
Abstract
Background:
Studies on the association between a priori dietary patterns and serum highly sensitive C-reactive protein (hs-CRP) have led to inconsistent results, and we are not aware of any study on interleukin 17A (IL-17A) as an inflammatory marker associated with autoimmune diseases.
Objective:
The present study aimed to investigate the association between Dietary Approaches to Stop Hypertension (DASH) and the Mediterranean dietary patterns with circulating hs-CRP and IL-17A levels.
Methods:
In this cross-sectional study, female teachers (aged 20-50 years) who lived in Yazd, Iran, were randomly selected from elementary, guidance, and high schools from September 2015 to February 2016. Anthropometric data, as well as general information and dietary food intakes, were gathered, and each participant gave 1 blood sample. Participants were categorized into tertiles based on the DASH and the Mediterranean diet calculated scores. The associations between the dietary patterns and serum hs-CRP and IL-17A levels were assessed in the crude and multivariable models. In total, 320 female teachers aged 40.38 (8.08) years were included.
Results:
The DASH diet was associated with lower serum hs-CRP levels in the crude (P = .05) and the fully adjusted models (P = .02), while it was not significantly associated with IL-17A levels. The participants with the highest adherence to the Mediterranean diet had significantly lower circulating IL-17A levels (P = .04) even controlling for all confounders (P = .02); however, there was not a significant relationship between this diet and hs-CRP levels.
Conclusions:
The DASH and the Mediterranean dietary patterns might be differently associated with inflammatory markers. Further prospective studies are recommended to confirm our results.
Introduction
Systemic inflammation has been implicated in the etiology of a wide range of chronic diseases including type-2 diabetes mellitus (DM), atherosclerosis, 1,2 cardiovascular diseases, bone diseases, muscular dystrophy, osteoporosis, neurological disorders such as Alzheimer disease and multiple sclerosis, Parkinson, chronic renal failure, and different types of malignancies such as colon, pancreatic, and lung cancers. 3 -7 Systemic inflammation can be measured by the use of different markers, such as interleukins (ILs), tumor necrosis factor-α (TNF-α), and highly sensitive C-reactive protein (CRP). 8 -10 Elevated hs-CRP, a widely used marker for individuals’ systemic inflammatory status, has been associated with increased risk of type 2 diabetes 11 ; furthermore, it is considered to be an independent predictor of cardiovascular diseases. 12 -14 An IL-17 is also a small family of proinflammatory cytokines, and the IL-17A is a well-known and characterized member. 15,16 Notably, IL-17A levels have been positively correlated with a variety of human chronic diseases with an autoimmune background, including psoriasis, 17 rheumatic diseases, 18,19 multiple sclerosis, 20,21 and Crohn disease. 22 -24
A number of studies have tried to examine the association between patterns of dietary intake and inflammatory markers. For instance, in a cross-sectional study, it was revealed that a healthy dietary pattern (high in fruits, vegetables, tomato, poultry, legumes, tea, fruit juices, and whole grain) is inversely related to inflammation. In contrast, they found that the Western dietary pattern score is positively related to inflammatory markers. 25 The inverse relationship between healthy dietary patterns and hs-CRP concentration was also confirmed by a number of investigations. 26 -29
The Dietary Approaches to Stop Hypertension (DASH) diet is a diet rich in fruits, vegetables, low-fat dairy products; dietary fiber, potassium, calcium, and magnesium; moderately high in protein; and low in saturated fat, cholesterol, and total fat. 30 Although the DASH diet was originally developed to prevent or treat hypertension, 31 it is understood that it might also favorably affect weight, 32 lipid profile, 33 markers of blood glucose control, 34 -37 and risk of cardiovascular diseases. 38 The Mediterranean diet is also a healthy diet, which emphasizes high intake of fruits, vegetables, cereals, olive and its products, potatoes, beans, nuts, fish, and seeds. 39 It includes olive oil as a major fat source, and dairy products, meat, and poultry are consumed in low to moderate amounts. 40 It has been found that there is an inverse association between Mediterranean diet and overall morbidity and mortality from cardiovascular diseases and cancer. 41 A limited number of observational investigations have tried to assess the relationship between imitating these 2 dietary patterns and inflammatory markers. For instance, Fung et al found that an alternative Mediterranean diet index is associated with significantly lower concentrations of inflammatory markers including CRP. 28 Byung-Joon Ko also performed a cross-sectional study and showed an inverse relation between a DASH-style diet and circulating hs-CRP levels. 71 We are not aware of any observational study examining the association between dietary patterns and IL-17A.
Data are limited regarding the association between a priori dietary patterns and inflammation. As the DASH and the Mediterranean dietary patterns are regarded as healthy dietary patterns, we hypothesized that they both might be inversely associated with serum inflammatory markers; however, as they are different in their recommended food groups, they might be different in their association with different inflammatory markers. Therefore, the present study targeted to investigate these dietary patterns in association with serum hs-CRP as a general marker of systemic inflammation and IL-17A as a novel marker of autoimmune diseases in a sample of female teachers living in Yazd, Central Iran.
Methods and Materials
The present study was conducted in the context of a parent cross-sectional study among a sample of 450 Yazdi female teachers aged 25 to 50 years who were selected by cluster random sampling method from elementary, guidance, and high schools. The recruitment of the participants was done from September 2015 to February 2016. The aim of the parent study was to assess the prevalence of metabolic syndrome among female teachers. The methodology of the parent study is extensively described elsewhere. 42 In brief, anthropometric measures, blood pressure, physical activity, and biochemical markers were assessed in all cases. The information required for the other variables, such as age, smoking status, marital status, menopause, medical history, medication, and supplement use, were also collected using a self-reported questionnaire. The dietary intakes were also assessed using a self-administered semiquantitative food frequency questionnaire (FFQ). Participants were invited to give 5 mL of blood sample in a laboratory for the assessment of their serum lipid profile (for the parent study) in maximum 2 days after filling the questionnaires. If the extracted serum samples were more than the amount needed for the parent study, the additional samples were collected and kept at −70°C for the present investigation (additional samples were available for 350 participants).
Eligibility Criteria
Participants with available serum samples for the laboratory assessment were included in the current study (n = 350). Those who left more than 70 items of the FFQ blank and participants whose daily energy intake was out of 800 to 4500 kcal (under- and overreporters) were excluded from the current analysis (n = 30). Therefore, data from 320 participants were available for the final analysis. The flow diagram of the participants’ selection for the current study is described in Figure 1.
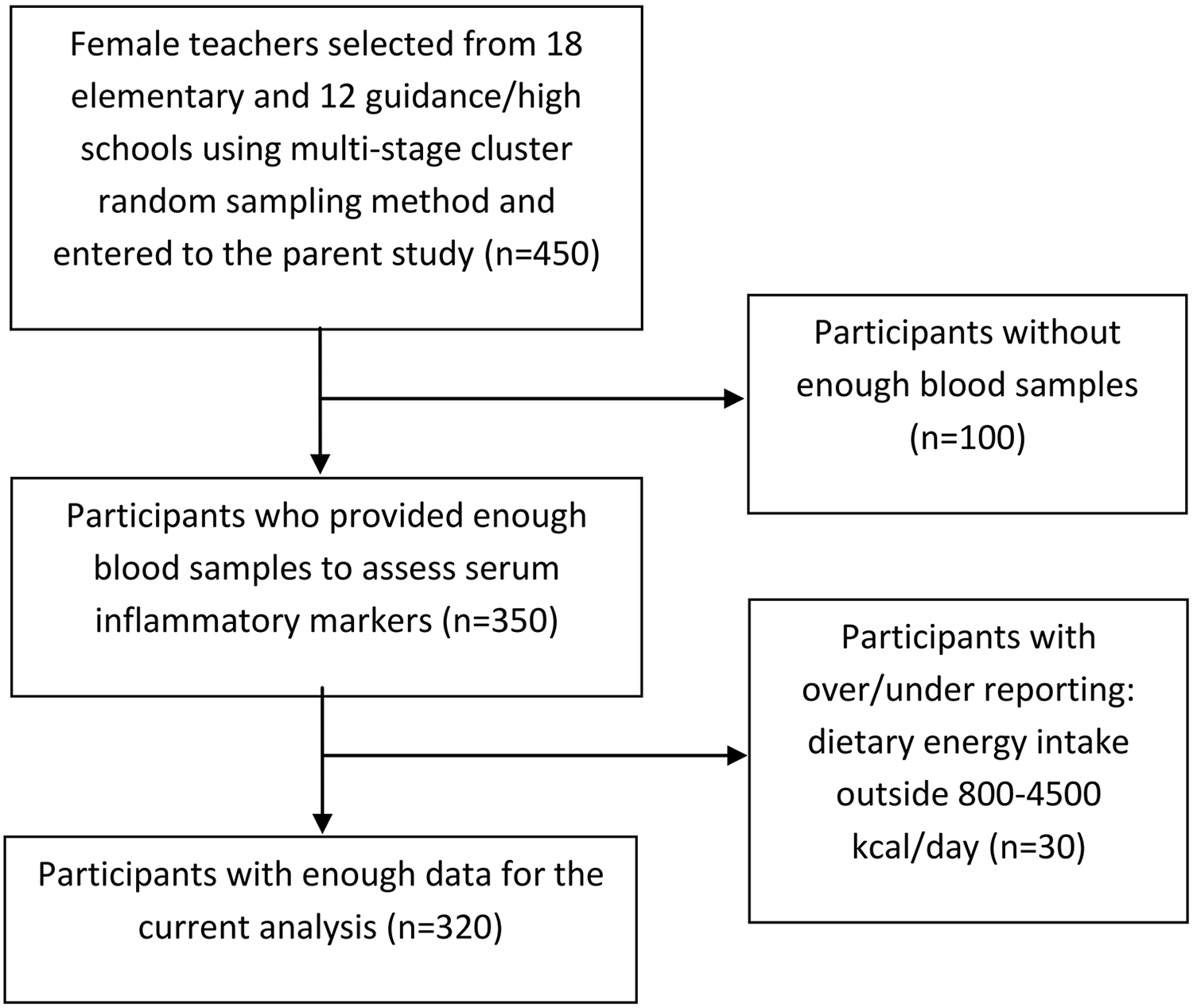
Flow diagram for selection of study participants.
Ethical Considerations
The present study was conducted according to the Declaration of Helsinki, and written informed consents were obtained from all participants. The study protocol was approved by the Research Council of the Nutrition and Food Security Research Center of Shahid Sadoughi University of Medical Sciences and the ethics committee of Shahid Sadoughi University of Medical Sciences (record number: IR.SSU.SPH.REC.1395.155).
Anthropometric Measurements
Weight was measured using a digital scale (SECA, model: 813) and recorded to the nearest 100 g while the participants were minimally clothed. Height was measured in a standing position, without shoes, using a tape measure while the shoulder was in a normal position and the head was fixed in the horizontal plane. Waist circumference was also measured using a tape measure, which was not stretchable at the level of the umbilicus with the accuracy of 0.5 cm. 43 All anthropometric measurements were done by a trained nutritionist. To calculate the body mass index (BMI), weight (kg) was divided by the square of height (m). 44
Biochemical Evaluation
Participants were referred to a laboratory for collecting the blood samples. Five milliliter samples of venous blood were taken after 10 to 12 hours of fasting. Serum samples were separated and kept at −70°C for further analyses. The circulating hs-CRP and IL-17A levels were measured using enzyme-linked immunosorbent assay (ELISA) kits (Zellbio, Germany for hs-CRP [ZB-1805-H9648] with intraassay coefficient of variation [CV] <9.9% and interassay CV <12% and human IL-17A ELISA development kit [horseradish peroxidase], MABTEC, Sweden [3520-1H-6] with intraassay CV <5%).
Dietary Assessment
Dietary food intake during the last year was assessed using a self-administered Willett format semiquantitative FFQ. The questionnaire was a modified version of a 168-item questionnaire used for the Tehran Lipid and Glucose Study (TLGS), which was validated for adults living in Tehran, Iran. 45 We added 10 native food items (confections) that were specific to Yazd and were frequently consumed in the region, because this might help researchers to accurately calculate the dietary refined grain and sugar intakes. Therefore, we had 178 food items in this questionnaire. The 168-item FFQ used in TLGS was designed to be open ended in its original form; for the current study, the questionnaire was modified to a multiple-choice questionnaire. Participants answered 2 questions about each food item: (1) the frequency of food consumption (number of times per month, week, or day the food was eaten) in the past year and (2) the usual portion size consumed for that food item. To increase precision and accuracy of the estimates, we attempted to give the portion size of foods as a unit with the same perception for all people. Participants were asked to report their frequency of food intake based on 10 multiple-choice frequency responses varying from “never or less than once a month” to “10 or more times per day.” The portion size for each item was asked using questions with 5 predefined choices. The choices were different according to each food item. A separate multiple-choice questionnaire was also provided to ask about the participants’ supplement use. Daily intake of all food items was converted to grams per day using household measures. 46 For the population-specific food items, we calculated their ingredients based on their standard cooking method for a common portion size. Then we calculated the daily intakes of their ingredients that were used to calculate the final nutrient intakes. Daily nutrient intakes for each participant were calculated using the Nutritionist IV (version 3.5.2, Axxya Systems, Redmond, Washington) software modified for Iranian foods.
Calculating Mediterranean Diet Score
Conformity to the Mediterranean diet was calculated for each participant using a modified version of the method proposed by Trichopoulou et al. 47 The scoring was based on median values of vegetables, legumes, fruits and nuts, fish and seafood, cereals, dairy products, poultry, meat, ratio of monounsaturated and saturated fats, and ethanol consumption. For the present study, we assigned a value of 1 to people whose consumption was below the median values for meat and meat products, poultry, and dairy products, and those with consumption equal to or above the median values received 0. In contrast, we assigned a value of 0 to people whose consumption was below the median values for food groups, such as vegetables, legumes, fruits and nuts, fish and seafood, cereals, and ratio of monounsaturated and saturated fats, and a value of 1 to people with consumption equal to or above the median for these food groups. Thus, the total Mediterranean diet score would be from 0 (minimal conformity to Mediterranean diet) to 9 (maximal adherence to Mediterranean diet).
Calculating DASH Diet Score
Conformity to the DASH diet was calculated using the proposed method by Fung et al. 48 This method of scoring was based on 8 food groups/nutrients, including fruits, vegetables, nuts and legumes, low-fat dairy products, whole grains, sodium, sweetened beverages, and red and processed meats. Participants were classified into quintiles according to their intake ranking. One point was assigned to quintile 1 and 5 points to the highest quintile. Higher scores were allocated to the higher consumption of fruits, vegetables, nuts and legumes, low-fat dairy products, and whole grains. For sodium, red and processed meats, and sweetened beverages, low intake was desired; therefore, the reverse method for scoring was applied. In this method, the score might range from 8 to 40.
Covariates
Self-reported data on usual physical activity were obtained using the International Physical Activity Questionnaire (short format). The data were converted to metabolic equivalent hours per week (MET-h/wk), 49 and participants were categorized to sedentary and active based on the median of the MET-h/wk levels.
Economic status was also assessed using a 9-item self-administered questionnaire. In the questionnaire, we asked about family size, husband’s occupation, person who is responsible for the family bills (husband/herself/other family members), house ownership (owner/tenant), house type (apartment/house), number of bedrooms in the house, car ownership (yes/no), number of cars owned by the family, and family income per month. We assigned 1 score to each item’s level, and participants were categorized into low, middle, and high economic status based on tertiles of the overall summed score. Some other variables were also collected by administration of a self-reported questionnaire. The questionnaire included the following variables: age, marital status (single/married), participants’ education level (college/bachelor degree/master degree or higher), number of deliveries (none/one/2/3 or more), menstruation status (pre/postmenopausal), oral contraceptives use (yes/no), history of chronic diseases including cardiovascular diseases, type 2 diabetes or metabolic syndrome (yes/no), family history of diabetes (yes/no), and lifestyle change in recent year (yes/no). We also asked about the smoking status of the participants, and none of them reported to be a current or ex-smoker. Therefore, we did not consider this variable in our statistical analyses.
Statistical Analyses
Each participant received a score for the Mediterranean and the DASH dietary pattern, separately. Participants were categorized based on tertiles of the 2 dietary patterns’ scores. The minimum sample size was calculated to be 75 participants in each tertile, considering 0.9 mg/L difference in hs-CRP levels between participants with highest and lowest adherence to the dietary patterns 45 with the power of 80% and an α level of 5%. 50 Comparison of continuous and categorical variables across tertiles of the dietary patterns scores was done by the use of analysis of variance and χ2 test, respectively. Quantitative data are represented as means (standard deviations) or means ± standard errors.
The correlation between hs-CRP and IL-17A was assessed using Spearman correlation test. Analysis of covariance (ANCOVA) with Bonferroni correction was used in crude and several multivariable models to compare the log-normalized serum hs-CRP and IL-17A levels across tertiles of the dietary patterns. Age and energy intake (kcal/d) were adjusted in the first model. In the second model, marriage status (married/single), physical activity (sedentary/high), education level (college/bachelor degree/master degree or higher), lifestyle change in recent year (yes/no), current oral contraceptive use (yes/no), menstruation status (pre/postmenopausal), economic status (low/middle/high), and disease history (yes/no) were additionally adjusted. In the third model, we controlled dietary-related variables, including omega 3 (yes/no), calcium (yes/no), vitamin D (yes/no), and multivitamin–mineral (yes/no) supplement use plus variables included in the second model. In the fourth model, we adjusted all variables included in the previous models plus BMI (kg/m2) and waist circumference (cm).
We also conducted linear regression analysis, including log-normalized serum inflammatory markers as the dependent variable and the dietary patterns’ scores as the independent variable in crude and multivariable-adjusted models to check if a linear association exists between adherence to dietary patterns and circulating levels of inflammatory markers. The variables adjusted in the models were the same as variables controlled in the ANCOVA. All statistical analyses were done using the Statistical Package for Social Sciences (version 15.0 for Windows, 2006; SPSS, Inc, Chicago, Illinois). P < .05 was considered as statistically significant.
Results
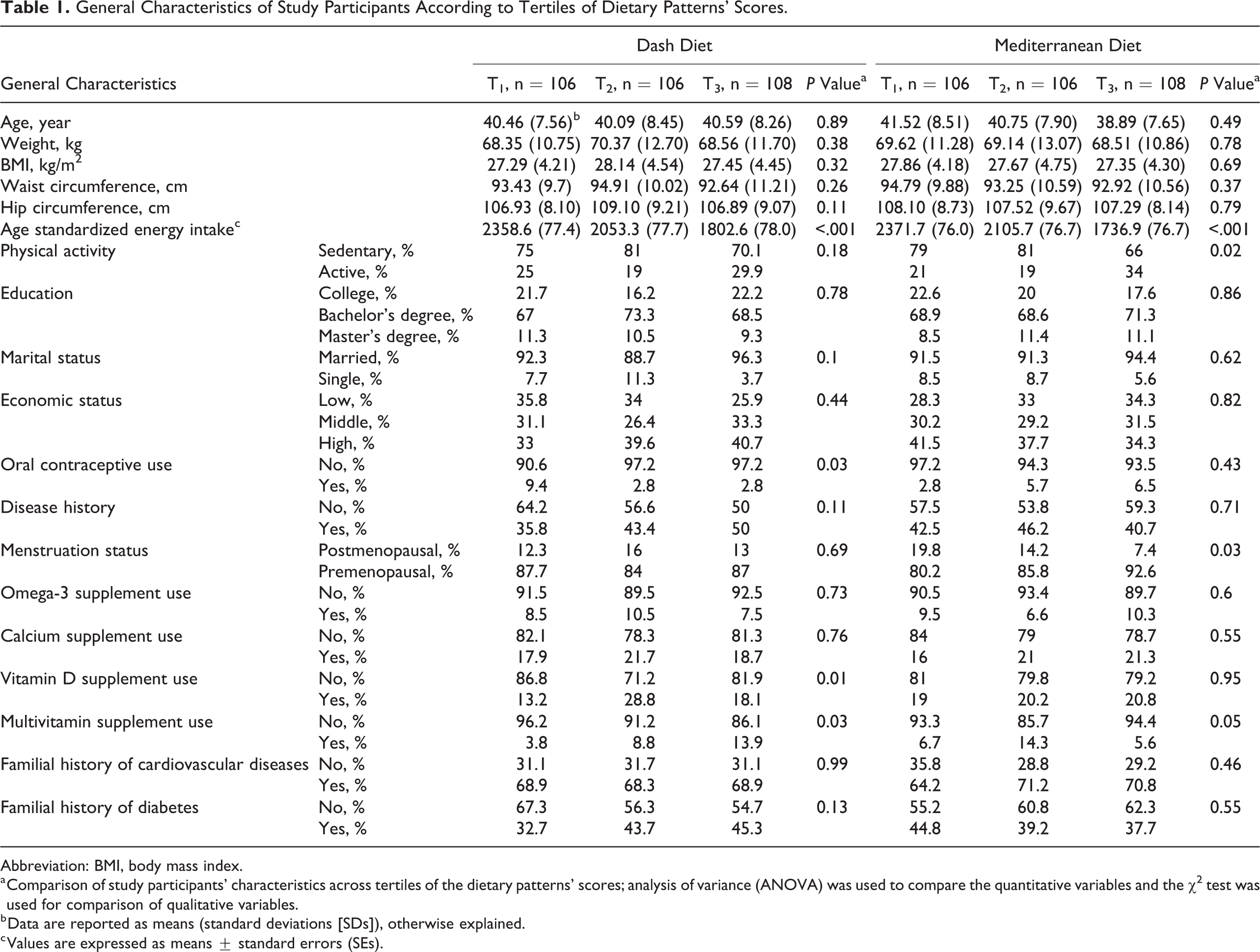
In total, 320 female teachers aged 40.38 (±8.08) years were included in this study. The general characteristics of the study participants based on the tertile categories of the DASH and the Mediterranean dietary pattern score are represented in Table 1. Participants with higher conformity to DASH diet had higher intake of multivitamin and vitamin D supplements, while they had less oral contraceptive use (P < .05). Furthermore, the Mediterranean diet was inversely associated with sedentary physical activity, and higher rates of individuals with higher concordance with this diet were in the premenopausal age (P < .05). Both dietary pattern scores were positively associated with age-standardized energy intake (P < .05). Other characteristics of participants were not significantly different across tertile categories of the 2 dietary patterns (Table 1).
General Characteristics of Study Participants According to Tertiles of Dietary Patterns’ Scores.
Abbreviation: BMI, body mass index.
a Comparison of study participants’ characteristics across tertiles of the dietary patterns’ scores; analysis of variance (ANOVA) was used to compare the quantitative variables and the χ2 test was used for comparison of qualitative variables.
b Data are reported as means (standard deviations [SDs]), otherwise explained.
c Values are expressed as means ± standard errors (SEs).
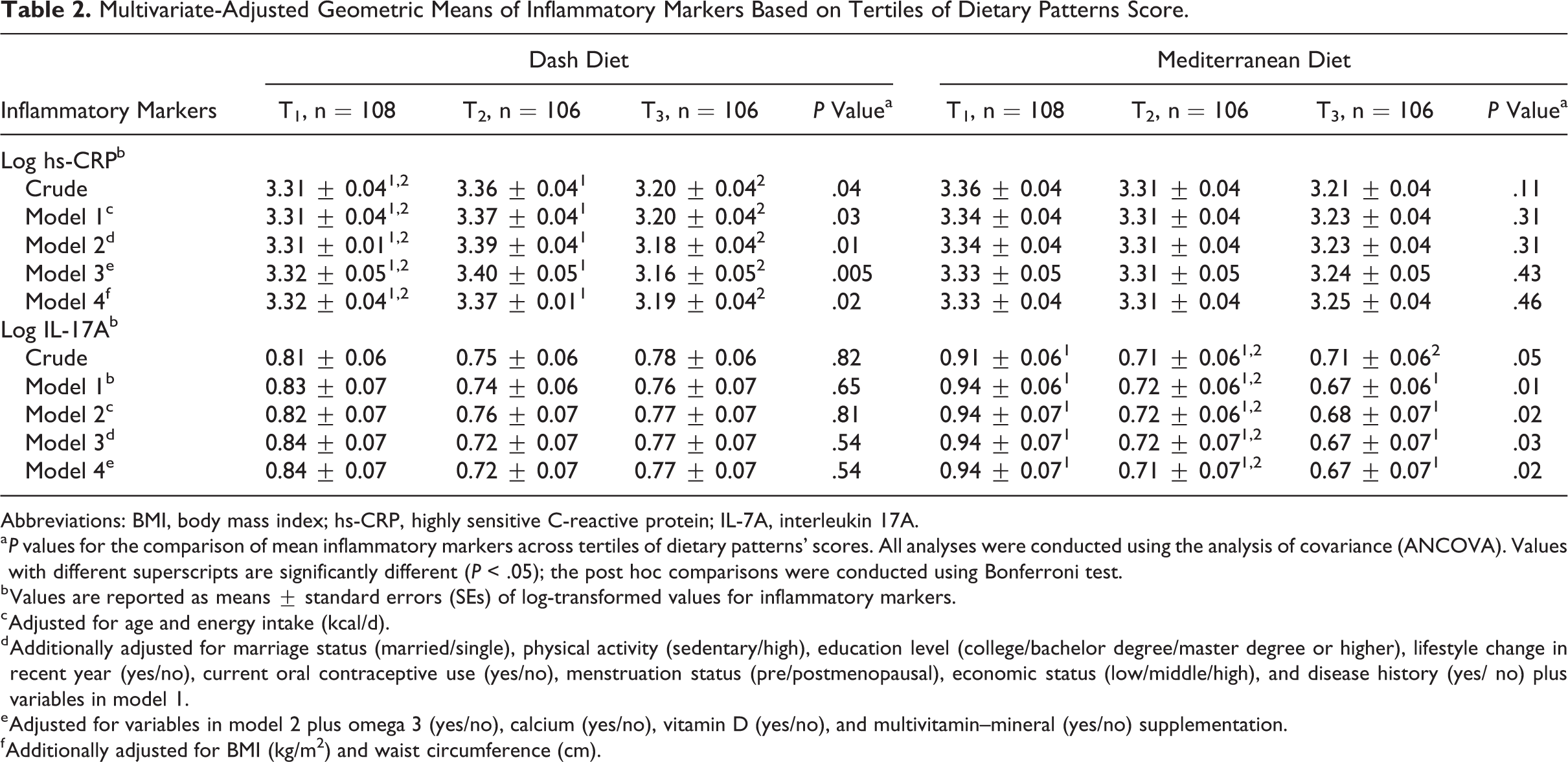
There was no association between serum hs-CRP and IL-17A concentration using Spearman correlation test (r = −0.045, P = .425). The comparison of log-normalized serum inflammatory markers across tertiles of the dietary patterns’ score in crude and multivariable-adjusted models is represented in Table 2. The analysis revealed that the DASH-like diet is associated with lower serum levels of hs-CRP levels in the crude analysis (P = .04). The association remained significant after adjustment for age (year) and energy intake (kcal) in the first model (P = .03) as well as further adjustment for marriage status (married/single), physical activity (sedentary/high), education level (college/bachelor degree/master degree or higher), lifestyle change in recent year (yes/no), current oral contraceptive use (yes/no), menstrual status (pre- or postmenopausal), economic status (low/middle/high), and disease history (yes/no) in the second model (P = .01). After controlling the dietary-related variables including omega 3 (yes/ no), calcium (yes/no), vitamin D (yes/no), and multivitamin–mineral (yes/ no) supplementation plus variables included in the second model, the association was also significant (P = .005). Additional adjustment for BMI (kg/m2) and waist circumference (cm) did not change the inverse association found between DASH diet and serum hs-CRP levels (P = .02). DASH-like diet was associated with serum IL-17A levels neither in crude nor in multivariable-adjusted models (P > .05). The ANCOVA also revealed that those in the top tertile of the Mediterranean diet score had lower concentrations of serum IL-17A compared to those in the lowest tertile either in the crude and in the multivariable-adjusted models (P < .05). However, this dietary pattern was not associated with serum hs-CRP levels (Table 2).
Multivariate-Adjusted Geometric Means of Inflammatory Markers Based on Tertiles of Dietary Patterns Score.
Abbreviations: BMI, body mass index; hs-CRP, highly sensitive C-reactive protein; IL-7A, interleukin 17A.
a P values for the comparison of mean inflammatory markers across tertiles of dietary patterns’ scores. All analyses were conducted using the analysis of covariance (ANCOVA). Values with different superscripts are significantly different (P < .05); the post hoc comparisons were conducted using Bonferroni test.
b Values are reported as means ± standard errors (SEs) of log-transformed values for inflammatory markers.
c Adjusted for age and energy intake (kcal/d).
d Additionally adjusted for marriage status (married/single), physical activity (sedentary/high), education level (college/bachelor degree/master degree or higher), lifestyle change in recent year (yes/no), current oral contraceptive use (yes/no), menstruation status (pre/postmenopausal), economic status (low/middle/high), and disease history (yes/ no) plus variables in model 1.
e Adjusted for variables in model 2 plus omega 3 (yes/no), calcium (yes/no), vitamin D (yes/no), and multivitamin–mineral (yes/no) supplementation.
f Additionally adjusted for BMI (kg/m2) and waist circumference (cm).
To confirm the linear association between dietary patterns’ scores and serum inflammatory markers, linear regression was applied in crude and multivariable-adjusted models (Table 3). The analysis showed that there is a significant inverse association between DASH dietary pattern score and serum hs-CRP levels in either crude (P = .05) or confounder-adjusted models (P = .04). The DASH diet score was not linearly associated with serum IL-17A levels (Table 3). Our analysis showed that there is an inverse linear association between Mediterranean diet and serum IL-17A levels (P = .04). This association remained significant after adjustment for all possible confounders (P = .01). Mediterranean diet was also marginally associated with lower hs-CRP levels in the raw model (P = .06). However, this association did not remain significant after further adjustment for confounders (P > .05).
The Linear Association Between Dietary Pattern’s Score and Markers of Systemic Inflammation.
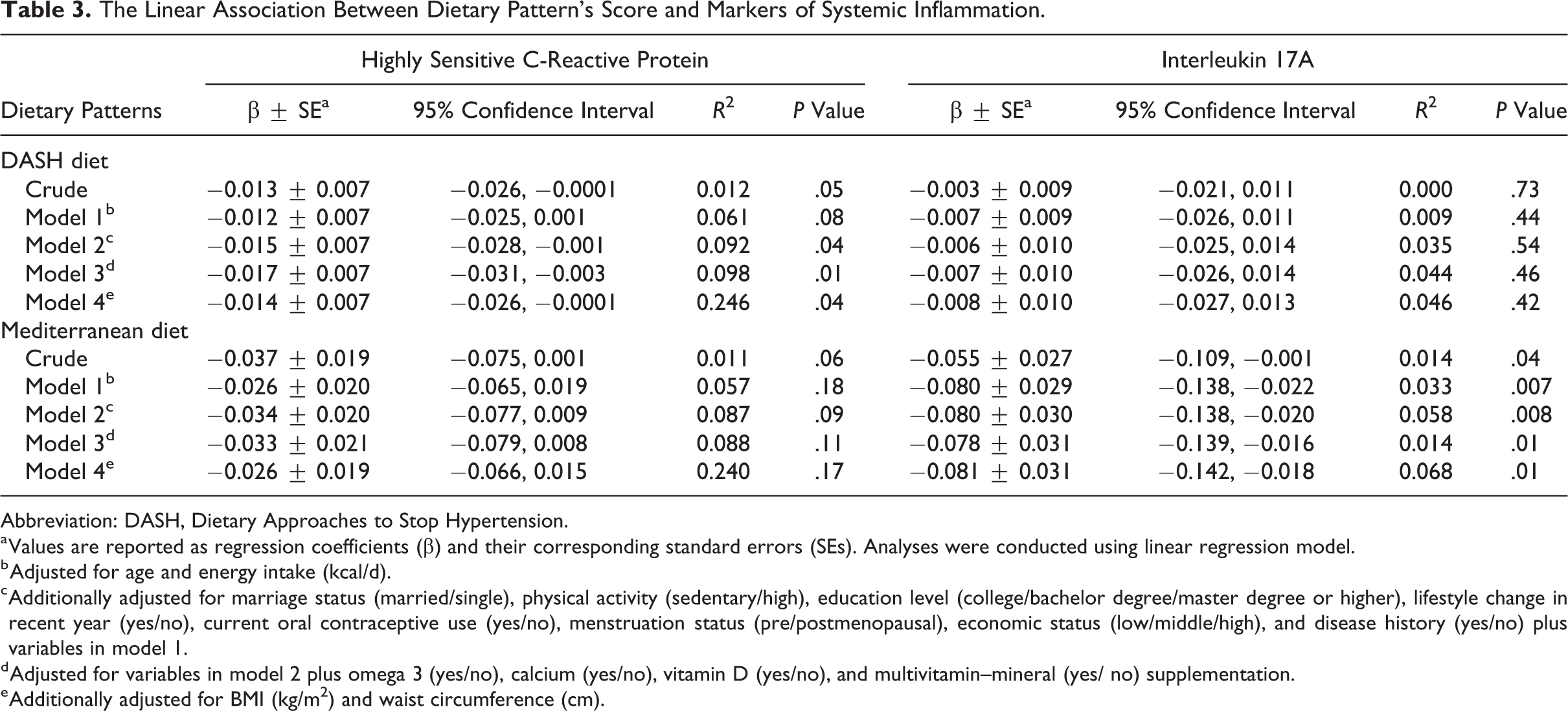
Abbreviation: DASH, Dietary Approaches to Stop Hypertension.
a Values are reported as regression coefficients (β) and their corresponding standard errors (SEs). Analyses were conducted using linear regression model.
b Adjusted for age and energy intake (kcal/d).
c Additionally adjusted for marriage status (married/single), physical activity (sedentary/high), education level (college/bachelor degree/master degree or higher), lifestyle change in recent year (yes/no), current oral contraceptive use (yes/no), menstruation status (pre/postmenopausal), economic status (low/middle/high), and disease history (yes/no) plus variables in model 1.
d Adjusted for variables in model 2 plus omega 3 (yes/no), calcium (yes/no), vitamin D (yes/no), and multivitamin–mineral (yes/ no) supplementation.
e Additionally adjusted for BMI (kg/m2) and waist circumference (cm).
Discussion
The current study was designed to examine the DASH diet and the Mediterranean diet in association with systemic proinflammatory markers among female teachers. Our hypothesis was that both the DASH and the Mediterranean diets might be inversely associated with inflammatory markers, and this was accepted by the study results; on the one hand, it was shown that the higher concordance with DASH diet is associated with lower hs-CRP levels, while it was not significantly related to IL-17A levels. On the other hand, the Mediterranean diet was inversely associated with IL-17A; however, the relation between the Mediterranean diet and hs-CRP levels was not significant. The dose–response analysis using linear regression also confirmed the same associations. Therefore, we also accepted that these healthy dietary patterns might be differently associated with the 2 selected markers of inflammation.
The IL-17A is predominantly synthesized by T-helper 17 cells and is suggested to be as an inducer of tissue-mediated innate immunity by triggering proinflammatory chemokines, cytokines like TNF-α, IL-1, IL-6, granulocyte–macrophage and granulocyte colony-stimulating factors, antimicrobial peptides, and tissue remodeling and acute-phase responses. 51 Interleukin 17A is associated with a wide range of diseases, particularly autoimmune diseases. 51 The hs-CRP is an acute-phase inflammatory marker that is released predominantly by hepatocytes in response to proinflammatory cytokines, such as TNF, IL-1, and IL-6. 52 It is suggested that IL-17 triggers IL-6, which in turn increases hs-CRP levels; however, we could not find any correlation between IL-17a and hs-CRP concentrations. It is suggested that the increased IL-17 concentration cannot be interpreted as a simple reflection of acute-phase activation, and it seems that IL-17 is related to wider immune/inflammatory responses independent from the acute-phase response. 53
The DASH diet is determined by the high content of fiber, nuts, and low-fat dairy products and contains higher amounts of antioxidant nutrients such as vitamins A, C, and E, which are proposed to be beneficial to human health. 34,48,54 The effects of the DASH diet on inflammatory markers, such as IL-6, CRP, TNF-α, and Soluble intercellular adhesion molecule-1 (ISCAM), have previously been studied. 34,48,55 Studies have revealed that high intake of dairy products is associated with a lower concentration of CRP levels. 34,55 Conjugated linoleic acid, riboflavin, and high-quality protein, which are present in dairy products, might beneficially affect systemic inflammation. 56,57 The DASH diet is also high in fiber and antioxidant-rich fruits and vegetables that might reduce circulatory CRP levels. 58 -60 Moreover, the DASH diet is low in glycemic index that is also inversely associated with inflammation. 61 A recent meta-analysis demonstrated the beneficial effects of the DASH diet on circulating hs-CRP levels compared to unhealthy/usual diets. 62 The Mediterranean diet is high in monounsaturated fat and low in saturated fat; the main source of fat in this diet is olive oil, which contains monounsaturated fatty acids. 63,64 Moreover, the Mediterranean diet contains complex carbohydrate from legumes, and the main source of fibers is vegetables and fruits. High intake of antioxidants through vegetables and fresh fruits, cereals, and olive oil, which are high in β-carotene, vitamin C, vitamin E, and other different minerals, might have resulted in low IL-17A levels in participants who had higher adherence to the Mediterranean diet. 39,47,65 A cross-over study demonstrated that high-fat, high-energy diet increase IL-17 plasma levels, whereas healthy mixed fruit juices significantly reduce the production of IL-17 and other inflammatory markers. 66 It is also revealed that higher adherence to the Mediterranean diet is inversely associated with several inflammation markers, including IL-6 and hs-CRP. 28,29,67 In contrast, we observed a marginally significant linear inverse association between adherence to the Mediterranean diet and serum hs-CRP levels; however, the association became nonsignificant after adjusting possible confounders. This shows that the intake of other food groups that were not considered in this pattern might predict serum hs-CRP levels in this population.
The DASH and the Mediterranean diets are both regarded as healthy diets; however, there are some differences in the recommendations between these 2 dietary patterns, and these differences in the recommendations might have resulted in different associations found between dietary patterns and inflammatory markers in the present study. Reduction in sodium intake plays a key role in the DASH diet recommendations, whereas the Mediterranean diet offers no suggestion about the sodium intake. Both diets suggest low saturated fat intake and advocate higher intake of vegetable oils; however, the Mediterranean diet insists on the olive oil intake. Another major difference between these 2 diets that might explain their difference in association with serum IL-17A levels is the amount of dairy products intake. The DASH diet recommends the consumption of low-fat or nonfat dairy products; however, lower intakes of dairy are suggested in the Mediterranean diet. 47 It is proposed that dairy consumption is positively associated with reduced serum CRP levels in human adults. 68 A study on the association between food groups’ intake and IL-17F among children 69 also revealed that vegetables or grains are associated with lower levels of IL-17F, whereas consumption of dairy or sweets was associated with higher IL-17F.
To the best of our knowledge, the present study was the first study that investigated the relationship between a priori dietary patterns and IL-17A. Furthermore, in the present study, we were able to control the association between dietary patterns score and inflammatory markers for the maximum number of possible confounders. In addition, we could represent both the linear and the nonlinear association by exploring the inflammatory markers’ concentration across tertiles of the dietary patterns’ scores.
The current study has a number of limitations that should be considered when interpreting its results. It should be noted that the sample size in our study was small, and we just examined the association in female teachers. Therefore, generalizing the findings should be done with caution. It would be of great interest to include both women and men in the future studies. In addition, although statistically significant differences in the inflammatory markers were found across tertiles of dietary patterns’ scores, the size of the effects was small. However, the differences found were confirmed using linear regression analysis. The small effects found in the present study might be because of the limited number of sample size in each tertile and including participants with chronic conditions in the same analysis. It would be better to examine the associations separately in those with and without chronic diseases and based on age; however, we did not conduct the stratified analysis because of the limited sample size. The age and the distribution of participants with history of chronic diseases were not significantly different between tertiles of the dietary patterns’ scores, and also, we tried to adjust both variables in multivariable models. In addition, although we tried to control for several confounding variables in our analyses, residual confounding from unknown or unmeasured factors such as other medications use (aspirin or statin) is inevitable. As the present study was cross sectional in its design, casual association between dietary patterns and the inflammation cannot be inferred from its results; therefore, conducting prospective cohort studies is highly recommended. Furthermore, randomized controlled clinical trials investigating the effect of DASH and/or Mediterranean diet compared to a control diet on IL-17A levels might be more conclusive. Moreover, using FFQ for assessment of the dietary patterns has its own limitations, such as measurement error and misclassification of the study participants and reporting bias; however, we tried to reduce these problems using a modified version of a validated FFQ and excluding the over- and underreporters by removing those who reported unreasonable amounts of energy intake. It should also be noted that within-person variation might lead to attenuated associations if inflammatory markers are measured once in the epidemiologic studies like the present study and the differences might be even larger if several samples were assessed for each participant. 70
In conclusion, our results showed that the adherence to the DASH diet is significantly associated with reduced serum hs-CRP concentrations, whereas it was not significantly related to serum IL-17A levels. Furthermore, higher conformity to the Mediterranean diet might be associated with lower circulating IL-17A concentrations, but not hs-CRP levels. Future prospective cohort studies are recommended to confirm our results.
Footnotes
Acknowledgments
The authors would also like to thank all teachers involved in the study; without their collaboration, the authors could not accomplish the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was extracted from a thesis for MSc degree in nutrition and was funded by the international campus of Shahid Sadoughi University of Medical Sciences, Yazd, Iran.