
Abstract
Wasting, stunting, and anemia are persistent and important forms of malnutrition in preschool-age children in the less developed world, in particular the Republic of Guinea, which was the site of a large outbreak of Ebola virus disease in 2014 to 2015. We analyzed data from 3 Demographic and Health Surveys done in Guinea in 1999, 2005, and 2012 to identify possible determinants of wasting, stunting, and anemia. All analyses, both bivariate and multivariate, were carried out separately for each of 3 age groups: less than 6 months, 6 to 23 months, and 24 to 59 months. Variables found statistically significantly associated with stunting, wasting, or anemia in bivariate analysis were placed in an age-specific logistic regression model for that outcome. Overall, anthropometric indices were available for 9228 children and hemoglobin concentrations were available for 5681 children. Logistic regression found relatively few variables associated with nutrition outcomes in children younger than 6 months. More variables were associated with nutrition outcomes in children aged 6 to 23 months. Such variables measured a wide variety of conditions, including estimated birth size, child health and nutritional status, child caring practices, mother’s nutritional and health status, and household water source and sanitation. A similarly broad range of variables was statistically significantly associated with one or more nutrition outcomes in children aged 24 to 59 months. Few of the standard infant and young child feeding indicators were associated with any nutrition outcome. Improvement in the nutritional status of young children in Guinea may require a broad range of nutrition and health interventions.
Introduction
Stunting, wasting, and anemia in children younger than 5 years have important short- and long-term consequences. 1 As a result, reduction in stunting and wasting played a major part in attempts to achieve the 2015 targets for nutrition and child mortality listed in the Millennium Development Goals. 2 To direct future efforts, reductions in and eventual elimination of stunting and wasting are also mentioned in the Sustainable Development Goals for the year 2030 and the World Health Assembly Global Nutrition Targets for the year 2025. 3,4 Although these documents do not directly address anemia in young children, they all mention reducing anemia in reproductive-age women as an important public health goal.
Malnutrition remains a major public health problem among children in Guinea. According to the 2012 Demographic and Health Survey (DHS) in Guinea, 31.2% of children aged 5 years were stunted, 9.6% were wasted, and 76.6% were anemic. 5 These indicators denote a very severe or severe public health problem according to World Health Organization (WHO) classifications. 6,7 Moreover, the prevalence of various forms of malnutrition remained largely unchanged in the past 10 to 15 years. 5,8,9 The recent Ebola crisis has severely disrupted an already weak health system. As of March 27, 2016, a total of 3811 cases of Ebola virus disease had been recorded in Guinea, resulting in 2543 deaths. Both community-based nutrition interventions and institution-based nutrition services were heavily hit by the epidemic. Following the crisis, the Guinea government, with support from its development partners, developed a multiyear recovery plan. To better inform nutrition programming in Guinea during this post Ebola recovery phase, we aimed at identifying the main determinants of stunting, wasting, and anemia in children younger than 5 years.
Methods
Data Sources
Data for this analysis came from the 3 most recent DHS carried out on nationally representative samples of households in Guinea in the years 1999, 8 2005, 9 and 2012. 5 More detailed descriptions of the methods used in these surveys are included in the survey reports, as well as other publications. 10,11 Table 1 below shows the dates of data collection and the number of households, mother–child pairs, children with valid length- or height-for-age Z-scores (HAZ) and weight-for-height Z-scores (WHZ), and children with valid hemoglobin concentrations in each survey. Biological children of eligible women in all selected households were weighed and measured in the 1999 survey, but in the 2005 and 2012 surveys, all children residing in a subsample of one-half of the selected households were recruited into the survey sample regardless of whether the biological mother was included in the survey sample.
Selected Information about the 3 DHS Surveys Included in Data Analysis.
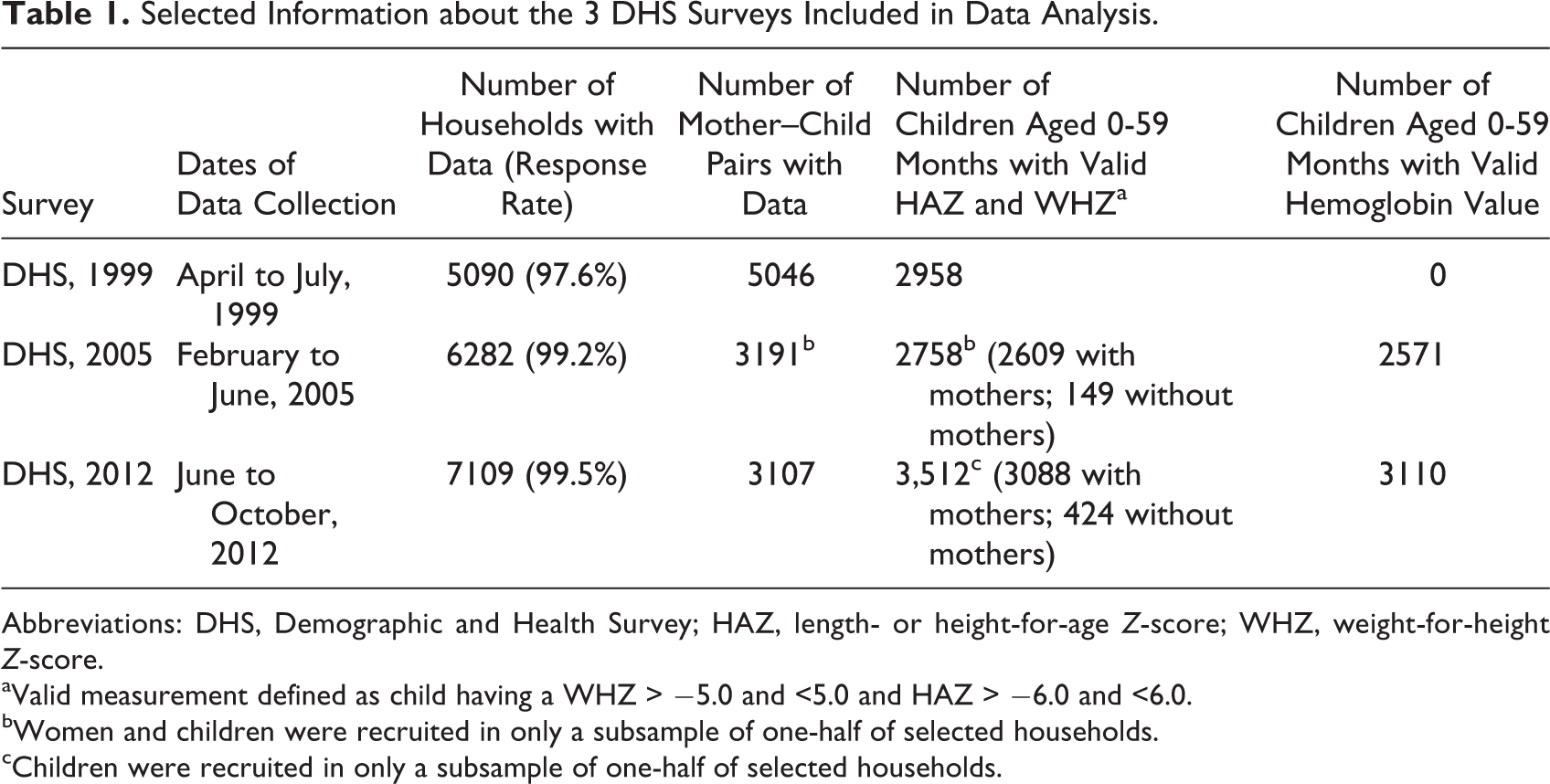
Abbreviations: DHS, Demographic and Health Survey; HAZ, length- or height-for-age Z-score; WHZ, weight-for-height Z-score.
aValid measurement defined as child having a WHZ > −5.0 and <5.0 and HAZ > −6.0 and <6.0.
bWomen and children were recruited in only a subsample of one-half of selected households.
cChildren were recruited in only a subsample of one-half of selected households.
Stunting and wasting were measured in all 3 DHS by measuring the weight of each child along with the length of children younger than 24 months or the height of children aged 24 to 59 months using standard procedures. 11,12 Z-score calculations for all surveys were calculated using the WHO Child Growth Standards. 13 Stunting was defined as having an HAZ less than −2.0 (more than 2 standard deviations below the reference median). Wasting was defined as having a WHZ less than −2.0. As widely recommended, children with HAZ less than −6.0 or greater than +6.0 were excluded from analyses of stunting and children with WHZ less than −5.0 or greater than 5.0 were excluded from analyses of wasting because such indices are considered most likely the result of faulty measurement or recording. 14 The outcomes, wasting and stunting, were analyzed as dichotomous variables (stunted vs not stunted and wasted vs not wasted). Although any child with nutritional edema should automatically be classified as severely wasted regardless of his or her WHZ, these DHS did not collect data on the presence of edema in children. As a result, only the WHZ could be used to indicate acute malnutrition.
Hemoglobin was measured only in the 2005 and 2012 surveys on finger-stick blood using the HemoCue portable hemoglobin meter (HemoCue AB, Ängelholm, Sweden). Hemoglobin results were adjusted for altitude of residence according to standard recommendations. 15 In order to analyze risk factors with the greatest statistical power, children with moderate and severe anemia (hemoglobin concentration: <10 g/L) were compared to children with mild or no anemia (hemoglobin concentration: 10 g/L or greater).
Selection of Factors Potentially Associated With Growth
The recently published WHO conceptual framework on childhood stunting was used to identify the most comprehensive set of factors potentially associated with stunting. 16 Using this framework, the 3 DHS data sets, DHS reference materials, data set maps, and data collection forms were thoroughly reviewed in order to select variables included in the DHS that may be considered potential determinants of stunting in Guinea. A similar review process was carried out to determine factors potentially associated with wasting based on the United Nations Children’s Fund (UNICEF) Nutrition Framework. 17 Because there is no comparable widely recognized framework for anemia, the same variables were analyzed as potential risk factors for anemia. In total, 83 potential risk factors were identified. In addition to values provided directly in the DHS data files, a new household wealth index was calculated on pooled data from all 3 surveys using principal component analysis of the same variables used in the original DHS calculation. 18 This allowed assessment of trends in household wealth between 1999 and 2012.
Data Analysis
The data from all 3 surveys were pooled, and an initial bivariate analysis was carried out separately for each of 3 age groups: children younger than 6 months, children aged 6 to 23 months, and children aged 24 to 59 months. These age-specific analyses were done because potential determinants of stunting, wasting, and anemia are thought to be quite different among children of different ages.
Depending on the DHS, some variables were collected using different questions or different response coding. For example, dietary diversity was not measured in children in the 1999 DHS. Although 24-hour dietary diversity was measured in both the 2005 and 2012 DHS, the food categories utilized were not consistent and required recoding to have harmonized response options. Only in the DHS 2012 was dietary diversity measured in accordance with new standard recommendations on the assessment of infant and young child feeding (IYCF), which were published in 2010. 19
In addition, some variables were not collected in all surveys; analyses of such variables were, by necessity, restricted to those children included in those surveys in which the variable exists. For such variables, fewer children in the combined data sets have data available and could be included in specific analyses. As a result, the number of children included in each analysis is different for different potential determinants. Data on other variables may not have been collected for all children in a specific age category. For example, measles vaccination status has little meaning for children younger than the recommended age of receipt of 9 months. 20 As a result, this variable could not be analyzed for children in the age category of less than 6 months and in the age category of 6 to 23 months, only children aged 9 months or older could be included.
Some variables were combined into indices or summary measures. For example, the woman’s questionnaire for the DHS in 2005 and 2012 included questions which asked women which of 5 circumstances justified being beaten by her partner. A score was calculated by giving each circumstance 2 points if cited as justification and summing the 5 circumstances. Thus, possible scores ranged from 0 if none of the 5 circumstances justified beating and 10 if all 5 justified beating.
Variables associated with stunting, wasting, or anemia with statistical significance in the bivariate analysis, as defined as a P value less than .05, were included in age-specific logistic regression models. However, certain variables were excluded from the regression models regardless of their statistical significance in bivariate analysis. The most common reason was that the data for a variable were collected in only 1 survey, and its inclusion in the model would decrease the sample size too much. For example, whether a child’s household drinks safe water is most commonly defined using a combination of safe water source and adequate home treatment; however, information on home water treatment was collected only in the 2012 survey. Instead, only the safety of the water source from which drinking water was obtained was included in the regression model. A second reason for excluding a variable was that exposure was rare. For example, the child’s biological mother was dead for only 54 (0.9%) of 6270 children for whom this information was collected in the 2005 and 2012 surveys. A third reason for excluding a variable was if it duplicated the information contained in another variable. For example, place of delivery and having a skilled attendant at delivery are, for the most part, redundant. Of the 5558 women reporting delivery at home, none had a skilled attendant, and of the 3039 women reporting delivery in a health facility, only 80 (2.6%) reported not having a skilled attendant.
Once the list of variables to be included in logistic regression was determined, backward elimination of those variables which did not contribute to the model with statistical significance, that is, with a P value of less than .05, was carried out until all factors were statistically significant. However, even if not statistically significant in the model, a factor was retained if its removal caused a substantial decline in the overall explanatory power of the model, as indicated by a decrease in the Nagelkerke statistic of 10% or more.
All data analyses were carried out using SPSS version 23. Measures of precision, such as adjusted χ2 P values and confidence intervals, were calculated accounting for the clustered and stratified sampling employed by DHS. As per recommendations from DHS, no statistical weighting was used for bivariate or multivariate analyses. 21
Results
Overall, anthropometric indices were available for 9228 children and hemoglobin concentrations were available for 5681 children younger than 5 years in all 3 surveys. The prevalence of stunting rises with age, from 12.6% in children younger than 6 months to 27.2% in children aged 6 to 23 months and to 41.3% in children aged 24 to 59 months. The prevalence of wasting peaks in children aged 6 to 23 months: 13.5% in children younger than 6 months, 16.4% in children aged 6 to 23 months, and 5.6% in children aged 24 to 59 months. The prevalence of anemia similarly peaks in this age-group: 34.4% in children younger than 6 months, 64.3% in children aged 6 to 23 months, and 47.0% in children aged 24 to 59 months.
Bivariate Analyses
The complete results of bivariate analysis of the association between each factor and stunting, wasting, and moderate and severe anemia are shown in Supplemental Tables 1 to 3. Overall, for all 3 nutrition outcomes, fewer variables are statistically significantly associated in children younger than 6 months compared to the older age groups. This is true even for those factors concerning fetal health and growth. Relatively few factors measuring child dietary intake and nutritional status are statistically significantly associated with any of the 3 nutrition outcomes. Many more factors measuring environmental and sanitation risks to health are associated with stunting than with wasting or anemia.
Logistic Regression Analysis of Stunting
The 3 age-specific logistic regression models of the correlates of stunting are shown in Table 2. In children younger than 6 months, among variables reflecting fetal health and growth, only estimated birth size remains statistically significantly associated with stunting. The only other variables in the model are being a twin and mother’s receipt of vitamin A supplementation after delivery. The model includes no variables measuring child nutrition and feeding, child health, household wealth, sanitation and environmental hygiene, women’s empowerment, or other demographic characteristics. Although being a twin seems to be most strongly associated with stunting, the wide confidence intervals around the odds ratios for all 3 variables do not permit definitive conclusions about their relative strengths of association.
Final Logistic Regression Models for Stunting for Children Younger Than 6 Months, 6 to 23 Months, and 24 to 59 Months.
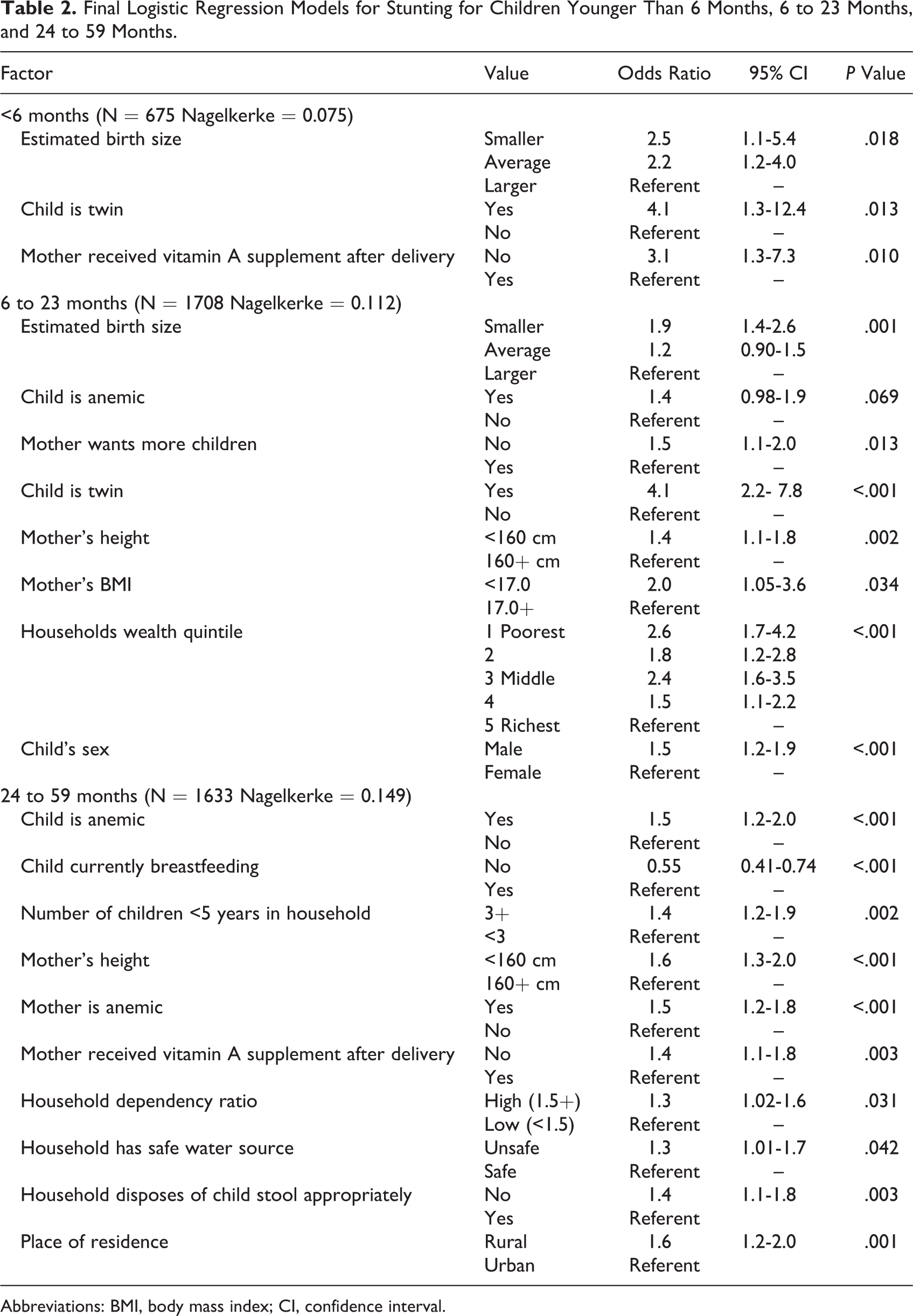
Abbreviations: BMI, body mass index; CI, confidence interval.
The final logistic regression model for children aged 6 to 23 months includes more variables. However, few child feeding or health variables remained in this model because most such variables showed no statistically significant associations with stunting in the bivariate analysis, and the remainder did not contribute significantly to the model. Estimated birth size, child anemia, and being a twin are also associated with stunting in this age-group, as well as measures of mothers’ nutrition status and household wealth. In this age-group, boys were more likely to be stunted than girls. Being a twin again has the strongest association with stunting. Many variables in this final model, such as mother wanting more children, are relatively weakly related to stunting, with most odds ratios being 2.0 or lower.
For children aged 24 to 59 months, child’s anemia and current breastfeeding, which measure child nutrition and feeding, remain in the logistic regression model, but no variables measuring child health remain. The only variable measuring child caring remaining in the model is the number of children less than 5 years in the household. Measures of mother’s nutrition status (mother’s height, mother’s anemia, and receipt of vitamin A supplementation after delivery) remain in the model, as do the household dependency ratio. Water source and disposal of child’s stools as measures of environmental sanitation and hygiene remain. As with younger children, no measures of women’s empowerment are statistically significantly associated with stunting. However, in this age-group, rural children are more likely to be stunted than urban children. All of these associations are relatively weak, with odds ratios less than 2.0. Moreover, current breastfeeding, regardless of whether it is exclusive, is a risk factor; breastfed children in this age-group are more likely to be stunted than children who are not breastfed.
None of the regression models account for a large proportion of the variance in the outcome stunting. In the oldest age-group, only about 15% of variance is explained by the 10 variables in the model, and a smaller proportion of variance is explained by the fewer variables in the models for younger children.
Logistic Regression Analysis of Wasting
The 3 age-specific logistic regression models of the correlates of wasting are shown in Table 3. For children younger than 6 months, none of the measures of antenatal care remain significant in the final model. Like stunting, mother’s postpartum receipt of vitamin A remains in the model, but unlike stunting, estimated birth size does not. The final model includes only 1 household wealth and demographic variable, education of mother’s partner, and 1 measure of environmental sanitation and hygiene, disposal of child’s stools. No variables in other categories are significantly related to wasting in logistic regression; these categories include variables measuring fetal health and growth, child nutrition and feeding, child health, child caring practices, women’s empowerment, or other demographic characteristics.
Final Logistic Regression Models for Wasting for Children Younger than 6 Months, 6 to 23 Months, and 24 to 59 Months.
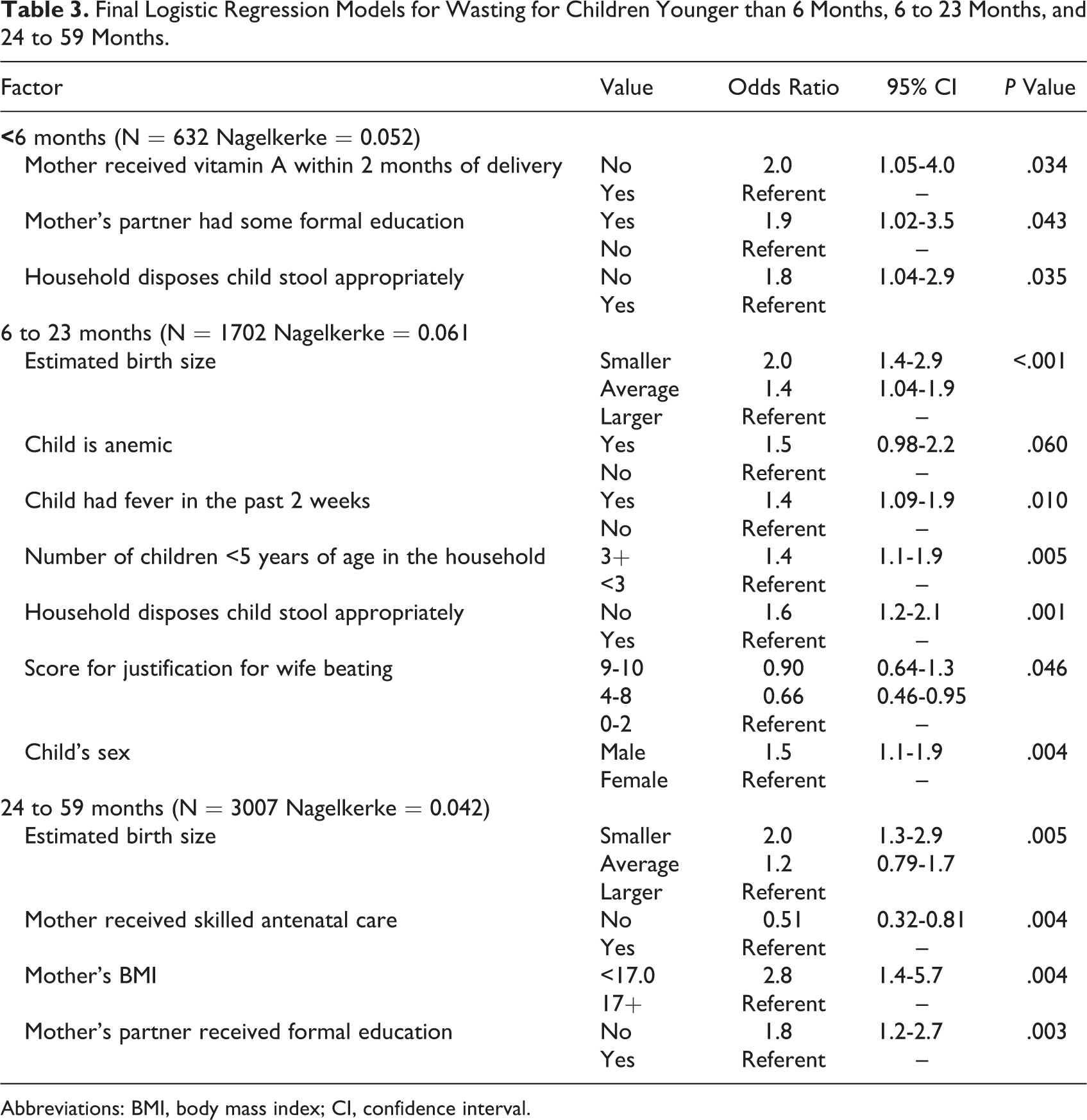
Abbreviations: BMI, body mass index; CI, confidence interval.
The final logistic regression model for children aged 6 to 23 months includes variables measuring fetal health and growth, child nutritional status, and child health status but does not include dietary intake or feeding variables. Unlike the younger children, variables measuring child caring practices and women’s empowerment remain in the final model. Moreover, as with stunting, boys are more likely to be wasted than girls.
Variables measuring fetal health and growth, mother’s nutritional status, and household wealth remain in the logistic regression model for children aged 24 to 59 months. However, variables measuring child nutrition and feeding, child caring practices, child’s nutrition and feeding, child’s health, environmental sanitation and hygiene, or women’s empowerment are not statistically significantly associated with wasting in logistic regression.
In all 3 models, the strength of association between each variable and wasting is relatively weak. Only mother’s body mass index (BMI) in the model for children aged 24 to 59 months has an odds ratio greater than 2.0. Moreover, these 3 logistic regression models account for 6% or less of the variability in wasting, substantially less than the models for stunting. Unlike stunting, all 3 age groups show similarly poor explanatory power.
Logistic Regression Analysis of Anemia
The 3 age-specific logistic regression models of the correlates of moderate and severe anemia are shown in Table 4. Unlike stunting and wasting in children younger than 6 months, measures of child health are statistically significantly associated with anemia in logistic regression in this age-group. In addition, a measure of child caring is also associated. However, the final model does not include measures of fetal health and growth, child nutrition and feeding, mother’s health and nutritional status, household wealth and demographic characteristics, environmental sanitation and hygiene, or women’s empowerment. Although the association between child diarrhea and anemia is not statistically significant, this variable was retained because it substantially improves the explanatory power of the model. A greater total number of children born to the mother is protective; children whose mothers have 4 or more previous deliveries are less likely to be anemic than children of mothers with fewer deliveries.
Final Logistic Regression Model for Moderate and Severe Anemia for Children Younger than 6 Months, 6 to 23 Months, and 24 to 59 Months.
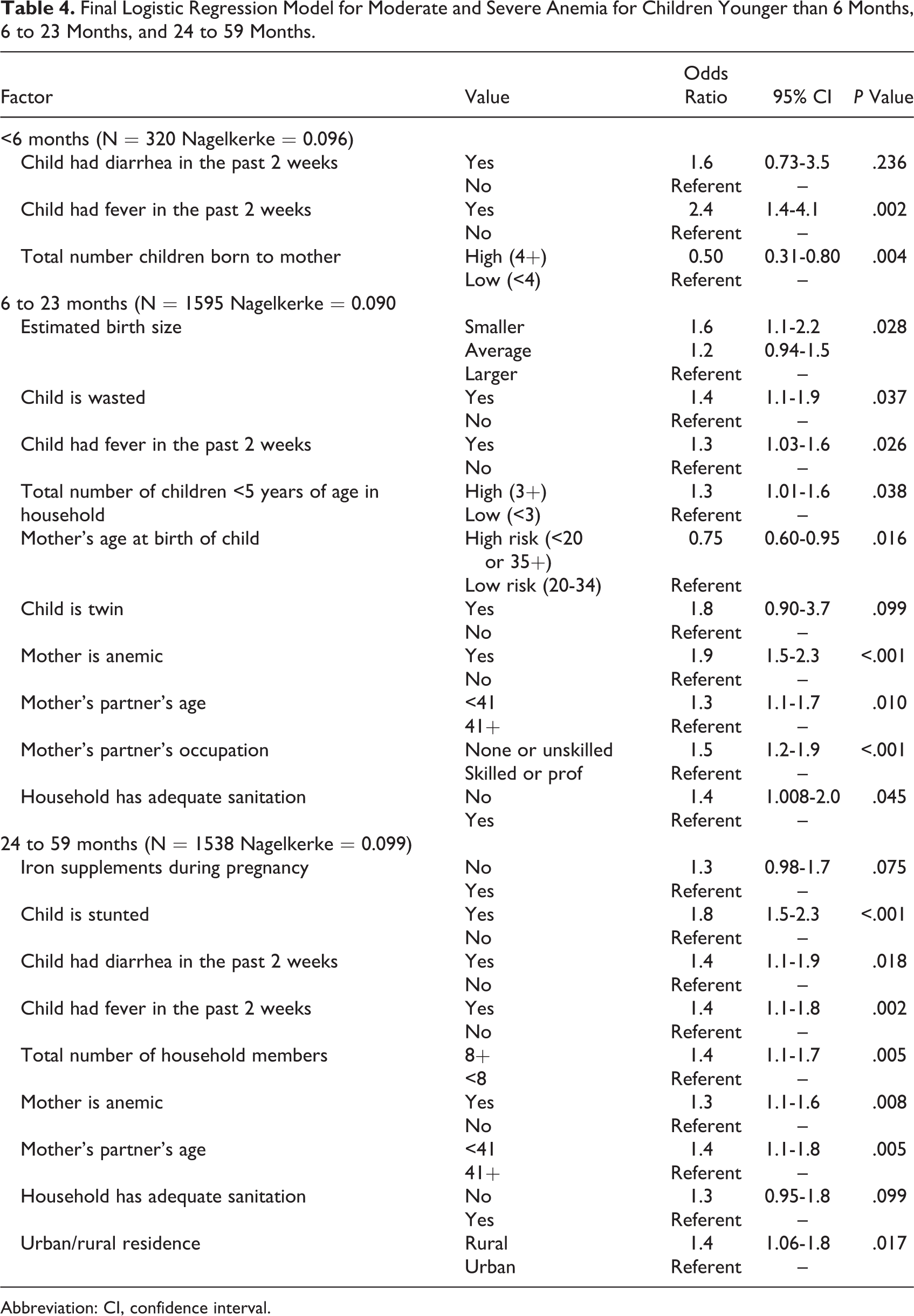
Abbreviation: CI, confidence interval.
The final logistic regression model for children aged 6 to 23 months includes variables measuring fetal health and growth, child nutritional status, child health, child caring practices, mother’s health and nutritional status, household wealth and demographic characteristics, and environmental sanitation and hygiene. The only category of variables missing from this model is women’s empowerment. Nonetheless, no measures of IYCF, including the standard indicators, is statistically significantly associated with anemia. Paradoxically, children born when their mothers were at younger or older ages with higher risk of complications of pregnancy and delivery were less likely to be anemic.
For children aged 24 to 59 months, the categories of variables remaining in the logistic regression model for anemia are similar to that in the model for children aged 6 to 23 months; however, the specific variables may differ. For example, instead of estimated birth size as a measure of fetal health and growth, the model in older children retains only iron supplementation during pregnancy. Instead of wasting in younger children, stunting is associated with anemia in older children. In addition, children living in rural areas are more likely to be anemic than children in urban areas.
As with wasting, the strength of association between variables in all 3 models and moderate and severe anemia is relatively weak, with the majority of odds ratios being 1.5 or less. And as with both stunting and wasting, the explanatory powers of the models for anemia are poor; all 3 models explained only 9% to 10% of the variability in anemia.
Discussion
Of the 83 variables measured in DHS and included in this analysis, relatively few proved statistically significantly associated with stunting, wasting, or anemia in multivariate modeling and none showed a strong association. In addition, there is no single or small group of risk factors which play a predominant role in determining wasting, stunting, or anemia in Guinea. Nonetheless, those possible determinants of malnutrition remaining in the final logistic regression models represent a broad range of factors. These include variables measuring fetal growth and health, child nutritional status, child health, child caring practices, mother’s nutritional status, household wealth and demographic characteristics, sanitation and environmental hygiene, women’s empowerment, and basic demographic characteristics. Many other studies from various parts of the world, including analyses of DHS data, have identified similarly broad ranges of factors associated with stunting, wasting, or anemia 22 –26 and confirm that multiple factors simultaneously contribute to these forms of malnutrition.
For children younger than 6 months, the odds of being stunted or wasted were much higher in children whose mothers were not supplemented with vitamin A after delivery. Postpartum vitamin A supplements have been shown elsewhere to increase retinol concentrations in breast milk for 4 to 6 months, improve vitamin A status of the breastfed child, and reduce the severity of illness during infancy. 27,28 Furthermore, other analyses have found vitamin A supplementation during pregnancy has resulted in improved linear growth of the mother’s child. 29 Thus, it is likely that maternal supplementation postpartum in Guinea helps to prevent growth faltering by improving immune function and reducing the disease burden during early infancy.
Recent diarrhea, recent fever, and total number children born to the mother were associated with anemia in children younger than 6 months. While diarrhea and fever have been associated with anemia in other studies, 32 it is difficult to speculate how increased number of children born could result in increased hemoglobin levels. To explore this further, we conducted ancillary bivariate analyses of the number of children born to the mother and various factors related to antenatal care, micronutrient supplementation during pregnancy, delivery, and breastfeeding, as these could potentially influence hemoglobin in children younger than 6 months (results not shown). No potentially explanatory associations were found. 30–32
Overall, many fewer possible risk factors were identified in children younger than 6 months than in older children. This may be because these children are less exposed to environmental factors outside of the household. It may also be due to using P values to select variables for inclusion in multivariate analysis. Because this age range is substantially narrower compared to the age groups of 6 to 23 months and 24 to 59 months, the number of children included in both bivariate and multivariate analyses is less than that in the other age groups, leading to higher P values for any given strength of association.
Few child feeding indicators were associated with stunting, wasting, or anemia, and of the 5 core WHO/UNICEF IYCF indicators 19 measured in these DHS, none were associated with stunting, wasting, or anemia. In other countries, associations between these child feeding variables and stunting and wasting have been mixed. A similar study using pooled DHS data from Ethiopia found no association between these core IYCF indicators and stunting. 33 In an analysis of DHS data from 9 countries, Jones et al 34 found consistent associations between HAZ and minimum acceptable diet and minimum dietary diversity; however, these same IYCF variables were not strongly associated with being stunted when defined as a dichotomous variable. One factor which may explain at least some of the variability in results is the fact that IYCF indicators only count the food groups consumed during a 24-hour recall to measure long-term dietary quality. In contrast, stunting and anemia are measures of nutrition and health status which result from long-term exposure to multiple factors. 35 In addition, IYCF indicators measured for children aged 6 to 23 months, such as minimum dietary diversity, minimum meal frequency, and minimum acceptable diet, do not directly reflect other IYCF behaviors that influence growth, such as the timely introduction of complementary foods. Timely introduction of complementary foods is, according to the WHO/UNICEF recommendations, 19 calculated only for children aged 6 to 8 months.
Our analysis of children aged 24 to 59 months found that breastfeeding was a risk factor for stunting. A systematic review on the association between nutritional status and continued breastfeeding at age 2 years and older indicates mixed results. 36 In contrast, studies of continued breastfeeding at younger ages have found that it increases the risk of stunting. Jones et al found that “continued breastfeeding for 1 year was…significantly negatively associated with HAZ in Ethiopia as well as Zimbabwe…and demonstrated similar, although nonsignificant, trends in all other countries.” 34 Although DHS data do not enable us to measure nutrient intake, our findings may suggest that breastfeeding of older children contributes to stunting by reducing caloric and nutrient intake from complementary foods.
Variables measuring various components of fetal health and growth, especially estimated birth size, remained potential determinants of stunting, wasting, and anemia even in older children. Similar findings were presented in a recent study by Danaei et al 37 who investigated the risk factors for stunting in children aged 24 to 35 months in 137 countries. These researchers found being born small for gestational age was the leading risk factor for stunting in 2-year-olds worldwide, contributing to nearly 11 million cases of stunting. In our analysis, variables measuring the current health and nutritional status of children were less consistently associated with nutrition outcomes. As expected, recent diarrhea or fever was associated largely with wasting, but not with stunting or anemia. In contrast, child caring practices were associated with stunting and anemia, but not wasting. Several variables reflecting mother’s nutritional and health status (including mother’s height, mother’s BMI, whether mother is anemic, and whether mother received vitamin A after delivery) were associated with stunting in children aged 6 months and older, but less so with wasting and anemia. Household wealth and demographic factors showed little consistent pattern of association; those variables associated with one form of malnutrition were not associated with other forms.
Regardless of the number of variables in the final logistic regression models, the overall explanatory power of each of the models was relatively small, as indicated by the Nagelkerke statistic. None of the models explained more than 15% of the variability in the nutrition outcome of that model. This implies either that the variables available in DHS and included in this analysis do not determine the majority of malnutrition or that the indicators measured in the DHS do not accurately and precisely measure the factors they are meant to measure. The former may be true to some extent, but the broad range of variables available in DHS measure the majority of factors contained in conceptual models of malnutrition. 16 One major exception is any direct measure of household food security. Nonetheless, it may be more likely that the nature of data collection in large cross-sectional surveys collecting data on many variables during long interviews may lead to recall bias and error. Moreover, the indicators used during such surveys may not perfectly measure the target conditions or behaviors. For example, IYCF indicators of dietary diversity and adequacy require recall of every food a child ate in the past 24 hours. Such detail may not be recalled perfectly during interviews. In addition, variables concerning pregnancy, antenatal care, and delivery require recall of occurrences months or years in the past. Such data may be subject to random error which would lead to underestimating the strength of association and identifying fewer variables as statistically significantly associated with a nutrition outcome.
Some studies analyzed all children younger than 5 years together, 24 –26,38,39 whereas others separately analyzed children aged 0 to 23 months with or without an overall analysis of children younger than 5 years. 23,40,41 Although separate analyses of children of different ages may decrease the available sample size for any specific analysis, the very different factors identified for the same nutrition outcome in the 3 age groups used in our study demonstrate that analysis of all children less than 5 years of age together may produce misleading summary estimates of the association between specific factors and specific forms of malnutrition. Age is clearly an effect modifier for many possible risk factors and should be taken into account by performing separate analyses of the determinants of wasting, stunting, and anemia. Specifically, children younger than 6 months should be analyzed separately from older children.
Although our analysis identified multiple factors associated with stunting, wasting, and anemia, some factors, such as urban/rural residence, child being a twin, or child’s sex, are not subject to modification by program interventions. Table 5 shows those factors which can be modified. Some of these factors, although modifiable, may require general social changes, such as enhanced education, alleviation of poverty, or changes in women’s status. Other factors are often targeted by nutrition and health programs, for example, provision of antenatal care and supplementation to pregnant women, family planning services for women, education for mothers regarding complementary feeding, and sanitation and hygiene education. These factors can be directly addressed by Guinean nutrition and health decision makers. Many of these factors reflect maternal health and nutrition starting even prior to pregnancy. Furthermore, other analyses in Guinea show a trend toward increased prevalence of underweight in adolescents along with persistently high anemia prevalence among reproductive-age women in general. 42 Also, about a quarter of adolescent girls aged 15 to 19 years have already delivered a child or are pregnant in Guinea. 5 These factors combined indicate that improving nutrition and health of adolescent girls is not only important for them but will also improve the nutritional status of their future children.
Overview of Modifiable Variables Remaining Significant in Regression Models for Stunting, Wasting, and Anemia in Children Younger Than 6 Months, 6 to 23 Months, and 24 to 59 Months.
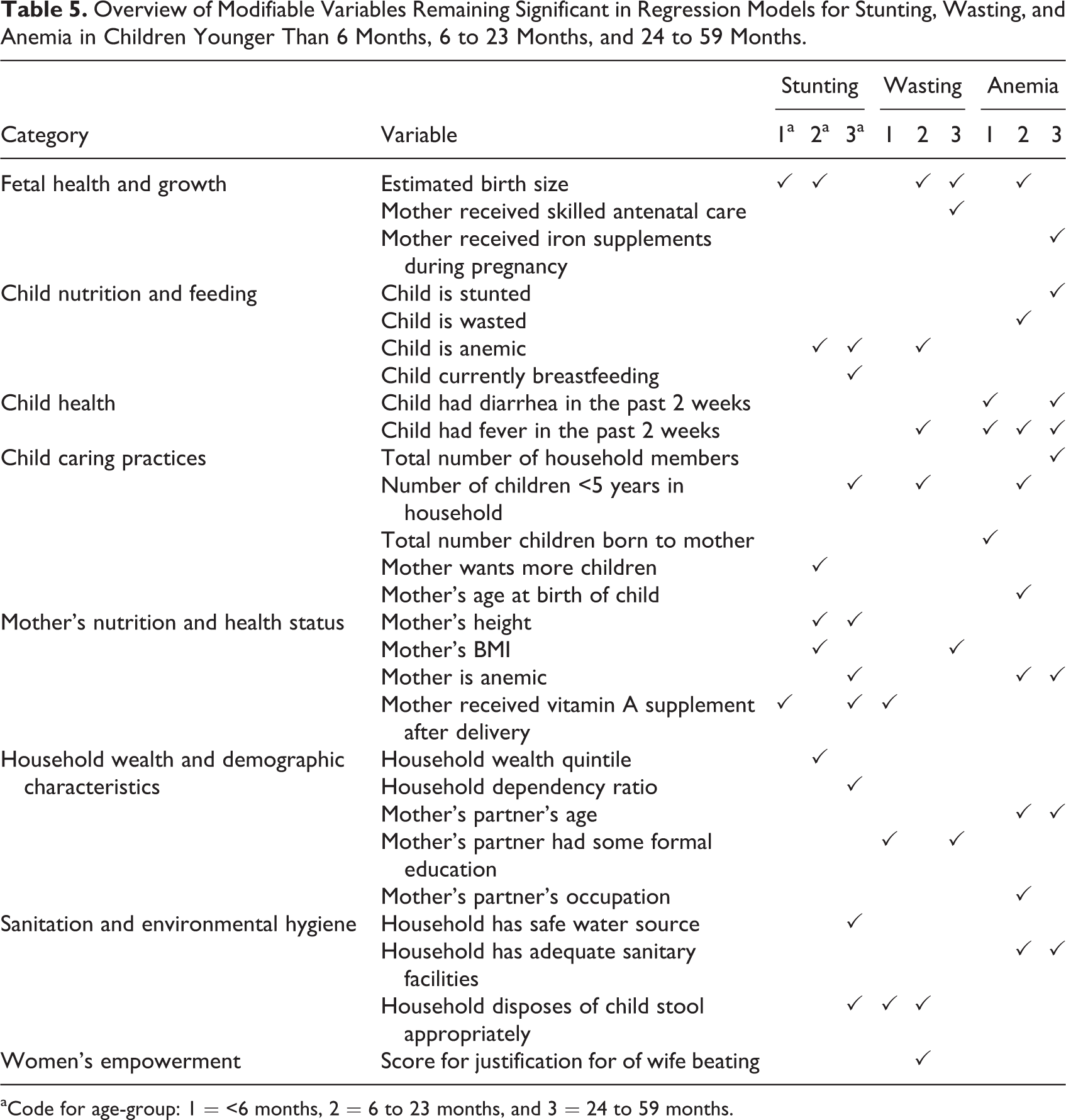
aCode for age-group: 1 = <6 months, 2 = 6 to 23 months, and 3 = 24 to 59 months.
Due to the impact of sanitation variables on stunting, wasting, and anemia found in this analysis, future investigations should explore the linkages between household sanitation and hygiene practices, enteropathy, and subsequent growth and anemia. Access to safe drinking water has been previously identified in multiple countries as a risk factor for stunting and wasting. 43 Because only about 65% of rural households had access to a safe drinking water source as of 2012, 5 considerable improvements can be made in Guinea. Interventions to promote and expand households’ use of improved sanitation facilities would also have a considerable impact on child health and nutrition status. According to the recent analysis conducted by Danaei et al, 37 unimproved sanitation was the second leading cause of stunting globally. While our analysis found that inappropriate disposal of child stool—and not unimproved sanitation—was related to stunting, these variables are interrelated in Guinea. According to standard recommendations, a child’s stool is considered “appropriately” disposed when (1) the child uses a toilet or latrine, (2) the stool is thrown away or rinsed in a toilet or latrine, and (3) the stool is buried. 44 Safe disposal is uncommon in Guinea because relatively few households had adequate sanitation facilities and burying a child’s stool was rarely practiced. 9
A comprehensive micronutrient survey in Guinea could also help identify additional determinants of anemia as well as other micronutrient deficiencies which may contribute to stunting and wasting. Other studies in West Africa have found that the determinants of anemia in children are variable and context-specific. 25,26 Multivariate analyses of data from Sierra Leone have shown that anemia in children was most affected by malaria and inflammation. 45 In Liberia, bivariate analyses have found anemia to be associated with iron deficiency, inflammation, malaria, recent fever, and unimproved household water source. 31
Conclusion
Our analysis found that the factors associated with child growth and anemia in Guinea varied considerably by age-group, and fewer risk factors were identified in children younger than 6 months compared to older children. Even among children aged 6 to 59 months, however, multivariate models explained a relatively small proportion of the malnutrition observed. In light of the limited explanatory power of our analyses, further efforts to explore the determinants of stunting, wasting, and anemia in Guinea are required. Future research should examine the associations between child malnutrition and indicators not collected as part of the DHS, such as household food security, dietary intake, micronutrient status, current or recent malaria, and exposure to environmental contaminants. Moreover, additional research is needed to identify the pathways associated with malnutrition in Guinea to guide programs which address stunting, wasting, and anemia. Nonetheless, the wide range of risk factors identified in this study shows that programs should encompass interventions at household, community, and institutional levels. Multisectoral foci should be on promotion of child caring practices, including family planning and household size; antenatal care and mother’s nutrition; water and sanitation interventions to reduce child diarrhea and to improve access to safe water; and others. Such interventions are likely to result in reductions in the prevalence of stunting, wasting, and anemia in Guinea.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was conducted as part of Contract No. 43188998 between UNICEF-Guinea and GroundWork.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.