
Abstract
Background:
B vitamins may have beneficial roles in reducing inflammation; however, research on the role of B vitamins in inflammation among HIV-infected persons is lacking.
Objective:
This study assessed the association between B vitamins and serum C-reactive protein (CRP) concentrations in HIV-infected persons.
Methods:
A cross-sectional survey was conducted among 314 HIV-infected persons (180 men and 134 women) aged 18 to 60 years residing in the Kathmandu, Nepal. High-sensitive and regular serum CRP concentrations were measured by the latex agglutination nephelometry and latex agglutination turbidimetric method, respectively. Dietary intake was assessed using 2 nonconsecutive 24-hour dietary recalls. The relationships between B vitamins and serum CRP concentrations were assessed using multiple regression analysis.
Results:
The multivariate-adjusted geometric mean of serum CRP concentrations was significantly decreased with an increasing B vitamins intake across quartiles of niacin (P for trend = .007), pyridoxine (P for trend = .042), and cobalamin (P for trend = .037) in men. In men, the mean serum CRP concentrations in the highest quartiles of niacin, pyridoxine, and cobalamin were 63%, 38%, and 58%, respectively, lower than that in the lowest quartile. In women, the mean serum CRP concentrations in the highest quartiles of riboflavin (P for trend = .084) and pyridoxine (P for trend = .093) were 37% and 47%, respectively, lower than that in the lowest quartile.
Conclusion:
High intake of niacin, pyridoxine, or cobalamin was independently associated with decreased serum CRP concentrations among HIV-infected men. Further prospective studies are warranted to confirm the role of B vitamins in inflammation among HIV-infected persons.
Introduction
In human body, B vitamins may reduce inflammation due to its enzymatic reactions in metabolizing amino acids, neurotransmitters, nucleic acids, and lipids including homocysteine. 1 –9 For example, B vitamins enzymes, such as methylene tetrahydrofolate reductase and flavin mononucleotide (coenzyme of riboflavin) and cystathionine-B-synthase and y-cystathionase (pyridoxal phosphate–dependent enzymes) are involved in the conversion of homocysteine to methionine and cysteine. 2, 3 Thus, decreased intake of B vitamins increases the accumulation of homocysteine. 1, 5 –9 An increasing level of homocysteine seems to promote inflammation by producing interleukin 6 (IL-6) by monocytes and endothelial cells. 10, 11 Moreover, pyridoxine is essential for cytokine production as well as for lymphocyte proliferation and activation that may characterize the response of inflammation. 12 –15 Similarly, folate may reduce inflammation due its beneficial effects in scavenging free radicals and reactive oxygen species and in lowering cholesterol and blood pressure that are associated with reducing inflammation. 16
A growing body of evidence supports the protective action of B vitamins in reducing inflammation in patients with inflammatory diseases 17 –20 and general populations. 21 –23 In the National Health and Nutrition Examination Survey 24 (NHANES) and the Framingham Heart Study, 24 pyridoxal 5’-phosphate (PLP), the active form of pyridoxine, was inversely associated with the inflammatory marker C-reactive protein (CRP). The beneficial effect of pyridoxine against inflammation was reported in other observational studies done among patients with inflammatory conditions such as rheumatoid arthritis, 18 inflammatory bowel disease, 19 or coronary disease. 25 –29 In an intervention study among patients with stable angina pectoris, pyridoxine treatment was negatively associated with CRP and other inflammatory markers. 26 Similarly, serum folate concentrations were inversely associated with CRP among pregnant women of South Korea. 30 In the same study, the beneficial effect of increased intake of riboflavin and pyridoxine was observed in reducing serum CRP concentrations in pregnant women.
Though studies have been done in the general population 21 –23 and in patients with inflammatory conditions, 17 –20 the relation of B vitamins with inflammation has not been investigated in HIV-infected persons. Chronic inflammation is a key process in HIV infection due to the chronic activation of adaptive and innate immune systems. 31 –35 The CRP has been shown to be an independent predictor of survival as it has been associated with multiple parameters of disease progression in HIV infection. 36,37 Among them, B vitamins deficiency is common due to malabsorption, diarrhea, impaired storage, and altered metabolism. 38 –43 Studies have shown that serum folate concentrations were independently associated with hyperhomocysteinemia in HIV-infected persons. 44, 45 The chronic inflammatory conditions in HIV infection possibly increase the use and metabolic turnover of B vitamins due to its greater involvement in the pathway of homocysteine remethylation to methionine. 2,3 As B vitamin deficiencies are common in HIV-infected persons along with inflammation, it is possible that dietary intakes of B vitamins have an effect on the inflammation process of HIV-infection.
Therefore, the aim of this study was to explore the relationships between B vitamins and serum CRP concentrations in persons infected with HIV while accounting for important HIV-related clinical and other confounders including antiretroviral therapy (ART). As B vitamins have a potential benefit in inflammation, it is hypothesized that lowering intake of a B vitamin is associated with increased serum CRP concentrations in HIV-infected persons.
Methods
Study Design and Setting
The present cross-sectional analysis used baseline data of a longitudinal healthy living study entitled “Positive Living with HIV (POLH)” conducted from February to March 2010. This study was conducted among HIV-infected persons living in Kathmandu, Lalitpur, and Bhaktapur districts of Kathmandu Valley, Nepal. The prevalence of HIV infection was particularly high among risk population groups for example injecting drug users (IDUs) (6%), female sex workers (4%), men who have sex with men (4%), and male labor migrants to India (2%). 46 The prevalence of HIV infection was 0.3% in the general population in Nepal.
Study Participants
The study procedures have been reported in detail elsewhere. 47 –51 Participants were recruited through the network of 5 nongovernment organizations (NGOs) working with HIV-infected persons in the Kathmandu Valley. Five different NGOs were providing need-based care and support services to HIV-infected persons in the Kathmandu Valley during the study period including weekly HIV clinics, CD4+ T-cell count monitoring, and home delivery of ART to needy persons. Altogether 322 HIV-infected persons, aged between 18 and 60 years, participated in the study voluntarily with their written informed consent. None of the participants reported receiving either vitamin or mineral supplementation in past 12 months. The study protocol followed the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Ethics Committee of the Nepal Health Research Council, Kathmandu, Nepal; National Center for Global Health and Medicine, Japan; and Waseda University, Tokyo, Japan. The study procedures were also approved by the institutional review board of the University of Massachusetts, Amherst, USA.
Outcome Measure
After an overnight, fasting blood samples were obtained from 322 participants during the survey period. About 10 mL of venous blood were drawn into an evacuated tube and centrifuged immediately for 15 minutes to separate the serum samples. The serum samples were transported to a local laboratory in Kathmandu by placing them in a cooler box with dry ice and were stored at −80°C in the same laboratory during the field work. After completion of the field work, the collected serum samples were transported with dry ice to a research laboratory in Tokyo, Japan, and were stored at −80°C until analysis. One tube of 2.0 mL was sent to an external laboratory (Mitsubishi Chemical Medience Corporation, Tokyo, Japan) for testing, where high-sensitive serum CRP concentrations and regular serum CRP concentrations were measured by the latex agglutination nephelometry method and latex agglutination turbidimetric method, respectively. The latex agglutination turbidimetric method was used to measure the regular serum CRP concentrations of those participants whose CRP value was 5 mg/L or more. The intra-assay coefficient of variation at CRP levels on the control serum was within 10%. Blood samples were drawn from mid-February to mid-March, so seasonal variation or difference in freezing time should not have significant effects on serum CRP concentration levels.
Dietary Assessment
The dietary intake was calculated from two 24-hour dietary recalls 1 week apart and on different weekdays. Trained person was hired to collect detailed information on all food and beverages consumed by participants in 24 hours. Real food samples and pictures of commonly eaten food and recipes were used to collect detailed information on food preparation methods. Locally available standard spoons, glasses, bowls, and food models, and diet measurement scale were used to measure the portion size of food. The daily intakes of B vitamins were calculated using Indian food tables from the Wfood2 program version 1.0 (Berkeley, CA, USA). 52 The intake of B vitamins was adjusted for energy intake using the nutrient density method calculated by dividing nutrient intake by total energy per 1000 kcal 53 and were categorized into quartiles for analysis.
Covariate Measure
A structured Nepali-version questionnaire was used to collect information in face-to-face interviews conducted in a private setting by trained interviewers. Each interview was about 45 to 60 minutes. Participants were informed about the study procedures using a prepared information sheet prior to conducting a survey. Participants were reassured about the confidentiality of their information. They were requested to sign informed consent forms prior to being interviewed.
The information on sociodemographic, lifestyle, cardiovascular risk factors, and ART were collected using the instruments from previous studies conducted in Nepal. 54 –57 Antiretroviral therapy use was measured by participants’ current use of medication at the time of the survey along with specified duration and names of medication and adherence. The past history of any disease was asked by a question “In the past 12 months, did you suffer from any type of diseases including minor illnesses?” with response options of yes or no. If the response was yes, the signs or symptoms of disease or disease diagnosis with details of health-seeking behavior and treatment of each disease were queried. The measurement of other sociodemographic and lifestyle variables was described elsewhere. 58,59
Physical Examination
The body weight of participants was measured in kilograms on a digital scale and the height was measured in centimeters by a stadiometer. Body mass index (BMI) was calculated as body weight in kilograms divided by the square of body height in meters. Blood pressure was measured with the Omron Automatic Blood Pressure Monitor (HEM-757, Omron, Japan) after the participants had been seated for at least 10 minutes with his or her feet on the floor and his or her arms supported at heart level. All anthropometric measurements were repeated to estimate mean values for these parameters.
Statistical Analyses
Out of 322 participants, 8 participants who did not have information on B vitamins intake were excluded, resulting in a final study population of 314 participants (180 men and 134 women). The t and chi-square tests were used to assess the difference in demographic, lifestyle, anthropometric, clinical parameters, and B vitamins intake by sex, for continuous variables and categorical variables, respectively. The relationships between B vitamins intake and serum CRP concentrations were assessed using multiple linear regression analysis. All analyses were done for men and women separately. To better approximate normal distributions, serum CRP concentrations were log transformed prior to analysis. The mean and their 95% confidence intervals (CIs) of log-transformed serum CRP concentrations were calculated for each quartile of B vitamins intake, then back transformed.
Major sociodemographic characteristics and other variables having previously established or plausible associations with the dependent variable were included as covariates or potential confounders in the analyses. Age (years, continuous), sex (men or women), alcohol intake (never or ever), smoking (never or ever), physical activity (
Further analyses were done by adjusting the serum vitamin D or zinc levels in the final model as we reported previously an inverse association of either serum vitamin D or zinc concentrations with serum CRP concentrations in the same study cohort. 49 ,51 The ordinal numbers 0 to 3 assigned to quartile categories of B vitamins intake were used to calculate trend associations. All P values were 2 sided and P values less than .05 were considered statistically significant. Analyses were performed with SAS statistical software version 9.1 (SAS Institute, Inc, Cary, North Carolina).
Results
The mean (standard deviation SD) age of the men and women were 35.6 (6.9) and 32.5 (6.9) years, respectively. The mean (SD) BMI of the men and women were 21 (2.8) and 22 (3.0) kg/m2, respectively. Women were less likely to smoke (P < .0001) or drink (P = .011) than men in the past month. The proportion of men and women who never smoke and drink were 28% versus 86% and 84% versus 93%, respectively. Women were more likely to report that they had a history of any disease in past 12 months than men did (70% vs 58%; P = .024). The median (range) CD4+ T-cell count in women (360 [15-1551] cells/μL) was significantly greater than that in men (333 [41-962] cells/μL; P = .019). There were no gender differences in B vitamins intake. Table 1 shows the B vitamins intake below the level of recommended dietary allowance (RDA) 61 of the participants by sex. More than two-third of participants’ B vitamins intake were below the RDA level.
Proportion of Study Participants with a B Vitamins Intake Below the Recommended Dietary Allowance.
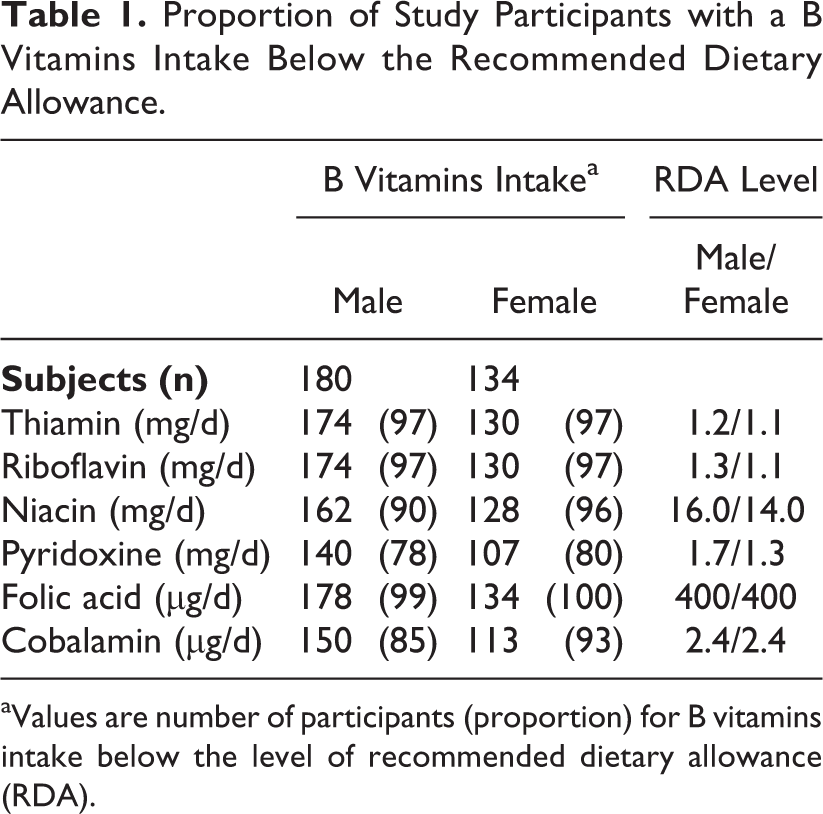
aValues are number of participants (proportion) for B vitamins intake below the level of recommended dietary allowance (RDA).
The relationship between B vitamins intake and serum CRP concentrations by gender is shown in Tables 2 and 3. The multivariate-adjusted geometric mean of serum CRP concentrations was significantly decreased with an increasing B vitamins intake across quartiles of niacin (P for trend = .007), pyridoxine (P for trend = .042), and cobalamin (P for trend = .037) in men (Table 2). The mean serum CRP concentrations in the highest quartiles of niacin, pyridoxine, and cobalamin were 63%, 38%, and 58%, respectively, lower than that in the lowest quartile in men. In women, the mean serum CRP concentrations in the highest quartiles of riboflavin and pyridoxine were 37% and 47%, respectively, lower than that in the lowest quartile (Table 3). However, these relationships were not statistically significant for riboflavin (P = .084) and pyridoxine (P = .093) in women. The relationships between B vitamins and serum CRP concentrations remained same in further adjustment with either serum vitamin D or zinc levels in the final model (data not shown in the table).
Multivariate-Adjusted Means of Serum CRP Concentrations According to Quartile of Dietary B Vitamins Intake in HIV-Infected Men.a
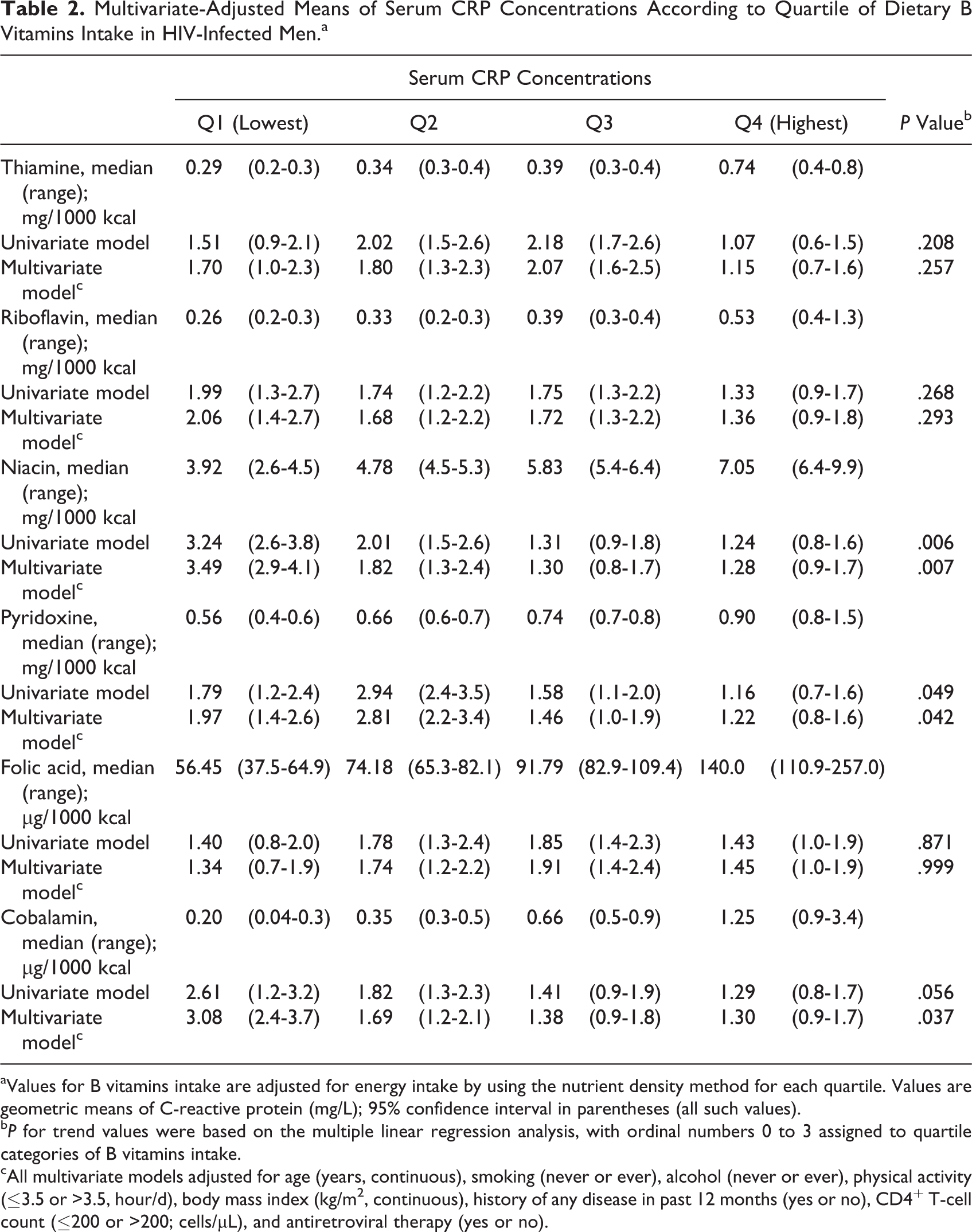
aValues for B vitamins intake are adjusted for energy intake by using the nutrient density method for each quartile. Values are geometric means of C-reactive protein (mg/L); 95% confidence interval in parentheses (all such values).
b P for trend values were based on the multiple linear regression analysis, with ordinal numbers 0 to 3 assigned to quartile categories of B vitamins intake.
cAll multivariate models adjusted for age (years, continuous), smoking (never or ever), alcohol (never or ever), physical activity (≤3.5 or >3.5, hour/d), body mass index (kg/m2, continuous), history of any disease in past 12 months (yes or no), CD4+ T-cell count (≤200 or >200; cells/μL), and antiretroviral therapy (yes or no).
Multivariate Adjusted Means of Serum CRP Concentrations According to Quartiles of Dietary B Vitamin Intake in HIV-Infected Women.a
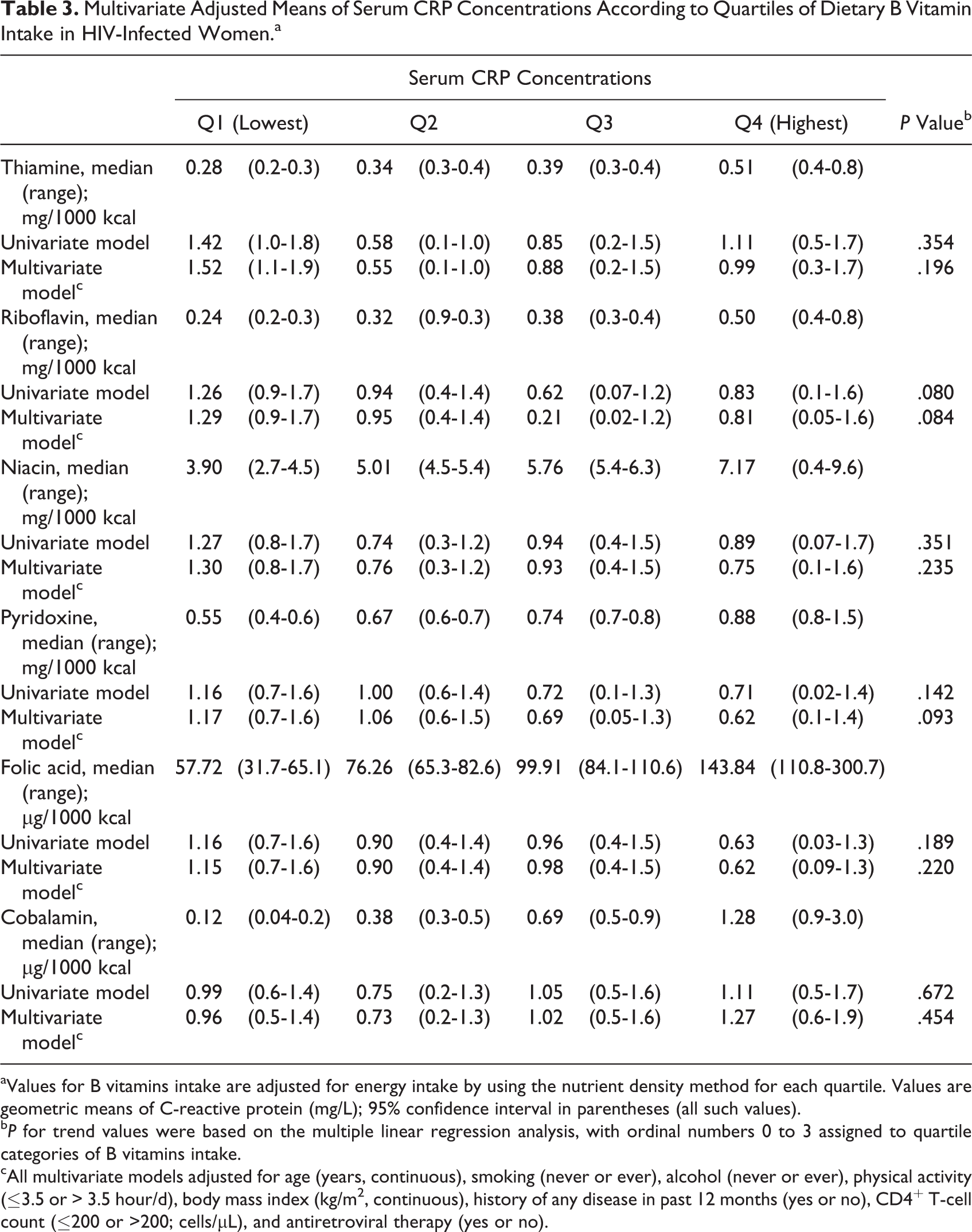
aValues for B vitamins intake are adjusted for energy intake by using the nutrient density method for each quartile. Values are geometric means of C-reactive protein (mg/L); 95% confidence interval in parentheses (all such values).
b P for trend values were based on the multiple linear regression analysis, with ordinal numbers 0 to 3 assigned to quartile categories of B vitamins intake.
cAll multivariate models adjusted for age (years, continuous), smoking (never or ever), alcohol (never or ever), physical activity (≤3.5 or > 3.5 hour/d), body mass index (kg/m2, continuous), history of any disease in past 12 months (yes or no), CD4+ T-cell count (
Discussion
This is the first study exploring the relationship between B vitamins intake and serum CRP concentrations among HIV-infected persons taking account of the use of ART and important lifestyle factors. Men with the highest intake of niacin, pyridoxine, and cobalamin and women with the highest intake of riboflavin and pyridoxine had lower serum CRP concentrations though the relationships being marginally significant in women. This study provides important new evidence about the beneficial effects of B vitamins intake against inflammation in HIV-infected persons.
HIV-infected men and women with the highest intake of pyridoxine had 38% and 47% lower serum CRP concentrations than the lowest intake group, respectively, in this study cohort. This study finding is in line with the previous studies highlighting an inverse association between vitamin B6 status and inflammatory markers in patient groups 17 –20 and general population samples. 21 –23 For example, a large population-based NHANES study 24 in the United States showed that higher vitamin B6 intake was significantly associated with lower serum CRP concentrations among 2686 participants. An inverse association between PLP concentrations and serum CRP concentrations was observed in 1976 women of the Women Health Initiative Observational Study. 62 High plasma PLP concentrations were associated with lower serum CRP concentrations among 891 participants of the Framingham Heart Study. 21 In the Boston Puerto Rican Health Study, higher PLP quartiles were significantly associated with lower CRP concentrations with a strong dose–response relation. 63
Furthermore, similar association was reported for plasma PLP and serum CRP concentrations in 1320 participants in CHIANTI study. 22 Among patients with rheumatoid arthritis, a large dose of vitamin B6 supplementation of 100 mg/d reported the significant reduction in proinflammatory cytokines at 12 weeks of follow-up. 64 These results suggest that vitamin B6 intake may help to control inflammation. This effect may be due to its active form, PLP, functions as a cofactor involved in several metabolic processes such as immune and inflammatory responses in the body. 65 Several components of the immune response, especially T-helper cells and IL-2, are significantly reduced in human with reduced availability of PLP. 12 The maturation and function of thymus and lymph nodes derived T-cells depend on the gradient of sphingosine 1 phosphate (S1P). The S1P is a potent metabolite that regulates immune response and inflammation processes including cell growth, vascular integrity, lymphocyte trafficking, and cytokine and chemokine production. 66,67 The concentration of S1P increases during inflammation, 68 which acts as a chemoattractant for the inflammatory cells. The synthesis and breakdown of S1P depend on the PLP-dependent enzymes.
The evidence about the effect of other B vitamins on serum CRP concentrations is sparse. This study suggests a beneficial effect of increased intake of riboflavin, niacin, or cobalamin on inflammation among HIV-infected persons with poor nutritional status. A study that assessed the association between cobalamin and type 2 diabetes mellitus reported the significant inverse correlation between cobalamin and homocysteine concentrations. 69 The findings are at variance with other studies that did not show the beneficial effect of riboflavin, 70, 71 niacin, 72 or cobalamin 73 in reducing serum CRP concentrations in populations other than HIV infection. It seems that very few studies have been published regarding associations between intake of riboflavin, niacin, or cobalamin and serum CRP concentrations. More mechanistic and observational studies are needed to further describe the mechanisms and to establish causal relations.
The inverse relationships between dietary intake of selected B vitamins (niacin, pyridoxine, and cobalamin) and serum CRP concentrations in our study were significant in men but not in women. However, the interaction terms between sex and intake of these B vitamins were not statistically significant, suggesting that the weaker association among women was not due to any true difference between the sexes but, rather, to other reasons, including much lower levels of B vitamins intake in women as compared with men. For example, the proportion of participants with B vitamins intake below the RDA levels was higher in women than men; 96% versus 90% for niacin (<14 mg/d vs <16 mg/d), 80% versus 78% for pyridoxine (1.3 mg/d vs <1.7 mg/d), and 93% versus 85% for cobalamin (<2.4 µg/d). Thus, the B vitamins levels in women might be below the threshold where B vitamin’s effect on serum CRP concentrations could be seen. Alternatively, estrogen may confound the association of B vitamins in women because of its effects on serum CRP concentrations. 74
The present study had some limitations. First, the cross-sectional design of the study cannot rule out a clear cause–effect relation. Prospective studies and randomized trials are needed. Second, a 24-hour recall may not provide good estimates of usual dietary intake because of within-person variation. However, this would be less relevant in the present study population due to the measurement of dietary recalls twice 1 week apart and of the limited variation in dietary intake. Third, the possibility of residual confounding cannot be excluded although we adjusted for known factors that could influence both B vitamin intake and inflammation. Finally, our study participants were not selected using random sampling method, thus caution should be taken in generalizing our study findings to the entire population of HIV-infected persons in the country.
In conclusion, the present study suggests that higher intake of pyridoxine and niacin may be associated with lower serum CRP concentrations among HIV-infected men even after taking account of ART and other important confounding factors. This finding adds the beneficial effect of B vitamins against inflammation in HIV-infected persons. Further prospective studies and/or clinical trials are needed to confirm the role of B vitamins against inflammation in HIV-infected persons.
Footnotes
Acknowledgments
The authors would like to thank all of the participants for their valuable information, cooperation, and participation. They would also like to gratefully acknowledge the support and coordination of 5 local NGOs working with HIV-positive populations in the Kathmandu Valley, Nepal—Youth Vision, Sneha Samaj, Srijansil Mahila Samuha, SPARSHA Nepal, and Shakti Milan Samaj for recruiting participants and collecting information. They would like to thank Dr. Krishna C Poudel, School of Public Health and Health Sciences, University of Massachusetts Amherst, for his support in the conception and design of the main study cohort and overall management of the study. They wish to thank Dr. Shinichi Oka, AIDS Clinical Center, National Center for Global Health and Medicine, Japan and Dr. Basu Dev Pandey, Everest International Clinic and Research Center, Kathmandu, Nepal for their laboratory support in storing blood samples.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the Grant-in-Aid for Young Scientists (B) (22790581), Japan Society for the Promotion of Science, The Ministry of Education, Culture, Sports, Science and Technology, Japan; Waseda University Grants for Special Research Projects, General Grant/Ippan Josei, Japan (2012A-101); and by the Grant for Research on Global Health and Medicine from the National Center for Global Health and Medicine, Japan (No. 21A-2). The funding agency had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.