
Abstract
The Institute of Nutrition of Central America and Panama (INCAP) longitudinal study of 1969 to 1977 was a community randomized trial in which 2 pairs of matched villages received either a protein-rich gruel (atole) or a nonprotein, low-energy drink (fresco). Both contained equal amounts of micronutrients by volume. I review the history and design of the study and impact on dietary intakes and physical growth. The design dates from the 1960s when protein was seen as the main dietary deficiency. During the 1970s, emphasis shifted to energy deficiency and this influenced early analyses. Energy from the 2 drinks during pregnancy was associated with improved birthweights and whether protein was also provided along with energy appeared to make no difference. These analyses, observational in nature, were possible because there was substantial overlap in energy intakes from the supplements during pregnancy across village types. In children, analyses initially focused on energy but eventually relied on the original experimental design. Exposure to the atole compared to fresco was associated with improved physical growth at 3 years of age but not from 3 to 7 years. Consumption of the fresco in the first 3 years of life was low such that there was little overlap in energy intakes from the supplements, not allowing for the type of analyses done for pregnancy. Diets in atole villages were greater from 15 to 36 months in protein, energy, and micronutrients, making attribution of impact on growth to a specific nutrient impossible. The atole improved linear growth, arm, and calf circumferences at 3 years but not skinfold thicknesses.
Introduction
The Institute of Nutrition of Central America and Panama (INCAP) carried out several longitudinal studies in the 60s and 70s 1 but none is as well-known and has contributed more to knowledge about human development than The INCAP Longitudinal Study (1969-1977). It was a community-randomized trial of a nutrition intervention that was delivered effectively as intended; its primary outcome was child development but it also included growth and related measures as secondary outcomes. The rigor with which it was designed and implemented remains state of the art today. The study is among the best known in nutrition because several follow-up studies have been and are being carried out. No other study has evaluated the impact of an early childhood nutrition intervention on such a wide array of adult dimensions such as stature, schooling, intelligence, work productivity, risk of chronic diseases, and mental health. The former participants of the study were between 42 and 57 years of age in 2019.
In this introductory article, I review the main features of the history and design of the study and review participation in the study and impact of the intervention in childhood on dietary intakes, birthweight, and physical growth. A different article reviews results for child development. 2 I also show how the perception of the relative importance of protein and energy deficits in the diets of low-income countries shaped the design and the analytic plans of the study.
History of the Design
The study was designed in the late 1960s when the principal deficiency in the diets of poor countries was believed to be protein. 3,4 Kwashiorkor was found widely throughout the world, responded well to protein supplementation, and this led the international community to focus policies and programs to close the “protein gap.” In 1968, the United Nations published a report with an alarmist title “International Action to Avert an Impending Protein Crisis;” 5 the report proposed, with urgency, several strategies for increasing the world’s protein food supply and these ranged from increased production from conventional land, marine, and fresh water sources to the use of novel technologies, such as single-cell proteins and synthetic amino acids production. One strategy that the report promoted was one that INCAP had been pursuing for several years: The development of vegetable protein mixes to provide ample amounts of protein with a satisfactory amino acid composition. 6 INCAP named its mix Incaparina and soon other versions appeared in Colombia, Mexico and around the world.
The study was designed to assess the effects of protein supplementation on human development. It came to be because of INCAP’s long-standing interest in the functional and behavioral consequences of early malnutrition and the creation of the National Institute of Child Health and Human Development (NICHD) in the early 1960s, mandated by the US Congress to explore interdisciplinary factors in human development. 7 NICHD supported the study under a contract mechanism. It was the principal activity of INCAP’s Division of Human Development for many years. The total cost of the study, mostly provided by NICHD, was nearly 6 million US$. 7 Psychological testing was the heart of the study and for ease of administration of the tests, the study sites were in the eastern, Spanish-speaking part of Guatemala rather than in the linguistically diverse Mayan highlands 7 where several of INCAP’s prior longitudinal studies were carried out.
The process of selecting the villages was sequential. 8 Based on predefined criteria that included population size, birth and death rates, family structure, village compactness, and patterns of migration, among others, around 300 potential villages were identified. After data collection in as many as 45 villages, 10 that had similar characteristics, where no public health interventions were planned and whose leaders were willing to participate, made the short list. The original design called for 3 sets of 3 matched villages (total of 9 villages) to be allocated to (1) atole, a protein rich supplement, (2) a control drink called fresco, or (3) nothing. The latter, the “super control villages” were dropped from consideration due to budgetary and ethical reasons, leaving only 2 sets of matched villages. 7 Ultimately, budgetary constraints led to the reduction of matched villages from 3 to 2. Of these, 2 were “large” (approximately 900 people) and 2 “small” (approximately 500 people). 7 This reduction to just 2 sets of 2 matched villages is a major limitation of the study. Villages were allocated at random to atole or fresco for each pair of matched villages.
An extensive description of the 4 villages is given elsewhere. 8 The primary livelihood was agriculture with most men being tenants or small landowners; wage labor was the principal occupation in only 15% to 20% of men. Key crops were corn, beans, tomatoes, sorghum, and manioc but this varied by village. Fewer than 10% of households had a source of water in the house and latrines were rare. Most owned their homes. The typical house had 1 or 2 rooms, adobe walls, dirt floors, and tile or metal roofs but poorer homes had reed walls and thatched roofs. The small fresco village differed in several respects. The climate was hotter and houses even of the wealthier families had walls made of reed and mud and thatched roofs. Cooking was done indoors or in a small area just outside the home; indoor air pollution from burning wood was common. The mean nuclear family size was between 4.6 and 4.7. About 25% to 40% of women were literate, less than in men, 38% to 60%. Spanish was spoken in all households.
Duration of Study and Target Population Groups
Most data collection began on January 1, 1969, in the large villages and a little later (March-May) in the small villages; it stopped in August 1977 for most data collection. 8 Census information, supplementation attendance and consumption, dietary intakes, home diet, morbidity, clinic visits, anthropometry, and mental development were collected longitudinally. Habicht and Martorell 9 describe the types of data collected and review the methods used. Unfortunately, some data, such as clinic visit information, have been lost.
The rigor with which the 1969 to 1977 longitudinal study was implemented owes much to the extensive planning and methods development that preceded the study, including a comprehensive pilot test of the entire operation, including supplementation, in 2 test villages from the same region of the country as the experimental villages. 7 This activity lasted several years and allowed for the correction of many deficiencies in implementation and the testing of innovative solutions to challenges encountered.
Census surveys and continuous updates provided INCAP with accurate household rosters to use in identifying the target groups and in planning data collection. The target groups of the study included women who were pregnant, breastfeeding, or who had formed unions or marriages but not yet had children. The second target group was children who were 7 years or younger when the study began as well as those born during the study. Children were followed until 7 years of age but this was possible only for a few because of the abrupt end of the study due to NICHD’s decision not to continue funding a study with escalating costs. Read and Habicht 7 note that NICHD “moved away from long-term studies of human development and toward shorter-term clinical types of research”. In effect, it became more like other institutes of NIH. It is not clear what the intended date of termination of the study was when it began but it was definitely not 1977. The study design was envisioned as one of cohorts that would inform as to the importance of the age at which children began receiving the supplements. 7 The cohort regarded to have the greatest value was that in which the mother received supplementation during pregnancy and the child to the age of 7. Seven years of age was selected because it was believed that tests at this age were sufficiently predictive of long-term abilities.
The Supplementation Centers and the Supplements
The supplements were prepared in the kitchens of supplementation centers, located in a central location of the villages. Tables and chairs were set up in a large-size room. They were served twice daily, midmorning and midafternoon so as not to interfere with mealtimes and were available all year round. All villagers were free to come and consume the supplement but attendance and supplement consumption were recorded only for pregnant and breastfeeding women and for children aged 7 years or younger. Each person was offered a cup with 180 mL of either atole or fresco; more was provided if requested and noted. Leftovers were poured into a measuring flask and recorded. From this information, daily volume intake was calculated.
The belief in the primacy of protein deficiency at the time accounts for the protein-rich nature of the atole as shown in Table 1. 10 It included Incaparina, a mixture of vegetable proteins developed by INCAP as a strategy for preventing malnutrition, dry skim milk, and some sugar. It provided 163 kcal and 11.5 g of high-quality protein per cup as well as key vitamins and minerals but was not a good source of zinc. The original idea was that the fresco would be a placebo drink, without energy or nutrients. As such, it was meant as a control for the considerable interaction that took place at the supplementation centers, which, by itself, could influence child development. The dropped “supercontrols” would not have experienced this social interaction permitting the quantification of the impact of social interaction by comparing child development data from supercontrols and fresco communities. The original plan was to use cyclamate (a noncaloric sweetener) for the fresco but emerging concerns about carcinogenicity in rats led researchers to use sugar instead, as little as possible, and flavoring. This proved to be wise because the US Federal Drug administration banned the use of cyclamates in foods in late 1969 after the study had begun. Per cup, the fresco contained 59 kcal. On October 1, 1971, in an attempt to sharpen the contrast in protein between the 2 drinks, and perhaps because of ethical concerns about providing empty calories, micronutrients began to be added to the fresco in equal concentrations per volume as in the atole (Table 1).
Formula and Nutrient Composition of Beverages Per Cup Serving (180 mL).a
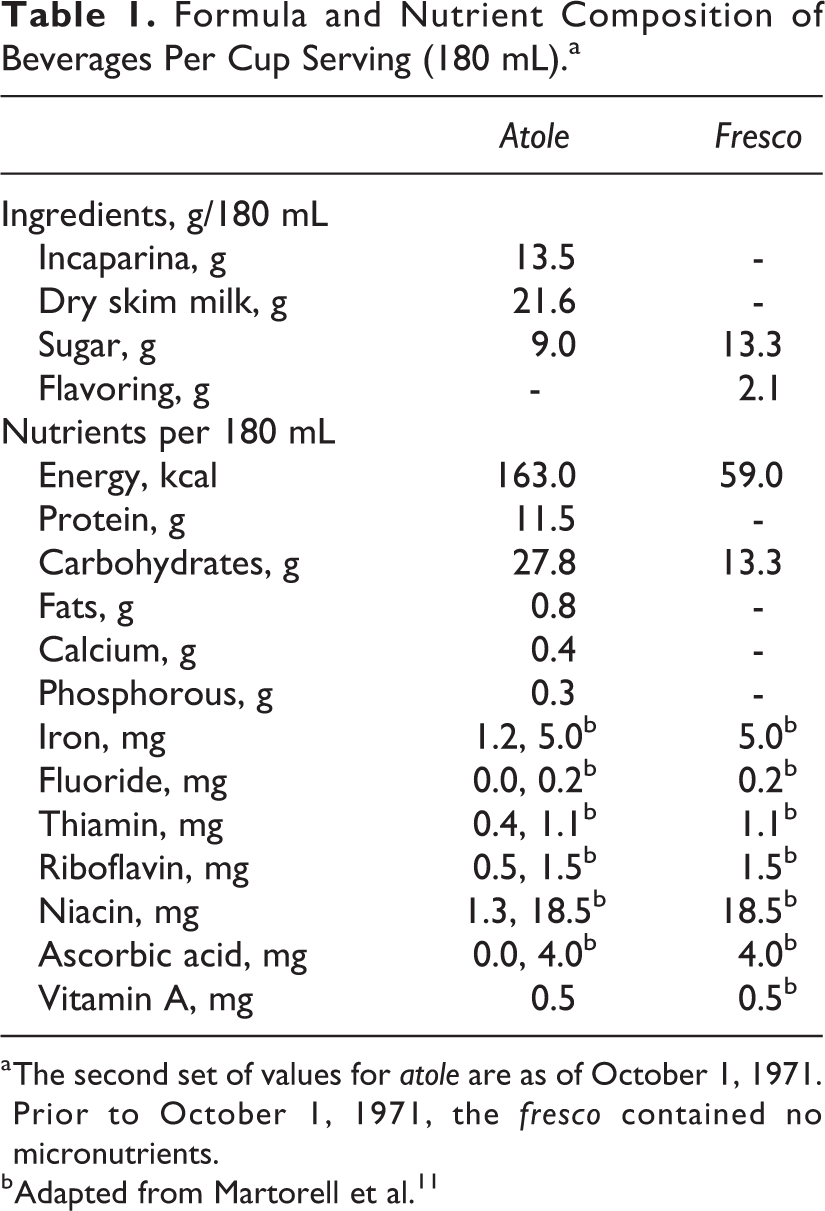
a The second set of values for atole are as of October 1, 1971. Prior to October 1, 1971, the fresco contained no micronutrients.
b Adapted from Martorell et al. 11
Villagers had very different perceptions of the drinks. The atole was served hot and was a thick gruel similar to the corn-based, hot drinks consumed in Mesoamerica; Incaparina, which some in the villages would have known, was similar in appearance and also consumed hot. The atole was thought to be a nutritious drink, whereas the fresco, similar to local sugar sweetened cool drinks, was seen as refreshing but not nutritious. These contrasting characteristics—nutritious versus refreshing, hot versus cold, thick versus light, were a limitation of the design and led to different patterns of consumption. 12
Attendance was greater in atole compared to fresco villages up to 36 months of age. Children in atole villages consumed more of the atole than the fresco at younger ages but these patterns were reversed later (Figure 1). Because the concentration of micronutrients was similar in both drinks, the intake patterns for these nutrients were identical to those seen for volume. The energy contribution of the supplements was greater at all ages in atole villages but more so at younger ages (Figure 2). For pregnant women, more of the fresco was consumed (247 vs 118 mL/d) but energy consumption was still somewhat greater in atole villages (107 vs 81 kcal/d). 13 The contribution of micronutrients on the other hand was greater in women in fresco villages.
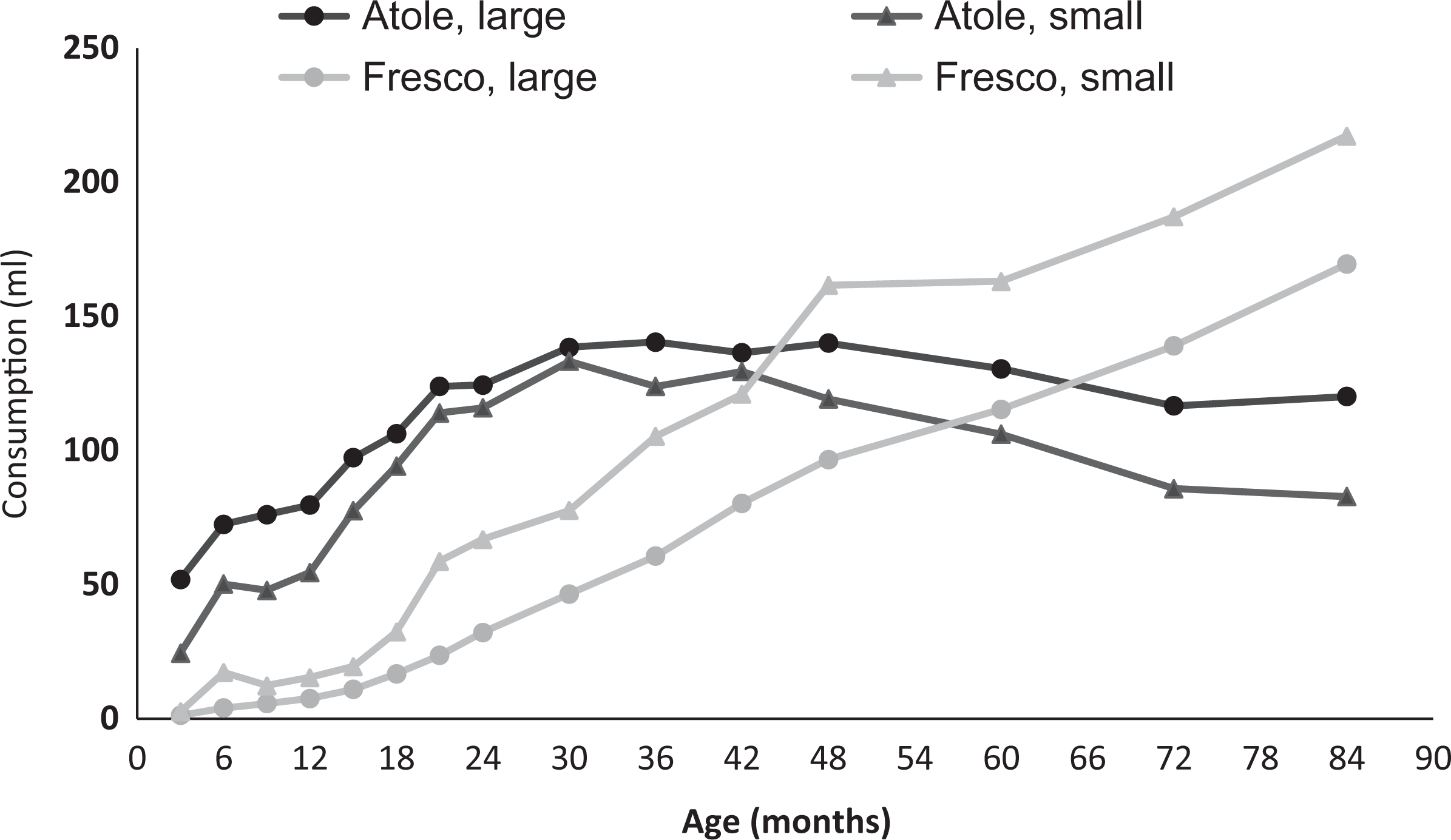
Mean volume (mL) of supplement consumed per day, by age and village (Reproduced from Schroeder et al).
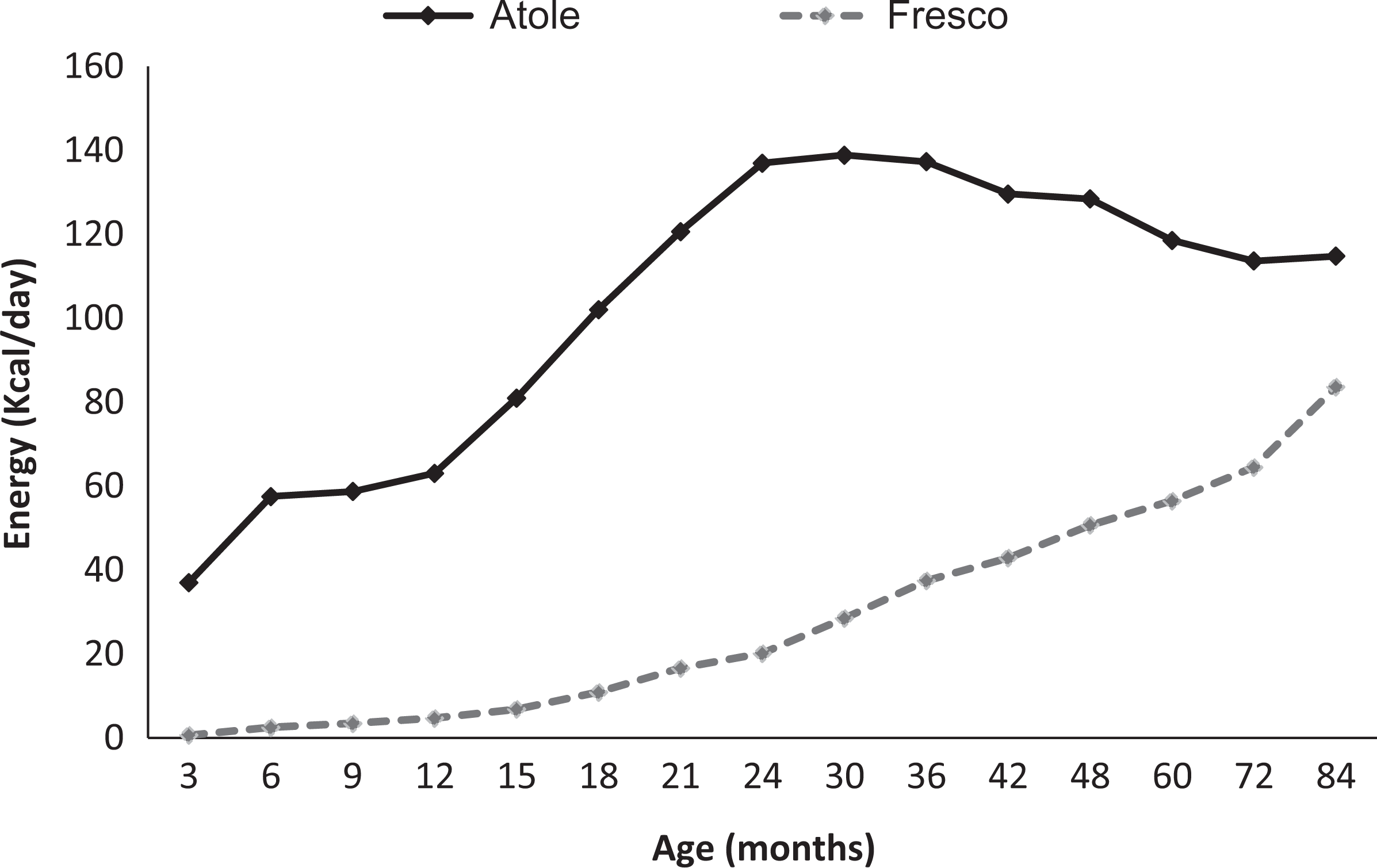
Mean energy intake (kcal) from supplement, by age and supplement type (Reproduced from Schroeder et al).
Primary Health Care
Despite some opposition from those wanting to provide only the nutrition intervention, an effective primary health-care program was designed and implemented in 1969. 8 The key rationale for disturbing “the natural environment” was ethical but the researchers also believed that it would help improve the causal inferences of impact of the nutrition intervention. In a previous INCAP study, an epidemic has struck one but not the other village, complicating data interpretation. The primary health-care model implemented used auxiliary nurses as providers working under the supervision of a physician; this was met with resistance because care was not provided by physicians directly, which would have made care more expensive. Jean-Pierre Habicht, a Swiss trained physician who also obtained a PhD in nutritional biochemistry from MIT, coordinated a systematic assessment of existing health conditions and the development of detailed protocols for diagnosis, treatment, and follow-up of cases and importantly, for identifying when cases needed to be referred to the supervising physician. By 1973, more than 99% of the patients were managed correctly and less than 1% had to be referred to the supervising physician and only 0.4% to hospitals. The primary health-care system was cost-effective and reduced infant and child mortality at a cost of US$5 per villager per year. Over the course of the study, the model implemented was accepted and admired as its results and those of similar experiences elsewhere became known.
Services were provide free of charge, including medicines, on weekdays to everyone at a clinic adjacent to the supplementation center. These services were not linked to study participation. Both curative and preventive care were offered. The latter included tetanus vaccines for pregnant women and tuberculosis, diphtheria, whooping cough, measles, and poliomyelitis vaccines for children. Deworming was offered twice a year. Children with severe malnutrition were placed under close supervision and treated in both atole (receiving dyed-red atole to signify that this was medicinal) and fresco villages (skimmed milk with sugar). Direct supervision of intake was essential because most of these children lacked appropriate care and attention to feeding at home. Importantly, health and nutrition education was not provided, apart from promoting attendance to the supplementation centers and participation in immunization and deworming campaigns.
Impact on Home Diets
Home dietary intakes in pregnant women were similar in atole and fresco villages for energy as well as protein. 13,14 There was little substitution of home energy by supplement energy. The relationship between supplement energy and home diet energy was weak and nonsignificant in analyses that pooled all villages and suggested that 100 kcal of supplement decreased home diets by 3 kcal. 14 When the pooled sample was divided into those consuming less than 20 000 kcal or equal or more than this amount throughout pregnancy, home dietary energy intakes were nearly the same; the high group consumed only 41 kcal less, despite the consumption of substantial amounts of energy from the supplements. The amount of energy from the supplements were 43 and 233 kcal/d, respectively, for low and high groups. 14
The impact of the intervention on children’s diets was assessed using dietary surveys that were administered every 3 months from 15 to 36 months of age. 11 Pooled estimates of home diet energy and protein intakes are shown in Table 2 stratified by sex and type of supplement. Also shown are average daily intake from supplements and total nutrient intakes. Home dietary intakes were similar across supplement groups. Energy intake from the fresco was about 25 kcal/d, substantially lower than the energy obtained from the atole, over 150 kcal/d. In addition, the atole contributed about 11 g of protein per day. Comparison of total nutrient intakes shows that children in atole villages had intakes that were greater by 101 kcal/d and 8.6 g of protein in boys and 89 kcal and 8.8 g in girls, respectively. The atole did not appear to have displaced much of the diet as suggested by comparisons of home diets in atole and fresco villages, which were only slightly lower in the former, by 33 kcal and 2 g of protein, on average.
Dietary Intake Differences Between Atole and Fresco Villages (15 to 36 Months of Age).a
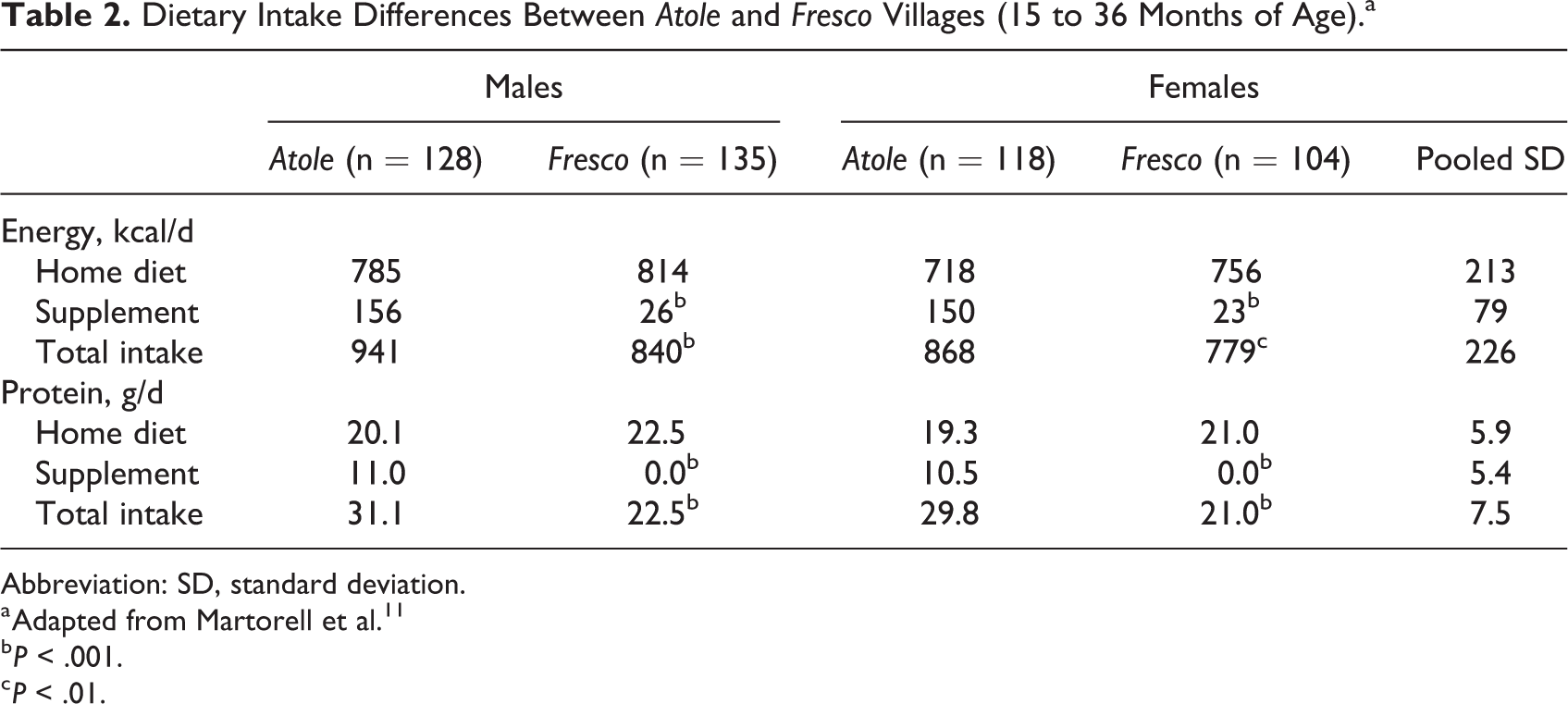
Abbreviation: SD, standard deviation.
a Adapted from Martorell et al. 11
b P < .001.
c P < .01.
Other analyses also suggest little substitution. Dietary intakes of energy and protein are shown in Table 3 for home diet, atole intake and total nutrient intakes in boys and girls stratified by arbitrary levels of atole intake. 15 Home dietary intakes do not appear to change appreciably as the amount of atole intake increases. Total nutrient intakes, by contrast, increased substantially.
Energy and Protein Intake in Atole Villages by Level of Atole Intakea,b
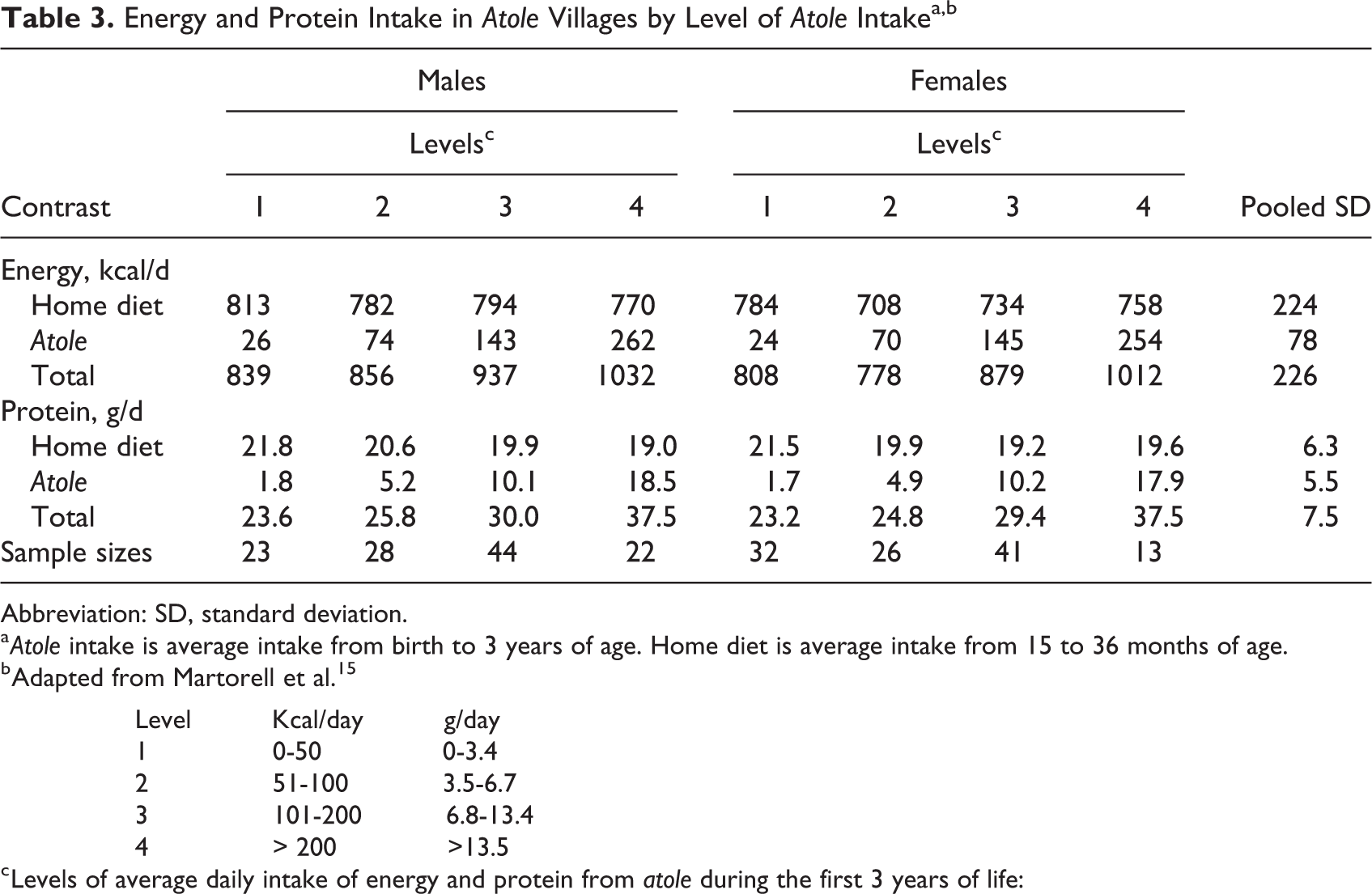
Abbreviation: SD, standard deviation.
a Atole intake is average intake from birth to 3 years of age. Home diet is average intake from 15 to 36 months of age.
b Adapted from Martorell et al. 15
Level Kcal/day g/day
1 0-50 0-3.4
2 51-100 3.5-6.7
3 101-200 6.8-13.4
4 > 200 >13.5
c Levels of average daily intake of energy and protein from atole during the first 3 years of life:
The Evolving View About Protein
The protein crisis vanished during the middle of the INCAP Longitudinal study. In 1974, McLaren published his famous paper entitled “The Great Protein Fiasco” in which he expressed the view that more and better protein was not the priority for most of the world; instead, the lack of food, and therefore energy, was the main problem. 16 The only exception he was willing to accept was where the staple foods were plantains or roots and tubers like manioc, which are low in protein. In 1973, a committee of the Food and Agriculture Organization/World Health Organization (WHO) lowered protein requirements by 20% but left the energy requirements largely unchanged and this precipitated the shift in views. 17 The protein gap vanished when researchers compared dietary intakes to the revised requirements. Payne 18 noted that when energy is limiting but protein is ample, some of the protein will be used to provide energy and this may cause amino acid deficiencies at the cellular level. Theoretically, when energy intake alone is increased, that protein that would have been used for energy metabolism will be spared for synthesis of lean mass and growth.
Protein champions like John Waterlow, a member of the committee, conceded. 19 Nevin S. Scrimshaw, another champion of protein and also a member of the committee, was not convinced and remained a proponent of protein until the end of his long life. It is possible that he was responsible for a cautionary note by the committee…that the estimates of requirements were for healthy individuals and that needs would be greater where chronic and acute infections are endemic. 17(p99) In 1977, Scrimshaw wrote “to the extent that the pendulum swung too far in emphasizing protein in the 1960s, and too far in emphasizing calories in the 1970s, it must come to a more appropriate intermediate position for the 1980s and beyond.” 20(p335) The pendulum swung in yet another direction after the 70s, toward micronutrients, but a more balanced view is emerging today as there is increasing evidence of the additional importance of protein and protein quality in the diets of poor children growing up in environments of deficient environmental sanitation and widespread infection. 4
Analyses of Birthweight
Among the first outcomes to become available for preliminary analyses in sufficient numbers were pregnancy outcomes such as placental weight and birthweight. The demise of the protein era led researchers involved with the INCAP Longitudinal Study to explore relationships between energy from the supplements and these outcomes. 14,21 In effect, they abandoned the experimental design in favor of observational analyses. Although the fresco had no protein, it contributed almost as much energy as did the atole. Recall that the volume of supplement consumed by pregnant women was more than double in fresco compared to atole villages, making up to a large extent for its smaller energy concentration. Average energy intakes from the supplements overlapped significantly although 25% greater in atole compared to fresco villages (107 vs 81 kcal/d). 13 Researchers reported positive associations between energy intakes from either of the supplements and birthweight. 14,21 Habicht et al 21 wrote “Contrary to expectations, protein ingestion from supplement had little, if any, additional effect on birthweight, a surprising finding since the home diet in these villages is kwashiorkorgenic for preschool children.” The basis for this conclusion was the observation that the relationship between energy from supplement and birthweight had similar slopes in fresco and atole villages; if protein provided additional benefit, the slope would have been greater for atole energy. 14
The main results about birthweight in what became the most cited paper are shown in Table 4. 14 Energy consumed from the supplements during pregnancy was divided by consumption level, below or 20 000 kcal and above, which was selected because it was close to the median and, probably, because it a nice round number. An analysis of variance showed significant relationships for high being greater than low consumption and for atole being greater than fresco; the interaction between supplement type and level of consumption was reported as “not significant.” However, the exact P value was not provided. For the combined atole and fresco sample, the mean difference in birthweight by level of consumption was 111 g. Other analyses showed that the prevalence of low birthweight (<2500 g) was around 18% in the low category and about half that in the high category of supplement intake and that this relationship was similar in atole and fresco villages. Results were robust to control for confounding.
Mean Birthweight (g) by Group of Energy Consumed From Supplementation++ During Pregnancy and Type of Supplement.a,b
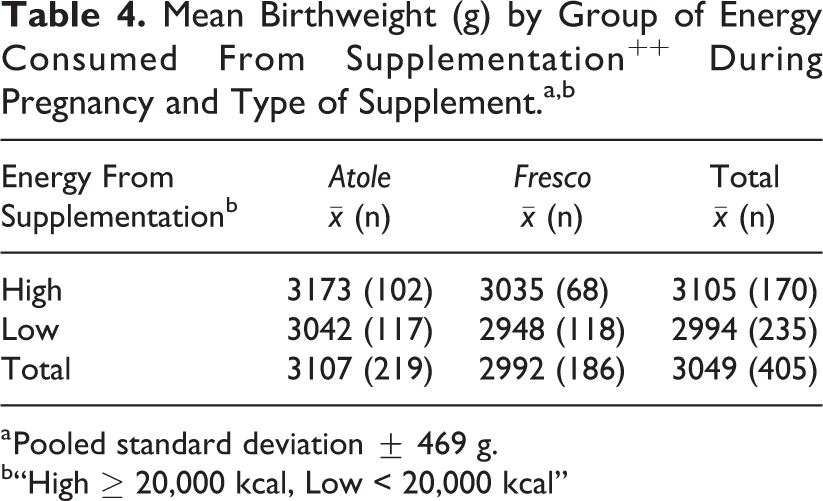
a Pooled standard deviation ± 469 g.
b“High ≥ 20,000 kcal, Low < 20,000 kcal”
The researchers concluded that the results supported the view that energy, and not protein, was the main dietary limitation in the diets of women. Likely influenced by the new belief in the primacy of energy deficiency, Lechtig et al 14 did not comment on the finding in Table 4 that showed that mean birthweight was significantly greater in women receiving atole versus fresco (P = <0 .025). To examine this finding further, I have used the data from Table 4 to make several additional comparisons: Atole: high versus low; fresco: high versus low; and atole versus fresco (Table 5). The relationship between supplement level and birthweight is stronger and only statistically significant in atole compared to fresco villages. The intent-to-treat comparison of atole versus fresco shows a difference in birthweight favoring atole of 115 g, which is 0.25 of a standard deviation, a small effect size but one of public health importance. Mean birthweights in atole villages may be greater because of the contribution of this drink to protein intakes (7.5 g of protein per day as reported by Delgado et al 13 ) and/or because of somewhat greater mean energy intakes in atole villages and by extension in other nutrients as well. Clearly, further analyses of these data are warranted, also considering that sample sizes at the end of the study in 1977 were greater than available by February 1973, the cutoff date for the analyses by Lechtig et al. 14
Selected Comparisons for Groups in Table 4.a,b
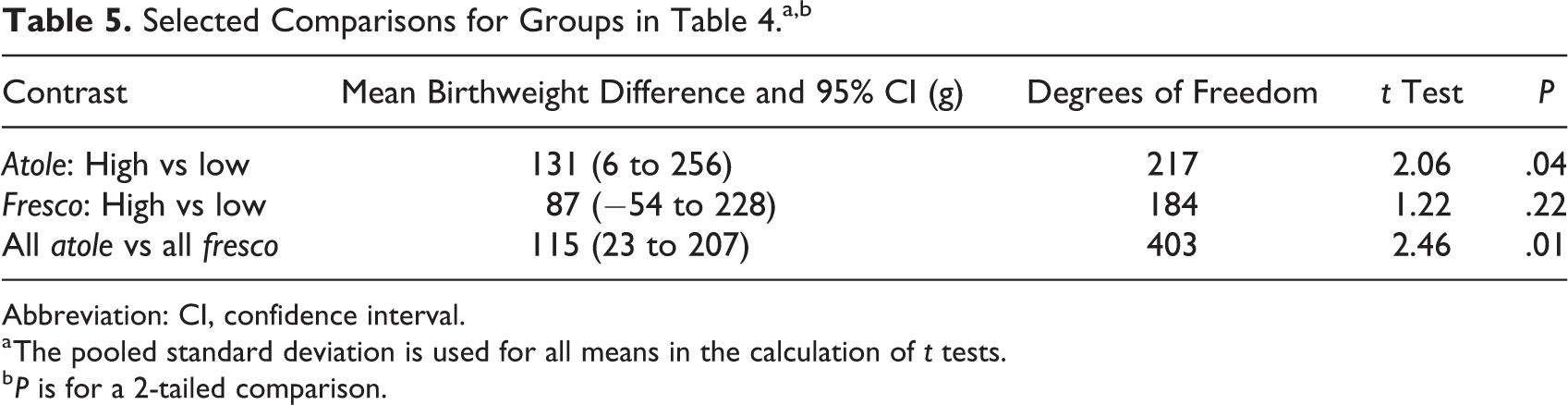
Abbreviation: CI, confidence interval.
a The pooled standard deviation is used for all means in the calculation of t tests.
b P is for a 2-tailed comparison.
Analyses of Child Growth
Physical growth was included as a secondary outcome to test if the atole was efficacious. Although preliminary analyses showed children in atole villages were growing faster than in fresco villages, this finding was not attributed to protein. Rather, there was a strong bias among all of us to show that the cause of better growth was the energy in the atole. There were the findings in pregnancy to consider; would not they also apply to children? In addition, comparison of the dietary intakes of children to the 1973 energy and protein requirements 17 indicated that protein was not limiting. 22 Like most, we ignored that the children were having heavy burdens of infection and accepted the new energy and protein requirements blindly.
In a 1978 article with the title “Energy intake and growth in an energy deficient population,” Martorell et al reported that the atole contributed 166 kcal/d and the fresco 28 kcal/d. When the data were pooled, the relationship between energy from the supplements and length and weight gains was not modified by controlling for the presence of protein in the supplement, a finding that led the authors to argue for an energy interpretation. Their final sentence was as follows: “Our data argue that populations whose diets are moderately low in energy but adequate in protein, an effective intervention would be one involving increased intake of foods traditionally consumed, rather than the introduction of costly high-protein foods.”
As the lead author of this article, I regret the conclusions and the final sentence. We went too far in seeing what we thought we should see. The correct interpretation should have been that “Little could be concluded about relationships between fresco intakes and child growth since so little of it was consumed.” Also, we overlooked that there was a total lack of significant findings with respect to fresco, unlike for atole. We should have realized that the regressions that controlled for the presence of protein were not informative since only a small part of the distribution of energy intakes from the supplements overlapped between atole and fresco.
As I continued to analyze the data, I became much more cautious. By 1992, I wrote as follow about possible impact on child growth: “The results on the effects of the nutrition intervention in children are best viewed as providing information on the value of improving food consumption in general rather than that of any particular nutrient.” 23(p272) This was an admission that the design, as implemented, does not allow for inferences about the relative importance of energy versus protein in the case of children; neither does it allow for any conclusions to be reached about the impact of the micronutrients.
Martorell et al 15 used baseline data collected in 1968 in assessing community changes in size at 3 years of age by village size, type of supplement, and sex. The results suggested little change in fresco villages after supplementation but consistent and significant changes in atole villages. These results used individuals as the unit of analysis. However, Habicht et al 24 used these data to carry out an elegant analysis where village became the unit of analysis (Table 6). Despite only 2 degrees of freedom, a 2-tailed t test was highly significant. Fresco villages showed little or no improvement while atole villages improved by about 3 cm. This suggested little impact of primary health care on length but substantial impact of the atole intervention.
Lengtha of 3-Year-Old Children Before and After Supplementation by Village Size and Type of Supplement (in cm).b,c
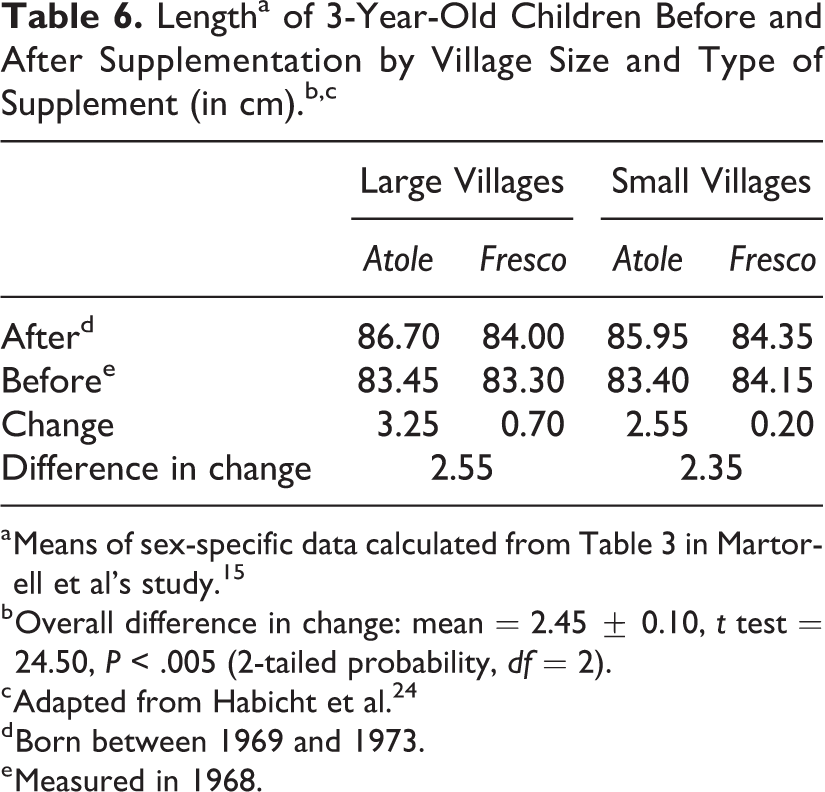
b Overall difference in change: mean = 2.45 ± 0.10, t test = 24.50, P < .005 (2-tailed probability, df = 2).
c Adapted from Habicht et al. 24
d Born between 1969 and 1973.
e Measured in 1968.
Other analyses showed that 3-year-old children who received atole during their entire lives differed in several characteristics compared to those who received fresco (Table 7). Effect sizes, representing the average difference between atole and fresco means across males and females divided by the pooled standard deviation, indicate a clear pattern of large effect sizes for linear and bone dimensions such as supine length, head circumference, and arm length as well as for body weight. Effect sizes for circumferences, representing lean tissue but also subcutaneous fat, are of large to medium size and skinfolds are the least affected.
Anthropometric Differences at 3 Years of Age Between Atole and Fresco Villages.a
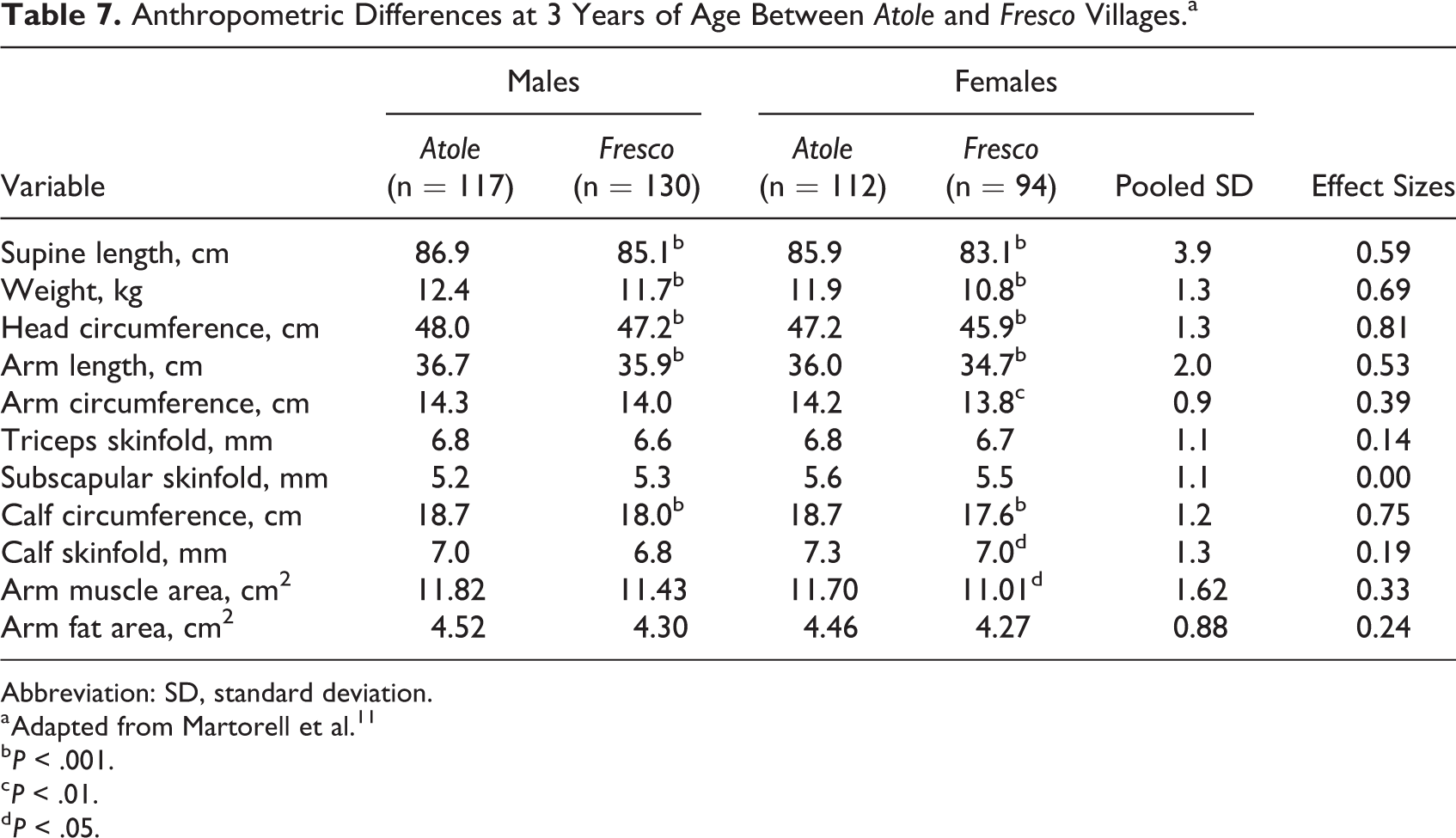
Abbreviation: SD, standard deviation.
a Adapted from Martorell et al. 11
b P < .001.
c P < .01.
d P < .05.
Anthropometric characteristics by level of atole intake, as defined earlier in Table 3, are shown in Table 8. The variables that increase across levels of atole intake are weight and the 3 linear growth measures, namely supine length, head circumference, and arm length. Effects sizes for the differences between highest and lowest levels show large effect sizes. Importantly there is no evidence that measures of fatness increased as atole intake increased; if anything, there is a tendency for thinner skinfolds in the children with the greatest intake of atole, which had substantial amounts of energy and protein and whose home diets did not appear to have changed.
Anthropometric Characteristics of 3-Year-Old Children by Sex and Level of Atole Intake as Defined in Table 3.a
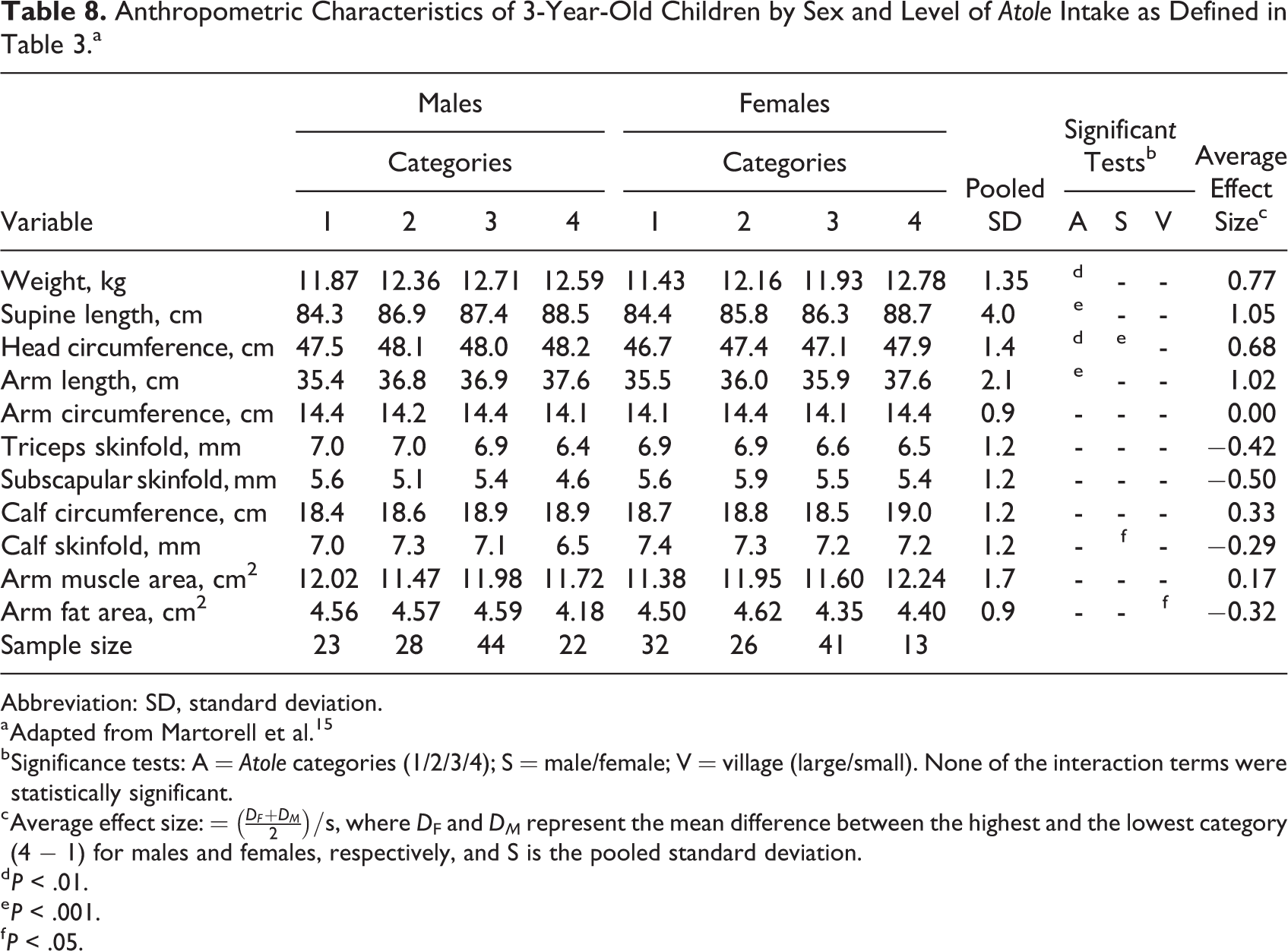
Abbreviation: SD, standard deviation.
a Adapted from Martorell et al. 15
b Significance tests: A = Atole categories (1/2/3/4); S = male/female; V = village (large/small). None of the interaction terms were statistically significant.
c Average effect size: =
d P < .01.
e P < .001.
f P < .05.
Atole is Only Related to Child Growth Before 3 Years of Age
Schroeder et al 25 examined relationships between yearly increments in length and weight and concurrent energy intakes from atole and fresco supplements. They reported stronger associations between atole intake and growth at younger ages, with little or no evidence of a relationship after 3 years of age. Also, there was no evidence of a consistent relationship between fresco intake and growth.
In new analyses for this article, I tested the hypothesis that exposure to atole compared to fresco was associated with better growth in length, weight, and head circumference before but not after 3 years of age. In addition to analyses with size at age 3, I carried out analyses for measures of change. I selected 4 samples, each approximately 3 years in duration: those exposed to the supplements from birth to 3 years, from 3 months to 3 years, from 3 to 6 years, and from 4 to 7 years. I show descriptive statistics in Table 9 for anthropometric variables and for supplement intake for birth to 3, 3 to 6, and 4 to 7 years. Growth during the first 3 years of life is much faster than from 3 to 6 and 4 to 7 years, particularly for head circumference. The supplement intake data show the patterns previously noted, with little consumption of fresco at younger ages.
Descriptive Characteristics of 3 Samples Based on Age at Exposure to Supplement.a
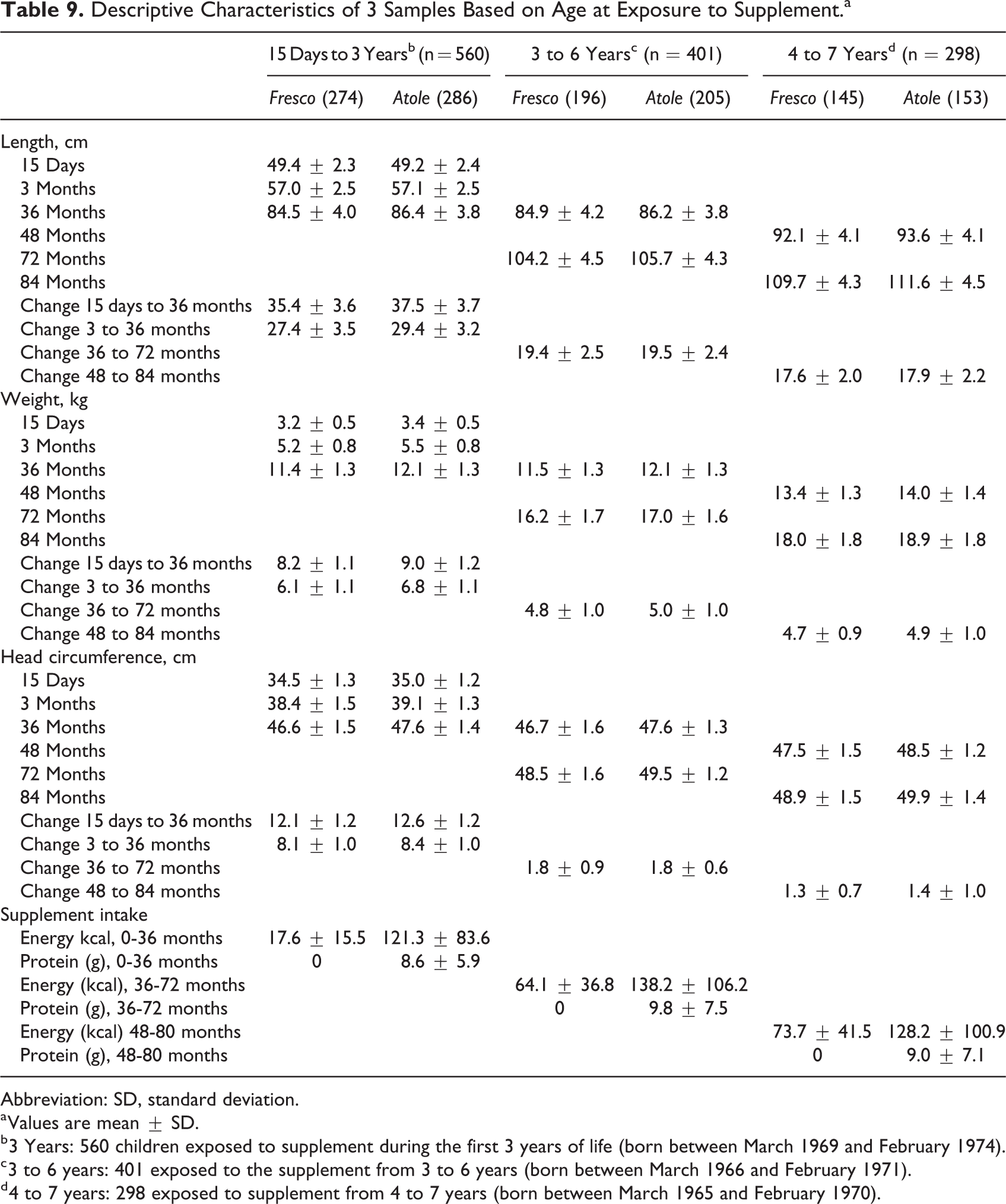
Abbreviation: SD, standard deviation.
a Values are mean ± SD.
b 3 Years: 560 children exposed to supplement during the first 3 years of life (born between March 1969 and February 1974).
c 3 to 6 years: 401 exposed to the supplement from 3 to 6 years (born between March 1966 and February 1971).
d 4 to 7 years: 298 exposed to supplement from 4 to 7 years (born between March 1965 and February 1970).
Linear regressions were carried out in which the anthropometric measure at the beginning of the period was regressed on the corresponding measure at the end of the period, followed by indicator variables for atole, village size, and sex and by several potentially confounding factors, including the predictors of supplement attendance and consumption: distance to supplementation center and socioeconomic status. This model in effect regresses atole exposure and the other variables on residuals for the following periods: 15 days to 3 years, 3 months to 3 years, 3 to 6 years, and 4 to 7 years. Multiple imputation was used in SAS 9.4 to account for missing information for socioeconomic status, maternal and paternal years of schooling, and number of family members. PROC MI was used to generate 20 imputed data sets using fully conditional specification. Linear regression was then conducted for each of the 20 imputed data sets and the estimates were pooled by PROC MIANALYZE. Results show that exposure to atole compared to fresco is associated with improved growth only in the first 3 years (Table 10). Several interactions (atole × sex, atole × village size) were tested but few were significant. These findings are consistent with Schroeder et al 25 who reported lack of association between intake of atole and growth after 3 years.
Associationa Between Exposure to Atole and Length, Weight, and Head Circumference at 3 Years and for Residuals.b,c
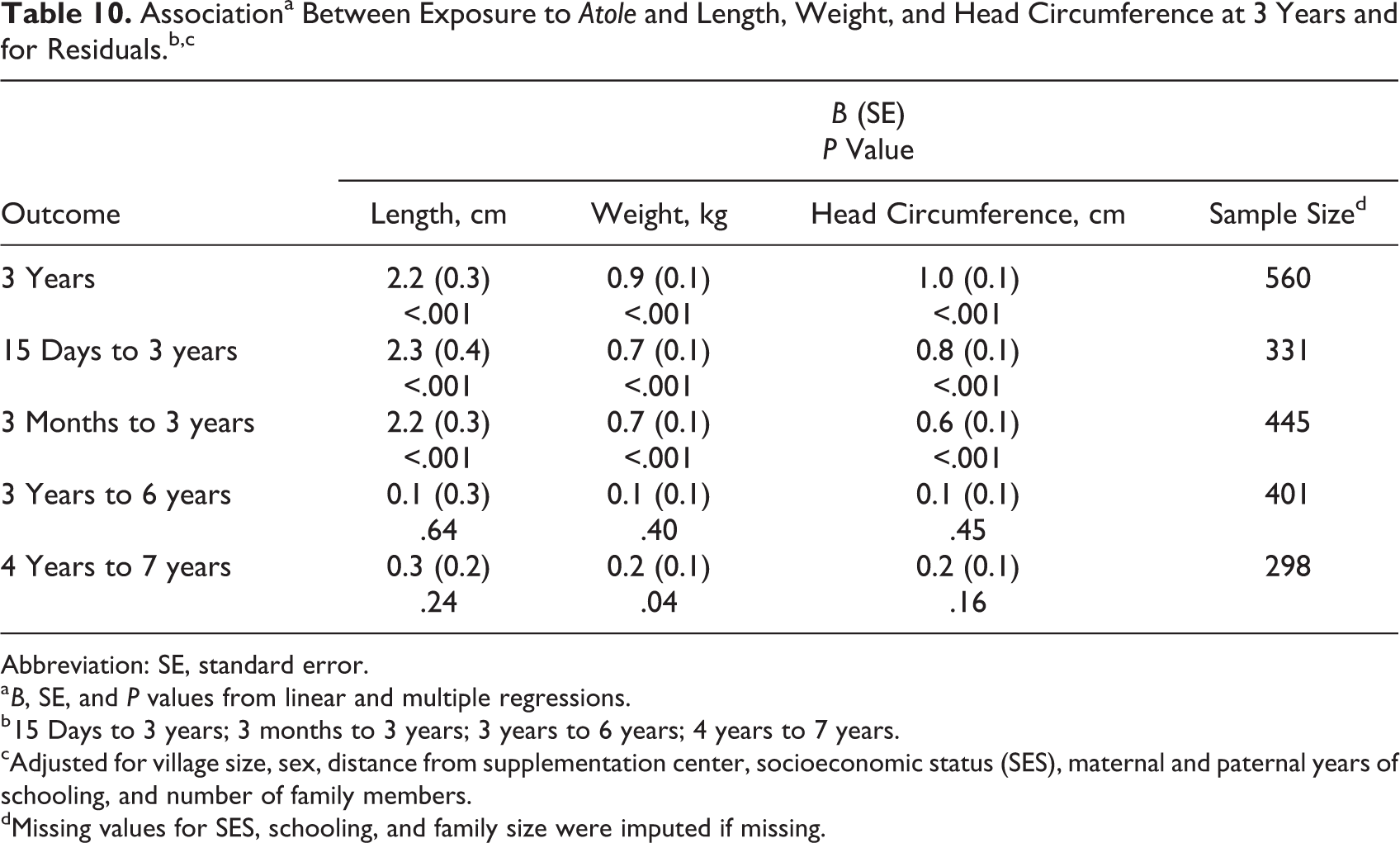
Abbreviation: SE, standard error.
a B, SE, and P values from linear and multiple regressions.
b 15 Days to 3 years; 3 months to 3 years; 3 years to 6 years; 4 years to 7 years.
cAdjusted for village size, sex, distance from supplementation center, socioeconomic status (SES), maternal and paternal years of schooling, and number of family members.
dMissing values for SES, schooling, and family size were imputed if missing.
Other Outcomes
Researchers explored associations between supplementation and other biological outcomes in early childhood to claim improvements in placental weights, 26 gestational age, 13 infant mortality 27 recovery from mild-to-moderate wasting malnutrition, 28 elimination of the negative effect of diarrhea on growth, 29 the timing of deciduous dental eruption, 30 maturation as measured by the number of centers of ossification, 31 and cortical thickness of the second metacarpal. 32
Discussion
The study ended abruptly in 1977. Analyses of these data at the time and later showed that the Atole was efficacious in improving dietary intakes and child growth. With the possible exception of supplementation during pregnancy and birthweight, researchers could not attribute impact on physical growth specifically to protein, energy or micronutrients, or any combination. Children in atole villages received more of all these nutrients in the first 3 years of life, the period when exposure to atole was related to improved growth. New analyses included in this article are conclusive in showing no impact of exposure to atole relative to fresco from 3 to 7 years of life. This is consistent with patterns of growth failure in children from developing countries that suggest similar growth velocities after about 2 years of age in children in developing countries as in the WHO standard. In other words, the atole was efficacious only in early life, when growth failure occurred. 33
The analysis of the INCAP Longitudinal study data is a case study of how prevailing notions in the field can influence the analysis and interpretation of results. The study was designed as a potent protein intervention because nutritionists in the 1960s believed protein deficiency was the main dietary limitation. The collapse of this view in the 1970s in favor of energy deficiency, just as the data began to be analyzed, led to analyses that considered the key exposure to be energy from the supplements, regardless of the presence of protein. The experimental design was abandoned, and the study was analyzed as if it were an observational design. Later, a more balanced view incorporating the importance of dietary quality, including protein and micronutrients, began to emerge and investigators returned to considering the experimental design.
I remember some disappointment among the psychologists when the study ended in 1977 that they did not have similar evidence suggestive of impact on child development as was shown for birthweight and child growth. The late Ernesto Pollitt, a Peruvian psychologist at UC Davis, was reluctant to accept my invitation to participate in the first follow-up study in 1988 to 1989 because he thought we would not find much. I insisted that this would be an important finding nonetheless and eventually he agreed to join the study. Pollitt led a reanalysis of the preschool psychological study and confirmed that there was little or no evidence that the experiment improved cognition in preschool children. 34 To his surprise, the study uncovered substantial impact among adolescents and young adults on tests of general knowledge, numeracy, reading, and vocabulary. 34
Footnotes
Acknowledgments
The INCAP Longitudinal Study was supported by contract HD-5-0640 from the National Institute of Child Health and Human Development, National Institutes of Health, Bethesda, Maryland. Additional sources of support were from the Agency for International Development, Washington, DC (AID-TA-C/1224) and the Rockefeller Foundation (73030-E73352). The author thanks Dr Inés González-Casanova for carrying the analyses in Tables 9 and ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.