scale response option. The score of each scale can vary from 20 to 80 and a higher score indicates a greater chance of having anxiety. For descriptive analyses, we also classified mothers as recommended 33 -36 with and without symptoms of depression (≥14 points) and trait and state anxiety (≥40 points for each scale).
The poverty latent variable was created from 3 observed variables: maternal educational level (0 = incomplete or complete elementary school, 1 = incomplete or complete high school, 2 = incomplete or complete college education or above); household monthly per capita income, which was classified according to extreme poverty or poverty lines based on Brazilian minimum wage (0 = up to US$60, 1 = >US$60 ≤ US$120, 2 = >US$120); and participation in Programa Bolsa Familia (0 = yes, 1 = no), which is the Brazilian cash transfer program and targets families with monthly per capita income lower than US$43.
The neonatal health latent variable was created from 3 dichotomous observed variables: preterm birth, hospitalization for at least 5 days after birth, and neonatal intensive care unit (NICU) needed after birth, all classified as 0 = no and 1 = yes.
Data Analyses
Initially, descriptive analyses (mean, SD, and frequency distribution) were conducted using the statistical software SPSS version 20.0. The SEM analyses were conducted using the statistical software AMOS version 25.0 following the 3 steps as recommended by Kline 37 : (1) The measurement model was tested by confirmatory factor analysis to evaluate whether the indicators chosen to measure the 3 latent constructs were acceptable. (2) The SEM model was tested to obtain the total, direct, and indirect standardized effects (β) and bias-corrected 95% CI, enabling comparisons of relative magnitude of the effects related to different paths in the model. (3) A parsimonious model was estimated removing nonsignificant direct pathways in accordance with the theoretical model and the χ2 test used for comparison with the full model. The following prior criteria were used to evaluate the adequacy of model fit: goodness of fit and comparative fit indices ≥ 0.95, χ2 to degree of freedom (df) ratio < 3.0, and root mean squared error of approximation ≤ 0.05 (90% CI upper limit ≤ 0.08). For the estimation of the parameters, we used the asymptotic distribution free bootstrap method with 900 replications. 37 For the SEM analyses, AMOS Bayesian imputation was used to handle missing data in the following variables: HFI (0.84% missing), ECD (1.17% missing), household per capita income (6.33% missing), and preterm birth (0.84% missing).
Results
Nearly half (48.1%) of the 474 participants reported to live in food insecure households, with 8.7% living under moderate or severe food insecurity. Most mothers had a partner in the household (73.0%) and wanted their pregnancy (84.4%). The mean age of infants was 8.12 (SD = 1.74). The majority of them was born at term (91.9%) and was currently breastfed (81.9%). Most of the infants (74.1%) did not have a healthy and diverse diet (Table 1). The mean ECD standardized score was 95.13% (SD = 6.92%). The mean score in the questionnaires evaluating depression, trait anxiety, and state anxiety were 11.51 (SD = 8.86), 39.56 (SD = 10.61), and 37.83 (SD = 9.45), respectively. Nearly one-third of the mothers were classified as having depression (32.5%) and state anxiety (35.4%), and almost half of them as having trait anxiety (48.3%).
Descriptive Analysis of Household Food Insecurity, Poverty, Neonatal Health, Presence of a Partner at the Household, Wanted Pregnancy, Current Breastfeeding, and Healthy and Diverse Diet. Brasília (DF). 2018.
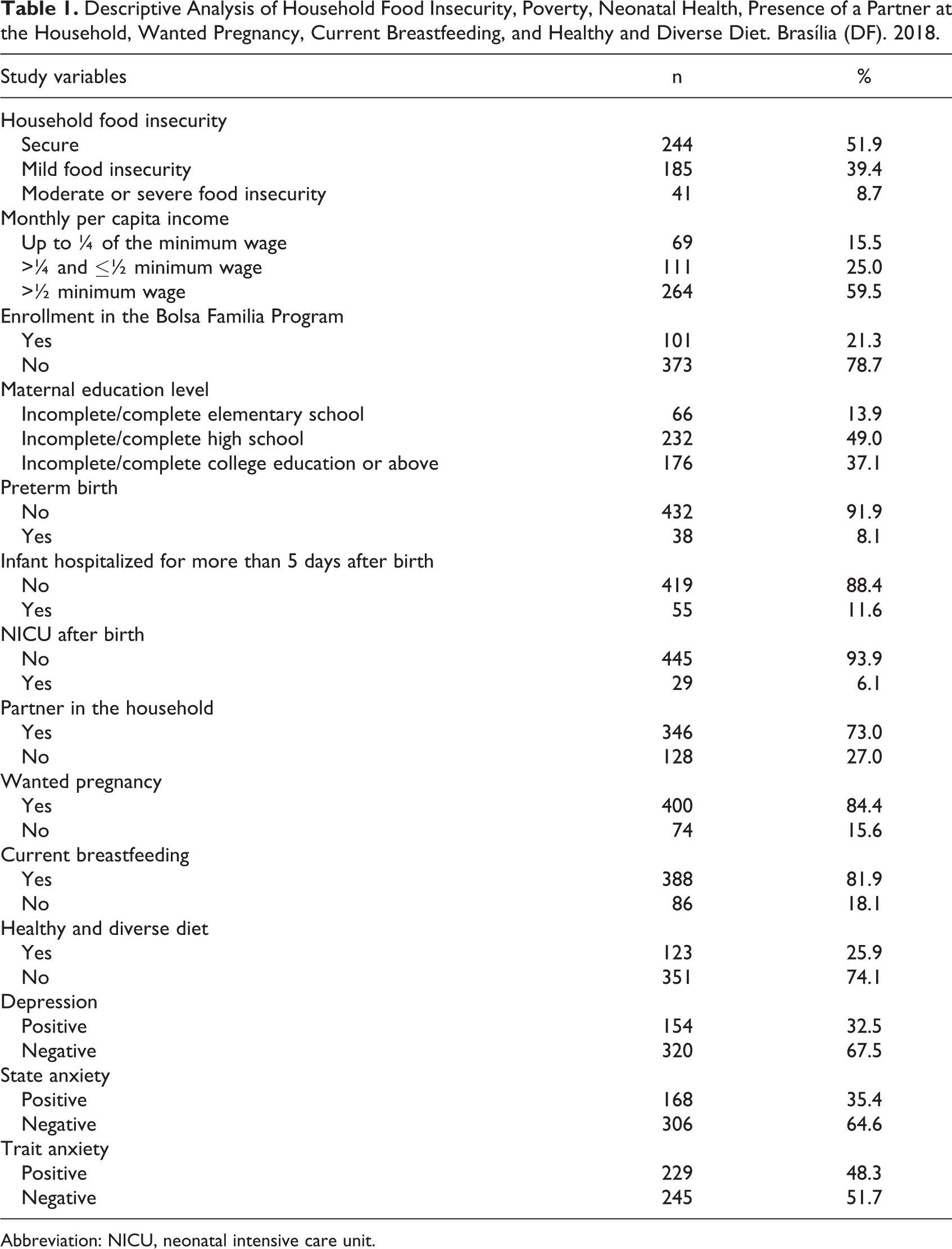
Abbreviation: NICU, neonatal intensive care unit.
In the measurement model, the use of the 3 latent factors mental health, poverty, and neonatal health was supported by confirmatory factor analyses with good model fit (Figure 1). The factorial loadings confirming “mental health” were depression (β = .74), trait anxiety (β = .88), and state anxiety (β= .74), while the ones confirming “poverty” were income (β = .80), educational level (β = .62), and participation in PBF (β = .58). In addition, the item loadings confirming “neonatal health” were preterm birth (β = .39), hospitalization (β = .78), and place in NICU after birth (β = .79; Figure 1). The full and the parsimonious model were not statistically different (χ2 difference= 45.52, df difference = 34, P = 0.09) and showed a good fit according to the criteria established a priori (Figures 2 and 3). The variables neonatal health and current breastfeeding did not remain in the parsimonious model.
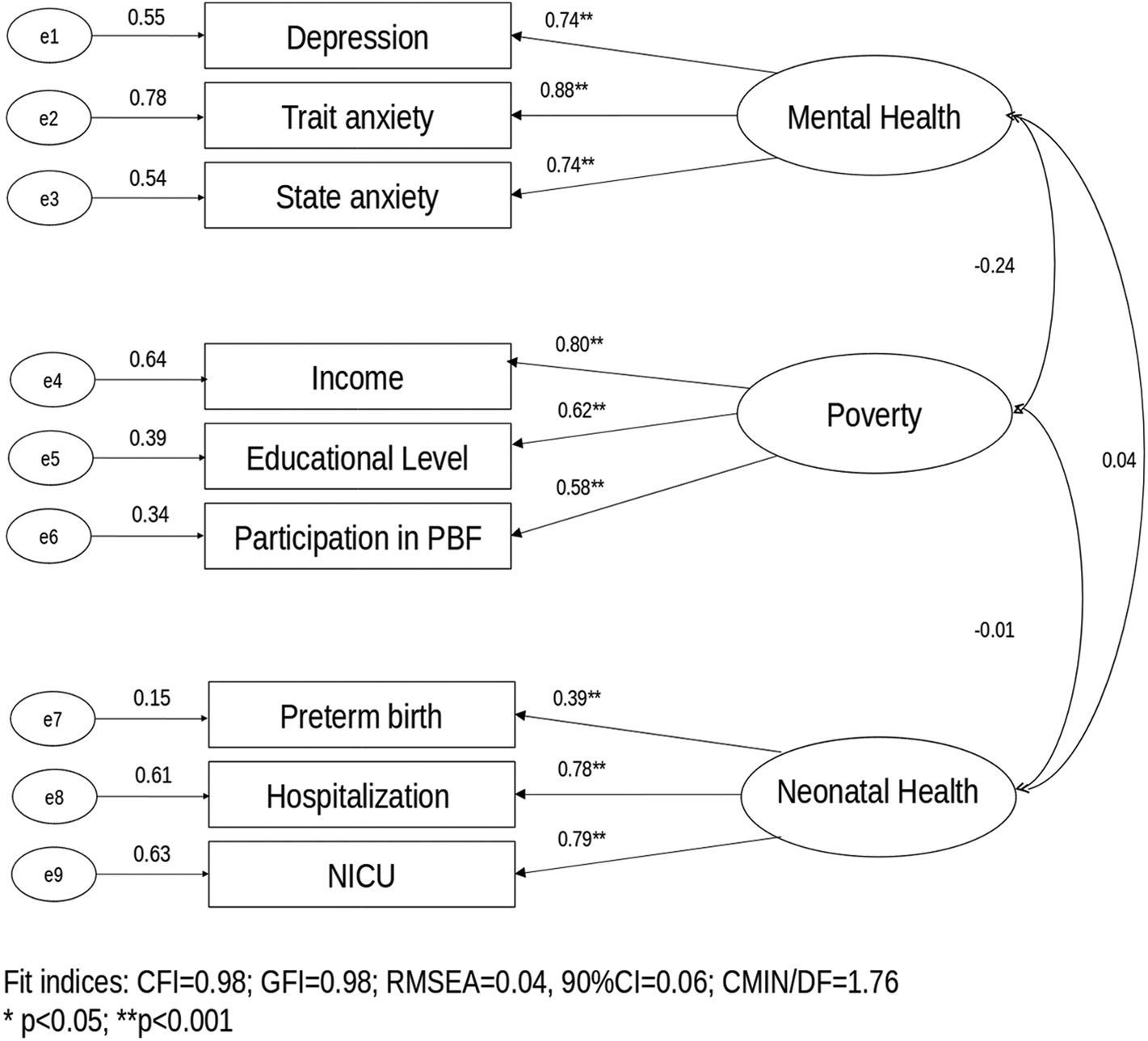
Confirmatory factor analysis of the 3-factor 9 items (measurement model) obtained through bootstrap asymptotic distribution free item loading (standardized coefficients/standard errors). Brasília (DF).
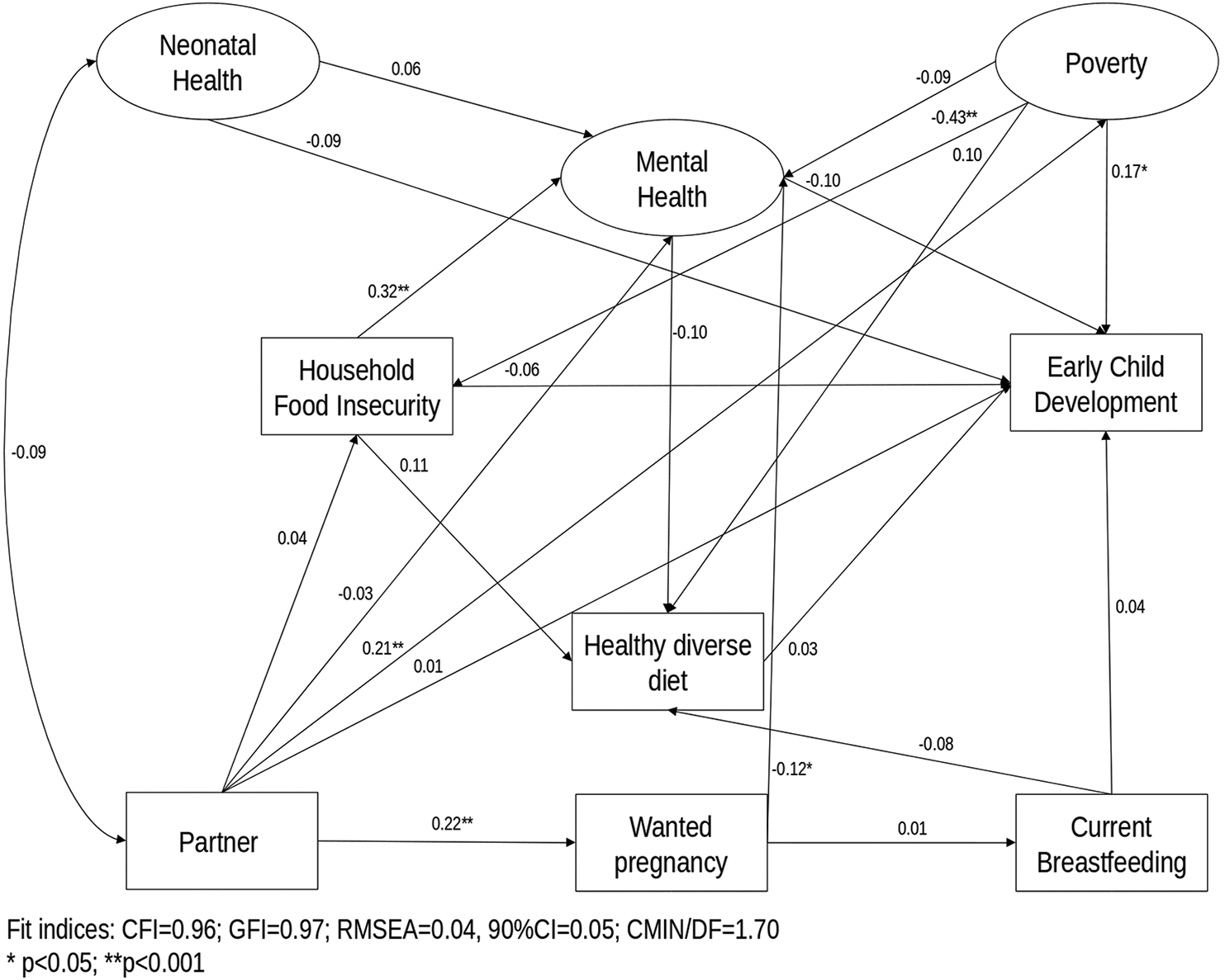
Structural model of the association between household food insecurity, mental health, healthy diverse diet, poverty, neonatal health, partner, wanted pregnancy, current breastfeeding, and early child development outcomes. Brasília (DF). 2018. Solid lines indicate standardized direct effects.
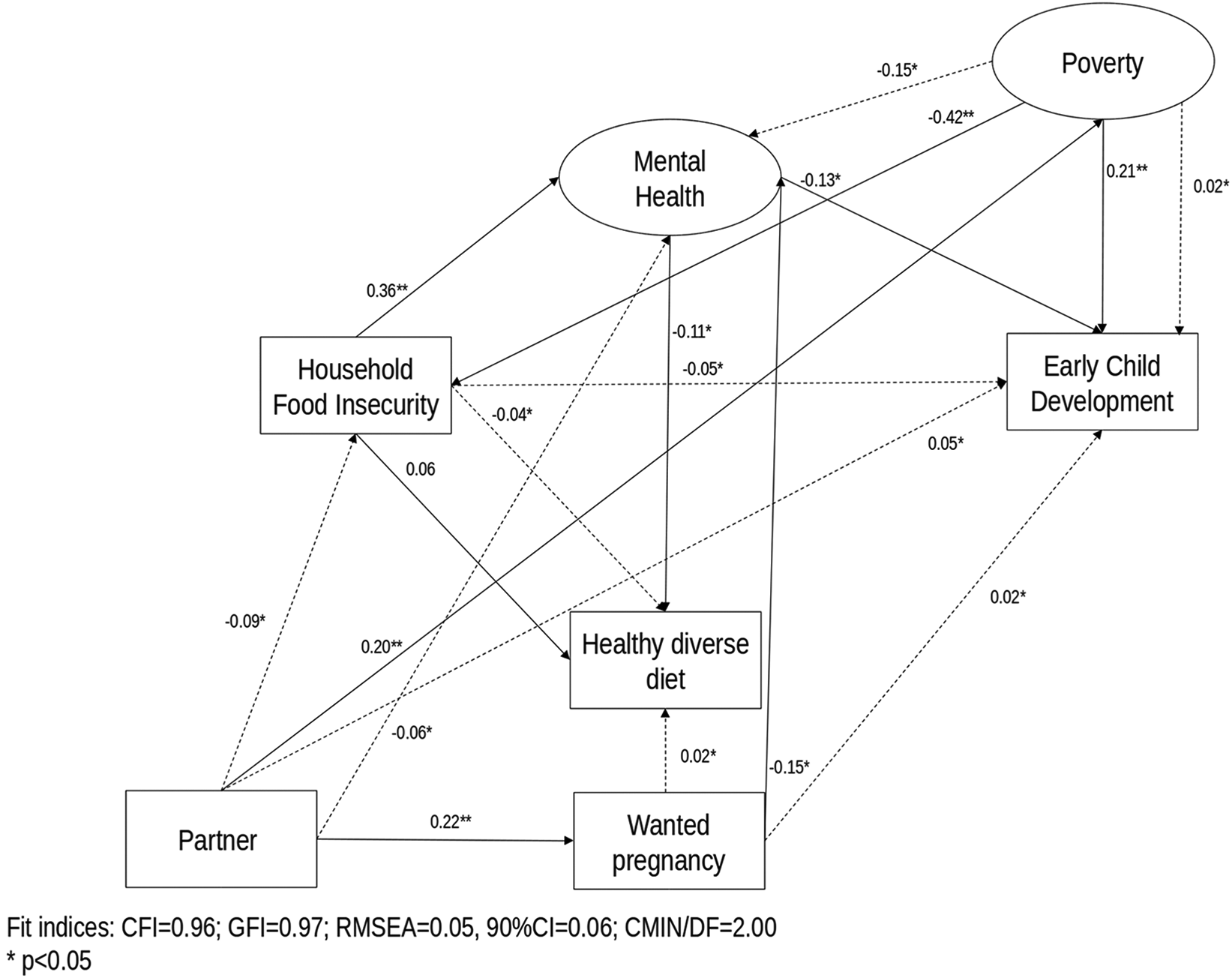
Parsimonious model of the association between household food insecurity, mental health, healthy diverse diet, poverty, neonatal health, partner, wanted pregnancy, and early child development outcomes after the removal of the structural model’s nonsignificant direct pathways. Brasília (DF). 2018. Solid lines indicate standardized direct effects. Dashed lines indicate standardized indirect effects.
Table 2 presents the results of the direct and indirect effects as well as the interpretation of the results. In relation to direct effects, we found that poverty was associated with lower ECD scores (β = .21) and to higher levels of HFI (β = −.42); not having a partner was associated with poverty (β = .20) and to an unwanted pregnancy (β = .22); an unwanted pregnancy (β = −.15) and higher levels of HFI (β = .36) were the direct predictors of poor maternal mental health; and poor maternal mental health directly predicted lower ECD scores (β = −.13) and an unhealthy and nondiverse diet (β = −.11; Figure 3 and Table 2).
Description of the Direct and Indirect Paths Standardized Effects on the Structural Equation Model. Brasília (DF). 2018.
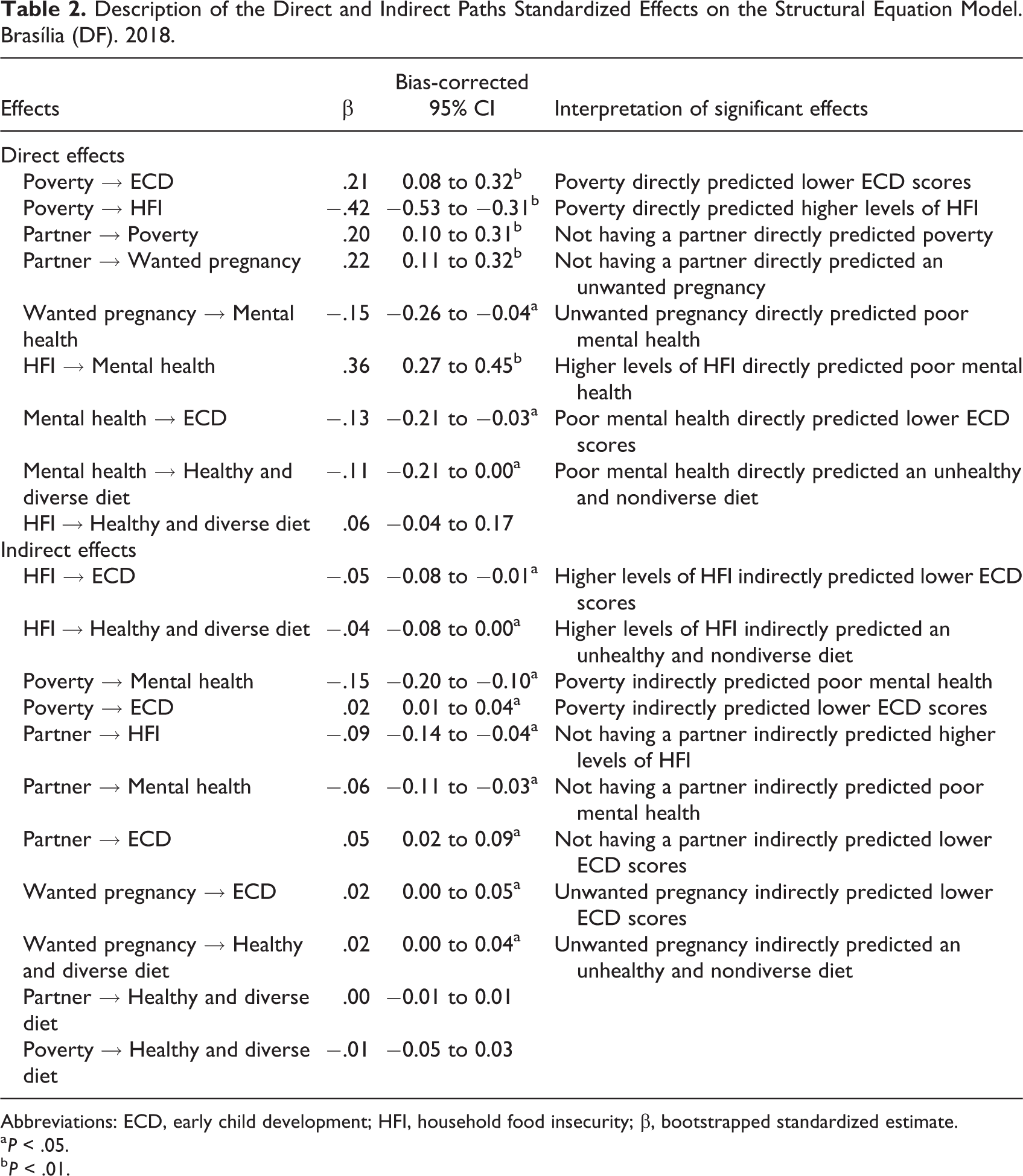
Abbreviations: ECD, early child development; HFI, household food insecurity; β, bootstrapped standardized estimate.
a P < .05.
b P < .01.
Regarding indirect effects, in accordance with our hypotheses, poor maternal mental health mediated the relation between HFI and ECD (β = −.05). However, a healthy and diverse diet was not a mediator in this relation (Figure 3 and Table 2).
Higher levels of HFI were associated with an unhealthy and nondiverse diet mediated by poor maternal mental health (β = −.04).
Poverty was associated with poor maternal mental health mediated by HFI (β = −.15) and linked to lower ECD scores mediated by HFI and poor maternal mental health (β = .02; Figure 3 and Table 2).
In addition, not having a partner was associated with higher levels of HFI via poverty (β = −.09). Not having a partner was also linked to poor maternal mental health mediated by 2 pathways: (1) unwanted pregnancy (52.2% of indirect effects) and (2) first poverty and then HFI (47.8% of indirect effects; β = −.06). Not having a partner also predicted lower ECD scores also mediated by 2 pathways: (1) poverty (90.7% of indirect effects) and (2) first unwanted pregnancy and then poor mental health (9.3% of indirect effects; β = .05).
An unwanted pregnancy predicted lower ECD scores mediated through poor maternal mental health (β = .02) and was linked to an unhealthy and nondiverse diet mediated by poor maternal mental health (β = .02).
Regarding total effects, the variables that presented greater effect magnitude on ECD were poverty (β = .23) and poor maternal mental health (β = −.13).
Discussion
We found that maternal mental health mediated the association between HFI and ECD. This finding addresses an important gap in the literature, being the first study that investigated this pathway in a middle-income country in the Latin America and Caribbean Region. Previous studies conducted in the United States observed similar findings, with caregivers’ mental health mediating the relation between HFI and child’s development and behavior problems. 14,38 -40 Household food insecurity is a chronic stressor and worries about the availability of food for the family—and especially for the offspring—can increase the rates of anxiety and depression in mothers living in food insecure households. 5,13 In this context, maternal poor mental health can affect parenting skills including the ability to interact and attach with the infant, which in turn can result in a poor ECD. 5,12 -14,38,41,42 Given the consequences for the health and well-being of the family and the offspring, it is important to screen mothers for HFI and mental health as a routine in health services, aiming to refer food insecure families to nutrition and food assistance programs, as well as depressed and anxious mothers to adequate health care. 5 -7,39,40,43
Contrary to what was hypothesized, infant’s diet was not a mediator in the relation between HFI and ECD. This is an important finding since to our knowledge this is the first study that evaluated poor dietary intake as a potential mediator in the relation between HFI and ECD. 5 First, HFI was not significantly related to an unhealthy and nondiverse diet. The lack of association between HFI with lower dietary quality might be explained by caregiver’s behavior tending to protect and buffer their young children from HFI, by using coping strategies and perhaps compromising their own food intake over their offspring’s. 5,6,44,45 It is possible that caregiver’s nutrition depravation and effort to protect the child from HFI may increase the risk of poor mental health and irritability. 6,45 Even though this pathway was not explored in the present study, we suggest that future studies examine it. Second, an unhealthy and nondiverse diet was not associated with lower ECD scores. We hypothesize that ECD might have not been affected by the infant’s diet because the infants in this study were very young (between 6 and 12 months) and may have started complementary feeding recently. However, this does not exclude the possibility that this effect may appear in the future, given that an unhealthy and nondiverse diet was already being predicted directly by maternal mental health and indirectly by HFI. Therefore, considering that a consumption of a high-quality diet is crucial for the adequate growth and development, 1,46,47 longitudinal studies should be designed to address the impact of an unhealthy and nondiverse diet in ECD.
As expected, poverty was also a predictor of lower ECD scores, HFI, and poor maternal mental health, which agrees with previous research. 48 -51 Tella et al 50 observed in Brazil that maternal education was associated with better child’s language and cognition development, while socioeconomic status was related to better infant’s language and motor development. Families that experience poverty may provide a less stimulant environment to the infant, due to the lack of access to toys and books. 48 -50 In addition, lower maternal educational level has been related to a lack of learning activities in the household, such as reading books, playing, and drawing. 18,48,50 The impact of poverty on infant’s development in such an early age highlights the need for public policies that target these populations aiming to prevent the intergenerational transmission of poverty. 52
We found that not having a partner was indirectly associated with HFI, poor maternal mental health, and lower ECD scores through different pathways. Single mothers were also more likely to experience poverty and unwanted pregnancies. Previous studies also observed that single parenting increased the chance of experiencing poverty, poor physical and mental health, and suicidal ideations. 16,17,53,54 The responsibility of taking care and providing financially for their child as well as the stigma and lack of social support can be stressful, challenging, and demanding, which in turn can affect parenting practices. 16,17,53,55 Therefore, health professionals, social workers, and policy makers could focus on approaches that take into account the specific needs of single parents.
Our findings show that women who had unwanted pregnancies are also a vulnerable group, since they were more likely to have poor mental health and through this pathway predict ECD and infant’s diet. Theme-Filha et al 56 observed in a national survey in Brazil that almost one-third of pregnancies were unwanted and that these women were nearly 5 times more likely to not have a partner. Unintended pregnancy (mistimed or unwanted) is a public health problem since it can affect birth outcomes, maternal physical and mental health, mother–child relationship, breastfeeding, child’s well-being, and socioemotional development. 56 -61 Therefore, there is a need for family planning programs with high coverage and quality, aiming to inform women and guarantee access to contraceptive methods. 56,59 Additionally, these programs should cover maternal mental health, supporting women with unwanted pregnancies and/or children with mental health adequate assessment and treatment. 60
The present study was limited by its convenience sampling and cross-sectional design limiting the external validity and drawing causal inferences. In addition, we only evaluated infants from 6 to 12 months and HFI can have different impacts in older children; thus, we suggest that future studies also include children in different age groups. Also, the PIPAS questionnaire was created to evaluate the overall development, and we suggest that subsequent research also explore different development domains. However, in spite of these limitations, this study is innovative and fills in an important gap in the literature, through the use of the statistically and conceptually robust SEM, to explore and understand the relation between HFI and ECD. Longitudinal cohort studies are needed to determine causality and identify promising approaches to improve parenting skills and ECD outcomes in the context of HFI.
In conclusion, our main result is that poor maternal mental health mediates the relation between HFI and ECD. Our study also highlights that poverty, single motherhood, and unwanted pregnancy influence ECD through different pathways. The impact of these factors on ECD in the first months of life is alarming and highlights the importance of routinely assessing ECD in child health services and providing adequate environment, stimulation, and nutrition for children to reach their developmental potential. 1,5 Furthermore, it is necessary that public policies and interventions that aim to promote an optimal ECD in the first year of life also approach HFI, maternal mental health, nurturing care, financial issues, family planning, social support, and empowerment of women. 1,55,62
Footnotes
Authors’ Note
Pedroso J. contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Herkrath F., Buccini G., Venancio S., and Perez-Escamilla R. contributed to analysis and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Gubert M. contributed to conception and design, contributed to analysis and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES; finance code 001) and CAPES scholarship Programa Doutorado Sanduíche no Exterior (process number 88881.189710/2018-01).