
Abstract
Food fortified with folic acid has been available for consumption in North America for over a decade. This strategy has led to an increase in folate levels in the general population and, more importantly, a significant decrease in the incidence of neural tube defects. However, this increase in folate intake has been associated with a greater risk of cancer disease. Many African countries are now embracing this concept; however, because folate promotes malaria parasite division, as it does in cancer cells, there is a possibility of malaria exacerbation if folate intake is increased. A precedent for such a concern is the now compelling evidence showing that an increase in iron intake can lead to a higher malaria risk; as a result, mass administration of iron in malaria-endemic areas is not recommended. In this article, we review work on the effect of folate on malaria parasites. Although this topic has received little research attention, the available data suggest that the increase in folate concentration could be associated with an increase in malaria infection. Thus, the introduction of food fortification with folic acid in malaria-endemic areas should be attended by precautionary programs to monitor the risk of malaria.
Keywords
Introduction: Folate Fortification Around the World
In many countries in the world, food fortified with micronutrients (including vitamins) is being consumed by the general population as a strategy to lower their deficiency. Evidence to support this concept stemmed from work carried out in the United States on fortification using folic acid (FA) as a strategy to reduce neural tube defects (NTDs) in pregnancy. Neural tube defect is the second most common birth defect in the world and occurs during the first 28 days postconception. Early studies showed that supplementation with folate before and during pregnancy was associated with a substantial reduction in NTD, 1 providing evidence for an association between NTD and folate deficiency 2 and reviewed in the studies by Christianson et al, Osterhues et al, and Daly et al. 3 –5 This evidence led the US Food and Drug Administration to mandate in 1996 that cereal grain be fortified with FA, which, when consumed by the population, would reduce the risk of NTD in pregnancy. 6 Since the introduction of folate-fortified cereal, monitoring programs have shown increases in folate levels in the general population. 7 –9
The concept of food fortification with vitamins and minerals was, in fact, initiated from the 1920s, with the fortification of salt with iodine against goiter, milk with vitamin D to reduce the risk of rickets, and cereals with iron, thiamine, niacin, and riboflavin to reduce anemia related to iron deficiency, beriberi, pellagra, and riboflavin deficiency, respectively. 10 However, evidence of the reduction in NTD in the general population as the result of fortification of cereal with FA has been an important milestone in this approach. The wide availability of food fortified with folate (and other micronutrients) has now spread to many African countries. 11,12
For instance, South Africa (in 2003) was among the first countries to implement fortification of flour with FA, and a monitoring program has shown a reduction of more than 40% in NTD as compared to prefortification. 13 Legislation and strategies have now been developed to implement this concept in other African countries, 12 and food fortified with FA will thus be an increasingly common occurrence in Africa.
The experience in the developed world, especially in the United States, shows that although this strategy has improved folate levels in the population, it is also associated with some untoward consequences, especially in relation to diseases whose progression is associated with the availability of folate. For instance, evidence indicates that folate can promote the progression of cancer and mask megaloblastic (pernicious) anemia. 14 –17 Malaria disease is endemic in sub-Saharan Africa, and like cancer cells, malaria parasite growth relies heavily on the availability of folate derivatives, 18 thus, the increase in folate levels in the general population could promote the progression of the disease. For instance, compelling evidence shows that high iron concentrations exacerbate malaria disease, and as a result, an increase in iron consumption in the population living in malaria-endemic areas is not recommended. 19 –22 In this review, we discuss the possible impacts of increasing folate intake on malaria disease (either as part of fortification or supplementation) in areas where malaria is endemic.
Folate Biochemistry
Folate derivatives consist of a molecule of reduced pterin linked to para-aminobenzoate (pABA) and glutamate. The parent biologically active molecule, tetrahydrofolate (THF), is substituted with 1-carbon moieties on the N5 and N10 positions of the pteridine ring. These molecules are important cellular cofactors in the synthesis of nucleotides required for DNA replication and in the synthesis and metabolism of the amino acids serine, glycine, methionine, histidine, and glutamate. Folate cofactors are also required for the initiation of protein synthesis in mitochondria through formylation of methionine. 23 The most important biologically active folate cofactors are 5-CH3-THF for the synthesis of methionine; 5,10-CH2-THF for the formation of the pyrimidine deoxythymidine monophosphate (dTMP);10-CHO-THF for the formylation of methionyl-tRNA; 5,10-CH=THF and 10-CHO-THF for the synthesis of purines; and THF and 5,10-CH2-THF for the metabolism of serine, glycine, histidine, and glutamate. The folate cofactor central to the synthesis of methionine, 5-CH3-THF, is the predominant folate molecule in the circulation, representing over 95%, in human populations not fortified with FA. 24,25 Methionine is then used to synthesize S-adenosylmethionine, the universal methyl group donor involved in many reactions, including the methylation of ribonucleic acid (RNA) and deoxyribonucleic acid (DNA) bases, histones, and many other molecules. These methylation reactions are important for regulating various cellular functions such as chromatin remodeling, gene transcription, messenger RNA translation, cell signaling, and epigenetic phenomena, 26 all of which can be disrupted if the availability of methyl group donor is reduced.
The lack of free nucleotides, mainly dTMP, as the result of folate deficiency, causes misincorporation of uracil into DNA, leading to decondensed chromosomes and double-stranded breaks and translocations, and these effects are associated with higher cancer risk, neuropsychiatric diseases (especially in geriatric population), and neural defects. 4,14,27 Hypomethylation can lead to several complications including atherosclerosis, neural damage, and carcinogenicity. For instance, the etiologies of colorectal, cervical, breast, pancreatic, esophageal, and gastric cancers have been associated with low folate levels. 28 Thus, folate deficiency is associated with many complications, and a priori, increasing the intake of folate to correct this deficiency will be beneficial to human health. 29 However, there is evidence that the indiscriminate increase in folate intake in the population can also cause various undesirable complications, especially in populations that are not folate deficient or have diseases whose progression can be affected by folate levels, such as some types of cancer. 14,30
Malaria Disease
Malaria Parasites
Malaria is associated with very high morbidity and mortality. For instance, in 2010, more than 216 million cases and 665 000 deaths were reported, the latter mainly (more than 90%) occurring in children under the age of 5 and pregnant women. 31 Over 125 million pregnant women are at risk of malaria, and more than 100 000 infant deaths occur each year as a result of malaria-associated pregnancy. 32,33
Malaria parasites, in the form of sporozoites (in general less than 10), are transmitted to the human host by a female mosquito during blood feeding. These sporozoites will invade and divide in hepatic cells to produce 10 000 to 30 000 new parasites, known as merozoites. 34 Subsequently, each merozoite will potentially invade a red blood cell (RBC) and will multiply to produce 6 to 8 new merozoites in a 48-hour cycle. 35 The new merozoites in turn will invade new RBC, and the cycle continues. The RBC cycle is associated with the development of clinical signs of the disease. In high endemic areas, up to 50 000 infected RBCs [IRBCs]/μL of blood (approximately 1 IRBC for every 100 RBCs) can be found, 35 corresponding to more than 1010 IRBCs in an adult. Thus, malaria is associated with rapid multiplication rates, both in the liver and the RBC, and this process is heavily dependent upon the availability of folate. Below we summarize the main features of folate biochemistry in malaria parasites.
Folate Biochemistry in Malaria Parasites
Malaria parasites have 2 folate pathways
Malaria parasites, like cancer cells, are highly dividing cells, thus relying on the availability of folate to sustain their growth. This parasite, unlike other living organisms described so far, has 2 folate pathways: a salvage pathway (from exogenous sources) and a pathway of de novo synthesis. The parasite uses both of these to sustain its folate requirements. The inhibition of de novo folate synthesis by antifolate drugs is used as a rationale to block parasite growth. 36,37 Likewise, reducing folate uptake by the parasite leads to an increase in the activity of antifolates, a clear indication that the salvage pathway contributes to folate availability. 38 Whereas mammalian cells (including cancer cells) have only the salvage pathway, the 2 pathways of the malaria parasite emphasize its critical reliance on folate availability.
5-CH3-THF is not utilized by the parasite
The malaria parasite is selective in the form of folate it salvages. The parasite synthesizes folate de novo to generate methylene-THF, the methyl donor for the synthesis of dTMP. Interestingly, investigations have shown that the parasite does not utilize 5-CH3-THF, despite it representing over 95% of folate normally present both in human serum and in RBC. 25,39 The role of this folate form in other organisms is to synthesize methionine from homocysteine. However, the parasite obtains its amino acid supply, including methionine, predominantly from hemoglobin degradation, a protein that is stored in the RBC. 40,41 We will discuss later the implication of this lack of 5-CH3-THF utilization in relation to folate intake.
Folate Intake and Malaria Risk
Information from clinical trials in humans
The challenge of studying the folate effect on malaria is that there are no available data on the intake of folate alone in relation to the progression of the disease, unlike in the case of iron. Studies in which folate was administered have indeed been reported, however, they were carried out in the context of malaria treatment. In fact, most of these investigations were driven by the need to establish the effect of folate (mainly FA) on the activity of antifolate drugs such as pyrimethamine–sulfadoxine (PM/SD; Fansidar). In these studies, which we have recently reviewed, 41 patients (including children, pregnant women, and adults) who received FA were also treated with an antimalarial drug, and the results show that the use of a high dose of FA (>2.5 mg/d) was associated with decreased antifolate efficacy, while no change was observed when a nonantifolate drug was used (chloroquine or Malarone). Conversely, the use of a low dose of FA (<1 mg/d) did not reduce the efficacy of PM/SD. 41,42 Since in all these studies, patients were treated with an antimalarial drug, one cannot disentangle the “folate effect” from that of the drug on the progression of the disease.
However, in one of the aforementioned studies, interesting information was provided on folate levels in blood and parasitemia. While investigating the effect of high-dose folate supplementation on the efficacy of PM/SD in pregnant women from Kenya, van Eijk et al 43 also measured serum folate levels before and after treatment and correlated these levels with parasitemia. Interestingly, before treatment, 12 women with the highest parasite density (defined as the density within the highest tercile of the 467 pregnant women in the study population) were among those with the highest folate serum levels (>15.4 ng/mL). These data indicate that the higher the folate level, the higher the parasitemia. These observations are in line with an early report on malaria cases in relation to folate levels in Guinea. 44 In this longitudinal study, a cohort of children was followed at 2, 6, and 12 months, and malaria blood slides, RBC counts, and serum folate concentrations were assessed. Interestingly, children who were parasitemic had a higher RBC folate, and in those at 12 months, these elevated levels achieved statistical significance (728.3 vs 489.1 μg/L, n = 56 and 187, respectively, P < .001). 44 In another study, folate levels were measured in pregnant women (with no history of antimalarial intake before the study). Interestingly, mean RBC folate concentrations at day 0 (before treatment) in women with parasitemia were significantly higher than nonparasitemic women. 45 Similar results have been reported in a study involving 200 primigravidae women. In this study, RBC folate levels were higher in women with parasitemia than in parasite-free women. 46 All these aforementioned studies are summarized in Table 1.
Summary of Studies on the Impact of Folate Levels on Malaria Infections In Vitro, in Animal Models and in Human.
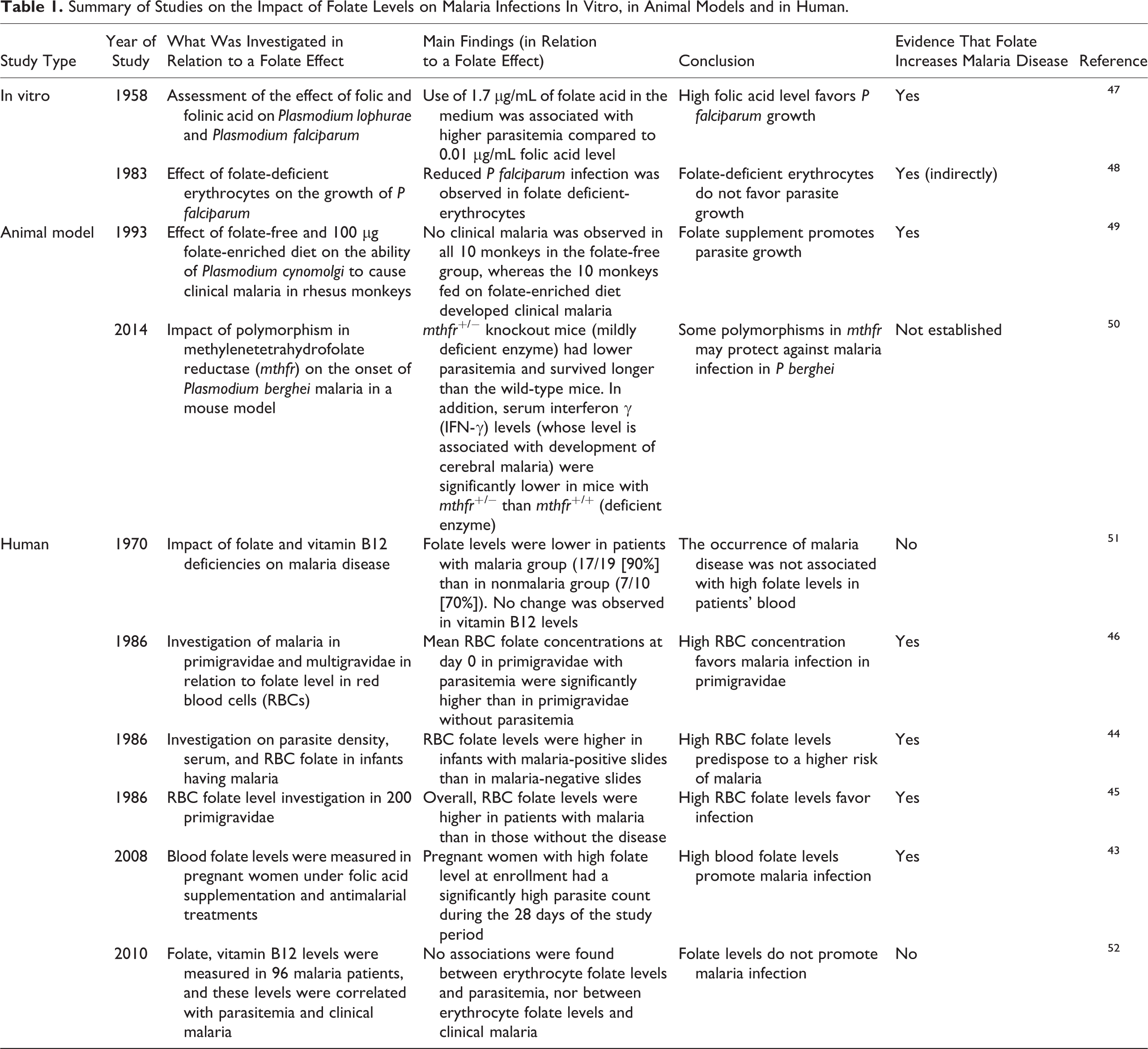
However, this folate effect (the association between high folate levels and promotion of malaria growth) was not confirmed in a study carried out in Columbia on 92 adult patients. In this study, no significant association between erythrocyte folate and patient parasitemia nor clinical malaria was found. 52 Likewise, an early study in 1970s, involving adult men, showed that high blood folate levels were not associated with high malaria infection. 51
In a further scenario, an inverse relationship between folate level and rate of malaria disease was reported in early studies. Fleming and Werblinska 53 reported a higher parasitemia in patients having megaloblastic anemia than those who did not, an indication that folate deficiency may in some circumstances favor the disease. Another study reported a low rate of malaria infection in pregnant women whose diet was rich in folate, indicating again that folate intake could be inversely related to malaria disease. 54 However, it is worth noting that in these studies that show an apparent inverse relation between folate level and disease, actual physiological folate levels were not measured, thus limiting the conclusions that can be drawn from them.
Thus, although several studies have tested the supplementation of folate in the context of malaria, none has yet investigated the detailed effect of this supplementation on malaria progression. The objectives of these studies were to investigate either the effect of folate on the activity of antimalarial drugs or the ability of folate to reverse anemia. In 6 studies only, the relationship between folate concentrations and parasitemia was investigated, and as discussed, 4 studies showed a growth-promoting effect of folate, whereas 2 did not (Table 1). In summary, the available clinical data tend to indicate a possible parasite growth-promoting effect in the context of high folate levels, although the supportive data are limited. The increase in folate levels has a double effect, first, it makes this vitamin available to sustain parasite divisions, and in addition, it promotes erythropoiesis, a process that leads to the generation of RBCs, 55 thus leading to more infection. Below we summarize the available data in animal models.
Evidence in animal models
Evidence of a folate effect was provided in vivo in a monkey model with Plasmodium cynomolgi, where in 10 monkeys, folate deficiency was induced with a folate-free diet (test group), and another 10 were fed with a diet enriched with 100 μg of folate daily (control group). All the monkeys were then infected with P cynomolgi. Interestingly, none of the animals in the test group (folate deficient) developed clinical malaria, but all monkeys of the control group did, with 5 deaths and 5 recoveries after treatment with chloroquine (cited in Herbert 49 ; Table 1). This was the first evidence that folate deficiency could protect against malaria disease, and it might be expected that this observation would spur investigations to test this concept in humans. However, this has not been the case (based on an extensive literature review), a situation different from the one that pertains to iron. 19,22
Even in animal models, to the best of our knowledge, no studies have been dedicated to further investigating this protective effect of folate deficiency. However, recently, a mice model, using the Plasmodium berghei ANKA strain (which induces potentially lethal cerebral malaria), was used to study how disruption of folate metabolism might affect the development of this condition. 50 The enzyme methylenetetrahydrofolate reductase (MTHFR) synthesizes 5-CH3-THF, the primary circulatory form of folate in humans, utilized as a methyl donor for methylation reactions. One variant MTHFR, the 677TT genotype, has been reported in humans and causes an approximate 70% loss of enzyme activity, resulting in a mild hyperhomocysteinemia with attendant consequences. 56 Meadows et al have reported that a mildly deficient variant of this enzyme protects against malarial infection in a mouse model by interacting with the mouse immune response. 50 However, in this study, the change in folate levels (as a result of the presence of the MTHFR 677TT genotype) was not measured, and so conclusions cannot be drawn as to the relationship between folate availability and malaria infection.
Evidence in vitro
Standard in vitro culture of Plasmodium falciparum parasites is routinely carried out in a nutrient-rich medium (RPMI 1640 medium), supplemented with 5% to 10% human serum or Albumax (a synthetic serum) and human RBCs, typically between 3% and 5% (vol/vol) of packed cell volume to the volume of the medium. The standard RPMI medium is also supplemented with 1 mg/L FA, which is 100 times higher than physiological folate concentrations (of around 10 μg/L), 57 together with 1 mg/L pABA—a folate precursor derived from folate catabolism in humans that can be used by the parasite to sustain its de novo folate synthesis. Thus, the total amount of folate in the culture is derived from the supplemented folate, the folate present in the serum (if human serum is used) and RBCs.
One of the earliest in vitro studies on the effect of folate on plasmodial growth in human erythrocytes dates back more than 50 years. 47 In this study, the effect of differential FA concentrations on the development of P falciparum in suspensions of human erythrocytes was assessed using 0.01 and 1.7 μg/mL FA. After a complete cycle, parasite smears showed the highest rate of reinvasion and the highest number of multinucleate trophozoites in the flasks with high FA concentration, indicating more favorable growth in this medium. A related study involved the testing of 2 media (normal medium and minimal medium) and 2 different sources of RBCs, one from a normal donor (N cells) and the second from a patient having folate deficiency (D cells). 48 The results showed that parasite growth was substantially reduced in minimal medium (without folate supplementation), and in addition, parasite growth was also lower with D cells than with N cells when normal medium was used. This experiment indicated that low folate concentration is associated with low parasite growth (Table 1). Complementary investigations have also been carried out in vitro by increasing folate concentration up to 1000 times physiological levels, and parasite growth was sustained in these conditions. 39
Limitations in establishing a folate effect on malaria disease
One of the difficulties in establishing a folate effect on malaria disease (unlike the case with iron) is that, as discussed earlier, the parasite is selective about the folate forms it can utilize. Folate is actually a generic term covering at least 9 different biological molecules, and in humans, the predominant form by far is 5-CH3-THF, which is not utilized by the parasite, and so an increase in this form would not impact on parasite growth. Thus, the intake of folate and the risk of malaria should also be analyzed in the context of folate diversity. Indeed, the total amount of folate may not matter much; it is how this “folate” is distributed among the different forms that will determine how much impact there may be on malaria, if any. Thus, just measuring total folate is not sufficient, and this may explain why contradictory results have been observed on the association between folate and malaria disease.
Despite all these limitations (limited studies and the complexity of folate biochemistry in malaria), based on our current knowledge of folate metabolism in the parasite and the experience of folate intake in cancer disease, we propose different scenarios that could be associated with an increased FA intake in the context of malaria.
Proposed dual effects on malaria risk
Protective effect
Folate deficiency is common in malaria-endemic areas and is associated with several complications, including anemia, cancer, heart disease, and neural impairment, as discussed earlier. An increase in folate intake will correct these complications and improve the general health of the population. Thus, in those who live in malaria-endemic areas but are parasite free, it is undoubtedly the case that an increase in folate intake will be beneficial to their health and this in turn will increase their ability to resist infections, including malaria.
Increased risk at high FA doses
However, problems may arise, not only in those already having clinical malaria but also in those with asymptomatic parasitemia (who represent a high proportion of the population in malaria-endemic areas). Indeed, since malaria parasites rely heavily on folate, an increase in its availability would promote parasite growth, as seen with cancer cells, a situation that could exacerbate the disease.
Folic acid is one of the active folates that the parasite can utilize to promote growth and is the form commonly used in supplementation and food fortification. Once administered in humans at low dose (≤0.5 mg/d), this form is quickly converted to 5-CH3-THF, 58 an inactive form for the parasite, as discussed earlier. In food fortification, FA is normally added at a ratio of 100 to 200 μg of FA/100 g of cereal or flour. With an average of 100 to 200 g of cereal/flour consumed per day, 59 the amount of FA ingested will correspond to a low dose, as defined above, which will rapidly be lost to the parasite as inactive 5-CH3-THF. Thus, under these circumstances, food fortification with FA may not exacerbate malaria disease.
However, in the case of folate supplementation or in the treatment of anemia, a much higher dose of 5 mg FA/day is usually used. Pharmacokinetic investigations have shown that at such a dose, the bulk of this remains in the blood circulation as FA, and only a small fraction of which is converted to 5-CH3-THF. 58 Thus, the parasite can exploit the high level of active FA and use it to support growth, a situation that will exacerbate malaria. Likewise, in a recent review of the folate intake in the context of malaria, it was proffered that high dosages of supplemental FA should not be given to preschool age children in malaria-endemic areas as these supplements may favor the growth of P falciparum. 60 Thus, we argue that the effect of increases in FA intake on malaria will be dose dependent.
Concluding Remarks
Food fortification with FA has been implemented in North America and elsewhere, and evidence shows a greater risk of cancer disease and the masking of megaloblastic anemia as a result. The same concept is now being introduced in Africa, and based on the role folate plays in malaria cell division, this strategy could also lead to an increased risk of malaria. We have reviewed the literature, and although there has been many decades of work on folate metabolism in malaria parasites, 36 surprisingly, little has been directed at the questions raised here, and the data are as yet scanty to draw any firm conclusions on the relationship between increase folate intake and the development of malaria disease. The little available data support promotion of malaria growth associated with high folate levels; however, based on our current knowledge of folate biochemistry in malaria parasites and the known association between folate intake and cancer risk, we propose a dose-dependent effect, whereby intake of low doses of FA (which correspond to the daily amount from food fortification) would have a marginal impact on malaria disease. However, monitoring of malaria cases in the context of food fortification should be carried out to ascertain that this is indeed the case. Where high-dose folate supplementation is used, the greater risk of exacerbating clinical malaria should be clearly recognized. Finally, though we have largely focused this review on the folate effect in malaria, we would argue that, based on experience from North America, the risks of increasing cancer growth and of masking megaloblastic anemia also exist in the context of Africa. Thus, as the concept of food fortification with FA is now being introduced more widely into Africa, both health professionals and policy makers should be cognizant of these possible untoward effects, and measures should be put in place to monitor and, if necessary, counterbalance such consequences.
Footnotes
Acknowledgments
A.N. is grateful to the King Fahd University of Petroleum and Minerals (KFUPM) for personal support. J.O. is grateful to the University of Cape Town Library Services for assistance with accessing articles.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.