
Abstract
Background:
Iron and zinc are the 2 micronutrients that are deficient in the diet of the people of Third World countries.
Objective:
Assessment of iron and zinc status of 6-month to 5-year-old children from low-income rural families of Punjab, India.
Methods:
Thirty clusters (villages) from 12 blocks of Ludhiana district of Punjab, India, were chosen randomly to select 413 households of agricultural laborers and of small and marginal farmers to obtain a sample of 312 children (6 months to 5 years).
Results:
Wheat is the major contributor of iron (65.5%) and zinc (58.0%) in the diets of children. The percentage of adequacy of iron in 0.5- to 2-year-old and 3- to 5-year-old children was 18.5% and 37.2% when compared to the estimated average requirements of World Health Organization/Food and Agriculture Organization. The corresponding zinc adequacy was only 7.2% and 25.3%, respectively. The results showed that 65% of 2- to 5-year-old children had dietary zinc adequacy. Serum zinc values below normal values were 17.9%, whereas 84.6% and 71.8% of children had low serum iron and serum ferritin levels, respectively. The raised soluble transferrin receptors were found in 79.8% of children. Anemia was found in 55.8% children, of which 20.2%, 33.0%, and 2.9% of children were mildly, moderately, and severely anemic, respectively.
Conclusions:
Iron-deficiency anemia is a more serious problem among reference children, however, zinc deficiency also prevails. The suboptimal iron and zinc status pose a serious threat to the physical and mental growth of these children. Hence to curb these deficiencies necessary steps should be taken.
Introduction
Micronutrient malnutrition alone afflicts more than 2 billion people, mostly among resource-poor families in developing countries, with iron, iodine, zinc, and vitamin A deficiencies most prevalent. 1 More than 5 million childhood deaths occur from micronutrient malnutrition every year. A diverse diet, consisting of vegetables, fruits, dairy, and meats, is rich in micronutrients but is out of the reach of many of the world’s poor because of it being expensive. Resource-poor people rely primarily on a few starchy staples that are rich in energy but not in micronutrients. 2 Iron and zinc are the 2 micronutrients that are deficient in the diet of the people of Third World countries. Although sufficient food is available, still over 2 billion people in poorer countries of the world have iron deficiency. Since micronutrient deficiencies go unnoticed, these are termed as “hidden hunger.” Predictably, half of the global population is at the risk of low intake of zinc.
Zinc deficiency is an important cause of morbidity due to infectious diseases and growth faltering among young children. Increased demand of zinc due to rapid growth and decreased intake of zinc due to inadequate feeding practices predispose pre-schoolchildren, especially living in communities of low socioeconomic level, to an elevated risk of zinc deficiency. 3 Zinc deficiency in children leads to retardation in growth and also morbidity from many diseases such as diarrhea, pneumonia, and malaria. 4 Around 800 000 deaths among the children below 5 years of age occur annually due to diarrhea (176 000), pneumonia (406 000), and malaria (207 000). High mortality rate among children resulting from these infections has been reported to be associated with inadequate zinc intake. 5 -7 The studies reported 54.2% children and 37.1% pre-schoolchildren to be zinc deficient. 8,9 Several studies indicate that zinc deficiency results in poor growth in infants 10,11 and children 12,13 and also depressed appetite. 14,15 Zinc deficiency may also lead to impaired motor development in infants 16,17 and thus can interfere with cognitive performance.
Prevalence of iron-deficiency anemia among children is much higher than among adult women and may be partly attributable to the high prevalence of hookworm infestation among children. National Family Health Survey (NFHS) reported that 7 of the every 10 children of age 6 to 59 months in India are anemic. Three percent of children aged 6 to 59 months are severely anemic, 40% are moderately anemic, and 26% are mildly anemic. The prevalence of anemia in children of age 6 to 59 months increases steadily with the mother’s level of anemia, reaching 82% in children of mothers who are severely anemic. 18
Anemia is a major health problem in Punjab, especially among women and children, and can result in maternal mortality; weakness; diminished physical and mental capacity; increased morbidity from infectious diseases; perinatal mortality; premature delivery; low birth weight; and impaired cognitive performance, motor development, and scholastic achievement among children. In Punjab, majority (66%) of children between the age of 6 and 59 months were anemic. This includes 22% of mildly anemic, 38% of moderately anemic, and 7% of severely anemic. 19 Several studies are available on prevalence of iron and dietary iron intake in different population groups, however, scanty information is available related to deficiency of zinc as well as zinc consumption levels in India and particularly in Punjab.
Methods
Dietary Survey
Sample selection
The study was conducted in the rural areas of Ludhiana district of Punjab. The study was of a 3-stage sampling design. Ludhiana district is divided into 12 blocks with a rural population of 13 39 178 living in 918 villages. Thirty clusters (villages) from all blocks were chosen randomly to select 413 households of agricultural laborers and of small and marginal farmers to obtain a sample of 312 children (6 months-5 years). The number of clusters from each block was proportional to the rural population of each block. This total sample size calculation was based on the prevalence of zinc deficiency of 44%, 95% individual response, 90% household response, 92% confidence level, design effect of 2.0, and the percentage of the population composed by children 6 to 59 months of age (∼13.5%) and household composition (∼5.6 people per household). The study design was planned after discussion with a statistician and by following the guidelines for the HarvestPlus method of “Interactive 24 h recall for assessing the adequacy of iron and zinc intakes in developing countries.” 20 (pp. 9-156) Institutional Ethical Committee’s approval has been obtained prior to the start of the study. Informed consent was taken from each participant in the study.
Development and validation of questionnaire for assessing dietary intake
The 24-hour recall survey based on the HarvestPlus method was carried out for each participant for 1-day using a questionnaire. Repeat on 20% of sample by different investigator and for a different 24-hour period was carried out. The developed questionnaire was pretested on an additional 10% of the participants for its validation. The daily food and nutrient intake was assessed by using HarvestPlus C.S. Dietary Software, IFPRI, Washington DC. Use of CS Dietary required the development of conversion factors and recipes databases among other databases.
Dietary Assessment
Dietary intake was assessed using the 24-hour recall method. This method was chosen as a valid and feasible way to estimate the usual intakes of nutrients, where mothers of children were asked to recall all foods and beverages, including amounts consumed, during a 24-hour period of the previous day. An interactive, multiple pass, and 24-hour recall method was adopted, and the interactive approach incorporates several tools to aid women’s memories in recalling details of foods and beverages consumed, including preparation methods and portion sizes.
The adequacy of nutrients, namely, energy, protein, calcium, iron, zinc, vitamin C, folate, vitamin B12, thiamine, riboflavin, niacin, and vitamin B6 was determined by using the recommended dietary allowances (RDAs) of Indian Council of Medical Research (ICMR) for children. 21 The data of all children were also compared with estimated average requirements (EARs) of World Health Organization/Food and Agriculture Organization (WHO/FAO). 22 Estimated average requirements were for low (5%) and moderate (10%) iron bioavailability (WHO/FAO 22 ) for iron. For zinc, EARs were corresponding to low bioavailability (International Zinc Nutrition Consultative Group [IZiNCG] 23 ), assuming that Indian diets have low to moderate bioavailability of the 2 minerals.
The tabulated data for different foods were classified into 8 groups, namely, wheat, maize, legumes, meat and poultry, nuts and oilseeds, vegetables and fruits, sugars and fat, milk and its products, and others. The percentage of contribution of the above-mentioned food groups to total energy, iron, and zinc consumption was calculated.
Blood Collection and Analysis
Biochemical assessment was carried on all selected 312 children. The biochemical parameters were studied in Biochemical Analysis Laboratory of Dayanand Medical College and Hospital, Ludhiana. Zinc and iron in serum were estimated by Auto Analyzer: Hoffman-La Roche Ltd. Serum ferritin was measured by chemiluminescent detection method using the kit of Roche Diagnostics (Germany). Soluble transferrin receptor (sTfR) was tested using Roche methodology. The normal ranges mentioned in Standard Operating Procedures of each biochemical parameter were taken for reference.
The samples were placed in tightly fitting slots in trays surrounded by dry ice in a thermocol box. An air-conditioned vehicle, with good suspension was hired to transfer the samples from the field to the laboratory within 2 hours following blood collection. Within 2 to 3 hours from the field, samples were transported to the biochemical analysis laboratory of Dayanand Medical College and Hospital, Ludhiana, where they were stored prior to analysis.
Data Analysis
The data entry was completed by project staff in duplicate to ensure accuracy. Following duplicate input, data were validated for accuracy and corrected where necessary. Statistical analysis was carried out using CPCS 1 software (Punjab Agricultural University, Ludhiana, India) for statistical analysis.
Results
Dietary Sources of Energy, Iron, and Zinc
The dietary sources of energy, iron, and zinc in the diets of children are shown in Figures 1 to 3. The findings revealed that wheat is the major contributor of energy (37.3%) in the diets of children. The second major contributor to energy in case of children was milk and milk products followed by sugars and fats. The contribution of nuts and oil seeds was negligible. Contribution of milk and milk products to energy intake in the studied population was satisfactory because a good number of households had their own cattle for milk supply to their family members. Wheat contributes 65.5% of iron to the diets of children. Vegetables and fruits as well as legumes also contributed fairly to the iron intake of children. The consumption of meat and poultry was negligible among children mainly because of cultural and religious reasons. The major contributor of zinc in the diets of children was wheat (58%) followed by nuts and oilseeds (8.3%) and milk and its products (6.1%).

Sources of energy in the diets of children.
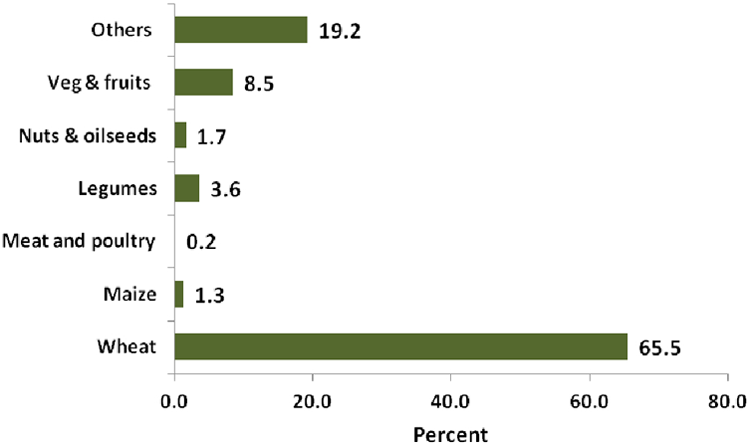
Sources of iron in the diets of children.
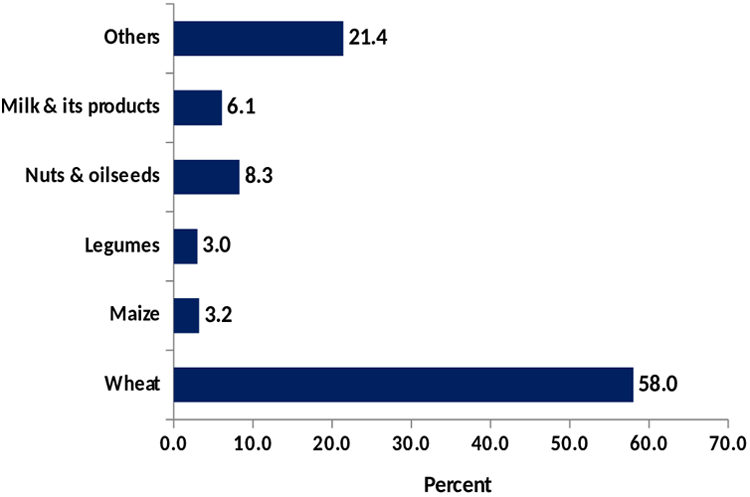
Sources of zinc in the diets of children.
Nutrient Intake
Table 1 shows the daily nutrient intake and RDAs of ICMR 21 for 6- to 12-month-old, 1- to 3-year-old, and 4- to 5-year-old children. A gross inadequacy of all the nutrients was observed in 6- to 12-month-old children because the data did not include the nutrients derived from breast milk. Hence, these data are not relevant for the youngest age-group as breast milk intakes were not measured in this study. The energy intake was inadequate in 1 to 3 years and 4 to 5 years, the percentage of adequacy being 63.6% and 71.7%, respectively (Figure 4). The percentage of contribution of carbohydrates, proteins, and fats to the total energy intake in 1- to 3-year-old and 4- to 5-year-old children was 59%, 12%, and 29% and 61%, 12%, and 27%, respectively. Calcium intake was marginally inadequate in 1- to 3-year-old and 4- to 5-year-old children. The adequacy of iron among 1- to 3-year-old and 4- to 5-year-old children was found to be 55.4% and 65.8%, respectively. Zinc intake was grossly inadequate among 1- to 3-year-old and 4- to 5-year-old children, the adequacy being only 33.8% and 42.3%, respectively (Figure 4). Other nutrients such as vitamin C, folate, riboflavin, vitamin B6, and niacin were inadequate against the RDA, while vitamin B12 was adequate in the 2 age-groups. Thiamine was adequate in 4- to 5-year-old children but inadequate in 1- to 3-year-old children.
Daily Nutrient Intake of 6 to 12 Months, 1- to 3-Year-Old, and 4- to 5-Year-Old Children.a
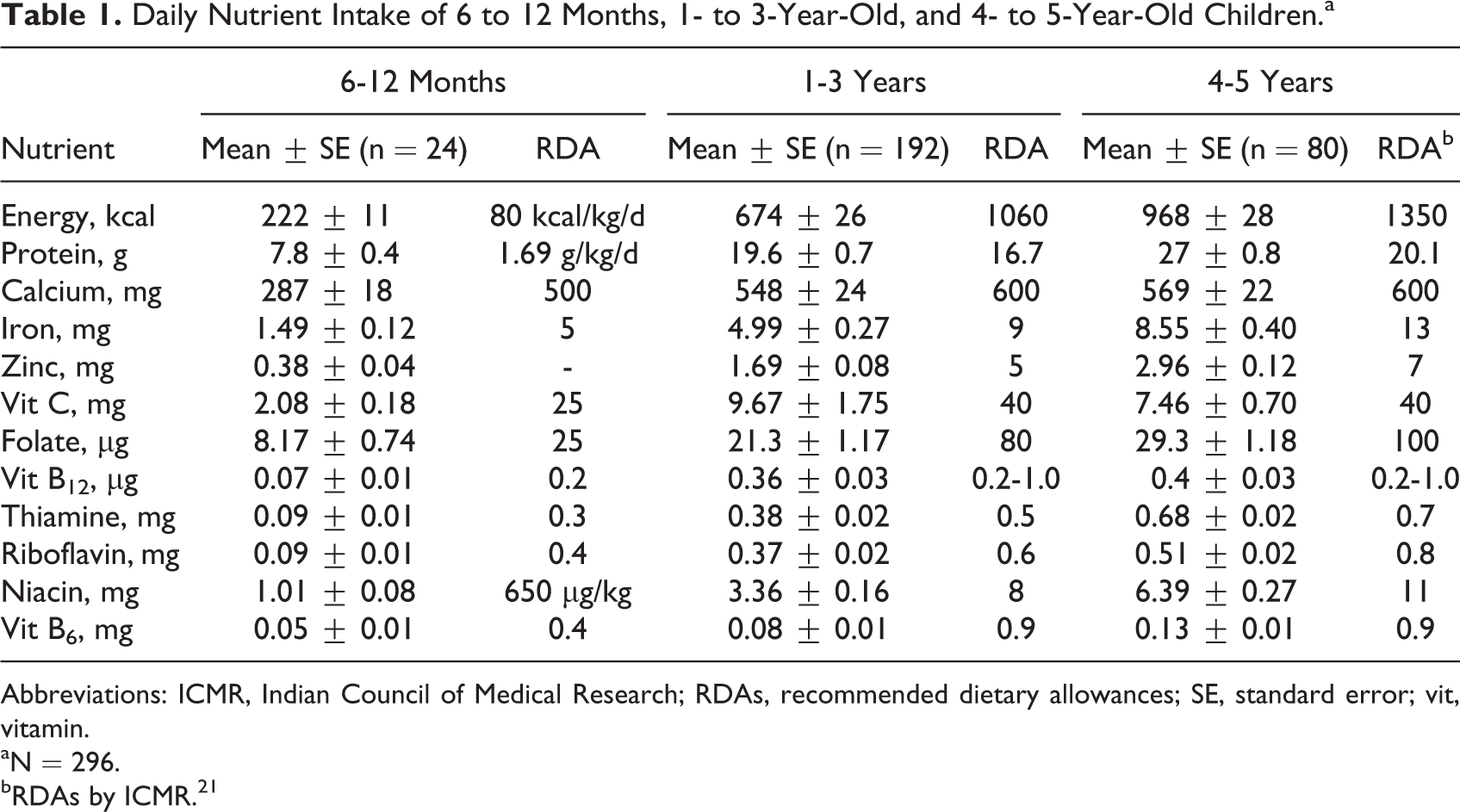
Abbreviations: ICMR, Indian Council of Medical Research; RDAs, recommended dietary allowances; SE, standard error; vit, vitamin.
aN = 296.
bRDAs by ICMR. 21
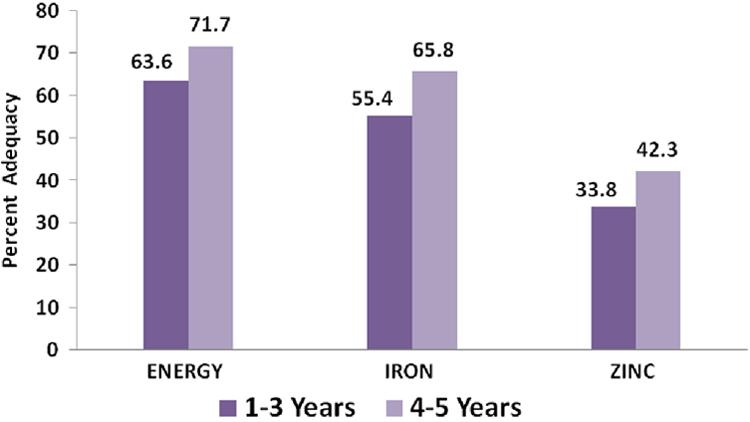
Percentage of adequacy of energy, iron, and zinc among children (6-59 months).
Table 2 shows the daily energy and nutrient intakes of 0.5- to 2-year-old and 3- to 5-year-old children as well as all children (0.5-5 years) along with EARs. 22,23 There was gross inadequacy of iron and zinc in both the age-groups. The percentage of adequacy of iron in the 2 groups was 18.5% and 37.2% when compared with EAR meant for low bioavailable iron diets and 37.0% and 74.3% for moderate bioavailable iron diets. 22 The situation is dismal for zinc as the adequacy was found to be only 7.2% and 25.3% when compared to EARs of WHO/FAO, 22 however, the percentage of adequacy was 25% and 55% against the EARs of IZiNCG 23 for the 2 age-groups. Figure 5 shows that 65% of 2- to 5-year-old children had dietary zinc inadequacy. The results showed that calcium intake was inadequate in 0.5- to 2-year age-group but adequate in 3- to 5-year-old children. Other nutrients such as vitamin C, thiamine, riboflavin, niacin, folate, vitamin B12, and vitamin A were inadequate against the EARs in 0.5- to 2-year age-group while inadequacy of all vitamins except thiamine was found in 3- to 5-year-old children. Breast-feeding is continued up to 2 years in India, especially in low-income group, hence the data are not relevant for 0.5- to 2-year age-group as it did not include nutrients derived from the breast milk.
Daily Energy and Nutrient Intakes of All the Children.
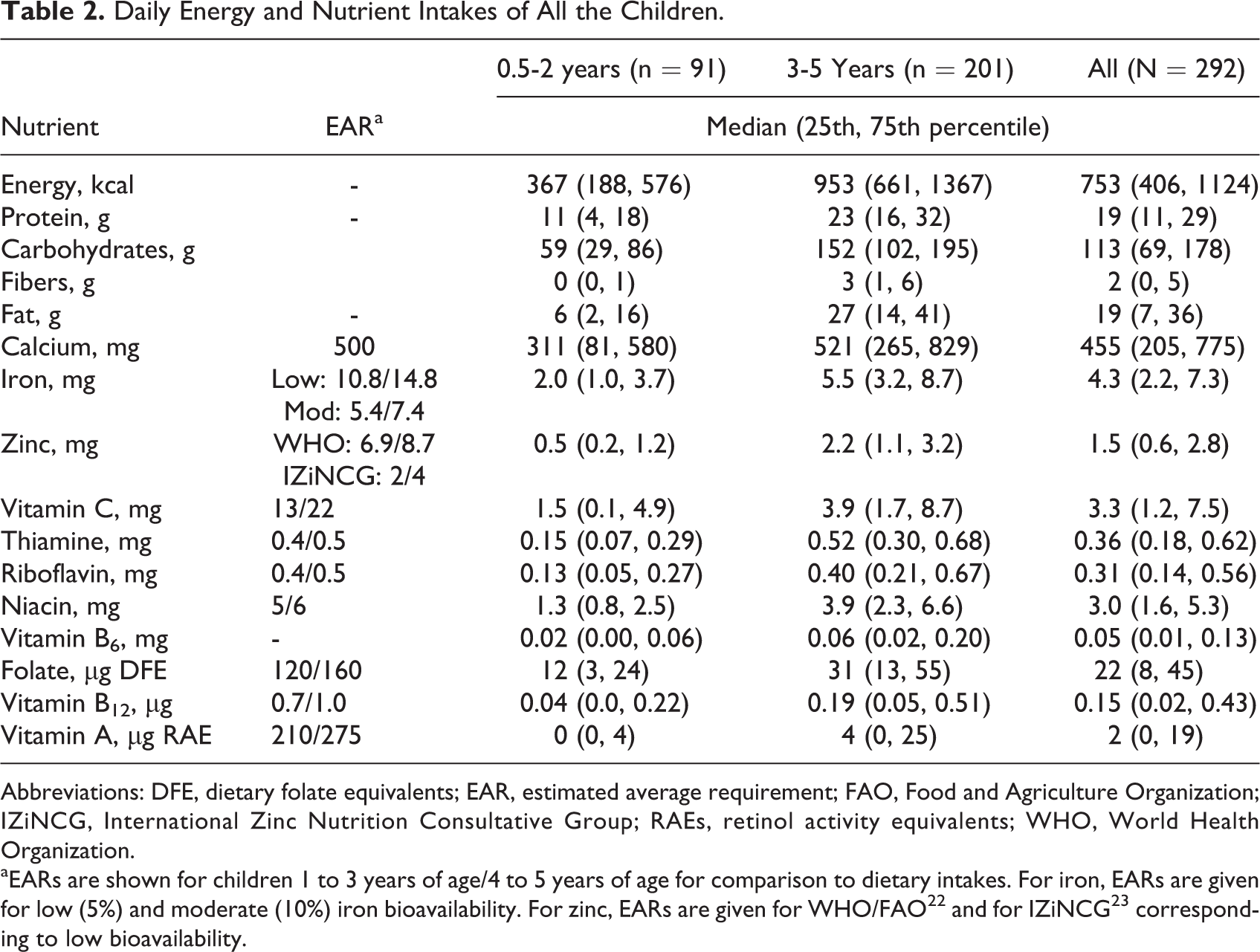
Abbreviations: DFE, dietary folate equivalents; EAR, estimated average requirement; FAO, Food and Agriculture Organization; IZiNCG, International Zinc Nutrition Consultative Group; RAEs, retinol activity equivalents; WHO, World Health Organization.
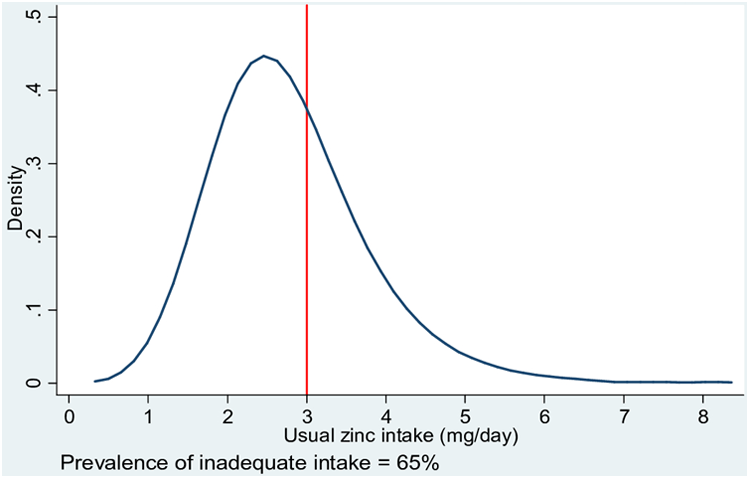
Zinc intake distribution (mg/d) and prevalence of inadequate zinc intake among 2- to 5-year-old children.
Zinc and Iron Blood Parameters
The zinc and iron status as predicted by blood analysis of the reference children is shown in Table 3. The mean serum zinc level in the children was between the normal range of 60 to 110 µg/dL, but 17.9% of the children had serum zinc values below 60 µg/dL. The blood hemoglobin levels of reference children were below normal in 55.8% of children, whereas 84.6% of children had low serum iron levels. Low serum ferritin values were observed in 71.8% of the participants, while raised sTfRs was found in 79.8% of children. The categorization of children on the basis of degree of anemia showed that 55.8% children was anemic, of which 20.2%, 33.0%, and 2.9% of children were mildly, moderately, and severely anemic, according to WHO classification of iron deficiency anemia (Figure 6). 24
Zinc and Iron Status of Reference Children (0.5-5 Years).
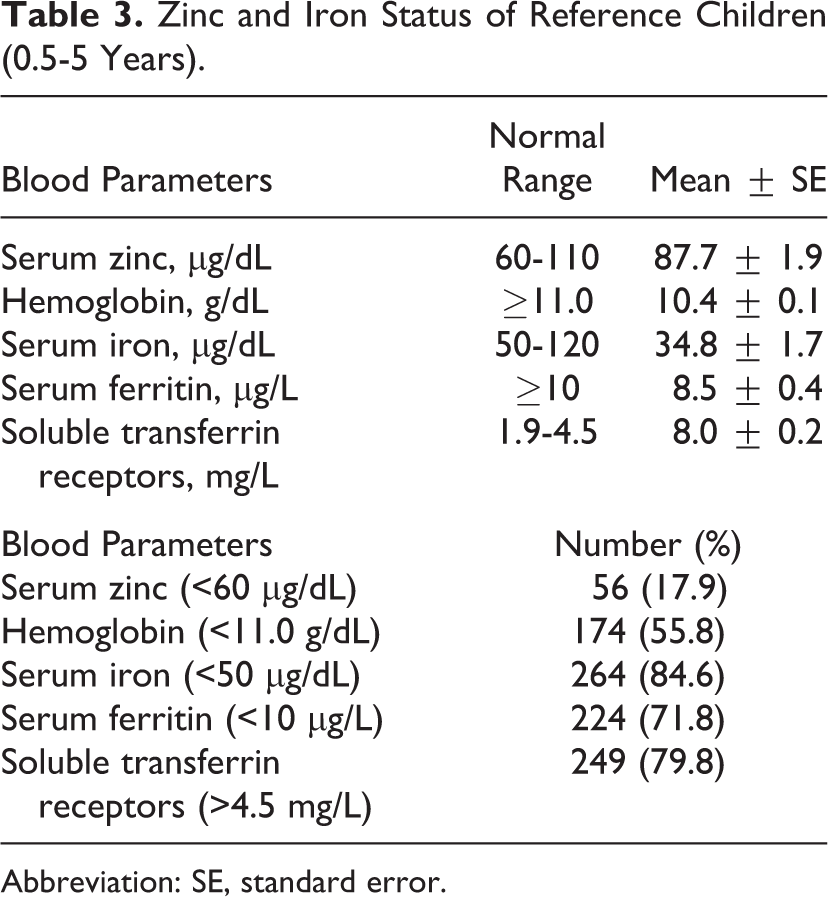
Abbreviation: SE, standard error.
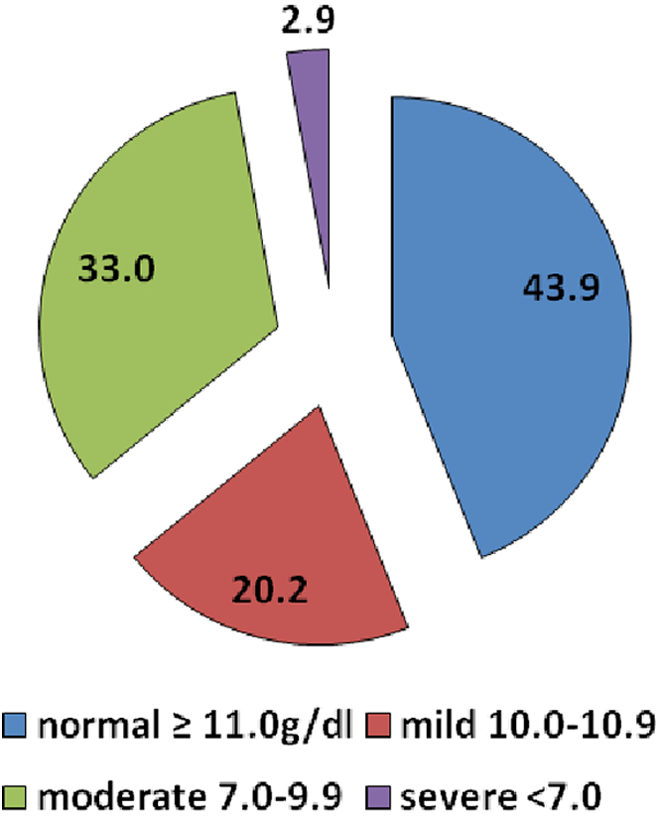
Categorization of reference children (6-59 months) according to WHO classification of iron-deficiency anemia.
Discussion
The findings clearly indicated that after the wheat, milk, and milk products were the major source of energy in the diets of children followed by sugars and fats. An analysis of nutrient intake of rural pre-schoolchildren in Punjab 25 revealed that their diets were low in cereals, pulses, and green leafy vegetables but high in milk and its products. In another study, the intake of macro- and micronutrient rich foods such as cereals, pulses, green leafy vegetables, milk and milk products, and fats and oils was lower than the RDA among pre-schoolchildren of Punjab. 26 The zinc intake of pre-schoolchildren in Sri Lanka was only half of the RDA due to inadequate consumption of foods of animal origin. 27 A study conducted in Bangladesh reported that zinc deficiency is more existent in communities consuming restricted meat-based diets and increased amount of vegetables. 28
A fairly large percentage of children showed inadequate intake of iron and zinc when compared with RDAs of ICMR and EARs of FAO/WHO and IZiNCG, thus, the study presented poor dietary intakes of these 2 vital nutrients. A study conducted on intake and dietary sources of heme and nonheme iron in Flemish preschoolers (2.5-6.5 years) reported that 35% of the children below 4 years and 55% of those between 4 and 6.5 years presented inadequate iron. 29 On the other hand, most of the pre-schoolchildren achieved the EAR for key micronutrients, including iron, zinc, calcium, and vitamin C in pre-schoolchildren in Adelaide, South Australia. 30
According to the RDAs of ICMR, there was an inadequacy of energy, iron, and zinc among 6 to 12 months, 1- to 3-year-old, and 4- to 5-year-old age-groups. Similarly, the intake of the iron and zinc was inadequate in 0.5- to 2-year-old and 3- to 5-year-old children when compared to EARs of FAO/WHO and ZiNCG. A study on Indian preschoolers of low-income group revealed that the energy and iron intakes were 56% and 45%, respectively, of the RDA. 31 In another study carried out in urban slums of Punjab, the adequacy of energy and protein of 1- to 4-year-old children was 53.5% and 51%, respectively, 32 while in the rural low-income group, the percentage of adequacy of the 2 nutrients was 86.1 and 89.7. 33 There was no reported study on the zinc intakes of children from Punjab.
The results revealed that iron-deficiency anemia is a more serious problem among reference children as compared to zinc deficiency on the basis of their blood analysis. The descriptive epidemiological study of zinc deficiency among Indian children aged 6 to 35 months found that 33.8% had levels of serum zinc below 60 µg/dL. 34 The situation of zinc status of children as predicted from serum zinc levels in the present study was far better than that in the reported study.
Epidemiological studies have confirmed high prevalence of zinc deficiency among children below 5 years of age belonging to low socioeconomic groups in 5 major Indian states, reporting an overall zinc deficiency of 43.8%, with highest in Orissa (51.3%) followed by Uttar Pradesh (48.1%), Gujarat (44.2%), Madhya Pradesh (38.9%), and Karnataka (36.2%). 35,36 High zinc deficiency was also prevalent among school going children (54.2%) and pre-schoolchildren (37.1%) in neighboring country Pakistan. 37,38 Another study confirmed low serum zinc concentrations in Sri Lankan populations. Nearly 57.0% male and 50.0% female pre-schoolchildren were found to be zinc deficient. 27 One of the studies reported a significant difference in serum zinc levels of healthy children in comparison with mild growth failure children and severe growth failure children. 39 High prevalence of iron deficiency in infants of 12 to 24 months of age was reported in a probabilistic sample of Mexican children and explores its association with some dietary and sociodemographic variables. 40
The blood picture depicts a gloomy situation of iron status of the children in the present study. According to NFHS-3 in 11 states of India, 53.0% to 74.6% of children between 6 and 35 months were anemic. 41 A study by International Institute for Population Sciences (IIPS) in Punjab revealed that 66% of children were anemic, which included 22% of mildly anemic, 38% of moderately anemic, and 7% of severely anemic. 19 Another study reported that more than half of young children in 24 states of India have anemia, including 11 states where more than two-third of children are anemic. Seven percent of children in Rajasthan and Punjab are severely anemic, more than twice the level in India as a whole. 18 Another study of 1- to 4-year-old children from low-income families of urban slums of Punjab revealed that the mean hemoglobin level of all the children was below the normal level. The majority of the children (62%) were moderately anemic, followed by mildly anemic (30%) and severely anemic (8%). 32 The present study along with previous studies carried out in India and other developing nations confirmed an inadequate zinc and iron status of young Indian children, which may have detrimental effect on physical and mental development of the children.
Conclusions
The results revealed that iron-deficiency anemia is a more serious problem among reference children. However, zinc deficiency also prevails. The findings indicated that wheat is a noteworthy source of energy, iron, and zinc in diets of children in Punjab state. The suboptimal iron and zinc status pose a serious threat to physical and mental growth of these children, hence to curb these deficiencies necessary steps should be taken for the overall development of young children. The information regarding appropriate dietary approaches and hygiene practices to curb the 2 deficiencies needs to be assimilated to the target groups through educational interventions. Further, the governments should focus on elemental iron and zinc supplementation to all under 5 children. Moreover, biofortification of staple crops like wheat with iron and zinc can go a long way to overcome the problem of iron and zinc deficiency among young children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to HarvestPlus, c/o IFPRI, Washington, DC, for its technical and financial assistance to conduct this study.