
Abstract
Background:
While considerable progress has been made in reducing undernutrition in Bangladesh, regional disparities are known to exist, and certain population subgroups may lag behind.
Objective:
To characterize nutritional status among school-age children in a historically marginalized population of Bangladesh.
Methods:
We conducted a cross-sectional assessment of children attending 14 nongovernmental organization-operated schools serving the tea estate population in Kulaura Upazila, Sylhet Division. We randomly selected 168 children from a population of 418 whose parents attended school-organized Parent–Teacher Association meetings. Parents provided consent and data on household food consumption in the past week, foods consumed by children in the past 24 hours, and household food insecurity. We drew venous blood from assenting children for the analysis of hemoglobin and plasma retinol, C-reactive protein, and α1-acid glycoprotein. Children were classified as stunted, underweight, or thin based on comparisons with the World Health Organization standards for height-for-age, weight-for-age, or body mass index-for-age, respectively.
Results:
Food insecurity was highly prevalent, with ∼85% of households affected. Roughly half of children had low dietary diversity. Prevalence estimates for stunting, underweight, and thinness were 32%, 50%, and 49%, respectively. Approximately 60% of children had a hemoglobin concentration <11 g/dL. The mean (±SD) plasma retinol concentration was 0.79 μmol/L (±0.23 μmol/L), with 34% deficient using a 0.70 μmol/L cutoff.
Conclusions:
A heightened focus on tracking progress in underserved populations and appropriately targeted programming will be critical as Bangladesh seeks to accelerate progress toward global development goals for nutrition.
Introduction
Bangladesh has made considerable strides in reducing the prevalence of undernutrition over the past quarter of a century—progress that is thought to be driven by overall gains in economic development, education, and water and sanitation. 1 Still, the country faces an elevated prevalence of childhood stunting and micronutrient deficiencies. At the national level, 36% of children under the age of 5 are stunted, 33% are anemic, 11% are iron deficient, 45% are zinc deficient, 40% are vitamin D deficient, and 21% are affected by vitamin A deficiency. 2 Levels of undernutrition vary widely between divisions. Prevalence estimates are consistently higher in Sylhet Division, for example, than elsewhere in the country, 3 in concordance with the Division’s relatively poor social indicators such as low female literacy. 4 Historically, populations living and working on Sylhet’s tea estates have been a particular concern due to their low incomes, lack of access to services beyond those provided by the estates, and social exclusion. 5,6 However, limited data exist on the nutritional status of this high-risk group. Data are also limited among school-age children—a life stage characterized by dynamic growth and cognitive development. We carried out an assessment of children attending primary schools serving tea estates in Sylhet Division. We report here on nutritional status indicators of this high-risk population.
Methods
This was a cross-sectional survey designed to inform site selection for a randomized controlled trial of Golden Rice, which is a genetically engineered rice designed to biosynthesize β-carotene as a strategy to improve the vitamin A intakes and status of rice-consuming populations. We focused on schoolchildren, as this group does not regularly receive nutrition interventions, and schools operated by nongovernmental organizations (NGOs), which target underserved and/or high-risk students. The survey covered 2 potential study sites—one in the tea estates and a second in the Dhaka slums—where we anticipated an approximately 30% prevalence of vitamin A deficiency. Assuming an α = 0.05 and a desired precision of ±5%, our target sample size was 320 children, which we increased by 5% to account for refusals. We divided the sample evenly between the 2 sites, affording ∼80% power to detect a 0.1 μmol/L difference in mean plasma retinol between sites, assuming an SD = 0.3 μmol/L and α = 0.05. We report data here from the Sylhet site.
We identified local NGOs operating schools in our targeted study area using a directory maintained by the Campaign for Popular Education. Working with NGO directors, we listed preprimary (kindergarten) or primary (grades 1-5, depending on the school model) schools serving a minimum of 20 students each, of whom >80% were drawn from tea garden populations. To be eligible, schools had to have plans for up to 2 years of continuous operation, without any current or planned coverage with micronutrient-fortified biscuits. Eligible schools were purposively selected from the listing based on location, focusing on clustering of schools to facilitate data collection, and approached for sensitization activities and for consent to provide the roster of enrolled students. Following school consent, we convened Parent–Teacher Association (PTA) meetings, during which we described the study and obtained verbal consent to collect contact information and approach families. All children for whom we obtained contact information were considered eligible for the study. A random sample of children was selected using a random sorting procedure in Excel from each school roster for study enrollment.
Data collection was carried out from March to April 2018. Interviewers visited households of eligible children to obtain consent and collect data on household demographics, assets, and the availability of a clean water source and latrine. We used the Household Food Insecurity Access Scale and the Food Consumption Score to characterize household food security. We collected the child’s date of birth, morbidity in the past 7 days, and a 24-hour dietary diversity recall. A 1-week recall period was used for morbidity, as opposed to the 2-week recall used in Demographic and Health Surveys, as the latter has been shown to underestimate the prevalence of diarrhea, 7 which is a critical public health concern in Bangladesh. A team then visited schools to conduct nutritional status assessments. After obtaining the child’s assent, we measured weight on a Seca 874 digital scale and height using the Seca 217 stadiometer according to standard protocols 8 and collected a 5 mL venous blood sample by antecubital venipuncture into EDTA vacutainers. We measured hemoglobin concentration using a portable HemoCue Hb 201+ photometer (HemoCue), referring children with a hemoglobin concentration of <90 g/L for treatment at a local clinic. Blood was collected in dim light conditions, and samples were stored in cooler boxes for transport.
Whole blood samples were centrifuged at 3000 rpm for 10 minutes to separate plasma, and aliquots were stored in liquid nitrogen for transfer to the International Centre for Diarrheal Disease Research, Bangladesh (icddr, b). At icddr, b, we measured plasma retinol by high-performance liquid chromatography. C-reactive protein (CRP) and α1-acid glycoprotein (AGP) were measured on a Roche automated clinical chemistry analyzer (Cobas c311).
Dietary diversity was described using the 10-group Women’s Dietary Diversity Score classification system, which has been shown to better capture dietary quality in this age-group than other scores, 9 defining food groups according to guidelines from the Food and Agriculture Organization, but without the inclusion of the 15-g intake restriction. 10 We calculated children’s body mass index (BMI) by dividing the child’s weight (kg) by his or her height squared (m2). Anthropometric indices were derived using the World Health Organization Stata macro, 11 based on sex-specific reference data for children aged 5 to 19 years. 12 Children with a height-for-age, weight-for-age, or BMI-for-age Z score less than −2 were considered stunted, underweight, or as having a low BMI (ie, thinness), respectively. The prevalence of anemia was calculated using a hemoglobin cutoff of <11 g/dL. We used linear regression and published methods to estimate an inflammation-adjusted plasma retinol concentration. 13 Both unadjusted and adjusted plasma retinol concentrations were used to calculate the prevalence of marginal vitamin A status and vitamin A deficiency using cutoffs of <1.05 μmol/L and <0.70 μmol/L, respectively. We created binary inflammation variables consistent with classifications in the literature: >5 mg/L for CRP and >1 g/L for AGP.
The protocol for this study was approved by the Ethics Review Committee at the Institute for Diarrheal Disease Research, Dhaka (icddr, b) and the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health.
Results
We worked with 2 NGOs in the tea estates, both of which operated in Kulaura Upazila. A total of 14 schools were selected and PTA meetings convened. The PTA attendance was 93% and 100% of parents and guardians consented to their child’s participation. We obtained biospecimens from 97% of children. Households were predominantly Hindu, and about half of all paternal and maternal occupations were reported as tea estate workers (Table 1). Approximately 50% of fathers and 40% of mothers had received any schooling. Few households (<10%) owned land or small livestock (∼20%), although almost two-thirds of families owned cattle. Food insecurity was highly prevalent, with greater than 40% of households classified as severely food insecure.
Characteristics of Selected Tea Garden Households, Kulaura Upazila, Sylhet Division (n = 168)a
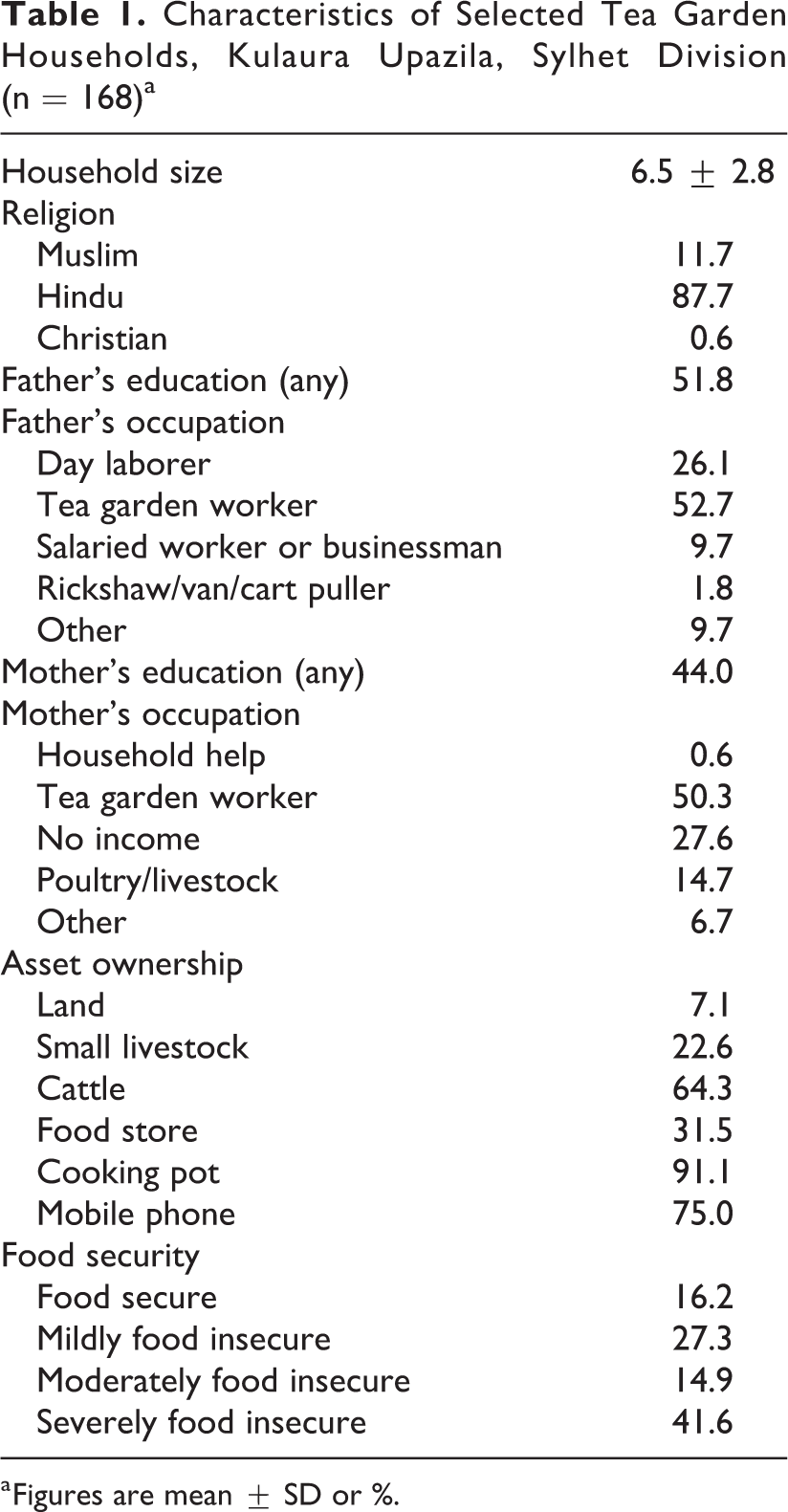
a Figures are mean ± SD or %.
Food frequency data indicated that a little over half of children had low dietary diversity (Table 2). This was consistent with the overall poor nutritional status: roughly one-third of children were stunted and the prevalence of both underweight and low BMI approached 50%. As shown in Table 3, the mean (25th-75th percentiles) hemoglobin concentration was 11.3 g/dL (10.1-11.9 g/dL). Anemia was highly prevalent, with 60% affected. Categorizing this based on severity, ∼14% could be classified as mild, 42% as moderate, and 6% as severe. The overall mean (±SD) plasma retinol concentration was 0.79 μmol/L (±0.23 μmol/L), with almost 90% of children classified as having marginal vitamin A status and one-third of children falling below the 0.70 μmol/L cutoff for vitamin A deficiency. While <10% of children had elevated inflammatory proteins, adjustment for these did decrease the estimated prevalence of vitamin A deficiency to ∼25%.
Characteristics of Children Attending Tea Garden Schools, Kulaura Upazila, Sylhet Division (n = 168)a
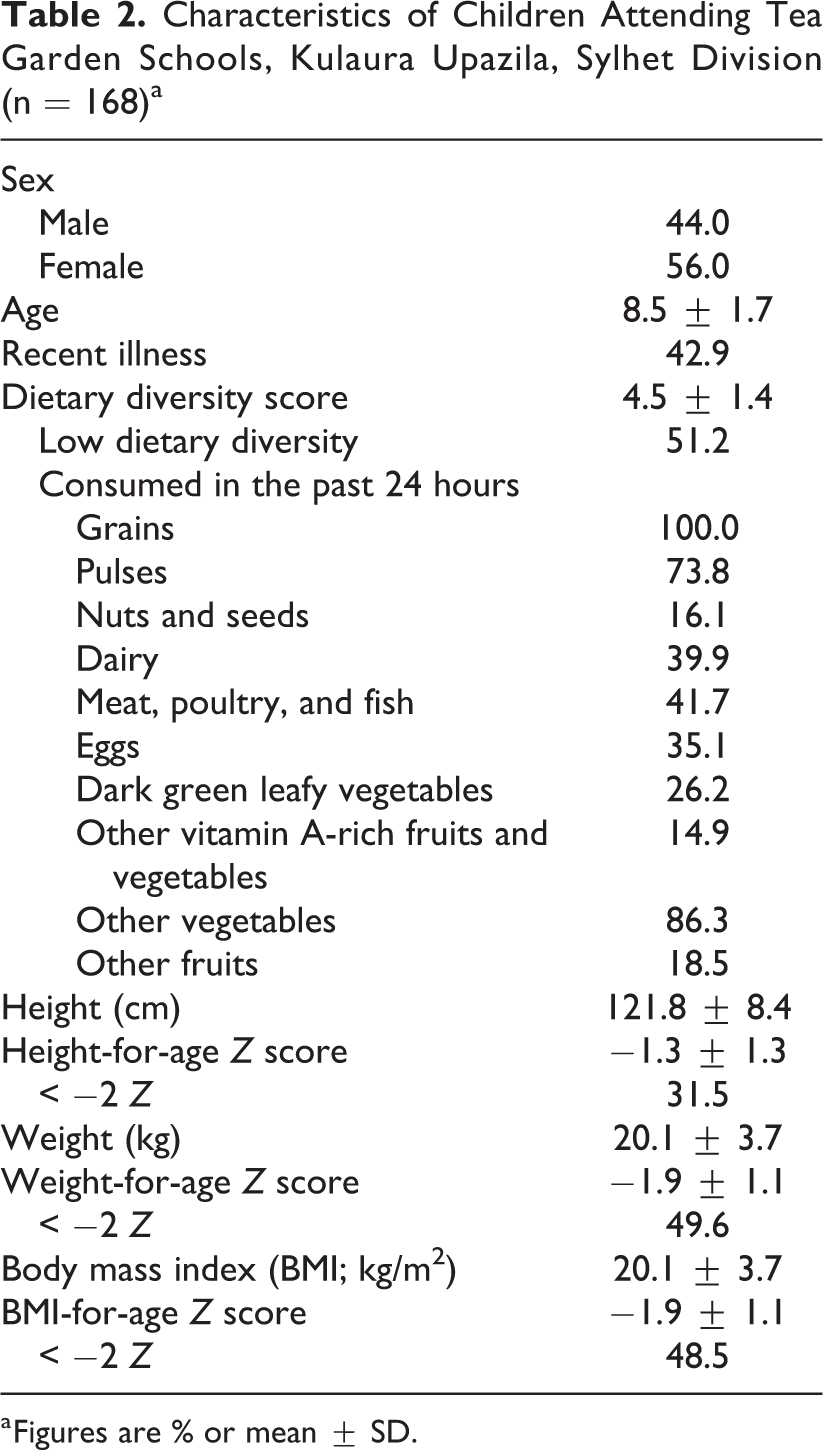
a Figures are % or mean ± SD.
Nutrient and Inflammation Status Measures and Indicators From Children Attending Tea Garden Schools, Kulaura Upazila, Sylhet Division (n = 168).a
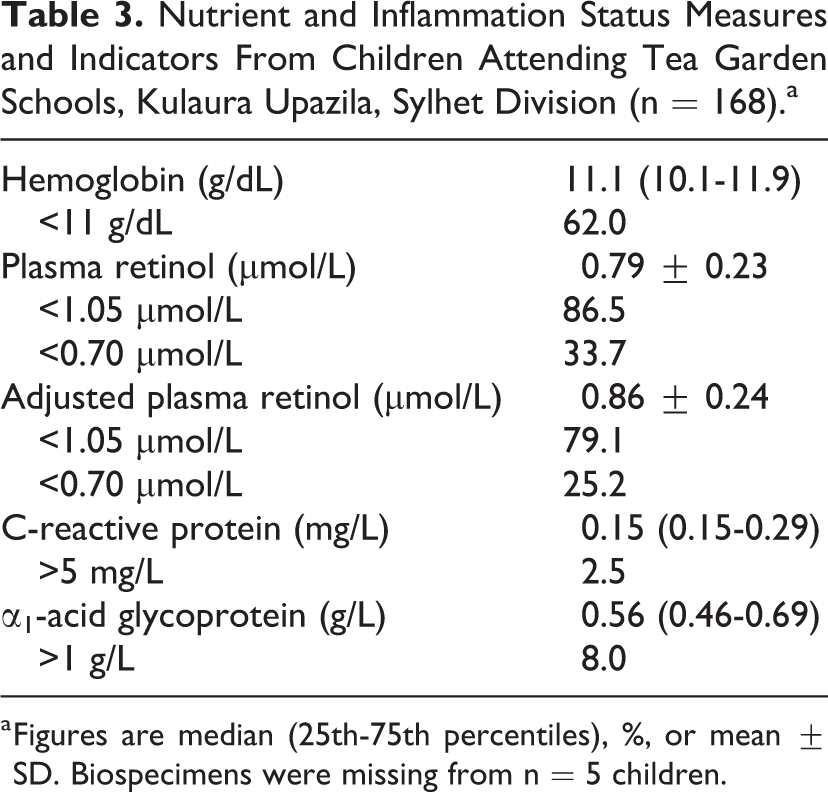
a Figures are median (25th-75th percentiles), %, or mean ± SD. Biospecimens were missing from n = 5 children.
Discussion
Despite progress toward global development goals in Bangladesh, undernutrition remains an important public health concern, with implications for child health, growth, development, and long-term disease risk. Certain hard-to-reach population subgroups may face an elevated risk due to geographic location or marginalized status. Our results from this school-age population from tea estates in Kulaura Upazila, Sylhet Division, are consistent with historical data pointing to high levels of food insecurity and limited dietary diversity. 5 There are limited comparison data on anthropometric indicators for this age-group. Our data suggest a lower prevalence of stunting (31.5%) compared to national- or Sylhet Division-level estimates for children under the age of 5, which were 36.1% and 49.5%, respectively. 3 However, this lower prevalence would be consistent with evidence of catch-up growth during the school-age years, where there is some degree of shifting between height categories. 14 In contrast, our data indicate a notably higher prevalence of anemia in this population than has been reported previously for school-age children nationally: 62% versus 19%. 15
As our survey was intended to inform site selection for a provitamin A carotenoid biofortified rice intervention trial, we had a particular interest in studying vitamin A deficiency. Here, the vast majority of children (∼85%) had marginal vitamin A status and between 25% and 35% could be classified as deficient, depending on adjustment for inflammation. This exceeded the ∼20% estimate reported from the 2011-2012 National Micronutrient Survey, 16 although unadjusted national estimates were unavailable and adjustment methods differed. While we purposively selected schools that were not served by micronutrient-fortified biscuit programs, children may have had access to fortified oil. However, analysis of a limited number of oil samples collected in the community also indicated that these did not meet target levels for vitamin A (unpublished data). Our study indicates that the tea estates of Sylhet would be an appropriate setting to test a vitamin A deficiency control intervention. Given the limited dietary diversity, an intervention to improve usual provitamin A intakes through staple crops shows promise. Also promising in this context is the limited proportion of children with elevated inflammatory proteins in comparison to prior research on biofortification in sub-Saharan Africa. 17 This suggests that observed hyporetinolemia in this setting is likely driven more by diet than inflammatory stimuli, such that a dietary intervention may prove more efficacious than in Africa.
The present study focused on a high-risk population in Bangladesh, where more granular data will be critical as the country seeks to accelerate progress toward global development goals for nutrition. While providing data on a unique population, our study was limited in its scope. Importantly, our sample is unlikely to be representative of children living on tea estates in the greater Sylhet Division. In Sylhet, we might expect nutritional status to be poorer on the more rural tea estates of Kulaura, for example, than in neighboring Sreemangal Upazila. Overall, food insecurity and limited dietary diversity remain major concerns in pockets of Bangladesh, placing children at high risk of undernutrition—including a persistent level of vitamin A deficiency in areas where other strategies may not yet reach. Going forward, it will be necessary to monitor status and improve program targeting to ensure that these high-risk population subgroups are protected from the consequences of undernutrition. Improving on existing strategies will be key, including strengthening fortification programs. The introduction of new strategies to improve diet and reduce disease burden should also be considered and tested to protect those at greatest risk.
Footnotes
Authors’ Note
All authors contributed to the study design and implementation. J.W. analyzed the data. M.S.I. and A.C.P. wrote the first draft. All authors interpreted the data and reviewed and contributed to the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Bill and Melinda Gates Foundation through a grant to Helen Keller International. Additional support was provided by the Sight and Life Global Nutrition Research Institute at Johns Hopkins University.