
Abstract
Vitamin and mineral (micronutrient [MN]) deficiencies are common in lower income countries, especially among young children and women of reproductive age. These deficiencies are cause for serious concern because of their high prevalence and their associated complications, which include depressed immune function and increased risk and severity of infections, impaired neurocognitive development, and anemia, which together result in elevated mortality and reduced human productive capacity. A broad range of different intervention strategies are available to control MN deficiencies. At present, these interventions are usually implemented at a national scale through different public and private sector entities, often with little coordination. We have developed a set of models based on the estimated ability of different interventions to achieve effective coverage and the necessary financial resources required to deploy these interventions. The models provide a unified and transparent framework for considering different options using the common indicator of effective coverage. More specifically, information on nutritional benefits and costs are analyzed using an economic optimization model to identify the mix of interventions that could be delivered to specific target groups in particular geographic areas to achieve a desired level of effective coverage at lowest cost. Alternatively, these optimization models can be developed to identify the combination of interventions needed to achieve the maximum effective coverage, given specified budgetary limitations. The results of these models can be useful input into policy-making processes. To introduce this analytical approach, the set of papers in this volume addresses the problem of vitamin A deficiency among young children in Cameroon.
Prevalence and Complications of Selected Micronutrient Deficiencies
Vitamin and mineral (micronutrient [MN]) deficiencies are common in lower income countries (LICs), especially among young children and women of reproductive age (WRA) because of their relatively high MN requirements. The World Health Organization estimates that 33% of children <5 years of age and 15% of pregnant women are deficient in vitamin A (VA), as indicated by low serum retinol concentration <20 µg/dL, 1 and the International Zinc Nutrition Consultative group estimates that 17% of individuals in LICs are at risk of zinc deficiency, based on the amount of absorbable zinc in national food supplies. 2 Other MN deficiencies of recognized public health importance include deficiencies of iron, iodine, folate, and other B vitamins. 3 –6
These deficiencies are cause for serious concern, both because of their high prevalence and their associated complications, which include depressed immune function and increased risk and severity of infections, impaired neurocognitive development, and anemia, which together result in elevated mortality 7 –9 and reduced human productive capacity. 10,11 According to somewhat conservative estimates published in the second Lancet Nutrition Series, 8 more than 400 000 excess deaths of under-5 children occur annually due to childhood vitamin A and zinc deficiencies and to iron and folate deficiencies among pregnant women, which represents 6.3% of all young child deaths (Table 1). However, for several reasons, these figures probably underestimate the true mortality impact of MN deficiencies. For example, the Lancet analyses did not consider the impact of maternal VA deficiency on infant mortality during the first 6 months of life, whereas recent analyses indicate that early infant mortality may be reduced by ∼13% among supplemented infants of VA-depleted mothers. 12 Moreover, the Lancet papers did not include estimates of the effects of maternal zinc supplementation on excessive infant mortality due to prematurity. Thus, the impact of MN interventions may be nearly 2-fold greater than suggested by the Lancet papers.
Total Number of Under-5 Child Deaths Attributable to MN Deficiencies Among Children and Pregnant Women.
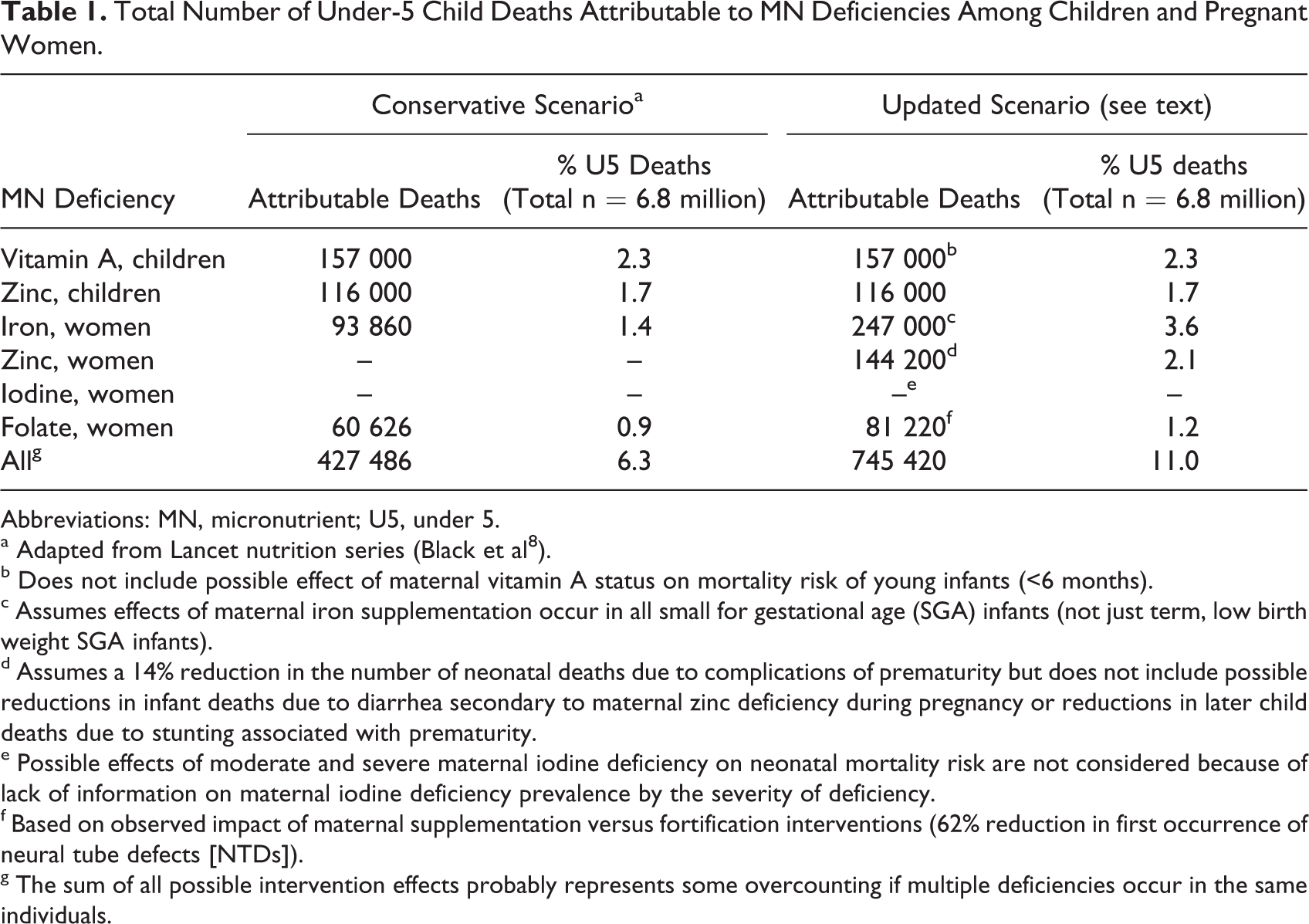
Abbreviations: MN, micronutrient; U5, under 5.
a Adapted from Lancet nutrition series (Black et al 8 ).
b Does not include possible effect of maternal vitamin A status on mortality risk of young infants (<6 months).
c Assumes effects of maternal iron supplementation occur in all small for gestational age (SGA) infants (not just term, low birth weight SGA infants).
d Assumes a 14% reduction in the number of neonatal deaths due to complications of prematurity but does not include possible reductions in infant deaths due to diarrhea secondary to maternal zinc deficiency during pregnancy or reductions in later child deaths due to stunting associated with prematurity.
e Possible effects of moderate and severe maternal iodine deficiency on neonatal mortality risk are not considered because of lack of information on maternal iodine deficiency prevalence by the severity of deficiency.
f Based on observed impact of maternal supplementation versus fortification interventions (62% reduction in first occurrence of neural tube defects [NTDs]).
g The sum of all possible intervention effects probably represents some overcounting if multiple deficiencies occur in the same individuals.
Using slightly more liberal assumptions than used in the 2013 Lancet nutrition series, and also considering the effect of maternal zinc deficiency during pregnancy on the risk of prematurity, we estimate that as many as 745420 under-5 children may succumb each year because of MN deficiencies, which represents 11.0% of all young child deaths (Table 1). The true attributable mortality risk of MN deficiencies probably lies somewhere between these 2 sets of estimates. Whichever attributable mortality estimate is correct, the toll is unacceptably high, and large-scale intervention programs are needed to achieve high levels of effective coverage of vulnerable population groups to prevent these deficiencies.
Definitions of Program Coverage and Issues of Inadequate, Unnecessary, and Redundant Coverage
Before considering the possible impact of different intervention strategies for controlling MN deficiencies, it is worthwhile reviewing several concepts concerning program coverage. Program “reach” refers to the percentage of individuals in a particular population who are exposed to an intervention program, regardless of their underlying health or nutritional status. By contrast, program “coverage” refers to the percentage of individuals in the population who are identified as being affected by the health condition (ie, a particular MN deficiency in the case of the present discussion) or at high risk of the condition (eg, because of low dietary intake) and who are exposed to the program. Only these deficient or high-risk individuals have the capacity to benefit from the intervention, so, ideally, they should be targeted by the program. Of course, high program coverage does not necessarily ensure that the MN deficiency problem will be resolved in a particular individual unless the quality and intensity of the intervention are sufficient to overcome the deficiency. Thus, the term “effective coverage” refers to the percentage of individuals in the population who are initially deficient, or at high risk of deficiency, and who are both exposed to the program and change from a condition of deficiency to nondeficiency (or from inadequate to adequate dietary intake) following program exposure.
Incomplete program coverage of individuals at high risk of deficiency leaves them vulnerable to the health and other complications described earlier. On the other hand, unnecessary reach of programs to unaffected individuals results in inefficient program expenditures and a possible risk of inducing excessive intakes and associated toxicity. Thus, efficient programming should attempt to maximize effective program coverage of deficient individuals and minimize its reach to those who are not deficient. The challenge, then, is how to select which interventions are able to target the deficient or higher risk individuals most efficiently.
In the analyses presented in this series of papers, we focus primarily on how best to achieve effective coverage of the target populations, using currently available and potential future intervention strategies, rather than focusing on just program reach or coverage. We have selected this particular indicator of program impact (ie, effective coverage) because it is most consistent with the objectives of public health programs, namely, to reduce the prevalence of the deficiency diseases most cost effectively.
Selection of Intervention Strategies for Controlling MN Deficiencies
A broad range of different intervention strategies are available to control MN deficiencies, including intermittent or continuous preventive or therapeutic MN supplementation, large-scale or targeted food fortification, behavior change efforts to encourage greater consumption of MN-rich foods (including optimal breast-feeding practices), agricultural interventions (including biofortification) to increase the year-round availability of and access to such foods, food processing to enhance MN uptake from these foods, and health interventions (such as deworming and diarrhea control) to maximize MN absorption and utilization. 13
At present, these interventions are usually implemented at a national scale through different public and private sector entities, often with little coordination. For example, MN supplementation and specific health interventions are typically managed by the public health sector, food fortification is implemented by private industry (often with regulatory guidance from public sector health and/or commerce or trade agencies), and modifications of food production fall within the province of the agricultural sector. Few guidelines exist to assist policy makers and program planners in selecting the optimal intervention or mix of interventions to control specific MN deficiencies with greatest efficiency. This problem may be further compounded by the lack of timely and sufficiently disaggregated information on the population’s MN status or risk of deficiency to allow for subnational programming to target higher risk population subgroups. Moreover, planning is often accomplished with a fairly short-term time perspective, which may discourage consideration of interventions that require a longer period of development before achieving measurable benefits. Finally, different donors and political interest groups may favor one or another approach, without considering the full range of possible intervention strategies. Given this set of uncertainties and competing interests, a more systematic approach is needed for prioritizing MN intervention programs.
Use of “Bioeconomic” Modeling for Policy Formulation
To address this challenge, our research group proposes using a set of models based on the estimated ability of different interventions to achieve effective coverage, and the necessary financial and other resources required to deploy these interventions. The combined sets of information are analyzed using an economic optimization model to identify the mix of interventions that should be delivered to specific target groups in particular geographic areas to achieve a desired level of effective coverage at lowest cost. Alternatively, these optimization models can be developed to identify the combination of interventions needed to achieve the maximum effective coverage, given specified budgetary limitations.
As described in more detail in the subsequent papers in this series, these models are developed in several steps. First, information must be obtained on the distribution of the MN deficiency or risk of deficiency within the broader population, to be able to estimate the coverage and effective coverage of different interventions. Second, information is needed on the actual or potential reach of these interventions and their ability to transform an individual from deficient to nondeficient status, or to convert them from inadequate to adequate intake. Third, information is needed on the financial cost of delivering these interventions to the targeted population groups (and other possible constraining factors, like available personnel and transportation infrastructure). Finally, the information generated on predicted impact and estimated costs of the various interventions is analyzed using economic optimization modeling to determine the most cost-effective set of interventions that should be deployed to specific target groups over selected periods of time.
We refer to these combined analyses as “bioeconomic” optimization modeling because they rely both on knowledge of the biological impact of different interventions and information on the resources required to implement these interventions. Ultimately, the results of these analyses must be considered in the context of the sociopolitical, cultural, and financial circumstances in particular countries before policy decisions are finalized. The models provide a unified and transparent framework for considering different options using the common indicator of effective coverage. We have now applied this analytical framework to examine the most cost-effective intervention strategies for addressing MN deficiencies among young children and WRA in selected settings. For the sake of simplicity in introducing this analytical approach, we confine the current presentation to the problem of VA deficiency in Cameroon, as explained subsequently.
Vitamin A Deficiency in Cameroon
We selected Cameroon for the present case study because (1) most of the information required for the optimization modeling was already available, (2) our partners in the Helen Keller International country office in Cameroon offered to assist with generating and interpreting additional relevant information, and (3) local counterparts in the Ministry of Health and international donor community in Cameroon expressed a strong interest in this approach. Cameroon is also particularly suited for this work because of its sizable regional and urban–rural differences in food availability, food choices, and program delivery costs, which make targeted, subnational programming especially advantageous.
The information on MN status used in the current analyses was derived from a sample survey completed among young Cameroonian children (12-59 months of age) and WRA in 2009. The survey methods and results have been described previously in detail. 14,15 Briefly, the study sample was selected to provide representative information for 3 distinct geopolitical macroregions: the Northern region (comprising the Far North, North, and Adamawa provinces), the Southern region (comprising the remaining provinces), and the 2 major metropolitan areas (Douala and Yaoundé). Information was collected on VA status, based on plasma concentration of retinol binding protein (RBP) adjusted for systemic inflammation, and on VA intake, using quantitative 24-hour dietary recall histories. Information was also obtained to determine whether the children had received a high-potency VA supplement during the past 6 months and, if so, where it was received. Finally, the caregivers were questioned about consumption of potentially fortifiable, industrially processed foods, including edible oil, bouillon cubes, wheat flour, and sugar by the index child and the caregiver.
As illustrated in Figure 1, the risk of VA deficiency varied by geopolitical region, regardless of whether deficiency was defined in terms of low plasma RBP concentration or inadequate VA intake. According to the RBP results, 43% of children in the North had low plasma RBP concentration, compared with 29% of those in the South and 37% of those in the cities. Likewise, children in the North were more likely to have inadequate dietary intake of VA than those in the other regions. Similar patterns were observed among the women. Regional differences were also observed in the reach of the national delivery program for high-potency VA supplements, which are distributed during semiannual child health days. Specifically, 89% of children in the North had received a VA supplement in the last 6 months, compared with 64% of those in the South and 58% of those in the cities (Figure 2). We also discovered that households in the different regions had different likelihoods of consuming potentially fortifiable foods. 14 Finally, we learned during subsequent data collection efforts that the financial cost of delivering VA supplements varied by region, largely depending on the regional population density and the agency responsible for implementing the program (Figure 3). This regional variability in the distribution of VA deficiency and potential reach and cost of different VA intervention platforms implies that subnational programs might be more efficient than national ones.
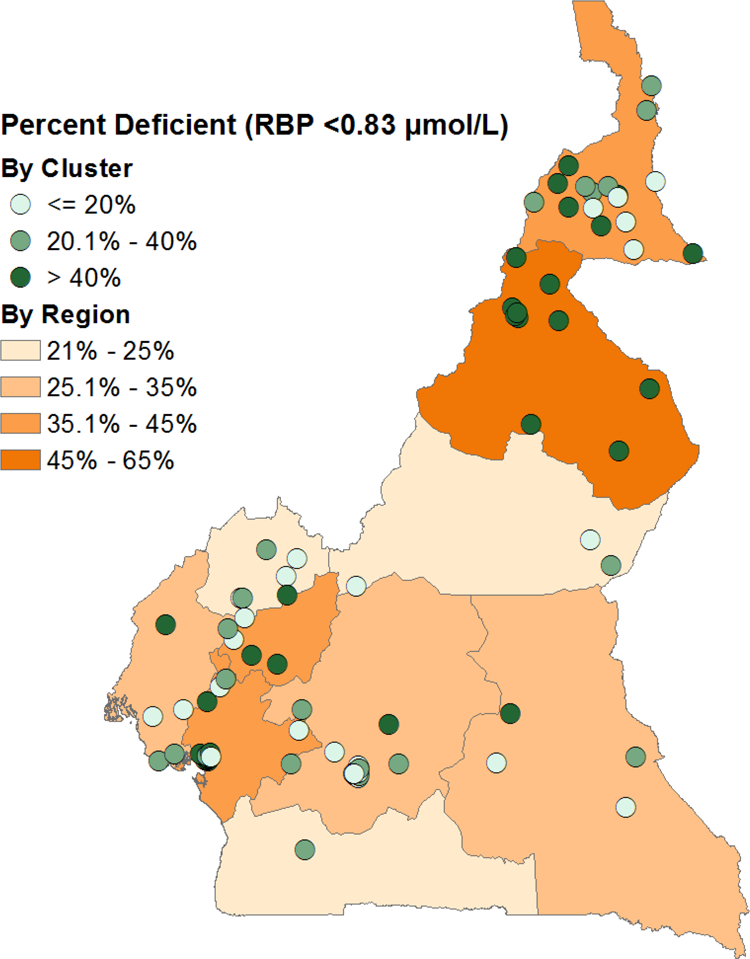
Prevalence of vitamin A deficiency (defined as inflammation-adjusted plasma retinol binding protein <0.83 µmol/L) among Cameroonian children 12 to 59 months of age, by region.
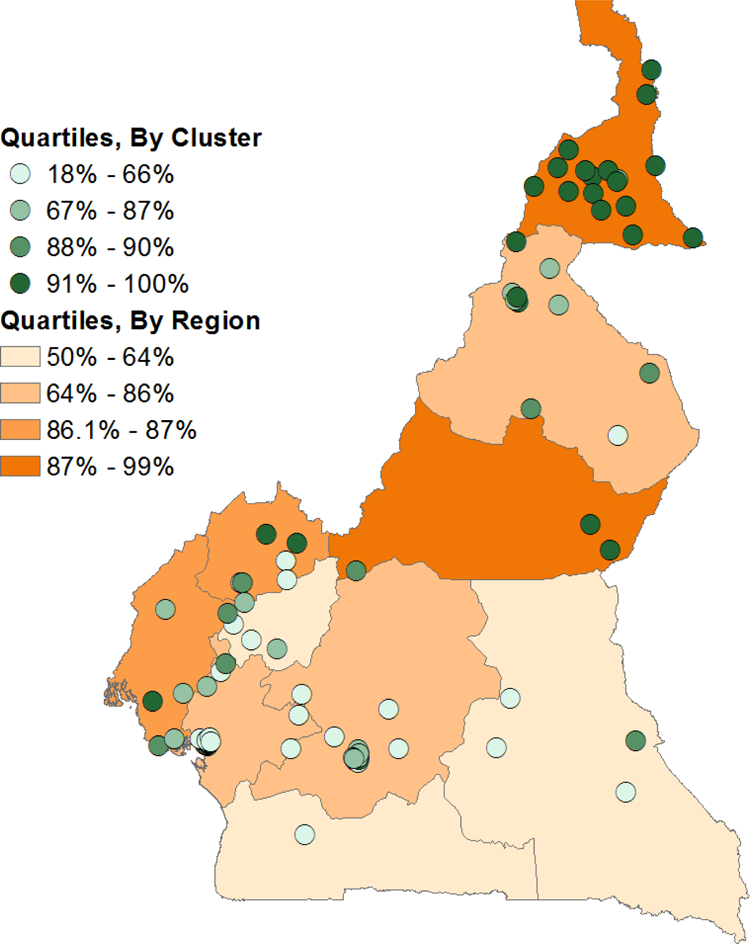
Percentage of Cameroonian children 12 to 59 months of age who received high-dose vitamin A supplementation during the previous 6 months, by region.
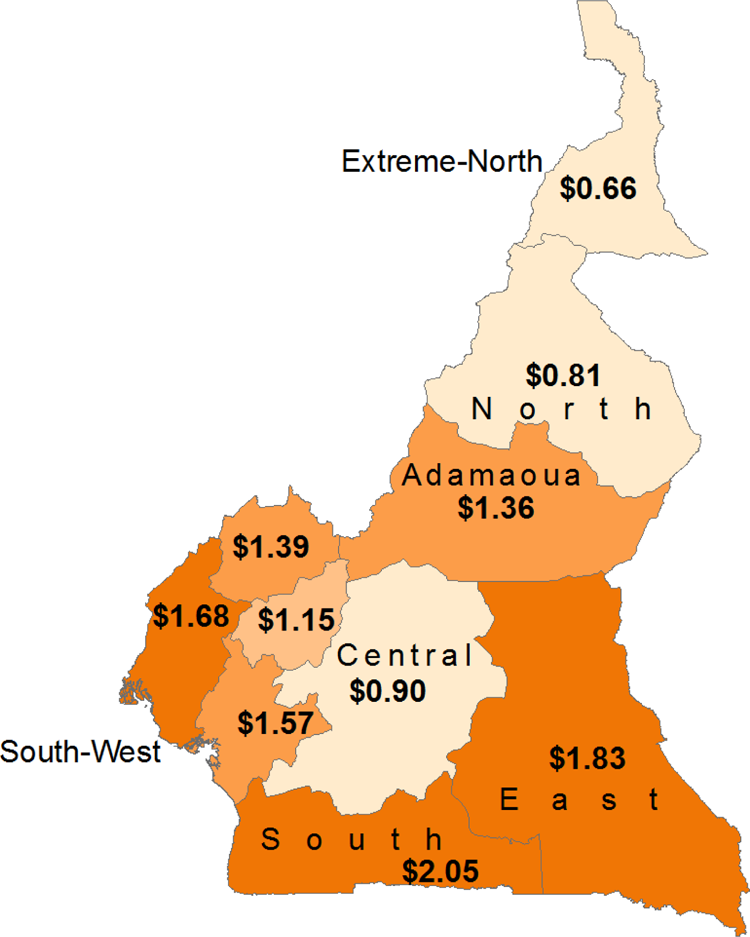
Estimated cost per targeted child for delivery of high-dose vitamin A supplements to Cameroonian children 6 to 59 months of age during Child Health Days, by region.
As suggested earlier, and discussed in greater detail in recent publications 16,17 and the forthcoming BOND Vitamin A Expert Panel report (under review), several different methods can be used to assess VA status and the risk of VA deficiency. Specific biomarkers of VA status, such as inflammation-adjusted plasma retinol or RBP concentration, provide information on current VA status. By contrast, dietary VA intake data can only be used to assess the risk of inadequate intake. Notably, in Cameroon, the VA biomarker and the dietary intake data identified the same high-risk groups for VA deficiency. Thus, we were able to use the dietary data as our indicator of effective coverage, albeit not without some challenges, as explained in the subsequent paper in this series (Engle-Stone). 18 The advantage of using the dietary data to determine effective coverage is the ability to estimate the impact of different interventions on dietary intake, hence the percentage of the population with dietary adequacy or inadequacy before and after different interventions. By contrast, the impact of different interventions on plasma retinol and RBP concentrations is not known for all types of interventions, which limits the ability to compare these interventions using the same outcome. For this reason, we used the change in the percentage of the population with adequate VA intake as our indicator of effective coverage.
Overview of Subsequent Papers in this Series
To describe each of the steps used to complete the optimization modeling, we have prepared a set of 4 papers. Following this current brief overview, the second paper (Engle-Stone et al) 18 presents the methods used to estimate the impact of different VA intervention strategies on dietary VA intake and on the percentage of the population with adequate intakes, by macroregion. In other words, the paper illustrates the effective coverage that can be achieved by different intervention strategies, using the dietary intake information. The third paper (Kagin et al) 19 provides the methods used to determine the costs of planning and delivering different types of intervention programs, by region (where appropriate), including the spatial and temporal dimensions of costs and the estimated cost per individual reached or effectively covered by these programs. The fourth paper (Vosti et al) 20 describes the economic optimization model and the results obtained for estimating the most efficient VA delivery strategies, considering subnational approaches over a 10-year time frame, and compares the effective coverage and costs of a newly proposed mix of interventions with “business as usual.” Finally, in the fifth paper (Baker) 21 , we have invited several individuals with experience in planning and implementing nutrition interventions to comment on this approach from the perspectives of policy makers and program managers. In other analyses, not included in the present series, we have also considered the potential influence of effective coverage on mortality attributable to VA deficiency, which can affect the ultimate choice of program target groups, by preferentially focusing on those with greatest mortality risk.
Limitations of Optimization Modeling
Despite our enthusiasm for this approach, we also recognize some of its limitations. First of all, the current models just focus on single MNs, whereas many types of intervention programs can deliver multiple MNs simultaneously. Thus, the analytical framework will still need to be expanded to encompass consideration of multiple MNs. Second, we discovered during early applications of this method that the results can vary according to the target groups and outcomes selected. For example, selected interventions may have different impacts on breast-fed versus non–breast-fed children or on children versus WRA, and different interventions might be prioritized when selected just to maximize coverage versus effective coverage. Third, the current models only estimate the effects of MN intervention programs on health and mortality outcomes, without considering possible simultaneous effects of specific health interventions, such as diarrhea control or immunization programs, on these same outcomes. Similarly, it must be recognized that certain interventions may have effects above and beyond their nutritional effects, which are not accounted for in the model. For example, deworming may have other health benefits beyond its direct effect on VA absorption. Finally, there is a considerable cost required to obtain the subnationally disaggregated data sets needed for these analyses and to complete the modeling and final interpretations, but as we will show in the fourth paper, the potential savings gained from more efficient programming, based on the modeling results, may far outweigh the cost of obtaining and analyzing the necessary information.
Conclusion
In this series of papers, we describe the advantages of using bioeconomic optimization modeling as decision-support tool for selecting the most efficient set of interventions to address MN deficiencies. A case study of this method, which was applied for prioritizing VA intervention strategies in Cameroon, suggests a tremendous potential for program cost savings using this systematic decision-making approach. Strengths and limitations of the method and remaining research issues are described in the following papers.
Footnotes
Acknowledgments
We appreciate helpful comments on earlier versions of this manuscript that were contributed by Robert E Black, Rafael Flores-Ayala and Roland Kupka.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded, in part, by a grant from the Bill & Melinda Gates Foundation to the University of California, Davis.