
Abstract
Background:
In Thailand, despite widespread improvements in child nutrition, stunting is still highly prevalent among northern hill tribe children.
Objective:
To understand how villagers and health workers (volunteers and officials) gauge health of children younger than 5 years, whether growth monitoring is salient, and the relationships of villagers with the health system in this remote location.
Methods:
Qualitative research was undertaken with 8 hill tribe villages. A workshop on infant and young child health and nutrition was held with 8 village health volunteers, 2 per village, selected by a public health officer. In-depth interviews were conducted with 20 villagers and 2 volunteers who had children 0 to 5 years. Eight other health workers were also interviewed. All dialogue was conducted in Thai through bilingual facilitators and recorded, transcribed, and translated into English. Transcripts were coded and analyzed thematically within and across participant groups.
Results:
Overall, villagers considered strength and independence of children to be hallmarks of health; the size of children featured rarely. Volunteers did not perceive local benefits of growth monitoring, and the extent of child malnutrition was unclear to them. Nutrition counseling was seldom mentioned by villagers or health workers. Across all accounts, and considering silences, relationships of villagers with the health system seemed fragile.
Conclusion:
Villagers understand child health in terms of functional abilities rather than size. Volunteer health workers in this remote location have limited resources and support. Together this helps explain why, against a background of poverty and food insecurity, growth monitoring does not translate to improvements in child nutrition.
Keywords
Introduction
In Thailand, a growth monitoring program for all preschool children was introduced as a part of the second National Food and Nutrition Plan (1982-1986). 1 In the 1980s, undernutrition was common among children aged younger than 5 years, with stunting affecting up to half. 2 Over the next 30 years, stunting was significantly reduced in this age-group, with a prevalence of 16% reported for 2012. 3 The decrease has been attributed to a combination of improvements in household income and in the health system. 4,5
Despite noteworthy advances at a national level, the nutritional status of infants and young children younger than 5 years of age in the northern hill tribes of Thailand has not improved to the same degree. (The official term given by The Ministry of Thailand to the ethnic highlander communities is “Chao Khao,” which translates to “hill people” or more often “hill tribes” and is not considered discriminatory.) Up to two-thirds of children in the hill tribes were stunted in the 1990s, 4,6,7 and recent reports indicate a third are affected, 8 a prevalence considered by the World Health Organization (WHO) to be severe. 9
Elsewhere we have described how women in the hill tribes must return to subsistence farming in distant fields, usually within 3 months of giving birth. 10 This impedes exclusive breastfeeding (EBF) for 6 months, with water and rice mixtures introduced early, partly to allow other family members to care for infants. Bananas, grown locally, are fed to older infants and sometimes eggs, but beyond this, there is little variety in infants’ diets. Poverty and food insecurity mean that the diets of children older than 12 months are also poor. 11
The persistence of stunting also invites consideration of the provision of health services in this remote location, where some villages do not have an electricity supply and the roads to Chiang Mai are frequently unpassable in the monsoon season. Thailand has had a primary health-care strategy that involves both “bottom-up” (from community) and “top-down” (central government) approaches since 1979. 12 Village health volunteers (VHVs) support public health officers (PHOs) in outreach to communities. 13 Villagers who take on the VHV role are given a minimum of 5 days’ training and assist their PHO with duties such as provision of medications, simple health checks, hygiene awareness, and growth monitoring. Each VHV is responsible for 10 to 15 households.
The aims of this study were to investigate perceptions of health of young children (up to 5 years) among parents and caregivers of hill tribe children and those with roles in the remote health system, and to explore how growth monitoring is understood and whether it resonates locally. A further aim was to explore whether and how aspects of the remote health system feature in accounts given by these participants.
Methods
Study Setting
The study was conducted in the district of Mae Chaem, northern Thailand, in June 2014. Four villages were involved, of Karen and Lua ethnicity, located approximately 1 to 3 hours drive from the nearest town with a hospital and markets. The villages were chosen due to their planned involvement in a nutrition-sensitive agriculture program. They ranged in size from 50 to 120 households, and 3 had no electricity. The majority of villagers are subsistence farmers, growing enough food for themselves and their families, often supplemented with cash crops (mainly maize for animal feed). Some households also raise animals and tend small homestead gardens.
Participants
Study participants attended a 2-day workshop or completed an in-depth interview, as detailed in the next section. Two individuals contributed to both activities.
The workshop was for VHVs, with 5 men and 3 women, ranging in age from 24 to 38 years (see Table 1). All VHVs had at least 1 child of their own. The 2 who had a child aged 0 to 5 years also accepted the invitation to do an in-depth interview. Twenty other villagers with children aged 0 to 5 years completed in-depth interviews, the majority being women (see Table 2).
Characteristics of the Village Health Volunteers (VHVs).a
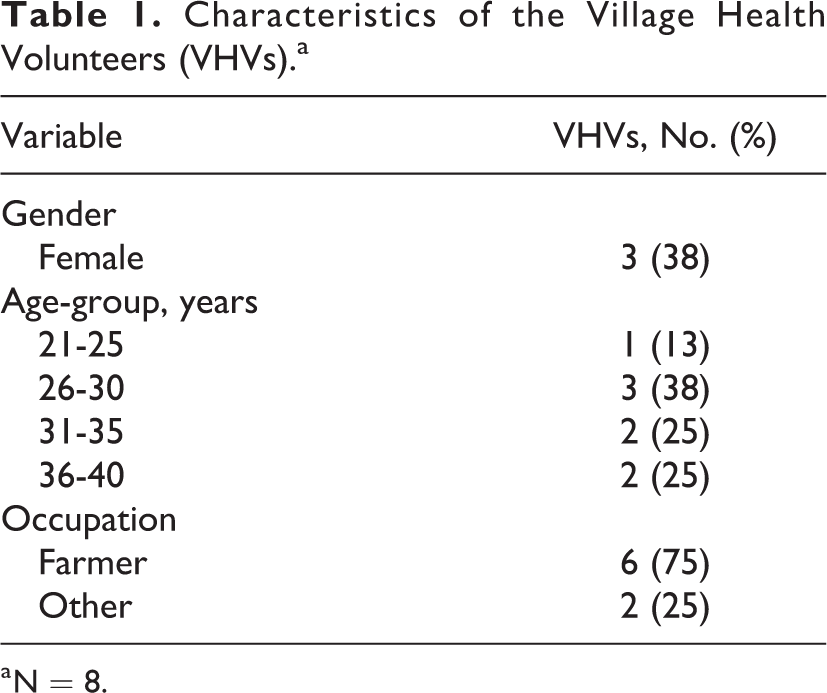
a N = 8.
Characteristics of the Villagers.a
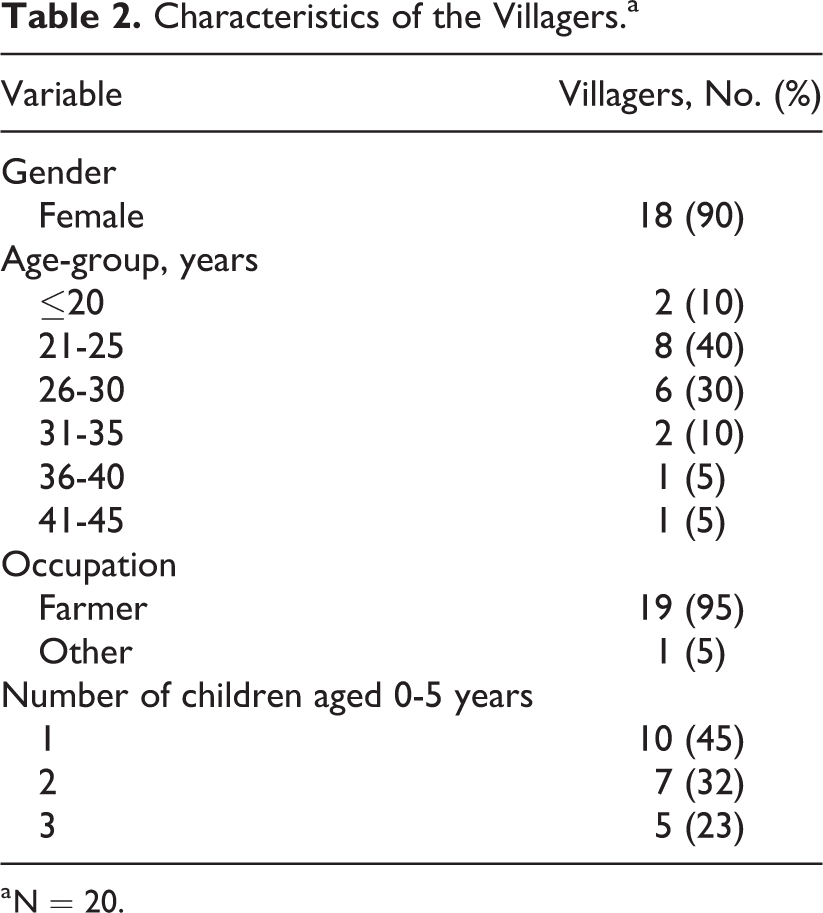
a N = 20.
In-depth interviews were also undertaken with 3 community and 3 subdistrict PHOs (3 males and 3 females, age range: 30 to 50 years) as well as 2 nurses (both female, aged 25 and 32 years). Community PHOs work in clinics or public health offices near the villages. They provide basic health services that may include immunization, provision of medications, birth control, deworming tablets, blood pressure checks, antenatal checks, and growth monitoring. Subdistrict PHOs usually have responsibility for several of these activities across a wider area.
Study Design
The first author was introduced to the participating health workers and villagers by colleagues who were already known to them. She visited the villages on 3 occasions before the study commenced to establish relationships and learn about village life, during which time she made field notes. The Thai coauthors were consulted over the course of the study so that the work was culturally sensitive.
The study involved conducting a 2-day workshop to collaboratively investigate infant and young child health. 14 The following topics were addressed: health of infants and young children, feeding practices for children younger than 5 years, nutrition recommendations, and how child nutrition could be promoted within the village.
The workshop was conducted in Thai by 4 experienced bilingual (Thai/English) facilitators. Two were researchers from Chiang Mai University who had previously undertaken research in the villages and were known by some of the participants. A further 2 were community outreach workers from Chiang Mai who had worked in other hill tribe villages but were not known to workshop participants. Semistructured guides were developed by the first author in partnership with the facilitators, drawing upon the extensive experience of those who did community outreach work in lieu of pilot testing for questions and concepts. Workshop sessions were audio-recorded and later concurrently transcribed and translated from Thai to English by the facilitators.
The VHVs were invited to the workshop by the subdistrict PHO by telephone, where possible 1 male and 1 female VHV from each of the 4 villages. The workshop proceeded as a series of discussions in response to open-ended questions, first in small groups (typically for 75 minutes) and then as a whole group (for around 60 minutes). Reflection on lived experiences was encouraged, allowing for different experiences to be shared.
In-depth interviews were subsequently conducted with villagers, VHVs, and other health workers, with these participants described in the previous section. Facilitation, preparation of semistructured guides, audio-recording, and translation occurred in a similar manner as for the workshop. The VHVs selected villagers for interview; a few villagers chose to have a family member or friend in attendance. In-depth interviews were usually 45 minutes long and, for villagers, continued until data saturation appeared to have been reached. Other health workers were approached through a subdistrict PHO and interviewers were confined to those available, so saturation was not necessarily reached.
All transcripts were reviewed by the first author in consultation with the facilitators to clarify meanings so that consistent terms were used in translation. The names of participants have been changed for privacy. In selecting quotes to present, care has been taken to ensure information is not identifying. All transcripts and analyses have been stored on password-protected computers and/or in secure, locked cabinets.
Data Analyses
A thematic analysis was conducted guided by a social constructionist epistemology. 15 While meaning is understood to be learnt and shared culturally, thereby shaping practices, there is scope for variation and multiple points of view within communities so that attention was paid to this. 16 Themes were coded and identified iteratively, initially focusing on notions of child health and whether size featured in these descriptions, then following strands representing alternative conceptions while attending to comments and silences around growth monitoring. Descriptions of roles of health workers were attended to within participant types and across accounts from all participants, as well as expectations of and encounters with health services. NVivo 10 software (QSR International Pty Ltd, Doncaster, Victoria, Australia) was used to code and organize data.
All data coding was undertaken by the first author. She mapped themes and their interrelations, with cross-checking and expansion by the second and last authors occurring through recurrent reading and discussion. The Thai authors commented on interpretation and implications throughout. Understanding of transcripts was supplemented by observations from the first author’s field notes, made throughout her time in the villages, and by communication with the World Agroforestry Centre team at Chiang Mai University that also works with the villagers.
Ethics
The study was granted ethics approval by University of Adelaide, Australia (HREC# H-2014-51) and The Research Institute of Health Science, Thailand (Study code 4/57). Participants were given verbal and written information about the study in Thai, including the first author being a student with relationships to Thai institutions and the University of Adelaide. Participation was voluntary, and written informed consent was sought from all the respondents.
Results
Perceptions of Child Health
Participants were asked “what is a healthy child?” referring to children younger than 5 years. Four main themes emerged in relation to this and what it required, as shown in Table 3.
Themes Around Child Health and Their Frequency Among VHVs and Other Villagers.a
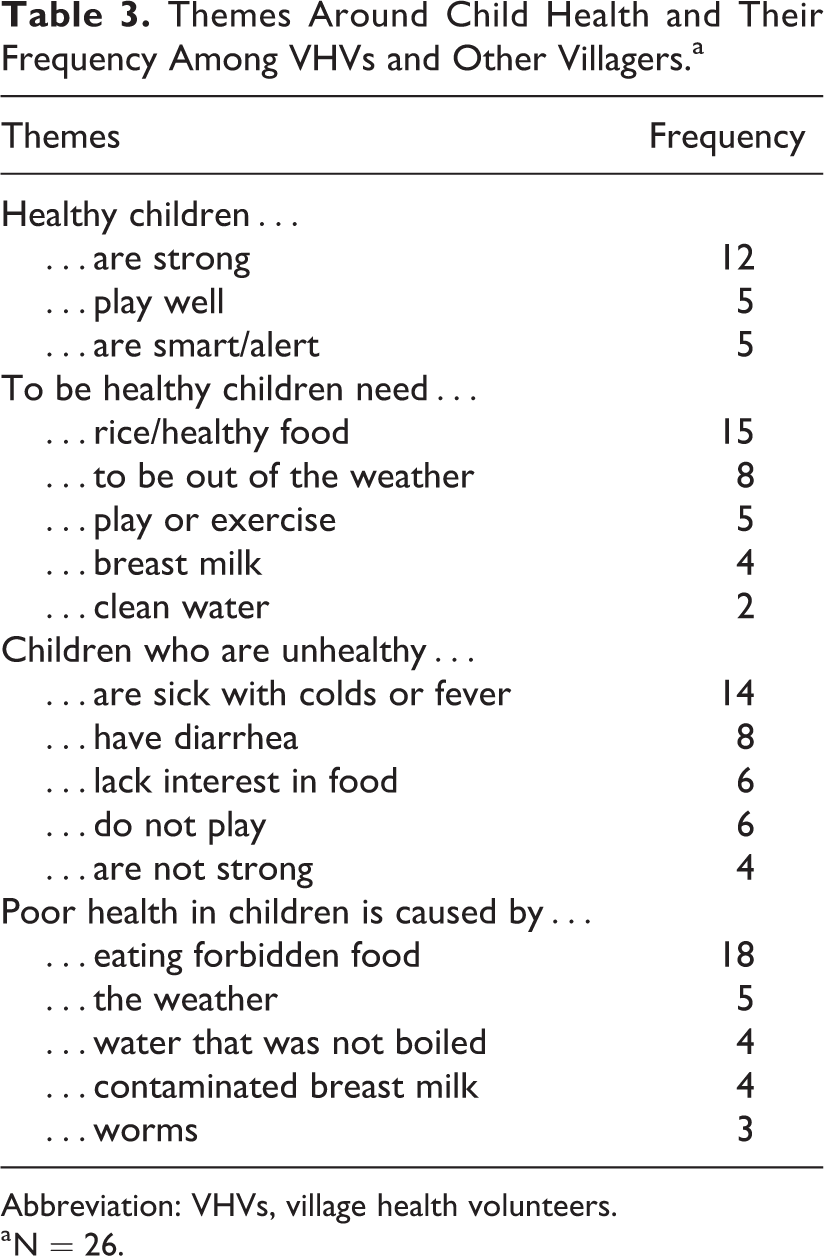
Abbreviation: VHVs, village health volunteers.
a N = 26.
If you want to know [if the child is healthy], mostly, the child will be wandering around and playing with friends in the village. From morning until evening, walking around. Not coming home. (Nut, father and VHV)
Some villagers spoke of health as the child having a completely healthy body without signs of sickness. The Thai term “somboon,” meaning healthy (or even plump) or perfect, was often used to describe complete health. Villagers frequently used the term “strong.” It is noteworthy that hill tribe children often have physically demanding duties, such as preparing animal feeds and feeding animals.When discussing what is important for healthy children, villagers said that warm clothes, play, or exercise was necessary. Breast milk was also seen as important, consistent with the findings from studies conducted throughout Thailand
3,17
: If they drink a lot of milk, the child will be completely healthy (somboon). (Ghai, mother) We need to stress feeding food, because if they eat healthy food, the children will be strong and their bodies will be fresh. (Aek, father and VHV) Now they [children] have the pre-school and they have a good basis…When opened the school had a centre and they had the practice of giving food for lunch and how to cook to make for a smart brain and it helps kids know about things, know about language, and come together in a group and come together as a society. (Noom, father and VHV) Warm water, when it’s hot, it will kill the germs…You can give cold water, but you must boil it first. That’s how it is. (Pong, father and VHV)
Signs of an unhealthy child were said to include lack of interest in food, low activity levels, crying without meaning, and symptoms such as a runny nose. For example: My daughter is 4 years old, when she gets sick, she likes to cry. If she’s well, she will wander around. If she’s sick she just cries. And her face is pale. Her whole body is pale. And she’s tired. (Kip, mother and VHV) Three times [diarrhea, including] after [the] baby’s hand hurt, when [she (the mother) arrived] back from work [and the breast] milk [was fed to the child] hot and [the] third [time when she (the mother) ate] sour food - mango and maryong [a local sour fruit], fermented and fresh, with chilli paste. (Luuk, mother) When she (the breastfeeding mother) goes to work and her breast milk is hot, then [if] the baby drinks they (the child) gets diarrhea…she [must] shower first and squeeze the hot milk out. (Luuk, mother)
The most common causes of diarrhea according to a recent review
22
are drinking contaminated water and inadequate sanitation and hygiene, which do not match the reasons given here. Villagers did not spontaneously mention water, but when prompted they indicated that they gave children boiled water. However, one PHO said: Some people [do] not boil [the water]. They put it [the water] in the tank then let residue drop to the bottom then drink it.
During the first author’s time in the villages, hand washing and water sanitation practices varied in their consistency. The cleanliness of living conditions varied. Penned or staked animals, including pigs and chickens, lived underneath stilted homes. Manure could be trodden on; however, shoes were always left outside the house. Refrigeration was not available for storage of food.
Village Children and Malnutrition
Children in the community were generally seen as healthy. Parents usually said their children were strong, played well, and had healthy bodies. No problem [with child health] as they [children] are strong and all…healthwise they are ok, they are strong. (Geb, mother)
If there were malnourished children, the villagers saw this as a result of a childhood abnormality. Mostly not have [unhealthy children]…most of them (children) are healthy, but some of them, just a few [are unhealthy] but mostly it [is because of] things that have happened from their childhood. It is like when they are young they are already disabled—they are very weak from a young age. (Song, mother) Like we’re working as village health volunteers, if we observe, we can’t really say that they have malnutrition. Actually when we weigh the children aged 0-5 years, if we compare with the pink booklet (growth chart), most of them are not way below the [normal growth] standard. There are none that are way below standard, because a few times that we weighed the children and compared to the pink booklet that belongs to the mothers, as far as we were concerned, not too many are malnourished. (Aek, father and VHV) Mountain kids (children from the village) compared with same aged kids in the town, the town kids are larger and taller. (Win, VHV) Sometimes we can observe the children, those who are tall are tall and those who are short are short. The strength of some of them is equal. Their balance (height to strength ratio) is not equal. (Noom, father and VHV) Is it possible that heredity is a part of the reason? Maybe the parents are short so the kids are also short. (Maew, mother and VHV) I mean the older one (sibling) is short because he takes care of the younger one. They love their younger sibling so they carry them. This also has a reason [for the elder child being short]. (Pong, father and VHV)
Remote Health System Roles and Growth Monitoring
The health system and growth monitoring were absent from almost all discussions with villagers about Infant and Young Child health. Thus, the accounts below are from PHOs and VHVs.
It is important to bear in mind that VHVs, like most villagers, contribute intensive labor to subsistence farming. Varying degrees of involvement with their role in the remote health system were spoken of by VHVs as well as different collections of duties. For example: Mainly it about vaccine and mosquitos [and] help with promote in each village about sending unwell people to hospital [as] not have anyone come take them [as] the road is difficult…we (VHVs) help each other. Work of VHV [occurs] when they (PHOs) order us. (Noom, father and VHV) No we don’t do growth monitoring. (Nan, father and VHV) VHV come measure weight uses scales…height and measure head circumference…every child when measure they bring the pink book…they look [if] follow the standard or not…Have a form that has name, weight then write down this…lots of forms, this form has name, weight, height head circumference send to PHO. VHV goes to see small child…visit after birth ask mother if scar [cesarean] ok and if child healthy (somboon)…need to get information about mother and child. Ask the mother if the child is healthy. Milk good? Mother good? Scar good?…Finished send to PHO like that. VHV help recommend [women and children] go to PHO. (Aek, father and VHV) Taught [women with breastfeeding pain how to manage it] but they like to eat medicine more…want medicine from here. (PHO3)
Growth monitoring of children aged 5 years and younger occurred when children visited the public health office due to immunization or illness and was also sporadically conducted within the villages by VHVs. There were a few instances of growth monitoring during the first author’s fieldwork, and what took place was quite varied and it was not always clear whose responsibility it was. It is the duty of another girl to collect all this information [weights and heights children and related nutrition status] and send it to the [provincial] PHO. (PHO 2) Even if we know who is lower [than healthy growth standards], there is not much we can do anyways. In the past I knew the kids. When I knew who had a problem I would give [formula] milk, but now [the formula milk] goes to the local council. (PHO 2)
Infant and Young Child Feeding (IYCF) Understanding and Counseling
Nutrition education and counseling was rarely mentioned by villagers and did not feature in VHVs’ descriptions of their roles. All PHOs reported providing simple nutrition advice for breastfeeding, such as recommending banana flower to increase breast milk. Beyond this, one PHO explained that there was nothing to be done, which may point to a lack of lactation management support for this PHO: Even if they come here [to the public health office with breastfeeding problems], there is nothing they [the PHO] can do, they can give suggestions, but usually they [the villager] will work it out in the village. (PHO 2) not go [to anyone for help] and finally it [breast milk] came out by itself. (Fan, mother)
There were no reports of villagers receiving significant advice on complementary feeding nor any of this being provided by VHVs or PHOs. One PHO indicated that it was “not very clear who will tell them” about complementary feeding (PHO 2), aligning with previous reports. 24
The nurses said that women should receive the Mother and Child Health Handbook at their first antenatal visit. The “pink book” includes information on the benefits of breastfeeding, proper attachment and positioning, how to express and store breast milk in a refrigerator (not available in most villages), and examples of complementary foods and portion sizes. Supporting pictures are also provided, but they rely on comprehending the Thai explanations that may prove difficult for many villagers. Thus, the predominant source of advice on IYCF was older women in the village, as we have described elsewhere. 10
The villagers’ contacts with the health system seem to be sporadic. There were numerous difficulties in accessing health services, including the demands of farming work, lack of transport, cost of transport, poor or unpassable roads, and limited ability to speak Thai. One PHO provided an example of a pregnant woman visiting the public health office for an antenatal checkup: …Problem that they (pregnant women) face is that the far away homes…the roads are so bad so a lot of the women they come 1 or 2 times but once getting bigger they are afraid to come [to the public health office]. Some places they have to walk or on the motorbike and very bumpy ride so they feel rather than come for a check-up for health, it is safer to stay at home…especially in the rainy season…the roads are not possible to go. (PHO 1) Even my own child the doctor said that [feed EBF 6 months] and I did not listen. When I was a kid at birth they (my parents) would give rice. Then the doctor said for 3 months [give EBF and no rice] and we just followed the doctor as we might as well follow what the doctor says. But now…the doctor said 6 months and we did not listen. If the doctor is going to tell us 6 months we are not going to do it as it is so different from what we are used to doing…3 months is an acceptable difference, but 6 months is too much…If they (PHO) tell us the good things we will listen to them and those things not good we will not listen. (Sarn, father)
Discussion
In the villages, child health is generally perceived as related to the strength of the child, absence of overt illness, and independent play, thus functional capacity. Self-reliance in children is valued in other indigenous communities, including Australian Aborigines 25 and farmers/herders in the highlands of Peru. 26 Ethnotheories explain this in terms of the need for children to learn both independence and interdependence in contexts requiring constant cooperation and labor for survival. 27 -29 The villagers rarely referred to the height of the child and thus did not follow the Western medical model in which heights and weights are key indicators of the health of children. Growth monitoring does not appear to have a clear role in helping villagers to recognize malnutrition. Instead, villagers generally thought there was no problem with being short. This has been reported in other poor rural communities; for example, in Guatemala, caregivers did not recognize that their children are malnourished because it is “normal to have short children” 30,31 ; similarly, in rural Kenya, low weight is considered normal. 32
There were few differences between the perspectives of villagers who had roles as VHVs and others, perhaps not surprising, given the small amount of training VHVs receive and the remoteness of the location. The VHVs seemed to have greater awareness of Thai government (and WHO) nutrition recommendations and related concepts, although that did not mean they adopted these practices, with local knowledge continuing to be prioritized. 10
Growth monitoring has long been endorsed and promoted by WHO. 33 It has important functions beyond providing measurements. Ideally, these include counseling and education, regular contact with the health system, community mobilization, and targeted supplementary feeding. For example, the Tamil Nadu Integrated Nutrition Program in India has generated benefits partly through bringing community together each month on the special community weighing days. 34 At a population level, growth monitoring can be used to identify areas where malnutrition requires concerted efforts 24 and to assess whether interventions are working. 35
Counseling is key to the success of growth monitoring programs. A systematic review found insufficient evidence for direct benefits of making measurements—the greatest benefits flowed from the “opportunity to discuss any queries about childcare”. 36 A more recent review demonstrated that growth monitoring was not efficacious in “large-scale programs with weak nutrition counseling”. 35 In Brazil, a review of research on growth monitoring was undertaken recently 37 to understand how “the everyday reality of public health services” meant that difficulties were encountered, even though growth monitoring was classified as a feasible health technology. A range of impediments were reported, from lack of equipment and appropriate space to the precarious and improvisational structure of the health services in some locations. Many specific problems highlighted the need for growth monitoring to be part of a comprehensive program in which continued education and support was provided to the health workers who were responsible, and continuous care was available where children with suboptimal growth were identified.
In the hill tribes, the VHVs and PHOs appear to have variable knowledge about the growth monitoring process and its wider purposes; many appeared to see it mainly as a bureaucratic activity. Neither PHOs nor VHVs see IYCF counseling as a noteworthy part of their role. This is arguably a consequence of lack of appreciation of the purpose and local benefits of growth monitoring, reflecting problems upstream in the health system, as will be discussed in the next section. The persistence of IYCF issues is thus not surprising nor is the villagers’ reliance on traditional knowledge and advice.
The Remote Health System: Considerations From “Bottom-Up” and “Top-Down”
The international model of the VHV (also known as community health worker) emerged in the 1970s in response to a shortage in the health workforce and a need to reach dispersed and poor populations in developing countries. This arrangement promoted a self-help approach, aligning with a “bottom-up” primary health-care ethos, supposedly at a low cost. 38 The VHV role was introduced in Thailand in the 1980s, 5 with selected community members given sufficient training to enable them to provide basic health care and health promotion, including growth monitoring which was a concerted focus. 38 Severely malnourished children received special attention, including free complementary food, 5,38 and parents were counseled. 13 However, it is not clear whether this ever occurred in the hill tribes. 24
The effectiveness of the VHV model is dependent on a chain of support, supervision, and resources, as VHVs turn to their PHOs who, in turn, are reliant on the next level up. Perry et al 39 discuss serious problems within this chain that became evident in large-scale programs in a number of countries in the 1980s. At that time, global political and economic forces undermined the commitment of some governments, as well as their ability to finance the VHV model, which was not as low cost as anticipated.
These intersecting problems arguably foreshadow some of the experiences in Thailand. With the East Asian Financial crisis of 1997, the Thai baht fell in value 40 and the Thai government had to review expenditure, cutting the public health budget by 15%. 41 Although public health programs continued, there were indications of reduced impact, as low birthweight in newborns increased, as did underweight in schoolchildren and outbreaks of diseases that were the subject of immunization efforts (eg, diphtheria and pertussis). 41 A review of health indicators from the 1960s through to 2010 suggests that the retrograde trends were transient, but there has been little further improvement. 42
In 2002, Thailand introduced universal health-care coverage that meant all Thai citizens had no out-of-pocket expenses for primary core health requirements. 43 This important innovation represented a change in health priorities. 42 In addition, globalization is reported to be affecting the ancient subsistence economies of Asia. The poor have become poorer and have to labor for longer, disproportionately affecting the lives of women. 44,45 Thus, both internal and external circumstances have meant that the context in which the Thai VHV program was first implemented has changed.
The volunteer model has been found to work well in some places at some times 39 but arguably needs to be reviewed periodically, especially when other major changes occur. 46,47 The VHVs remain a valuable connection between the health system and the community, with the potential to have greater influence than outsiders on what occurs in their own village, particularly in isolated communities such as the hill tribes. However, VHVs need to be well supervised and supported and their livelihoods considered in order to see benefits at the community level.
Some limitations of this study should be acknowledged. The need for language translation and possible confusion generated by that has been mentioned. The number of health officers in the study was small, and data saturation was not necessarily reached, but the views presented resonate with the extensive experience of the third author. Due to time and resource constraints, a single person coded all data; it would have been preferable for a subset of interviews and themes to have been coded by others and cross-checked. We did not have the resources to formally evaluate growth monitoring practices and procedures.
Conclusion
High levels of malnutrition in young children in the hill tribes of northern Thailand have persisted over several decades. While growth monitoring and accompanying activities have greatly improved child nutrition in much of Thailand, this model has not been as successful in these remote and poor villages for a range of contextual factors, from the local to the global.
To be effective, counseling must be integral to a growth monitoring program, with VHVs well trained, supported, and supervised—and remunerated for their time. This model is not as inexpensive as it was thought to be 40 years ago, and the lives of subsistence farmers have become harder. However, engaging with communities and building trust through respectful dialogue, opportunities that the model could provide, remain essential to changing practices.
The PHOs who oversee VHVs also need appropriate skills and ongoing support. However, investment in the workforce at the periphery has been difficult in Thailand in the face of competing health system priorities and impacts of globalization and international financial crises. Consideration needs to be given to preventing the poor from getting poorer and to the livelihoods of the poor who service their communities.
Footnotes
Authors’ Note
A.R., V.M., L.S., P.W.i., P.W.a. designed the research. A.R. collected the data. Data were analyzed by A.R., V.M., and L.S. A.R., V.M., and L.S. drafted the article. All authors critically revised the article and read and approved the final manuscript.
Acknowledgments
The authors thank all participants including the villagers, village health volunteers, public health officers, and nursing staff at Mae Chaem hospital. The authors also thank the workshop facilitators for their input and advice: Posri Leelaprat, Dr Sakda Pruenglampoo, and Somluck Nimsakul from Research Institute for Health Sciences and Pailin Limwattanachai. Thanks also goes to Golbang Jafari for organizing and facilitating workshops as well as translating recordings from Thai to English. Thanks to the KSC-GMS/ ICRAF team including Surachet Jinakeaw, Palika Champrasert, Anantika Ratnamhin, Natjan Chairat, and Tanawit Wongsur and to Dr Peter Berti (HealthBridge, Canada). The authors are grateful to Dr Chawapornpan Chanprasit for advice during planning and to Dr Ari Patcharaporn.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A.R. was supported by a scholarship from the Faculty of Health and Medical Sciences, University of Adelaide, and a Prime Minister's Australia-Asia Scholarship.