
Abstract
Introduction:
Childhood malnutrition is a major public health issue. Multidisciplinary approach for Improvement of Nutritional Status of Children in Iran was implemented in order to reduce malnutrition among children.
Objective:
This study aimed to evaluate the implementation aspect of the program and to explore key informants’ perceptions and experience regarding the factors affected its implementation.
Methods:
Data were collected through the review of secondary data and semistructured interviews at national, province, and local levels. Four layers of key informants were selected purposefully for interviewing, including policymakers, senior nutrition officers, head of Hygiene, Remedy and Insurance Affairs in Imam Khomeini Relief Foundation, and community health workers. Qualitative content analysis was carried out based on Supporting the Use of Research Evidence framework and Tailored Implementation for Chronic Diseases’ checklist to interpret the viewpoints of the study participants.
Results:
Results showed that the program had successes in improving mother’s knowledge on health, nutrition, and child care through health system and increased families’ access to food, but there were some aspects that affected program’s implementation. Some of these factors are the lack of clarity in the program’s protocol and indicators, human shortage and inadequate financial resources, poor facilities, inattention to staff motivation, insufficient commitment among different sections, poor communication and supervision among different executive sections, and program protocols designing regardless of practical condition.
Conclusion:
Based on the results, top-down approach in policymaking and inadequate financial and human resources were responsible for most of the challenges encountered in the implementation.
Keywords
Introduction
Childhood malnutrition is a major public health issue which adversely affects short- and long-term health and economic well-being of children 1 and can ultimately lead to inadequate adult productivity and national economic growth. 2 Multidimensional nature of malnutrition 3 emphasizes on the need for a multisectoral response for alleviating undernutrition. Community-based nutrition programs linked with health, water, sanitation, and other relevant interventions, including poverty reduction are priority strategies that can bring measurable improvements in children’s nutritional status, survival, and development. 4,5 Success in addressing undernutrition is essential in contributing to human rights for health and freedom from hunger.
In the Islamic Republic of Iran, malnutrition is a public health problem, especially in low-income and deprived segments of the nation. 6,7 According to the first national Anthropometric Nutritional Indicators Survey (ANIS1) in 1998, 13.9%, 9.5%, and 5.3% of children younger than 5 years were stunted, underweight, and wasted based on height for age, weight for age, and weight for height z score, respectively. 8 In the ANIS2 in 2004, the figures were improved to 4.7%, 5.2%, and 3.7% for stunting, underweight, and wasting, respectively. 7 Implementation of primary health care (PHC) across the country is known as one of the powerful reasons behind the decline of malnutrition in Iran. 9 –11 Following this successful experience, in 2005, the Multidisciplinary Program for Improvement of Nutritional Status of Children in Iran was initiated nationwide aiming to improve nutritional status of children and reduce malnutrition among children younger than 5 years, especially those from socially or economically deprived families.
Ten years after the establishment of this large-scale government-sponsored program, no evaluation of its implementation and effectiveness in reducing childhood undernutrition is available. This study is part of a comprehensive evaluation of the process, effectiveness, and cost of the program which intends to measure the “gap” between what was planned for (policy expectation) and what occurred in reality. The present article aims to explore perceptions and experience of key informants regarding the program design and implementation and factors affected its implementation.
Description of the Program
The program started in 2005 aiming to reduce malnutrition among 6-month to 6-year-old children of the country. The program is mainly sponsored and led by the Department of Community Nutrition of the Ministry of Health and Medical Education (MOHME), the Ministry of Cooperatives, Labor and Social Welfare, and Imam Khomeini Relief Foundation (IKRF). It consists of 2 major parts—collaborative and supportive. The “collaborative” part has intersectoral approach. Based on the instruction of the program, major components of this part include the promotion of good sanitation and access to clean drinking water, illiteracy elimination, and health and nutrition education sessions for mothers on child feeding, breast-feeding, healthy meal planning for households, complementary feeding, family planning, growth monitoring, and some empowerment strategies including home gardening, income generating activities, and increasing food accessibility. In addition, in-service workshops are held for health workers to improve their health and nutritional knowledge. Different sectors, including agriculture, education, rural development, social welfare, and Iran Literacy Movement Organization collaborate with the health system on these activities. Based on the program instruction, in rural areas, free seeds should be provided to the families in order to promote home gardening and to increase their access to vegetables. There are also some activities related to income-generating schemes for households through loans for ranching, bee keeping, carpet weaving, and confectionery production in the instruction of the program. 12
The “supportive” part of the program has a targeted approach and its main targets are malnourished or growth retarded children who live in poor families. The main purpose of this part is to improve food intake and weight status of malnourished children who mostly have nutritional deficiencies. These children are identified and screened actively through growth monitoring services of the PHC system, and introduced to IKRF for families’ economic status confirmation. After nomination process, children receive free food basket on a monthly basis, the content of which is defined by the nutritionists in the provincial PHC system based on child’s age group. The food baskets or food vouchers are funded and provided by IKRF and distributed among beneficiary households through health house/centers. Over the year prior to this study, the distribution mode of the food baskets was changed to electronic credit cards, thereby; families should buy specified food items from predefined stores/supermarkets. The monetary value of the food basket is approximately 16 US$/month/child which was provided to 62 522 children in late 2013.
In addition, based on the program instruction, mothers are required to attend regular visits in health houses/centers for health and nutrition monitoring. Through these visits, children’s weight and height are measured according to the National Integrated Management of Childhood Illness protocol. 13,14 Children up to the age of 3 years are covered by the program even if their weight-for-age is improved. For children older than 3 years, monitoring visits were defined every 6 months, and they would be excluded if their weight-for-age has improved and reached to the standards and this trend remains constant in 2 consecutive measurements. The program progress is being monitored through the count of defaulted, improved, and death rate of the covered children in every 6 months.
Methods
Study Design and Settings
Qualitative research methods, including review of secondary data, and semistructured interviews were employed to evaluate implementation of the program. “Implementation” is defined as “what happens between policy expectations and (perceived) policy results.” 15 Qualitative methods were employed as proper approaches to determine objects and issues from the point of views of the people involved. 16 Data were collected at national, provincial, and local levels from March 2014 to September 2014. The local level data were collected in 2 provinces (Qazvin and Semnan). To conduct semistructured interviews with key informants, purposive sampling frame was used to recruit interviewees with rich and relevant experience. 17 Four layers of key informants were selected—(1) Policymakers who were involved in designing the program, from the involved organizations, including MOHME, IKRF, and, the Ministry of Cooperatives, Labour and Social Welfare; (2) senior nutrition officers with at least 4 years of experience in the program within the medical universities, identified through the Nutrition Department of MOHME. Medical universities were chosen from different geographical regions of Iran to represent diversity of the implementation in different provinces. (3) In the same city, the head of Hygiene, Remedies and Insurance Affairs in IKRF was also interviewed. (4) Community health workers (CHWs) in urban (Kardan) and rural (Behvarz) areas of Qazvin and Semnan (2 selected provinces) with at least 6 months of experience in the program. All participants accepted to take part in the interviews.
Sampling and Data Collection Techniques
Secondary data review
All available documents related to the initiation and implementation of the program were collected from official sources, including MOHME, IKRF, the Ministry of Cooperatives, Labour and Social Welfare, and deputy of health in medical universities. Program’s protocol and criteria were reviewed. The rate of improved/defaulted/death children and the nutrient content of food basket during the last 3 years were studied via progress reports sent to the Nutrition Department of Iran’s MOHME by medical universities. The review of documents helped to get an overview of program’s initiation and its collaborating organizations and their responsibilities in the program.
Semistructured interviews
Thirty-five face-to-face semistructured interviews were held by the first author, from March 2014 to September 2014 using an interview guide 18 in a location selected by the interviewees. The interview guide was tested in 2 pilot interviews. Although, the order of questions was modified to better align with the flow of conversation, no essential changes were made following the pilot. Participants were asked a set of questions concerning the objectives of the program, the implementation of different components of the program, and any perceived barriers and facilitators to the implementation of the program. Questions were semistructured, but the interviewer was able to ask follow-up or probing questions based on participants’ responses to previous questions. 19 All interviews were conducted in the native language (Farsi) of the respondent. Each interview lasted between 30 and 80 minutes and was audio recorded with written consent of the participants.
Data Analysis
The recorded interviews were transcribed verbatim and checked with field notes for the accuracy of transcription as soon as possible after each interview. Field notes were used as supplements to the recordings. Preliminary analysis was done at the same time by the first author. Interviews continued until the saturation of the data, 20 which occurs when further interviews do not add new information. Two additional interviews were conducted to confirm data saturation. All transcripts were imported into MAXQDA software (version 2010) for analysis. Qualitative content analysis was used for coding data to come up with comparable categories and interpret their meaning into concepts that describe the implementation of the program. 21 In organization phase, open coding was undertaken, and then related concepts were condensed into categories on the basis of underlying properties and dimensions. Similar categories were grouped under higher order headings. 21 Categorization was done based on Supporting the Use of Research Evidence (SURE) framework and Tailored Implementation for Chronic Diseases’ (TICD) checklist. Categories were allocated within these frameworks as far as possible. The SURE framework provides a comprehensive list of possible factors that may influence the implementation of the program and health system intervention. The TICD checklist provides comprehensive and nonoverlapping determinants of health-care professional practice. 22,23 To check whether interpretation is true, we returned to the data continually. Finally, the categories were abstracted to refine major codes and subcodes. One author was involved in coding all the data. 24 To ensure similar understanding of the concept and increase the ease of comprehension, 25 another member of the research team coded and analyzed the transcripts independently. Then the coded text was discussed with the authors and coding was adjusted where appropriate. Wherever the meaning was unclear or doubtful, the interpretation was discussed with different members of the research team. Discussions continued until no contradictions existed and a common understanding was attained. This prevented researcher’s bias and strengthened internal validity. 26
Ethical Consideration
All participants were informed about the scope of the study and the overall subject of the questions. The interviewees were informed that they could leave the interview at any point or request for the termination of the interview. Confidentiality and anonymity was assured to all of them and maintained throughout the study. Ethical approval of the study protocol was obtained from the National Nutrition and Food Technology Research Institute of Iran (contract number 450.88, 2014.05.21). Furthermore, permission was granted by the deputies of health in medical universities in each province.
Results
Interviewees included 5 policymakers, 11 senior nutrition experts in deputy of health of medical universities, 5 experts in IKRF, and 14 CHWs in Qazvin and Semnan provinces. The results were reported according to the SURE framework and TICD checklist in 5 levels, including program’s specification, program’s recipients, the implementers of the program, health system constraints, and social and political constraints. Major themes in each level are presented in Table 1. Throughout the text, direct quotes from participants are shown in italics.
Factors Affecting the Implementation of MuPINSC.
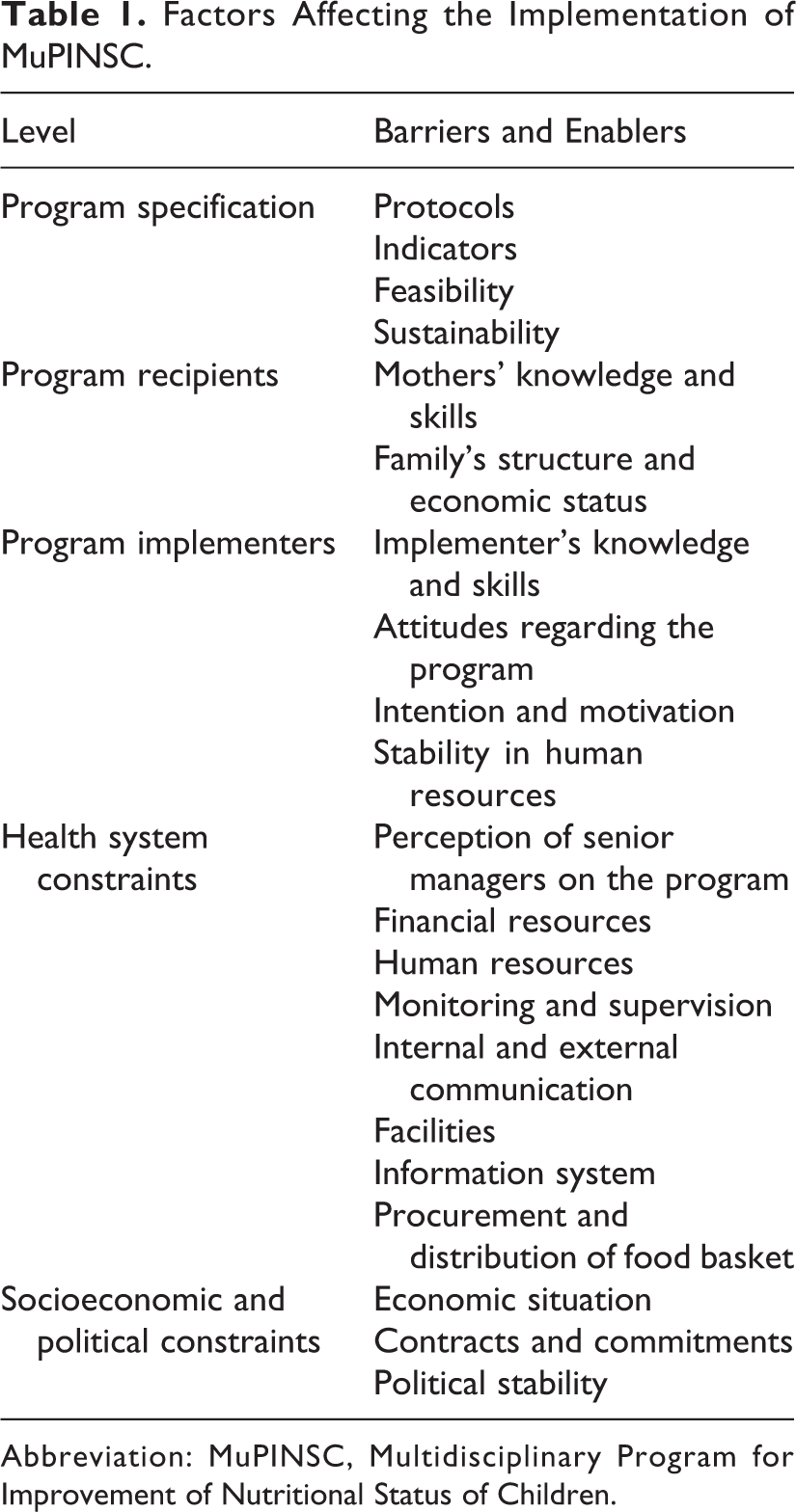
Abbreviation: MuPINSC, Multidisciplinary Program for Improvement of Nutritional Status of Children.
Program’s Specification
Protocols
Through the documents reviewed, the program goal is stated in a very general term, and no clear plan on steps to achieve program goals is in place. Despite the fact that all of the casual factors of malnutrition identified in the UNICEF framework 3 have been addressed in the protocol of the program, there are no clear instructions on how to act upon those factors. In the meantime, the need for protocol updating was the main complaint of the interviewees in these provinces. While the last version of the protocol was developed in 2010, health deputies/centers are still following the old protocol developed in 2006. In the updated protocol, there were some clarification on instructions related to monitoring system(s) and children’s exclusion criteria within the program. However, there is still no improvement in terms of children’s eligibility criteria and bottom-up communication within the program.
Indicators
Ambiguity in defining indicators both for child selection/family Socio-Economic Status (SES) assessment and also child recovery was a concern for most of the interviewees. There was no clear definition for the SES of family as one of the eligibility criteria for attending in the supportive part of the program. Therefore, it is defined in a subjective manner.
Almost all of the CHWs believed that there was a problem with the excluding criteria of children and it needed major revision. They stated that acting on the present protocol has resulted in a relapse after children exclusion as reflected in the program progress reports. Most of the children, who recovered and excluded from the program, became malnourished two or three months later. Therefore, we decided to cover children until six years of age, and excluded them if they did not recover. We suppose that if malnourished children did not recover with food basket, food was not the main cause of his/her malnutrition or the family shared the food basket with other members of the household or sold it. (A Nutritionist participated in interview)
Feasibility
Most of the nutritionists in health deputies agreed that it seems impossible to implement all parts of the program in the present resource-poor setting. A shortage of health workers, lack of motivation to perform additional work related to this program, and inefficient training for health workers and others involved in the program may have caused difficulties in implementing all aspects of the program. Lack of enough facilities for implementation affected feasibility and effectiveness of the program.
Sustainability
For the program to have sustainable effects, proper strategies to empower families economically and to increase access to food are required. More than 85% of interviewees stated that many children will become malnourished after exclusion from the program. Based on the interviews, relapse of children mainly occurred due to the low-economic status of families and lack of household’s ability to provide proper care for the children after recovery. Some household empowerment and income-generation strategies have been laid out in the program’s protocol (eg, loans for animal husbandry, bee keeping, carpet weaving, and confectionary making), but none of them has been actually implemented yet. Almost all of the nutritionists stated that no memorandum exists between collaborating organizations and the health sector regarding family empowerment. One of our problems is weakness in inter-sector parts. Unless there is a memorandum between the ministries, I cannot focus on home gardening or activities like this which require collaboration with other sections. An agreement between ministries makes our work easier and feasible. (A nutritionist participated in an interview) I think helping families with supplementary food basket is not bad but we have to think outside the box. We identify families and IKRF provides them with the food baskets. But it should empower them as well. They should spend their funds in this way. IKRF should have job creation scheme and provide marketing support for families. We have to pay attention to these issues in designing the program. We have to use the capacity of supportive organizations, donors, Non-Governmental Organizations (NGOs), State Welfare Organization, and IKRF for empowerment, job creation, and the income generation of families. (A nutritionist participated in an interview)
Program Recipients
Mothers’ knowledge and skills
About half percent of interviewees agreed on the effect of the program on mother’s knowledge and skills regarding their child health, and nutrition; however, they believed that increasing mother’s knowledge was one of the success points of the program. Based on the program’s protocol, receiving food basket was conditional to attending mothers in the training sessions and children routine health care. This was the reason that many interviewees mentioned the effect of the program on mothers’ knowledge. However, after the E-cards distribution, this obligation does not work anymore. More than half of the interviewees believed that in spite of the program and PHC’s emphasis on mothers’ education on the healthy feeding of children, educational activities of the program are rather weak. Interviews showed that face-to-face education of the mothers was in place, but there were no group education or skill development session(s), especially in urban health centers.
There was also disagreement on the content of the counseling sessions. The policymakers and some of the nutritionists believed that contents and methods of nutrition counseling needed to be changed. They suggested replacing the use of technology (eg, educational film) with face-to-face counseling to increase effectiveness CHWs emphasized on face-to-face education and believed that some information on child feeding needed to be repeated for them continually.
Family’s structure and economic status
The cultural background and economic status of families is another factor affecting implementation of the program. In some areas, families look at the program as their unconditional right, and in some cases, families argued about their eligibility with CHWs. A few interviewees mentioned that it was possible that parents make children malnourished to become eligible for the program. In some cultures, children live in the extended families and these environments affect child’s nutrition despite receiving the food basket. Within such families, grandparents may not pay enough attention to a child’s nutrition, and as a result, implementing the program recommendations may be interrupted. Economic status of families is another factor that can affect mothers’ compliance with the program recommendations. When they could not afford to purchase essential basic needs, it seems reasonable for them to buy nonfood item(s) using the E-card received through the program.
Program Implementers
Implementer’s knowledge and skills
Staff training is a necessity for program’s success. Good training makes staff more confident and competent and helps keep the program moving forward. Based on policymakers’ narrations in MOHME, intersectoral workshops had been held for implementers at all levels. In addition, there were limited educational materials in health centers for CHWs due to financial constraints. Most of the CHWs stated that they use their own knowledge for training mothers, and their knowledge and skills needed to be updated through the program. One of our major problems in this program was unjustified believes of experts about the program, its initiation and goals. For example, as an expert who was working in a town at that time, I got information on the program by myself. There was no class, or training for me.(A nutritionist participated in an interview)
Attitudes regarding the program
There were different perceptions regarding the program goals among the policymakers and implementers. They defined the program goal in different ways, including reducing health problems and malnutrition in poor rural communities, improving malnutrition among children in poor families, and eliminating poverty through partnership with other organizations. Its main goal was supplementation of malnourished children specifically those who lived in poverty and poverty was the main cause of their malnutrition, those who didn’t have access to required growth nutrients. They want to prevent further complications. (A nutritionist participated in an interview)
In spite of IKRF staff, most of the interviewees in health sector believed that the program has not reached its predetermined goals in reducing malnutrition among children. Some health workers stated that implementing the program in this manner is wasting resources. They believed that the program has made most of the families’ dependent to the food basket without empowering them; there were families who thought that it is their right to be a beneficiary of the program. Almost all the nutritionist believed that this program provides a bottleneck for the growth monitoring of the children in health house/centers.
Intention and motivation
Financial and nonfinancial incentives are necessary to boost the morale of the health worker,
27
contribute to the motivational processes and affect the individual’s real and perceived ability to carry out their tasks, and stimulate their adoption of the program goals.
28
However, CHWs have to do duties related to this program (eg, selecting eligible children, growth monitoring, and mother’s education and preparing progress reports) in addition to their daily routines with no incentives. High workload of staff and shortage in human resources within the program indicated a need for financial and nonfinancial incentives to motivate present workers. Despite the health policymakers’ emphasis on the need for motivating health workers within the program, none of the health workers had received any incentives through this program. First, we are working for GOD’s sake but if the administrators have encouraged us more, we would have been motivated and would love our job more. It is correct that the result of our work may not always be good, or it may even be bad, but we should be informed in a proper way. This really destroys our motives. (A CHW participated in an interview) This is encouraged to give incentives to health workers. In the other hand, they are not justified. They are not supported through the program. This issue could influence the success of the program. They have to be encouraged to do extra work for this program. (An interviewee in IKRF participated in an interview)
Stability in human resources
Frequent replacement of CHWs is one of the constraints of health sector. In the recent years, health centers in Iran usually use employees on short-term contracts as their personnel; therefore, they leave their work by the end of their contract. This was a common issue in deprived areas and those with bad climate. As a result, after 2 years, they left their position to beginners with no experiences. Therefore, there is a need for training beginners in negotiation and advocacy skills. The implementation goes well in places with stable and more experienced staff. This is because of their awareness of the program and its implementation. (A policy maker participated in interview)
Health System Constraints
Perception of senior managers on the program
Interviewees believed that the perception of senior managers, including dean of universities and deputies of health, about the program can influence program implementation. For example, if they believe in the importance of child nutrition programs and their effects on political and economic development, they may facilitate funding for the program and encourage staff to collaborate. As a matter of fact, in terms of budget, hospitals and curative approaches are still the main priorities in medical universities in Iran, compared to primary and secondary preventions. Most of the times, top managers perceive this program as a burden. I believe that the main problem is lack of stability in our management and supervisory system. (A nutritionist participate in an interview)
Financial resources
Almost all of the interviewees considered low budget of the health sector as a key factor affecting the implementation of different parts of the program, including staff recruitment, training mothers, and health/intersectoral workers, producing educational materials, providing supervision, motivating health workers, and for intersectoral partnership. Such limitations have resulted in partial implementation of the program in many provinces. Interviewees expressed financial limitation as a reason for not implementing of intersectoral part. I knew that the education component would fade out, because education and training needs energy, money, and support…(A policy maker participated in an interview)
Human resources
High workload was the major complaint of CHWs. There were staff shortages in the health house/centers, as well as in the deputy of health. At the national level, policymakers were well aware of staff shortage and were in favor of hiring more health workers to deal with this problem; however, it was not possible because of organizational and financial restrictions. For example, they could not recruit more behvarzes or midwives in health house/centers. Based on the organizational chart of health-care system in Iran, there is no acting nutritionist in health house/centers, except for the health districts. For this reason, some parts of the program, especially nutrition counseling, could not be implemented properly. When in inter-sectoral part, they ask us to activate our nutrition counseling centers, do they consider the workload? Needed staffs? Space? Equipment?…Is there any position for defined nutrition experts at all? When I don’t have a position for a nutritionist in my organizational chart, when there is no budget for the head of the center to use for the program, how can I run a nutrition counseling center? (A nutritionist participate in an interview)
In IKRF provincial office, 1 person was responsible for this program. They mentioned that because of the shortage of human resources in this program, they were not able to screen families based on SES; therefore, in many provinces, this task is delegated to health workers. We have to introduce malnourished or growth retarded children to IKRF. Then their experts should assess their eligibility regarding the families’ SES. Today, they said that they don’t have enough staff to do the assessment and did not do it. (A CHW participated in an interview)
Monitoring and supervision
Supervision is intended to improve performance and to motivate staff. Most of the CHWs declared that they have not been supervised by health inspectors regarding this program and have not received any feedback from health districts on their performance. They believed that regular visiting could help them to speak about their daily difficulties and could lead to practical solutions. In addition, it could motivate them to improve their performances. Nutritionists in the deputies of health believed that supervision is necessary in all aspects of the program, including child screening and selection, growth monitoring, mothers’ education, and retail stores. This is our weakness. Lack of a monitoring system results in a poor performance. (A nutritionist participate in an interview)
Internal and external communication
In recent years, only the supportive part of the program has been implemented, whereas the intersectoral section is somehow ignored. Most of the interviewees believed that intersectoral meeting between health section and IKRF in all national and provincial levels was the leading cause of success of the supportive part. All of the interviewees acknowledged that implementation suffers from communication gaps between health sector and other partners from national and provincial levels and consider this as the main reason for not implementing the intersectoral part.
Another raised issue was lack of bottom-up communication within the program, specifically in the health sector. In addition, there are several offices in health deputies that work in parallel with each other, and this may influence their work. Actually the relationship between different departments of the health sector was a big issue in the implementation of some parts of the program. We have different departments in the deputy of health. They work separately. Here is nutrition department and we should work on child’s nutrition. There are family health department with a children’s health office beside us. For example, they are responsible for breast feeding and complementary feeding of children and we are responsible for this program and the improvement of nutritional status of children. We should form one group to increase our efficiency. We have to collaborate with each other; however, sense of collaboration is very weak in Iran. (A policy maker participated in interview)
Facilities
Almost all of the CHWs mentioned that the facilities were not in line with what was forecasted by the program. For example, it was impossible to equip kitchens in the health house for practical nutrition education (cooking sessions) due to the lack of adequate space and funding to purchase raw materials and cooking equipment. Moreover, equipped kitchens in most cases were limited to a stove and a pot. On the other hand, some of the interviewees in health deputies mentioned that some of the health staff did not value cooking sessions. Some of our nutritionists declared that ‘we are not chefs to teach cooking and complementary feeding’. (A nutritionist participate in an interview)
Information system
Monitoring and evaluation reports are rigorous enough to identify well-implemented programs.
29
Providing information on program progress and failure is necessary for the program’s success and sustenance. The progress report on the program was the only source of information for policymakers. Based on their opinion, this information was necessary for them for funding and decision-making about this program. They always complained about the delay in receiving the progress information from MOHME to lobby the parliament for the budget of the program. In my opinion, the design of the program is good and tasks are well defined. However, the implementation is poor e.g. in data analysis and report for policy making. (A policy maker participated in interview)
Procurement and distribution of food baskets
The IKRF is responsible for providing food baskets monthly or bimonthly. The IKRF staff claimed that they distributed food baskets regularly, since they have solved their financial limitations through good administrative strategies. On the other hand, health workers complained about irregular distribution of vouchers or charging E-cards.
Socioeconomic and Political Constraints
Economic situation
Inflation is a limiting factor affecting the quality of the food baskets. Almost all of the interviewees agreed that it has resulted in reducing the amount of food in the baskets despite the increase in its monetary value.
Some of the interviewees believed that unconditional cash transfer, another policy being implemented in the country over the last 4 years, has affected the implementation of this program via decreasing mothers’ motivation to visit health centers and taking their food baskets. As CHWs believed that this is due to the monetary value of the food basket which is not economical for some families compared to the cash transfer. Before the cash transfer program initiation, food baskets were a motivation to bring them (mothers) to the health centres for receiving educational programs. Some of the mothers now say that it is not worthy to come all this way to weigh the children and sit in the classes. It is not as important as it was before…(A nutritionist participated in an interview)
Contracts and commitments
At the start of the program, all of the organizations involved in both intersectoral and supportive parts agreed on strategies defined for the improvement of nutritional status of children. The lack of an updated contract between MOHME and involved organizations (except for IKRF) in recent years and changes in organizational structure and the agenda of involved organizations over time have resulted in the lack of enforcement in the intersectoral part. Some of the nutritionists in the deputy of health believed that these problems can be solved if the national nutrition and food security policy note is approved.
Political stability
Some of the interviewees believed that the instability of administrations due to changes in ministers, deputies, governor general, and managers following the presidential election every 4 years is an important issue that affects program’s stability. The justification of new managers is hard and time consuming. Governor general was the president of intersectoral meetings in each province. When he was sensitized enough about the importance of nutrition and specifically child nutrition, he would allocate enough funds.
Discussion
This study intended to explore key factors affecting the implementation of the national Multidisciplinary Program for Improvement of Nutritional Status of Children younger than 6 years in Iran. The findings show that in the opinion of most of the interviewees, program has had successes in improving mother’s knowledge on health, nutrition, child care, and families’ access to food. The program has managed to encourage mothers to bring their children to the health house/centers for routine health care and to participate in the training sessions in order to receive food basket. Good communication between IKRF and different parts of MOHME within the program resulted in the implementation of supportive part of the program for nearly 10 years and increased the capacity of children admission.
However, based on the key informant’s interviews, there are aspects of the program implementation that need serious considerations to ensure its effectiveness and sustainability. Some of the factors that negatively affected the program’s implementation are lack of clarity in the program’s protocol and indicators, human shortage and inadequate financial resources, poor facilities, inattention to staff motivation, insufficient commitment among different sections, poor communication and supervision flow among different executive sections, and designing program protocols regardless of practical conditions, as well as the political and economic situation.
Poor implementation of policies leads to policy “evaporation.” 30 To avoid this gap, policymakers should develop a strategy for implementation that explicitly takes into account the financial, managerial, and technical aspects of the policy (capacity) and the anticipated resistance and support from all the actors in the subsystem within and outside government. 31
Although nutrition interventions are consistently ranked as excellent investments, commensurate resources and policy support do not often follow. 32 Policymakers need data for decision-making, improving, and changing the plan of the program. The present study revealed the need for designing appropriate and clear definition of indicators and data collection techniques while being sensitive to practical conditions. According to the results, the program’s protocol is not adequately clear and practical. In addition, lack of communication between policymakers and implementers at different levels was responsible for most of the challenges encountered in the implementation of its updated version. Bottom-up approach can solve this problem. 33 With this approach, communication gaps among actors at all levels should be disappeared. There is a need to integrate the implementation process at district, provincial, and national levels. This approach can help to establish an upward communication flow.
Another factor that influenced the implementation of program was lack of commitment on nutrition interventions among different sectors involved in the program, even though policymakers had verbally and symbolically committed to address different sections of the program. There was not any memorandum on the implementation of the intersectoral part of the program; therefore, financial resources were not properly allocated to the implementation of this section. This is a common problem in the implementation of national food and nutrition programs in other countries. 34,35 In order to make different sectors more involved, highlighting the importance of children’s malnutrition from their perspective, signing new contracts, and allocating enough financial resources can be effective strategies.
Mothers had a major role in using the food baskets for their target children, and this was dependent on their awareness regarding malnutrition, and their knowledge and skills about proper use of food items included in the basket, as well as motivation and incentives to follow the program’s instructions with the support of family members. Meanwhile, CHW awareness about the program’s goals and their knowledge, skills, and incentives to deliver the program are other factors that can help to support mother’s child feeding behaviors. These are factors that should be considered in the planning phase of the program to ensure good implementation. 36 Based on key informants, specifically CHWs, there is not enough emphasis on such factors in program implementation. There is a need to support mothers and staff. Supporting staff can also alleviate these barriers by motivating and allowing adequate time for mother’s training and motivating. Indeed, protocol often stresses the need to train mothers and staff, but what this exactly entails is never detailed.
The pace and quality of implementation can be severely constrained by weaknesses in human and organizational capacities from national to frontline levels. 36,37 According to the present study, insufficiency in health staff within the PHC system, and for this program, as well as inadequate financial resources have prevented implementation of some parts of the program, including practical feeding and nutrition educational sessions for mothers, nutritional consultations, home gardening, and in-service training sessions. Considering low-budget share of MOHME in this program, options such as participation of private investors, donors, NGOs interested in food and nutrition issues, national and international foundations should be examined in order to widen the pool of available funds for the program. 38
This is the first evaluation study on this program in Iran. The qualitative design of the study made it possible to have a deeper understanding of the barriers and facilitators to the implementation of the program. One of the limitations of this study was “respondent validation,” and participant checking did not occur due to time and budget constraints and delays in preparation of the analysis report. It was assumed that the respondents were likely to forget or change their views. The other limitation of this study was lack of any archive related to the program design in MOHME. The analyses were strengthened through the use of the SURE framework and TICD checklist to categorize and analyze data related to the implementation of the program. Flexible and purposive approach to sampling resulted in recruitment of diverse participants. The study participants belonged to different geographic regions of the country and made it possible to explore the effects of different situations and contexts on the implementation of the program. The range of methods used is the other strong point of this research. A high degree of consistency of views from these diverse methods and participants provides confidence in the validity of the findings.
In conclusion, policymakers and implementers agreed on the importance of policy commitment, human and financial capacity development, and communication in the implementation of this large-scale program, like other national nutritional programs. In addition, they believed that social, political, and cultural factors that influence implementation of the program at local levels should be considered in designing the program. There were concerns about inadequate empowerment strategies that resulted in the dependency of the beneficiary households on the program and some negative related behaviors. The findings call for the need to redesign certain aspects of the program such as the protocol, allocating enough financial resources, hiring additional staff to focus on the program, engaging ways to prioritize children malnutrition within the collaborating organizations and good internal and external communications in order to pave the way for more effective implementation.
Footnotes
Authors’ Note
UNICEF played no role in the interpretation of the data or in the preparation of this article. DGh was involved in study design, collection, analysis, and interpretation of the data and writing of the article. NO was involved in study design, interpretation of the data and provided comments to the draft. AR contributed to the study design and interpretation of the data. HEZ were involved in study design and provided comments to the draft. ME contributed to data analysis and interpretation of the data and HR involved in study design. All authors were involved in the decision to submit the article for publication.
Acknowledgments
This work was administered under a cooperative agreement between UNICEF and NNFTRI with the support from Community Nutrition Department of MOHME and health deputies in medical universities of each province. The authors would like to thank Dr. Zahra Abdollahi and Ms. Mina Minaee in the Community Nutrition Department of MOHME for their great support in facilitating and enabling data gathering and interviews through the medical universities. We are grateful to Ms. Maryam Aghaian for transcription and type of texts related to interviews. We thank the policymakers, staff, and CHWs in all provinces, as well as Mr. Mostafa Hosseini, Mr. Ali Aziz-Khani, and Ms. Atiyeh Razzazi who coordinated the surveys in Semnan and Qazvin provinces.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the UNICEF office in IRAN under the cooperative agreement with NNFTRI for the research.