
Abstract
Background:
Growing evidence highlights the linkage between body image, eating, and exercise behaviors among adolescents.
Objective:
This study aims to determine the association between body image perception, nutritional status, and dietary and physical activity behaviors among adolescents in Indonesia.
Methods:
A cross-sectional household survey was conducted among a representative sample (n = 2160) of adolescent girls and boys aged 12 to 18 years in Klaten and Lombok Barat districts. The association between adolescents’ body image, their diets, and physical activity patterns was determined using complex samples Cox’s regression analysis. Separate multivariate models were developed for adolescent girls and boys.
Results:
Physical appearance was considered important to nearly all adolescents. Approximately 11% of girls and 14% of boys were overweight or obese, the majority of whom (∼70%) correctly perceived themselves as overweight or obese. More of overweight or obese adolescents felt unhappy about their perceived weight than their thin counterparts. With respect to the overweight/obese girls, the adolescents’ perceptions of being overweight or obese was associated with a 63% reduction in the prevalence of overweight/obese girls consuming fatty snacks, such as deep-fried crackers (adjusted prevalence ratio (PR): 0.37, 95% confidence interval (CI): 0.19-0.71) and a 40% reduction in the prevalence of overweight/obese girls engaging in moderate-intensity physical activity (adjusted PR: 0.60, 95% CI: 0.38-0.94), after adjusting for potential confounders. No association between body image and eating and physical activity behaviors was observed among adolescent boys.
Conclusions:
Body image may be one of the most important determinants of dietary and physical activity behaviors, and thus future efforts to foster healthy eating and physical activity behaviors among Indonesian adolescents need to address body image concerns.
Introduction
The double burden of malnutrition, characterized by the coexistence of undernutrition and overweight and obesity, is a global public health concern which affects all countries and age groups. 1 Adolescents in low- and middle-income countries are among the hardest hit, and an important target group for early interventions. In Indonesia, 11% of adolescent girls and boys aged 13 to 15 years were estimated to be thin in 2013, while a further 11% of adolescents of the same age were overweight or obese. 2 Changes in dietary intake patterns, coupled with the decrease in physical activity associated with industrialization and urbanization, are known to have contributed to an increased prevalence of overweight and obesity and related noncommunicable disease, whereas the problem of undernutrition remains undefeated.
Adolescence is a period of rapid growth and development, accompanied by prominent psychosocial and emotional changes. 1 Various health-related behaviors, including food intake and physical activity, are developed during adolescence and carry over into adulthood, with major implications for health prospects. 3 Notably, body image perceptions formed during the early life course contribute to nutritional status, and body size and shape at a later life-stage, which, in turn, influence a range of physiological and psychological outcomes. 4,5
Body image is a multidimensional construct, which reflects an individual’s perception, thoughts, feelings, and behaviors about the size, shape, and structure of his or her body. 6 It is a dynamic perception, which can change according to mood, physical experience, and the environment. 4 Most adolescents develop their body image perception due to the influence of their peers, parents, and the media, as well as wider social perceptions of what constitutes an ideal body type. 7,8 Their personal (physical and physiological changes during puberty), cultural, and environmental factors may also influence their perceptions. Body image is also highly gender-influenced, with girls and boys expressing different body image perceptions, 9,10 such as the perception that girls should be slim and boys should be muscular. 8
Evidence is conflicting on whether accurate body image perception (perception relative to anthropometric norms) has adverse or positive consequences on adolescents’ health-related behavior. Research has shown that concerns about being overweight or obese have the potential to lead to eating disorders, excessive exercise, depression, and other unhealthy weight management. 11,12 Conversely, overweight adolescents who accurately perceive their body weight were reported to engage in healthy weight-related behavior compared to their counterparts. 13 Importantly, much of the existing evidence on adolescents’ perception of their body weight and shape, and its influence on their dietary intake and physical activity, has been generated by high-income countries. 14 -17 Given the epidemiologic transition and emerging burden of obesity and noncommunicable disease in low- and middle-income countries, additional evidence from these contexts is essential for informing public health interventions.
This study aims to describe body image perceptions among Indonesian adolescent girls and boys in relation to their actual nutritional status and to examine associations with diet and physical activity behaviors. The findings will have implications for the design, planning, and implementation of localized gender-responsive intervention strategies.
Methods
Study Design and Participants
A cross-sectional household survey was conducted across all subdistricts in Klaten district in Central Java province and Lombok Barat district in West Nusa Tenggara province between April and May 2017. The 2 districts were selected in consultation with the national and subnational government and having taken into account differences in cultural context, infrastructure, and adolescent nutritional status. The survey was administered among a representative sample of adolescent girls and boys aged 12 to 18 years and their parents or guardians, as appropriate. The survey sample (n = 2160) was obtained using a multistage cluster sampling strategy powered to detect a 7.5% difference in key physical activity and dietary behaviors between boys and girls and between the 2 districts. A probability proportionate to size sampling strategy was first employed to select 45 clusters in each district to ensure that more clusters were selected in subdistricts with more villages. Subsequently, at least 12 girls and 12 boys aged 12 to 18 years were selected from each cluster in one or more subvillages using simple random sampling. If there were more than 12 adolescents of either sex in a cluster, we selected 12 using simple random sampling. If there were less than 12 boys and 12 girls, a second or potentially a third subvillage were randomly selected to obtain the required sample size. Only one adolescent from each household was included in the sample. The methods has been described elsewhere. 18
The study excluded those refusing an interview or anthropometric measurements, those with any form of mental and/or physical disability, and/or those not physically living in the selected village. Married or pregnant adolescents were excluded in the analysis. The survey was approved by the Ethical Committee of Gadjah Mada University in Yogyakarta, Indonesia. Interviews and assessments were only conducted after written consent was obtained from both the adolescent and the parents/guardian.
Data Collection
Data were collected by 2-person field teams using standardized digital questionnaires on a mobile data collection system on Android-based tablets. All interviews and anthropometric measurements were conducted in the respondent’s home. Interviews were conducted either in Indonesian or the local language (Javanese/Sasak), separately with both the parents and adolescents in order to minimize any parental influence on the adolescents’ answers.
Information was collected from adolescents on their demographic characteristics, education, morbidity, reproductive health, dietary intake, physical activity, smoking and alcohol use, and body image. Specifically, the body image perception was assessed using a standard questionnaire developed based on locally adapted validated tools from other settings, including the Figure Ranking Scale and Body Shape Questionnaire. The standard questionnaire inquired about adolescents’ awareness and perception of their body size and shape, relevant influencing factors, and efforts being made to improve their body weight. Dietary intake was determined by using a 7-day qualitative food frequency questionnaire (FFQ), for which the list of food items was developed in line with the food groups used in the Household Dietary Diversity Score (HDDS). Adolescents were also questioned about their consumption frequencies of snacks, fast food, ready-to-eat meals, sweetened beverages, and fruits. Data on physical activity were collected using a 7-day activities frequency table, 19 which assessed the number of days in which each activity was performed, and the average duration of the performance of each activity. A wide range of mild, moderate, and vigorous activities was included in the questionnaire. In addition, household sociodemographic characteristics, access to sanitation, the source of drinking water, and other relevant information were collected from the parents and/or guardians of the adolescents.
The adolescent’s height and weight were assessed following standard procedures. The height measurement was taken to the nearest 0.1 cm, using a SECA 206 Mechanical Measuring Tape (Microtoise), and weight was assessed to the nearest 0.1 kg, using SECA 874 flat digital weighing scales, which were calibrated regularly. The height and weight were measured in a duplicate manner. If the differences between the 2 measurements were more than 0.1 cm and 0.2 kg, the third and fourth measurements were taken. Hemoglobin concentration was assessed using HemoCue cuvettes from peripheral blood obtained from the participants’ fingertip with the use of a softclix device and lancet. In Klaten, HemoCue 201+ (HemoCue) was used and in Lombok Barat, Hemocue 201+ and HemoCue 301+ were used. Efforts were made to obtain the adolescent’s date of birth from his/her birth certificate, family/ID card, or other official documents, to the extent possible. Otherwise, the adolescent’s self-reported date of birth was used.
The field enumerators were trained according to the study protocols prior to the survey and were directly supervised by field coordinators as data collection proceeded. All data were checked for measurement bias and underwent stringent quality control (QC) checks. At least 10% of all respondents of each enumerator were reinterviewed by the QC team on selected indicators. The QCs were selected from the trained enumerators who scored highest during the training. Height and weight measurements of 10% participants were also repeated. The QC team revisited the respondents within 2 to 7 days of the original data collection period.
Statistical Analysis
A total of 2144 adolescent girls and boys were included in the analysis, after the exclusion of married and pregnant adolescents (n = 16). All data were double-entered, and appropriate data cleaning procedures were conducted. Descriptive analyses were employed to examine the distribution of the full range of variables. The data were weighted for probability of selection and adjusted for the multistage cluster sampling design.
Body mass index (BMI) was defined as the adolescent’s weight in kilograms divided by height in meters squared (kg/m2). Z-score of BMI for age (BMIZ) were estimated using the 2007 World Health Organization (WHO) growth reference standard. Thinness and overweight or obesity were defined as BMIZ less than −2 and above 1, respectively.
Appropriate cutoffs were applied to create dichotomous or categorical variables. Household wealth quintile was assessed using the principal component analysis outlined in the Demographic Health Survey, while household food security was determined by applying the Household Food Insecurity Access Scale. Household sanitation and drinking water sources were dichotomized into private (private facility with/without a septic tank) or nonprivate facilities (shared/public latrine, pit latrine without slab, yard/bush/forest, river/stream/creek, and others); and improved (piped water, well with pump, protected well, protected spring, and rain) or unimproved sources (unprotected well, unprotected spring, bottled water, refilled water, river/lake/pond/irrigation/dam, and others), respectively.
The adolescents’ dietary diversity was assessed following the recommended methodology for determining the HDDS. A dichotomous variable was created to define low and high dietary diversity intake using the following cutoffs: low (<5 food groups) or high (≥5 food groups). Similarly, adolescents were classified into 2 groups, as to whether their daily physical activity met the recommendations from the WHO or not (at least 60 minutes of moderate to vigorous daily physical activity for adolescents aged 12-17 years, and at least 150 minutes of moderate or 75 minutes of vigorous daily physical activity for 18 year-olds). 20
Analyses were performed separately for adolescent girls and boys to understand the differences in their perceptions. First, the adolescent’s body image perception was compared to their nutritional status through the use of a χ2 test. No comparison was made for the normal weight adolescents due to specific interest to understand the perceptions of thin and overweight or obese adolescents. Subsequently, among adolescents who were overweight or obese, the association between body image perception and their dietary and physical activity behaviors was determined using a complex samples χ2 test. No analysis on the above associations were made for the adolescents who were thin due the small numbers of thin adolescents who misperceived their body weight. The key binary variables of dietary and physical activity behaviors were included as the dependent variable, and body image perception was included as the independent variable, adjusting for all potential confounders such as age, education, place of residence, and maternal education. Potential confounders were selected based on their known association with individual dietary and physical activity behaviors and were included in the final regression models if they were significantly associated with dietary and physical activity behaviors in the bivariate analyses (P < .05). Separate regression models were constructed for each key dietary and physical activity behavior using complex samples Cox regression with fixed time effect. All analyses were performed using the Statistical Package for Social Science Complex Samples module version 24.0 (SPSS Complex Samples, Inc).
Results
Of the 2144 adolescents included in the analysis, 48% were girls, and about two-thirds (65%) were living in Klaten district (Table 1). Half the adolescents (51%) lived in food-insecure households. Most adolescents (94%) were enrolled in school, and almost all the adolescent girls (89%) had had their first menstruation at the time of interview. Approximately 4% and 10% of the adolescent girls and boys were thin, respectively, whereas 11% and 14% were overweight or obese, respectively. Less than half adolescent girls (46%) and boys (44%) reported consuming more than 5 food groups in the past week, and only around one-third of girls (35%) and boys (37%) met the daily recommendations for physical activity (Table 1).
Characteristics of Adolescent Girls and Boys Included in the Analysis.a
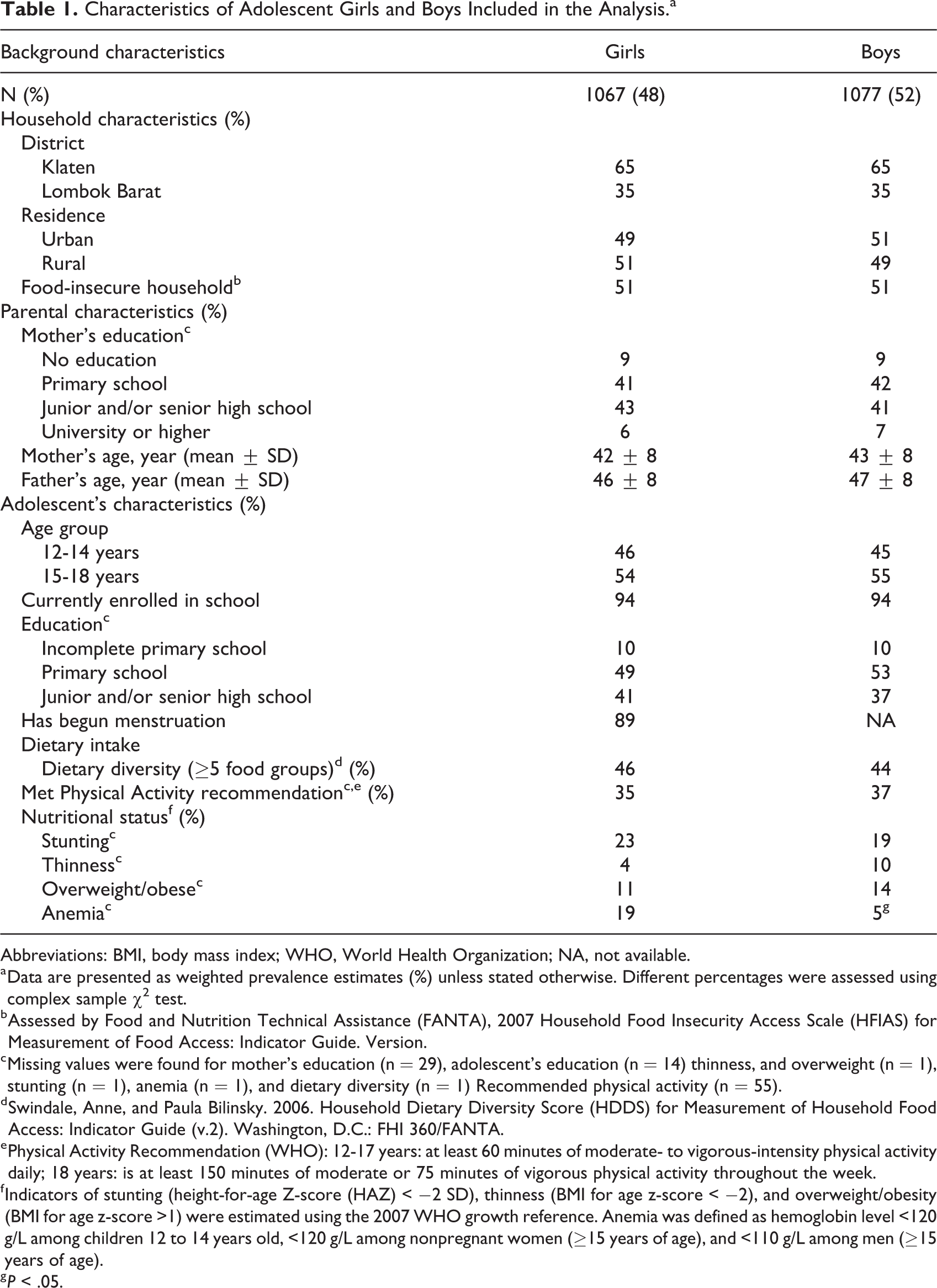
Abbreviations: BMI, body mass index; WHO, World Health Organization; NA, not available.
a Data are presented as weighted prevalence estimates (%) unless stated otherwise. Different percentages were assessed using complex sample χ2 test.
b Assessed by Food and Nutrition Technical Assistance (FANTA), 2007 Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide. Version.
c Missing values were found for mother’s education (n = 29), adolescent’s education (n = 14) thinness, and overweight (n = 1), stunting (n = 1), anemia (n = 1), and dietary diversity (n = 1) Recommended physical activity (n = 55).
d Swindale, Anne, and Paula Bilinsky. 2006. Household Dietary Diversity Score (HDDS) for Measurement of Household Food Access: Indicator Guide (v.2). Washington, D.C.: FHI 360/FANTA.
e Physical Activity Recommendation (WHO): 12-17 years: at least 60 minutes of moderate- to vigorous-intensity physical activity daily; 18 years: is at least 150 minutes of moderate or 75 minutes of vigorous physical activity throughout the week.
f Indicators of stunting (height-for-age Z-score (HAZ) < −2 SD), thinness (BMI for age z-score < −2), and overweight/obesity (BMI for age z-score >1) were estimated using the 2007 WHO growth reference. Anemia was defined as hemoglobin level <120 g/L among children 12 to 14 years old, <120 g/L among nonpregnant women (≥15 years of age), and <110 g/L among men (≥15 years of age).
g P < .05.
Two-thirds (66%) and slightly more than half (55%) of adolescent girls and boys, respectively, knew their current weight (Table 2). About 60% of adolescent girls and boys perceived themselves as being thin, whereas 13% considered themselves to be overweight or obese. Overall, more adolescent boys than girls (87% vs 76%, P < .05) felt either neutral or satisfied with their body image. Nearly all (96%) adolescents thought physical appearance was important, and about a quarter of girls (26%) and boys (27%) reported feeling under pressure to maintain a certain body image. More than half of adolescents reported feeling embarrassed about or lacked confidence in their body image, whereas only 41% of girls and 37% of boys reported having made efforts to change their body weight in the 30 days prior to data collection (Table 2). Many adolescent girls (61%) and boys (50%) compared their own body shape with that of others, including their friends. Peer groups had the greatest influence on defining the ideal body shape of adolescents (Table 2).
Body Image Perception of Adolescent Girls and Boys Included in the Analysis.a,b
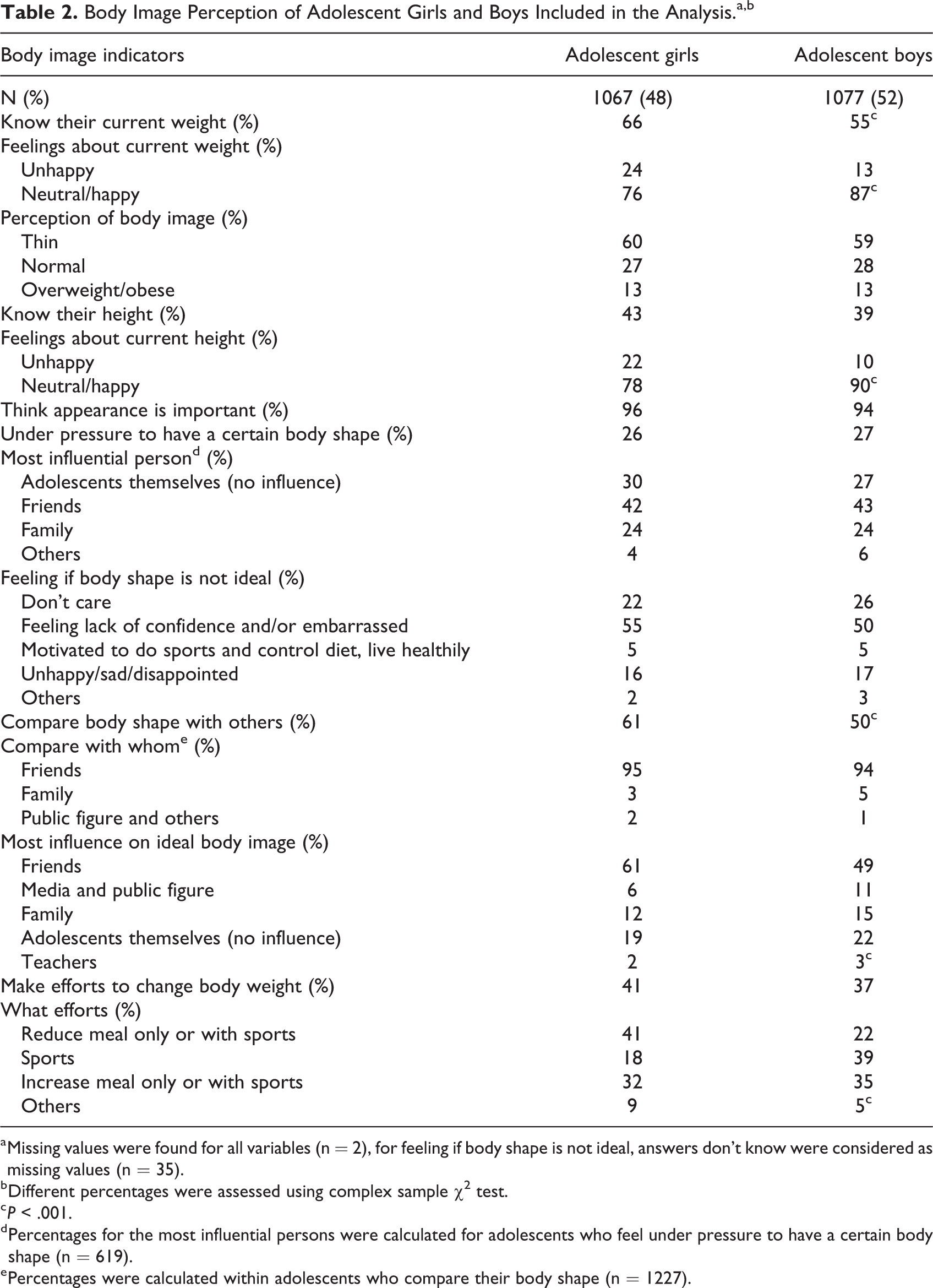
a Missing values were found for all variables (n = 2), for feeling if body shape is not ideal, answers don’t know were considered as missing values (n = 35).
b Different percentages were assessed using complex sample χ2 test.
c P < .001.
d Percentages for the most influential persons were calculated for adolescents who feel under pressure to have a certain body shape (n = 619).
e Percentages were calculated within adolescents who compare their body shape (n = 1227).
More overweight and obese girls (57% vs 31%) and boys (34% vs 20%) felt unhappy about their current body weight than their thin counterparts (Table 3). Whereas the majority of thin adolescent girls (92%) and boys (94%) perceived themselves as being thin, only about two-thirds of overweight or obese girls (67%) and boys (70%) perceived themselves as being overweight or obese. More overweight or obese adolescent girls (60%) and boys (55%) reported having made efforts to change their weight than their thin counterparts (51% and 47%; Table 3).
Description of Body Image According to the Nutritional Status of Adolescent Girls and Boys in Klaten and Lombok Barat Districts, Indonesia 2017.a
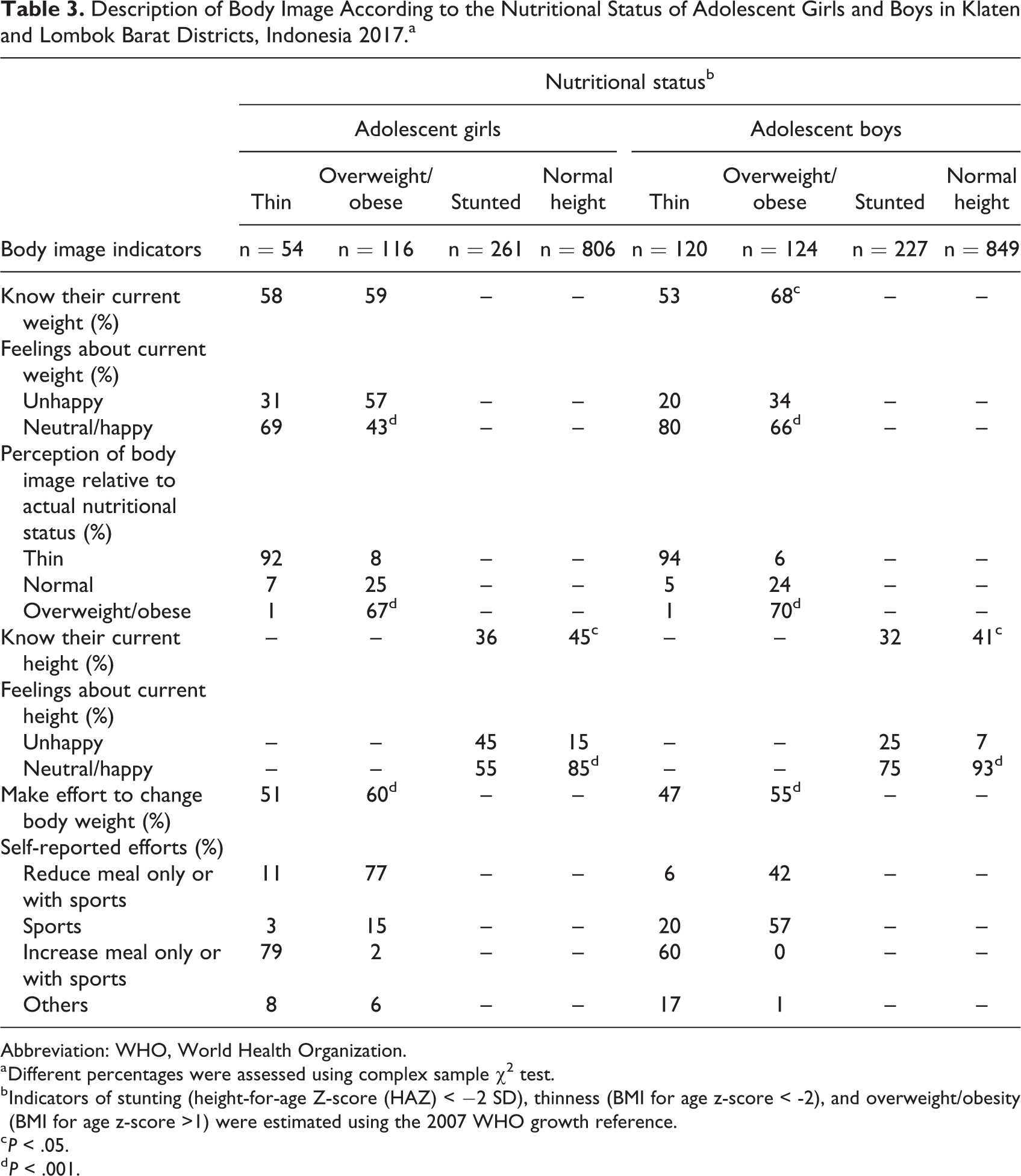
Abbreviation: WHO, World Health Organization.
a Different percentages were assessed using complex sample χ2 test.
b Indicators of stunting (height-for-age Z-score (HAZ) < −2 SD), thinness (BMI for age z-score < -2), and overweight/obesity (BMI for age z-score >1) were estimated using the 2007 WHO growth reference.
c P < .05.
d P < .001.
In a multivariate analysis, overweight or obese adolescent girls who also perceived themselves as being overweight or obese were 0.37 times as likely consuming deep-fried crackers, after adjusting for the mother’s education (prevalence ratio (PR) = 0.37, 95% CI (Confidence Interval): 0.19-0.71) compared to overweight or obese adolescent girls who perceived themselves as being normal weight or thin (Table 4). Likewise, overweight or obese adolescent girls who also perceived themselves as being overweight or obese were 0.64 and 0.60 times as likely meeting physical activity recommendations and engaging in moderate-intensity physical activity on a daily basis, respectively, adjusting for district, adolescent’s age, and education compared to overweight or obese adolescent girls who perceived themselves as being normal weight or thin (PR = 0.64, 95% CI: 0.21-0.90; PR = 0.60, 95% CI: 0.38-0.94). No association between body image and eating and physical activity behaviors was observed among adolescent boys (data not shown).
Univariate and Multivariate Analysis of the Association Between Sociodemographic Characteristics, Body Image Perception, and Snack Consumption and Physical Activity Behavior Among Overweight/Obese Adolescent Girls.a
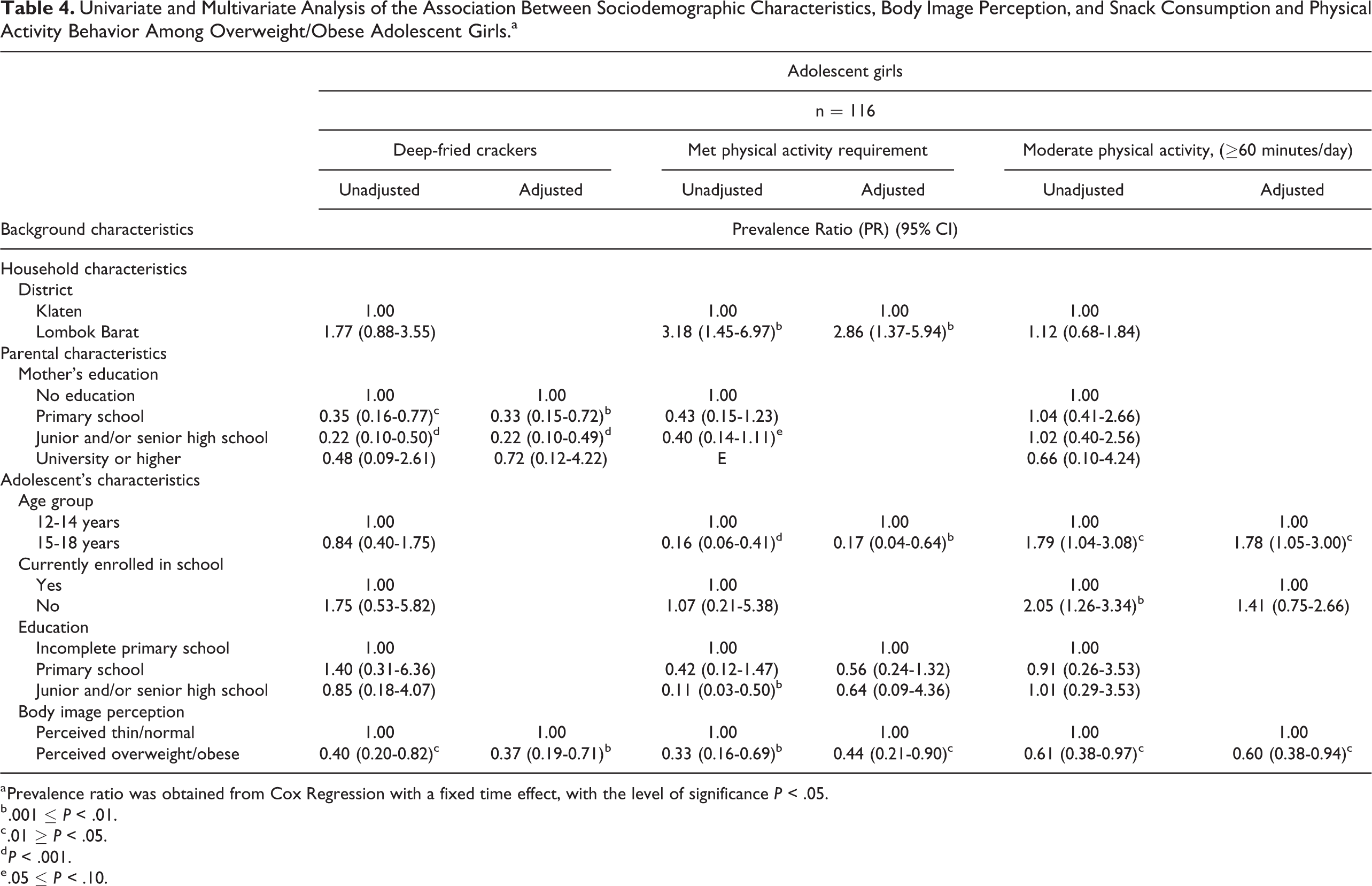
a Prevalence ratio was obtained from Cox Regression with a fixed time effect, with the level of significance P < .05.
b .001 ≤ P < .01.
c .01 ≥ P < .05.
d P < .001.
e .05 ≤ P < .10.
Discussion
Few studies have examined the body image perception of adolescent girls and boys in Indonesia and its association with their nutritional status, dietary intake, and physical activity. In this cross-sectional analysis, body image emerged as an important determinant of dietary and physical activity behaviors, particularly among adolescent girls. Specifically, among overweight or obese adolescent girls, the perception of being overweight or obese was associated with a reduction in the prevalence of overweight or obese adolescent girls consuming certain high-caloric snacks and reduced the likelihood of meeting daily physical activity recommendations. Overall, ∼25% of adolescent girls and ∼10% of boys felt unhappy about their body image, and these proportions were higher among overweight or obese adolescent girls and boys. Importantly, however, less than half of Indonesian adolescents reported having made efforts to change their body weight.
In this study, physical appearance was considered to be important by nearly all adolescent girls and boys, and 1 in 4 adolescents felt under pressure to have their perceived ideal body image which described as slim for girls and muscular for boys. 21 More than half of adolescents reported comparing their body weight and shape with that of their friends. These findings are supported by evidence highlighting the perceived importance of physical appearance among adolescents, 22 -24 and associations with adverse psychological consequences, including sadness, lack of confidence, and even depression. 25,26 Adolescents’ excessive concerns about their physical appearance have also led to various eating disorders and disturbances, 27 -29 which are hazardous to their growth and development.
Nutritional status is a well-accepted determinant of body image perception. 30 -32 More overweight or obese adolescent girls and boys in this study were found to be dissatisfied with their body image than their thin counterparts. Notably, while most of the thin adolescents correctly perceived themselves to be thin, only about two-thirds of overweight or obese girls and boys perceived themselves to be overweight or obese. Comparable results were reported from a previous study conducted in South Korea, in which 64% and 59% of overweight adolescent girls and boys, respectively, correctly perceived their body weight. 25
Body weight perception has been suggested as a predictor of food choice. 33 In the current study, overweight or obesity self-perception was associated with a reduction in the prevalence of overweight or obese adolescent girls consuming certain fatty snacks, such as deep-fried crackers, indicating that the overweight or obese girls who perceived themselves accordingly were more likely to restrict unhealthy food intake. This corroborates previous research, including a study on Slovak adolescents aged 13 to 15 years, which reported that adolescent girls who perceived themselves to be fat were eating less fatty foods. 15,34 However, we did not find an association between body weight perception and intake of fruits and vegetables, indicating that having a corresponding body weight perception and nutritional status among overweight and obese adolescents may contribute to a reduced intake of unhealthy foods but may not necessarily promote healthy eating.
Our results also indicated that perception of overweight or obesity was associated with a reduction in the prevalence of overweight or obese adolescent girls engaging in moderate-intensity physical activity, especially among those adolescent girls who were truly overweight or obese. This is consistent with previous research suggesting that overweight or obese girls who perceived themselves as such, had higher social physique anxiety scores, and were less confident about performing physical activities in a public setting. 34,35 A few studies also revealed that there were several perceived barriers to performing physical activity among adolescent girls, such as feeling lazy, a lack of time, no partner, menstruation, and concerns about physical appearance. 36,37 Thus, overall, our findings correspond with earlier research, which revealed that, despite having strong intentions to lose weight, overweight adolescents who perceived themselves accordingly did not improve their eating or physical activity behaviors. Other research also showed that these adolescents engaged in unsafe and health-compromising weight loss behaviors, such as fasting, meal skipping, taking diet pills, and vomiting. 16,38,39
Importantly, our findings highlighted the gender differences across various aspects of body image perception. Overall, more girls than boys knew their weight and height and were dissatisfied with their body size and shape. Perceived body image was only associated with eating and exercise behaviors in overweight or obese girls and not in boys. This is not surprising, as previous research has consistently shown that females tend to perceive a negative body image more frequently than men 40 -42 and want to have a slim body in order to conform to the social ideals shaped through the media and by their peers. 43 Earlier qualitative research conducted in these same districts suggested that girls were generally less motivated to perform physical activity because they did not want to get sweaty. There was also a perception that “sports are not a girl’s thing,” which lessened the motivation to perform physical activity. These findings highlight the need to apply a strong gender dimension for interventions aiming to improve body image perception, nutritional status, diet, and physical activity.
A few limitations need to be considered. First, the body image assessment tool was adapted and pretested in local settings, but future efforts are needed to validate the findings with a more robust assessment tool. Second, this was a cross-sectional analysis, which limits causal inferences. Third, the use of a qualitative FFQ in the current study limited our ability to accurately assess the total amount of food intake. Fourth, the out of school adolescents may be underrepresented in this study due to response bias related to their consent to participate in the study. Nonetheless, we believe this study adds significantly to existing knowledge on adolescents’ body perception, and its association with their nutritional status, dietary intake, and physical activity, a neglected area of research in Indonesia.
In conclusion, body image perception may be an important predictor of eating and physical activity behaviors among adolescents in Indonesia, and this association may be influenced by the gender and nutritional status of adolescents. However, the extent to which adolescents’ body image perceptions trigger their intention to change body size and shape, make healthier food choices, and increase their physical activity level deserves further investigation. In an emerging middle-income country setting such as Indonesia, obesity prevalence is rapidly increasing among adolescents, and thus effective gender-responsive social and behavior change communication strategies are warranted to promote a healthy lifestyle. Various efforts, such as establishing a peer education group and counseling sessions, may be needed to promote a more positive body image perception among adolescent girls and boys. Importantly, these interventions need to incorporate the influence of body image perception.
Footnotes
Acknowledgments
The authors wish to thank Harriet Torlesse for her contributions to the study design, Damayanti Soekarjo, Julia Suryantan, and Asrinisa Rachmadewi for their support with data collection, Doddy Izwardy and Dyah Yuniar Setyawati for their support and leadership in relation to the adolescent nutrition pilot project, and Paul Pronyk for his insightful comments on the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by The Government of Canada, the Canadian UNICEF Committee, and the 25th Team for the “Addressing MNCH gaps to create scalable investments for the future” project implemented by the UNICEF Indonesia Country Office and the Ministry of Health Republic Indonesia.