
Abstract
Background:
Overweight/obesity during adolescence in lower-middle income countries has become a public health problem with consequences in adulthood. Inadequate dietary habits, poor diet quality, sedentary behavior, and parental obesity have been reported.
Objective:
To describe management of obesity-like food habits and behavior of adolescents from lower-middle income countries with respect to what keeps them using this diet (barriers) and what helps them avoid it (enablers).
Methods:
Systematic review of the literature related to obesity and food intake of adolescents conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
Results:
We classified 11 eligible studies describing the barriers to and enablers of the management of obesity-like food intake and obesity lifestyle. The dual burdens of malnutrition and increased urbanization have been observed. There is preference for processed food, dietary habits, and obesity-like food intake and sedentary behavior. Barriers to managing body weight gain included mostly consumption of fast-food and snack food, less vegetable and fruit intake, skipping meals, and sedentary behavior. Enablers of managing body weight gain included changes in nutritional habits, perception of the consumption of healthy food, physical activity, and engagement in programs to change lifestyle.
Conclusion:
The globalization of the fast food industry has provided an obesogenic environmental stimulus for adolescents in lower-middle income countries.
Introduction
The consequences of the demographic, epidemiologic, and nutritional transitions in developed countries have been well described. 1 Conversely, related sets of this transition are also occurring in lower-middle income countries. Undernutrition has commonly been the nutritional concern of those countries, but changes in the composition of diet, food habits that have replaced traditional diets, globalization, rapid urbanization, and physical inactivity have led to the coexistence of under- and overnutrition in the lower-middle income population. 2 -4 This phenomenon is known as a “dual burden” and may manifest within a community, household, or individual. 5 This dual burden has been observed in a number of countries with consequences for both adults and children/adolescents. 6
The classification of a country as lower-middle income is according to 2016 gross national income (GNI) per capita using the World Bank Atlas method. 7 Lower middle-income economies are those with a GNI per capita between US$1,026 and US$4,035; upper middle-income economies are those with a GNI per capita between US$4,036 and US$12,475; high-income economies are those with a GNI per capita of US$12,475 or more. 7 Most of the lower-middle income countries are in Latin America, Africa, the Middle East, and Asia. 7 Previous studies have assessed secular trends in the nutritional status of children as indicators of overall population health; trends in each country reflect its progression through the nutritional transition. In South African children (ages 8-11 year) from primary school, there was a reduction in mild and moderate stunting followed by an increase in overweight/obesity between 1994 and 2004. 8 In Mozambican children/adolescents (aged 8-15 years), there was a reduction in malnourished youth together with an increase in the prevalence of overweight and obesity between 1992 and 2012. 9 A recent systematic and meta-analysis review described differences in the obesity and undernutrition according to the national income level and the consequences of a cumulative exposure to an obesogenic environment. 2 The problem of overweight and obesity in adolescents in developing countries has been neglected mostly because of an erroneous traditional belief on the part of the population concerning nutritional habits, as well as specific sociocultural perceptions regarding nutrition, gender, and parental obesity.
The National Institute of Health and Clinical Excellence has published guidelines for the prevention and management of overweight/obesity and described barriers and enablers that adolescents with obesity encounter for healthy nutrition, physical activity, sedentary behavior, and sleep habits. 10 Despite recognition of the issues concerning nutritional transition in lower-middle income countries, studies are few in the literature on the barriers to and enablers of the management of body weight gain, eating-related habits, and behavior leading to overweight/obesity in adolescents. Thus, this review will discuss studies on food intake and habits of adolescents living in lower-middle income countries. This review will describe management of obesity-like food habits and behavior of adolescents with respect to what keeps them using this diet (barriers) and what helps them avoid it (enablers). Specifically, this systematic review aims to examine the risk of an obesogenic environment in lower-middle income countries and the relationship to nutritional transition.
Methods
This is a systematic-review of the literature related to obesity and food intake of adolescents from lower-middle income countries conducted according to the Preferred-Reporting-Items-for-Systematic-Reviews-and-Meta-Analysis statement. The search was conducted in August 2018 in the electronic databases MedLine/PubMed, Cochrane Library (Wiley; 2000-2018). The following terms were used (including “entry terms” like synonyms, derivation of theme and closely related words) as index terms or free text words: body weight changes OR body weight OR obesity OR overweight AND attitude OR attitude to health OR perception OR body image OR awareness OR behavior OR adolescent behavior OR health behavior OR personal satisfaction OR lifestyle OR feeding behavior OR food preferences OR motivation OR achievement OR drive OR goals OR intention OR primary prevention OR motivation OR food habits OR barrier OR enabler AND diet OR food OR beverages OR sugar sweetened beverages OR discretionary food OR take away OR eating OR nutrition AND adolescent OR adolescents OR teenage OR adolescence OR students. The complement of the search was performed using all countries listed in the 38th Annual Conference of the International Society for Clinical Biostatistics.
Eligibility Criteria
The criteria for inclusion were published original articles conducted with adolescents (aged 10-19 years); low-middle income countries with multidimensional poverty above 30%; articles with themes of overweight and obesity; data from the habits and/or food consumption and lifestyle. Articles were excluded when chronic diseases were also evaluated, such as diabetes, hypertension, mental deficiency, and pregnant or lactating adolescents.
Study Selection
Titles and abstracts of the articles were read during the screening phase by an independent reviewer for the selection of relevant studies. After this screening phase, the eligible articles were chosen after reading the full-text for possible inclusion in the systematic review.
Data Extraction
The extraction and check of the data were carried out by 2 reviewers. The extracted data included lower-middle income countries, and descriptions of dietary habits, specifically in adolescents.
Results
A total of 225 papers were identified in the initial search. Some papers were excluded on the basis of the following factors: range of age related to adolescence, country not on the list of lower-middle income countries, no information on nutritional habits, sample did not include obesity/overweight (Figure 1). Thus, 11 papers published between 2001 and 2018 met the inclusion criteria. The majority of these studies had been carried out in India. 11 -16 Some countries, for example, Sudan, 17 Nigeria, 18 Lesotho, 19 Yemen, 20 Ghana, and Uganda, 21 were also represented in this review. Studies were moderate in quality because of the small size of the sample. Cross-sectional design study and questionnaires about food frequency (24 hours recall), socioeconomic status, sedentary and physical activity behavior, alcohol consumption, and smoking were used. Studies included both genders with ages between 10 and 19 years (Table 1).
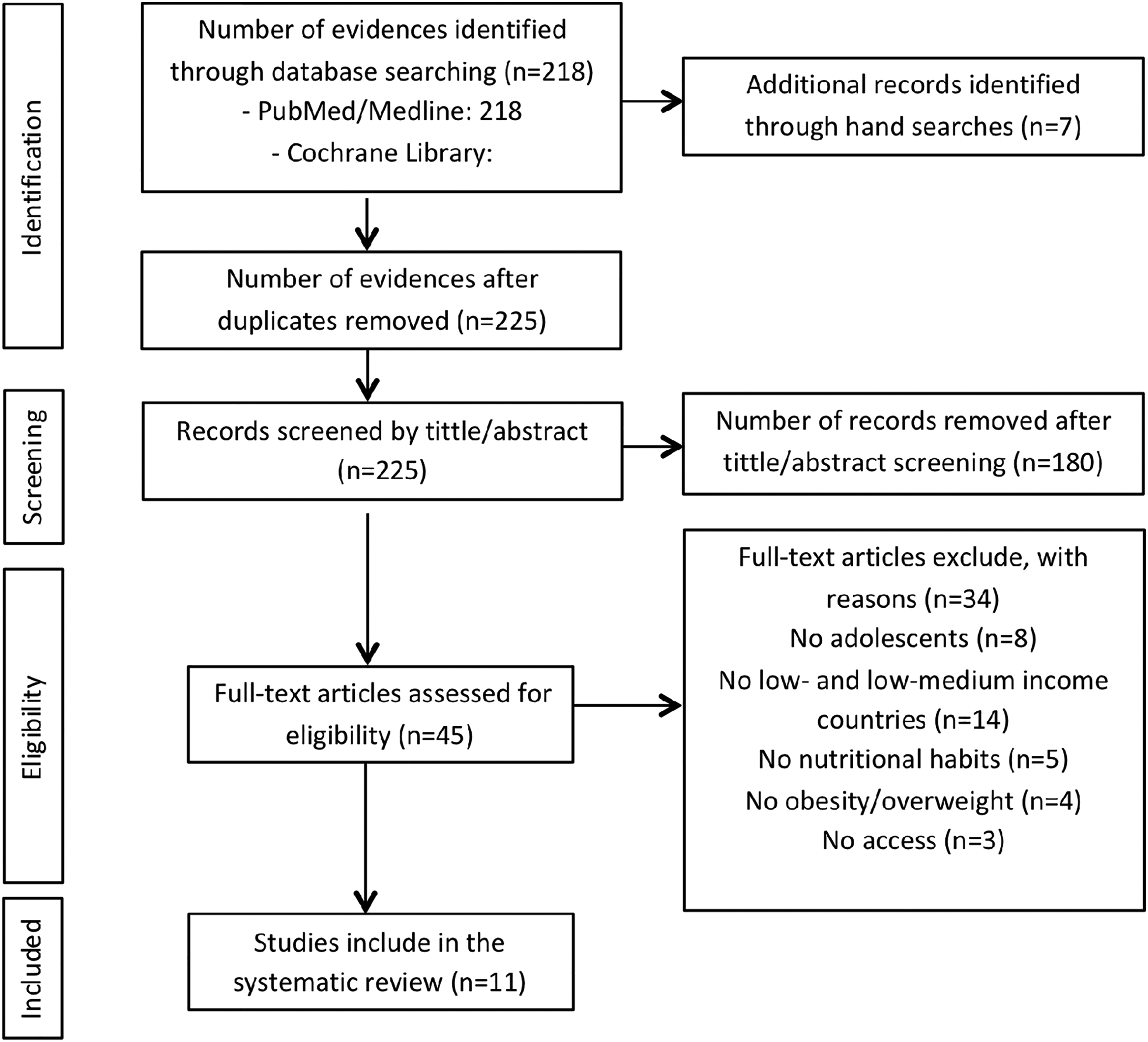
Flow of articles in the review process.
List of Studies That Were Eligible for Inclusion.a
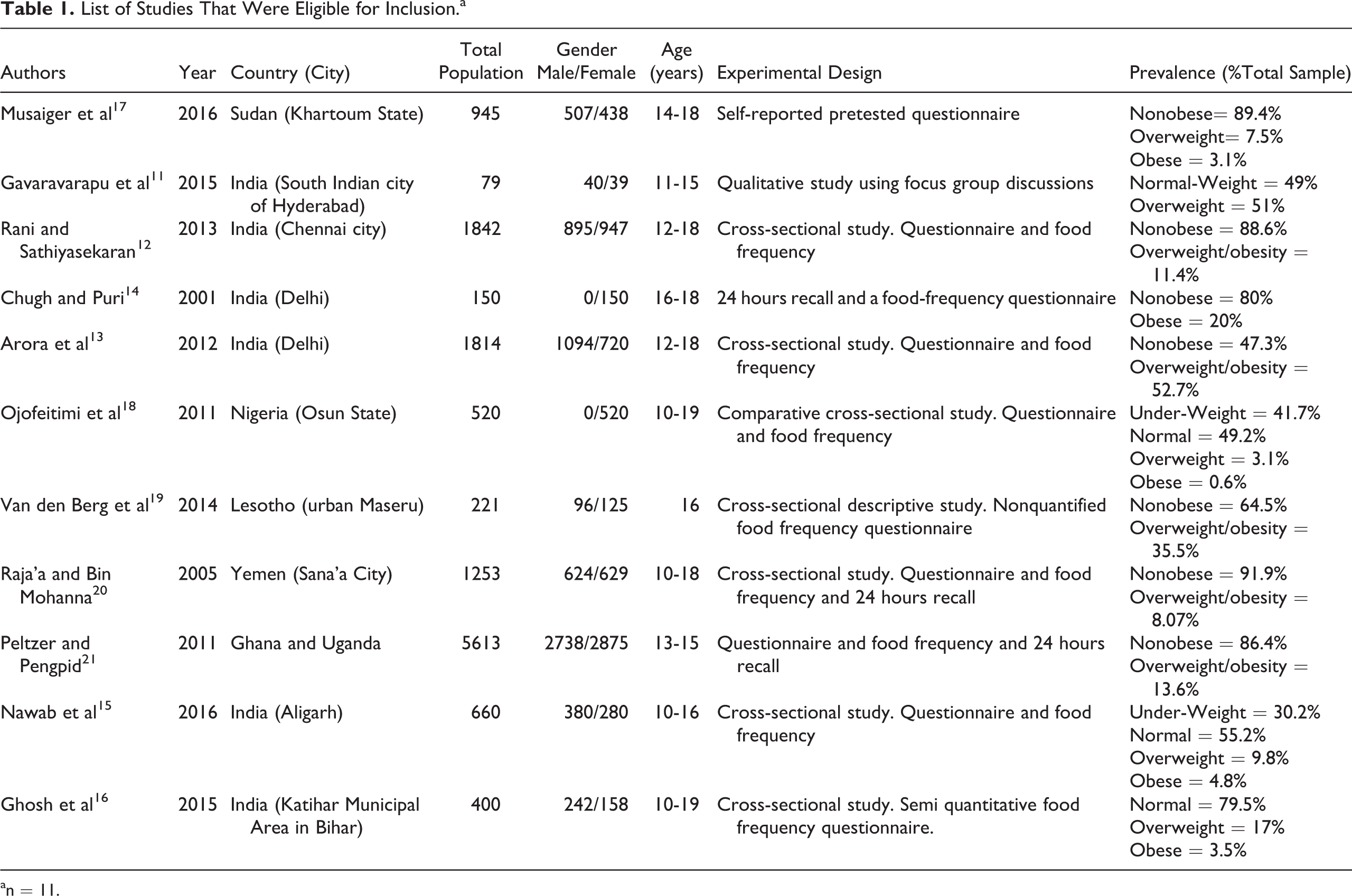
an = 11.
Regular consumption of fruit, vegetables, and healthful nutrients, one or more times per day was reported by most studies; however, overweight or adolescents with obesity self-reported low or very low consumption of nutritionally healthy foods. On the other hand, all studies reported the high consumption of food rich in fat, sugar, and salt among adolescents of both genders. Time spent on TV/computer for more than 2 hours per day was seen in all studies. In addition, outdoor activity, sports participation, and physical education programs were minimally evident among adolescents with overweight or obesity in the selected studies. There was a significant positive association to the parental education level, parental obesity, alcohol consumption, and overweight/obesity adolescence (Table 2).
Barriers and Enablers Quoted From Articles.
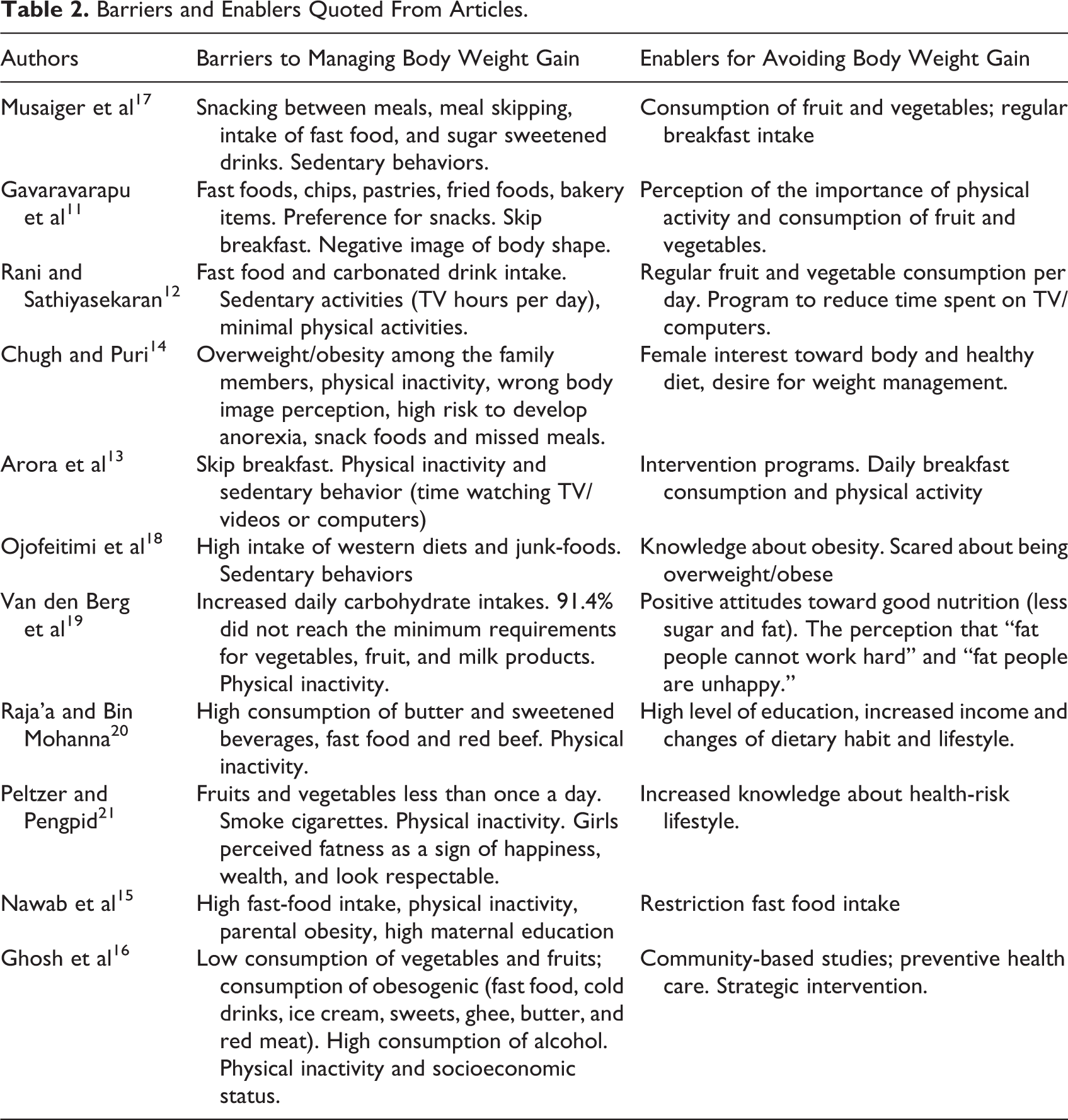
The detection of the barriers to and enablers for the management of the overweight/obesity condition of adolescents are summarized in Table 2. The barriers included chiefly the consumption of fast-food and snacking foods, less vegetable and fruit intake, skipping meals, and sedentary behavior. Enablers for weight management included changes in nutritional habits, perception of the consumption of healthy food, engagement in physical activities, and programs to change the lifestyle of adolescents. The prevalence of adolescents with overweight/obesity in the selected studies ranged from 3.7% to 52% of the sample.
Discussion
Adolescence is a critical period of development with large physical, chemical, and emotional changes. 22 Nutritionally adequate diets, physical activity, and psychosocial factors are determinants for growth/development and the prevention of noncommunicable diseases in adulthood. 23 Adolescents are relatively autonomous in their food habits and largely influenced by their social group. 24 -26 Skipping meals, snacking, consuming sweetened drinks, using an excess of salt, and eating junk and processed foods are common features of the diet of adolescents in developed countries, where most of the studies have been conducted. 23 -25 In lower-middle income countries, increasingly some of these food habits are being observed as having the same characteristics of habits of consumption as in developed countries. 12 -14,20 Conversely, a high proportion of adolescents classified as inactive or minimally active has also been observed. 9,12 There is scarce research available, however, on the dietary intake and lifestyle of adolescents in these countries. We found only 11 studies conducted in lower-middle income countries that assessed the food habits, lifestyle, body image, and issues for the management for overweight/obesity in adolescents.
The selected studies reported the high consumption of snacking, missed meals and unhealthy eating behavior, although the participants had information about the importance of vegetables and fruit and weight management. In the selected studies, participants with obesity did not follow the recommended dietary allowances in terms of micronutrients and fiber. Preferences were for high fat and carbohydrate diet. In Lesotho, for example, the reported diets of majority of the adolescents from Basotho did not reach the nutritional recommendation for energy, carbohydrates, fiber, fat, fatty acids, cholesterol, protein, and amino acids. 19 Additionally, 221 adolescents were evaluated in terms of dietary intake and around 85% of these did not meet the minimum daily requirements for vegetables, fruit, milk, and milk products. A elevated percentage of adolescents (74.7%) reported a high daily intake of starchy foods and energy derived from carbohydrates. 19
The existence of overweight/obesity during adolescence in lower-middle income countries may be related to the inadequate nutritional habits and poor diet quality followed by overload in energy intake in later childhood. 17 In India, a dose–response relationship was demonstrated between breakfast consumption and being overweight and obese among adolescents in private schools. 13 A qualitative study 11 showed that adolescents are concerned about “good nutrition,” but they are confused about how to elaborate the answer and just consider eating vegetables and fruit enough to maintain good health. 27 It seems that children and adolescent are abandoning traditional diets in exchange for low cost energy-dense foods, refined carbohydrates, sweetened carbonated beverages, and diets low in polyunsaturated fatty acids. The consumption of processed foods, sugar, and sodium may be involved in the early development of chronic diseases in children/adolescents and adult obesity. 17
Sedentary behavior, time spent on TV/computer, psychosocial determinants, and body shape perceptions are also factors that can explain the increase of overweight/obesity in lower-middle income countries. 9 Simultaneously, increased indoor leisure activities and entertainment (TV shows, computer games, and social interaction on cellphones), insecure neighborhoods, and lack of open spaces in communities are causing children and adolescents become sedentary. 17 The selected studies identified the minimum or no physical activity, and 2 to 4 hours per day of TV/computer in almost all adolescents with overweight/obesity. The time spent by watching TV can negatively influence patterns of feeding behavior. 28 Inadequate levels of physical activity per day may increase the risk of metabolic diseases such as hypertension, diabetes type II, and dyslipidemia. 1 However, because it is difficult to classify the level of physical activity, sedentary behavior seems to be the better marker of a risk factor for obesity in adolescents. 9,29
The recognition of enablers for and barriers to dietary management contributes to a change in dietary and lifestyle habits among adolescents. The selected studies outlined the significant role of alcohol consumption and smoking as barriers to the management of a healthy diet, contributing to the adolescent’s overweight. Around 1.4% of the Bosotho adolescents reported drinking 14 to 21 units of alcohol per week. 19 In India, there was significant association between alcohol consumption and occurrence of overweight/obesity (4.98 times). 16 Similarly, smoking cigarettes and loneliness were associated with overweight or obesity in girls from Ghana and Uganda. 21 Lower socioeconomic status and parental history of obesity were also considered as barriers to weight management and there was an association to the incidence of overweight/obesity. 12,20 In some studies, the enablers for dealing with obesity and overweight included awareness that physical activity is related to good physical form and health. 11,13,14 A substantial proportion of studies related 40% to 75% of the adolescents studied showed basic knowledge about nutrition and a negative attitude toward overweight and/or obesity. In India, higher maternal education level was associated (3.1 times) with overweight and obesity among adolescents. 15
Previous studies have shown that in both developed and developing countries, there are patterns of behavior associated with urbanization and nutritional/epidemiological transition. 2,30 -32 Together, these contribute to increased overweight/obesity in the lower socioeconomic groups of lower-middle income countries where the fight with undernutrition continues, even as the population suffers an increase of obesity and overnutrition. For example, Sudan is one of the poorest countries in the world and preschool children in a rural area of Northern Sudan suffer from poverty and food insecurity. 33 However, in urban areas, there is a situation of 7.5% of overweight and 3.1% of obesity among Sudanese adolescents. 17 In Ghana and Uganda, the situation of overweight or obesity was 10.4% among girls and 3.2% among boys. 21 In Yemen, the overall occurrence was 8.07% of overweight and 6.2% of obesity. 20 Using the body mass index, the condition of overweight and obesity in Nigeria was around 4.0%. 18 These situations, however, are not very high compared to developed countries, and the “dual burden” is clearly identified due to the widespread poverty in these lower-middle income countries, where about 70% of the population still live below the international poverty line of US$1.25 a day. In the present review, problems have been highlighted that need to be targeted through intervention studies with educational programs in order to address the early appearance of metabolic and cardiovascular diseases in adulthood in low-middle income countries.
The limitations of the present review include the small number of eligible studies that may not be representative of description of the problem of overweight and obesity in adolescents in all lower-middle income countries. In addition, most of the studies (6 of the 11 studies) reviewed were from India which makes difficult the intercultural comparisons. The differences in the methods used across the 11 studies (self-report; focus groups; food frequency questionnaires; 24-hour recall) did not allow a precise interpretation of data.
Conclusion
The present study reviewed 11 articles that describe the problem of overweight and obesity in lower-middle income countries. Meal skipping, high consumption of fast-food and soft drinks, low consumption of green vegetables, tubers, legumes and roots, as well as sedentary behaviors, minimal practice of physical activity, parental obesity, and socioeconomic status were associated with obesity. These data may serve to increase understanding of the emerging problem of overweight/obesity among the youth in developing countries where emphasis is generally given only to the prevention of undernutrition. In addition, the small sample of studies that were eligible for this review is indicative of the scarcity of existing literature on the participants. Thus, it is important to encourage dietary-habits surveys to assess the full extent of the consumption of processed food, increase of the fast food industry, and the power of media advertising on the adolescent lifestyle. The findings of this study are thus important in guiding future studies that will focus on nutrition interventions to address the recovery of healthy and traditional foods in this population group.
Footnotes
Authors’ Note
Mario Eugénio Tchamo is also affiliated to Research Center for Sports and Physical Activity and Health in Mozambique (CIDAF).
Acknowledgments
This study was supported by National Council for Scientific and Technological Development (CNPq), Coordination for the Improvement of Higher Level or Education Personnel (CAPES) and State of Pernambuco Science and Technology Support Foundation (FACEPE). The English text of this article has been revised by Sidney Pratt, Canadian, MAT (The Johns Hopkins University), RSAdip–TESL (Cambridge University).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.