
Abstract
Background:
This article synthesizes the results of 3 cluster randomized controlled trials of dairy-containing ready-to-use supplementary foods (RUSFs) to address malnutrition in primary schools, preschools and villages in Guinea-Bissau, one of the world’s poorest countries. Together, these studies document widespread malnutrition across infants, young children, adolescents, and pregnant and lactating women and point to intervention options that were not previously presented.
Objective:
To combine the evidence from the United States Department of Agriculture–funded pilot studies in Guinea-Bissau on the effects of dairy protein supplementation to gain a broader perspective on the role of dairy containing RUSFs in various age-groups, the importance of the mother–child dyad and family food dynamics for infant and child growth. Translate the results into action and the next generation of effective products.
Methods:
A comparative analysis of data and synthesis of evidence from 3 published studies and ongoing research conducted by our team in Guinea-Bissau.
Results and Conclusions:
Higher dairy supplements have the potential to achieve broad benefits for malnutrition, especially in mothers and early childhood (first 1000 days and 36-59 months). Higher levels of dairy protein also can prevent moderate acute malnutrition in children younger than 2 years, independent of the family food dynamic. Community-level nutrition behavior change education should target older children and adolescents at the community level and through the preschool/school platform.
Keywords
Introduction
This article is based on a presentation given at the 2017 Dairy for Global Nutrition Conference: Dairy Nutrition, An Engine for Economic Growth. It presents a synthesis of results from 3 cluster randomized controlled trials (RCTs) conducted in Guinea-Bissau with a focus on the role of dairy protein in supplementary foods and program implications based on the combined evidence. Together, these studies 1 -3 document widespread malnutrition across infants, young children, adolescents, and pregnant and lactating women in Guinea-Bissau, and point to intervention options that were not previously presented or published.
This body of work helped build in-country capacity for conducting high-quality research protocols and strengthened the very limited nutrition evidence base in Guinea-Bissau, the 11th poorest country in the world. 4 Its population of approximately 1.85 million residents rely mainly on small-scale farming and fishing. Food grown for family consumption consists of millet, groundnuts, sweet potatoes, and mangoes. Families typically combine subsistence farming with harvesting cashews, which are sold for basic supplies, including rice and grains. Consumption of animal source protein is limited. 5
Research in low-income nations continues to be hampered by lack of ability to conduct sophisticated studies. Our research team was able to locally build capacity and conduct RCTs in Guinea-Bissau through a special program, the Micronutrient Fortified Food Aid Pilot Project (MFFAPP) funded by the United States Department of Agriculture (USDA). The MFFAPP was designed to develop and pilot test new micronutrient-rich food products for the McGovern-Dole International Food for Education and Child Nutrition (MGD) program. Before this public–private partnership, the country had little research capacity and even less information on the nutrition status of populations beyond the age of 59 months and reproductive-age women. 6,7
This body of research has generated nutrition data on over 7000 residents (infants, children, adolescent males and females, and mothers) and provides a unique understanding of the role of nutrition and family food dynamics in the communities of Guinea-Bissau. 1 -3 These studies shed light on the micronutrient status (Vitamin A and Iron), levels of malnutrition, growth (anthropometric measures), cognitive status, primary and preschool attendance, and reported illness. This is the first large-scale research program in the country. Our team has continued research on nutrition in Guinea-Bissau through other funding and now has baseline nutritional data on over 8000 people from infancy to adulthood.
Our team established unique partnerships between villages and our well-trained local research staff; we had strong support from the Government of Guinea-Bissau’s Ministries of Health and Education and excellent participation from village elders, community health workers, school principals, teachers, parents, and parent-teacher association members. Global Food & Nutrition Inc and Tufts University executed the study design, research, analysis, training, capacity building, and quality assurance. Challenge Dairy Products, Inc produced and supplied the dairy-based supplements pilot-tested in these studies. International Partnership for Human Development (IPHD) provided logistics and the platforms for the pilot projects.
Methods
The 3 intent-to-treat RCT protocols, methods, and results have been described in full in 3 published articles; the reader is referred there for details. 1 -3 The RCTs assessed the effectiveness of dairy ingredients (whey and nonfat dry milk) and micronutrients in ready-to-use supplementary foods (RUSFs) to address malnutrition in pilot projects in schools, preschools, and village health centers in 2 food-insecure regions of Guinea-Bissau. The 3 studies were the first of their kind to program RUSFs containing different levels of dairy-source protein (whey and/or nonfat dry milk) using the school platform for children, adolescent boys and girls, and village health centers for infants, children, mothers, and pregnant women.
The studies collected the same outcome indicators at baseline and end line using the same methods. We obtained approvals from Guinea-Bissau Institutional Review Board, and the following measurements were permitted: anthropometric assessment (weight, length, or height as appropriate depending on age, and mid-upper arm circumference for children [MUAC]) and finger-stick blood samples. Outcome measures were Z-scores for height for age (HAZ), body mass index for age (BAZ), and weight for age (WAZ) as well as blood levels of hemoglobin (Hb) measured with HemoCue (Angelholm, Sweden) and Vitamin A measured as retinol-binding protein (RBP) from dried blood spots.
There were no prior studies on nutrition status, iron or vitamin A, so we could not complete appropriate power calculations. The intervention studies therefore are pilots and may have limited power to observe significant differences among all primary outcomes. However, baseline data gathered from the pilots are valuable nationally and can be used to effectively power studies in the future.
Study 1: Baseline Nutrition Status of Primary School Children Enrolled in RCT
Programmed in 32 primary schools in Oio and Cacheu, in 2011/2012, the first study was a cluster-randomized trial of an RUSF provided as a snack at the beginning of class. 1 At school, students also received one meal per day over 75 days and a micronutrient supplement weekly. The intervention included 1 RUSF provided in 2 sizes on 2 schedules (30 g or 50 g, 3 or 5 days a week) to deliver different levels of macro- and micronutrients, randomized to the 4 treatment groups. There also was 1 control group that did not get the supplement but received the meal and micronutrient supplement. This pilot study was not powered to detect statistically significant changes in anthropometric or biochemical measures.
The pilot did produce valuable nutrition baseline information for the country from 4784 school children aged 5 to 19 years old (older than expected), which we present in Table 1 and Figures 1 and 2 from Saltzman and Schlossman 1 to inform the results from study 2 (preschools) and study 3 (village children and mothers). Table 1 summarizes nutritional status indicators by gender, age-group, and region. In total, 61% of all primary school students had one or more indicators of moderate to severe malnutrition at baseline. Anthropometric assessment determined that widespread malnutrition in children older than 5 years of age occurs despite receiving 1 school meal per day. Moderate/severe anemia and vitamin A deficiency were most prevalent in children 5 to 9 years old, making up 30% of children in this age-group on average. Stunting and low body mass index (BMI) were most prevalent in teenage boys. Approximately 20% of this age-group had Z-scores <−2 for HAZ and BAZ.
Summary of Demographic and Anthropometric Data From Study 1. From Saltzman and Schlossman.a
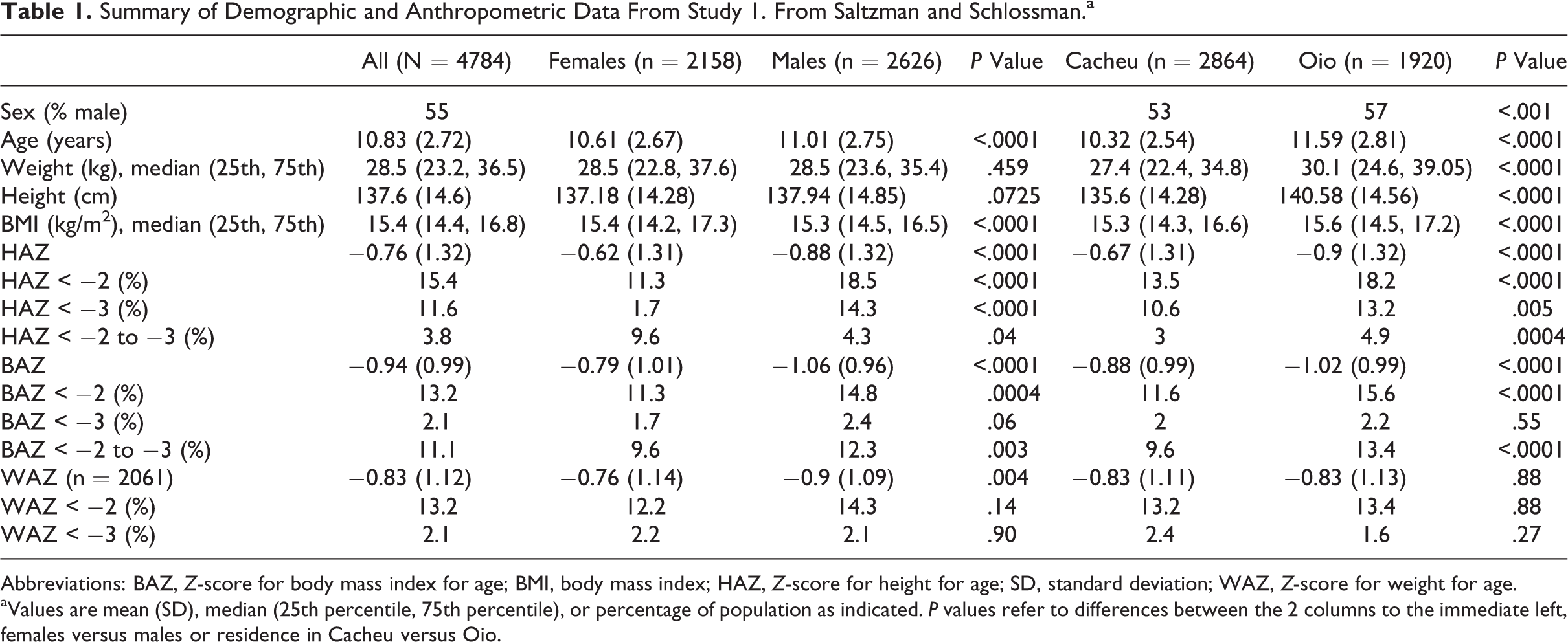
Abbreviations: BAZ, Z-score for body mass index for age; BMI, body mass index; HAZ, Z-score for height for age; SD, standard deviation; WAZ, Z-score for weight for age.
aValues are mean (SD), median (25th percentile, 75th percentile), or percentage of population as indicated. P values refer to differences between the 2 columns to the immediate left, females versus males or residence in Cacheu versus Oio.
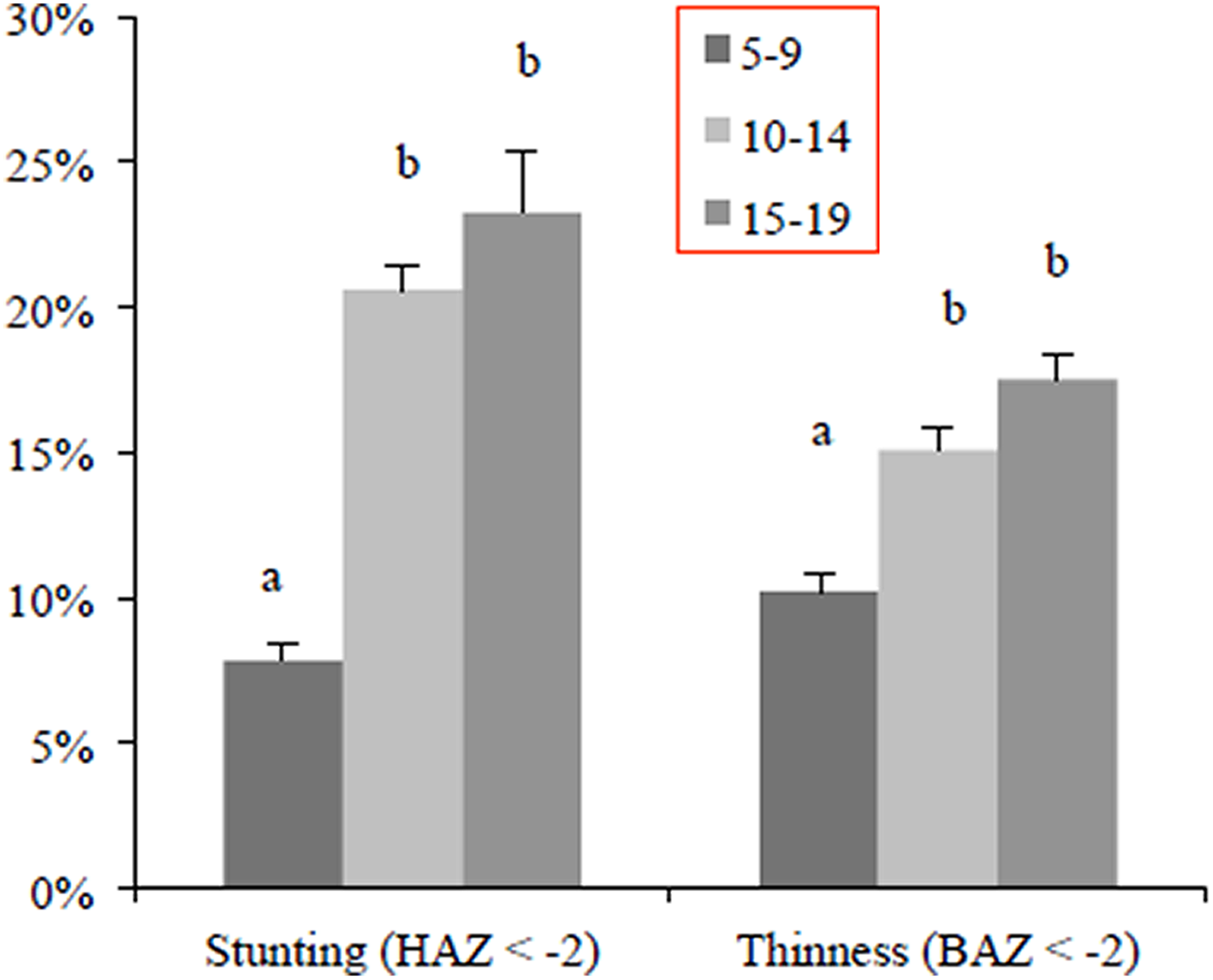
Stunting and thinness by age of children and adolescents in study 1. Adapted from Saltzman and Schlossman. 1
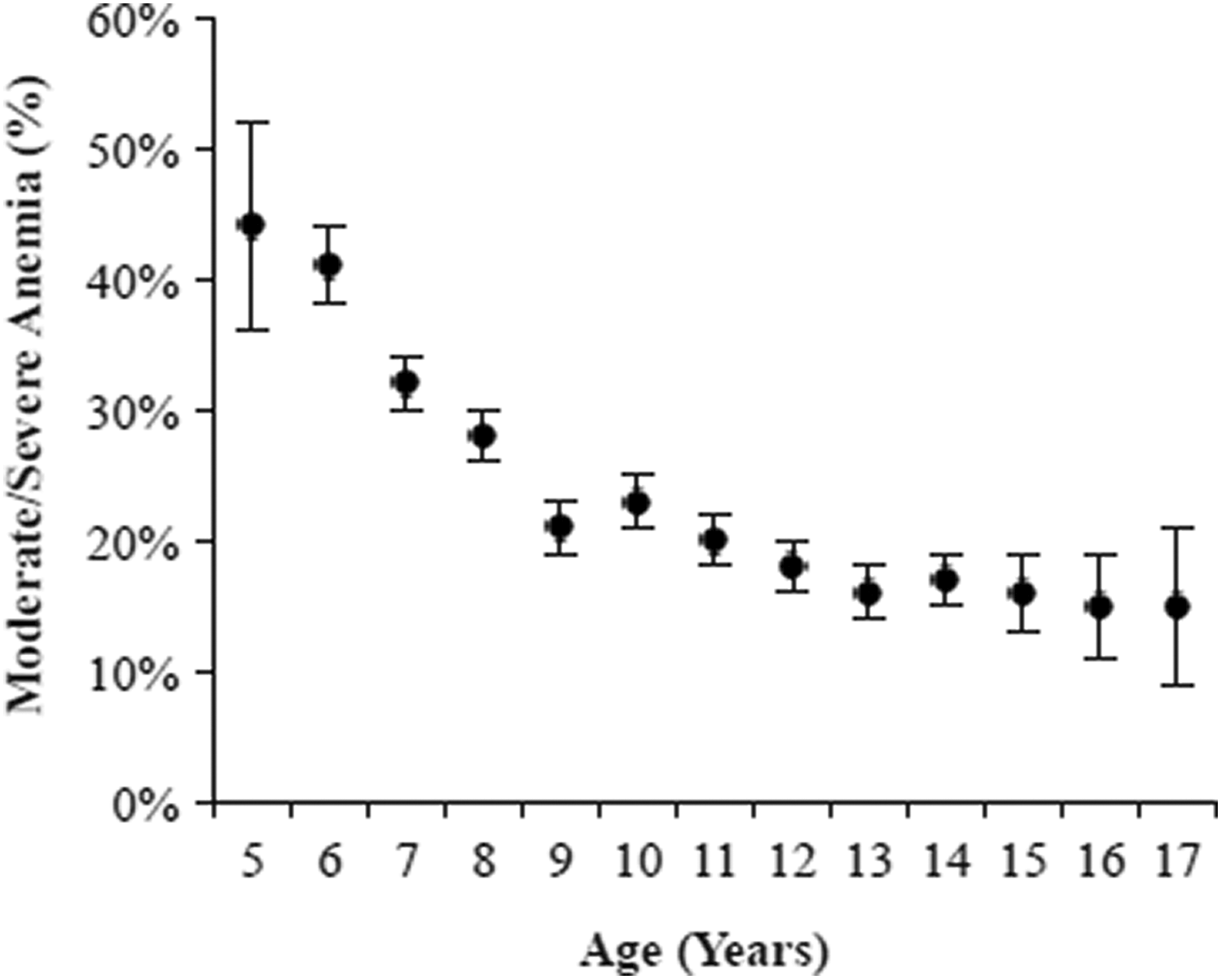
Anemia severity by age of children and adolescents in study 1. Adapted from Saltzman and Schlossman. 1
Vitamin A deficiency (RBP < 0.7) was detected in 21.5% of primary school students, with no significant differences by region or gender, as shown in Figure 1. Prevalence of anemia is high, especially early in life. Anemia ranged from 42% among the 5 year olds leveling off at about 20% among teenagers (Figure 2).
Study 2: Comparison of High- and Low-Dairy RUSFs in Preschools
Based on the high levels of malnutrition detected among children in Oio and Cacheu primary schools, a second pilot study was conducted in 2013 among preschools to see whether supplementation at an earlier age would be more beneficial, in order to determine the best point of intervention. 2 The 3-month (12-week) cluster RCT in preschools compared children randomly assigned to 2 identical RUSFs differing only in the amount of dairy protein (as whey or whey and nonfat dry milk) and a wait-listed control that did not receive RUSFs during the study but received the RUSFs after completion. The 2 RUSFs were identical in composition (total energy, energy density [5.2 kcal/g], calories, micronutrients, etc) except for the protein content. They were provided in 92 g sachets (478 Kcals/92 g sachet) for the preschoolers. The RUSFs were made to deliver the same nutritional profile (but not the same ingredients) as the RUSFs used by the World Food Program at the time. They contained either 15% of protein from dairy (whey) or 33% of protein from dairy (50% whey and 50% nonfat dry milk), with the balance of the protein from soy isolate. The supplements were the state-of-the-art to treat/prevent moderate acute malnutrition (MAM) at the time the study was conducted and were within the guidelines of the 2012 World Health Organization Technical Note for composition of supplementary foods to prevent MAM. 8 The supplements were highly palatable, and the flavor and texture profiles were very well accepted. The Consolidated Standards of Reporting Trials (CONSORT) diagram for the study, from Batra et al 2 is provided in Figure 3.
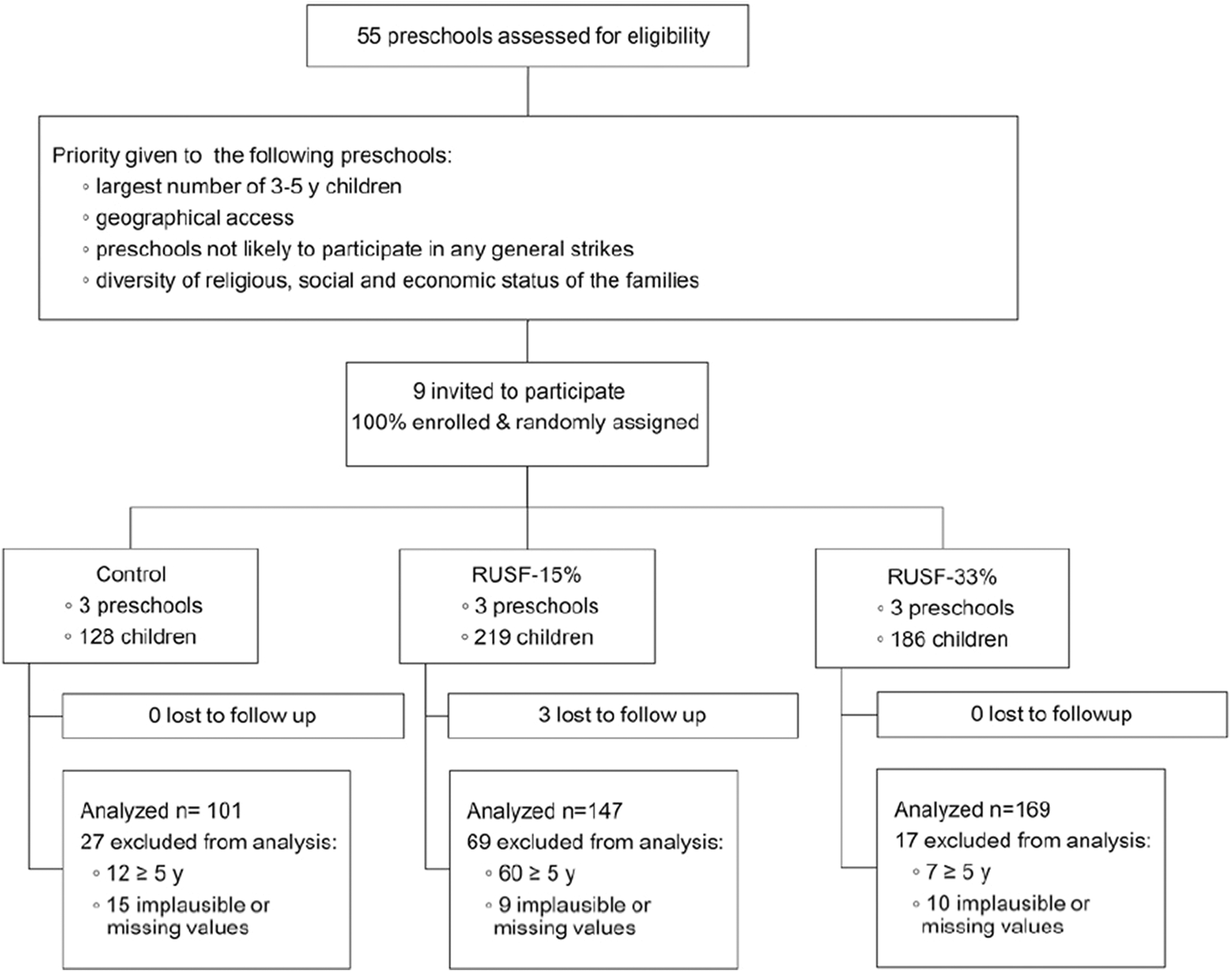
CONSORT diagram for study 2: a cluster-randomized controlled trial (RCT) of 2 ready-to-use supplementary foods (RUSFs) provided as a second daily meal in preschool children in Guinea-Bissau. Ready-to-use supplementary food-15%, ready-to-use supplementary food with 15% of protein from dairy sources; RUSF-33%, ready-to-use supplementary food with 33% of protein from dairy sources. Adapted from Batra et al. 2
Using the same indicators and methods as in the primary school study, baseline nutritional data (anthropometry, finger-stick blood for Hb and RBP/Vitamin A) were collected from 2018 children aged 3 to 5 years old in 9 preschools in the Oio and Cacheu regions. Preschool children randomized to the treatment groups were given either RUSF-15% or RUSF-33% dairy supplements on days they attended preschool and compared to the control group. All the children received daily meals at preschool through the IPHD MGD program.
Weight for age and HAZ Z-scores improved from baseline in all students due to the provided daily preschool meal. Children in the control group, however, did not improve in body mass; they gained weight, but their body composition did not improve. In the RUSF-33% group, however, children added 1 unit of weight gain as per the MUAC, indicating better body composition. The MUAC measurement is a proxy for lean body mass and muscle mass. Children who received RUSF-33% also gained WAZ.
Both the RUSF-15% and RUSF-33% supplements had a significant effect on increasing weight in preschool children who were not the most malnourished, indicating an opportunity to prevent malnourishment. Decreases in weight for height Z score (WHZ) and MUAC in controls signify worsening nutritional status, not seen in supplemented children. The MUAC decrease in control versus RUSF-33% is significant. The mean HAZ and WAZ were negative, but less negative than among the older children measured in the primary school study. The MUAC and Hb measurements indicate that meals with 33% compared with 15% of protein from dairy may help prevent wasting and anemia.
Study 3: Comparison of High- and Low-Dairy RUSFs in Village Children and Mothers
In 2013/2014, the final MFFAPP study was conducted across 13 villages that included infants 6 to 23 months of age, children 24 to 59 months old, and mothers. The first of its kind to compare 2 levels of dairy protein in otherwise identical RUSFs, this was a cluster-randomized supplementation of infants and children with MAM and mothers in villages. The CONSORT Diagram in Figure 4 is from the study by Schlossman et al 3 and shows the study design. Measurements were taken on 1080 mothers, children, and infants: WAZ, HAZ/length-for-age Z-score (depending on age of child), and weight for height Z score (WHZ)/weight for length Z score (WLZ) and MUAC.
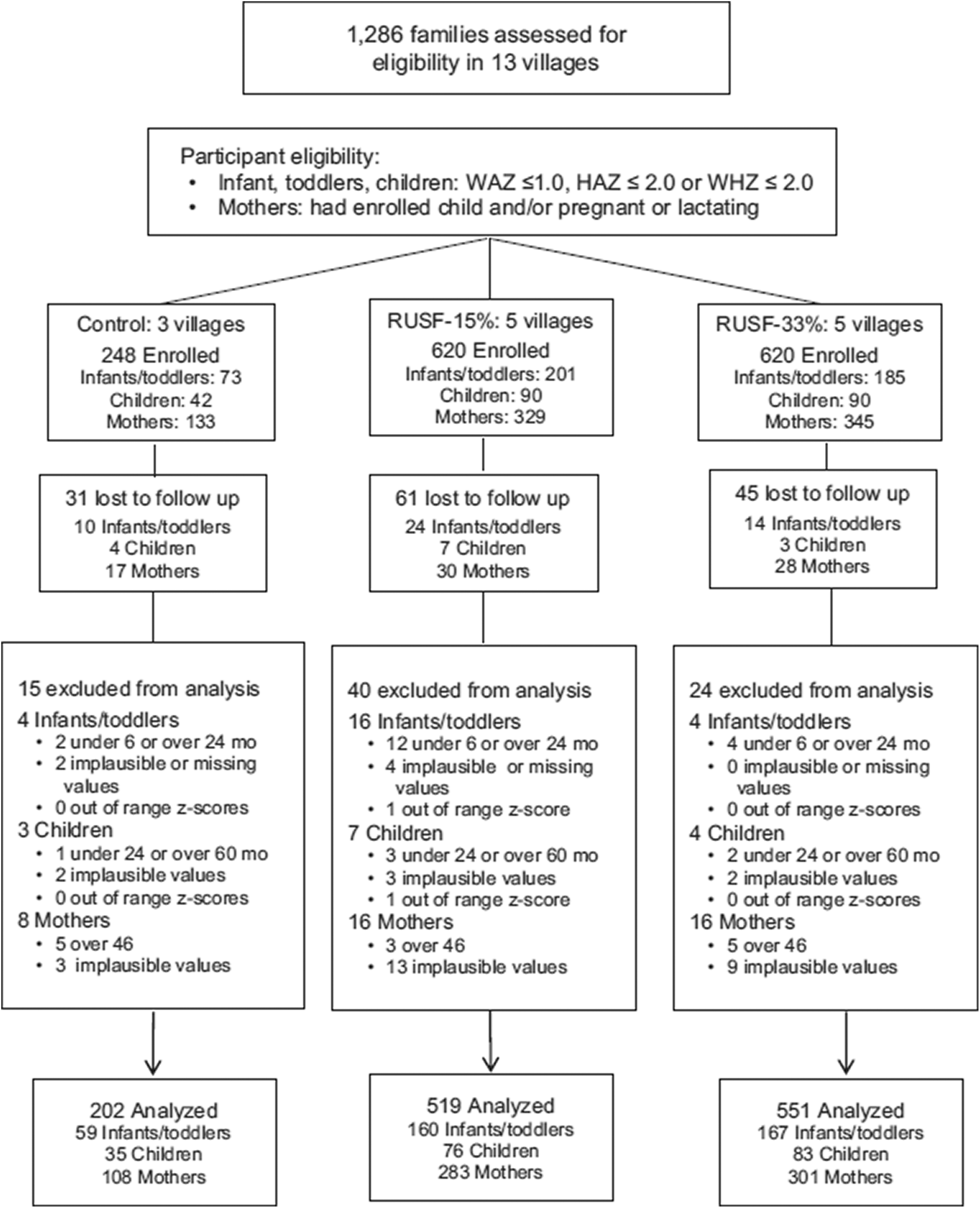
CONSORT diagram for study 3: a randomized controlled trial (RCT) of 2 ready-to-use supplementary foods (RUSFs) and control groups in Guinea-Bissau villages. Adapted from Schlossman et al. 3
Following 12 weeks of treatment, the women in the villages randomized to receive the RUSF-33% had an increase in MUAC compared to women in the RUSF-15% group and those in the control group. Both treatment groups showed significant increases in MUAC, but there was a more protective effect detected in the RUSF-33% group. Infant WAZ scores compared to baseline improved the most among those who had the lowest scores at baseline. This effect was observed in children as well, although it was more pronounced among infants 6 to 23 months old than among children 24 to 59 months old.
Mother and child MUACs were correlated in the RUSF-33% group, indicating that the supplements with the higher dairy content improved the mother’s nutritional status and beneficially contributed to the child’s nutritional status as well. In the 6- to 23-month age-group, supplementation resulted in improved growth, but this was uncorrelated with mother’s nutritional status.
The mothers responded better to treatment than did the infants and children. Mothers’ nutritional status after 12 weeks of supplementation improved more with the RUSF-33% than with the RUSF-15%, demonstrating that the higher dairy amount was crucial to success. Those on the higher dairy supplement had increased maternal weight, height, BMI, and MUAC. The intervention was also correlated with reduction in illness (diarrhea, malaria, colds). Higher iron is essential for women of reproductive age, and both RUSFs had a protective effect on the mother’s iron status compared to the controls, in whom Hb decreased considerably.
Discussion
In study 2, the preschool study, all the children also received meals from the USDA MGD Program. Weight for age and HAZ improved from baseline in all preschoolers, which may be expected given the additional school feeding. The control students gained weight, but based on MUAC, their body composition did not improve. In the RUSF-33% group, by contrast, preschoolers added 1 full unit of weight gain as per the MUAC, indicating improved body composition. The supplements were effectively distributed by teachers and popular with children, and they had significant effect on increasing weight in preschool children who were not the most malnourished, demonstrating a feasible intervention point.
In study 3, the village study, the positive effect observed in infants independent of mother’s intake may indicate that the families prioritized preventing malnutrition during the first 1000 days. In older children, food sharing may reduce the impact of the supplementation. Success of treatment among children 24 to 59 months of age may depend more on the adequacy of food supply in the household and may be a potential point of behavior change/communication intervention targeted at older children and family food dynamics.
School children in Guinea-Bissau cannot achieve their potential without greater intensity of food assistance, especially in Oio, where study 1 (primary schools) data were consistently worse than those in Cacheu. Widespread malnutrition, anemia, and wasting were documented in primary schools, which reinforces the need for early intervention. Regional differences were observed depending on context and food supply. Even children (preschool and primary) receiving a school lunch were seen to have widespread malnutrition including anemia, making it harder to learn. There is a continued need for research to ensure effectiveness of supplements/fortification and to provide improved meals for preschoolers and school children. It is not unusual for youths to stay in school for a longer period compared to the United States, simply because they are provided a school meal.
In summary, higher dairy protein supplements have potential to achieve broad benefits in treatment and prevention of MAM, especially if the treatment is in early childhood. Higher levels of dairy protein also can successfully prevent MAM in children younger than 2 years of age, independent of the family dynamic. Further, the supplements were associated with decreased reported illness in children. While it is important to ensure that children develop physically, it is imperative that they develop cognitively as well. Ongoing studies continue to take place in Guinea-Bissau to measure cognition in infants and children with a specially designed, next generation supplement. 9
Recommendations for Translating Research Results into Action
To translate these results from the field, the next generation of nutritional products should focus on protein quality and nutrients known to support cognition, as the current generation of nutrition support products do not. More research is needed to confirm optimal protein content, but according to the studies summarized here, 15% protein from dairy is not enough, and 33% may not be enough either. In school-aged children, focusing on the family feeding environment is crucial to success, as the family food basket is often heavy with starchy foods; improving school meals to include dairy or equivalent animal or marine protein will also be important, as this meal is often the only one the child receives. For older youth, a specialized RUSF, whether it is a paste, a bar or a biscuit, especially if made locally, should include iron (with antihelminthic medicine if parasites are prevalent), as appropriate to the local context (ie, may be different in areas with a high prevalence of malaria and/or helminths). The school platform is currently underutilized for nutrition interventions and teaching opportunities about food, intrafamily food dynamics, and food systems. It is the one place girls can be reached systematically before pregnancy to improve prematernal nutrition and health status.
In terms of programs and people, both the farm and the pharmacy are needed. Locally based food solutions with consumer-based approaches to behavior change will be needed to achieve successful results. Consumer-based approaches that tap into local production, even as the products incorporate imported micronutrients and dairy ingredients, can stimulate the local economy and food processing industry. Gaining local interest can lead to public–private partnerships that will benefit producers and consumers alike.
The next generation of nutrient-rich supplementary food products will need to integrate with local food systems to target mothers and infants, with special attention to cognition early in life and iron status among adolescent girls. Dairy is critical, particularly in the first 1000 days—for mothers and babies—and optimal components in the right amounts need to be determined in order to achieve and sustain optimal health and well-being of populations over the long term.
Footnotes
Acknowledgments
The author (principal investigator) would like to thank our research team without whom this body of work would not be possible: Susan B. Roberts (co-principal investigator), Edward Saltzman, Payal Batra, Molly Schleicher, Mary Kayla Shea, Madeleine Gamache, Carrie Brown, and Paul Fuss of the Friedman School of Nutrition Science and Policy, USDA Human Nutrition Research Center, Tufts University, Boston, MA; William Pruzensky, Adrian Balan, Ionela Balan, Carlito Bale, and Augusto Braima de Sa of International Partnership for Human Development, Leesburg, VA, and Bissau, Guinea-Bissau; and Lauren Wood and Mandy Bridges of Global Food & Nutrition Inc, Washington DC, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded entirely by the US Department of Agriculture as part of a pilot project to improve nutrition under the McGovern-Dole International Food for Education and Child Nutrition Program (agreements no FFE-657-2011/035-00 and FFE-657-2012/043-00) and conducted with local implementation by International Partnership for Human Development.