
Abstract
Background:
A better understanding of nutrient intakes and predicting factors will help in designing more effective programs that address the nutrition requirements of pastoral children.
Methods:
Dietary diversity score (DDS) and amounts of food items consumed were recorded for 538 children aged 6 to 59 months from August to October 2015. The nutrient contents per 100 grams of foods consumed by children were calculated. Median energy and nutrient intakes of children were calculated and compared with the World Health Organization (WHO) recommended nutrient intakes (RNI). The effects of various factors on the median energy adequacy ratio (EAR) and on nutrient adequacy ratio (NAR) were analyzed using logistic regression.
Results:
Children had low DDS (2.7) with diets dominated by dairy and cereal preparations. Thus, only a few children received the minimum DDS (11.7%) and minimum acceptable diet (5%). Most of the children had low intakes of energy, vitamins (C, B, A, folic acid), iron, and zinc. Autonomy of mothers in decision-making, nonpastoral incomes, crop cultivation, and keeping diverse livestock species had positive effects on nutrient intakes. Children living in villages closer to markets and those aged 6 to 23 months had better NAR than others. The median EAR was higher for children aged 6 to 23 months, when households possessing more animal species and engaged in crop cultivation compared to others.
Conclusion:
Study children had lower DDS than WHO standards and intakes of several micronutrients were inadequate. Variables associated with median EAR and NAR point to those in need of improvement.
Introduction
Optimal infant and young children feeding practices and enhancing adequate nutrition are vitally important for ensuring the survival, growth, and development of children to their potential. The critically vulnerable time to undernutrition coincides with the introduction of complementary feeding, from the age of 6 months onward when children require diets that supplement breast milk and provide adequate nutrients to meet rapid growth. 1 However, most complementary diets in sub-Saharan Africa are likely to be inadequate quantity and lower nutritional quality, resulting in micronutrient deficiencies and in growth faltering, which can be further worsened by prevailing poor sanitation and hygiene. 2
Pastoralists and their children have been generally considered to have better access to and consumption of foods of animal origin compared to farming communities. 3,4 In particular, dairy is the major animal source foods in the system that provides the children with a good source of energy, protein, other micronutrients, and bioactive substances with growth-promoting abilities. 5 High consumption of dairy, by nearly all individuals followed by cereals has been reported for adults 6,7 and their children from pastoral areas. 8,9 But milk consumption depends on its availability which is prone to dry seasonal short supply, selling for cash income, and the increasing tendency of cereal intakes. Additionally, the unsuitability of the arid environments for crop cultivation and for growing vegetables and fruits might limit the dietary diversity of pastoralists. Recent accounts show that the Borana pastoral system of southern Ethiopia is undergoing various alterations including environmental and socioeconomic changes, the impacts of which on dietary intake are yet unknown. 7
Most East African pastoral communities (as well as many others) are facing climatic and ecological changes, and undergoing rapid socioeconomic transformations that result in livelihood shifts toward agropastoral or settled farming. 7,10,11 In the Borana community, a growing trend towards opportunistic crop cultivation and nonpastoral income-generating activities has have been reported as a means of poverty alleviation and in response to increased climate variability and recurrent droughts. 7,10,12 Additionally, the tendency of trading dairy products for food grains and other consumable items may also speed the rate of dietary transition toward cereal-dominated diets. Under cereal dominated diets, children tend to consume diets that are not only low in protein, calcium, and other critical micronutrients but also contain compounds (eg, phytate) that reduce the bioavailability of iron and zinc from other food sources. 2 Case studies comparing the nutritional status of children in pastoral versus settled communities have also shown the negative impacts of livelihood shifts in Kenya 4 and Nigeria. 13 Alternatively, increased involvements in agropastoralism (cropping) and nonpastoral (off-farm) income activities are expected to increase dietary diversity and nutrient intakes. Thus, investigating the extent of dietary intake and nutritional status of pastoral children facing changes is vitally important for planning nutrition intervention programs.
Dietary diversity score (DDS) of 7 food groups has been recommended as a proxy indicator to assess the nutrient intake of infants and young children 14 (though it has recently been modified to 8 food groups). Dietary diversity score has been reported to be an important predictor of mean adequacy ratio (MAR) as well as underweight and stunting in children. 15 -18 Minimum DDS (proportion of children who received at least 4 or more out of the 7 food groups) is also commonly used as an infant and young child feeding (IYCF) indicator. 14 Overall, information on the dietary intake and nutritional status of infants and children in pastoral areas of Ethiopia is very scarce. The adequacy of energy and nutrients intakes from consumed food items could vary considerably with socioeconomic variables and environmental factors. Understanding how a dietary intake could vary with socioeconomic variables will help in designing an intervention program that addresses the nutrition requirements of children in pastoral areas. Accordingly, this study was intended to assess the dietary intake, energy and nutritional adequacy, and associated factors among infants and young children in the Borana pastoral system of southern Ethiopia.
Methodology
Study Design and Sampling
A Community based cross-sectional study of dietary diversity and milk intakes was conducted in Borana zone, Oromia region, southern Ethiopia, between August and October 2015. The Borana area is characterized by arid and semiarid conditions and a pastoral or agropastoral production system. A total of 6 pastoral associations (PAs), out of 18 PAs in Yabelo district, were randomly selected. Pastoral association is the lowest administrative unit (with about 200 households) that composed of clustered villages or pastoral encampments (locally called Olla) having 10 to 20 households. Disparities in livelihood sources such as major livestock species herded (cattle or camel based livelihood) were also taken into account in PA selection. Following the sampling of 50% of villages per PA, all eligible households in a village who had at least one child within the age range of 6 to 59 months were included. Every mother of a selected household and her one or more children were recruited for the study. Exclusion criteria were children with physical disability or abnormalities, mental impairment, edematous conditions, evidence of chronic disease, and those with signs of fever, vomiting, diarrhea, and cough.
Sample size was estimated using a presumed population proportion of minimum meal frequency (42%) report of the Ethiopian demographic and health survey, 19 95% confidence level, the marginal error of 5%, and design effect (1.5 times) which gave a total of 561 children. The sample size was stratified into 2 major livelihoods, that is, 70% cattle and 30% camel herding groups. Finally, we able to sample a total of 538 children (6-59 months) with complete information from 406 households. Thirteen children with incomplete data (n = 8) or with physical abnormalities and health problems (n = 5) were not included in the final data set and analyses.
Data Collection
Before the actual survey, a pretesting of the questionnaires was carried on limited number participants (ie, using 7 mothers whose data were not included in the study) for further improvements. Three experienced data collectors with a diploma in clinical nursing were recruited and trained for 2 days using an interactive 24-hour recall technique validated for use in developing countries. 20 The questionnaire survey focused on collecting socioeconomic variables, household characteristics, maternal and child characteristics, IYCF practices and child health care, and access to safe water and sanitary facilities. The interviews also included questions on perceptions of mothers on changing trends in milk production, consumption and sale, on child feeding practices, dietary intake, and on growth and health status of children.
Mothers or primary caregivers were asked to list and qualitatively describe all the food items consumed by their children during the previous 24 hours according to the 7 food groups model of World Health Organization (WHO). 14 Mothers or caregivers were requested to provide separate information for each child in cases of multiple children per mother. Recipes and ingredients used to prepare the food were recorded and the portion size of each food item consumed by a child was estimated. Household utensils were used to estimate the portion size of consumes food items. Then actual food samples and dairy products collected from villages were weighed using SF-400 digital kitchen scale to estimate the amount consumed. Milk, other liquid, and semisolid food preparations are often served in locally used cups known as “Koki” (about 350 mL) and this amount was converted into mL or grams. Milk consumed in the form of tea (20-25% milk) was quantified by estimating the proportion of milk to water in the household tea and then in the amount consumed by children (in cups or glasses).
Weight and height measurements of children wearing light clothing and no shoes were recorded according to WHO guidelines. 14 Weights were taken at standing or hanging positions using Seca scales (Seca GmbH) graduated by 0.1 kg. Heights (standing) or lengths (lying for children <24 months) in centimeters were measured with a measuring board graduated by 0.1 cm. Data on age of a child (in months) was obtained either from birth certificates or the child’s vaccination card. For those without records, the mother’s recall was used, assisted by referring to the local time calendar, local events, seasons, and months to help determine the birth date.
Estimation of Nutrient Intakes
The nutrient contents per 100 grams of food items and recipes consumed by children were calculated using the Food Composition Table of Ethiopia. 21,22 Missing values were estimated from Nutrisurvey2007 software using the Kenyan food database for diets common in northern Kenya and southern Ethiopia. The energy and nutrient intakes from complementary foods were calculated for breastfed children separately and compared with estimated needs from complementary foods assuming the daily average breast milk intake (equivalent to 533 mL/d) and composition as described by Dewey and Brown. 23 The energy and nutrient intakes of nonbreastfed children were compared with the WHO/Food and Agriculture Organization of the United Nations recommended nutrient intake (RNI). 24,25 Contributions (%) of various food groups to the total energy and nutrient intakes were also estimated.
The adequacy of energy intake was assessed as the ratio of the actual energy intake per day to the estimated energy requirement, from which the median energy adequacy ratio (EAR) was estimated. Similarly, the adequacy of a nutrient was assessed by estimating the nutrient adequacy ratio (NAR) for each nutrient as the ratio of the actual intake of the nutrient per day to the RNI. Then median, first and third quartiles of each nutrient were estimated for different age groups of the study children. Finally, the median of nutrient adequacy ratio was calculated for each child by summing of all 10 NARs and estimating their median as 50th percentile in addition to their first and third quartiles.
Data Analysis
Different socioeconomic variables, perception of mothers, dietary diversity, meal frequency, milk frequency were descriptively summarized as a proportion or mean. The contribution of different food groups to energy and nutrient intakes was presented as percentage. The median and interquartile range (first and third quartiles) of energy and nutrient intakes were compared with recommended intakes, and summarized by age groups. The median EAR and median NAR were used to create binary data of below median (intake = 0) or above median intake (intake = 1). Possible cluster effect of multiple children per mother (per household) was assessed using mixed effect logistic regression model, but there was no significant correction within a household. Then the associations of various explanatory variables with median EAR and median NAR of study children were analyzed using logistic regression with stepwise backward selection procedure of Stata version 14.2.
Ethical Considerations
Following the submission of proposal and questionnaire formats, ethical approval was obtained from the Ethical Committee of the Health Bureau of South Regional State. Permission was also received from the Borana zone health department. Informed consent was obtained from each mother or caretaker of children after informing them about the purpose, benefit, and confidentiality of the information. Participants were told that their participation in the study is voluntary, and they can withdraw at any time. They were also given the opportunity to ask study-related questions.
Results
Sociodemographics and Perceptions
General characteristics of households (n = 406) and study children (n = 538) are summarized in Table 1. The study households are mainly dependent on livestock production for their livelihoods in addition to crop cultivation (88%) and nonpastoral income activities (25%) such as petty trading, labor, and sale of bush products. The average family size was 7 persons. In polygamous families (10%), spouses often live in separate houses (sometimes with separate herds), and only one of them had one or more under-5 children. Over half of the households had a toilet and mobile phone and 35% of them owned a radio.
General Characteristics of Study Households (n = 406), Children (n = 538), and Mothers.
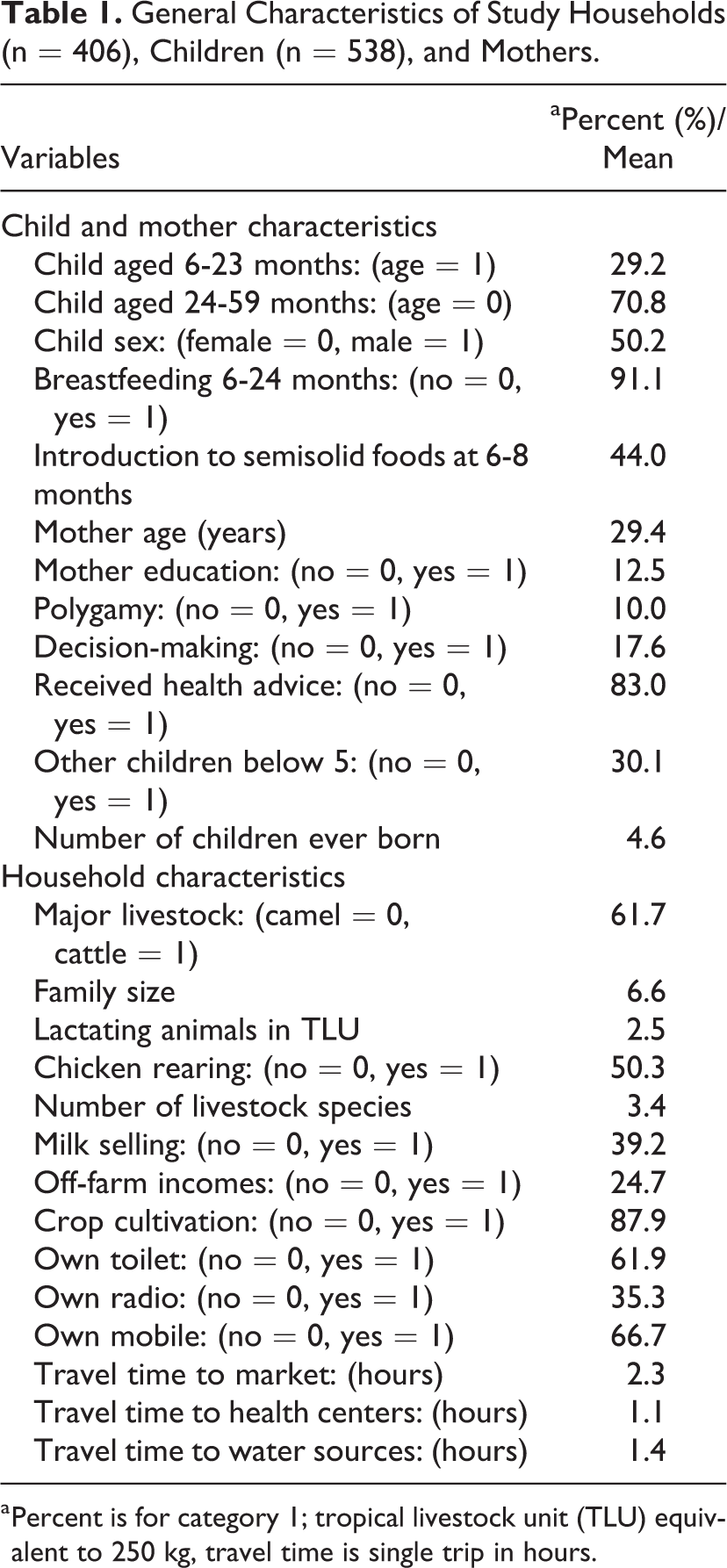
a Percent is for category 1; tropical livestock unit (TLU) equivalent to 250 kg, travel time is single trip in hours.
The study children had a sex ratio of nearly 1:1 and average age of 32.7 months. All children aged 6 to 11 months (n = 57) and 86% of those in the age range of 12 to 23 months were breastfeeding. Introduction to semisolid food was mostly initiated at a later age (8 months and above). Low level of literacy (12%) and participation in decision-making on household resources (18%) were observed among mothers. Most mothers (83%) were visited by health extension agents and received advice on general hygienic and sanitary practices as well as on child feeding practices.
Feeding Practices, Energy and Nutrient Intakes
Perception of mothers regarding trends of dietary condition of children showed that the majority of them (90%) perceived an ongoing decline in animal source food intakes and increased consumption of cereal-based foods (95%). More than half of them believed that food variety is increasing (57%). They also felt that these changes had negative effects on child growth and health outcomes. Dairy products of different animal species remained the major animal source foods (Table 2). The most commonly consumed forms were fresh milk (43%) followed by boiled milk (31%) and milk boiled with tea (22%). Very few children also consumed milk boiled with unhulled roasted coffee locally known as Bunakala. Cattle milk accounted for a higher proportion (83%) of dairy consumption.
Proportions of Consumed Dairy Products by Different Animal Species.
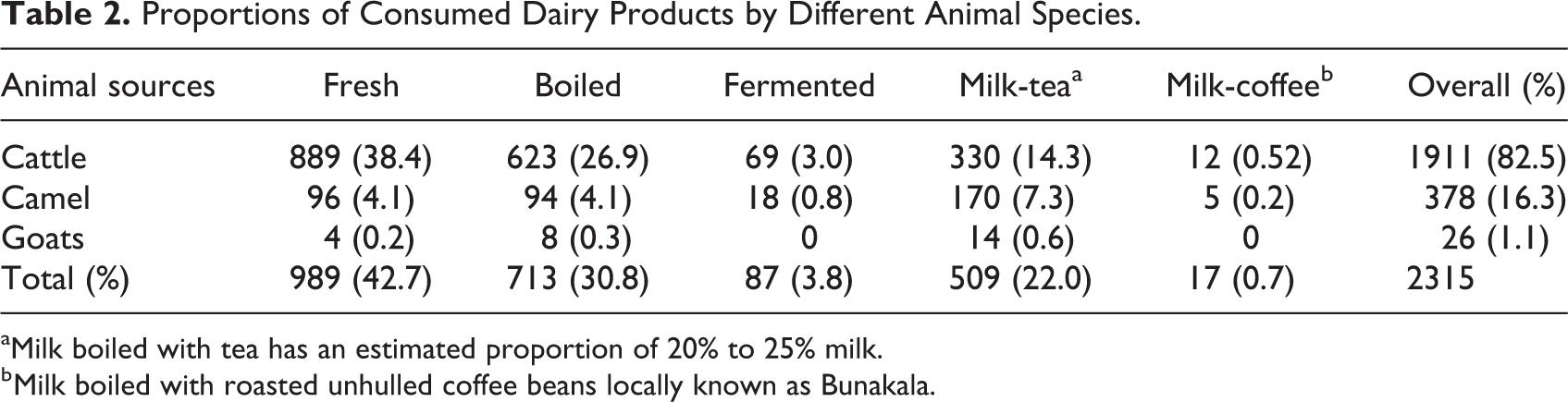
aMilk boiled with tea has an estimated proportion of 20% to 25% milk.
b Milk boiled with roasted unhulled coffee beans locally known as Bunakala.
Table 3 presents percentage of children by food group consumption. Nearly all children consumed dairy products with cereals (83.6%) and legumes (53.5%) also widely consumed. Very few children consumed other animal source foods such as meat and eggs while none of them ate fish or chicken. Vitamin A rich fruits and vegetables were among the least consumed items. The Ethiopian kale (Brassica carinata), which is cultivated with cereal crops, was the most commonly consumed vegetable.
Proportions of Infants and Young Children by Food Group Consumption, DDS, Meal, and Milk Frequency by Age Groups.
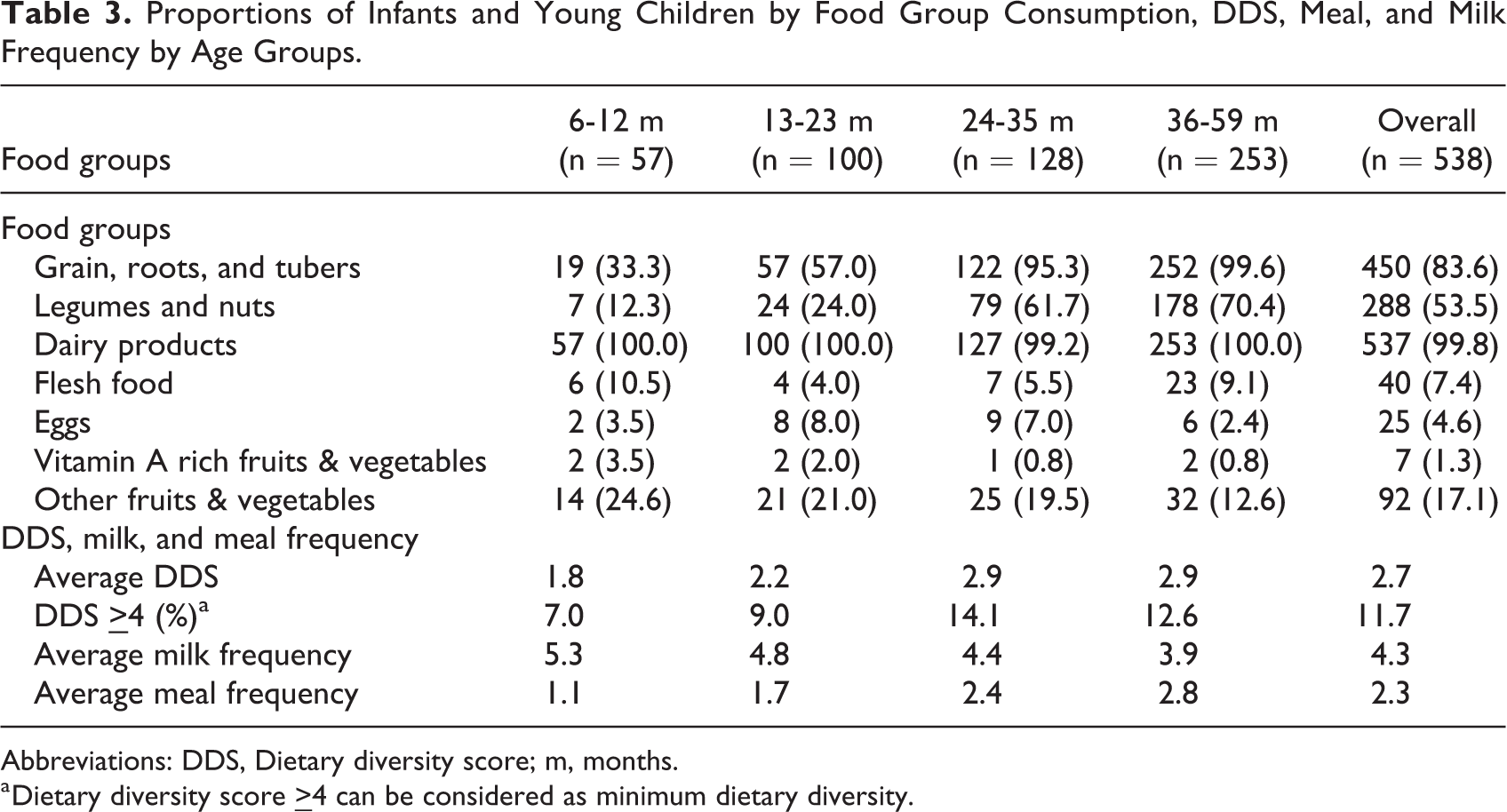
Abbreviations: DDS, Dietary diversity score; m, months.
a Dietary diversity score
A lower dietary diversity score (2.7) than the recommended 4 food groups was observed in the study children. Thus, very few children received the minimum dietary diversity (11.7%) and minimum acceptable diet (5%). Dietary diversity score was found to be lower in age groups of 6 to 11 months (1.8 DDS) and 12 to 23 months (2.2) compared to those above 24 months (2.9 DDS) while milk frequency tended to decreased with age.
Dairy products have contributed more than 50% to energy, protein, calcium, zinc, and vitamins A, B1, B2, and C intake. Cereals and tubers were the principal contributor for iron (54%) and folic acid (52%) intakes. Likewise, over 25% of energy, vitamin B6, and vitamin C were contributed by cereals and tubers. Legumes also contributed to
Contributions of Different Food Groups to Energy and Nutrient Intakes (%).
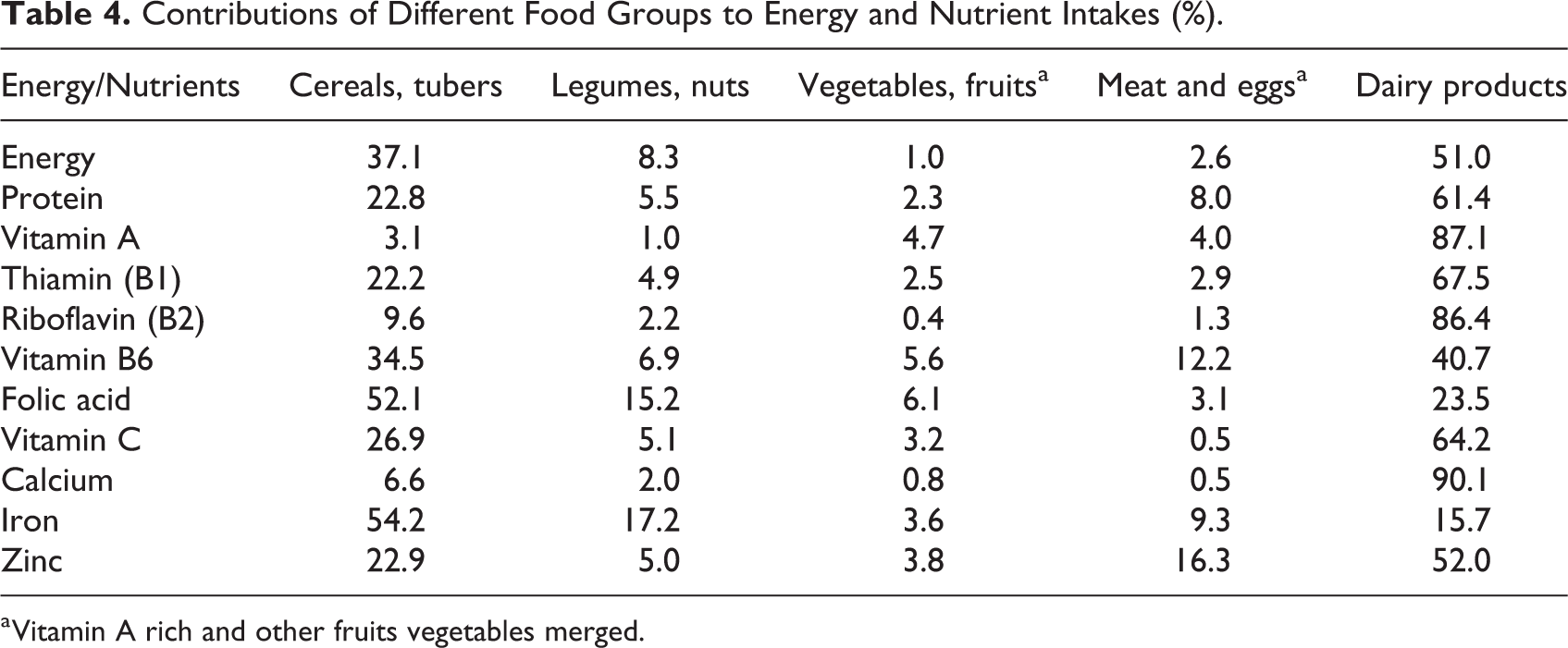
a Vitamin A rich and other fruits vegetables merged.
Table 5 presents a summary of median energy and selected nutrients intakes of infants and young children in comparison to estimated needs. Energy intakes were adequate for breastfed infants and young children (6-23 months), but were lower than the estimated needs for children in the age range of 24to 59 months. Similarly, median intakes of vitamin A and thiamin (B1) met the estimated needs for breastfed children while those above 23 months had lower intakes. All age groups had sufficient intakes of protein, calcium, vitamin B6, and riboflavin (B2). However, median intakes of zinc, iron, folic acid, and vitamin C were below the estimated needs (RNI) for all age groups.
Median (Q1, Q3) Energy and Selected Nutrients Intake of Infants and Young Children in Comparison With Estimated Needs From Consumed Foods.
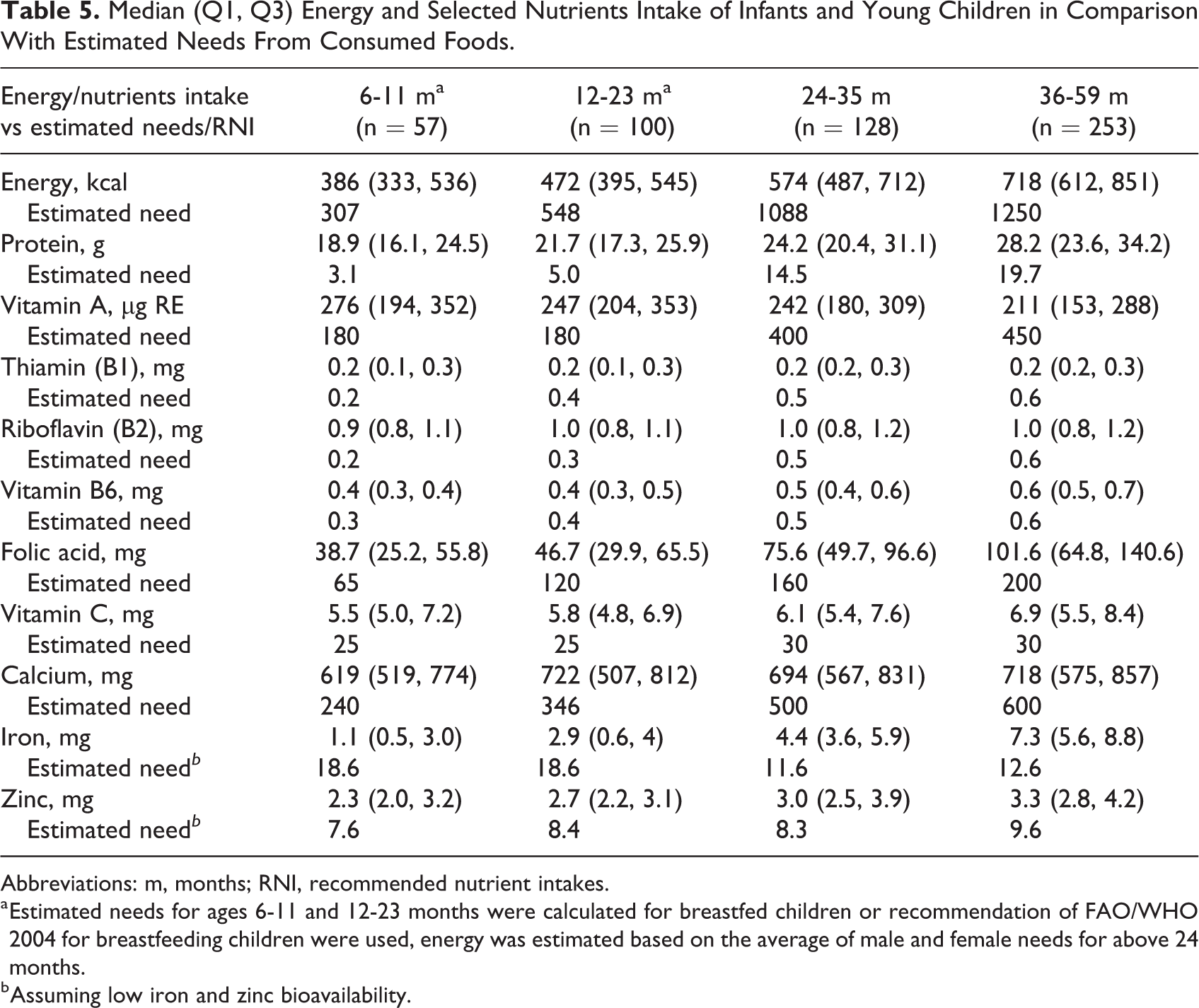
Abbreviations: m, months; RNI, recommended nutrient intakes.
a Estimated needs for ages 6-11 and 12-23 months were calculated for breastfed children or recommendation of FAO/WHO 2004 for breastfeeding children were used, energy was estimated based on the average of male and female needs for above 24 months.
b Assuming low iron and zinc bioavailability.
Overall, the median energy adequacy ratio showed better energy intakes among children aged 6 to 11 months (100%) and 12 to 23 months (86%) compared to older kids 24 to 36 months (52.8%) and 36 to 59 months (57.4%). The median of nutrient adequacy ratio (NAR) also decreased with increasing age (Table 6).
Median Energy Adequacy Ratio (EAR) and Median Nutrient Adequacy Ratio (NAR), and Their First (Q1) and Third Quartiles (Q3) by Age Groups.
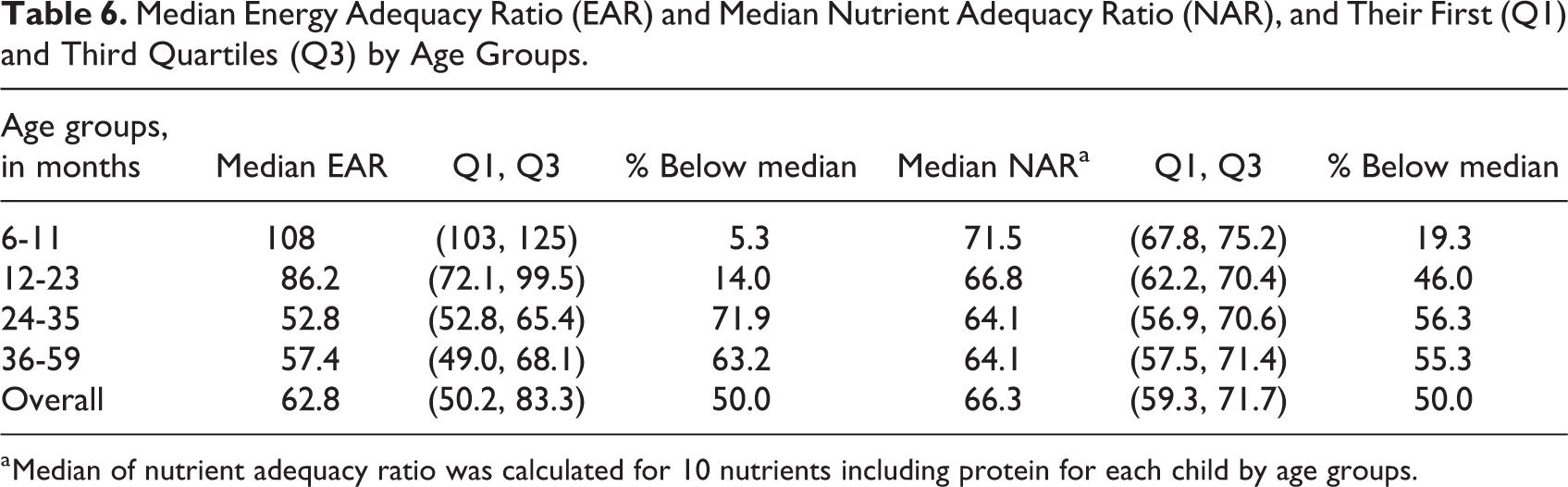
a Median of nutrient adequacy ratio was calculated for 10 nutrients including protein for each child by age groups.
Various socioeconomic variables were found to affect the median energy and nutrient adequacy ratios of study children (Table 7). Children from households that engaged in crop cultivations or off-farm income activities kept more diverse livestock species or whose mothers could decide on some resources were 2.8, 2.0, 1.3, and 2.0 times more likely to have above the median nutrient adequacy ratios compared to their counterparts. Conversely, median nutrient intakes were found to decrease with mother education and distance to markets. Being in the age-group of 6 to 23 months increased the likelihood of being above the median 2.4 times more for NAR and 18.6 times more EAR. Similarly, median energy intakes were 1.3, 1.9, and 1.5 times higher when households keep more livestock species, cultivate crops, and have mobile phone compared to other groups.
Factors Associated With Median Energy Adequacy Ratio and Nutrient Adequacy Ratio of Infants and Young Children.
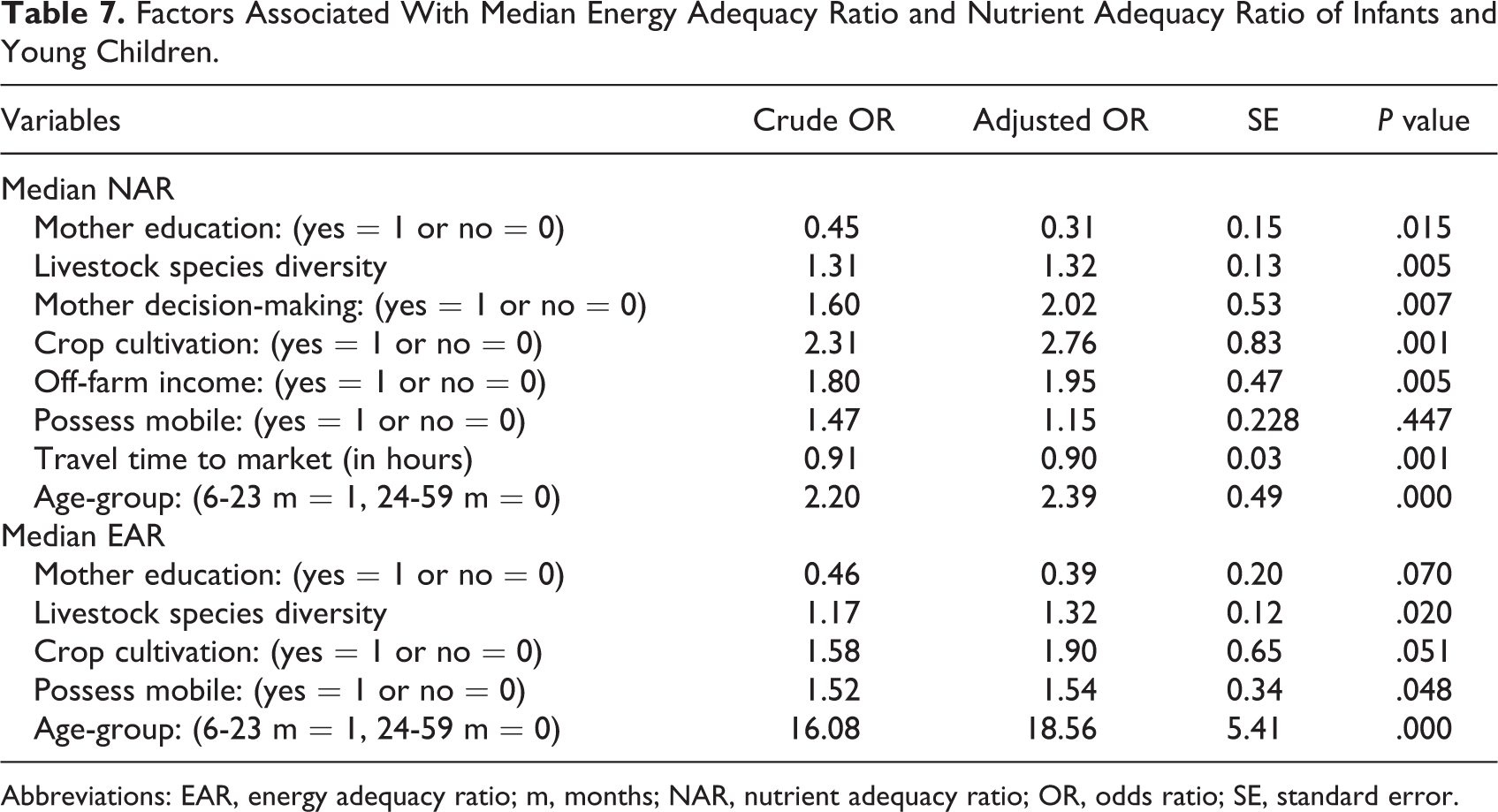
Abbreviations: EAR, energy adequacy ratio; m, months; NAR, nutrient adequacy ratio; OR, odds ratio; SE, standard error.
Discussion
Most of the study children consumed a narrow range of food groups, primarily cereal preparations with beans, and dairy products that help explain observed lower proportion of minimum dietary diversity and acceptable diets compared to the minimum standards of WHO. 14 Figures of Demographic and Health Surveys of Ethiopia 19 also showed remarkably low minimum dietary diversity (4.3%) and acceptable diets (4.0%) for countrywide children. Similar patterns of low DDS (< 3), very low intake of animal source foods (non-dairy), and vitamin A-rich fruits and vegetables has been reported from pastoral 8 and non-pastoral areas of Ethiopia. 26,27 Though pastoral societies derive a large share of their foods and livelihoods from their livestock, consumption of animal source foods was much less than expected (7.4% meat and 4.6% eggs). Animals are rarely slaughtered for meat consumption (other than for ceremonial purposes) and buying meat from butchery is also uncommon, resulting in low intake of meat. Existing tradition or unfamiliarity with some food items such as chicken, eggs, and fish might have restricted their consumption in the area. It worth noting that egg consumption by some children can be considered as a positive step in dietary transition, and calls for further awareness about this food source. As nearly half of the households’ rear backyard chicken mainly for egg selling, promoting consumption of chickens and eggs may improve the dietary quality of children in the area.
Similar to our findings, low dietary diversity with dairy and cereals being the main food groups have been reported from other pastoral areas of Ethiopia 6,8,28 and Kenya. 9 Hence, the observed higher contribution of dairy products and cereals to energy and other nutrient intakes is not unexpected and supports previous findings from Ethiopia 8 and Kenya. 9 In general, the low dietary diversity observed in our study can be linked to the limited access (both physically and economically) of pastoralists to a variety of food groups, lack suitable environment for growing crops, fruit and vegetables, unfamiliarity with some food items (eg, chicken, eggs) and increasing climate variability and related food insecurity.
Observed adequacy of energy, vitamin A and thiamin (B1) in breastfed children, as well as optimum intakes of protein, calcium, vitamin B6, and riboflavin (B2) in all age groups might be attributed to a high intake of dairy products, which is a good sources of protein, vitamins A, thiamin, riboflavin, and calcium. 29 Observed continued breastfeeding by 86% of the children (12-23 months) could contribute better intake of these nutrients as reported by authors who observed that children with continued breastfeeding had better energy and nutrient intakes compared to their counterparts. 8,30 Suboptimal intakes of folic acid and vitamin C as well as zinc and iron for all age groups, similar to a previous finding, 8 can be attributable to very low consumption of meat and eggs, fruits, and vegetables. Though fresh camel milk is assumed to be a good source of vitamin C, dairy products were mainly from cattle and this effect could not be observed in this study. Inadequate intakes of various micronutrients reported from elsewhere varied considerably depending on agroecology, dietary patterns, and types of food groups consumed. For instance, a study from the agrarian area of Ethiopia reported low intakes of zinc, vitamin A, and vitamin C, but not of iron. 30 Other authors also reported low intakes of vitamin A and vitamin C from Mali, 18 iron and zinc from South Africa, 17 and low intakes of folic acid and zinc from the Philippine. 31
Besides their poor contents of some nutrients (eg, iron and zinc), diets and beverages consumed by children (eg, high intakes of cereals and cattle milk) also contain compounds that may interfere with the absorption of those scarce nutrients. For instance, cow milk is not only deficient in iron but also rich in casein protein that interferes with the absorption of iron and zinc, and reduces their bioavailability. 32,33 A literature review 2 also showed that diets of infants and young children in sub-Saharan Africa is dominated by cereals and tubers, which are not only poor in nutrient contents but also contain compounds such as phytate that reduce the bioavailability of micronutrients. The prevailing consumption of tea and coffee with milk, which is assumed to contain polyphenolic compounds could also inhibit the absorption of iron and zinc, 33 worsening the existing inadequacy of these micronutrients.
The positive effects of crop cultivation can be related to increased availability of own sourced food and reduced pressure on livestock off-take for food expenditure. 7 Opportunistic crop cultivations (in the season with good rains) provide yields of cereals, beans, and some vegetables (eg, local kales) that can contribute to improved dietary diversity as well as nutrient intakes. In a study from Mali, 16 the number of crops cultivated was found to have significant effects on the MAR of individuals. Another study from Ethiopia also demonstrated that growing vegetables and ownership livestock had significantly increased the dietary diversity and nutritional intake of children. 27 This suggests that the initiation of nutrition-sensitive agriculture might be essential for the improvement of children’s nutritional quality. Ownership of more diverse livestock species also increases food supply (eg, milk from different ruminants) besides increasing cash income by offering more options for off-take that ultimately improve access to food and dietary intakes. 7 Similarly, existing nonpastoral income sources can also improve household incomes and access to foods with a large share of cereals, legumes, tubers, and vegetables coming from local markets.
The observed significant effect of access to market places on the median nutrient adequacy ratio also reflects the importance of marketing own produce and buying food items in improving dietary intake and nutritional status. Stifel and Minten 34 observed higher per capita consumption expenditures and relatively more diverse diets among households residing closer to market compared to those in remote areas where transaction costs and terms of trade disfavor them. A study in Malawi also identified access to markets for buying food and selling farm produce as an imperative determinant of dietary diversity. 35 This suggests that remoteness may force households to sell livestock and their products at a lower price in villages and so spend less on food items. In pastoral areas, long-distance walks to market destination require endurance and strength that discourage women from frequently travel to such far-off markets to purchase food items. Additionally, households in close proximity to market might have a better opportunity for nonpastoral income sources and better access to information. Among the factors considered as sources of information (eg, visit by health extension workers, ownership of radio and mobile) for children feeding practices and for nutrition knowledge, possession of mobile phone had a significant positive association with energy intake but did not affect nutrient adequacy ratio. A study in Nigeria 36 also reported a significant positive effect of mobile phone possession on the dietary diversity of preschool children, reflecting the role of communication tools and information sharing in remote pastoral areas.
Though men are the major decision makers on household resources in a pastoral community, few mothers reported having some autonomy in deciding on resources (except for cattle and camel selling) which had a positive effect on the nutrient intakes of their children. Our finding supports previous studies from India 37 and Bangladesh 38 that reported positive effects of women’s autonomy on the nutritional status of children. This observation reflects the general notion that women spend more money on acquiring food items to ensure the dietary needs of their children and family. Children from literate mothers had a significantly lower median NAR compared to those from illiterate ones contrary to our expectations and reports elsewhere. For example, a study in Kenya 39 showed that mother’s education was associated with improved nutritional status of children in the slums of Nairobi. But Dangura and Gebremedhin 27 did not observe a significant effect of mother literacy on dietary intakes of rural children in Ethiopia. The impact of mother’s education on a child’s nutritional status varies with settings (may be stronger in urban than rural areas) and effects increase with education levels. In our study, most of the mothers with education were young mothers who attended mainly elementary school and also own less livestock wealth (resources), which may explain our findings.
Higher energy and nutrient intakes among children aged 6 to 23 months compared 24 to 59 months could be explained by the termination of breastfeeding and by lower dietary intake during the period of complementary feeding given the prevailing poor dietary diversity and nutritional quality of complementary foods. Additionally, the lower intake of energy and micronutrients in the older children could be related to the reduction of dairy consumption coupled with the increased nutritional requirement.
Conclusion
Our results demonstrate that the diets of the study children were below the minimum WHO standards. Cereals and dairy products remain integral parts of their diets and contributed to larger proportions of energy, protein, and other micronutrients intake. The diets of study children were generally inadequate in for several micronutrients of which, vitamins B1 and C and iron are critical ones. Important positive predictors of median energy and nutrient adequacy ratio were autonomy of mothers in decision-making, off-farm incomes, crop cultivation, livestock species diversity, and residing closer to markets; and these predictors need to be considered when addressing dietary requirements.
Footnotes
Authors’ Note
B.M. performed study design, data acquisition and analysis, drafting and revising the manuscript, and interpretation of results. A.H. and U.K. were participated in designing the study, drafting and revising the manuscript, and interpretation of findings. All authors read and approved the final manuscript.
Acknowledgments
Authors are thankful to mothers and caretakers of study children, staffs of Yabelo health center, and IMMANA coordinating team whose supports were extremely valuable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of IMMANA fellowship research on milk consumption, nutrition, and health in southern Ethiopia, which was funded by UKAID from the UK government. This study was funded by UKAID in collaboration with Tufts University.