
Abstract
Background:
Vitamin A deficiency (VAD) remains a widespread public health problem in the developing world, despite changes in under-5 mortality rates, morbidity patterns, and intervention options.
Objective:
This article considers the implications of a changing epidemiologic and programmatic landscape for vitamin A (VA) programs.
Methods:
We review progress to prevent VAD and its health consequences, assess gaps in VA status and intervention coverage data, and assess data needed to guide decisions regarding the optimal mix, targeting, and dose of VA interventions to maximize benefit and minimize risk.
Results:
Vitamin A supplementation programs have contributed to the reduction in under-5 mortality rates, but alone, do not address the underlying problem of inadequate dietary VA intakes and VAD among preschool-aged children in the developing world. A combination of VA interventions (eg, supplementation, fortified foods, multiple micronutrient powders, and lipid-based nutrient supplements) will be required to achieve VA adequacy in most settings. Current efforts to measure the coverage of multiple VA interventions, as well as whether and how much VA children are receiving, are few and fragmented.
Conclusions:
Where intervention overlap exists, further effort is needed to monitor VA intakes, ensuring that targeted groups are consuming adequate amounts but not exceeding the tolerable upper intake level. Vitamin A status data will also be critical for navigating the changing landscape of VA programs. Data from these monitoring efforts will help to guide decisions on the optimal mix, targeting, and exposure to VA interventions to maximize public health benefit while minimizing any potential risk.
Background
The epidemiologic landscape for interventions aimed at improving vitamin A (VA) status and preventing VA deficiency (VAD)-related mortality in preschool-aged children has changed over the past 2 decades. Under-5 mortality has dropped by almost 50% in many countries since 1990. 1 Modest improvements have also been documented in exclusive breast-feeding rates, which rose from ∼34% in 1990 to ∼39% in 2010, 2 and measles immunization coverage, which increased from 72% to 84% over the same period. 1 Overall, child survival initiatives have achieved major reductions in deaths due to measles, diarrhea, and malaria during the past decade. 3
Vitamin A interventions have contributed to the reduction in under-5 mortality rates and progress toward the child survival Millennium Development Goal. Globally, semiannual VA supplementation (VAS) remains the most prominent means for controlling VAD-related mortality and xerophthalmia. 4 A growing number of low- and middle-income countries are implementing large-scale VA fortification of sugar, wheat, and/or oil, targeting the general population. There have also been initiatives to introduce and expand the use of home fortification products containing VA, such as micronutrient powders (MNP), among children under the age of 5 years. Pilot programs are introducing similar lipid-based “multi-nutrient” supplements (LNS), such as Plumpy’Doz, for the prevention or treatment of undernutrition. Both home fortification and LNS are designed to be consumed 2 to 3 times per week.
Child survival gains and the broadening scope of VA programs have not happened uniformly across all countries or regions. However, they do form a backdrop of change, raising questions about if and when to scale back universal VAS, the appropriate mix of VA interventions, and the potential risk of VA toxicity.
Prevention of Vitamin A Deficiency and Associated Public Health Consequences
Vitamin A deficiency remains a widespread public health problem among women and children in the developing world. Twenty-nine percent of all preschool-age children 5 (∼190) and nearly 8% of all pregnant women (∼10 million) are estimated to have VAD and its adverse health consequences. 6 Vitamin A deficiency remains the leading cause of preventable childhood blindness in the world and a leading cause of morbidity and mortality among preschool-aged children. 7 -9 Vitamin A deficiency also appears to extend through the preadolescent years, 10 although both its scope and its health consequences during this period of life remain uncertain.
Guidelines for preventing VAD in the preschool years have long been available, 11 practiced, 12 and periodically reaffirmed and updated to take into account new scientific information and programmatic experiences. 13 The strength of existing evidence continues to inform and justify global policies and programs to prevent VAD and its associated public health consequences during the preschool-age years.
The scientific basis for providing twice-annual, high-dose VAS for children 6 to 59 months to reduce risks of mortality and nutritional blindness is unequivocal. 14 -16 The impact of VAS has been demonstrated in diverse populations, with child mortality rates ranging from 5.3 to 126.2 per 1000 child years and estimates of baseline VAD ranging from 1.9% to 13.2% based on xerophthalmia and 37.5% to 56.9% based on serum retinol concentration less than 0.7 µmol/L. 14 Well-executed, population-based, mostly randomized and placebo-controlled field trials enrolled and followed ∼165 000 children between the ages of ∼6 to 12 months through 72 months. The investigative teams employed a range of study designs and dosage regimens across Southern Asia (ie, Indonesia, India, and Nepal) and Sub-Saharan Africa (Ghana and Sudan). These studies and analyses by different authors arrived at the same conclusion: VA interventions—whether periodic supplementation or smaller doses on a regular basis, for example, via fortified food products—reduce child mortality by 23% to 34%. 14 Recent estimates of the number of deaths attributable to vitamin A deficiency range between 105,700 5 and 160,000 9 . Although most of the VAS mortality trials were not powered to test impact on specific causes of mortality, the mortality effect is likely explained, in part, by an ability of VA to lower case fatality from measles and mortality from severe diarrhea, dysentery, and febrile illness. 14
Evidence from these trials was translated into international guidelines, the most recent of which was released by the World Health Organization (WHO) in August 2011. 13 National programs in populations where VAD is considered a public health problem typically deliver 1 dose of 100 000 IU for 6- to 11-month-olds or 2 annual doses of 200 000 IU for children 12 to 59 months of age as a child survival intervention. Giving a high dose of VA twice annually is based on the principle that a single large dose of VA is highly absorbed, stored in the liver, and mobilized, as needed, over an extended period of time. 12 This dosing schedule is also considered feasible for most at-risk countries, where health infrastructures are generally poor and unable to reach children at more frequent intervals. Distribution efforts generally target all children in the 6- to 59-month age range and are most commonly operated on a national scale. However, unlike “blanket” interventions such as fortification of staple foods, supplementation can be targeted as needed to specific population groups or regions depending on the distribution of VAD within a country and coverage of other interventions.
Progress to Date
Approximately 80 countries currently implement VA programs—the vast majority of which are centered on supplementation. 17 Early VAS programs generally achieved high once-annual coverage of children by being “piggy backed” onto National Immunization Day campaigns for polio eradication. 17 In some African countries, this remains a mode of VA delivery. But in most other countries, as polio eradication activities ceased or became subnational, VAS delivery has transitioned to semiannual Child Health Weeks. Many countries package VAS with other preventive health services targeted to young children, including deworming, catch-up immunizations, growth monitoring, nutrition education, and screening for acute wasting. 18 Thus, the cost-effectiveness of delivering VAS through the Child Health Week platform depends in part on the extent to which delivery costs can be shared among multiple interventions and is built into existing health systems. 18
Global coverage rates for twice-annual VAS have improved from 16% in 1999 to ∼65% in 2013—progress that has been cited as a major public health success story. 17,19 This success at the global level, however, masks wide country-to-country variation in coverage. Perhaps more importantly, it may distract from the significant proportion of regularly unreached children, mostly in rural, poor communities. This latter “hard-to-reach” group may be more likely to be at increased risk of severe morbidity and mortality attributable to VAD in some settings. 20 Sustainability is also a concern. Although countries such as the Philippines have supported integrated VAS programs for over 15 years, 18 programs of this nature depend on continued political commitment and financial resources. Both commitment and resources may wane as other, more visible, and politically expedient interventions are rolled out.
While VAS programs have contributed to the reduction in under-5 mortality rates, alone they do not address the underlying problem of inadequate dietary VA intakes and chronic VAD among preschool-aged children in the developing world. Food fortification offers a direct and potentially sustainable way to correct VAD. The aim of such programs is to add VA to a staple food or condiment at a level that would correct an existing dietary deficiency in target groups, without posing significant risks of overdosing among those who habitually consume a large quantity of the fortified product. 21 To select appropriate food vehicles and fortification levels, WHO recommends collecting information on the amount of “fortifiable” food consumed as well as total nutrient intakes from all sources. 22 The information on total nutrient intake permits estimation of the intake “gap” or the amount of additional nutrient that is needed to meet theoretical requirements for each population subgroup. The amount of food vehicle consumed and its distribution within the population can then be used in conjunction with total nutrient intakes to calculate appropriate fortification levels.
To date, sugar has been the most successful vehicle, with its public health effectiveness being well-established in Central America 23,24 as discussed in paper 1 of this series. Oil is relatively easily fortified with VA and at relatively low cost, and many countries have established large-scale programs, including parts of West Africa. 21,25 Experimental testing of VA-fortified staple grain products has shown favorable results on the VA status of children in the Philippines. 26 Over the past decade, industrial-scale fortification of sugar, vegetable oil, and wheat 27 has been expanding throughout Asia and Africa. However, with the exception of sugar fortification programs, 23,24 there have been few evaluations of the nutritional or public health impact of large-scale food fortification programs.
Efforts are also ongoing to promote the production and consumption of VA-rich foods. There have been limited data on the efficacy and effectiveness of these interventions, although information is beginning to accumulate on biofortified crops. Efficacy trials testing provitamin A-rich varieties of sweet potatoes 28 and maize 29 have reported improvements in VA status. Promotion of orange-fleshed sweet potato in Uganda increased VA intakes and serum retinol concentrations among children. 30 One advantage of these strategies in the context of multiple, overlapping programs is that these approaches provide provitamin A carotenoids, as opposed to preformed VA, and thus would not be expected to contribute to excessive intakes; however, much work remains to scale-up these strategies.
Most recently, several major initiatives have been put in place to roll out multinutrient interventions—many including preformed VA—in the form of MNP. Approximately 60 countries have implemented or are planning to implement MNP programs, although this effort has only reached a national scale in 5 countries to date. The extent to which released MNP or other food-based multinutrient interventions are contributing to VA intakes or status in targeted children (ie, 6- to 24-month-olds) is not well known.
A Global Need for Micronutrient Status and Intervention Coverage Data
A recent paper by Stevens et al reports regional trends in VAD from 1991 to 2013. Based on a pooled analysis of 134 population-representative data sources, Stevens and colleagues report significant declines in VAD prevalence in east and southeast Asia and Oceania from 42% to 6%, and Latin America and the Caribbean from 21% to 11%; however rates in sub-Saharan Africa and South Asia have remained high and virtually unchanged at 48% and 44%, respectively. 5 Characterizing the magnitude, severity, and distribution of VAD across population risk groups is needed to plan appropriate strategies for prevention. Yet the majority of VAD prevalence data come from surveys conducted in the 1990’s. 5 There is a need to update the prevalence of VAD and other micronutrient deficiencies at the country, regional, and global levels with representative sampling and reliable and valid indicators and to facilitate the rapid dissemination of this information.
Dietary assessment can also provide insight regarding the relative contributions of low dietary intake and other factors (eg, infectious disease) that may contribute to biochemical deficiency. In addition, knowing the coverage levels of ongoing interventions and their contribution to VA intake is also needed to adjust intervention levels, targeting, and intervention mixes. Relatively good estimates exist for coverage with VA supplements, although the validity of these estimates may be questionable in some countries or contexts (eg, in emergency settings). Monitoring efforts for fortification programs vary widely across countries, but very few countries capture data on coverage with adequately fortified foods or consumption among specific age-groups. Coverage data for MNP may be collected via routine health information systems or surveys. For interventions such as fortification or MNP in which variable “doses” of VA are delivered, the definition of coverage must be considered. For example, in some cases, it may be sufficient to simply record whether a product was consumed at all during a specific time period. Other situations may require more in-depth data on the frequency of consumption, quantitative intake estimates, or the fortificant level in food vehicles at the point of sale or consumption. For fortification or food-based interventions, assessments should focus on filling the “intake gap”, that is, the minimum additional amount needed to achieve adequate dietary intake of a nutrient. 22 This approach requires measurement of total nutrient intakes, which is resource intensive but has nevertheless been applied successfully in a number of low- and middle-income countries. For some programs, multiple definitions of coverage (eg, “reach”, “effective coverage”, etc) may be useful.
In addition, with current data, there is lack of resolution with regard to intervention overlap. There is an urgent need to assess coverage of all VA interventions at the child level—both for the purpose of identifying those not yet reached with interventions to prevent VAD-related mortality and xerophthalmia and to monitor the potential risk of chronic excessive intakes.
Assessing Vitamin A Status for Planning and Evaluating Interventions
The ability to accurately, but feasibly, assess VA status in individuals and communities using responsive indicators is fundamental to quantifying the prevalence and severity of VAD; maintaining surveillance of a population over time; and designing, monitoring, and evaluating programs. Although valid methods exist for research, there is an ongoing and urgent need to refine, simplify, and lower the cost and processing times required to assess population VA status. There are often trade-offs between the detail and precision of information obtained and the cost, time, and technical capacity required for analysis.
The selection and use of monitoring indicators for VA interventions will differ depending on the program objective and implementation phase. In some cases, process indicators such as the availability of MNP in health facilities will be used; in others, biological indicators are appropriate. The indicators and tools that are likely to be useful for program impact evaluations should be selected based on consideration of (1) the purpose of the evaluation; (2) the type of VA program/intervention; (3) the target group intended for the VA program/intervention; (4) the indicator’s validity, reliability, and potential responsiveness relative to the VA program/intervention; and (5) feasibility within the cultural context and evaluation setting. Clear guidelines are needed to assist countries to select, use, and interpret appropriate impact indicators.
Assessment of VA intake and status is necessary during the planning stages of programs in order to determine the severity of deficiency and to identify population groups or geographic regions that would be most likely to benefit. Data on nutrient intakes from all sources (eg, from 24-h dietary recalls or weighed records) can also be used to predict the impact of interventions to increase VA intake as has been previously shown. 31 -33 The results of these simulations can be used to develop intervention strategies that are most likely to be effective in a specific population.
There is a growing interest in measuring the impact of VA programs in countries that have implemented national-scale programs for several years. Serum retinol concentrations do not respond to VAS, except in a transient manner (ie, for 1-2 months). While the kinetics of this transient effect have not been well characterized, it presumably reflects the rapid use of VA to support its biological functions when background dietary intake is low and/or VA losses resulting from infections. 34,35 Serum retinol concentration is therefore not recommended as an impact indicator where VAS is the only strategy for addressing VAD. 35 For this reason, the impact of VAS programs is not measured by a change in VAD prevalence in the population, and the mortality impact is instead modeled using coverage data. Serum retinol concentrations are, however, responsive to improved dietary intakes, sustained over time, and therefore can guide programmatic decisions about whether to maintain or change intervention mixes. 35 Thus, using serum retinol distributions among preschool-aged children—in conjunction with other vitamin A status markers or demographic/ecologic risk factors—from cross-sectional surveys to assess the need for VA interventions is still recommended, even in countries that have sustained high semiannual VAS coverage over several years. 36
With respect to monitoring the impact of VA fortification programs and other interventions that increase daily VA intake, evidence suggests that large-scale programs can be expected to shift distributions of serum retinol over time; thus, retinol is an appropriate indicator of response to these programs. 35 Several other biochemical indicators may also be appropriate; reviews of the advantages and limitations of these indicators are available 37 and are discussed further in paper 3 of this series. For example, plasma retinol binding protein (RBP) concentrations have been used more recently in large-scale surveys (eg, Cameroon) and could be expected to respond in a similar manner to plasma retinol. 38 Breast milk retinol concentration has also been suggested as a population-level indicator of VA status and response to interventions 36 because milk retinol reflects both maternal VA status and infant VA intake and responds rapidly to increased dietary VA. Some countries, such as Guatemala, have established nutritional surveillance systems that permit monitoring population VA status over time. 23 Where such systems are lacking, or where the costs of undertaking a biochemical assessment are prohibitive, efforts should be made to monitor quality assurance of the fortification process at the production facility, during packaging, storage, and transport, at retail outlets, and in homes. In addition, discretionary fortification of packaged foods with micronutrients, including VA, is increasingly common, even in low-income countries. Although not an official intervention program, this additional source of VA in the diet can be substantial and thus should be monitored. In the United States, for example, voluntarily fortified breakfast cereal alone provides 17% of total dietary VA among children aged 2 to 8 years. 39
A New Framework for Vitamin A Programs
The Global Alliance for Vitamin A convened a technical consultation in February 2012 to outline a framework for shifting from universal high-dose VA supplementation toward interventions that could sustainably eliminate VAD. 40 The consultation underscored the premise that addressing VAD, by any means, has a clear public health impact on child survival and xerophthalmia. However, it is further recognized that high-dose VA supplementation, while protective in the short term, will not improve VA status for an extended period. In contrast, there is good evidence to suggest that interventions that improve dietary intakes via regular consumption of adequately fortified foods or other food-based interventions are more likely to shift a population’s serum retinol distribution toward sustained adequacy.
Given the proven child survival benefits of VAS, the consultation highlighted the need for strong and compelling evidence to inform appropriate scaling back of this intervention. The consultation recommended that decisions to scale back or shift from universal VAS be made when governments can assure and verify that vulnerable populations have an adequate and sustained VA status from dietary and other interventions. Using the WHO VAD prevalence cutoffs to define a public health problem as a guide, a threshold of documented and verified subclinical VAD prevalence of <5% was proposed as a basis for scaling back or withdrawing universal VAS among preschoolers.
The decision points in the proposed framework for VAS programs are based on documenting the prevalence of subclinical VAD at the population level. In the absence of up-to-date cross-sectional biochemical data on preschool children, it first asks that countries examine the evidence for adequate VA intake among risk groups. This can be achieved via dietary assessments, or, where dietary data are lacking or inadequate, through a combination of coverage and daily VA “dose” data from food-based interventions. When available evidence suggests that VA intakes are adequate, a biochemical status survey is recommended to assess VA status among the risk groups.
Serum retinol concentration, when used in conjunction with other status markers or data on risk factors, is currently recommended for population-based assessment of VA status and serves as the global standard for defining VAD. 36 Retinol binding protein is increasingly used as a suitable proxy for retinol, reducing cost and technical capacity requirements for population-level assessments. However, there are known limitations for both serum retinol and RBP, 41,42 particularly in the context of infection and inflammation, but methods are available to assess and account for the influence of inflammation on both measures. 43, 44 Several decades worth of data from multiple countries illustrate the influence of supplementation alone or sustained improvements in dietary intake on the distribution of serum retinol concentrations in a population. 35 Following supplementation, the population’s retinol distribution improves for a period of 1 to 2 months and then returns to baseline levels. 35 By contrast, improving regular intakes of VA has a demonstrable impact on status, shifting the population’s serum retinol distribution toward adequacy. 35 Over time, if intakes are increased to and maintained at adequate levels, the distribution stabilizes at adequacy. 35 While these data come from the fortification literature, a similar improvement in the serum retinol or RBP distribution would also be expected to occur with other dietary interventions and/or overall improvements in health and nutrition. It is important to note that, in order to reflect adequacy of intake from the food supply alone, status surveys should be carried out at least 8 weeks following high-dose supplementation. 35 Planning should also take seasonality into account, potentially scheduling the field period during or just following periods of greatest concern for dietary inadequacy and/or infectious disease burden.
In the absence of population status data, countries are urged to continue to achieve high levels of preschool VAS coverage. Where VAS is the sole intervention, coverage levels ≥80% can be plausibly linked to lower child mortality and xerophthalmia risk. As supplementation does not address the underlying cause of VAD, successful programs will require a mix of interventions in order to increase dietary VA intakes to adequate levels. In countries that have demonstrated adequate and stable serum VA concentrations in specific regions or age-groups, but not in others, using a more targeted or subnational approach is justified. As the number of countries implementing large-scale VA-fortification programs increases and the use of other products containing VA (eg, MNP and LNS) expands, mechanisms are needed to monitor VA intake from overlapping interventions to guide program targeting, optimize intervention mixes, and minimize risk of excessive VA intake.
Safety of Vitamin A Programs
With the increased breadth of VA programs in select countries, there is concern that interventions intended to address the consequences of deficiency may be introducing a risk of toxicity to children who are already adequately nourished. 45 This risk can be assessed by measuring dietary VA intakes or biological indicators of VA stores, which is discussed further in paper 3 of this series. Excessive VA intakes are generally defined by consumption greater than the tolerable upper intake level (UL). 46 It is important to note that the UL applies only to preformed retinol intake and not to VA derived from carotenoids. Thus, additional dietary VA from fortified-food products, MNP, or LNS “counts” in the characterization of excessive intake, but additional provitamin A carotenoids provided via biofortified crops would not affect the prevalence of intakes above the UL. Retinol intake from high-dose supplements is generally not captured in dietary assessments, as they are given once every 6 months, and kinetic modeling suggests that the supplemental dose is completely metabolized over that period of time. 34 However, the impact on VA stores after multiple years of exposure to periodic supplementation is not known and warrants further investigation.
Defining risk based on excessive intakes is limited by the UL, as we currently lack data linking long-term VA intake to biological signs of toxicity. 46 As a result, adult values are extrapolated to children. Additionally, the UL includes an “uncertainty factor” to extrapolate from the lowest observed adverse effect level (LOAEL) to the UL. 46 The uncertainty factor relies heavily on expert opinion regarding the severity of adverse effects, likely interindividual variability in sensitivity, and for some data, extrapolation from animal models. 46 Thus, the UL is intentionally conservative; the potential adverse effects of chronic daily VA intakes between the UL and the LOAEL are not known. There are reports available of individuals with excessive intakes (defined using the UL) in the absence of any observed symptoms of toxicity. 47 The biological relevance of the UL is an urgent research priority.
Nonetheless, quantitative dietary assessments among the target population can provide estimates of the proportion of individuals exceeding the UL, with a particular focus on VA-fortified foods. Where implementation of independent dietary intake surveys is not feasible due to cost or time constraints, Household Consumption and Expenditure Surveys may provide useful information on dietary patterns and potential risk of inadequate and excessive intakes. In the absence of such data, it may also be possible to extrapolate information regarding excessive intakes from program coverage data. However, as noted earlier, current methods for measuring coverage of multiple VA interventions are fragmented. Going forward, it will be essential to capture data on whether children are receiving each intervention as well as a quantitative assessment of VA intakes from these combined efforts. It may be possible to integrate this effort with existing postevent coverage assessments for VAS campaigns or other coverage surveys by adding questions that simultaneously monitor the delivery of other nutrition and health programs, such as MNP and fortified foods.
To address safety concerns, biological indicators that reflect excessive liver VA stores can also be measured. When the liver’s VA storage capacity is exceeded, the proportion of VA circulating as retinyl esters begins to increase. 48 A cutoff of >10% of retinol circulating as esters has been proposed as indicative of excessive liver stores. 48 However, methodological challenges remain regarding the measurement and interpretation of serum retinyl ester concentrations as a marker of excessive VA stores. This is discussed further in paper three of this series.
Direct measurements of status that might indicate a safety concern are currently limited. Although serum retinol and RBP are accepted as indicators of deficiency, they do not capture risk at the upper end of the status distribution due to homeostatic controls. 37 Some researchers have suggested the use of retinol isotope dilution (RID) techniques as a means to monitor risk, as this method is informative across a wide range of VA status and allows quantification of liver VA stores. While RID is a powerful tool for highly controlled intervention trials, there is a need for further data to establish its validity in individuals and populations with inflammation, enteropathies, parasitic infection, exposure to aflatoxin, and selected micronutrient deficiencies, especially iron deficiency. Data are also needed to inform meaningful cutoffs of excessive VA intake and status for population assessments.
Finally, although still requiring validation with hepatic biopsy or necropsy, simulation models based on whole-body kinetics from tracer studies may be useful to predict the risk of high hepatic VA concentration under varying scenarios (ie, different assumptions regarding initial pool size; VA intake from breast milk and other dietary sources; and exposure to VA from supplements and/or fortified foods). 34
Conclusions and Research Needs
Although the epidemiology of VAD and the landscape of intervention programs have changed since the early VA mortality trials, the strength of existing evidence continues to inform and justify global policies and programs to prevent VAD among preschool-aged children. 9,49 Vitamin A supplementation remains a cost-effective and appropriate intervention to reduce child mortality in settings where VAD is a public health problem. 13 In this changing programmatic landscape, however, updated estimates of VA status at both the national and the subnational levels are critical. Guidelines are needed to inform the frequency of assessments, representative sampling, reliable and valid indicators, and the use of results to guide VA programs as summarized in Table 1. Although valid methods exist for assessing VA status in individuals and communities, there is an ongoing and urgent need to refine, simplify, and lower the cost and processing times for population VA status assessments.
Key Needs for Optimizing Vitamin A Intervention Packages, Program Monitoring, and Safety.
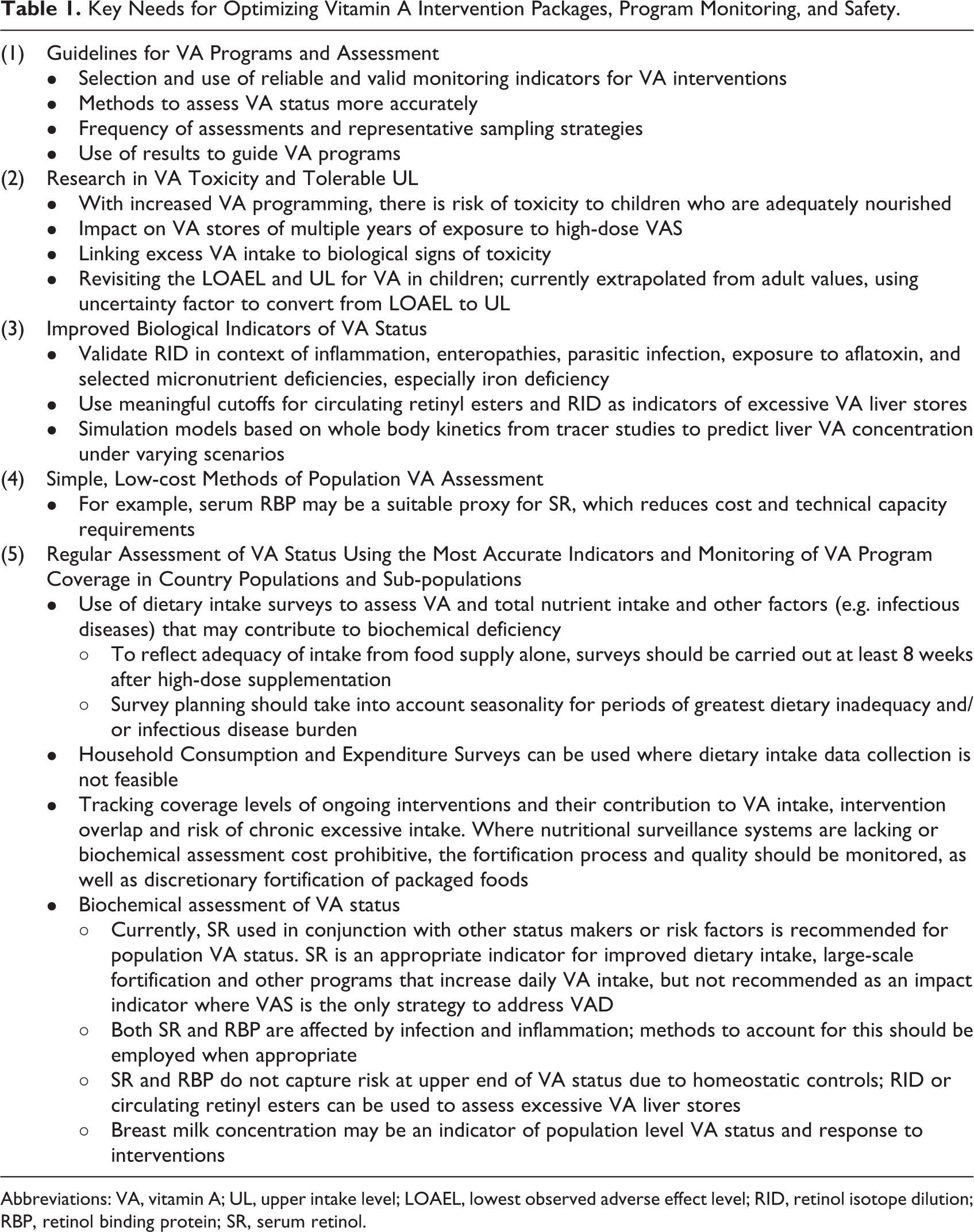
Abbreviations: VA, vitamin A; UL, upper intake level; LOAEL, lowest observed adverse effect level; RID, retinol isotope dilution; RBP, retinol binding protein; SR, serum retinol.
A combination of VA interventions (eg, VAS, fortified foods, MNP, and LNS) will be required to achieve VA adequacy in most settings. However, countries should be collecting information regarding whether and to what extent these interventions are reaching the same children. Methods to assess the contribution of multiple VA interventions to total VA intake and status are also needed. As these data become available, the programmatic community will require guidance on how best to use this information to modify intervention targets, to formulate doses and/or mixes, to minimize cost, and to minimize risks of excessive intakes. Simulation models based on whole-body kinetics may be useful to predict risk of high hepatic VA concentration under varying scenarios but require further validation.
The risks of VAD and child survival benefits of improving the VA status of preschool-aged children are well established. While there is no obvious benefit for healthy individuals to consume levels of VA above the UL, the risks of exceeding this limit need further investigation. All public health decisions need to weigh the benefits against potential risks of intervening or not intervening. Valid and reliable data on VA status, intake levels, and coverage of interventions at national, if not subnational levels, are essential for this risk: benefit analysis and for guiding decisions on the optimal mix, targeting, and dose of VA interventions to maximize benefit and minimize risk.
Footnotes
Acknowledgments
We thank Najat Mokhtar and Ken Brown for their comments on the manuscript.
Author’s Note
Rolf D.W. Klemm and Amanda C. Palmer drafted the manuscript. All authors contributed, read, and approved the final manuscript, and are responsible for the final content. Content of this article reflects the personal opinion of the authors, not necessarily the policy position of their organizations. This is paper 2 in a series of meeting reports from an International Atomic Energy Agency Technical Meeting (TM-48778) held in Vienna, Austria; March 24-25, 2014; entitled “Assessing Vitamin A Safety in Large-Scale Nutrition Intervention Programmes: Setting the Research Agenda”. Sherry A. Tanumihardjo acted as guest editor for this series.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.