
Abstract
Background:
Diet diversity of pregnant women is associated with nutrition sufficiency, micronutrient adequacy, and pregnancy outcomes. However, the sociodemographic determinants of diet diversity among pregnant women in low-income countries are not well studied.
Objective:
The analysis was undertaken to study the determinants of high dietary diversity and consumption of micronutrient-rich foods by pregnant women from rural Bangladesh.
Methods:
Pregnant women (508) were randomly selected from southwestern Bangladesh and interviewed to collect data about diet and sociodemographic characteristics. A 24-hour recall was used to collect information about diet. Diet diversity score was calculated for 9 major food groups. All analyses were conducted using STATA SE 12.
Result:
The overall mean diet diversity score was low at 4.28 and was significantly high among pregnant women who have higher educational achievement, whose husbands’ occupation was business, who live in households of 4 or more family members, and who were dwelling in a house with more than 1 room. Highest gap on knowledge and consumption was reported for 3 food groups including dairy foods, eggs, and dark green leafy vegetables. Consumption of dairy and eggs was lower among women from low socioeconomic status, but no significant association was found between sociodemographic characteristics and consumption of leafy vegetables.
Conclusion:
Our analysis has shown that diet quality of pregnant women was poor and intake of micronutrient-rich foods was low despite having knowledge about the importance of these foods, underscoring the need for promoting the diet quality in developing countries through behavior change communication programs.
Introduction
It is generally accepted that nutritional status has a relationship with maternal and child health. Compared to other developing countries, Bangladesh has a higher prevalence of female undernutrition. 1 The Bangladesh Demographic and Health Survey (BDHS) report published in 2011 showed 24% of married women of reproductive age (15-49 years) had a body mass index (BMI) less than 18.5 and are considered undernourished. 2 There is also a strong association between low BMI or underweight and mortality among married women in Bangladesh. 3 As in other developing countries where pregnant women have micronutrient deficiencies including iron, 4 iodine, zinc, and vitamin A and B complex, 5 –7 widespread deficiencies of iodine, 8 vitamin B12, zinc, 9 and vitamin E 10 among pregnant women have been reported in rural Bangladesh. Inadequate nutritional status of pregnant women may also be a widespread problem in other low- and lower-middle-income countries. 5
A review showed significant evidence that zinc, calcium, and magnesium status improved pregnancy outcome in developing countries; it was also reported that deficiencies of vitamin C and iodine are causes of preterm delivery and mental retardation of new born, respectively. 11 Moreover, there is evidence that underweight pregnant women are likely to have intrauterine growth retardation and babies with low birth weight 12 and preterm birth. 13 Additional evidence shows increased incidence of hypertension, 14 lung cancer, 15 and insulin resistance 16 among the children whose mothers were malnourished during pregnancy.
It has been known for many years that pregnant women should consume an adequate diet for maintenance of maternal health, to meet the needs of the growing fetus, and to obtain the strength and vitality required during labor and for successful lactation. 17 There is consistent evidence that dietary diversity is strongly associated with nutrition sufficiency and is therefore considered an essential element of diet quality. 18,19 Nutritional adequacy is shown to be increasing more with diet diversity among female children and adults than among males. 20 It is also reported that number of food eaten is positively associated with nutrient intake. 21 Food group diversity is associated with micronutrient adequacy among women of reproductive age in Bangladesh 22 and lactating women in Nepal. 23 Diet diversity score (DDS) is considered as a universally recognized healthy diet-measuring tool that is used as a key dimension of diet quality and is present in food-based dietary guidelines. 24,25
In Bangladesh, the leading causes for undernutrition, or low diet diversity, among the rural inhabitants include low family income, low education level, and periodic food shortage associated with inadequate dietary intake. 26 There is evidence that pregnant women having financial difficulties have lower intake of different micronutrients including niacin, pyridoxine, iron, zinc, magnesium, and potassium. 27 In addition, studies showed that consuming micronutrient-rich foods, including milk and vegetables, is highly associated with infant birth size. 28,29 Thus, it is important to understand the factors associated with the intake of different food groups, particularly intake of micronutrient-rich foods by pregnant women most at risk of having a diet with poor diversity. Such information may help policy makers and program managers identify vulnerable groups and promote consumption of dairy products and eggs, especially those who are unable to afford these through safety net and other programs.
Factors associated with inadequate diet diversity among pregnant women in Bangladesh are not well studied. In our study, the aim was to understand the factors associated with high dietary diversity (HDD), and we identified potential barriers associated with the consumption of micronutrient-rich foods such as milk, eggs, and leafy vegetables among pregnant women of rural Bangladesh, even when pregnant women have knowledge about the importance of such foods. This study would help design and implement programs to promote a diverse diet for pregnant women in low- and lower-middle-income countries.
Methods
Study Design and Participants
This study was conducted on pregnant women of rural Bangladesh to observe the dietary pattern and knowledge about dietary diversity. The data source of this study was a cross-sectional survey conducted before the inception of a US Agency for International Development (USAID)-supported intervention project in southwestern Bangladesh, aiming to improve the dietary diversity of pregnant women. Data were collected between November and December 2013 to assess pregnant women’s knowledge of diet diversity and consumption practices as well as related determinants.
Sample size for the cross-sectional surveys to assess the effect of the intervention program was calculated based on the hypothesis that the intervention would contribute to increase 0.5 units of DDS at the end of the program. With 5% level of significance and 80% power, the investigators came up with 302 pregnant women to be recruited in the cross-sectional survey conducted prior to the inception of the intervention. To account for the design effect due to clustering, the sample size was inflated by about 70% and eventually the number of pregnant women to be recruited increased to 508. A multistage random sampling technique was used with 1 subdistrict randomly selected from each of the 5 program districts where the project is implemented. Fifty-one villages were chosen randomly from each selected subdistrict and 255 villages were selected from 5 subdistricts. Two pregnant women were interviewed from each village.
Data Collection Tools and Techniques
As most pregnant women feel comfortable in providing data to female interviewers in Bangladesh, only female interviewers were recruited for data collection and were extensively trained by the investigators on data collection tools. One data collection team, consisting of 2 data collectors and 1 supervisor, was selected for each of the 5 subdistricts. The data collection team moved anticlockwise from the center point of each village and interviewed the first 2 consented pregnant women from each village. A structured coded questionnaire was used to collect data. Each pregnant woman provided information on sociodemographic characteristics including age, education, husband’s education, occupation, religion, number of household members, number of living rooms, and food security status. A 24-hour recall was used to collect information on the number of food groups consumed by the individual respondent.
Statistical Analysis
For every participant, an individual DDS was calculated using food groups based on Food and Agriculture Organization (FAO) guidelines including starchy staples, legumes and nuts, dairy, organ meat, eggs, flesh foods, vitamin A-rich dark green leafy vegetables (DGLVs), other vitamin A-rich fruits and vegetables, and other fruits and vegetables. 22 None of the respondents reported eating organ meat, so only 8 food groups were included in the analysis. The DDS was calculated by summing the number of different foods or food groups consumed over the past 24 hours prior to the interview. Women were also asked about the food that a pregnant woman should eat, and responses were recorded according to food groups as defined earlier.
Data on demographic and socioeconomic characters were presented categorically. Respondent’s age was divided into 3 categories: 19 years and under, 20 to 24 years, and 25 years and older. Pregnant women were divided into 3 categories based on their years of educational attainment: functionally illiterate (0-5 years), secondary incomplete (6-9 years), and secondary complete (≥10 years). Husband’s occupation was divided into 5 categories: daily wage earner, agriculture, service, business, and other (including religious leader, immigrants, and village doctors). Household information of the respondents was shown in terms of 1-room dwelling, electricity connectivity, and ownership of TV. Household food insecurity was assessed using 5-question scale used in the BDHS 2011. 2 Respondents were asked about their last 12 months’ food intake in terms of eating a full-stomach meal, skipping an entire meal, eating less food due to lack of food, eating wheat instead of rice, and borrowing food from neighbors or relatives. Each question was given a qualitative score of 0 to 3, with 0 being the most food-secure response. Household food insecurity was measured by summing the score of the individual question. A household was considered food secured if the score was 0 and food insecure if the score was ≥1. The mean and 95% confidence interval (CI) of DDS were shown by sociodemographic characteristic.
High dietary diversity was defined as having a score above the 66th percentile value (5.00 in our study); similar score was also used to classify HDD in other study 30 and inadequately diverse diet. 31 Association of social and demographic characteristics with HDD (DDS ≥ 5) was initially assessed using χ2 test. Effect of each characteristic on HDD was estimated using odds ratio. Multiple logistic regression model was used to estimate the adjusted odds ratio. The variables that were associated with HDD at P < .20 in χ2 test were included in the multiple logistic regression model. We also assessed the effect of each characteristic on DDS using the mean difference between categories of each characteristic from the reference category. Linear regression with a single predictor and multiple predictors was used to estimate crude and adjusted mean differences and their 95% CIs. In multiple linear and logistic regression models, all the characteristics that were associated with HDD at P < .20 in χ2 test were included. Respondents’ knowledge about the different food groups pregnant women should eat were assessed through asking unprompted question, and actual consumption of 8 food groups during the past 24 hours indicates a gap between knowledge and consumption of food groups. For dairy products, eggs, and DGLVs, substantial gaps were identified between knowledge and consumption. Socioeconomic factors were associated with the consumption of dairy products, eggs, and DGLVs among women with positive knowledge. All analyses were conducted using STATA SE 12.
Ethics
Women were interviewed only after they gave written informed consent. Ethical clearance for the study was obtained from the ethical review committee of the Center for Injury Prevention, Health Development and Research, Bangladesh, and also from the FHI 360 Office of International Research Ethics (OIRE).
Results
Dietary diversity by sociodemographic characteristics is shown in Table 1. More than one-fifth (22.8%) of the pregnant women were adolescent, and more than half (57.6%) were relatively young (≤24 years). Nearly one-fifth (17.1%) of the participants were functionally illiterate, and more than 80% had completed at least primary education. Around half (47.7%) of the pregnant women’s husbands were either daily wage earner or agriculturist, and the other half (52.3%) engaged in service, business, and other occupations. Few (9.2%) women were interviewed in their first trimester. Around two-thirds of the pregnant women lived in houses with more than 1 room (63.1%) and had electricity (65.03%), though 70.9% did not own a TV. Pregnant women’s education, husband’s profession, household size, housing size, electricity connectivity, ownership of a TV, and household food security were associated (P < .05) with HDD.
Dietary Diversity of Pregnant Women by Sociodemographic Characteristics.
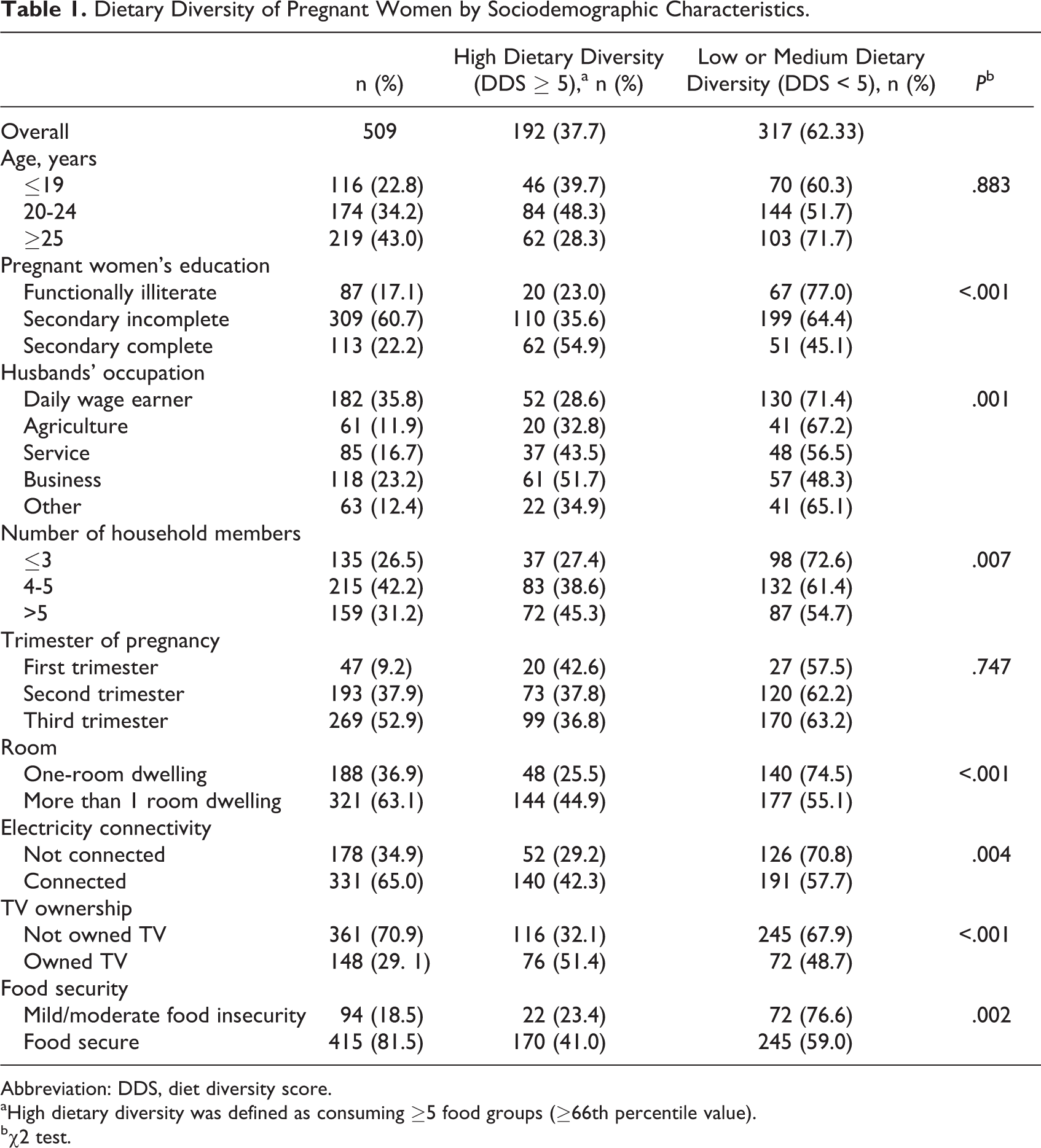
Abbreviation: DDS, diet diversity score.
aHigh dietary diversity was defined as consuming ≥5 food groups (≥66th percentile value).
bχ2 test.
High dietary diversity by sociodemographic characteristics is shown in Table 2. Women who completed secondary or higher level of education are 2.5 times more likely to have HDD than the functionally illiterate women, which is reflected by an adjusted OR (95% CI) of 2.58 (1.27-5.24; P < .001). Remarkably, only pregnant women whose husbands were engaged in business experienced an advantage as they are about 2 times more likely to have HDD than pregnant women whose husbands were daily wage earners and who were in other occupations, reflecting an adjusted OR (95% CI) of 1.85 (1.09-3.14; P < .001). Women dwelling in houses having more than 1 room are about 2 times more likely to have HDD than women dwelling in single-room houses, reflecting an adjusted OR (95% CI) of 1.78 (1.16-2.76; P < .001). Interestingly, pregnant women from a larger family are about 2 times more likely to have HDD than those from a smaller family (≤3 members), reflecting an adjusted OR (95% CI) of 1.77 (1.08-2.90) and 1.79 (1.06-3.02), respectively, for women having 4 to 5 and more than 5 household members. However, there were no significant differences between HDD and some sociodemographic factors such as trimester of pregnancy, electricity connectivity (P = .823), TV ownership (P = .111), and food security status (P = .083) of the pregnant women after adjustment for potential confounders.
Sociodemographic Characteristicsa Associated With HDD of Pregnant Women.
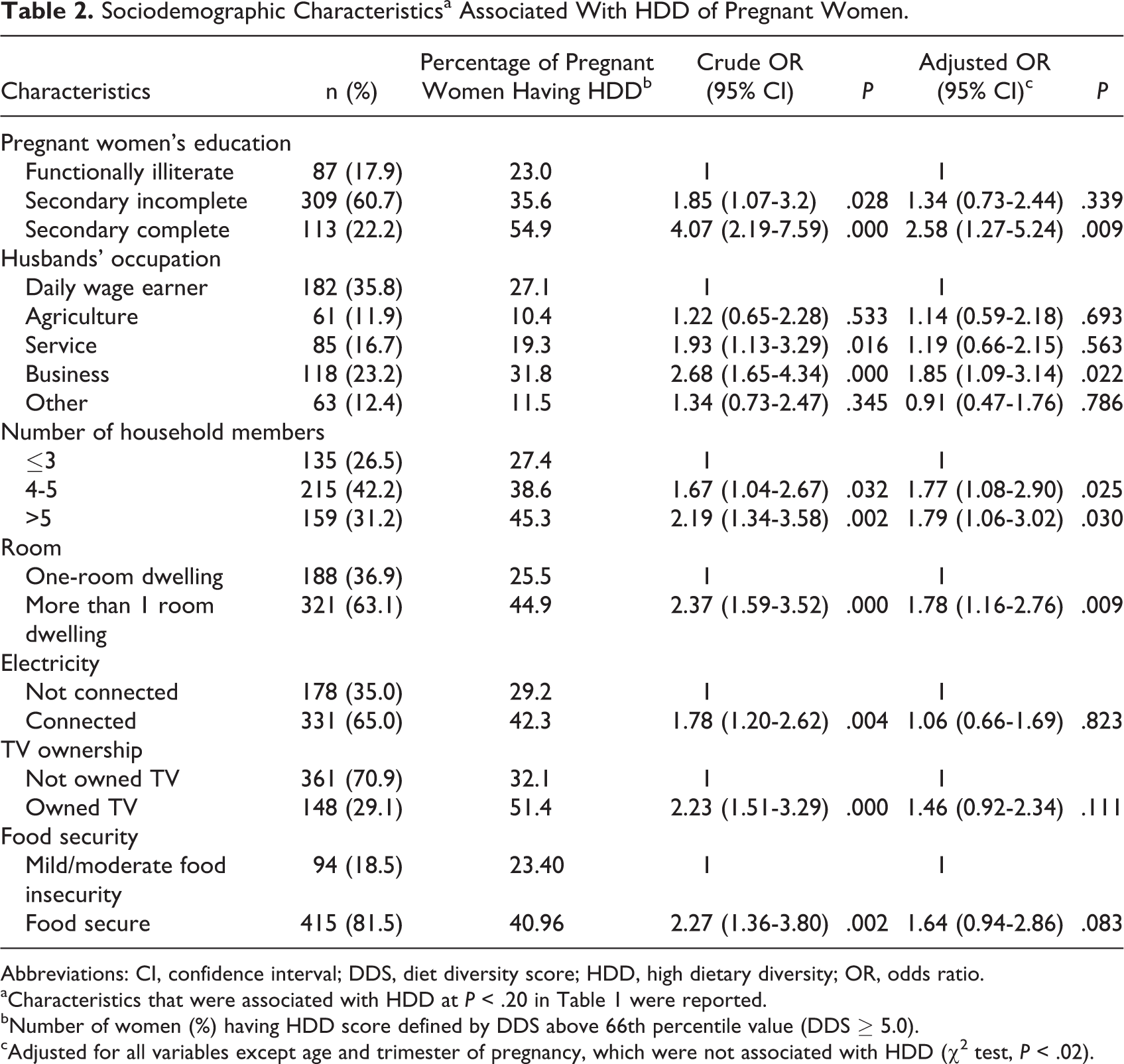
Abbreviations: CI, confidence interval; DDS, diet diversity score; HDD, high dietary diversity; OR, odds ratio.
aCharacteristics that were associated with HDD at P < .20 in Table 1 were reported.
bNumber of women (%) having HDD score defined by DDS above 66th percentile value (DDS ≥ 5.0).
cAdjusted for all variables except age and trimester of pregnancy, which were not associated with HDD (χ2 test, P < .02).
The overall DDS (Table 3) of the pregnant women was low, mean (CI): 4.28 (4.19-4.38). The mean DDS in unadjusted analysis was significantly lower (P < .05) among functionally illiterate pregnant women, mean (CI): 3.80 (3.60-4.00) compared to women with secondary incomplete and secondary complete level of education, mean (CI): 4.24 (4.13-4.35) and 4.77 (4.55-4.99), respectively. The DDS of pregnant women whose husband was a daily wage earner or whose husband’s occupation was agriculture was significantly low, mean (CI): 4.01 (3.86-4.15) and 4.15 (3.88-4.41), respectively, compared to those whose husbands were engaged in service, business, or other occupation, mean (CI): 4.48 (4.25-4.71), 4.60 (4.40-4.80), and 4.33 (4.04-4.61), respectively. Interestingly, DDS was found to be significantly lowest among pregnant women in households of 3 or fewer family members, mean (CI): 4.04 (3.88-4.20), compared to other pregnant women in households of 4 or more family members, mean (CI): 4.28 (4.13-4.42) and 4.48 (4.30-4.66), respectively. Moreover, DDS was found to be significantly higher among pregnant women dwelling in houses having more than 1 room, mean (CI): 4.45 (4.32-4.57) and 4.00 (3.86-4.13), respectively, having electricity connection, mean (CI): 4.43 (4.31-4.55) and 4.01 (3.86-4.16), respectively, owning a TV, mean (CI): 4.64 (4.46-4.82) and (4.14 4.02-4.24), respectively, and being food secure, mean (CI): 4.38 (4.27-4.48) and 3.84 (3.64-4.04), respectively. However, after adjustment for potential confounders, DDS was significantly increased among pregnant women who had secondary or higher level of education (P < .001), whose husbands’ profession was business (P = .010), having more household members (4 or more members; P = .002), dwelling in households with more than 1 living room (P = .024), and who were food secured (P = .005). Besides, we explored the food groups eaten by more than 50% of pregnant women having low (≤3 food groups), medium (4 food groups), and high (≥5 food groups) dietary diversity. Starchy staples, flesh foods and other small animal protein, and other fruits and vegetables were eaten by 50% or more women who had low or medium dietary diversity. On the other hand, more than half of the women who had HDD had also eaten legume and nuts, dairy, eggs, and DGLVs (data not shown).
Sociodemographic Characteristicsa Associated With Mean Changes in DDS of the Pregnant Women.
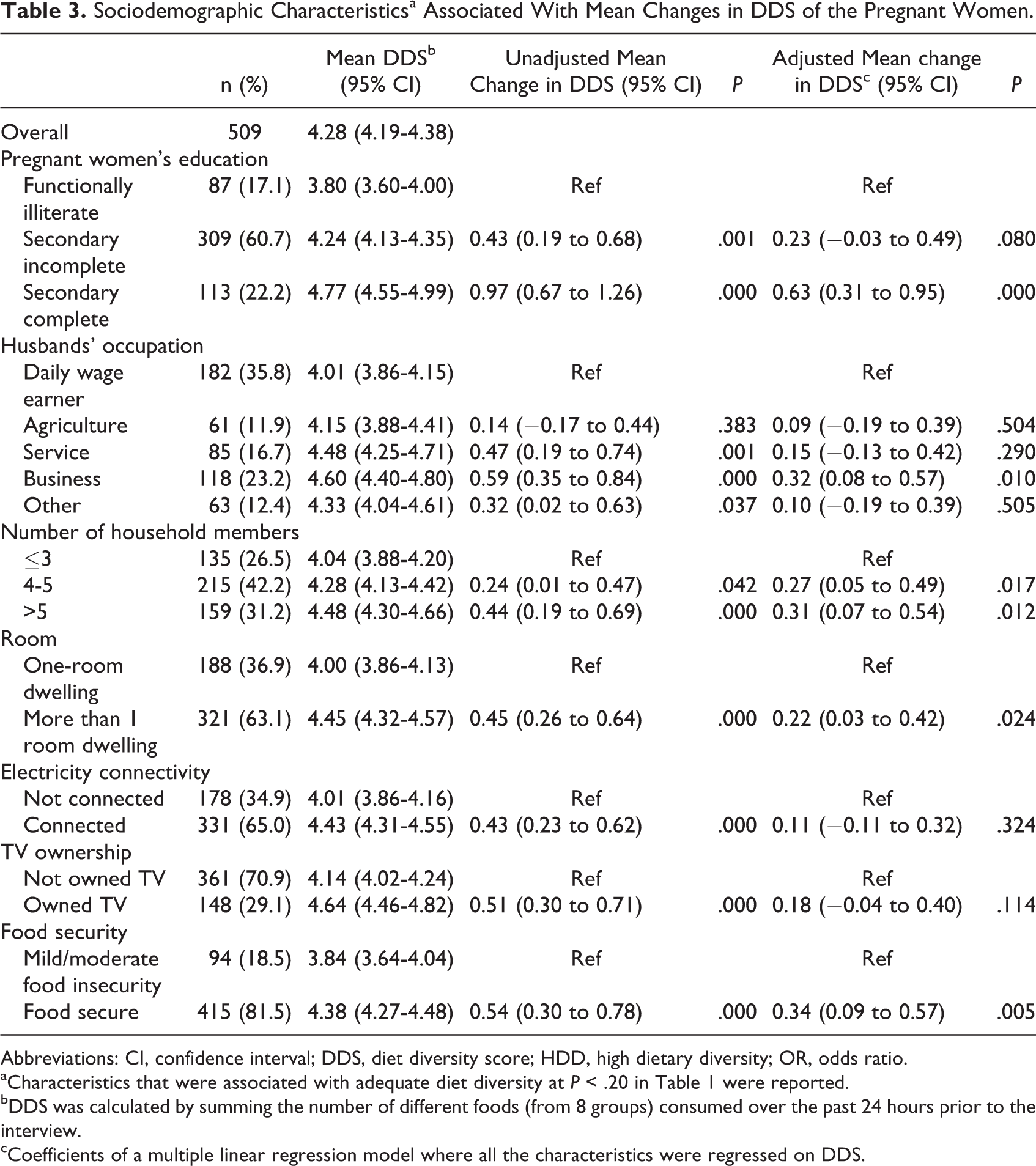
Abbreviations: CI, confidence interval; DDS, diet diversity score; HDD, high dietary diversity; OR, odds ratio.
aCharacteristics that were associated with adequate diet diversity at P < .20 in Table 1 were reported.
bDDS was calculated by summing the number of different foods (from 8 groups) consumed over the past 24 hours prior to the interview.
cCoefficients of a multiple linear regression model where all the characteristics were regressed on DDS.
We have also observed pregnant women’s knowledge and consumption of different food groups (Figure 1). All of the pregnant women consumed starchy staples. Most of them consumed flesh foods (86%), mostly fish. A relatively smaller proportion of pregnant women consumed dairy products, eggs, and leafy vegetables (16.9%, 28.3%, and 50.3%, respectively), despite two-thirds or more of the respondents (66.4%, 65.2%, and 72.9%, respectively) knowing that pregnant women should eat these foods. Knowledge about consumption of legumes and nuts (pulses) and vitamin A-rich fruits and vegetables was very low (11.0% and 6.5%, respectively). Although very few pregnant women consume the latter (5.7%), a significant percentage of women (42.8%) are eating legumes and nuts without realizing their health benefit.
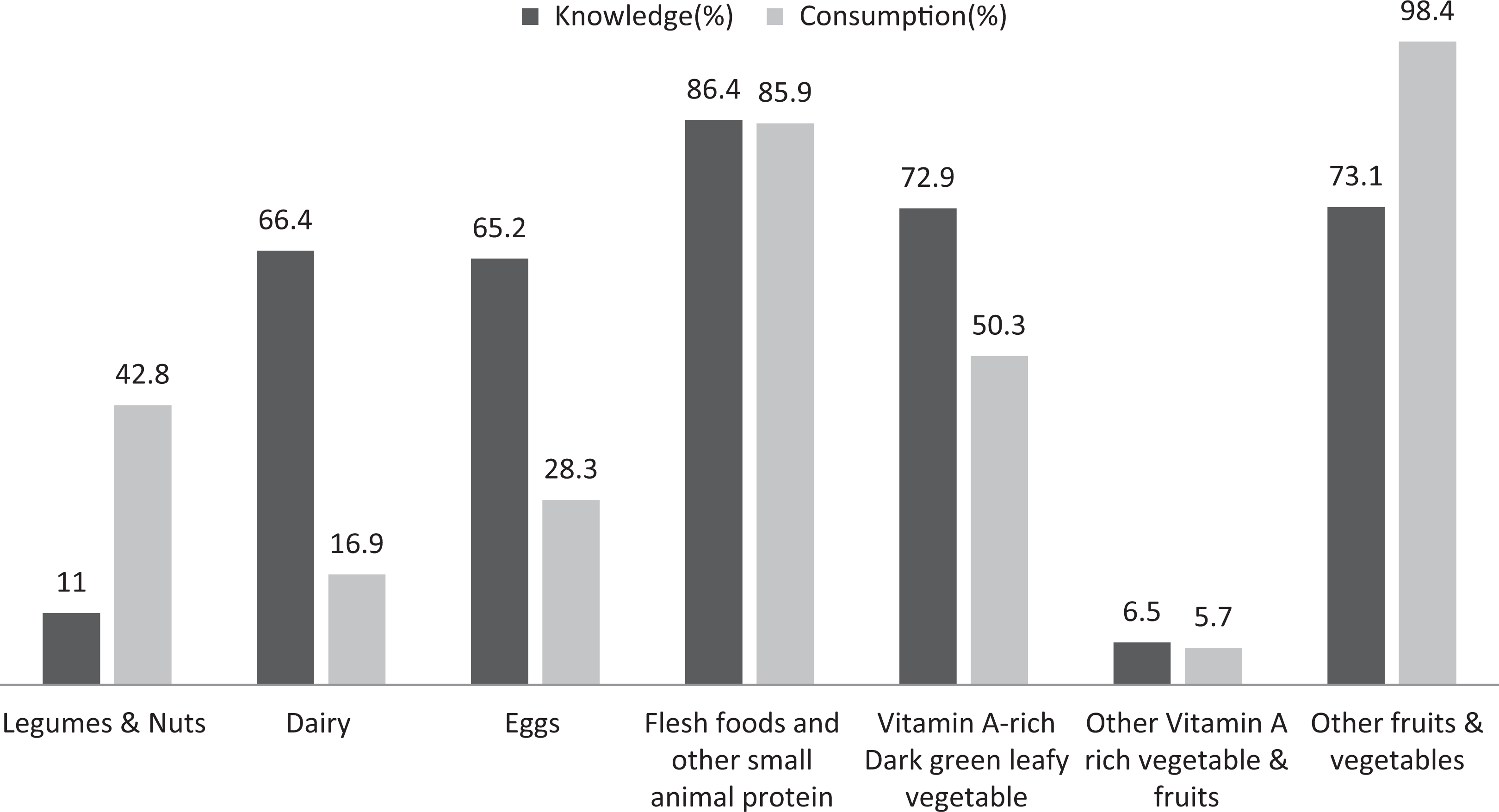
Pregnant women’s knowledge and consumption of selected food groups. 1
Given that fewer women ate dairy, egg, and DGLVs despite having knowledge about the importance of these foods, we analyzed social–demographic characteristics associated with the intake of these foods among pregnant women who know about the importance of these foods (Table 4). Educational achievement, husband’s occupation, dwelling size, electricity connectivity, TV ownership, and food security were associated with dairy food intake. All these characteristics except husband’s occupation were also associated with egg intake. However, consumption of DGLVs by pregnant women was not associated with any sociodemographic characteristics, except larger dwelling size.
Factors Associated With the Intake of Dairy Food, Eggs, and Leafy Vegetables During 24 Hours Prior to the Interview Among Pregnant Women Who Had Knowledge About Importance of These Foods.
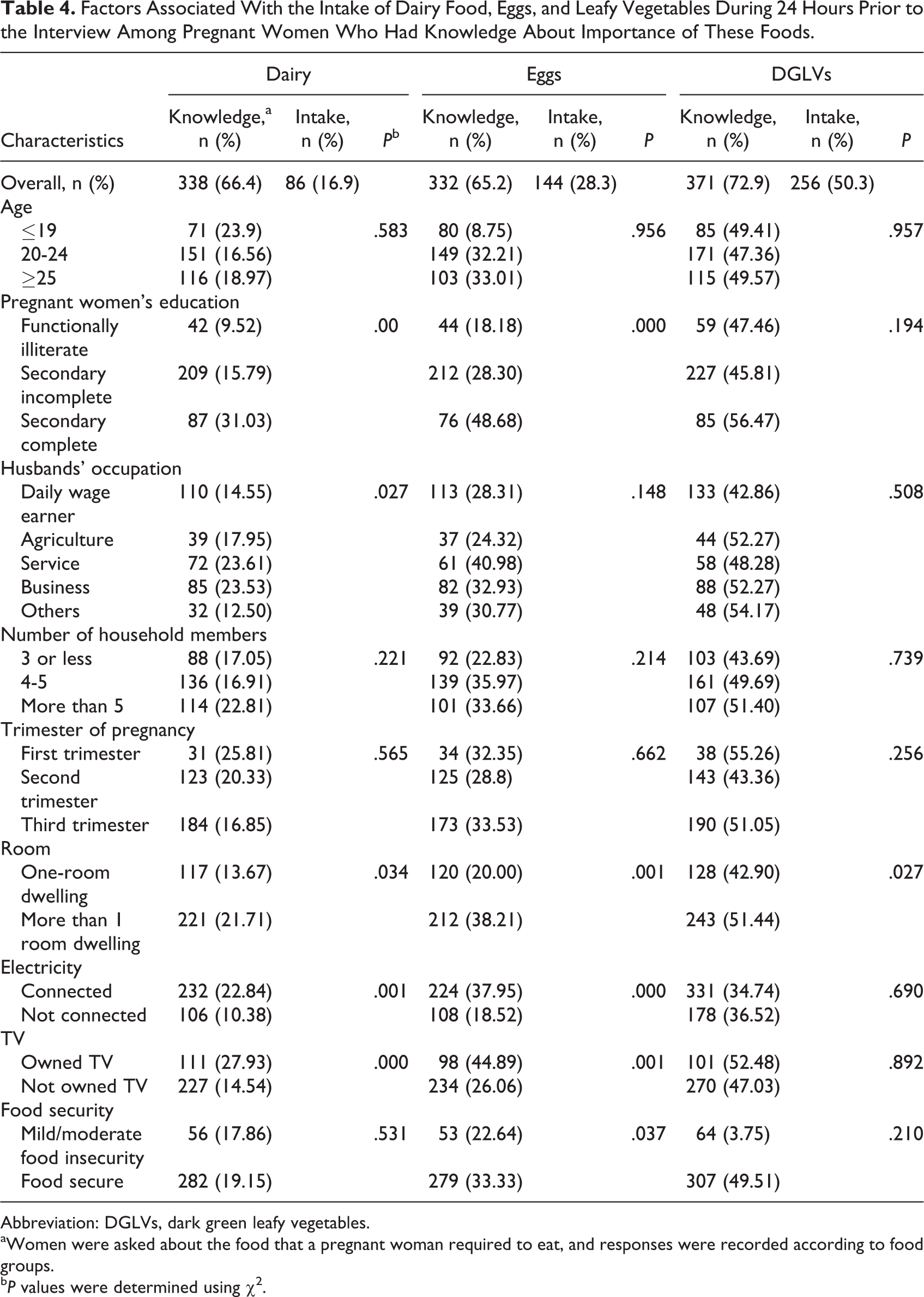
Abbreviation: DGLVs, dark green leafy vegetables.
aWomen were asked about the food that a pregnant woman required to eat, and responses were recorded according to food groups.
b P values were determined using χ2.
Discussion
Our results indicated an association between intake HDD and sociodemographic characteristics among a relatively large sample size of pregnant women from southwestern Bangladesh. The overall DDS was low (4.28). Different sociodemographic factors such as lower educational achievement, husband being a daily wage earner, smaller household size (3 or less family members), and smaller dwelling size indicated a group most at risk for both low mean DDS and low or medium diverse diet. Finally, we found large gaps between knowledge and consumption of 3 micronutrient-rich food groups including dairy foods, eggs, and DGLVs. In spite of having knowledge, consumption of dairy foods and eggs was low, and it was significantly associated with various sociodemographic characteristics. However, no significant association was found between sociodemographic characteristics and consumption of DGLVs.
Low DDS (4.5) similar to our study was also reported by Arimond et al 22 among Bangladeshi women of reproductive age, using the same definition of DDS. The consumption of 9 food groups was also similar in both the studies, except for eggs (28.3% and 7%), fish (85% and 72%), and other vitamin-rich vegetables and fruits (5.7% and 64%). 22 In Arimond et al’s study, 22 the data were collected in 1996, which might account for an improvement in the intake of eggs and flesh foods. Also, Arimond et al 22 included green and red chili as vitamin A-rich vegetables, but they were consumed only in nominal amounts as a spice, so we excluded them, which might explain such a large difference. Similar to our study, Arimond et al showed that none of the respondents consumed organ meat; similar findings were reported from 3 other developing countries. 22
Few researchers have reported determinants of diet diversity among women from South Asia. A recent study from Islamabad, Pakistan, reported that women’s diet diversity was not associated with any sociodemographic characteristics. 32 Similar to our analysis, Rashid et al 33 found significant roles of income, education, and other indicators as determinants of household diet diversity in Bangladesh; the authors reported that DDS was lower among rural Bangladeshi population who had low level of education. Similar to our findings, a study in West Bengal also showed that household DDS was higher in larger families. 34
We reported that only a few pregnant women consumed milk and eggs. It is known that dairy products, especially intake of cow milk during pregnancy, are efficient in providing many important nutrients for the development of fetus. 29 Consumption of egg is essential during pregnancy and lactation as it is one of the principle sources of choline—a vital diet component required for cell and brain development during pregnancy and early infancy. 35 Bangladesh Institute of Development Studies (BIDS) 36 reported that egg consumption in Bangladesh has doubled (3.2%-7.2% g/person/d) between 1995 and 2010, with production higher among small or marginal farms compared to medium or large farms. This suggests that egg consumption will be increasing in coming years, and there is a high scope of increasing egg production in poor families. Policy makers should consider promoting egg production and consumption among rural poor households and for women of reproductive age. Micronutrient-rich animal source foods are preferentially given to adult men in rural Bangladeshi households. 37 Because of the low affordability of such foods for poor households and it has also been reported that the intake is lower among pregnant women from lower socioeconomic status, household members should be educated to offer it to the women of reproductive age, adolescents, and children whenever it is available in the family.
Compared to the consumption of dairy foods and eggs, our analysis did not show any significant association with the sociodemographic indicators for DGLVs consumption as it may be considered an inferior food. However, vegetables are considered cheap and important sources of vitamin A, vitamin C, calcium, and iron. Also, production of vegetables and fruits in homestead gardens is cheaper and considered as source of higher diet diversity and nutrition utilization. 38 Therefore, educational intervention is needed to ensure that vegetable intake would be promoted.
Bangladesh is undergoing a nutritional transition, where high level of both overnutrition and undernutrition exists together at 17% and 24%, respectively. 2 Educational interventions have to emphasize reallocating family food budgets in favor of diverse foods as oppose to reliance on few calories of dense foods and give importance to improving the diet of pregnant women when diverse foods are available in the household.
We did not assess the quantity of food and nutrient intake and the nutritional status of pregnant women, which need to be studied further. However, our analysis identified vulnerable groups at risk of poor diet quality. We have shown that in spite of prevalent knowledge, gaps related to consumption of important food groups such as dairy, eggs, and DGLVs persist. Programs promoting adequate maternal diet need to address barriers related to increasing consumption of diverse foods, even when knowledge about such foods exists. Therefore, it is recommended that further formative research is needed to explain the gap between knowledge and practice of consuming DGLVs, dairy, and eggs for having a better targeted intervention.
Footnotes
Acknowledgments
The authors acknowledge the contribution of the field data collection team of CIPRB and the SHIKHA project implementation team of the health division of the BRAC and FHI 360. The authors also acknowledge contribution of Alamgir Kabir, ICDDR, B for providing valuable insights in developing the analysis plan.
Authors’ Note
A.A.S. conceptualized this analysis and led the writing, editing, and coordination of the manuscript; S.R.M., T.F., K.T., Z.R., and N.S. undertook the data analysis and contributed to the writing of the manuscript; A.F.R., S.R.M., S.R., R.H., and K.H. oversaw the design and supervised the overall data collection; T.G.S. and S.R. designed the SHIKHA project; And I.R., S.R.S., and M.R. contributed to the data analysis plan. All authors reviewed, commented on, and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was made possible with generous support of the American people (CA AID-388-A-13-00003) through the US Agency for International Development (USAID). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the US Government.