
Abstract
Background:
Moringa oleifera leaf powder (MLP) is a nutrient-rich and readily available food resource that has the potential to improve the micronutrient quality of complementary foods in developing countries.
Objective:
To investigate the acceptability of complementary foods fortified with MLP.
Methods:
Moringa oleifera leaf powder was fed to infants either as part of a cereal–legume complementary food blend (MCL-35 g) or by sprinkling as a food supplement (MS-5 g) on infant’s usual foods. Mother–infant pairs (n = 18 for the MCL-35 g group and n = 16 for the MS-5 g group) attending regular weight monitoring sessions were recruited to participate in the acceptability trial. The study consisted of an initial tasting session after which mothers were to feed the assigned foods to their infants for 14 days. Mothers rated color, odor, taste, and overall liking of the complementary foods using a 5-point hedonic scale. Primary outcome was the proportion of test porridge consumed.
Conclusion:
We conclude that complementary foods incorporating Moringa oleifera leaf powder either as part of a cereal–legume complementary food blend (MCL-35 g) or when sprinkled as a food supplement (MS-5 g) on infant’s usual foods were well accepted.
Introduction
Malnutrition in infancy has been associated with an array of factors including prelacteal feeding, shorter duration of exclusive breastfeeding, early weaning, mixed feeding, limited dietary diversity, low socioeconomic status, short birth interval, poor sanitation, and a weak health system. 1
Infants aged 6 to 24 months in developing countries are a nutritionally vulnerable population because of their relatively high energy and nutrients needs that are often not met in traditional complementary foods. This period of growth is further threatened by poor infant and young child feeding practices and repeated episodes of infection and complementary foods of poor nutrient quality. 2 The World Health Organization report on “Health in 2015” indicated that while new resources have been mobilized to address stunting in high-burden countries, the other forms of malnutrition, including micronutrient deficiencies, have received little attention. 3 In Ghana, for example, 66% of children under 5 suffer from varying degrees of anemia. 4
Several interventions have been considered in addressing micronutrient malnutrition; these include supplementation and fortification programs. Bhutta et al reported in their review that deaths in children younger than 5 years can be reduced by 15% if populations (in the 34 focus countries, Ghana included) can access 10 evidence-based nutrition interventions, scaled up to 90% coverage, the cost of which is estimated at Int $9.6 billion annually. 5
Interventions using a traditional food-based, comprehensive approach may be more effective and sustainable than programs targeting individual nutrient deficiencies. 6
Moringa oleifera, an edible plant found abundantly in the dry tropics, is known to be a rich source of micronutrients. Available data suggest that the leaves contain highly digestible proteins and are also rich in iron, calcium, vitamin C, and carotenoids. 7 It is an indigenous plant that grows all year round and has been used for the treatment of micronutrient deficiencies among children in Malawi and Tanzania. 7,8 Moringa oleifera leaf powder (MLP) has also been added to a local maize porridge in Nigeria, resulting in significant improvement in iron status, serum ferritin, and serum retinol of infants aged 6 to 12 months. 9 Fortifying the diets of rural households with M oleifera leaves could serve as a less expensive way of improving their nutritional status because the leaves could be cheaply dried with solar dryers and stored for use in rural households. 10 Moringa oleifera leaf powder thus has the potential for use as a complementary food supplement. Complementary food supplements are fortified food-based products that can be added to other foods (as “point of use” or “home” fortificants) or eaten alone to improve both micronutrient and macronutrient intake. 11 Dewey et al 2 have reported that home fortification of complementary foods also referred to as “point-of-use” fortification is a promising strategy that is able to deliver the appropriate amount nutrients for children aged 6 to 24 months without making major alterations to their diet.
Babu 7 however has emphasized the crucial role of food acceptance in determining the success of food and nutrition intervention programs. This was reiterated by Glover-Amengor et al 10 who reported that consumer acceptability of fortified dishes is key in the whole fortification process. There is an increasing interest in the use of M oleifera leaves to improve complementary foods. 12 –14 This interest notwithstanding, the unique sensory characteristics (color, taste, and odor) of MLP 15 call for an investigation of its acceptability when incorporated in infants’ complementary foods. Few studies, which have investigated the acceptability of complementary foods incorporating MLP, have employed 1-time sensory or organoleptic evaluations. 12 –14 This is however not an adequate test of acceptability, given the unique sensory characteristics of MLP. Furthermore, in these studies, although the formulated complementary foods were intended for infants and young children, the panels that took part in the sensory evaluation were adults. 12 –14
For a nutrition intervention to be successful, most consumers in the target populations (in this case, infants and young children) must accept and consume the food commodities in quantities sufficient to improve their nutritional health, 16 and this applies as well to interventions using MLP. There is a need for well-designed acceptability trials, involving mother–infant pairs that last for extended periods in order to ascertain acceptability of complementary foods that incorporate MLP.
Thus, in this study, an acceptability trial of complementary foods that were fortified with MLP was investigated. Two different approaches were employed in fortifying the complementary foods with MLP. In the first approach, MLP was used to fortify a cereal–legume blend (named MCL-35 g) in the following ratio—maize 60%, soybean 25%, and MLP 15%. In the second approach, MLP was aseptically produced and packaged (named MS-5 g) to be sprinkled on infants’ usual complementary foods. The objective of this study was to determine the acceptability of MCL-35 g and MS-5 g among Ghanaian infants. This was a necessary step ahead of conducting an efficacy trial with the 2 products.
Methods
Sample Preparation and Packaging
The preparation and packaging of both MCL-35 g and MS-5 g were carried out at the Nutrition Unit of the Food Research Institute of the Centre for Scientific and Industrial Research, Ghana.
MCL-35 g (maize 60%, soybean 25%, and MLP 15%) was formulated based on the cereal–legume ratios used for the preparation of Weanimix, 17 with some of the ingredients being partly substituted with 15% of MLP as a fortificant. MCL-35 g was packaged in 35 g sachets, with each sachet containing 5 g of MLP. The energy, protein, iron, and vitamin A composition of MCL-35 g and MS-5 g are reported in Table 1.
Energy, Protein, Iron, and Vitamin A Composition of MCL-35 g and MS-5 g.
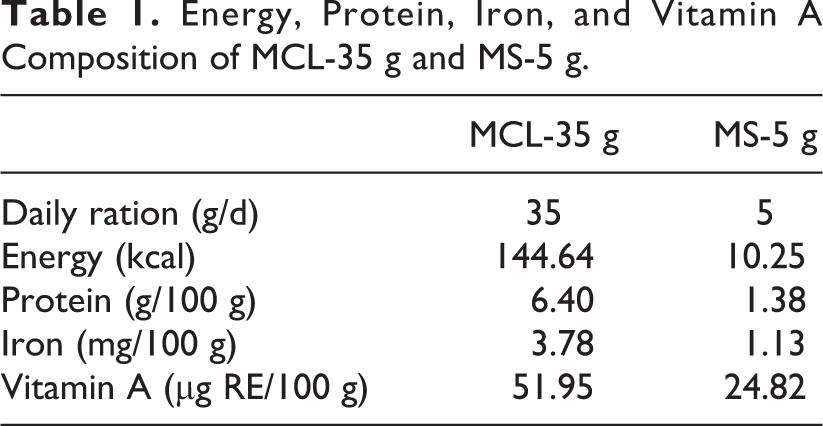
MS-5 g (MLP) was used as a micronutrient-rich powder that was sprinkled on infants’ usual foods. MS-5 g was packaged in 5 g sachets.
The 5 g daily supply of MLP would add 1.13 mg of iron and 24.8 µg/Retinol Equivalents of vitamin A to infants’ complementary diets. These levels translate into 10% and 7%, respectively, of the recommended nutrient intakes for iron and vitamin A for infants aged 6 to 23 months. 18 The 5 g daily dose of MLP incorporated in infants’ complementary foods was chosen due to concerns about acceptability of foods that are fortified with higher levels of MLP. 19
Study Area
The study was conducted from October to November 2014 at the University of Ghana, Nutrition Research and Training Centre (UG-NRTC) located at Asesewa in the Upper Manya Krobo District of the eastern region of Ghana. The eastern region registered the highest rates of stunting and anemia among infants and young children in the demographic and health survey. 20
Study Population and Sample Size
Healthy infants attending routine growth monitoring sessions at the Asesewa Child Welfare Clinic (CWC) were recruited to participate in the study. Inclusion criteria were infants aged 8 to 12 months, currently receiving breast milk, should have consumed complementary foods for at least 30 days, and mother/caregivers willing to report to the UG-NRTC (located nearby the Asesewa CWC) for 2 consecutive days. Infants were excluded if there were any known intolerances to any of the ingredients of the study foods, were ill requiring referral to hospital, or if their mothers/caregivers could not report to the UG-NRTC on the 2 consecutive days designated. Sample size was calculated based on the desire to test the hypothesis that mean consumption in the first part of the trial would be at least 60% of the amount offered. Standard deviation of consumption was assumed to be 20% of the amount offered. Thus, a sample size of 16 would be adequate to reject the null hypothesis with 80% power if the true mean was at least 75%. Assuming 15% attrition, at least 18 infants were required per group.
Study Procedures
The study was carried out as a 2-part acceptability trial for both MCL-35 g and MS-5 g. The first part of the study was a test feeding session where study participants were required to taste either a porridge that was made from MCL-35 g, or koko (a fermented maize porridge commonly fed to infants in Ghana), to which MLP (MS-5 g) had been added. In part 2 of the study, all study participants received a 2-week supply of either MCL-35 g or MS-5 g which they were to use in their homes for 14 days under real-life conditions.
The primary outcome of the study was the amount of food (MCL-35 g or MS-5 g) consumed by infants, whereas the secondary outcome was mothers/caregivers’ opinions of the color, odor, taste, and overall acceptability of the 2 products after using them under home conditions for 2 weeks.
Recruitment
On the recruitment day, nurses at the Asesewa CWC with the assistance of a trained field worker referred every infant aged 8 to 12 months to the study enrollment team. The enrollment team then verified the age of the infants from their child health cards as well as the other inclusion criteria. Details of the study were explained to mothers of infants who met all inclusion criteria before they were invited to participate. After consent was obtained, trained field workers completed a screening questionnaire to determine whether a potential participant had to be excluded because of illness or intolerance to any of the ingredients. Patients who remained eligible after the screening were randomized (by simple randomization) to receive either MCL-35 g or MS-5 g and given a specific day, depending on the study food to be received, to report to the NRTC to begin the trial. For mothers/caregivers’ who had phones, phone numbers were obtained and verified for the purpose of placing reminder calls. Trained field workers further accompanied mothers/caregivers of all recruited infants to their homes in order to be able to locate them during the second part of the trial.
Part 1—The test feeding trial
MCL-35 g
Mothers brought their infants to the UG-NRTC each morning for 2 consecutive days. Their time of arrival at the feeding center was recorded each day after which a questionnaire was used to obtain information about infants’ most recent food intake (including breast milk) and morbidity during the past 24 hours. The feeding session on the first day was to enable the study team to get familiarized with the mothers and children and for mothers and children also to get familiarized with the food and the procedures, thus data recorded on the first day were not included in the analyses. Study staff ensured that infants were offered the test meal at least 1 hour after they were last fed. If an infant had recently been fed any food/drink or breast milk at the time of arrival, mothers were first asked to estimate the time of the last feeding episode and required to wait until approximately 1 hour after the last feeding episode, after which period infants were offered the test meal. No infant was breastfed during the test feeding trial.
Trained field workers prepared porridge from MCL-35 g each morning at the study kitchen of the UG-NRTC as follows: about 100 g of MCL-35 g flour was weighed and mixed with about 200 ml of water. The slurry was brought to boil for about 10 minutes with continuous stirring. Additional 460 mL of water was added to obtain the desired consistency. Eighteen grams of sugar was added to taste.
Mothers were invited to observe the preparation of the porridge after which each of them was served about 10 g of porridge in a small plastic bowl to taste. Each infant was then served 50 g of the porridge. Mothers were instructed to spoon feed their children the porridge until the child refused to eat. Children were considered as refusing intake if they moved their head away from the food, cried, clamped the mouth shut or clenched the teeth, became agitated, spat out the food, or refused to swallow. The emotional state of the infant during the feeding was also recorded.
The weight of the test meal consumed within 15 minutes, or up to the time the child stopped eating and at least twice refused the mother’s attempt to refeed, was calculated by subtracting the left-over food from the offered amount. The duration of the feeding (excluding the intervening “pause periods”) was recorded by stopwatch. Each feeding episode took place under the direct supervision of a trained field worker to ensure that feeding was not forceful. Using a 5-point hedonic scale (1 = dislike a lot, 2 = dislike a little, 3 = neither like nor dislike, 4 = like a little, 5 = like a lot) in which each point was depicted by a facial drawing, mothers were asked to rate the food’s color, odor, taste, and overall liking.
MS-5 g
Mothers brought their infants to the UG-NRTC each morning for 2 consecutive days. Their time of arrival at the feeding center was recorded each day after which a questionnaire was used to obtain information about infants’ most recent food intake (including breast milk) and morbidity during the past 24 hours. Each mother was served 60 g of freshly prepared koko (a fermented maize porridge sweetened with sugar) and taught by a trained field worker to thoroughly mix 2 g of MS-5 g with the porridge while it was still very hot. Mothers were instructed to first taste 2 teaspoons of the porridge (about 10 g) and feed the remaining 50 g to their infants. The rest of the test feeding proceeded similarly as described for MCL-35 g. On the actual trial day (day 2) for both MCL-35 g and MS-5 g, we collected data on morbidity just as we did for the first day. There were no reports of illness or any adverse reaction attributed or perceived by the mother to MCL-35 g or MS-5 g on the second day.
Part 2—Home use of MCL-35 g and MS-5 g under real-life conditions for 14 days
MCL-35 g
After the first part of the trial, all participants were supplied with the respective study foods (MCL-35 g and MS-5 g) for use at home under real-life conditions for 14 days. With MCL-35 g, each infant was expected to consume a daily dose of 35 g of the complementary food flour. Each mother was given 14 sachets each of MCL-35 g, placed in a clean transparent plastic container with a firmly closing lid to be fed to the infant for the 14-day period. Two extra sachets were added just in case other individuals within or outside the home wanted to taste the food. Mothers were given small plastic bowls with spoons to feed their infants and a cake of soap to wash their hands before preparation of the foods. Mothers were taught how to prepare porridge from the MCL-35 g flour as well as how to use the flour to prepare other local dishes such as “banku/akple,” “aprapransa,” and “kakro.” Trained field workers demonstrated the preparation of the recipes. Each mother was instructed to continue breastfeeding as well as the feeding of other complementary foods aside the study foods.
During the first 7 days of the 14-day trial, each mother/infant pair was visited daily by a field worker for the purpose of monitoring how foods were prepared, how much food the infants had eaten and to obtain mother’s feedback on their experiences with the use of the study food as well as monitor infant morbidity using a questionnaire. Mothers were instructed to feed study food 2 to 3 times a day and also to feed much earlier in the day. Daily visits took place between 4 and 6
To help quantify how much of the study food each infant had eaten, mothers were instructed to store any leftover cooked food that infants could not consume for each day as well as any uncooked MCL-35 g. If an infant could not eat all the food in 1 sachet in the day, mothers were to store the left over flour and use a fresh/new sachet the following day. Field workers weighed the leftovers from both cooked foods and sachets and collected morbidity data (diarrhea, vomiting, symptoms of respiratory infections, and fever) during the daily visits using a questionnaire. With the knowledge of how much porridge as well as “banku/akple,” “aprapransa,” and “kakro” that 35 g of MCL-35 g would yield, an estimate of the total amount of MCL-35 g leftover foods weighed was calculated, and the results obtained were used to determine how much of the flour had been eaten by each infant per day.
During the second week, mothers were not visited every day. They were instructed to feed their children as they did in the previous week and use the feeding bowls they were given to estimate leftover cooked food (if any) for each day. On the 14th day, field workers visited mothers for the exit interview. Mothers were asked open-ended questions about what foods they commonly prepared MCL-35 g with, the number of times they typically fed the food every day, their reactions to the food and whether or not they were willing to use the food in the future if available. To quantify intake over the period, field workers weighed leftover MCL-35 g flour in the remaining 7 sachets, and mothers also estimated by recall, any leftovers of cooked study foods fed to infants. Data on morbidity during the period were also collected by recall.
MS-5 g
For the second part of the trial for the MS-5 g group, the supplement was provided in 5 g daily dose sachets, which was to be added to their usual complementary foods each day. Specifically, one-third to half of a sachet was to be added to each of 2 to 3 meals daily. To ensure that infants ate all the supplements fed, the supplement was to be added to half of the food a child usually consumed at a time and fed first after which the rest of the food was to be fed. Each infant was given 16 sachets (although they were expected to consume 14), for the same reason as for the MCL-35 g in the 14-day home use aspect of the trial. The MS-5 g sachets that were to be used on a daily basis (one 5 g sachet per day) were also packaged in clean transparent plastic container with a firmly closing lid. If an infant could not eat all the supplement in 1 sachet in the day, mothers were to use a fresh/new sachet the following day and not use the leftover from the previous day. Mothers were instructed to add the supplements to foods while they were still very hot, that is, freshly dished portions of infants’ usual foods. Each mother/infant pair was paid a daily visit during the first 7 days of the trial by a field worker. The purpose of the visit was to monitor how the supplement was being used, to obtain mothers’ feedback on their experiences with the use of the supplement and to record infant morbidity. Field workers also weighed any leftover supplement for the day to estimate the infant’s intake. Morbidity data (diarrhea, vomiting, symptoms of respiratory infections, and fever) were also collected during the daily visits. Leftover cooked foods to which MS-5 g supplement was added were however not weighed, as it would have been difficult to accurately estimate how much supplement it contained. Thus, for the 14-day home use of MS-5 g, daily amounts eaten were estimated from left overs in the sachets alone. Mothers were provided with plastic bowls with spoons to feed their infants, and a cake of soap to wash their hands before preparation of the foods. The rest of the MS-5 g part 2 trial proceeded similarly as described for MCL-35 g.
Data Analyses
Data analyses were performed using SPSS version 20 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY, IBM Corp.). Background characteristics of the participants were summarized using descriptive statistics. For the test feeding sessions, the mean percentage of the test food that children consumed was calculated. The median (minimum, maximum) proportion of the weight of study food consumed per day during the 14-day period was calculated, as these intakes were not normally distributed. For each study group, median proportion of intake for the first 7 days was compared to that for days 8 to 14, using the Wilcoxon-signed rank test. Mann-Whitney U test was used to compare the median proportion of intake between the 2 study groups, over the 14-day period. Data from the sensory evaluation were presented as median (minimum, maximum), and the data on different practices and beliefs mothers adopted by mothers at the exit interview at the end of the 2-week home-use period were also summarized.
Ethical Approval
The study protocol was approved by the institutional review board of the Noguchi Memorial Institute for Medical Research, University of Ghana, and the Ghana Health Service Ethical Review Committee. Permission to use the formulated foods was obtained from the Food and Drugs Authority in Ghana. Written permission to carry out the study in the Upper Manya Krobo District was obtained from the District Health Administration of the Ghana Health Service (GHS), and informed consent was sought and obtained from the parents/caregivers of each infant using a written form (translated into Krobo, the native language of the study area) that described the study and consent process.
Results
Sample Characteristics
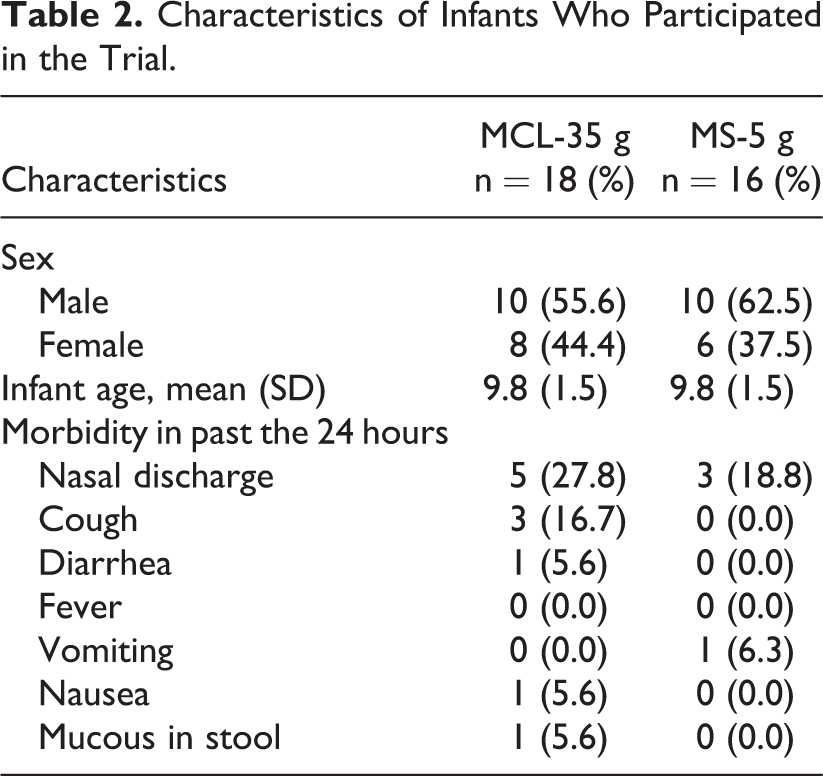
A total of 36 infant–mother pairs were screened and recruited into the study but 34 eventually participated in the study. Eighteen infants completed the MCL-35 g trial (Table 2), whereas 16 infants completed the MS-5 g trial (Table 2). Infants who participated in the MCL-35 g comprised 10 (55.6%) males and 8 females. Ten (62.5%) males also participated in the MS-5 g trial. Mean age of infants who participated in both groups was 9.8 (±1.5) months. Nasal discharge was the most commonly reported morbidity symptom within the past 24 hours for all infants for both MCL-35 g and MS-5 g.
Characteristics of Infants Who Participated in the Trial.
Part 1—Test feeding of MCL-35 g and MS-5 g
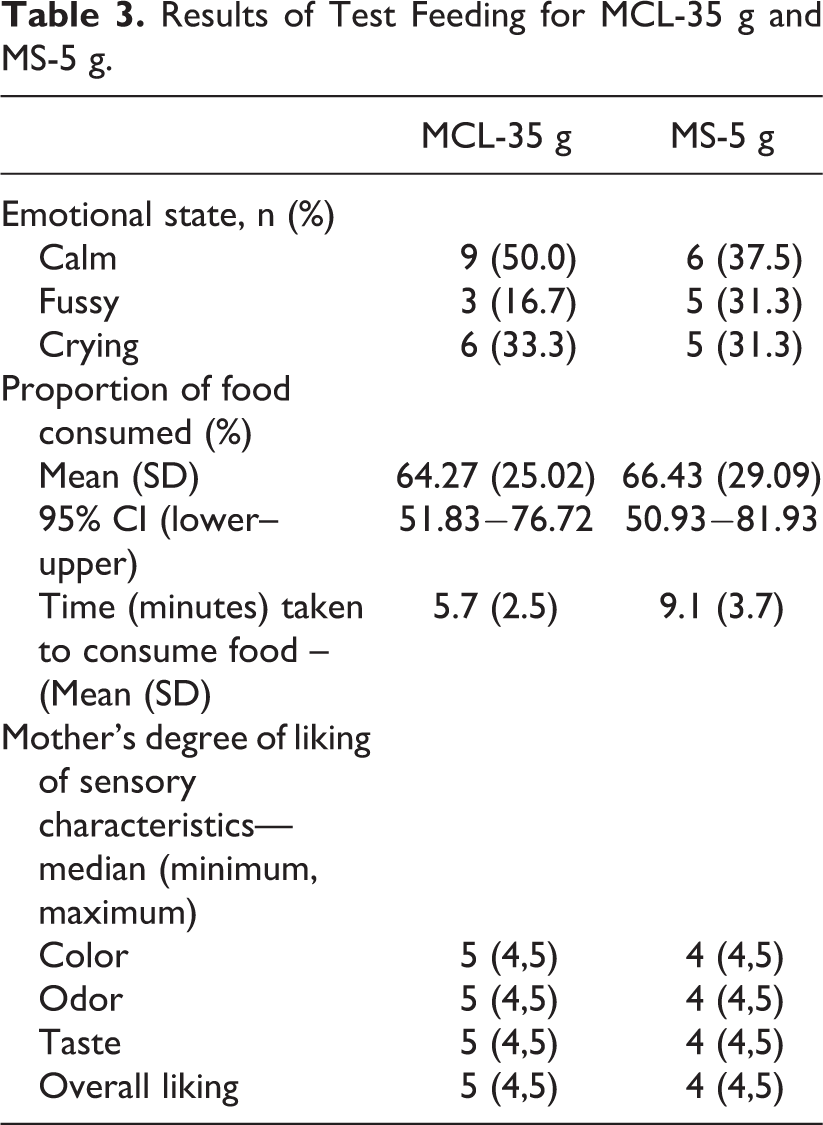
The emotional state of all infants during feeding was recorded during part 1 of the trial (Table 3). For the MCL-35 g group, infants consumed a mean proportion of 64.3 ± 25.0% of the test food offered within a mean duration of 5.7 ± 2.5 minutes, whereas MS-5 g infants consumed a mean proportion 66.43 ± 29.1% of the food offered within a mean duration of 9.1 ± 3.7 minutes. The 95% confidence interval for the mean proportions consumed is reported in Table 4. For mother’s perception, the median response for each sensory quality (overall liking, color, odor, and taste) for MCL-35 g was 5 (“like a lot”), and ranged from 4 to 5 whereas for MS-5 g, the median response for each sensory quality was 4 and it ranged from 4 to 5 (Table 3).
Results of Test Feeding for MCL-35 g and MS-5 g.
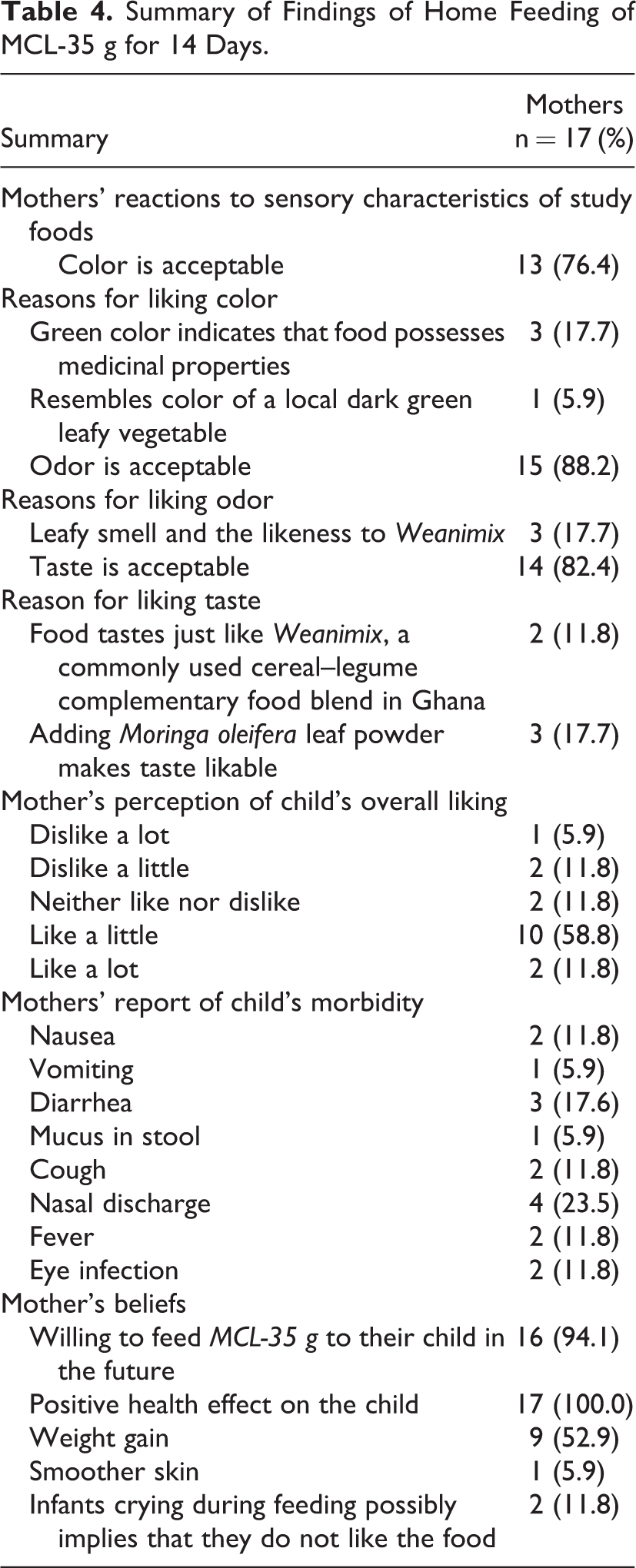
Summary of Findings of Home Feeding of MCL-35 g for 14 Days.
Part 2—Home use of study foods under real-life conditions for 14 days
MCL-35 g
The summary of mothers’ responses to acceptability of MCL-35 g after feeding children at home for 14 days is reported in Table 4 and that for MS-5 g is reported in Table 5. The median proportion of MCL-35 g consumed by the infants per day during the 14-day home use period was 71.5% (Table 6). Infants ate significantly more food daily, during the second week of the 14-day trial period compared to the first week (Table 6). It was observed during the monitoring period that all the leftover cooked food that needed to be weighed to estimate daily consumption of MCL-35 g was in the form of porridge.
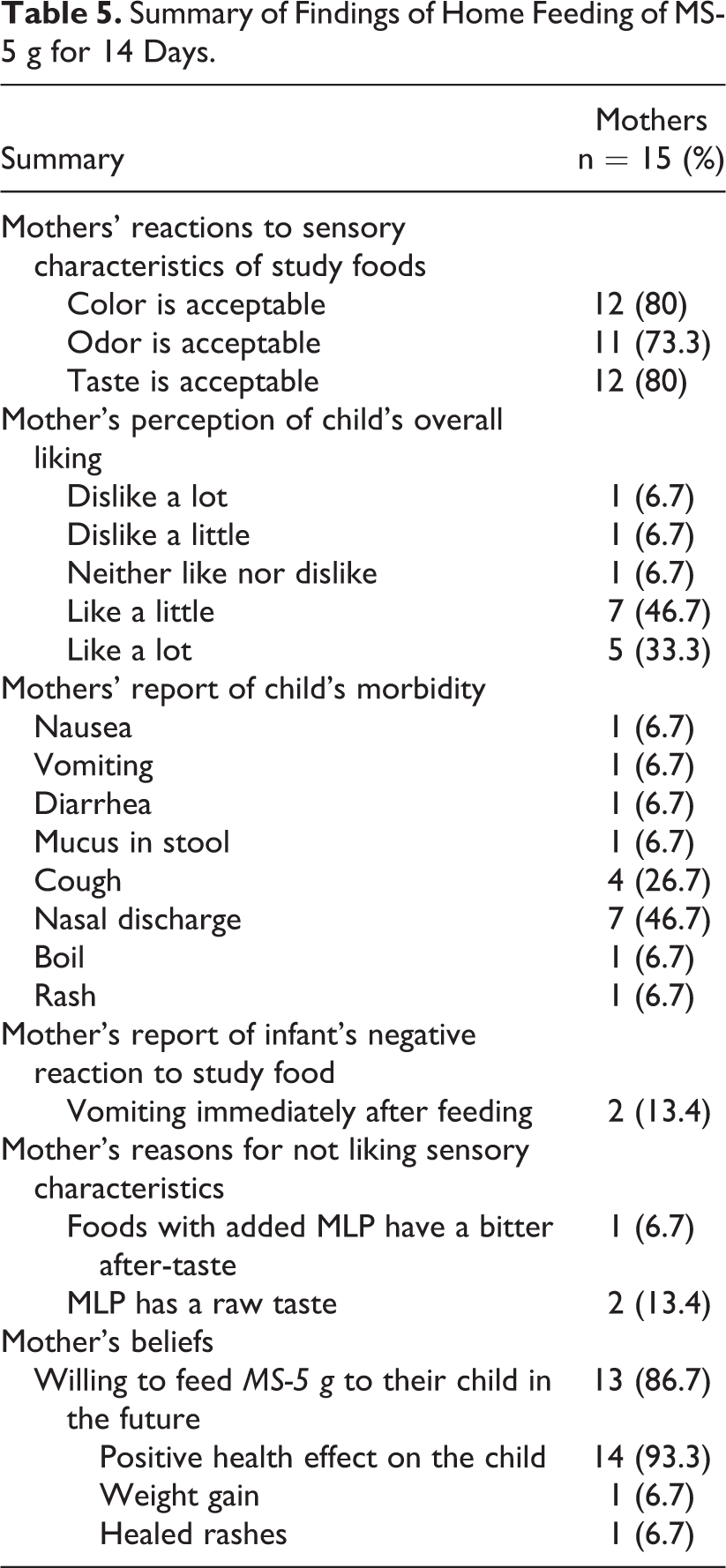
Summary of Findings of Home Feeding of MS-5 g for 14 Days.
Consumption of MCL-35 g and MS-5 g During the 14-Day Period.
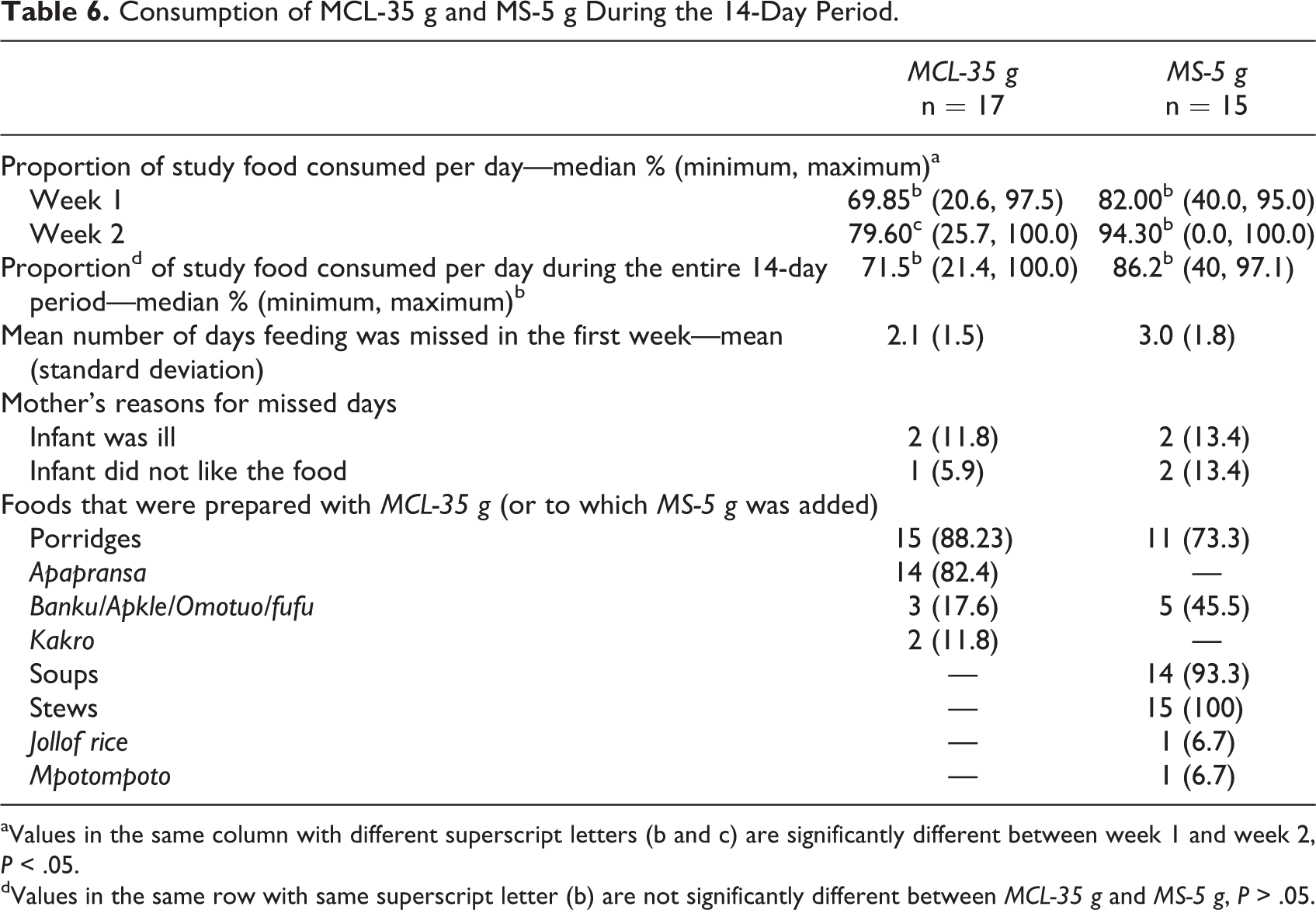
aValues in the same column with different superscript letters (b and c) are significantly different between week 1 and week 2, P < .05.
dValues in the same row with same superscript letter (b) are not significantly different between MCL-35 g and MS-5 g, P > .05.
Regarding mother’s perception of infant’s overall degree of liking of MCL-35 g during the 14-day trial, 10 (58.8%) mothers rated the supplement “4” (“like a little”), while 1 mother gave a rating of 1 (“dislike a lot”). On their reactions to the sensory qualities of foods prepared with MCL-35 g, majority of the mothers reported that they liked the color (76.4%), taste (82.4%), and odor (88.2) of MCL-35 g. Reasons for their reactions to the sensory qualities are outlined in Table 4. No mother reported a negative reaction to MCL-35 g when consumed by the child. All mothers believed the MCL-35 g had a positive health effect on the child, with majority (94.1%) of them indicating their willingness to feed the food to their children in the future. Two mothers however associated crying during feeding with the possibility of children not liking the food.
MS-5 g
The summary of mothers’ responses to acceptability of MS-5 g after feeding children at home for 14 days is reported in Table 5. The median (minimum, maximum) proportion of MS-5 g consumed by the infants per day during the 14-day home use period was 86.2% (40%, 97.1%; Table 6). Majority of mothers reported that they liked the color (80%), taste (80%), and odor (73.3%) of the MS-5 g. With the mother’s perception of infant’s overall degree of liking of MS-5 g, more than half of mothers (58.8%) rated the supplement “5” (“like a lot”; Table 5). Two of the mothers reported that their infants vomited immediately after they consumed the home food mixed with MS-5 g. Most mothers (86.7%) were willing to feed their children with MS-5 g in the future. Majority (93.3%) of them also believed that MS-5 g had a positive health effect on their child.
Discussion
Findings of this study suggest that both MCL-35 g and MS-5 g were accepted by mothers and infants who took part in the study. This finding is consistent with findings of an acceptability study among school children who were fed with MLP-fortified dishes over a 2-week period. 10 The assessment of the acceptability of foods for children is often a bit challenging because of the need to depend partially on the opinion of mothers whose tastes and food preferences, as adults, are different from those of the children. 21,22 For these reasons, the mean proportion of offered food consumed by the infants themselves was used as a proxy indicator for part 1, the test feeding aspect of the study, as was done in similar studies in Ghana and Bangladesh. 21,22 The study in Bangladesh, which tested the acceptability of 3 ready-to-use supplementary foods made from local ingredients, found that proportion of test food consumed ranged from 34% to 57%. 22 In the Ghanaian study, infants consumed 72% of the test meal. 21 The rationale for the test feeding is that with no forced-feeding, the amount of the offered food consumed by infants would depend largely on the extent to which they liked the food, given that none of the infants had been fed for at least 1 hour prior to the test meal. The organoleptic test responses from the mothers for both MCL-35 g and MS-5 g suggested a high level of acceptability, but as observed in similar studies, 21,22 such hedonic responses may not be conclusive because respondents could be reluctant to give negative evaluations. 23 Thus, combining the results from both the test feeding and the 14-day home use trial was considered probably the best way to judge the acceptability of the study foods.
Acceptability of MCL-35 g
Based on our findings, we can say with reasonable certainty that infants and their mothers accepted MCL-35 g when used to prepare a porridge. Porridge can be instantly prepared with cereal–legume composite flour and fed to children; hence, its preference over other dishes further enhances its use as a vehicle for MLP delivery. 10
It is however necessary that future studies observe the phenomenon of crying during feeding, as reported by 2 mothers to determine whether or not crying is an indicator of child’s dislike for porridges prepared with MLP. Regarding the maternal reports of infant diarrhea and nasal discharge during the study, it is impossible to rule out any causal relationship to the consumption of MCL-35 g. Ingredients used in the preparation of the study foods were familiar in the diets of the children, and all infants were screened at the time of enrollment for known intolerances to any of the study food ingredients. Thus, it is unlikely that the ingredients would cause an adverse reaction. However, future studies that incorporate MLP in infants’ diets should monitor the incidence of diarrhea, particularly during the first few days of the study.
Acceptability of MS-5 g
Based on our findings of both the test feeding and the 14-day home use period, we can say with reasonable certainty that infants accepted MS-5 g when added to their usual foods such as porridge and also when added to soups/stews particularly. The generally positive feedback given by mothers on the use of MS-5 g in their infants’ meals is indicative of their willingness to feed MS-5 g to their infants in the future. Majority of mothers in this study added MS-5 g to stews and soups during the 14-day trial period. This is consistent with the report by Glover-Amengor et al, 10 which indicated that M oleifera leaves are eaten in stews and soups mostly. Our findings on mothers’ reactions to the taste and color of MS-5 g provided useful insights for future research. The green color imparted to foods as a result of the addition of the Moringa oleifera leaf powder affected the rating by some mothers although for majority of mothers, this was not an issue. Olorode 14 in his study on sensory characteristics of maize porridge fortified with MLP noted that the green color of the formulated porridge is contrary to the normal white or yellow color of the maize porridge.
Reported morbidity during the 14-day feeding included nasal discharge, cough, and vomiting, all of which are common among children. It is important however that future studies clearly examine any adverse reactions related to feeding MLP.
One mother’s comment on her willingness to feed MS-5 g to her infant only if the supplement was available for sale from the health facility (but not the open market) reflected her concerns regarding the safety of the supplement. Food safety issues have been a challenge in developing countries and have been associated with morbidity and mortality. 24 This mother’s comment thus gives an indication of some awareness of food safety issues in the population, which is a step in the right direction.
Acceptability of Complementary Foods that Incorporate MLP
Wardle et al 25 have reported that repeated exposure to the taste of unfamiliar foods is a promising strategy for promoting liking of foods in children. This evidence by Wardle et al supports the findings of the 14-day “home use” period of our study foods. For both MCL-35 g and MS-5 g, median proportion of intake was numerically higher in the second week of the trial when compared to the first week (Table 6). This difference however was only significant for the MCL-35 g group but not the MS-5 g group. Although median proportion of intake during the 14-day was not significantly different between the 2 study foods, MS-5 g median proportion of intake (86.2%) was higher than MCL-35 g intake (71.5; Table 6). This gives an indication that complementary foods that incorporate MLP may be more acceptable when MLP is added as “sprinkles” to infant’s usual complementary foods (as was done with MS-5 g) than when used as part of a cereal–legume flour to prepare porridges and other meals (as was done with MCL-35 g). This is however an early speculation based on the findings of this study; further studies will have to be conducted to clearly identify which complementary foods that incorporate MLP will be more acceptable to infants. In their study of acceptability of locally produced ready-to-use therapeutic foods (RUTFs) in 4 developing countries, Weber et al 26 found that a child’s willingness to consume RUTF may differ when mixed with other foods. This finding may also apply in the use of MLP to fortify complementary foods. A limitation of our study is the fact that methods for estimating leftover foods for MCL-35 g for the first week and second week were different. The methods for estimating left over MCL-35 g and MS-5 g also varied. Further studies should consider more objective approaches to measuring proportions of MLP-fortified foods eaten throughout the trial period in order to avoid errors in estimation as well as recall bias.
Conclusion
Findings of our study suggest that MLP used either as part of a cereal–legume blend (MCL-35 g) or as a supplement (MS-5 g) to be added to infants’ usual diets are well accepted by infants and their caregivers in Asesewa in the Upper Manya Krobo district of Ghana. Young child feeding continues to be challenge in West Africa and much of the developing world. The findings of this study give further support to the emerging use of MLP to improve the nutrient quality of complementary foods and call for further research to identify which complementary foods that incorporate MLP will be more acceptable to infants.
Footnotes
Acknowledgments
The authors thank the nurses of the Asesewa Child Welfare Clinic (CWC) and the mothers, and caregivers of infants, for volunteering to participate in this study. A special thanks to Prof. Anna Lartey of the Food and agricultural organization, for her helpful contributions and comments at all the various stages of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the International Development Research Centre (IDRC), Canada, Research grant No 104519-009 (IDRC RC) to the University of Ghana; the UG-Carnegie PhD research grant No B8739 (R01) and the Association of African Universities (AAU).