
Abstract
Background:
Nutrition interventions targeting the first 1000 days show promise to improve nutritional status, but they require effective implementation. Formative research is thus invaluable for developing such interventions, but there have been few detailed studies that describe this phase of work within the Scaling Up Nutrition (SUN) movement.
Objective:
To inform a stunting prevention intervention in Cabo Delgado, Mozambique, by describing the sociocultural landscape and elucidating characteristics related to young child food, illness, and health.
Methods:
This formative research utilized a rapid assessment procedures (RAP) approach with 3 iterative phases that explored local perceptions and behaviors around food and illness among the Macua, Mwani, and Maconde ethnic groups. Ethnographic methods, including in-depth interviews, direct observations, free lists, and pile sorts, were used to collect data from community leaders, caregivers, and children 6 to 23 months. Data were analyzed drawing from grounded theory and cultural domain analysis.
Results:
Geographic differences drive sociocultural characteristics amid 3 ethnic groups that allow for segmentation of the population into 2 distinct audiences for behavior change communications. These 2 communities have similar classification systems for children’s foods but different adult dietary patterns. Small-quantity lipid-based nutrient supplement did not fall into the existing food classification systems of either community, and participants preferred its promotion through community leader channels. Community members in both groups have little recognition of and perceived severity toward nutrition-related illnesses.
Conclusion:
Within Cabo Delgado, the cultural heterogeneity yields substantial differences related to food, illness, and health that are necessary to consider for developing an effective nutrition intervention.
Keywords
Introduction
Developing effective behavior change interventions as a core component of nutrition activities is becoming increasingly important. 1 To date, 50 countries have joined the Scaling Up Nutrition (SUN) movement and more are likely to follow as the international nutrition community makes strides in improving key infant and young child nutrition indicators, and governments work to meet the 2015 Millennium Development Goals (MDGs), including MDG 1.C and MDG 4, which focus on halving the number of people who suffer from hunger and reducing by two-thirds the under-5 mortality rate, respectively. 2
Central to these efforts is the implementation of 13 evidence-based, nutrition-specific, and nutrition-sensitive interventions which have the potential to make the largest impact on infant and child health in the most cost-effective manner. Among them, the activities with the largest predicted effects on child mortality include the treatment of severe acute malnutrition, zinc supplementation, and the promotion of optimal infant and young child feeding (IYCF) practices, including adequate breast-feeding and appropriate use of complementary foods. 3
For many vulnerable populations in resource-limited settings, the lack of access to nutrient-rich, energy-dense complementary foods throughout the year is a great challenge. Infant diets in these contexts are usually cereal based and lack the nutritional adequacy for healthy growth and development. 4 One current measure to help overcome this nutritional impasse is the utilization of specialized nutritious foods such as micronutrient powders (MNPs) or lipid-based nutrient supplements (LNSs). 5
Specialized nutritious foods have great potential to positively impact the nutritional status of infants and young children, but like other public health tools such as insecticide-treated bed nets and condoms, they require substantial and sustained engagement in a new behavior by beneficiaries. There is ample evidence to suggest that with thoughtful formative research and planning, behavior change interventions can in fact positively improve IYCF practices, nutritional status, and growth. 6
With the advent of MNP and LNS, as well as the recognition that strong communications are necessary for effective nutrition behavior change programs in general, more projects now include formative research to inform intervention development and implementation. 7 –11 It is widely recognized that household food utilization is dictated not only by availability of and access to food resources but also by a complex host of interrelated factors including but not limited to gender roles and relations, local attitudes toward food and illness, and sociocultural rules that govern dietary behavior. 12 –16 These factors, coupled with the rich cultural diversity within contexts where undernutrition interventions are most often needed, are important considerations when designing and implementing nutrition interventions. There still, however, remain large gaps in knowledge related to the sociocultural drivers of food and specialized nutritious food utilization as well as beneficiary knowledge, attitudes, and practices regarding it within actual programs. Currently, the implementation science, a burgeoning field of research that supports the translation of evidence-based health care or prevention from a knowledge base into practical programming, 17 is lagging behind the basic nutritional science that shows the potential of nutrition interventions with such products to impact positively upon IYCF behaviors and nutritional status.
Objective
The objective of the formative research was to inform the design and implementation of a government of Mozambique integrated nutrition intervention in Cabo Delgado province as part of the SUN movement. Our research questions for this particular portion of the formative work were as follows: How do the sociocultural characteristics of the primary cultural groups in the intervention area compare and contrast in terms of conceptualization of health, illness, nutrition, and nutritional deficiency? What cultural perceptions and household behaviors exist related to food classification systems, nutrition-related illnesses, and food-related practices?
Answers to the research questions were used to generate context-specific recommendations for generating an effective and culturally appropriate behavior change communications (BCC) strategy.
Methods
Study Setting
This formative research was conducted in 7 districts in the southeast quadrant of Cabo Delgado, the northernmost province in Mozambique (note 1; Figure 1). This rural province is home to approximately 1 700 000 people. It has high agricultural potential with a favorable climate for farming. However, it is especially vulnerable to environmental shocks such as floods, which have negatively affected agricultural output and food security in recent years. 18

Map of Mozambique. (Note 3).
Due to chronic food insecurity, adult and young child diets in this setting are monotonous and predominantly include starchy roots and cereals that negatively impact nutritional status. Cassava, sorghum, and maize are the primary staple foods consumed, with added relishes or accompaniments that include a variety of seasonal vegetables (eg, cassava leaves). Small fish are a common source of animal protein in coastal areas. 18 Among children under 5 years of age, the highest prevalence of stunting (52.7%) exists in the country, 10% higher than the national average (42.6%), and underweight in the province (20.6%) is higher than that of the country (14.9%). The infant mortality rate in Cabo Delgado is 82 per 1000 live births. 19
Nutrition Intervention Overview
As part of its mission to improve the nutrition and quality of life of the most vulnerable populations during critical times in their lives, the World Food Programme (WFP) of the United Nations was, at the time, supporting the government of Mozambique to develop an integrated nutrition intervention for pregnant and lactating women and children aged 6 to 23 months, within the SUN movement. Mozambique joined the SUN movement in 2011 as part its concerted efforts to reduce chronic undernutrition as a government priority. 20 This large-scale, community-based intervention aimed to contribute to the prevention of stunting by using a BCC campaign to promote a range of positive health-seeking behaviors around pregnancy, IYCF, and hygiene and sanitation. It was also designed to provide a free distribution of small-quantity (SQ)-LNS (note 2) 21 to all households of children aged 6 to 23 months living within the intervention districts. As an initial phase of intervention development, WFP contracted researchers from Johns Hopkins Bloomberg School of Public Health to conduct formative research from May to August 2013 in this setting.
Research Design
A rapid assessment procedures (RAP) approach was used in order to collect ethnographic data to inform the intervention. 22,23 This formative research included 3 exploratory phases, each which built off the previous, in an emergent and iterative nature until the research questions were answered. The methodological approach of this research drew heavily from a RAP manual developed for WFP specifically for the introduction of specialized nutritious foods (note 4). This tool was successfully used previously to conduct formative research in Malawi in a similar stunting prevention program. 24
Sampling Strategy and Data Collection
Data collection efforts by method, cultural group, and phase of research are outlined in Table 1. A theoretical purposive sampling strategy 25,26 was used to identify participants from the 3 prominent cultural groups (Macua, Mwani, and Maconde) in this setting. 27 –29 The research team first met with the government administrator of each district. These administrators selected a number of community leaders, mainly village chiefs, in villages that they indicated were culturally representative of the district at large. With the help of activistas (community health workers), the village chiefs then identified specific caregivers of children aged 6 to 23 months and households for participation.
Summary of Data Collection Efforts by Phase of Formative Research.
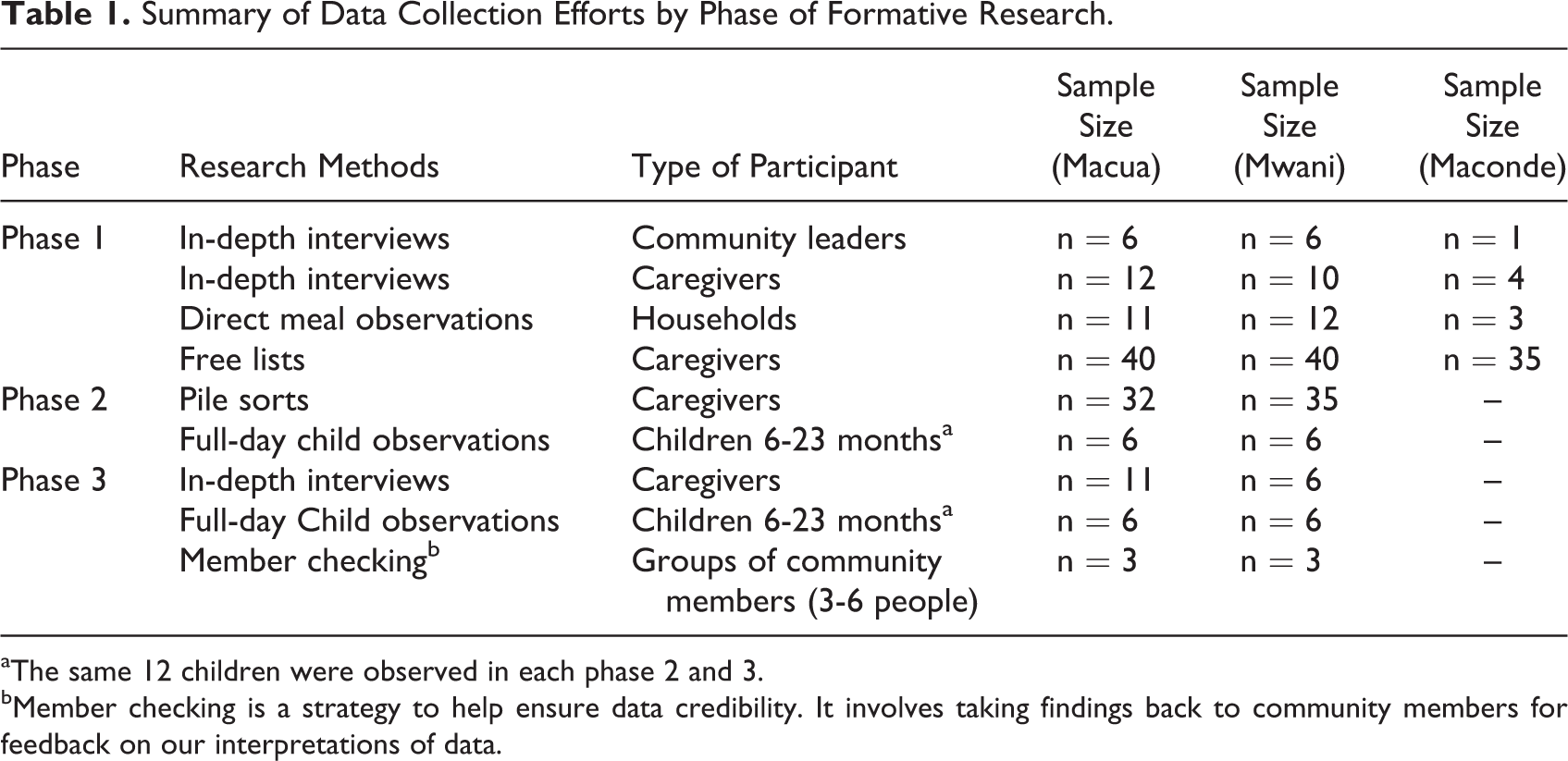
aThe same 12 children were observed in each phase 2 and 3.
bMember checking is a strategy to help ensure data credibility. It involves taking findings back to community members for feedback on our interpretations of data.
Fieldwork was completed by the lead author and 7 local data collectors (4 males and 3 females) who underwent 40 hours of research theory and methods training prior to data collection. Each local team member was fluent in both a local language and Portuguese as well as had completed a secondary school or university education. One member also worked for the regional government as a nutritionist. Team members were recruited, interviewed, and trained by the lead author with help from WFP.
Phase 1 (4 weeks)
In-depth interviews of cultural practices, illness, and nutrition
The research team identified a variety of leaders and male and female caregivers of children aged 6 to 23 months for in-depth interviews. Preference was given to caregivers who were willing to offer both rich information about their own cultural group in general and specific household information related to IYCF practices.
The interviews with leaders, who were entirely male and included community leaders, village leaders, neighborhood leaders, and block leaders, were conducted to explore characteristics that define the Macua, Mwani, and Maconde cultural groups. The interviews with caregivers of children aged 6 to 23 months were used to understand local perceptions of illness, food, and IYCF practices.
Interviewers used semistructured interview guides and digitally recorded all interviews in local languages. Each interview lasted between 40 and 60 minutes. Sampling was done until data saturation was reached in each cultural group. 30,31
Direct meal observations of household food allocation
After interviews, the village chiefs identified households in their communities that could participate in midday and evening meal observations. Households needed to have a child aged 6 to 23 months to be eligible, and sampling by cultural group was completed until data saturation was reached.
Observations documented household food preparation, feeding practices, and food utilization with special attention on the behaviors of children aged 6 to 23 months. Behaviors of other household and community members were also noted when relevant to the research questions. Observations were both event and time based. Each instance of a behavior related to the research question was recorded. In cases when behaviors were continuous for extended periods of time (eg, cleaning cooking pots), then observers recorded the actions only every 5 minutes to maintain continuity of description. 32,33 Each recording included information about who was doing the behavior, who was receiving the behavior, a description of the actual behavior, the name of the food/drink involved, an approximate food/drink quantity using local standard measures, and the duration of the behavior. Meal observations, which included an equal balance of early morning, midday, and evening meals, each lasted between 30 and 120 minutes and data collectors wrote descriptive field notes immediately afterward. 25
Free lists of salient foods and illnesses
We used stratified purposive sampling to recruit caregivers of children aged 6 to 23 months by gender, age, and number of children 34,35 for free listing of young child foods and illnesses. Free listing is a simple listing activity to elicit items from a participant’s cultural domain (eg, “Please list all of the foods for young children under 2 years in this community.”) Weller and Romney 36 suggest that with a coherent domain, such as causes of illness, 20 to 30 informants per cultural group are sufficient. Free list questions were pretested for appropriate wording in local languages among the research team prior to fieldwork. 36 Lists of items were recorded in local languages and/or Portuguese on free list forms. Data collectors used 4 types of probes (eg, providing semantic cues) to elicit longer lists from participants when necessary. 37
Phase 2 (3 Weeks)
Only Macua and Mwani households were sampled in phases 2 and 3 due to their large cultural representation throughout the intervention area.
Home-feeding trial with SQ-LNS
Within the larger sampling strategy described above, community leaders and activistas worked with the research team to purposefully sample 38 24 households with children aged 6 to 23 months for a home-feeding trial with the SQ-LNS, which is a 108-kcal paste based on peanuts, sugar, vegetable fat, skimmed milk powder, maltodextrin, and whey, enriched with a vitamin and mineral complex formulated specifically for children aged 6 to 23 months. 39 The team enrolled an equal number of children (n = 8) into each age stratum (6-12, 12-18, and 18-23 months). Each of the 24 households received 6 weeks (42 sachets) worth of the product and were provided 1-time verbal instructions on usage.
Continuous monitoring observations during the home-feeding trial
Among the 24 households participating in the home-feeding trial, 12 were randomly selected for 2 rounds of full-day observations (8 am-sundown) over 6 weeks. The household child aged 6 to 23 months was monitored throughout the entire day with the data collector following his or her movements. Although longer in duration, these observations were similar in format and collected the same type of information as the direct meal observations described previously. They were conducted primarily in household areas but extended to other parts of the community in cases when the child would leave the homestead.
Pile sorts of foods and illness domains
We used a stratified purposive sampling strategy to identify caregivers for pile sorts using the same categories that had been used for free lists. 34,35 Pile sorting is a technique where participants sort cards with salient items from their cultural domain written on them into piles based on their perceived similarities and differences (eg, “Please sort these illnesses into piles, in whatever way you think is best, in as many piles as you wish to see.”). The most salient food and illness items generated from phase 1, in addition to less salient specific nutrition-related illnesses of interest, were compiled and written on pile sort cards in both local languages and Portuguese.
Data collectors conducted 2 rounds of single pile sorts, with each caregiver who was asked to look through a shuffled deck of cards and sort it into piles according to a question. The first pile sort was constrained, asking participants to put the salient illnesses derived from free lists in phase 1 into 3 piles based on their severity: (1) most severe, (2) moderately severe, and (3) least severe. The second pile sort was unconstrained and it asked participants to put foods into piles, in whatever way they thought was best.
Both caregivers with literacy and those without participated in this exercise with the assistance of data collectors who read the cards aloud to participants and verified the piles upon completion of sorting. Data collectors asked participants to name and/or describe each pile that was created prior to completing the exercise. The number corresponding to each card was recorded by hand on a pile sort form. Pile sort data tend to be sparse, requiring between 30 and 40 participants for reliability. 36
Phase 3 (3 weeks)
In-depth interviews of caregiver experiences with SQ-LNS
We conducted interviews in phase 3 with caregivers who participated in the home-feeding trial to understand their experiences with the SQ-LNS vis-à-vis the cultural context. The other 12 households not chosen for observations were initially sampled for caregiver interviews. An additional 6 caregivers were sampled in order to reach data saturation of key themes. These interviews were similar in format to those of phase 1 but utilized a semistructured interview guide which was created based on findings from phases 1 and 2 and was specific to this phase of the study.
Data Analysis
In-depth interview data
The data collection team translated and transcribed interview data verbatim from local languages into Portuguese. They did so maintaining emic terminology so as to not lose valuable meaning in local words and phrases. 40 These Portuguese transcripts were reviewed, cleaned for errors, and then translated by 2 professional translators into English for analysis. A randomly chosen subset (25%) of the total sample was back translated from English into Portuguese into local languages by research team members who had not previously worked on the transcripts in question. Research team members then together compared the back translations to the original digital recordings and determined that meanings were not lost or misconstrued during the process (Figure 2).
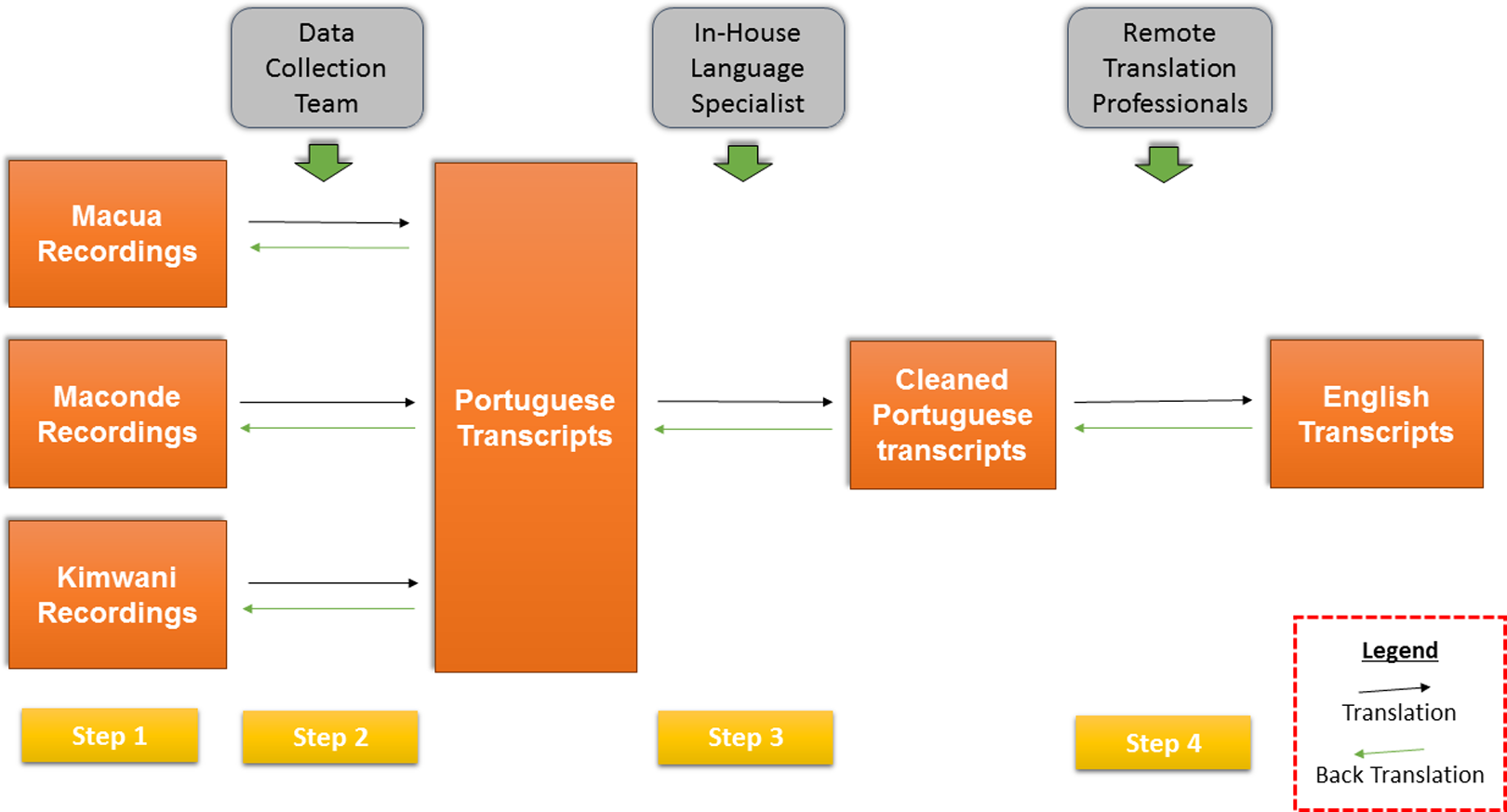
Process for translation and transcription of textual data during formative research.
Atlas.ti v7.0 computer software (Scientific Software Development, Berlin) was used for data management and coding. The data were coded shortly after translations become available using a codebook containing 48 codes for phase 1 interviews and a codebook with 47 codes for phase 3 interviews. Data were inductively analyzed drawing from aspects of grounded theory, an approach which applies an iterative strategy of working through the data set, using comparative methods, and intimate interaction with the data to generate theory. 41 The process began with line-by-line coding and then using the codebooks that had been created from that initial coding, focused coding was applied to the data set to sort, synthesize, and develop analytic categories. Axial coding, a process of relating these categories to subcategories and delineating relationships among them, helped to then assemble the data for coherence. 42 Constant comparisons of data were made throughout the coding process and memos were composed to draw comparisons among codes, categories, and quotations. 41
Direct observation data
Descriptions of behaviors from observation forms and field notes were inductively analyzed by the research team in order to identify themes in relation to household food utilization and barriers or facilitating factors to SQ-LNS usage. Salient themes were extracted and compared and contrasted by cultural group, phase of research, and household characteristics. Findings were then incorporated into the interview guides for triangulation during interviews with caregivers.
Free list data
Cultural domain analysis represents a range of analytic methods (eg, factor analysis, unidimensional scaling, consensus analysis, etc) used to understand cultural domains, and through an emic perspective we applied it to our free list and pile sort data. 43 To analyze the free list data, first the lists of food and illness items in local languages were entered into Anthropac version 4.98 (Analytic Technologies, Lexington, Kentucky), which generated frequencies and salience (S), a statistic accounting for rank and frequency. 44 Second, the local terms were translated into Portuguese and then the most approximate English terms. Where direct translations were not available, English phrases or emic language were maintained to avoid losing too much context in translation.
Pile sort data
The numbers identifying the Macua pile sort cards were entered into Anthropac and aggregate proximities were calculated, yielding 14 × 14 and 14 × 14, item-by-item matrices for illness and food items, respectively, with cells indicating the proportion of times 2 items appeared in the same pile across participants. The same approach was used for entering Mwani pile sort data into the software to calculate aggregate proximities yielding 19 × 19 and 14 × 14 matrices for illness and food terms, respectively. Then the aggregate proximity matrices were analyzed using multidimensional scaling (MDS) as recommended by Weller and Romney. 36 Stress, taken as a goodness-of-fit statistic in MDS analyses, was calculated for each aggregate proximity matrix.
Member Checking
After data analysis, the research team took findings and interpretations drawn from the research back to groups of community members as a strategy to help ensure data credibility. 45,46 We sought community member confirmation or rejection of our interpretations as well as explanations of findings that were challenging to interpret.
Ethical Approval
The study protocol was approved by the institutional review board of the Johns Hopkins Bloomberg School of Public Health and the National Bioethics Committee for Health of the Mozambique Ministry of Health. Adult participants gave verbal informed consent for themselves and assent on behalf of child participants.
Results
Comparing Cultural Groups of Cabo Delgado
Culture and context
Three distinct cultural groups, Macua (312 villages), Mwani (32 villages), and Maconde (13 villages), live within the 7 targeted districts of Cabo Delgado. While the Maconde cultural group has a small representation in comparison to the other groups, it has cultural similarities to the inland Macua communities around IYCF practices and societal organization, and both groups are matrilineal. Although similar, Macua and Mwani cultures have distinct characteristics of religion (Christianity vs Islam), language (Macua vs Kimwani), livelihoods (agricultural vs fishing), and dietary practices (3 meals vs 2 meals; Table 2).
Comparison of Key Characteristics of Macua and Mwani Cultural Groups.
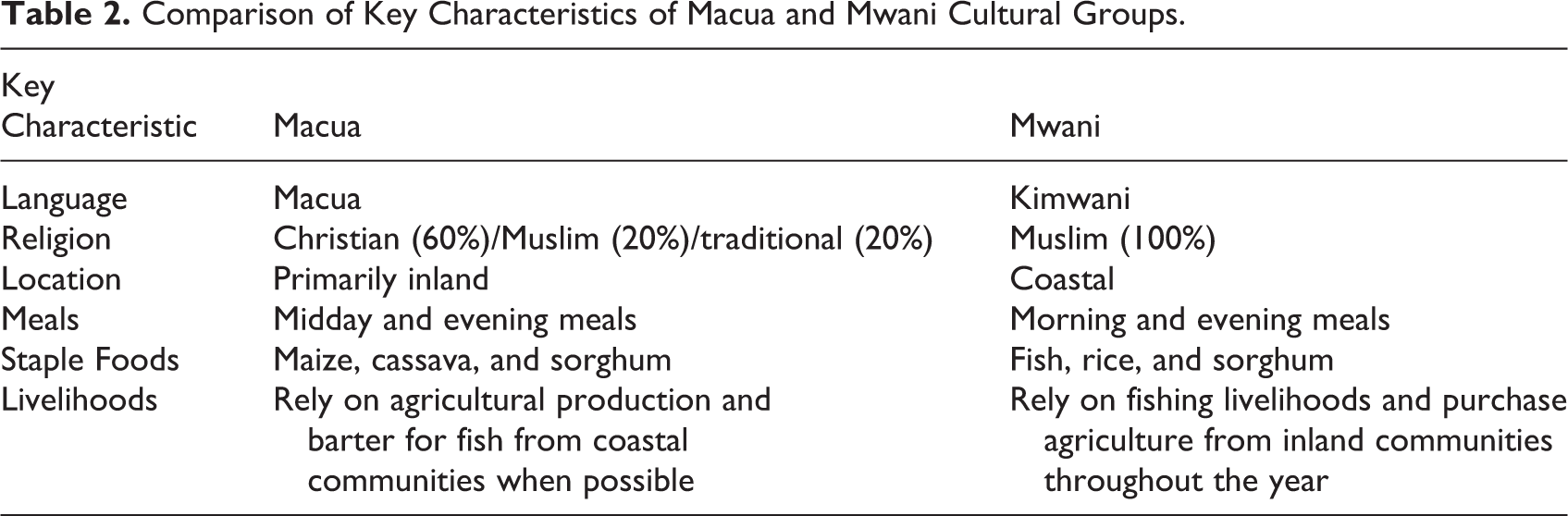
While these characteristics define 2 different cultural groups, our interview and observational data indicate that they are also strongly influenced by geography. The coastal communities, comprising both Macua and Mwani villages, have cultural similarities to those of the Mwani community at large, and they are primarily Islamic communities that have fish-based diets. The inland communities, comprising mainly Macua and some Maconde villages, are similar to each other, yet different from coastal communities in terms of many cultural practices. They largely practice Christianity and engage in agricultural livelihoods.
Community leadership
In all communities, there are up to 7 levels of leadership that influence life (Table 3). There is a government-appointed community leader as well as a locally elected and traditional village chief. Both leaders have strong influences over community, household, and individual behaviors yet are designated different leadership responsibilities. For implementing a nutrition intervention in this setting, the lider comunitario is important for granting formal permission, while the chefe de aldeia will only then provide support to that entity in whatever capacity is needed. While not all village chiefs are trusted due to perceived corruption, they are still important community influencers and gatekeepers.
Hierarchy of Community Leadership in Inland and Coastal Communities.
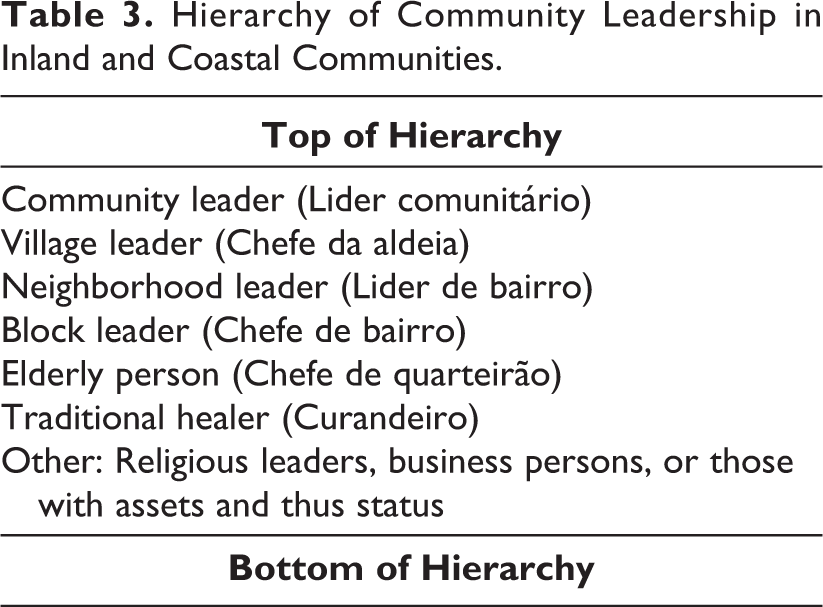
Most villages also have one or more traditional healers, whose assistance is sought for “spiritual illnesses” with which hospitals are unable to assist, for example, seizures as a result of epilepsy or “persistent cough” from tuberculosis. Their importance in village life highlights a societal belief system of disease causality that has at least a 2-tiered explanation, invoking both naturalistic (eg, parasites, too little food, and injury) and personalistic (eg, possessed by spirits and bewitching) causes to episodes of illness. You can make your best effort to keep your house clean, wash clothes, and maintain your children by bathing them properly, but when the day comes for them to get sick there is nothing you can do. Sick children become unable to eat and some of us come up with the idea that children are bewitched. (In-depth Interview, Macua Community Leader)
Cultural Perceptions and Household Food Utilization
Perceptions of Illness and Health
Community members pointed to 2 primary explanations for the “healthy growth and development” of a child: (1) the absence of disease and (2) noticeable weight gain. Caregivers emphasized that a “chubby” or “fat” baby indicates healthy growth and development and “weight gain” to be a key indicator of that process. No differences in perception existed between caregivers of coastal and inland communities on this topic.
Illnesses related to poor nutritional status were largely absent from the cultural domains of community members in this context. Within the Macua communities, the most salient community illnesses included ethecusa (malaria, S = 0.692), na’mmirimane (stomach ache/diarrhea, S = 0.476), muru (headache, S = 0.447), and mitho (conjunctivitis, S = 0.312). In terms of nutrition-related illnesses, only 2 were mentioned. Ohikalani ephone (lack of blood), which refers to anemia, was the 19th most frequently mentioned illness (S = 0.081). Okuvia (stunted growth) was the 51st most frequently mentioned illness (S = 0.004) being described by most as “This is not an illness” or “I do not know this illness.”
Similar findings applied to the Mwani community. The most salient illnesses were cucossomola (cough, S = 0.605), na’matumbo (stomachache/diarrhea, S = 0.554), feviri (fever, S = 0.512), and oma (malaria, S = 0.481). Ana damu (lack of blood), which refers to anemia, was the 12th most frequently mentioned illness (S = 0.015). Further down the list was n’nhala (stunted growth) being mentioned 17th most frequently (S = 0.088) by only 25% of the sample.
While members of both communities largely did not associate the causes of illnesses with food and nutrition, they did categorize signs and symptoms in relation to severity. Stunted growth, wasted or emaciated appearance, and slowed cognitive development are perceived to be less severe than other salient signs and symptoms (eg, diarrhea and cough), and in many cases, they are not perceived to be biomedical illnesses at all but rather individual characteristics that someone has inherited from birth.
Food classification systems
Inland Macua and coastal Mwani cultural groups have similar classification systems for children’s foods, although within those systems, the specific foods differed due to availability and access driven by geography.
Inland Macua communities categorized foods for young children into eyolia yomahucu otene (common foods), echjiolia chjovesta (special foods), and eyolia yoachjisso (early meal [morning] foods; Table 4). “Common foods” are staple foods eaten every day (eg, sorghum) and commonly shared by family members; “special foods” are complements to staple foods and include meats and vegetables, items that are more expensive and less available; and “early meal foods” are those consumed primarily as breakfast items (eg, banana). The SQ-LNS was placed in a cluster by itself due to its unfamiliarity. The MDS produced a 2-dimensional visual representation of 4 distinct clusters with a moderate stress of 0.156 (Figure 3). Data show no clear evidence of subcultural variation among the Macua respondents with respect to this domain of foods for young children aged 6 to 23 months (eigenvalue: 13.121; eigenratio: 4.759).
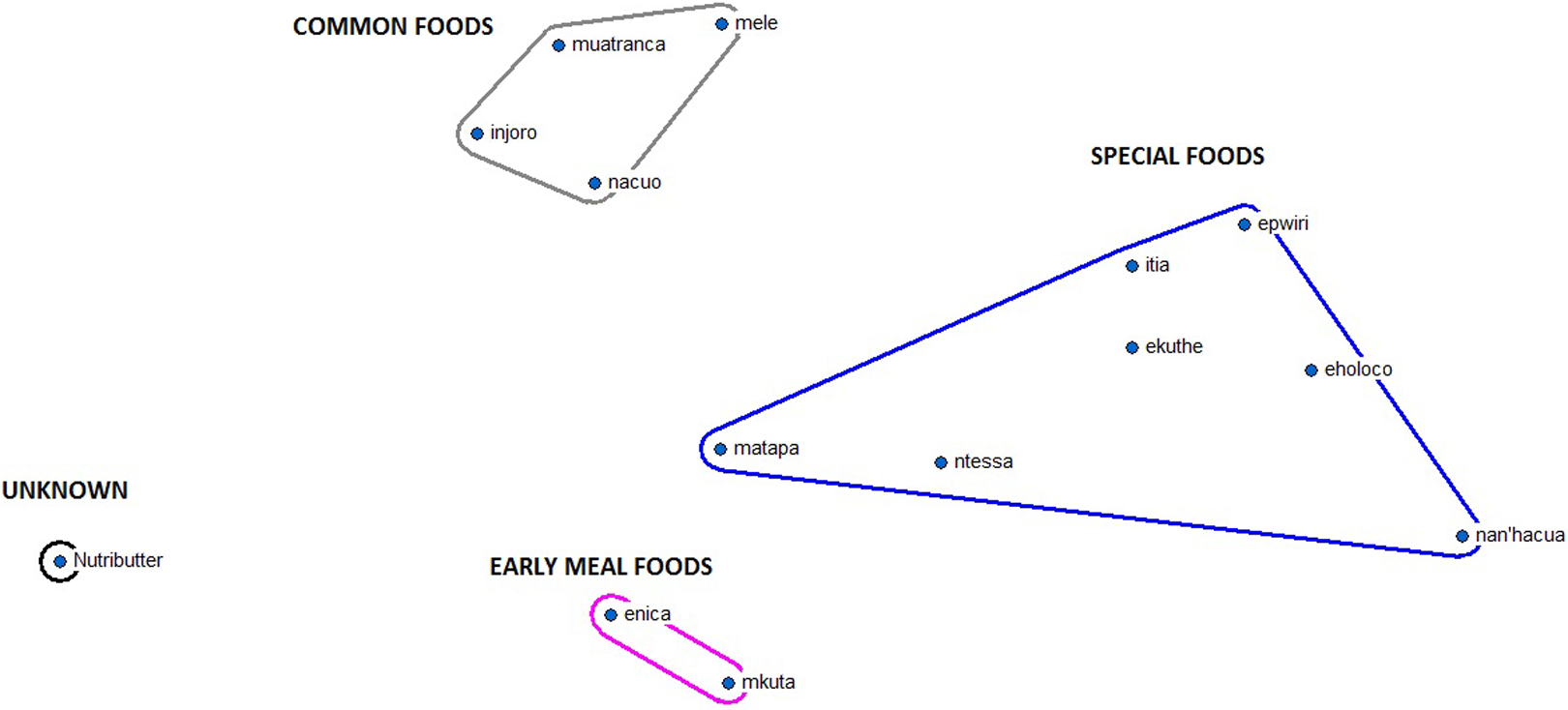
Multi-dimensional scaling map of Macua food items (n = 14).
Description of Clusters Based on Multidimensional Analysis of Macua Food Items.
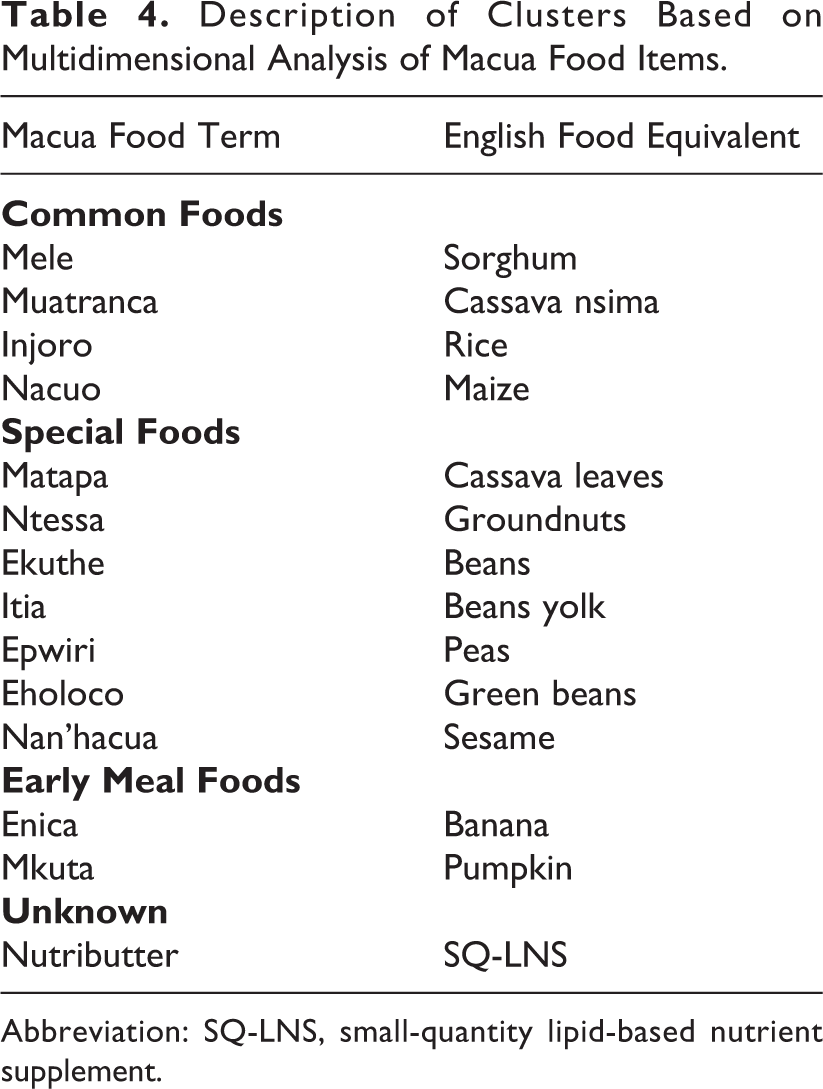
Abbreviation: SQ-LNS, small-quantity lipid-based nutrient supplement.
Among the coastal Mwani communities, foods for young children are grouped similarly into chjacuria chjassuku daima (common/everyday foods), nssuzi (side dishes/foods), and chjacuria chjassubu (breakfast/early meal foods; Table 5). The MDS map of young children’s food items produced a 2-dimensional representation of 3 clusters with a reasonable stress of 0.103 (Figure 4), and items exhibited a strong fit to the consensus model (eigenvalue: 9.668; eigenratio: 3.408) without evidence of subcultural variation among the Mwani participants for the foods for young children domain.
Description of Clusters Based on Multidimensional Scaling of Mwani Food Items.
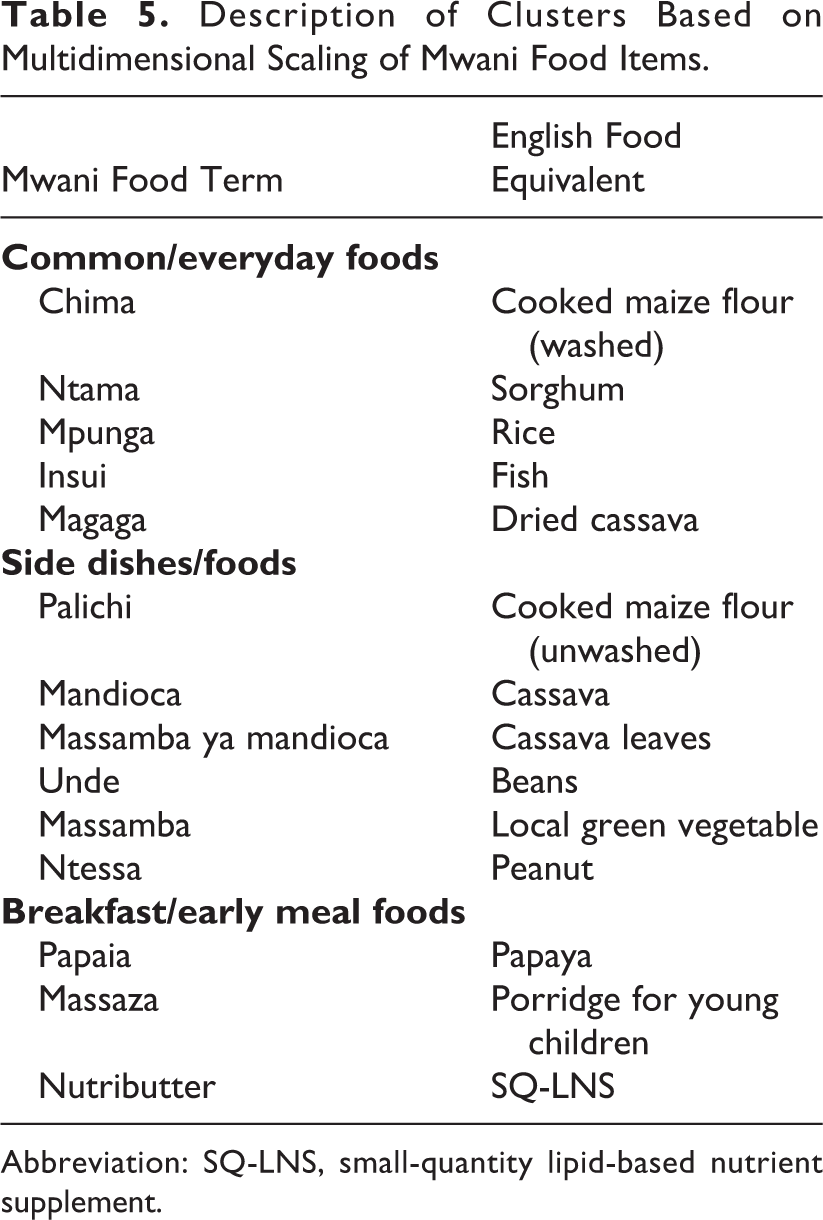
Abbreviation: SQ-LNS, small-quantity lipid-based nutrient supplement.
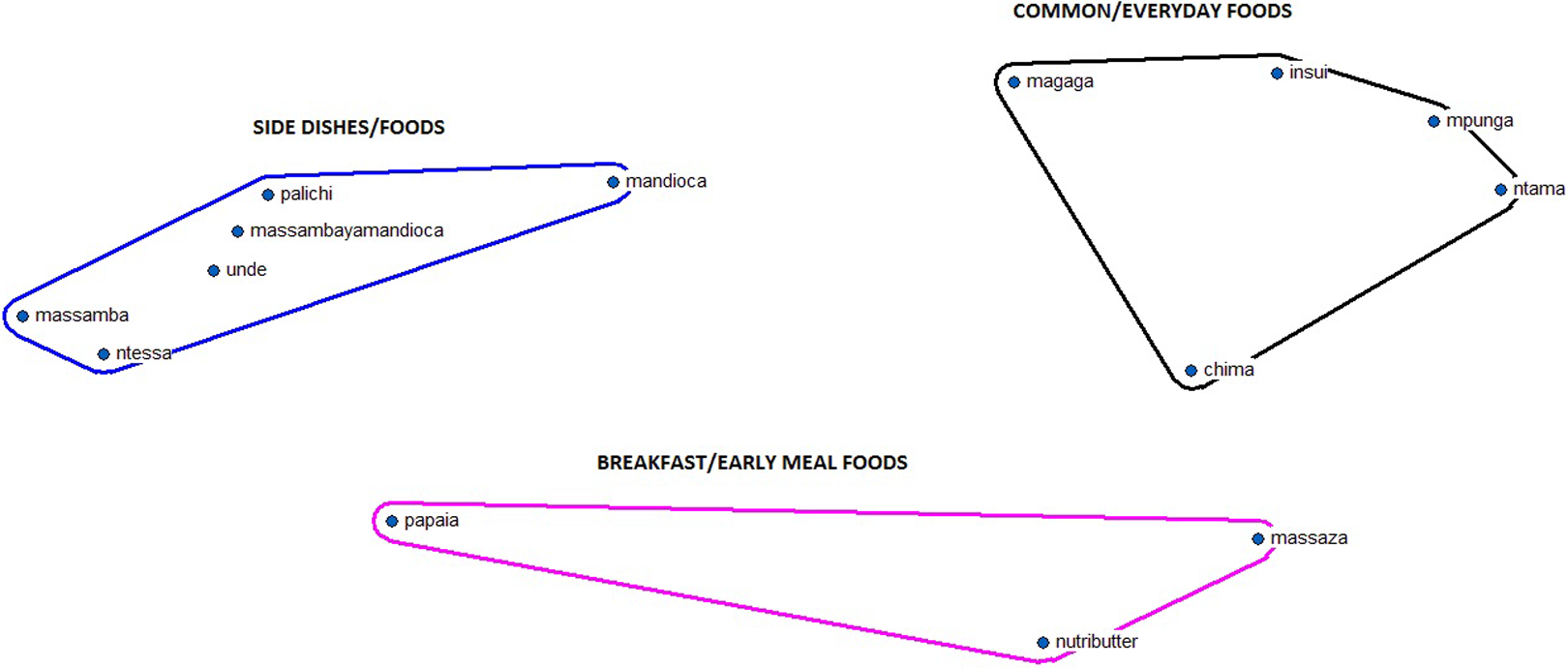
Multi-dimensional scaling map of Mwani food items (n = 14).
While “special” or “side dishes/foods” tend to be more nutrient rich, caregivers in both communities perceived “common” foods to be more important for the health of their young children, emphasizing dietary quantity over quality. SQ-LNS was considered to be a “breakfast/early meal” food by Mwani participants who ascribed this categorization to its sweet flavor.
Food-related practices
Adult diets and dietary patterns distinguish inland and coastal communities. Coastal communities consume fish-, rice-, and sorghum-based diets, whereas the inland communities eat maize, cassava, and sorghum as their staples. In addition to tea and bread consumption in the mornings, coastal communities generally eat only 1 large evening meal that includes coconut in some form. Inland communities eat both midday and evening meals without an early morning meal. In both communities, the youngest children (0-12 months) breast-feed and eat special meals, generally maize-based wet porridge, throughout the day, while older children (12-23 months) eat more closely aligned with adult dietary patterns. Both communities barter with each other to get foods that their respective areas lack in any given season.
For inland communities, which are exclusively agricultural, IYCF practices vary by season and quality of harvest. Food consumption varies between hot, rainy (December-April) and cold, dry (May-November) seasons. During the hot, rainy season, maize is often unavailable, so cassava is used to feed young children; however, during the cold, dry season when maize is abundant, it is the preferred staple to make wet porridge for young children. While coastal communities face seasonal food variation as well, they have more purchasing power than inland communities due to their more lucrative fishing livelihoods. Thus, they are able to barter or buy foods that are in short supply from inland communities.
Gender is an important dynamic at household meals. In both communities, female caregivers are exclusively responsible for IYCF practices but in coastal communities, men will help out in times of a mother’s sickness or absence. Within inland households, maternal caregivers eat with girls >10 years and paternal caregivers eat with boys >10 years in shared plate eating. Children between 3 and 9 years eat together from the same plate, despite gender differences. Sharing food with other community children who visit during mealtime was common practice but not so in coastal communities. Coastal communities do not share food with people whom they are unfamiliar and share much less than do inland communities…this is different from inland cultural groups where food sharing is common, expected, and central to mealtime. (Data Collector direct observation field notes)
Young children of both genders under 18 months, and to a lesser extent under 23 months, are favored during mealtimes in both inland and coastal communities. They are usually fed first and, depending on their age, physically protected from older children’s attempts of food theft by the maternal caregiver. As children grow older from 6 to 23 months, they are increasingly less protected by caregivers and eat more with older siblings when food sharing increases.
Special intervention considerations
During the hot, rainy seasons (December-April), villages in Cabo Delgado annually face cholera epidemics. Many communities blame international organizations for spreading the disease, causing ill will toward outsiders working there (note 5). Data suggested that this situation may be a major barrier to the successful implementation of a nutrition program with SQ-LNS if not addressed. Many people died of diarrhea in our community. Because of our community’s ignorance, when an epidemic like cholera appears, there is a tendency to blame somebody for it, without thinking about where the fault may really lie. (Coastal Female Caregiver, In-depth Interview)
Discussion
This study was the first of its kind to use ethnographic methods during formative research to generate context-specific recommendations to inform an integrated nutrition intervention aimed to improved IYCF practices in Mozambique and contribute to the government’s efforts to reduce chronic undernutrition as a SUN signatory. We elucidated key sociocultural differences of ethnic groups in this setting. These findings have direct implications for developing a culturally appropriate, behavior change intervention with effective communications 47 and illustrate how a RAP approach can yield useful programmatic information during formative research.
Our findings suggest that tailored BCC strategies considering both village ethnicity and location will be more effective than a one-size-fits-all approach in this setting. A 2-pronged BCC strategy will likely be more successful if it is tailored to consider “coastal versus inland” communities as opposed to exclusively “Macua versus Mwani” communities. Especially, the core cultural values, including distinct religions (Christianity vs Islam), languages (Macua versus Mwani), and dietary patterns of coastal and inland communities, are substantial. For instance, promoting fish as a complementary food during an early meal for an 18- to 23-month-old child would be contrary to cultural practices and confusing to an inland caregiver but acceptable to someone from a coastal village. Tailored messages and channels that are aligned with each community’s unique religious values, livelihood activities, and dietary behaviors will increase the likelihood that the messages will have optimal reach, impact, and recall. 48 Since the small Maconde cultural group does reside in some of the inland districts and has similar IYCF characteristics to inland Macua groups, a “coastal versus inland” approach should effectively and practically target the 3 cultural groups. Using a RAP approach to understand this cultural context allowed for strategic programmatic decisions related to sensitization efforts, BCC strategy creation, and monitoring and evaluation tool development, which otherwise may not have been possible.
Community leaders of multiple levels should be included in early intervention development to firstly provide permissions for staff to work in the desired areas and secondly to extend support for sensitization efforts around chronic undernutrition, which is neither a salient nor a severe health concern in these communities (Table 3). Doing so is particularly important in this context where cholera has mistakenly been linked to the previous work of development organizations and where disease causation is thought to stem from both impersonal systemic causes and supernatural agents. While village chiefs are necessary to give permissions for working in a particular area, traditional healers may have the power to impede a project working only from a biomedical lens and the motivation to promote one that is working within both paradigms. In 2000, for instance, traditional healers were employed as technical advisors under the head of state in Zambia to help combat its HIV/AIDS epidemic. 49 Using a similar strategy in other contexts where SUN activities are being implemented may help program staff to build strong rapports with communities, get early village buy-in, and set clear expectations. Utilizing traditional healers in programs can help bridge the communication gap between local and biomedical communities.
Explaining IYCF practices aligned with local understandings will also help to convey key health messages around chronic undernutrition in Cabo Delgado. For example, in this context, the promotion of IYCF practices should incorporate salient, local perceptions of healthy growth and development, including the absence of disease and noticeable weight gain. Messages should include images of a “chubby” or “fat” baby to symbolize health. They should also include the local Macua and Mwani concepts of food groups to communicate optimal IYCF teachings as has been done similarly in other culturally appropriate, nutrition education programs. 50 With a high prevalence of infectious disease in this province, 19 as well as great community concern towards it, messaging about the potential impact of an SQ-LNS to reduce bouts of morbidity may resonate with caregivers more than appeals to improvement of linear growth. The way that health messages are framed affects their impact on desired health behaviors. 51 Our findings provide important information about local concepts of illness and foods for crafting persuasive messages that may resonate more with community members than would generalized health messages.
The lack of accord between the ways the biomedical and the local communities conceptualize and discuss chronic undernutrition necessitates intense sensitization efforts, not only aimed toward communities about nutrition-related illnesses but also directed toward program managers about the perceptions of the local community. Utilizing a theoretical framework such as the Health Belief Model, which explains that one’s perceived susceptibility, severity, benefits, and barriers to illness prevention jointly predict one’s actions, may be useful for understanding the formative research findings in the context of human behavior and applying them to the program in Cabo Delgado. 52 This intervention, which aims to improve complementary feeding behaviors, could not expect full community participation, let alone compliance with an SQ-LNS, without first bringing to light chronic undernutrition as a significant public health problem with negative consequences for the community. Sensitization efforts that incorporate local concepts of nutrition-related illness underlying disease classification systems should not only include tailored communications to inland and coastal beneficiary groups but also be central to preprogram trainings of activistas and other health care workers. 53
Although rich data were collected in a short amount of time during this work, some limitations exist. First, there were multiple language barriers and it is likely that some contextual meaning and details were lost in translation. Through back translation, the utilization of professional translators, and verbatim translations using emic terminology, we are confident in the credibility of our data. 54,55 Also, data were only collected during the postharvest season and coincided with the cold, dry season, which overlapped Ramadan (July 8-August 7, 2013) when adult dietary behavior is atypical from that of the rest of the year, so season-specific findings should be taken with caution. By using a triangulation of multiple and different data sources over 10 weeks, however, we were able to develop a full contextual picture necessary to answer the research questions from corroborating angles. 38,46 Further, findings were taken back to the community through member checking in order to enhance our interpretations of data. 45,46
At a time when nutrition science is at the forefront of global health, researchers and practitioners need to consider the many social and behavioral aspects necessary for successful interventions. Dietary behaviors have social and cultural connotations derived from both acquired knowledge and long-standing traditions that are deep-rooted tenets of most societies. 56 Sound formative research using a RAP approach can provide the necessary foundations from which programs can understand such dynamics and launch most effectively, especially in programmatic settings where deep ethnographic studies are generally not possible due to limitations such as time and cost. After all, evidence suggests that health education can in fact improve complementary feeding practices, nutritional status, and growth with consideration for culture, local perceptions, and already-existing community resources. 57 To impact positively upon key nutrition indicators by utilizing specialized nutritious foods, nutrition researchers and practitioners should embrace the social and behavioral sciences as a core component to integrated nutrition interventions.
Footnotes
Acknowledgments
We would first like to acknowledge the local data collection team members who were integral to this project: Afonso Campos, Vasco Buanausse, Adriano Antonio, Dionisia Mucussete, Gustave Ndagijimana, Caolina Cardoso, Adao Eduardo, Abdul Faque, Focas Malimbili, and Amido Ussene. Also, we owe much gratitude to former WFP consultants Caitlin Sturridge and Rebecca Olsen, WFP nutritionist Israel Rios, and Boston Consulting Group associate Matias Pollman-Gomez for their great support at key times throughout this project. We thank these individuals, in addition to the many staff members who were directly or indirectly involved from the Mozambique government and WFP head and country offices.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stephen Kodish and Joel Gittelsohn were consultants to the World Food Programme funded by the Children’s Investment Fund Foundation (CIFF) and received support for the conduct of the research.