
Abstract
Background:
Malnutrition and food insecurity are major challenges in Somalia, particularly among small children living in internally displaced person (IDP) camps. Poor diet has been identified as a key driver of malnutrition in young children who depend for their diets on their household’s socioeconomic standing and access to food, as well as on the family’s caring and feeding practices.
Objective:
To assess the dietary diversity and identify the factors associated with it among children (6-23 months) in Somalian IDP camps.
Methods:
We used a cross-sectional survey conducted in 11 IDP camps in Somalia in June 2014 and in June 2015. A total of 3188 children aged 6 to 23 months were surveyed. Child diets were assessed using food frequency questionnaires, and dietary diversity was categorized using the minimum child dietary diversity (MDDC) indicator. Multivariable logistic regressions were used to identify the factors associated with the children’s dietary diversity. We built and compared 2 models using alternatively the household dietary diversity score (HDDS) and the food consumption score (FCS) as food security proxies.
Results:
Around 15% of children in IDP camps reached the minimum dietary diversity. Overall, our results confirm that not only are food security proxies the factors most associated with MDDC, but HDDS performs better than FCS. In addition, results identify that women as key decision-maker in the household, duration of household permanence in the settlement, women’s physiological status, frequency of milk feeding to child, type of toilet, and measles vaccination are positively associated with MDDC.
Conclusions:
To improve child dietary diversity in IDP camps, food security interventions should be broadened to include female empowerment and inclusive nutrition education (encouraging male participation) programs, as well as initiatives targeting children who do not live with pregnant or lactating women and that can support families beyond the first months after their arrival.
Introduction
Over the past 20 years, Somalia has suffered conflict, political instability, and natural and economic shocks that have resulted in acute hunger and malnutrition. Adequate food availability, access, and consumption are thus among its main concerns. Furthermore, the ongoing complex emergencies resulting from prolonged conflicts and recurrent droughts have led the country’s already unstable food security situation to progressively deteriorate. This hardship has brought about socioeconomic and political instability and has contributed to massive internal population displacement and cross-border migration.
As a result of these prolonged conditions, in 2016, an estimated 1.1 million people were internally displaced persons (IDPs), 1 making Somalia one of the top 10 countries in the world with the highest number of IDPs (note 1). The highest incidence of poverty (71%) in Somalia is found among households in IDP settlements. 2 Across the country, IDPs remain extremely vulnerable, and up to December 2016, they represented a major proportion (58%) of those facing either a crisis or an emergency (according to Integrated Food Security Phase Classification (IPC)) 3 (note 2).
Despite humanitarian efforts to reduce vulnerability, Somalians’ food and nutrition situation has not improved. Compared with 2015 post-Deyr (October to December), the number of people in food security stress in all regions has continually increased. 4 Similarly, the results of the 2016 assessment revealed that 14.3% of children under the age of 5 were acutely malnourished and that an increasing number of surveyed population groups (including IDPs) showed acute malnutrition levels above the 15% UN emergency threshold, compared with the previous year. 3
Over the years, the worst nutrition outcome indicators have been found consistently among IDPs. In the 2016 assessment, the highest malnutrition prevalence was recorded for the Dolow IDP settlement at 21.8% of global acute malnutrition (GAM). In addition, although in Somalia stunting is not considered a public health problem, as most populations report low (<20%) to medium (20-30%) stunting prevalence, there are exceptions, such as IDPs in Baidoa and Kismayo, among whom high prevalence is reported (higher than 30% and 39%, respectively). 3
The causes of the high prevalence of acute malnutrition in Somalia, including among IDPs, are considered multidimensional. This has led policymakers to focus on integrated approaches as well as specific food security and malnutrition policies. For example, the 2011-2013 Somali Nutrition Strategy was put in place to promote a shift toward a more integrated, multisectoral approach to address malnutrition. Integrated management of acute malnutrition was identified as a key approach, and as programs for managing acute malnutrition are reasonably well funded, this is highlighted as an important platform from which to deliver complementary activities. Since 2014, Somalia has also been a signatory of the Scaling Up Nutrition (SUN) movement and has established structures to support SUN’s implementation. The 2017-2019 National Development Plan of the Federal Government of Somalia also reflects this approach (note 3).
However, to better inform these policies, there is an increasing need to understand the causes and drivers of malnutrition, which has prompted researchers and agencies to further investigate them. For instance, Kinyoki et al 5 showed that crop production, food access, and morbidity were among the key drivers, and the Nutrition Causal Analysis, conducted by the SNS Consortium in 2015, identified the main causes of malnutrition among Somalian IDPs as disease and poor diet, resulting from poor household food security and social care environment and inadequate childcare practices. 6
One way of studying children dietary adequacy is measuring dietary diversity, which was shown to be associated with nutrient adequacy and appropriate nutritional status for different populations and contexts (Arimond and Ruel 7 and Arimond et al 8 ). Nevertheless, several studies have assessed the association between child nutritional status and household food security, 9 -11 and for that purpose they have used interchangeably either of the 2 most common measures of household food security: the household dietary diversity score (HDDS) and the food consumption score (FCS).
However, only seldom studies have assessed the association between household food security and the children’s dietary diversity. 12 Therefore, the aim of this article is to provide further insight on children’s dietary diversity in IDP settlements and show how this relates to other factors particularly to household food security. This aspect is even more relevant among Somalian IDPs where according to a recent household survey more than 80% of the households had acceptable food consumption and diverse diets, although child malnutrition rates continue at critical levels. 4
The information generated in this study has programmatic implications and will help to guide efforts aimed at improving the dietary diversity and micronutrient adequacy of children.
Methods
Study Area and Population
Somalia has been divided into 3 main UN operational zones: Northwest, Northeast, and South Central, with varied social, livelihood, and economic structures. The Northwest corresponds to the current administrative and political designation of State of Somaliland declared independent unilaterally in 1991; it has a relatively stable political situation and 3 IDP camps located within its geographical limits; the Northeast zone includes the regions of Bari, with 2 IDP camps (Bosaso and Quardo), and Nugal (with 1 IDP camp, Garowe). The South Central zone is impacted by higher intensity of conflict, flooding of the riverine areas, constant displacements, restrictions of movements and goods access due to clan and religious insurgency, and low availability and poor quality of health services (Matunga and Bush 13 ). It comprises the following regions (and IDP camps): Mudug (Galkayo), Galgadud (Dusharameb), Hiran, Bakool, Bay (Baidoa), Middle and Lower Shabelle, Middle and Lower Juba (Kismayo and Dhobley), Gedo (Dollow), and Banadir (Mogadishu) regions.
In the current study, we use data collected by the Food Security and Nutrition Analysis Unit (FSNAU) in 10 IDP settlements located in the Northeast and the South Central zone. The data correspond to the Food Security and Nutrition IDP surveys conducted toward the end of the Gu seasons in June 2014 and June 2015, and they are part of the FSNAU’s systematic collection during Somalia’s 2 seasons (Gu and Deyr). We used only Gu season data because dietary information was not collected in the Deyr seasons of those years, and nor has it been collected since.
Sample Design
The IDP population sampled was selected using the 2005 Somalian population estimate from UNDP. Using the 2015 version of ENA software, separate sample sizes for each stratum were calculated to estimate the prevalence of GAM and the crude death rate based on the prevalence of GAM from previous years and applying the corresponding precision figures. The larger of the 2 sample sizes obtained was then chosen as the final sample size to ensure that both components were represented.
The selection method was multistage (2-stage) cluster sampling. The primary sampling units were predefined areas of the settlement that were selected randomly and proportional to size, from a list provided by the camp authorities. In the second stage, the secondary sampling units (households) were selected randomly from a complete list of dwelling units/households provided by the camp areas chiefs.
Data Collection
Face-to-face interviews using structured questionnaires were carried out during June 2014 and June 2015. The IDP surveys obtained various information, collected in separate sections, such as household demographic characteristics, life assets, food consumption and coping strategies, water and sanitation facilities, child nutrition and health, and maternal nutrition and health.
It is worth to note that for logistical and cost-efficiency reasons, the food security-related measures were not administered in every household surveyed, but rather collected from a random subsample based on skip patterns (ie from a total of 15 selected households, it was followed an even pattern—2nd, 4th, 6th, 8th, 10th, 12th, 14th—meaning that only 7 were eligible for the food security questions).
Our target population were 6- to 23-month-old children (the age range for which the minimum child dietary diversity [MDDC] indicator is validated for). A total of 3188 children (aged 6-23 months) were surveyed, but only 2922 of them had dietary diversity data collected, of which 196 were recorded as having no food consumption in the previous 24 hours. Of these, however 86 were breastfeed.
Variables
Outcome variable: Children’s dietary diversity
The outcome variable we used is the MDDC indicator which is a dichotomization of the child dietary diversity (CDD) index. This is one of a set of indicators developed by the World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) to assess infant and young child feeding practices, 14 and it has been shown to be a strong predictor of the micronutrient density adequacy of their diet. 15,16 It is defined as the simple count of foods and food groups (FGs) consumed over the previous 24 hours by children aged 6 to 23 months ranging from 0 to 7. The MDDC is defined as children aged 6 to 23 months consuming 4 or more FGs out of the 7 predefined FGs, namely: grains and tubers, legumes and nuts, dairy products (note 4), flesh foods, eggs, vitamin A-rich fruit and vegetables, and other fruits and vegetables. The response options were “consumed” (scored 1) and “not consumed” (scored 0).
Covariates
Food security proxies
Food security is a multidimensional concept with no single indicator yet identified as the gold standard for its measurement. For this study, we used 2 of the most widely used indicators to measure it: HDDS and FCS. In the field, the decision of which indicator to use is often guided by the context and purpose of the study, as well as the trade-offs between comprehensiveness and the ease and cost of data collection. As the use of different indicators can provide contrasting accounts of the state of food security, this decision may have an impact on policy. 17 By constructing separate models on the association between CDD and each of these indicators, we expect to provide further insight on how food security measurements at household level relate to the dietary diversity of children.
The HDDS was calculated as the sum of FGs consumed by an average member of the household in the previous 24 hours. Unlike an individual dietary diversity indicator, the rule of thumb when calculating the household indicator is to include 12 FGs 15,18,19 and thus the HDDS ranges from 0 to 12. 20
The FCS is a composite score that incorporates dietary diversity, food frequency, and the relative nutritional importance of different FGs a household consumes. The FCS is measured based on a weighted sum of food frequency of 9 FGs consumed by a household during the 7 days before the survey. 21 The FCS ranges from 0 to 112, with higher scores representing a higher nutritious value of the household diets.
Other covariates
We include in our regression models other household and individual characteristics and socioeconomic factors that are commonly considered in nutritional studies of children 22 and that could potentially influence child diet. Sex and age of children were included to account for child dietary patterns across these factors, which can impact dietary diversity through cultural behaviors differentiating boys’ and girls’ diets, and/or different feeding practices across age groups. We also tested the total number of household members to control for household size, which may explain much of the underlying diversity of intrahousehold redistribution of food. Mother’s age and education, as well as sex of household member in charge of key decisions for and on behalf of the household members on health matters (subsequently called key decisions-maker), were tested to control for household-level behaviors associated with using available food and resources in the household. Source of drinking water and toilet was the only usable information capturing household wealth and/or access to community WASH services. As proxies of health services in the community, we used the reported status of measles vaccination of the child and if the child had received vitamin A supplementation. In relation to caring practices, we tested child breastfeeding status as well as frequency of child feeding and frequency of milk feeding (besides breast milk) on the previous day. A number of other nonconventional variables were tested as context-dependent explanatory variables. The duration of the household in the IDP settlement, which replicates the length of time the families have been living in a particular place, was included to control for household-level food security stress associated with a longer stay in an IDP camp. Similarly, the cause of displacement was included to capture behaviors associated with a household’s reasons for leaving their original home. Food aid received in the previous 6 months was included to control for the extent to which children achieve minimum dietary diversity thanks to external sources. Women’s registration at a food centre, women’s physiological status, child’s registration at a feeding centre, and child’s possession of immunization card were all included to capture any form of outside assistance that could affect CDD. Finally, we also included the main source of the milk consumed in the household, namely if the milk was purchased with cash or milk was obtained from another source (i.e. community gifts/donations, food aid, bartering, borrowing, and gathering), which may serve as a proxy of income or at least as an indicator of resources available for food-related expenditure within households.
Estimation Strategy
For the analytical statistics and in order to assess the association of the different covariates with MDDC, we used the following logistic regression model:
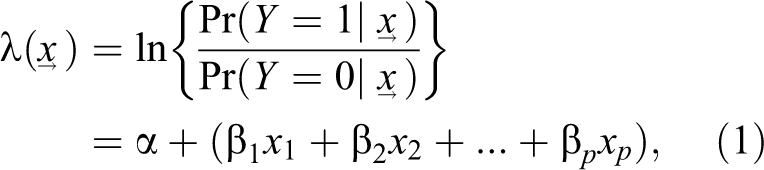
where Y represents the response variable (MDDC) with 2 categories (0, 1) and
Covariates were selected by performing univariate regressions; all variables associated with MDDC at the P < .10 level (see Supplementary Table 1) were included in the multivariable models and tested by using a manual forward stepwise procedure. We use 2 separate model specifications which use interchangeably the HDDS and FCS as food security proxies (subsequently called Model_HDDS, and Model_FCS, respectively). Variables remain in the final models if they were significantly associated with MDDC at the P = .05 level. The final selection of explanatory variables was the same across the 2 model specifications. The IDP camp dummy variables were included to control for unobserved socioeconomic, cultural, organizational, or conflict-related differences.
As many of the variables to be included in the multivariable model were independently associated with the food security proxies, we also performed a stratified analysis based on the HDDS and FCS tertiles. After cleaning for all missing observations in the selected variables, we ended up with a final sample of 1198 and 1190 observations to include in the model_HDDS and the model_FCS, respectively. In order to assess the differences between our analytical samples and the original sample of children aged 6 to 23 months, we compared the distribution of key variables in the 2 samples (see Supplementary Table 2). We observe that the mean age is slightly lower in the analytical sample when compared to the original sample and that fewer children consumed 4 or more FGs or had received vaccination. This implies that in interpreting the results we are most likely underestimating the impact of variables with negative and significant difference in means or overestimating the effect of those indicators whose difference in mean is negative and significant.
To bring additional insight into a comparison of the control variables used in our models including our 2 food security proxies, we also report the Pearson correlation matrix of the covariates used in our estimations (see Supplementary Table 3). The Pearson correlation measures the degree and direction of a linear relationship between 2 variables. Signs and directions of the relationship with pair of data points are all as expected and in line with our regression results.
A variety of sensitivity analyses were also conducted to test the model specification, the best-fitting functional form of all (potential) (note 4). To detect a specification error (that is, when the model has all of the relevant predictors and the relationship between the logit of outcome variable and the independent variables is linear), we used the Stata command linktest (note 5). Similarly, Hosmer and Lemeshow’s goodness-of-fit test, 23 which tests the observed against the expected number of responses using cells defined by the covariate patterns, indicates that our model fits the data well (note 6).
One of the assumptions of logistic regression is the linearity in the logit. To test for linearity in our regression, we used the Box-Tidwell transformation (note 6). In the model where HDDS was the main food security predictor, the test turned out to be significant for nonlinearity. This suggested transformation of this variable, and thus, a tertile variable was created. The same transformation was applied to the FCS variable in order to compare the strength of the correlation of the 2 food security proxy with MDDC.
We also tested influential observations by using the Pearson residual and its standardized version, deviance residual, and the Pregibon leverage (note 7). 24 We identified some extreme observations, but they did not affect the parameter estimates (note 8).
For the descriptive statistics, we used frequencies and percentages to summarize data and describe children’s dietary diversity distribution across key variables like sex, age, and IDP settlement.
Results and Discussion
Sample Characteristics
Table 1 shows children’s characteristics stratified by sex. Out of the 3188 children surveyed, 50.4% were male and the mean age overall was 14.8 months (standard deviation: 5.1), 18% were acutely malnourished (weight-for-height z score <−2) which is above the 15% emergency threshold as defined by the WHO, and 29% stunted (height-for-age z score <−2) which is high according to WHO thresholds and substantially higher than the 10% mean prevalence at country level, 25 reflecting the protracted deteriorated situation of these communities. Global acute malnutrition was significantly higher among boys (20.8%) as compared to girls (15.1%), and only 60% of the children were reported to have received the measles vaccination. Somalia is one of the largest known reservoir of unvaccinated children in a geographic area in the world and experiences recurrent measles outbreaks. 26
Sample Characteristics of 6 to 23 Months Aged Children, by Sex in IDP Camps in Somalia (N = 3188).
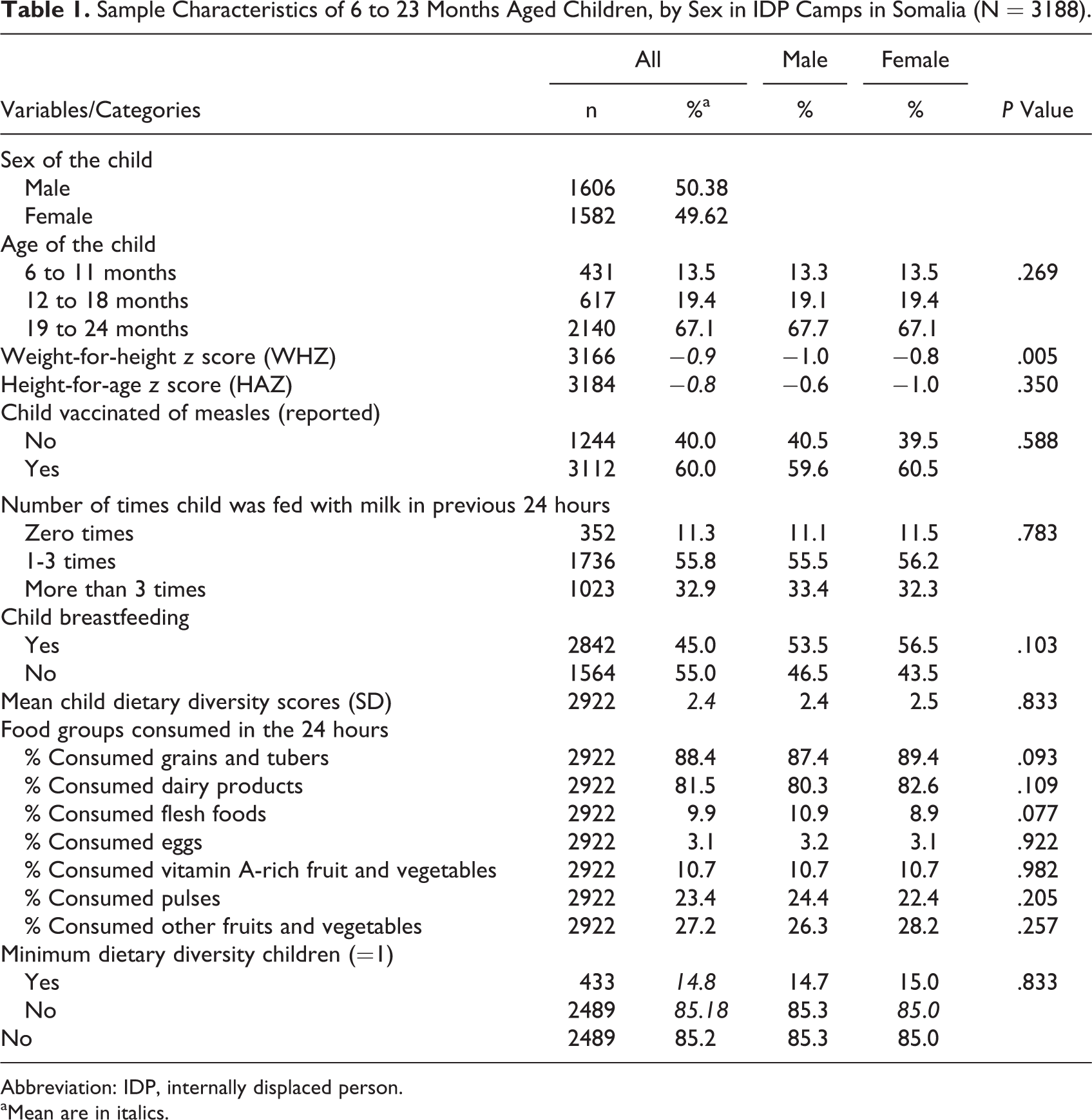
Abbreviation: IDP, internally displaced person.
aMean are in italics.
Household’s food security status was generally low, with a mean of 6 FGs for the HDDS and a mean computation of 58 points for the FCS. In terms of household sanitation, the majority of people living in the camps surveyed have access to protected sources of water, although they lack improved sanitation facilities such as latrines, and they live in congested settlements with poor hygiene, poor waste disposal, and no flush toilets. Most families lived in the camp for more than 1 year, and insecurity, conflicts, and eviction were recorded as the main causes of displacement. Returning to the original home continues to be quite problematic, leading to long-term stays in the camp that on average are over 3 years. Generally, men are the households’ key decision-makers, and from the high proportion of income allocated to food expenditure (81%), milk is the primary food item purchased. Women with education represent only 12% of the overall sample. Food availability through external aid remains critical. Access to camps is often hindered by armed conflicts or disrupted road connections. On the other hand, children’s and women’s health and nutrition services are not very frequently used. The characteristics of sample households are summarized in Table 2.
Characteristics of Households in the Sample With 6 to 23 Months Age Children (N = 3188).
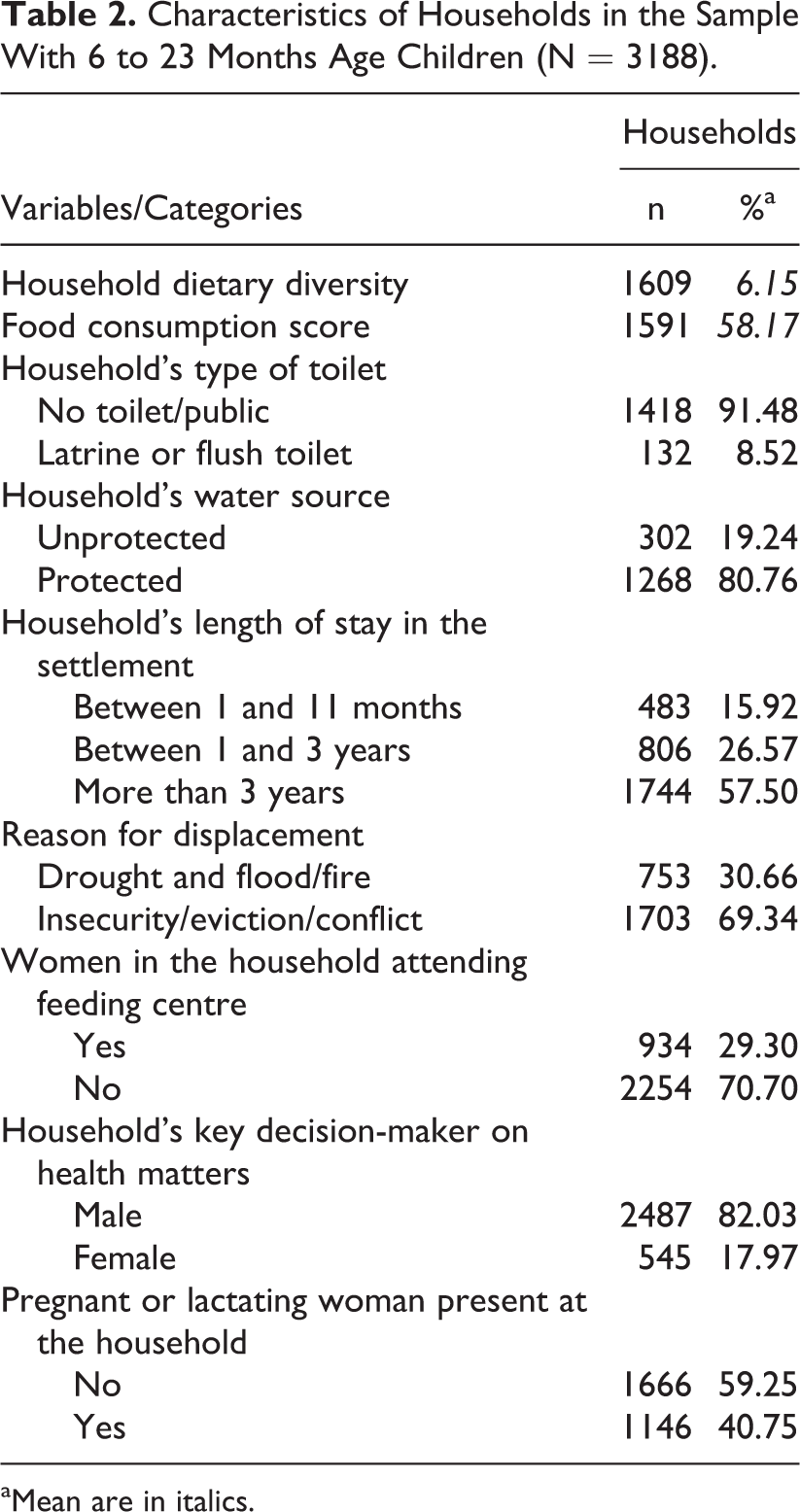
aMean are in italics.
Child dietary diversity characteristics in IDP settlements
The mean CDD was 2.4 FGs, and only 14.8% of surveyed children consumed 4 or more FGs, which is similar to the national mean for Somalia reported in 2016 (15%), but lower than the MDDC given for the IDP population in that particular assessment (22%). In that study we observed that “while more rural dwellers provide the minimum frequency of meals per day to their child than IDPs and caregivers in urban areas, the food provided is the least diverse” (FSNAU, Ministry of Health and UNICEF, 2016). However, the MDDC varied greatly by IDP camp, being above 20% in Mogadishu, Quardho, and Garowe and below 5% in Dusharameb, Dollow, and Galkayo IDP camps (see Figure 1). The highest MDDC was observed in Mogadishu IDP camp (27%) and may be explained by the fact that it is located in the capital city, where labor opportunities for IDP communities are much higher than in other areas, and also where more NGOs and agencies operate, concentrating humanitarian assistance and other type of interventions. Quardo and Garowe camps are located in the Northeast zone, where political situation is more stable and security has improved resulting in better conditions and increased interventions in relation to other areas. On the other extreme, the 1% of children reaching MDDC in Dusharameb camp may be related to cultural practices, as it is an IDP camp mainly comprised of pastoralists feeding children mainly with milk and cereals and also to the Al-Shabab presence in the area which limits any kind of humanitarian assistance or intervention. The case of Dolo camp (MDDC = 1.6%) can be explained by its location on the boundary with Kenya and Ethiopia in an area where fruits and vegetables are very limited, food prices very high, and food aid baskets consisted mainly on cereals.
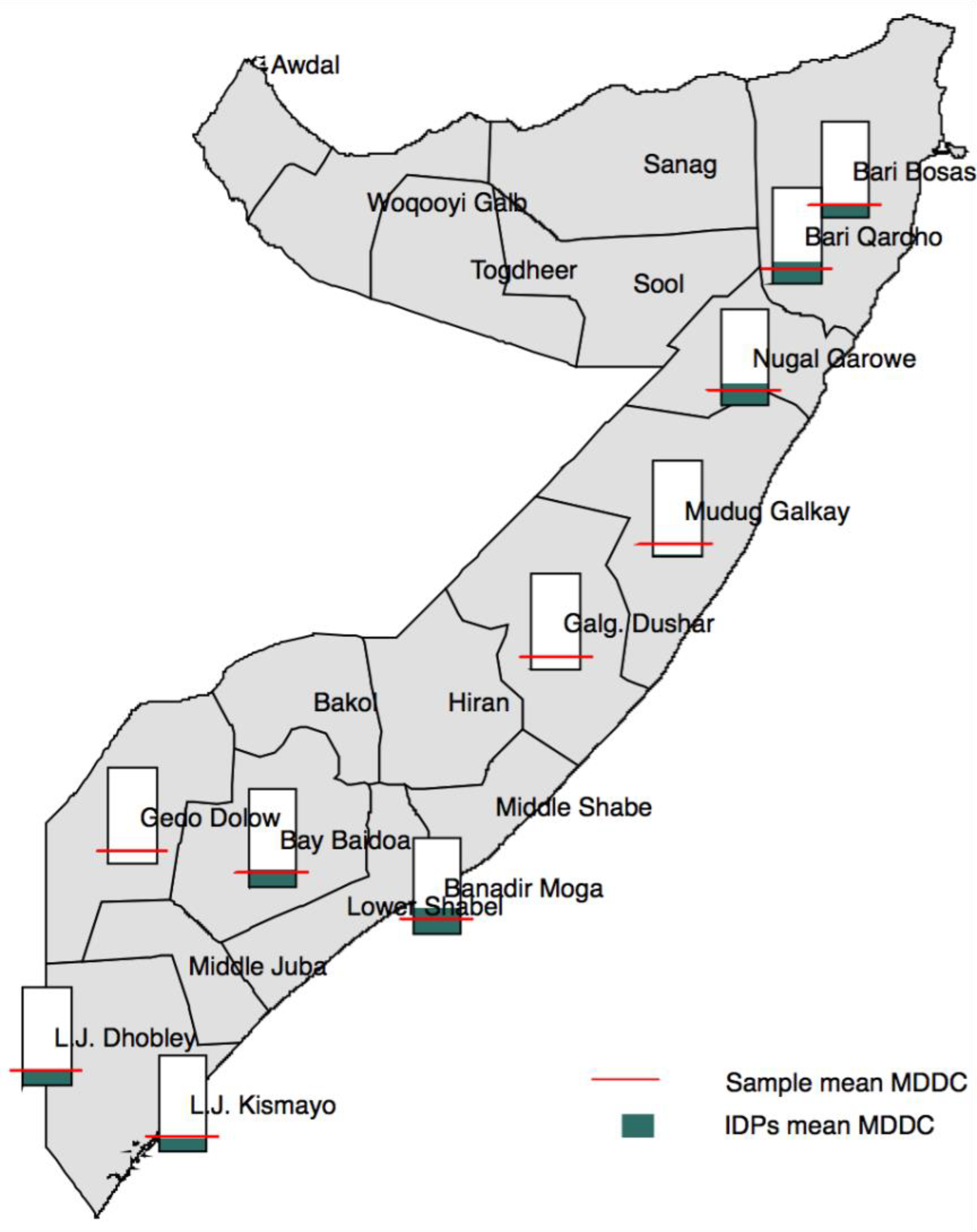
Share of minimum child dietary diversity in children aged 6 to 23 months across studied areas.
For the overall sample (IDP camps populations pooled), there were no differences in the number of FGs consumed by sex, but the proportion of children reaching the MDDC increased with age, being 11.5% for children 6 to 8 months old, 14.0% for children 9 to 11 months, and 15.7% for children 12 to 23 months, although not significantly. Looking at the distribution of CDDs by age-group (Figure 2), we note that, regardless of age, the majority of children surveyed consumed 2, or at most 3, FGs.
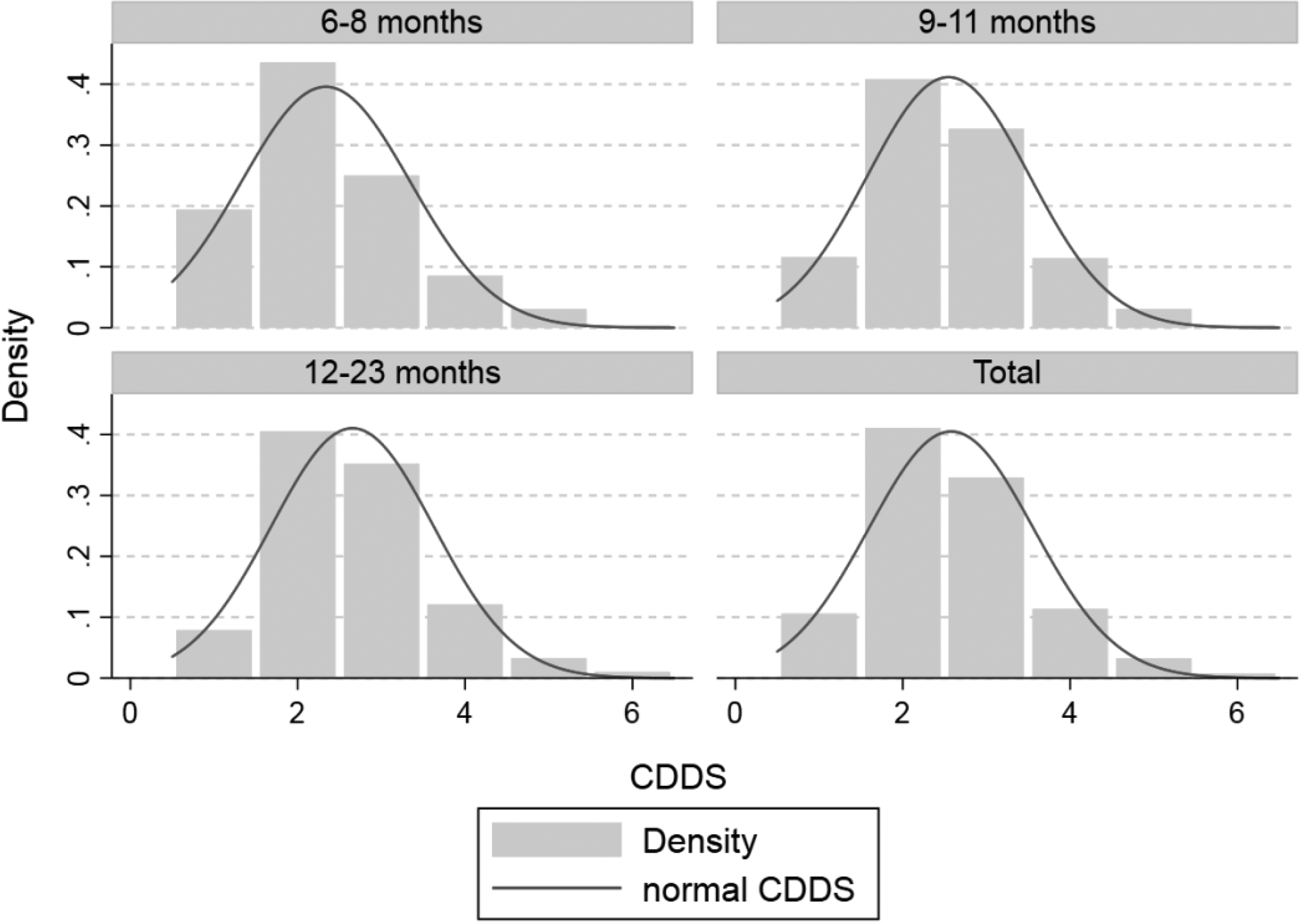
Distribution of child dietary diversity score (CDDS) by age groups.
Overall, the FGs more frequently consumed were the grains and tubers and the dairy (88.4% and 81.5%, respectively) followed by far by the legumes and nuts FG consumed by 23% of the children. The grains and tubers, the legumes and nuts, and the flesh (mainly consisting of meat in this context) FGs were consumed more frequently with increasing age (see Figure 3), and meat was also more frequently consumed by boys than by girls (Table 1). On average, meat accounted for about 10% of food consumed across the 3 age groups, while pulses or nuts accounted for 19%, 23%, and 25% among children aged 6 to 8 months, 9 to 11 months, and 12 to 23 months, respectively. In particular, we observed that pulses were eaten predominantly by children consuming 3 FGs and were mainly present in the diet of children who did not reach MDDC (67%, compared with 33% of those reaching MDDC). Dairy (mainly represented by milk consumption) is the second main FG consumed among all children. On average, more than 85% of children in the sample consumed milk, above the national mean of 75.2% found in 2016. 26
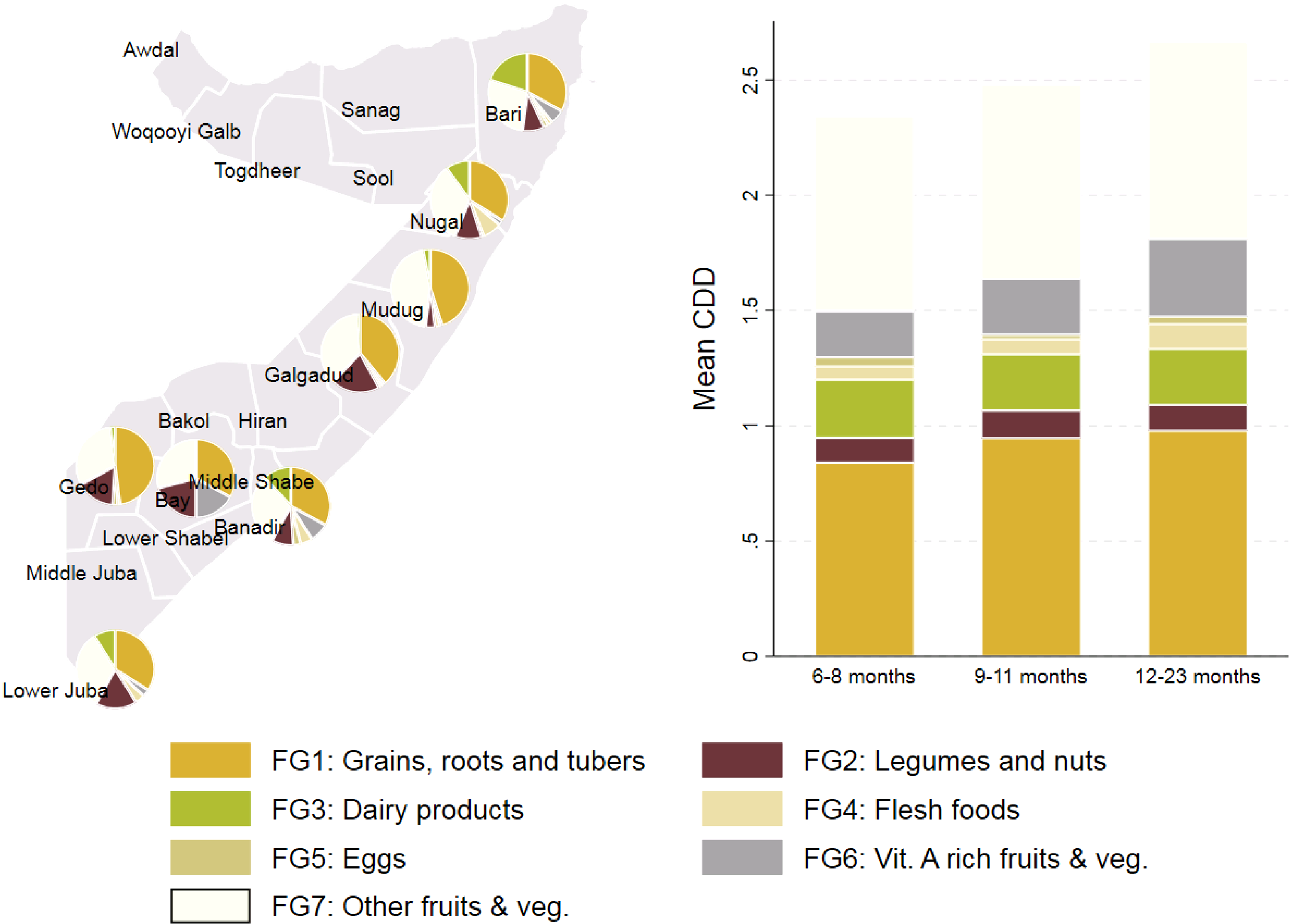
Share of food groups consumed by regions and age groups.
However, FGs’ consumption is not homogenous across the different regions. In Figure 3, we have pooled the IDP settlements data by region. Although there is no substantial difference in grains or milk consumption, children in the central-northern part of the country consume less pulses and legume than those in the southern/southern-west part. This is consistent with the results of the national 2016 Somali infant and young child nutrition assessment, which found the same distribution of pulses/nut consumption across regions in the overall population. Consumption of eggs is very low in all areas, and in Bay, it is completely absent. Similarly, meat consumption is relatively low in the studied population. The highest level occurs in the IDP camps located in Nugal, Banadir, and Lower Juba, where about 15% the children eat meat, although for those IDP camps located in Bay, Gedo, Galgadug, and Mudug, the reported consumption is below 5%. On the contrary, in Gedo, less than 2% of children eat meat. Figure 3 summarizes these results. Consumption of fruits and vegetables was low overall, especially in relation to vitamin A-rich fruits and vegetables (10%); in IDP settlements located in Gedo, Galgadug, and Mudug, less than 5% of children consumed food items from this FG. The highest consumption of all types of fruits and vegetables was observed in Banadir region where Mogadishu IDP camps are located, in the IDP camps in the Bari region, probably related to the closeness of the Bosaso IDP camp to the port and increased access to diverse foods, and in the region of Bay where most of the riverine, agricultural communities in Somalia are concentrated.
Dietary diversity-associated factors
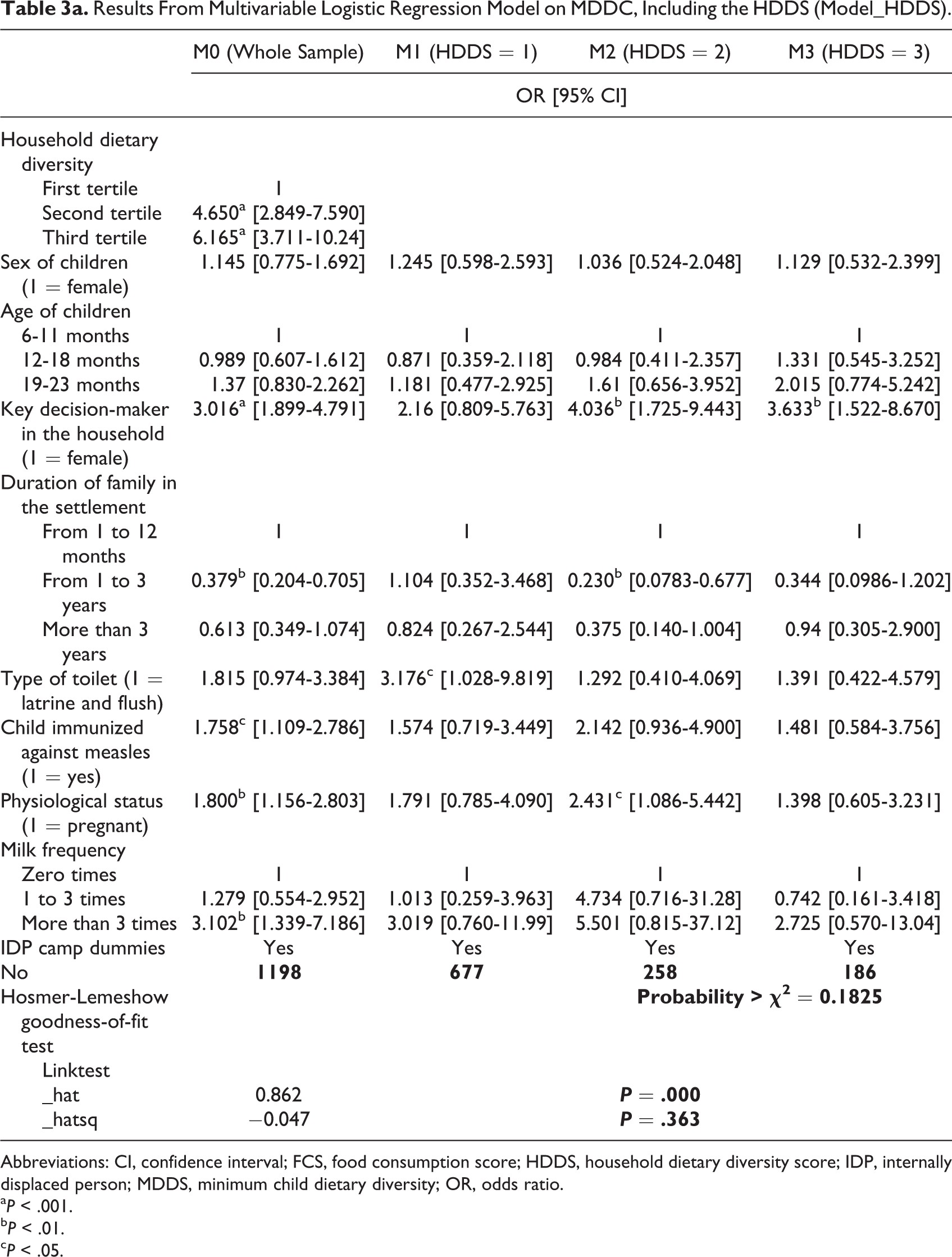
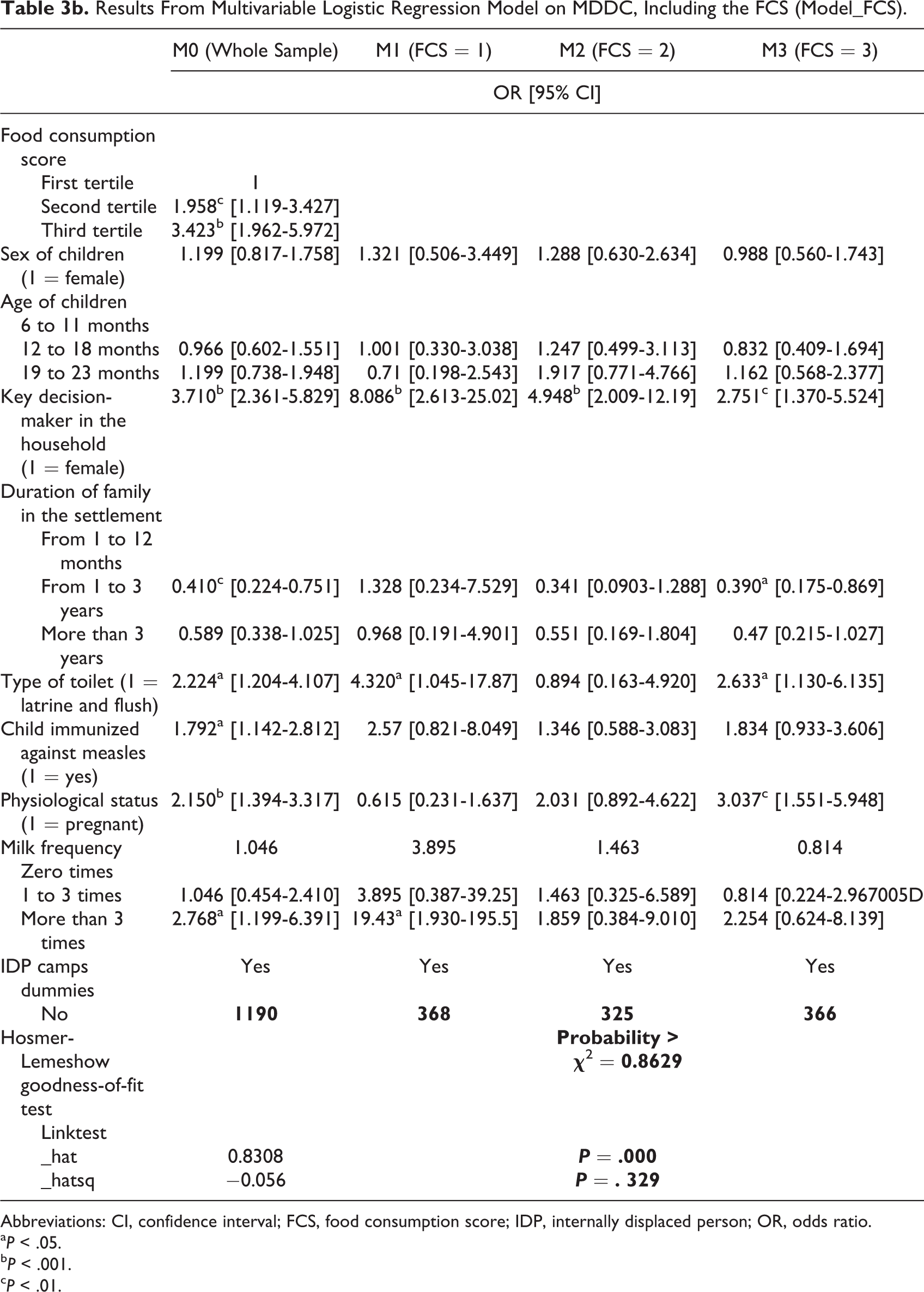
Tables 3a and 3b present the results of the logistic regression models. The first column of the tables show the results for the whole sample (without stratification), and the last 3 columns compile results of the model for each of the strata (HDDS and FCS tertiles, respectively).
Results From Multivariable Logistic Regression Model on MDDC, Including the HDDS (Model_HDDS).
Abbreviations: CI, confidence interval; FCS, food consumption score; HDDS, household dietary diversity score; IDP, internally displaced person; MDDS, minimum child dietary diversity; OR, odds ratio.
a P < .001.
b P < .01.
c P < .05.
Results From Multivariable Logistic Regression Model on MDDC, Including the FCS (Model_FCS).
Abbreviations: CI, confidence interval; FCS, food consumption score; IDP, internally displaced person; OR, odds ratio.
a P < .05.
b P < .001.
c P < .01.
Overall, the HDDS and the FCS were significantly associated with CDDS, with HDDS showing a stronger association. The results of Model_HDDS reveal that the log odds of having better child dietary adequacy increased by 6.2 when moving from the first to the third HDDS tertile and an increase of 3.4 when moving from the first to the third FCS tertile. One of the reasons for this higher correlation between HDDS and MDDC may be the fact that HDDS is collected on the previous 24 hours and is constructed by simple FG count, whereas FCS recalling period is 7 days, and its construction takes into account additional weights. In both models, children living in households with access to latrines or flush toilets were found to be 2 times more likely to reach MDDC. Sanitation in Somalian IDP camps is one of the main WASH problems (in our sample less than 10% of households had access to any type of toilet), and thus, the positive association may be seen as an effect of a proxy of settlement quality services.
The other variables significantly associated with MDDC in the multivariable analysis were household key decision-maker, women’s physiological status, the duration of the household in the settlement, the frequency of milk feeding to a child in the previous 24 hours, and child’s measles vaccination. These findings may reflect the fact that if women, who are generally responsible for distributing food in the household, are empowered to make key decisions, this contributes to improving the diet of children in the family, as has been shown in other contexts. 27 Notwithstanding, as from other study, 28 sensiting of man in nutritional needs of children can also enhance CDD.
In Table 3a, we can observe that the association with key decision-maker variable is stronger among households with high household dietary diversity, suggesting that women empowerment may have more impact on CDD in contexts of appropriate food access. In the Model_FCS (Table 3b), we see that women as key decision-maker can increase up to 5 times the likelihood of the children to reach MDDC as compared to the 3 times among households in the high tertile of FCS. This result suggests that the role of women as key decision-maker has a greater impact on households of low FCS.
Similarly, children in households where there are pregnant or lactating women were more likely to have an adequate diet. For these children, the odds of a more adequate diet were about 1.8 and 2.2 times higher than for those living in households with nonlactating nonpregnant women for Model_HDDS and Model_FCS, respectively. This positive association might reflect sociocultural, as well as internal household dynamics that may favor appropriate food consumption of pregnant and/or lactating women 29 and also implementation of interventions targeted to households with pregnant/lactating women (like the World Food Program and UNICEF food aid programs).
Staying in a camp for a period of 1 to 3 years has quite a strongly negative impact on the log odds of reaching MDDC relative to staying in a camp for a period of 1 to 11 months. This result supports the notion that people entering the camp for the first time might have better supplies than those who have lived there for a long time, and thus, they may be better equipped to cope with declines in food availability without having to sacrifice the nutrient adequacy of vulnerable family members. Moreover, new arrivals that are generally registered in the camp receive food assistance and/or other commodities for 3 months, whereas longer term IDPs are no longer eligible to receive that aid.
The number of times the child was fed with milk on the previous day was highly correlated with MDDC suggesting the role of caring practices in a context where milk is one of the main food items of children’s diet. Finally, measles vaccination was also positively associated with MDDC, which can be interpreted as a proxy of the effects of interventions directly targeting children on their diet, independent of the household food security status and intrahousehold caring practices provided.
Family size, child age and sex, reason for displacement, food aid received, source of drinking water, household women’s age or education, vitamin A supplementation, child breastfeeding, and mother or child registration at feeding centers were not statistically significant in these regression analyses. An examination of the underlying data shows that rates of registration at feeding and/or food centers among children and/or women were generally low. This may be because these centers are located not within the IDP camps but in urban areas, so people have to travel long distances to access them. However, recently (in the last 2 years), mobile units have been set up to reach these IDP communities.
Limitations
The authors recognize the limitations of using the FSNAU data set. Indeed, although the survey was carried out in waves among different IDP settlements, data on food consumption were not consistently collected. This analysis thus drew only from the pooled cross-sectional sample of households so as to take advantage of a larger sample size and ensure that all livelihood areas in the country were included. This prevents us from drawing a pattern of the observed relationships or causality of our estimation. In addition, we are aware that we are providing an overview of the relationship between household food consumption and child dietary intake for the IDP populations overall, although we acknowledge that the reality may change according to the specific characteristics of the IDP camp in our study.
Conclusions
The CDD among IDP populations in Somalia is low (15%), and it varies greatly within IDP settlements, reaching 27% in Mogadishu and less than 5% in other southern IDP camps. Most children consume 2 or 3 different FGs, being the most frequently consumed the basic staples and the dairy products (mainly fresh milk). Consumption of fruits, vegetables, and eggs is extremely low, thus we suggest the implementation of strategies aimed at promoting its consumption, as a way to increase the diversity of the diet.
Using data from FSNAU among 10 IDP camps across Somalia in the years 2014 and 2015, we found that the 2 household food security proxies, HDDS and FCS, showed the strongest association with the CDD, and the HDDS even more.
Other major factors that positively influence CDD include living in households where women are key decision-makers on health matters or in which there are pregnant or lactating women.
We recommend that projects strengthening gender equality and women’s empowerment should be embedded in the day-to-day running of camps. Any action promoting this aspect should be an integral part of camp-level governance.
Economic opportunities for women, access to basic services such as health, and the implementation of education in parallel with behavioral change communication activities on optimal child feeding practices, targeting both women and men, are what should be promoted.
Our findings also suggest that local governmental and nongovernmental organizations should be encouraged to implement long-term interventions for supporting families to achieve diverse diets, which could benefit children’s nutritional status, beyond the food assistance provided during the first month of arrival.
Supplemental Material
Supplementary_material - Child Dietary Diversity and Associated Factors Among Children in Somalian IDP Camps
Supplementary_material for Child Dietary Diversity and Associated Factors Among Children in Somalian IDP Camps by Federica Di Marcantonio, Estefania Custodio and Yusuf Abukar in Food and Nutrition Bulletin
Footnotes
Acknowledgments
The authors gratefully acknowledge FSNAU for sharing the data used in the analysis and Francois Kayitakire for supporting this research.
Author Contributions
Federica Di Marcantonio, the corresponding author, designed and supervised the study, ensured the quality of the data, performed the analysis, and drafted the manuscript and was responsible for submitting the manuscript for publication. Estefania Custodio made a substantial contribution to the implementation of the study assisted in the conception of the study as well as in the analysis and interpretation of the data and critically reviewed the manuscript. Abukar Yusuf contributed to the conception of the study and the interpretation of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Supplemental Material
Supplemental material for this article is available online.