
Abstract
Background:
The World Health Organization recommends daily iron and folic acid (IFA) supplementation during pregnancy, but consumption remains low, and high prevalence of anemia among pregnant women (PW) persists.
Objectives:
This study aims to (1) examine factors at the health system, community, and individual levels, which influence adherence to IFA supplements; and (2) describe a comprehensive approach for designing interventions to improve adherence based on lessons learned from 4 country experiences.
Methods:
We conducted literature search, formative research, and baseline surveys in Bangladesh, Burkina Faso, Ethiopia, and India and applied health systems strengthening and social and behavior change principles to design interventions. The interventions addressed underlying barriers at the individual, community, and health system levels. Interventions were further adapted for integration into existing large-scale antenatal care programs through continuous monitoring.
Results:
Key factors related to low adherence were lack of operational protocols to implement policies, supply chain bottlenecks, low capacity to counsel women, negative social norms, and individual cognitive barriers. We reinforced antenatal care services and linked them with community workers and families to address knowledge, beliefs, self-efficacy, and perceived social norms. Evaluations showed that adherence improved in all countries. Based on implementation lessons, we developed a program pathway and details of interventions for mobilizing health systems and community platforms for improving adherence.
Conclusion:
A proven process for designing interventions to address IFA supplement adherence will contribute to achieving global nutrition targets for anemia reduction in PW. This evidence-based comprehensive approach may be applied in other countries with high anemia prevalence and low IFA adherence.
Plain language title
Designing Comprehensive Interventions to Improve the Consumption of Prenatal Iron and Folic Acid Supplements in Low- and Middle-Income Countries
Plain language summary
Anemia among women of reproductive age, particularly during pregnancy, is widespread, but there are remedies such as iron and folic acid (IFA) supplements that can increase iron intake. This study documents the barriers faced by pregnant women (PW) in adhering to daily IFA supplementation as recommended by the World Health Organization. We designed interventions for large-scale antenatal care programs to improve adherence in Bangladesh, Burkina Faso, Ethiopia, and India. The barriers included poor supplies, lack of counseling during antenatal visits, and insufficient community and family support for PW. We strengthened service delivery protocols and the capacity of community workers to engage families. We trained health workers, improved supervision and counseling quality, strengthened supply systems for IFA tablets, and facilitated family support for PW. We improved women’s knowledge, beliefs, self-efficacy, and perception of social norms through interventions tailored for each country setting. Considering the high burden of anemia in low- and middle-income countries among women especially during pregnancy and health consequences for mothers and newborns of low iron intake, decision makers and implementers need to pay greater attention to understanding local barriers to adherence and designing interventions that can improve adherence. Social and behavioral science theories and health systems strengthening frameworks provide a strong technical basis for designing effective interventions to improve IFA adherence.
Keywords
Introduction
Globally, an estimated 36% of pregnant women (PW) are affected by anemia, with the highest levels documented in South-East Asia (48%) and Sub-Saharan Africa (46%). 1 The etiology of anemia is complex, and iron deficiency is considered a major factor. 2 Iron deficiency is the most common micronutrient deficiency in pregnancy with negative impacts on maternal and newborn health, including increased risk of maternal mortality, reduced work capacity in women, and impaired cognition and immune function in infants. 3 Iron demand rises in pregnancy to meet the needs of the growing fetus, expansion in blood volume, and to build iron stores for rapidly replacing red blood cells lost during childbirth. 4 Diet alone cannot meet the high need for iron, and PW need to consume supplemental iron to fill dietary gaps. 5,6
Oral supplementation with iron-containing products is currently the most widely used intervention for PW. 2 A daily supplement of iron and folic acid (IFA) containing 30 to 60 mg of elemental iron and 400 µg of folic acid during pregnancy has been shown to reduce maternal anemia and low birth weight 7,8 and has been recommended by the World Health Organization (WHO) for over a decade. 9,10 However, national health authorities and service providers have not consistently implemented this recommendation. While most countries have antenatal care (ANC) guidelines on IFA supplementation and IFA supplies are included in essential drugs lists for ANC services, 11 nationally representative Demographic and Health Surveys suggest that coverage of IFA supplementation remains low. Low iron intake in women due to the lack of IFA adherence is considered an impediment to global progress in reducing maternal anemia. 2
The overall level of IFA adherence across South-East Asia and Sub-Saharan Africa countries is low, and not even one-third of the countries in Africa have adherence rates higher than 50%, and in another review of 22 countries, in only 2 countries, the percentage of PW consuming 180 or more tablets exceeded 30%. 12,13 According to recent Demographic and Health Surveys (DHS), at least 90 IFA tablets were consumed by only 28% of PW in Mali, 30% in Nigeria, 39% in India, 42% in Ethiopia, and 46% in Bangladesh. 14 Large operational gaps in IFA interventions have been reported, including inconsistent supplies of IFA, inadequate health provider skills and tools to provide high quality counseling, insufficient emphasis on community and family engagement, and poor recognition of anemia and its serious risks. 11 The counseling provided during ANC visits does not address individual factors in PW that contribute to nonadherence. 12,15 The existing literature on IFA adherence provides insights on barriers and factors associated with adherence, 12,16 -19 but there are only a few studies with empirical evidence on the effectiveness of adherence interventions in the context of large-scale ANC services. 20,21 The WHO recommends that more investments be made to better understand how adherence can be improved for all long-term self-administered oral therapies. 22
In previous randomized controlled trials, we demonstrated how a multipronged approach to integrating a package of interventions and ANC uptake resulted in earlier and more ANC contacts and improved practices, including higher IFA consumption. 23 -25 In this article, we examine the steps in the process of designing and operationalizing the IFA adherence interventions by synthesizing and reporting on published and unpublished work, including implementation research in 4 countries. Specifically, we examined factors at the health system, community, and individual levels influencing IFA adherence and described the technical basis for designing adherence interventions and operational details of IFA adherence interventions.
Methods
We extracted information from published and unpublished studies and reports on IFA adherence barriers, designing of IFA adherence interventions, operational strategies, and monitoring approaches related to IFA adherence. The information was organized and documented to provide evidence on how to improve IFA adherence. We describe how we used a mixed-methods approach for identifying barriers and enablers of IFA adherence, developed a program pathway, and how we followed a systematic process for designing interventions in 4 diverse countries. Our work on IFA adherence is part of a broader set of previously completed implementation research studies on the integration of maternal nutrition packages in ANC services that included dietary improvement, weight gain monitoring, counseling on breastfeeding, and IFA and calcium supplementation. 11 We extracted information on IFA adherence from reviews of existing studies and from previously conducted situational analysis, formative research, and household and provider surveys in Bangladesh, Burkina Faso, Ethiopia, and India to identify strengths and weaknesses in IFA adherence activities in ANC. We grouped the influencing factors according to the Socio Ecological Model of behavior change 26 by various levels of influence: health system, community, and individual. To shape IFA adherence interventions for each level, we applied health systems strengthening 27 and social and behavioral science theories and frameworks proven to work in health promotion programs. 22,28,29 We tailored interventions to the national guidelines, national ANC program structures, and community contexts.
Factors Influencing IFA Adherence
We conducted a literature review of publications in PubMed and obtained unpublished reports from researchers and program implementers in each country. Search terms used were as follows: (adher* OR comply OR complian*) AND (pregnan* OR prenatal) AND (IFA OR IFAS OR “iron and folic acid” OR “iron with folic acid” OR “iron-folic acid” OR “iron folic acid”) AND Bangladesh OR Burkina Faso OR Ethiopia OR India. We also conducted the search without any geographic specifications. We excluded studies on micronutrient powders, iron-only and folic acid-only supplements and intermittent IFA supplementation, refugee camps, and descriptions of forthcoming clinical trials and studies with no results. The final set of references included studies published during 2010 to 2022 that measured adherence and described interventions and program contexts, with full-text availability in the English language.
Process of Designing IFA Adherence Interventions
Methods used to design the interventions were based on gaps identified in ANC service delivery and barriers to the consumption of IFA. We describe the processes used and rationale for selecting what to prioritize while developing packages of activities for each country context.
Situational analysis
The WHO’s health systems building blocks provided a structured construct for assessing relevant IFA-related components of the health system (eg, policies and protocols, supply system, provider capacity, information system). 30,31 In each country, we mapped the existing ANC services related to IFA supplementation and reviewed quantitative and qualitative studies on IFA adherence. 32 -34 The quantitative studies provided information on patterns of IFA procurement and consumption, and the timing and magnitude of shortfalls in IFA consumption over the course of pregnancy. 11 Qualitative studies provided the intervention design team with insights on what motivated PW to consume or avoid IFA and their perceptions about anemia and IFA supplements, how and where they obtained IFA supplements and the difficulties they encountered, and support provided by family members; and side effects (unpublished data). We also documented health manager perceptions, 35 PW interactions with ANC providers, and the knowledge of family members and peers in the community on anemia and IFA topics. Supply chain assessments identified the frequency, magnitude, and level where bottlenecks were occurring (unpublished data). Surveys of frontline health workers identified gaps in knowledge, challenges in counseling on IFA, and lessons learned for ANC services.
Interventions
We strengthened the delivery and uptake of prevailing government protocols for IFA supplementation in ANC by focusing on adherence. The Ministries of Health in 3 countries recommended 180 days and in 1 country (Ethiopia) “at least 90 days” of IFA supplements containing 60 mg iron was recommended. We referred to 90 days as a minimum for assessing compliance and as it is often the cutoff measured in national surveys. We designed IFA adherence interventions according to social and behavioral science principles and frameworks commonly used in health promotion programs and health systems building blocks. The Socio Ecological Model of behavior change emphasizes synergies among multiple zones of influence from individual, family, and community to health systems and policies. 36,37 Theories on what drives individual behaviors deepened our understanding of how to structure interventions for behavior modification in individuals. 22,29 For example, intentions are highlighted as the immediate precursors of behavior, and intentions are a function of knowledge and attitudes toward the recommended behavior that develop from past experience or learned from influential persons, as well as perceptions of social norms and ability to perform the recommended action or self-efficacy. 38 -40 Additionally, we reviewed approaches used for improving adherence to other drugs used for long-term adult chronic conditions, such as cardiovascular disease, hypertension, and diabetes. 22,41 The information showed that to reduce barriers to PW adherence to IFA, we needed to reduce knowledge gaps, strengthen favorable beliefs about the benefits of IFA, improve convenience and lower side effects, generate perceptions about social norms, and build self-confidence in being able to complete IFA doses.
Operational specifications
The interventions required detailed specification of protocols for tasks and tools to direct ANC managers, health providers, supervisors, and community workers. Formative studies and field tests provided feasibility checks for implementation, acceptability, and local relevance (unpublished data). National, regional, district, and community stakeholders added their perspectives on replicability and sustainability of the intervention packages through participatory co-designing processes. The ANC providers, community workers, PW, husbands, and community and other family members pretested the tools and materials.
Monitoring-based modifications
During implementation, interventions and operational details were modified as additional needs were identified, and further adjustments were made in response to monitoring, supervision, and assessments, particularly during the early stages of scaling up. For example, in Ethiopia, the implementers needed a “tracker” tool for PW so that women and providers at different venues had a complete picture of the timing and content of services received (eg, the number of IFA tablets, counseling on IFA adherence) from different ANC sites. We conducted additional focused assessments to supplement routine monitoring as needed, for example, when important indicators were missing in routine monitoring and supervision tools. For example, in Burkina Faso, we used exit interviews with ANC clients to determine the quality of counseling and IFA received and identified low performing health facilities for extra support. In Ethiopia, we assessed the status of service provision and need for extra training and supplies after ANC services resumed following COVID restrictions. In Bangladesh, we conducted rapid checklist-based household interviews to follow up on coverage gaps in lagging subdistricts. All primary data collection for research involving human subjects referenced in this article received ethical approval and informed consent.
Results
Factors Influencing IFA Adherence
We identified multiple published studies and systematic reviews on IFA adherence and related factors and conducted our own baseline surveys and formative research to adapt interventions. The studies used a range of methods, such as systematic review, 16,21 secondary analyses of nationally representative DHS surveys, 12,13 large-scale primary surveys, 33 in-depth interviews, focus group discussions, exit interviews, and observations of counseling sessions (unpublished data). The measurement of adherence was based on interviews with recently delivered or PW in most studies. Several studies measured adherence using self-reported total number of tablets consumed during the last or current pregnancy, while others used the criteria of 2 missed doses in the preceding 7 days as a measure of nonadherence. We categorized adherence factors for IFA supplementation into health systems level, community level, and individual level (Table 1).
Summary of Facilitators and Barriers of Adherence to IFA Supplementation in Pregnancy.
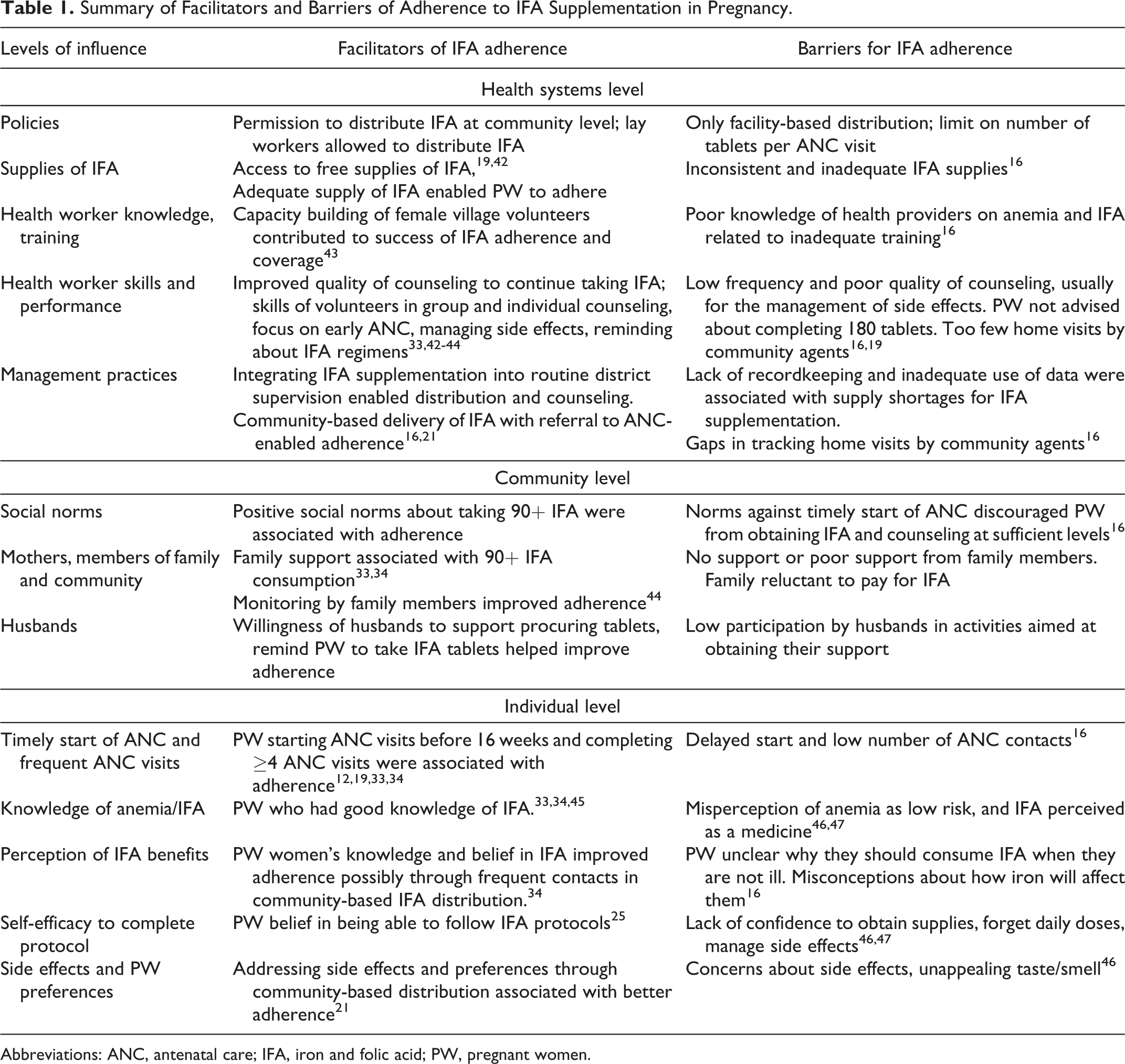
Abbreviations: ANC, antenatal care; IFA, iron and folic acid; PW, pregnant women.
Health system level
In each country, the priority areas that needed health system strengthening varied; health worker survey data, observations of ANC contacts, co-design workshops, and discussions with field managers were used to set priorities. Facilitating factors included policies that increased access of PW to supplies and frequent counseling on adherence by allowing community-based distribution and use of community volunteers and workers to distribute IFA; and flexibility for adjusting the number of tablets to meet the needs of individual PW. Other key factors were maintaining supply and distribution records, tracking adherence, and using the data to address gaps in number of tablets consumed. 11 Factors that limited PW access to adequate number of IFA doses included restrictive policies such as IFA tablets provided only at health facilities but not through community outreach, IFA distribution not permitted by trained lay workers, and not providing free IFA. 11,16,21 Studies reported difficulties due to disruptions in IFA supply chains due to inaccurate estimation procedures, delayed requisition, and regional/district as well as local transportation bottlenecks. 11 Inadequate counseling on IFA adherence was reported frequently in studies, including not explaining the dangers of anemia for mothers and newborns, not specifying the daily and monthly dosing schedule, and not helping to address forgetfulness and how to reduce or manage side effects. 12,44,48
Community level
The content of country-specific activities varied and types of approaches were based on household surveys, qualitative studies, field testing of counseling materials, and field discussions with community workers and family members. Social norms associated with gender inequalities, superstitions, taboos, and lack of information were barriers for PW to access health services and follow health recommendations to adhere to IFA protocols (Table 1). The norms were associated with delayed start and infrequent ANC, restrictions such as needing to be accompanied to ANC sessions by a male family member, not being permitted to interact with certain caste or ethnic groups at ANC sites, discouraging consumption of “medicines” in pregnancy, misperceptions about anemia symptoms being “normal” for PW, and lack of belief in the importance and effectiveness of IFA supplements. 16,21,46 Patterns of ANC use affected the total number of IFA tablets obtained and opportunities for problem-solving such as for side effects. In Bangladesh, multivariate analysis showed that PW who started ANC in the first trimester consumed 26 more IFA tablets during pregnancy 34 ; in Burkina Faso, starting ANC in the first trimester was associated with 1.5 times higher odds of consuming 90+ IFA tablets, and 4 or more ANC visits was associated with 10 times higher odds . Husband’s assistance and the perception of family support, for example, having someone facilitate IFA procurement and reminding about daily doses, were important. 42 In Bangladesh, we estimated that women who reported elevated level of husband’s support consumed 25 more IFA tablets. 34
Individual level
Surveys of recently delivered women and PW, focus group discussions with PW, and exit interviews with ANC users provided the basis for selecting the priority contents of activities for PW in each country. Key barriers associated with low IFA adherence at individual level include lack of knowledge of anemia and its dangers for women’s and children’s health, low belief in the effectiveness of IFA, not knowing the doses and protocols or how to manage side effects (Table 1). Findings from a previous study in Bangladesh showed that PW with high knowledge scores would consume 31 more tablets in pregnancy compared to PW with low scores. 34 Low self-confidence among PW in procuring adequate supplies, remembering the daily dose, and managing side effects was reported as important factor for IFA adherence. 33,34,44,49,50 In India, the number of IFA tablets were projected to increase by 1.5 times if women had high self-efficacy. 33 In Burkina Faso, the perception of supportive social norms and family support among PW were associated with about 2 times higher IFA adherence. 34
Interventions
In all countries, ANC providers and health managers implemented multiple interventions to address both the supply-side (provision) and the demand-side (utilization) barriers of IFA adherence. For example, supply disruptions were addressed through training on improved estimation of requirements, timely requisitions from storage hubs, including inspection of stocks in supervision, and better tracking of logistics records. Provision of counseling on IFA adherence was strengthened through multiple training and supervision rounds for ANC providers and community health workers, clear and concise illustrated job aids with key points to be covered, and recognition of good counseling performance by frontline workers. To manage work overload, tasks such as IFA distribution and counseling on IFA were distributed among ANC providers and community health workers (task-shifting). Demand-side barriers were addressed through focusing on the underlying drivers of PW adherence behaviors such as knowledge on the protocol to be followed and where and how to obtain IFA; belief in the dangers of anemia and efficacy of IFA; self-efficacy (by extending counseling to family members and obtaining their support for PW IFA procurement and reminders, and by teaching PW how to manage side effects); and encouraging social norms favoring IFA adherence through community activities. Figure 1 illustrates the pathway to improved adherence by intervening at multiple levels. Our study showed that the same categories of interventions were needed across countries, but the details and relative importance of interventions varied (Table 2). These findings emphasize the need to understand the underlying drivers of adherence and the strengths and gaps in program platforms in different settings. For example, supply chain bottlenecks can be at the point of requisition, or distribution sites, or at the regional warehouse or national level. Similarly, health staff can generate family support from mothers and mothers in law if husbands are difficult to access in some settings; and tracking approaches and tools for IFA tablets obtained and consumed by PW may vary.
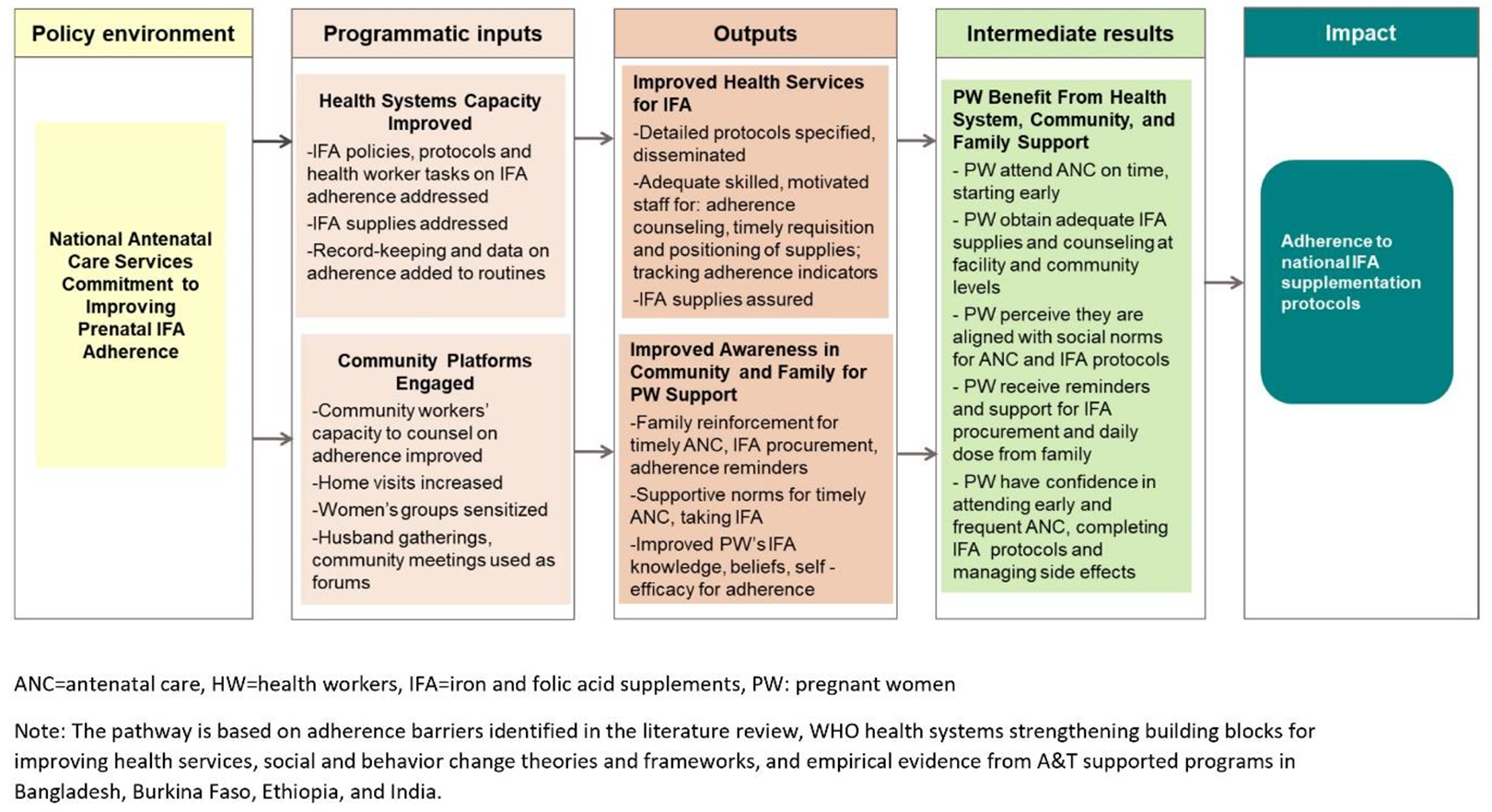
Program pathway for improving adherence to iron and folic acid supplementation. The pathway is based on adherence barriers identified in the literature review, World Health Organization health systems strengthening building blocks for improving health services, social and behavior change theories and frameworks, and empirical evidence from A&T supported programs in Bangladesh, Burkina Faso, Ethiopia, and India. ANC: antenatal care, HW: health workers, IFA: iron and folic acid, PW: pregnant women.
Content of IFA Adherence Interventions Integrated Into ANC Services in Bangladesh, Burkina Faso, Ethiopia, and India.
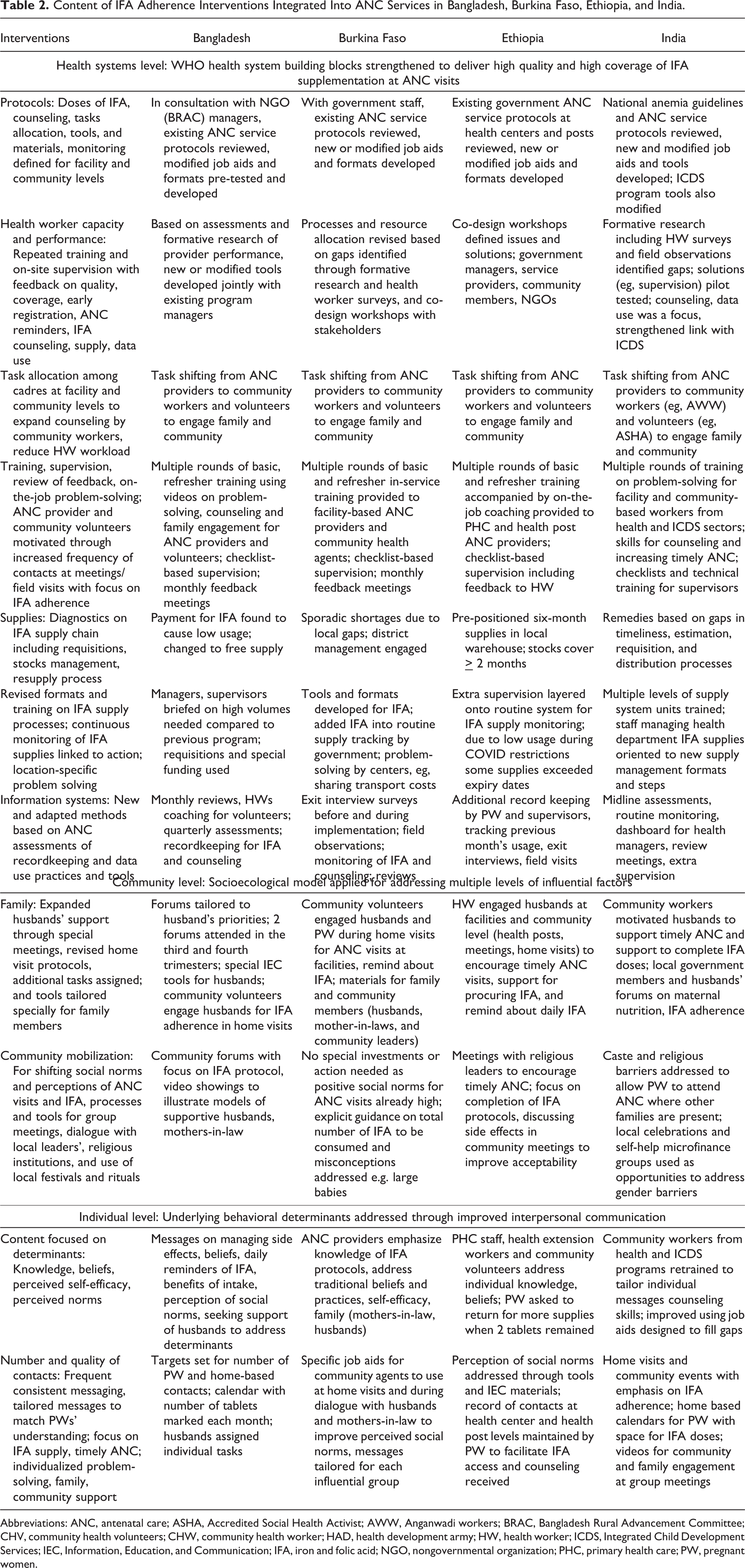
Abbreviations: ANC, antenatal care; ASHA, Accredited Social Health Activist; AWW, Anganwadi workers; BRAC, Bangladesh Rural Advancement Committee; CHV, community health volunteers; CHW, community health worker; HAD, health development army; HW, health worker; ICDS, Integrated Child Development Services; IEC, Information, Education, and Communication; IFA, iron and folic acid; NGO, nongovernmental organization; PHC, primary health care; PW, pregnant women.
Health services delivery
The early start and consistent provision of IFA supplements and high-quality counseling are critical for facilitating adherence to IFA protocols. The interventions needed to strengthen these components of health service delivery required development of specific protocols, health worker knowledge and performance improvement, building sturdy supply chains for IFA supplements, and functioning information systems to detect problems and identify solutions early.
Managers needed detailed protocols to oversee adequate doses of IFA, counseling quality and frequency, task allocation among facility and community workers, record keeping and the use of data. Health managers needed to fix and clearly communicate targets for the total number of IFA tablets per pregnancy in Burkina Faso, India, and Ethiopia. Trainers and supervisors focused on adherence during facility, community group meetings, and home visits.
Improving health worker capacity through basic and refresher training and monthly meetings emphasized maintenance of supplies at ANC sites, distribution and recording of correct amounts, and counseling on adherence, including seriousness of anemia and managing side effects. Health workers emphasized the importance of timely start of ANC, and they advocated for family/community support to increase the number of visits.
The pattern of supply bottlenecks showed the importance of ongoing diagnostics for maintaining IFA supply chains, timely requisitions, stock management, resupply, and distribution processes. In India for example, strengthening logistics management formats and training of warehouse and pharmacy staff was key. In Ethiopia and Burkina Faso, frequent field checks of IFA supplies by district and health center staff led to timely remedial action.
Information systems were inadequate for detecting and addressing IFA adherence and required new and adapted tools and methods. Higher level health managers needed data to act on bottlenecks. In Burkina Faso and India, we added indicators and pages to existing registers for tracking adherence. When needed, we collected supplementary data through service provision assessments (Ethiopia), exit interviews (Burkina Faso), and rapid mini surveys using checklists (Bangladesh).
Community and family engagement
Our multivariable analysis and qualitative studies validated the socioecological model of behavior change that highlighted the importance of an enabling environment at multiple levels for PW adherence to IFA. In India and Bangladesh, the teams strengthened the role of family members, especially husbands’ support for procuring IFA tablets and reminding about daily doses. The situational analysis identified gaps in utilizing existing opportunities to engage husbands or other family members to help PW. In Bangladesh and India, community mobilization managers assessed the feasibility of special husbands’ meetings. Bangladesh had a history of using this approach and specified the frequency and content of meetings where community managers would discuss IFA adherence. In Burkina Faso, India, and Ethiopia, managers revised home visit protocols to engage a more family members. Teams in Bangladesh and Burkina Faso tailored special tools for family members to facilitate dialog.
We linked ANC providers to community institutions to reach influential persons for removing barriers to timely ANC visits and adherence to IFA protocols. Village health committees in India and religious leaders in Somali region of Ethiopia are examples of entities who engaged in dialogue with health providers and families. In each country, we developed tailored processes and tools for local leaders,’ religious institutions, and family members. Ethiopian health authorities facilitated timely start of ANC visits and frequent contacts by decentralizing ANC services to health posts.
Individual support for PW
The content of interventions for improving PW adherence did not stop at information regarding the use of supplements but on addressing a range of knowledge gaps (eg, risk of maternal mortality and low birth weight, number of tablets, and how to reduce and manage side effects), perception of social norms about when to start ANC visits, and self-efficacy or confidence in being able to complete the protocol with the family’s help. In Bangladesh, mothers had knowledge of 180 tablets, but not of the seriousness of low iron for PW and newborns; they also needed more husbands’ support and frequent ANC contacts. In Burkina Faso, the knowledge that 180 tablets should be taken during pregnancy was not known by health workers and women.
The means of delivering key content and building confidence among PW relied on face-to-face counseling by ANC providers and community workers aided by visual communication materials, and group meetings in all countries. Encouraging frequent contacts during pregnancy was a key element of interventions. Service delivery managers facilitated this through decentralized provision of ANC at health posts in Ethiopia and monthly community outreach sessions in India. Frontline workers needed to expand coverage and raise the frequency of contacts per PW, and they followed revised home visit routines and protocols in Bangladesh, Burkina Faso, and Ethiopia. In India, Integrated Child Development Services (ICDS) workers were trained and equipped to counsel of IFA adherence during home visits and community group meetings.
Discussion
We aimed to identify factors influencing IFA adherence and document a comprehensive process for designing locally adapted interventions to improve adherence using a balanced package of supply-side and demand-side interventions. Our findings on adherence barriers highlight operational management and community factors for the first time while being consistent with previous studies on the importance of IFA supplies and counseling to address knowledge gaps. 12,15 -17,21 At the health system level, our intervention studies showed that key factors included specifying IFA supplementation protocols and how health workers needed to help PW remember the protocols, need for monitoring indicators to include tracking of operational bottlenecks, gaps in providers’ counseling skills and motivation to counsel PW, lack of suitable counseling tools, and building capacity among health workers in engaging families to improve IFA adherence. We found that social norms about timing and frequency of ANC visits and community understanding of anemia risks and belief in benefits of IFA were important. Counseling of PW should focus on individual-specific knowledge and perceptions about the effectiveness of IFA, self-efficacy in completing the protocol, and how to manage side effects. Our interventions focused on 6 key action areas: (a) timely attendance at ANC starting in the first trimester; (b) routine tracking and follow-up of individual PW adherence; (c) health personnel knowledge and performance of IFA adherence tasks including IFA distribution and counseling, supply management, and monitoring supplies, coverage of counseling, and adherence; (d) community factors such as social norms that support timely ANC and completion of IFA protocols; (e) engagement of family members to facilitate PW attendance at ANC sessions, help to maintain IFA supplies at home, and remind PW about doses; and (f) adequate knowledge, beliefs, and self-efficacy in PW to complete the recommended IFA doses.
Our findings align with studies on adherence to other long-term oral therapies and highlight the multiple adherence barriers that need to be addressed through a comprehensive set of activities. 22,41,51 Findings from other IFA adherence studies and other therapies also reported the importance of frequent health system contacts and access to supplies, 12,13,16 individualized communication on adherence concerns, 32,34 an enabling social environment, 43,46 and patient self-efficacy. 21,34,46 The relative importance of health system, community, and individual factors can vary by health system characteristics, patient attributes (such as health condition and family/living environment), and characteristics of the medication/supplements. 12,16,50,51
We documented how IFA adherence programs in 4 low- and middle-income countries (LMICs) responded to the prevailing strengths and weaknesses of existing ANC services and prioritized relevant factors based on assessments and formative studies and used evidence-based frameworks. 49,52,53 Although countries aligned their ANC guidelines with global recommendations on IFA supplementation prior to intervention, we noted gaps in implementing them effectively. 11
Supply-side health system elements have dominated the literature on IFA adherence frameworks and interventions. 12,15,16 Our intervention packages also focused on detailed policies and protocols, ANC provider performance of IFA distribution and counseling functions, IFA supply logistics (eg, estimating needs, arranging local transportation to ANC sites), and information systems (eg, tracking adherence indicators and intensifying data use by program managers). Health systems strengthening was done at multiple levels based on the type of improvements needed. In India at state level and in 2 districts, in 2 regions each in Ethiopia and Burkina Faso, and in 4 districts in Bangladesh. Our findings are consistent with experiences related to other long-term drug therapies; both noted the importance of regular follow-up with the healthcare system, delegating services to community levels for proximity to clients, and recordkeeping to track adherence. 22,41,51,52 Both types of drug adherence (IFA and other long-term therapies) require client education, frequent reminders, and lowering economic barriers. Both also need to improve standard measurements of adherence and routine tracking of adherence trends in clinical and public health programs. 11,41 Tracking supplies, restocking, and utilization data from the point of service may be proxies for adherence trends.
Demand-side factors were equally important in explaining IFA adherence in our programs. Effective IFA supplementation depends upon a daily self-administered protocol. Even if supplies are sufficient and health workers provide counseling to individual PW, community, household, and individual factors influence consumption of the daily IFA dose. We aimed to improve the relevance of solutions from PW perspectives, including their recognition of risks, fears, and misperceptions regarding IFA which led to practical, do-able options for resolving adherence difficulties. Our programs leveraged community platforms such as government community health agents in Burkina Faso, health extension workers in Ethiopia, ICDS workers in India, and nongovernment organization community health volunteers and husbands’ forums in Bangladesh. 11 This emphasis on strengthening community platforms and their links to the ANC health system is consistent with theoretical models of behavior change and lessons learned from successful IFA supplementation programs in other similar settings. 43
Our evaluation results validate our approach. The evaluations applied cluster randomized study designs after implementing the interventions for 7 to 18 months in Bangladesh, Burkina Faso, Ethiopia, and India. Process indicators showed better ANC utilization, coverage of IFA adherence services (IFA tablets and counseling provided), PW belief in benefits of IFA, and family support. 24,25 The proportion of PW attending 4 or more ANC sessions increased in 3 of 4 countries and ranged from 69% to 91% at end-line; coverage of counseling on IFA adherence ranged from 87% to 95%; PW perceptions of IFA benefits to prevent anemia and improve newborn health improved in all countries; and PW in 3 of 4 countries reported family members’ support in procuring IFA tablets and reminding them about the daily IFA doses. Pregnant women consumed on average of 139 tablets in intervention areas compared to 94 in noninterventions areas at end line in Bangladesh, 133 compared to 115 in Burkina Faso, 125 compared to 101 in Ethiopia, 60 tablets compared to 54 in India.
Other programs that apply our program pathway should be guided by formative studies and implementation research to adapt this approach. Our pathway shows that health systems, community, and individual level barriers need to be addressed by program planners collectively and the pathway builds on previously proposed IFA pathways. 2,12,16 It also presents a balance of interventions not focused exclusively on individual PW limitations but also on their larger environment and proposes building their capacity as well as self-efficacy and family support for managing constraints. Successful programs such as in Nepal, 43 implementation research in Uganda, and our recent Bangladesh, Burkina Faso, and Ethiopia programs 11 are examples of what can be achieved when the factors shown in our pathway are systematically incorporated into IFA adherence strategies and implemented diligently within ANC programs. Changes in social and economic conditions of communities, access to health services, education levels, and other drivers of behavior require ongoing tracking of determinants to maintain a focus on the most important barriers and the relevance of solutions for sustaining impacts on adherence. 21,43,46,54 Although the intervention design process developed by us is relevant for LMIC settings, we took into consideration experiences reported by researchers on other long-term drug therapies from developed countries, thus findings may also apply to other initiatives aimed at improving adherence behaviors.
Conclusions
Our article documents in detail how a contextualized set of activities for improving IFA adherence was designed, based on program experiences in 4 countries. Our program pathway is evidence based and illustrates how ANC programs can apply specific social and behavioral science theories and principles of health systems strengthening to address supply-side and demand-side factors comprehensively. The approach can facilitate achievement of global nutrition targets for anemia reduction.
Footnotes
Authors’ Note
All primary data collection for research involving human subjects referenced in this article received ethical approval and informed consent. We do not require ethical approval for this study as it used data from existing reports and articles. All studies included in the article declared prior clearance from ethical review boards.
Author Contributions
Conceptualization, T.G.S., P.H.N., T.F. and S.S.K.; methodology, T.G.S., P.H.N., S.S.K.; data curation, T.G.S., P.H.N., S.S.K.; writing – original draft preparation, T.G.S.; writing -review and editing, S.G., Z.M., T.W., and M.Z.; supervision, T.G.S., P.H.N., S.S.K. All authors have read and agreed to the final submitted manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Bill & Melinda Gates Foundation (grant number: OPP1135090) supported this study in whole or in part through Alive & Thrive, managed by FHI Solutions. Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission.