
Abstract
Background:
In 2003, Taiwan’s iodine policy changed from mandatory to voluntary. The Nutrition and Health Survey in Taiwan (NAHSIT) 2001-2002 for schoolchildren showed adequate iodine nutrition, while NAHSIT 2005-2008 for adults showed the iodine status was at borderline adequacy.
Objective:
To investigate the iodine status of the Taiwanese population from schoolchildren to adulthood 10 years after the change of the salt iodization policy.
Method:
Urinary iodine was measured in samples from subjects in NAHSIT 2013.
Results:
The median urinary iodine concentration (UIC) of the Taiwanese population aged 6 years and above in 2013 was 96 μg/L, indicating mild iodine deficiency. The median UIC of 6- to 12-year-old schoolchildren was 124 μg/L (interquartile range [IQR]: 92-213 μg/L), and 115 μg/L (IQR: 80-166 μg/L), 125 μg/L (IQR: 74-161 μg/L), 73 μg/L (IQR: 52-131 μg/L), and 78 μg/L (IQR: 52-132 μg/L) in populations aged 13 to 18 years, 19 to 44 years, 45 to 64 years, and ≥65 years, respectively. Declining iodine nutrition in age groups ≥45 years old was noted that the median UIC of populations aged 45 to 64 years and ≥65 years was 99 and 88 μg/L, respectively, in NAHSIT 2005-2008. The median UIC of schoolchildren was not lower than that during the mandatory salt fortification period, but the distribution of urinary iodine levels signified a dietary pattern change.
Conclusion:
Wide-ranging variation in iodine nutrition levels was observed in different age groups. Universal salt iodization, as suggested by the World Health Organization, should be the best strategy to achieve adequate iodine nutrition.
Introduction
Iodine is an essential dietary nutrient required for the synthesis of thyroid hormones. Deficiency of iodine causes disorders (iodine deficiency disorders [IDDs]) such as goiter, intellectual impairment, growth retardation, neonatal hypothyroidism, cretinism, and increased risk of fetal and infant mortality. 1,2 In 1993, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) recommended universal salt iodization (USI) as the main strategy for eliminating IDD. 3 In 2016, based on surveys of school-age children, the total number of countries with adequate iodine nutrition was 102. 4 The great progress in iodine nutrition worldwide over the past 10 years is owed to the USI programs and the regular monitoring of urinary iodine. However, the iodine status of some countries has deteriorated from sufficient to deficient due to changes in iodine policies or other reasons such as replacement of iodophore disinfectants by noniodine-containing sanitizers in the dairy industry. 2 Sustaining the achievement of iodine adequacy is an important issue that requires ongoing monitoring to eliminate IDD. 5
In Taiwan, despite its island geography, endemic goiter was the fifth most common disease in the 1940s. 6 The implementation of island-wide salt iodization campaign with iodized salt of 33 ppm potassium iodate produced by the Bureau of Salt Administration in collaboration with the UNICEF was started in 1967. Four years after salt iodization, the goiter rates of schoolchildren had decreased from 21.6% to 4.3%, suggesting that the iodine status of the Taiwanese population had improved from moderate deficiency to adequacy by 1971. 7 However, the mandatory salt iodization policy was discontinued after Taiwan acceded to the World Trade Organization in 2002. There had been no nationwide iodine nutrition monitoring since the last goiter survey in 1971, and little was known about the iodine status in Taiwan during the previous 40 years. Recently, a retrospective study conducted by measuring the urinary iodine concentration (UIC) of samples collected from schoolchildren in the Nutrition and Health Survey in Taiwan (NAHSIT) 2001-2002 showed a median UIC of 123 μg/L, 8 inferring an adequate iodine status during the period of mandatory salt iodization in Taiwan. After changing from mandatory to voluntary salt iodization in 2003, an iodine nutrition survey of the adult population over 19 years old in NAHSIT 2005-2008 showed a median UIC of 100 μg/L, indicating that the iodine status was at borderline adequacy during the early transitional period. 9 To understand the long-term effects of the iodine policy changes and the iodine status of the Taiwanese population, we analyzed the UIC of the population of NAHSIT 2013 aged 6 years and older. The results were compared with the previous surveys of NAHSIT 2001-2002 (schoolchildren) and NAHSIT 2005-2008 (≥19 years) to evaluate the iodine status 10 years after the switch from mandatory to voluntary salt iodization.
Methods
Study Design
The study measured the UIC of samples from subjects in NAHSIT 2013 with age ≥6 years old. A total of 1185 samples were measured. The NAHSIT was funded by the Health Promotion Administration, Ministry of Health and Welfare, to produce extensive background data on health and nutrition in Taiwan, to understand the nutritional status of different age groups, and to investigate trends in nutrient and dietary intake among people in Taiwan. The data collection methods of NAHSIT had been published previously. 10 –12 In brief, a stratified 3-staged probability sampling design was used to obtain a representative sample of Taiwan. The 358 townships and city districts in Taiwan were divided into 5 sampling strata based on geographical location and population density (northern 1, northern 2, central, southern, and eastern strata). The NAHSIT 2013 was approved by the research ethics committee of the National Health Research Institutes, and informed consent was obtained from all adults who participated and from one of the parents of all schoolchildren and adolescents. The study of Urinary iodine analysis of the Nutrition and Health Survey in Taiwan (NAHSIT) 2010-2013 was approved by the institutional review board of Taipei Veterans General Hospital (Taipei, Republic of China).
Urine Sample Preparation
Overnight urine collected in a jar was aliquoted and clearly labeled. Then the urine samples were placed in the sample boxes and immediately stored in liquid nitrogen. The samples were transported to Taipei in a tank within 2 to 3 days and stored at −70°C in freezers located in the Academia Sinica, Taiwan, until analysis. 10,11
Urinary Iodine Assay
Urinary iodine concentrations were determined using the thermal cycler digestion method, as previously described. 13 Briefly, 25 μL of standard iodine solutions covering the range 0 to 400 μg/L iodine and urine samples were pipetted into a MicroAmp optical 96-well reaction plate, followed by addition of 50 μL/well of 1.35 M ammonium persulfate solution (freshly made; Sigma, St Louis, Missouri). 14 The reaction plate was covered with a 96-well full plate cover and digested in the GeneAmp PCR system 9700 Fast Thermal Cycler (Applied Biosystems, Foster City, California) at 95°C for 30 minutes and 4°C for 5 minutes. Aliquots of the resulting digestion were transferred to a 96-well reading plate (MicroWell; Nalge Nunc International, Naperville, Illinois) for the Sandell-Kolthoff reaction (S-K reaction). 15,16 The absorbance of the reaction mixture was read at 405 nm after the mixture had been sitting at room temperature (∼25°C) for 30 minutes. Samples with concentration >340 μg/L were diluted with water to fit the calibration curve, while samples <25 μg/L were measured using a low urinary iodine protocol (LIP). 13 For the LIP, volumes of the standard iodine solution covering the range 0 to 50 μg/L and samples were doubled (50 μL), while the volume of the ammonium persulfate, prepared at a higher concentration (2.5 M, heating to 50°C-60°C to facilitate dissolution), was halved (25 μL). The rest of the digestion and S-K reaction were the same as the standard protocol previously described. All samples were analyzed in duplicate in 2 separate assays, with measurement repeated for samples with discordant values exceeding 15%. The limits of detection were 6.0 and 1.5 μg/L of iodine by the standard protocol and the LIP, respectively. The intra- and interassay coefficients of variation (CVs) at iodine concentration >20 μg/L were both <10% by the standard protocol, and the intra- and interassay CVs of UICs in the range of 10 to 20 μg/L were <10% by the LIP. External quality control samples were provided by the Ensuring the Quality of Urinary Iodine Procedures program 3 times a year to ensure the accuracy of urinary iodine analyses.
Data Analysis
The samples were weighted to obtain representative estimates. Weight derivation was performed using the poststratification method based on the distribution of age and sex across areas as previously described. 11 The samples from the 5 geographical strata were divided into 2 gender and 5 age groups: schoolchildren (6-12 years), adolescents (13-18 years), young-age (19-44 years), middle-age (45-64 years), and seniors (≥65 years). The iodine status of the population was presented as median UIC of the sampled population. The cutoff points proposed for classifying iodine nutrition in the population ≥6 years (except pregnant and lactating women) based on median UIC by WHO/UNICEF/International Council for Control of Iodine Deficiency Disorders (ICCIDD) were as follows: <20 μg/L, severe iodine deficiency; 20 to 49 μg/L, moderate iodine deficiency; 50 to 99 μg/L, mild iodine deficiency; 100 to 199 μg/L, adequate iodine nutrition; 200 to 299 μg/L, above requirement; and ≥300 μg/L, excessive. For adequate iodine nutrition, no more than 50% and 20% of the population should have urinary iodine levels below 100 and 50 μg/L, respectively. 5
Statistical analyses were conducted using SAS 9.2 (SAS Institute, Cary, North Carolina). Differences in median UIC among age groups and areas of residence were compared using the Kruskal-Wallis test and multiple comparison test (Dunn test). The trend of changes in specific variables among age groups was analyzed using the chi-squared test for trend. Significance was taken as P < .05.
Results
Urinary Iodine Condition in NAHSIT 2013
As shown in Tables 1 and 2, the median UIC of Taiwanese population aged 6 years and above surveyed in NAHSIT 2013 was 96 μg/L (interquartile range [IQR]: 63-158 μg/L), suggesting mild iodine deficiency. Among the different age groups, the median UIC was lowest in middle-age (73 μg/L, IQR: 52-131 μg/L) and highest in young-age (125 μg/L, IQR: 74-161 μg/L). The median UIC of schoolchildren was 124 μg/L (IQR: 92-213 μg/L), which was significantly higher than those of the middle-age and seniors (both P < .05), lower than that of the young-age (P < .05), and not statistically different from that of adolescents. The median UIC of the population seemed to have a threshold at 45 years. For those age groups <45 years (schoolchildren, adolescence, and young-age), the median UIC was above 100 μg/L, while for age groups ≥45 years (middle-age and seniors), it was <80 μg/L.
Median Urinary Iodine Concentration in the Nutrition and Health Survey in Taiwan 2013 by Age, Gender, and Geographic Area.
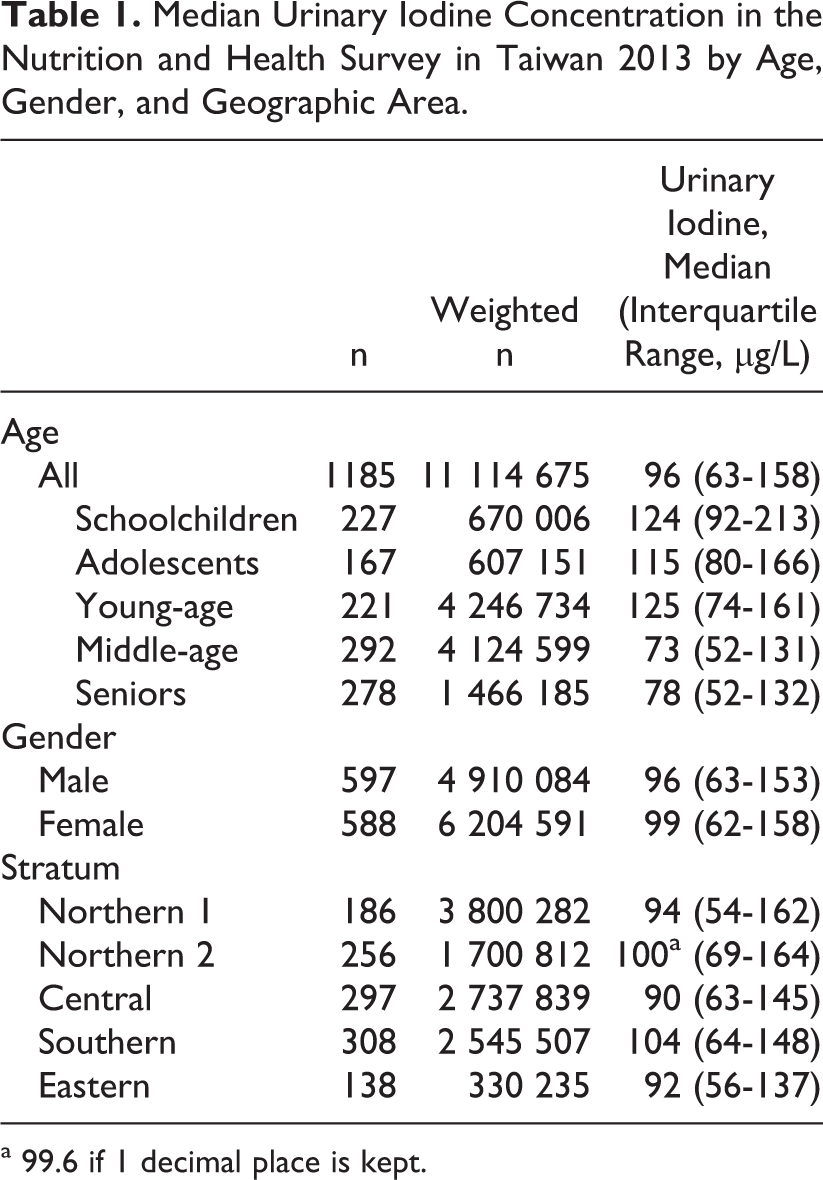
a 99.6 if 1 decimal place is kept.
Percentage of the Population of Different Age Groups with Low Urinary Iodine (<20, <50, and <100 μg/L) in the Nutrition and Health Survey in Taiwan 2013.
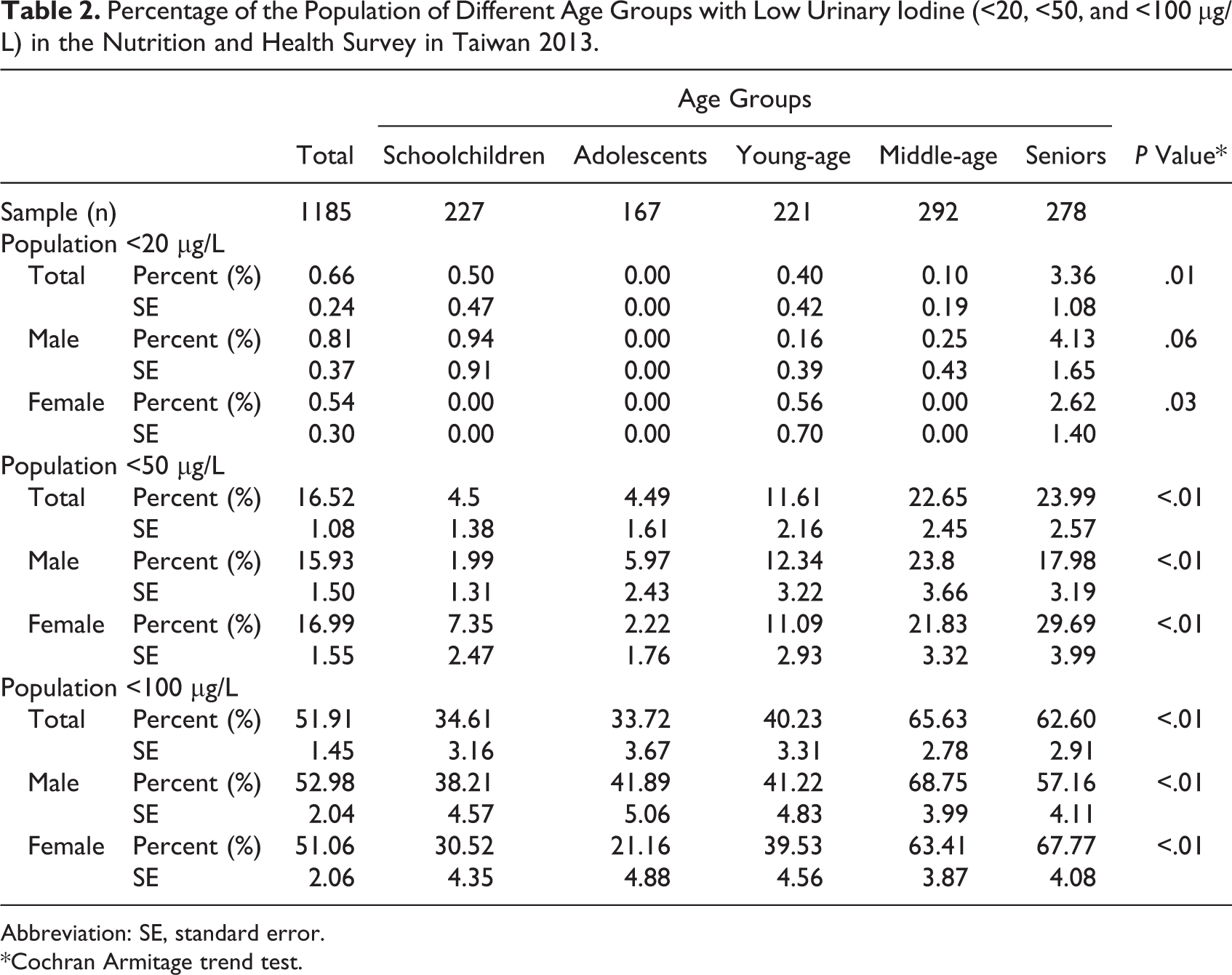
Abbreviation: SE, standard error.
*Cochran Armitage trend test.
The median UICs for all males and females were 96 μg/L (IQR: 63-153 μg/L) and 99 μg/L (IQR: 62-158 μg/L), respectively. There were no significant differences in median UIC between the sexes (P = 0.695). As shown in Figure 1, the median UIC was highest in young-age males (125 μg/L, IQR: 75-159 μg/L) and in adolescent females (155 μg/L, IQR: 106-212 μg/L). Both males and females showed the lowest median UIC in middle-age (76 μg/L, IQR: 51-130 μg/L and 71 μg/L, IQR: 52-131 μg/L, respectively). Of note, the median UIC in women of childbearing age (young-age females) was 124 μg/L (IQR: 74-177 μg/L).
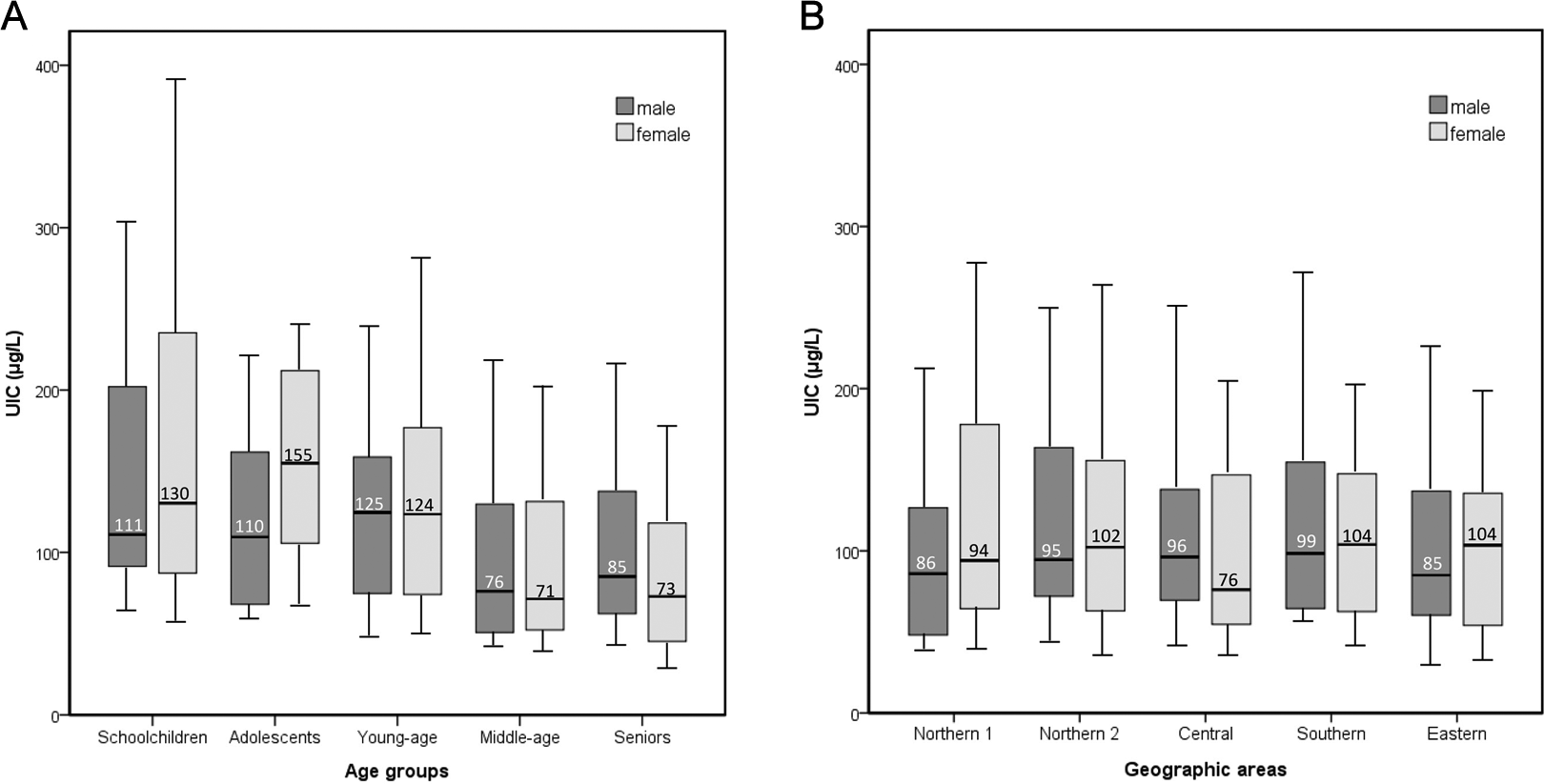
Box and whisker plot of the urinary iodine concentration data from the Nutrition and Health Survey in Taiwan 2013 by age group and geographic area. In each box, the central horizontal line marks the median value. The bottom and top of the box represent the 25th percentile and 75th percentile (interquartile range), respectively. The bottom and top of the whiskers signify the 10th percentile and 90th percentile, respectively.
As shown in Table 2, the percentages of the Taiwanese population 6 years and older with UIC <100, <50, and <20 μg/L were 51.91% ± 1.45%, 16.52% ± 1.08%, and 0.66% ± 0.24%, respectively. There was a tendency toward increasing percentage of population with lower UIC (<100, <50, and <20 μg/L) with increasing age. In middle-age and among seniors, the percentages of UIC <100 and 50 μg/L exceeded 60% and 20%, respectively. For the childbearing age group, the percentages of female with UIC <100 and 50 μg/L were 39.53% and 11.09%, respectively.
As shown in Table 1 and Figure 1, the median UICs of populations residing in the 5 strata ranged from 90 to 104 μg/L. The southern stratum had the highest median UIC and was the only stratum with median UIC >100 μg/L. The lowest median UIC was in the central stratum. The differences in median UICs among strata didn’t achieve statistical significance.
Comparison of Iodine Status of Different Iodine Fortification Periods
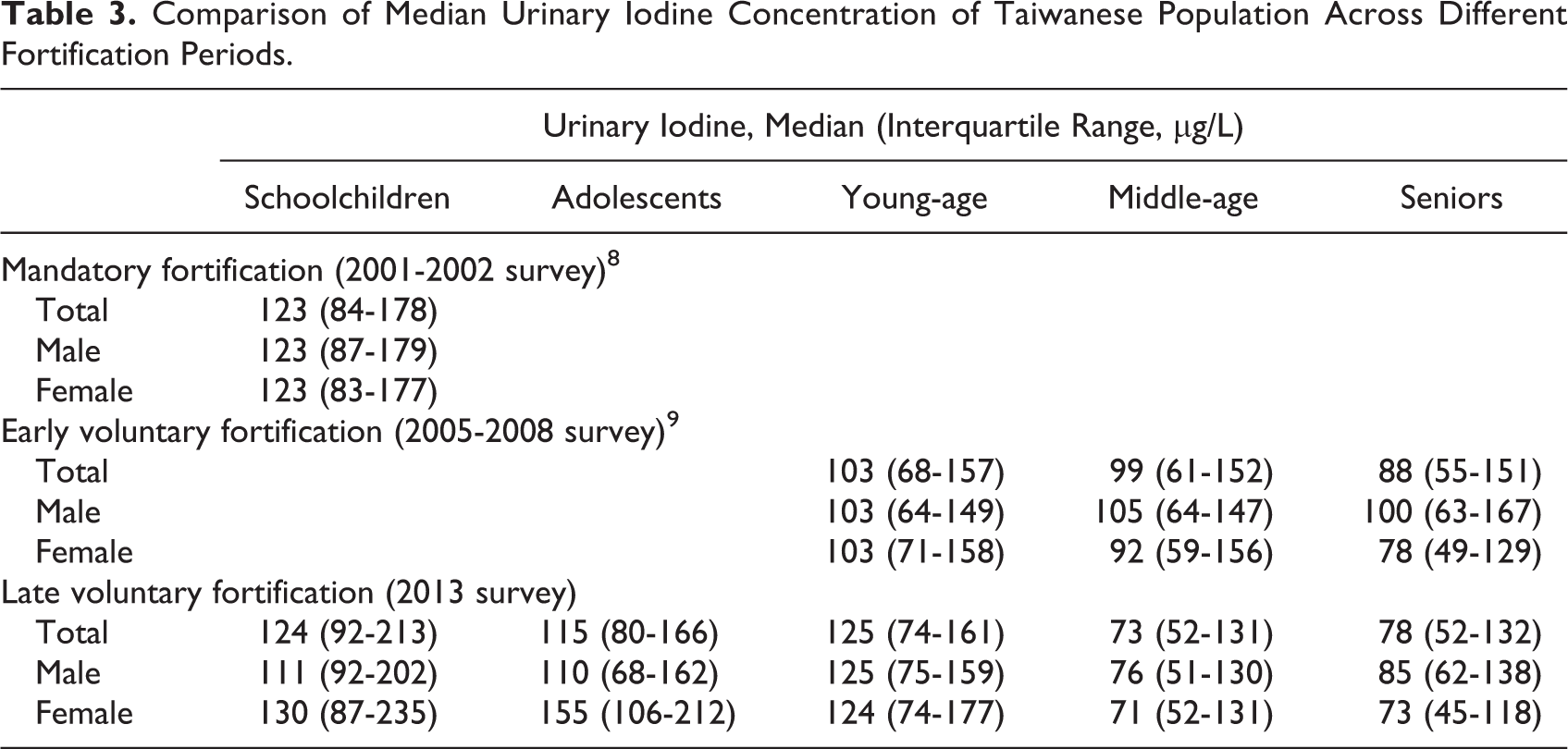
To demonstrate the effects of the mandatory and voluntary salt iodization on iodine nutrition in the Taiwanese population, we compared the UIC data obtained from 3 different iodine fortification periods (2001 survey as mandatory, 2005 as early voluntary, and 2013 as late voluntary iodine fortification) in the corresponding age groups. In general, the median UIC of Taiwanese population was decreasing from the mandatory to early and late voluntary iodine fortification periods (123, 100, and 96 μg/L). When comparing data between corresponding age groups (Table 3), the median UIC of schoolchildren was 123 μg/L in 2001 and 124 μg/L in 2013 (Figure 2A and B). The percentages of UIC <50 and 50 to 100 μg/L were similar in 2001 and 2013 (4.4% and 30.8% vs 4.5% and 30.1%, respectively). However, the proportion of population with UIC between 100 and 200 μg/L decreased from 45.9% in 2001 to 33.3% in 2013, while there was an increase from 6.7% to 14.7% in the population with UIC >300 μg/L.
Comparison of Median Urinary Iodine Concentration of Taiwanese Population Across Different Fortification Periods.

A, Comparison of the median UIC and (B) distribution of UIC in schoolchildren in the NAHSIT 2001-2002 () and 2013 ( ). C, Comparison of the median UIC and (D) distribution of UIC in young-age in the NAHSIT 2005-2008 (
). C, Comparison of the median UIC and (D) distribution of UIC in young-age in the NAHSIT 2005-2008 ( ) and 2013 (). E, Comparison of the median UIC and (F) distribution of UIC in middle-age in the NAHSIT 2005-2008 () and 2013 (). G, Comparison of the median UIC and (H) distribution of UIC in seniors in the NAHSIT 2005-2008 () and 2013 (). NAHSIT indicates Nutrition and Health Survey in Taiwan; UIC, urinary iodine concentration.
) and 2013 (). E, Comparison of the median UIC and (F) distribution of UIC in middle-age in the NAHSIT 2005-2008 () and 2013 (). G, Comparison of the median UIC and (H) distribution of UIC in seniors in the NAHSIT 2005-2008 () and 2013 (). NAHSIT indicates Nutrition and Health Survey in Taiwan; UIC, urinary iodine concentration.
The median UIC of adults aged ≥19 years decreased from 100 μg/L in the early voluntary period (2005) to 91 μg/L in the late voluntary period (2013). However, the median UIC of young-age increased from 103 μg/L in 2005 (UIC <100 μg/L of 47.7%) to 125 μg/L in 2013 (UIC <100 μg/L of 40.2%; Figure 2C and D). Similar to the young-age of both sexes, the median UIC of women of childbearing age (young-age females) increased from 103 μg/L (UIC <150 μg/L was 71.5%, <100 μg/L was 46.5%) in 2005 to 124 μg/L (UIC <150 μg/L was 63.6%, <100 μg/L was 39.5%) in 2013, whereas the proportion of UIC >300 μg/L decreased from 10.8% in 2005 to 5.2% in 2013. The median UICs of the middle-age and seniors groups were substantially lower in 2013 than in 2005 (73 and 78 μg/L vs 99 and 88 μg/L, respectively; Figure 2E and G), and the percentages of UIC below 100 μg/L increased from 51.2% and 57.6% in 2005 to 65.6% and 62.6% in 2013, respectively (Figure 2F and H).
Discussion
In the 1940s, Taiwan was an iodine-deficient area, and the mandatory salt iodization program implemented since 1967 had effectively corrected the iodine deficiency. However, the rules were relaxed and the salt iodization strategy could not be sustained. The government-run salt company was privatized in 2003, and Taiwan’s salt market was liberalized. Salt imported to Taiwan increased from 9904 tons in 2005 to 10-fold of 111 225 tons in 2013. 17 In a 2012 survey of salt products sold in the market, of the 24 blends of regular/plain salt, only 8 were iodized. 18 Six blends of iodized salt were products of Taiwan, with fortification levels of 14 to 20 ppm. The 2 imported iodized salt products were from the United States and Thailand, with fortification levels of 45 and 3 ppm, respectively. The 13 blends of imported noniodized salt products were from 10 countries. 18 Labeling information regarding iodization is not displayed in most of the salt products. Although the proportion of households using iodized salt was not available, the increasing number of noniodized salts emerging in the market is believed to have affected the iodine intake in Taiwan. The present study measured the urinary iodine levels in samples from subjects in NAHSIT 2013, and the median UIC of the Taiwanese population aged 6 years and above was 96 μg/L, indicating a status of mild iodine deficiency. A similar pattern of reemergence of iodine deficiency also appeared in Vietnam, where the USI program was downgraded from mandatory to voluntary in 2005, and the iodine status in schoolchildren declined as a result. 19
Variations in UIC among different age groups were observed in this survey. The median UICs of age groups <45 years including schoolchildren, adolescents, and young-age were >100 μg/L, which were higher than those of middle-age and seniors, in whom the median UICs were in the category of mild iodine deficiency. This finding was consistent with previous observations reported from Switzerland, and also with NAHSIT 2005-2008, in that older people had a lower UIC than schoolchildren or young age. 9,20 When compared with the previous data of middle-age and seniors in 2005, further decrement of the iodine nutrition in 2013 was observed, particularly in women. The reasons for poor iodine nutrition in the elderly are unknown but may be related to dietary variations, physiological requirements, salt iodization policy changes, and low-sodium diet for the prevention of cardiovascular diseases. The mean salt intake in middle-age males and females decreased from 11.2 and 7.7 g/d in 2005 to 8.0 and 6.9 g/d in 2013, respectively. 12 It appears that the most possible contributing factors for iodine deficiency in the elderly people were the impact of voluntary salt iodization as well as the reduction in dietary salt intake. Close monitoring of changes in iodine nutrition, as well as coordinating the reduction in sodium consumption and the maintenance of adequate iodine intake by resuming the USI strategy, should be essential for the Taiwanese population.
When compared with the previously available data, the median UIC of schoolchildren in 2013 was similar to the results of 2001 survey during the mandatory fortification period (124 vs 123 μg/L). However, further analysis showed that the distribution of the UICs plotted from the data of these 2 studies was quite different. When compared with the results of 2001, the percentage of population with UIC >300 μg/L was 2-fold in 2013, but those with UIC between 100 and 200 μg/L was less in 2013. From the iodine concentration analysis of salt products as mentioned above, 18 it is reasonable to speculate that an UIC greater than 300 μg/L might represent a recent iodine intake from iodine containing food in addition to salt. Therefore, these results implied a dietary pattern change of increased intake of food rich in iodine in schoolchildren in 2013. Another possible explanation for sustaining iodine adequacy in schoolchildren after voluntary salt iodization is the promotion of iodized salt in school lunches. 21 Therefore, the iodine condition in schoolchildren might not accurately reflect the impact of the iodine policy change in Taiwan. Historically, most surveys assessing the iodine status of populations targeted schoolchildren. However, discrepancies of median UIC between schoolchildren and other age groups were observed. 20,22 Urinary iodine data should be collected in the respective target groups instead of using schoolchildren as proxy for the entire population.
In the present study, the median UIC was higher in females than males among schoolchildren and adolescents, lower in middle-aged adults and seniors, and similar between both sexes in young adults. The pattern of UIC between sexes in adults was consistent with observations in the 2005 survey. 9 However, the median UICs of both male and female schoolchildren were 123 μg/L in 2001. 8 This implies that the median UIC of male schoolchildren had declined by 2013, although it is still in the range of adequacy. There are no previous data for comparison of the urinary iodine condition in adolescents, while the median UIC of 110 μg/L in male adolescents is similar to that in male schoolchildren (111 μg/L). The reason for the decrease in UIC of male schoolchildren is not clear. Further monitoring of iodine status change and dietary assessment are necessary to explain this issue.
The median UIC in young adults was higher in 2013 (125 μg/L) than in 2005 (103 μg/L). The distribution showed the proportion of populations with an UIC <100 μg/L decreased from 47.7% in 2005 to 40.2% in 2013, and the proportion of populations with an UIC between 100 and 200 μg/L increased from 37.2% in 2005 to 44.5% in 2013, respectively. The reason for this change is unknown; however, an increased population with higher education (university level) in 2013 was noted. 12 Since NAHSIT did not enroll pregnant women, assessing the median UIC in women of childbearing age may provide helpful information regarding the iodine status in early gestation. The median UIC of young-age females (124 μg/L) appeared to be sufficient for the age, but it was inadequate for pregnant women (150-249 μg/L). Thyroid hormones are essential for normal neurodevelopment of the fetus and neonates, so pregnant and lactating women and their offspring are considered to be the subgroups most vulnerable to iodine deficiency. The majority of studies evaluating the dietary changes before and during pregnancy in women report an increase in energy intake, but the dietary component changes vary. 23 Pregnant women require more iodine intake for the increased production of thyroid hormone, increased renal clearance of iodine, and the supply of iodine for the fetus. The fetus relies upon maternal iodine for thyroid hormone synthesis before the maturation of the fetal thyroid, and even mild iodine deficiency during pregnancy may cause irreversible decrease of cognitive function in children. 24 Furthermore, data from Taiwan’s newborn screening program showed that the detection rates of neonatal hypothyroidism were 0.06% to 0.08% in 1999 to 2003, 0.08% to 0.11% in 2004 to 2008, and 0.08% to 0.14% in 2009 to 2013, respectively. 25 The relationship between the changes of iodine policy and the incidence of neonatal hypothyroidism is unknown. The synchronicity between the increased neonatal hypothyroidism and the policy changes requires special attention. Up to 2016, recent surveys in pregnant women have been available from 65 countries worldwide. The iodine status of pregnant women was sufficient in 23 countries and insufficient in 37 countries. 4 Iodine nutrition surveys should be carried out in pregnant, breastfeeding women, and neonates in future surveys in Taiwan, and prenatal iodine nutrition education and iodine supplementation may be helpful to prevent pregnant women from iodine deficiency. 26 –28
Current analysis has shown geographic differences in urinary iodine, with the southern stratum being the only region with adequate iodine nutrition, which is consistent with the results of the 2005 survey. 9 However, all the geographic strata in Taiwan were iodine sufficient during the mandatory fortification period. 8 Historically, the southern area was the only nonendemic regions (goiter rate <5%) in Taiwan in 1965, before the introduction of salt iodization, 29 and that was considered to be related to the plain terrain in this region. This implies that the USI campaign had corrected the geographic cause of the previous iodine deficiency, and the change in iodine policy might lead to the reemergence of geographic difference in iodine nutrition in Taiwan.
Conclusion
The mandatory salt iodization program in Taiwan was first launched in 1976 and successfully reduced the prevalence of goiter in schoolchildren from a level of moderate iodine insufficiency to normal. However, the mandatory salt iodization program could not be upheld because of the change in salt policy. In 2013, the median UIC of the Taiwanese population was mildly iodine insufficient. When comparing with previous surveys, the median UIC of the middle-age and senior populations declined. A wide range of variation in iodine nutrition levels was observed in the different age groups. In June 2017, the Taiwan Food and Drug Administration modified Standards for Specification, Scope, Application, and Limitation of Food Additives to raise iodine content in salt fortified with potassium iodide or potassium iodate to 20-33 mg/kg. 30 Besides, the Ministry of Health and Welfare will mandate labeling of iodine content on dietary salt should it exist. As suggested by WHO, Iodine Global Network, and UNICEF, USI should be the best strategy to sustain iodine sufficiency. 31 Large systemic studies of iodine status of pregnant women, lactating women, and neonates should be conducted, and the monitoring of urinary iodine should be continued in Taiwan.
Footnotes
Acknowledgments
The authors would like to thank Ya-Fen Lo (Department of Medical Research and Education, Taipei Veterans General Hospital, Taipei, Taiwan) for her assistance in laboratory analysis, and Shu-Yi Lin (Center for Public Health, Department of Education and Research, Taipei City Hospital, Taipei, Taiwan) and Wen-Ting Yeh (Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan) for their assistance in statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project of Urinary iodine analysis of Nutrition and Health Survey in Taiwan 2010-2013 was sponsored by the Health Promotion Administration, Ministry of Health and Welfare in Taiwan (B1021019).