
Abstract
Aim:
The aim of this study was to compare the clinical outcomes of arthroscopic Bankart repair (ABR) using two types of knotless suture anchors (KSAs) in patients with post-traumatic recurrent anterior glenohumeral instability (AGHI).
Methods:
Thirty-two patients underwent an ABR using KSAs: a permanent KSA (PushLock) and an absorbable counterpart (BioKnotless). There were 16 patients in each group. Pre-and post-operative assessment for shoulder function using the American Shoulder and Elbow Surgeons and Constant–Murley scores, recurrence of instability, post-operative limitation of external rotation (ER) and ability to return to pre-injury level were recorded in both groups.
Results:
Both groups displayed significant improvements in functional scores (p < 0.0001) without a significant difference between the groups. Of the 32 patients, 9.4% had recurrence of instability (one re-dislocation in group 1 and two symptomatic subluxations in group 2). Return to pre-injury level occurred in 87.5% and 81.3% of group 1 and group 2, respectively. There was 2° to 3° loss of ER after ABR in both groups; the difference between the groups was not significant (p = 0.45).
Conclusion:
ABR for recurrent AGHI using a permanent or absorbable KSA offers comparable successful outcomes; no significant statistical difference was found.
Introduction
Recurrent post-traumatic anterior glenohumeral instability (AGHI) most often leads to a Bankart lesion; less frequently, Hill–Sachs and superior labrum anterior and posterior (SLAP) lesions, capsular laxity and rotator interval dilatation are known to occur. 1,2 The Bankart lesion is an avulsion of the anterior–inferior labrum that starts from the glenoid rim and results in laxity of the antero-inferior glenohumeral ligament (AIGHL). 3 The surgical goal of Bankart repair is anatomical restoration of the labral complex to restore the tension of the AIGHL; subsequently, stability of the glenohumeral joint is achieved or reinforced to prevent re-dislocation or subluxation. The re-tensioning of the AIGHL as well as secure fixation of the capsulolabral tissues to the glenoid are the two critical factors for success. 4 Failure to achieve this has been shown to increase failure rates after arthroscopic Bankart repair (ABR), especially in young active patients in whom the incidence of re-dislocation is high. 5
Bankart repair can be performed using the traditional open technique or with the ABR, which is currently considered the gold standard procedure. 6,7 Arthroscopy provides a minimally invasive tool with both diagnostic and therapeutic potential. It also allows shorter hospital stay (day-case procedure) and rapid return to work. 8 A variety of arthroscopic techniques using different fixation devices have been described in the literature. 9 Among these, suture anchors are the most widely used device with favourable long-term outcomes. 10,11
Suture anchors, whether traditional (knotted) or knotless, should be placed in an adequate number at the appropriate angle and place. Capsulolabral fixation to the glenoid based on the use of three anchors placed at distinct points has been recommended. 10,12 These multiple points of fixation, opposite the inserted anchors, maintain the labral tissues in contact with the glenoid until healing occurs. The use of knotless anchors obviates the need for knot tying; this has proved to be a fast technique for secured labral fixation and will be the basis for the present article. 13
The purpose of this study was to compare the clinical outcomes of ABR at a mid-term follow-up in patients treated for post-traumatic AGHI using two different types of knotless suture anchors (KSAs): a permanent one, the PushLock (Arthrex Inc., Naples, Florida, USA) and an absorbable counterpart, the BioKnotless (DePuy Mitek, Warsaw, Indiana, USA).
Methods
Following Institutional Review Board approval, we conducted retrospective analysis of prospectively collected data of patients who underwent ABR using KSA for recurrent AGHI between January 2011 and August 2011. The inclusion criterion was recurrent AGHI (symptomatic subluxation or dislocation) of a traumatic aetiology with a confirmed Bankart lesion visualised on magnetic resonance imaging (MRI). The exclusion criteria were acute dislocations accompanied by glenoid or tuberosity fracture, rotator cuff tear, capsular laxity, posterior instability and multidirectional instability. Patients who underwent an additional procedure (capsular plication, thermal modification or interval closure) during the ABR were also excluded. Preoperative evaluation included history taking, physical examination and imaging work-up. The degree of instability, number of dislocations, details of the initial trauma, duration of immobilisation, time-to-surgery and expectations from surgery were recorded. Physical examination included range of motion measurement with a goniometer and laxity assessment using the sulcus sign, load and shift, apprehension, Jobe’s apprehension–relocation and posterior apprehension tests. Imaging work-up included shoulder radiography (antero-posterior and axillary views) and an MRI. The American Shoulder and Elbow Surgeons (ASES) and Constant–Murley (CMS) scores were recorded. 14,15
All operations were performed by a single surgeon using a standardised technique with the patient under general anaesthesia. Patients were operated in a beach-chair position, and the involved arm was kept in 10° of external rotation (ER) and abduction during the procedure to reduce post-operative ER restriction. The operated shoulders were evaluated for antero-posterior instability and inferior sliding. A standard posterior viewing portal and two anterior portals were established using the outside-in technique with a spinal needle to achieve proper placement of the cannulas. Diagnostic arthroscopy was initially performed to evaluate the labrum, rotator cuff, humeral head (Hill–Sachs lesion), biceps tendon and glenohumeral ligaments. Capsular laxity was examined with a probe and the drive-through sign was checked. After confirming antero-inferior instability caused by the Bankart lesion, the capsulolabral tissues were mobilised from the glenoid rim using a periosteal elevator and were shifted superiorly and laterally to the glenoid edge. We aimed whenever possible to insert three anchors; however, depending on the size of the lesion, only two anchors were required in some cases. These were placed between 1 o′clock and 5 o′clock positions for the right shoulder (7 and 11 o′clock positions for the left one). The patients were classified into two groups according to the type of KSA used: group 1 (PushLock) and group 2 (BioKnotless). Fixation was generally performed using size 2.9 × 12.5 mm2 anchor, with No. 2 FibreWire suture in the PushLock group and size 1 anchor, with No. 2/0 Ethibond suture in the BioKnotless group.
Post-operatively, the patients were placed in a shoulder immobiliser for 6 weeks. Passive pendular exercises were initiated at the third week, active range of motion exercises at the sixth week and full return to sports by the ninth month. All patients were followed up at the outpatient clinic at regular intervals (3 weeks, 6 weeks, 3 months and every 6 months thereafter). Post-operative assessment included evaluation of the ASES and CMS scores for shoulder function, recurrence of instability defined as re-dislocation or symptomatic subluxation preventing full return to daily activities or that necessitating additional surgical stabilisation and the degree of ER restriction.
Statistical analysis was performed using SPSS statistical software version 22 (IBM Corp., Armonk, New York, USA). Continuous variables are presented as means with standard deviations if they are normally distributed. Student’s t-test was employed to compare continuous variables that have normal distribution, while the Mann–Whitney test was used for variables with non-parametric distribution. Categorical variables are presented as proportions. The χ 2 or Fisher’s exact test was used to compare categorical variables, as appropriate.
Results
Thirty-two patients met our inclusion criteria and were included in the study. There were 16 patients in each group; all were male patients with a mean age of 22.8 ± 4.2 (range 18−37) years. The demographic and clinical parameters of both groups are summarised in Table 1. Physical examination revealed a positive apprehension test in all patients. Anterior translation was present in 13 patients (40.6%) and sulcus sign in 5 patients (15.6%). At the time of the procedure, one patient had insufficient anchor (group 1) and four anchors in four patients were broken (two patients in each group). The insufficient and broken anchors were removed and replaced. MRI revealed no post-operative complications related to anchor use, such as misplacement, backing out or chondrolysis.
The demographic and clinical parameters.a
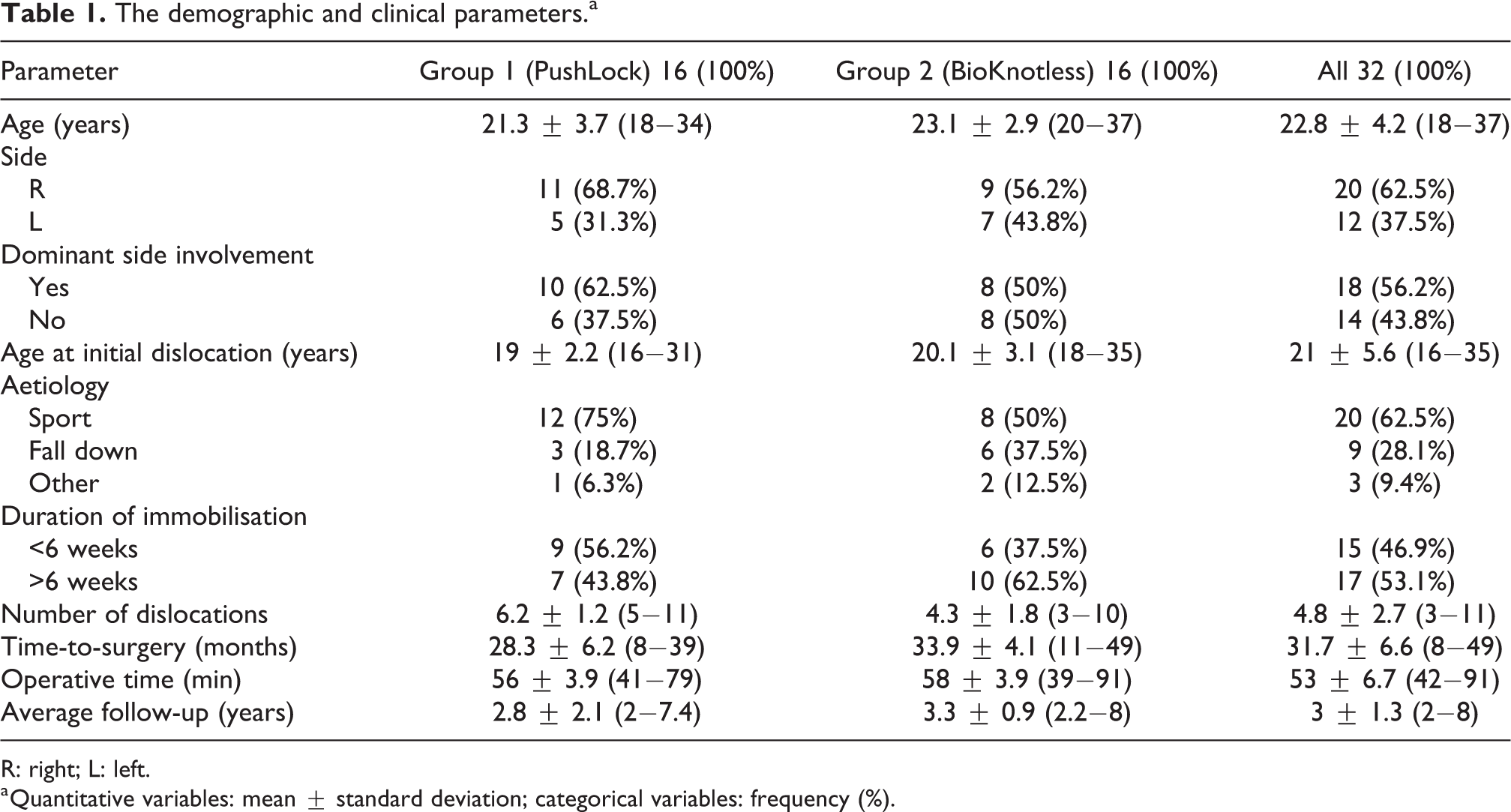
R: right; L: left.
a Quantitative variables: mean ± standard deviation; categorical variables: frequency (%).
The mean follow-up duration was 3 ± 1.3 (range 2−8) years. The mean preoperative ASES score significantly improved post-operatively at the time of the final follow-up in both groups. In group 1, the mean score improved from 60.47 ± 3.48 to 82.53 ± 7.85 (p < 0.0001); in group 2, it improved from 57.80 ± 3.23 to 81.13 ± 6.56 (p < 0.0001). The pre-and post-operative results of the CMS score are summarised in Tables 2 and 3. Of the 32 patients, three (9.4%) had post-operative recurrent AGHI; one re-dislocation occurred in group 1 (6.3%) and two symptomatic subluxations in group 2 (12.5%). The re-dislocation was treated with a Latarjet procedure and one of the dislocations was treated with redo KSA fixation; both patients had an uneventful post-operative course thereafter. The third patient refused further intervention. Fourteen patients in group 1 (87.5%) and 13 in group 2 (81.3%) could return to pre-injury level with regard to daily life and sports activities without significant differences between the groups (p = 0.32). The mean pre-and post-operative ER in group 1 and group 2 was 65.73 ± 1.98 and 63.27 ± 2.22 and 66.67 ± 1.63 and 63.87 ± 1.68, respectively. The mean ER was reduced by 2.46 in group 1 and by 2.8 in group 2 (p = 0.45); however, this did not reach statistical significance, nor did it affect function in either group.
The distribution of the overall pre-and post-operative Constant–Murley score.a
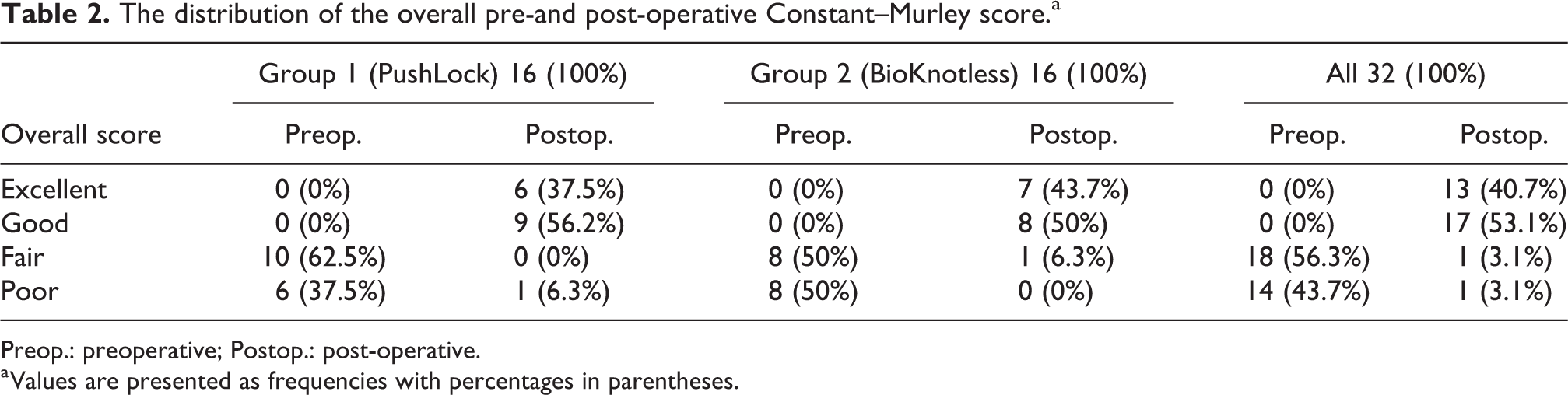
Preop.: preoperative; Postop.: post-operative.
a Values are presented as frequencies with percentages in parentheses.
The mean pre-and post-operative values of the individual items of the Constant–Murley score.
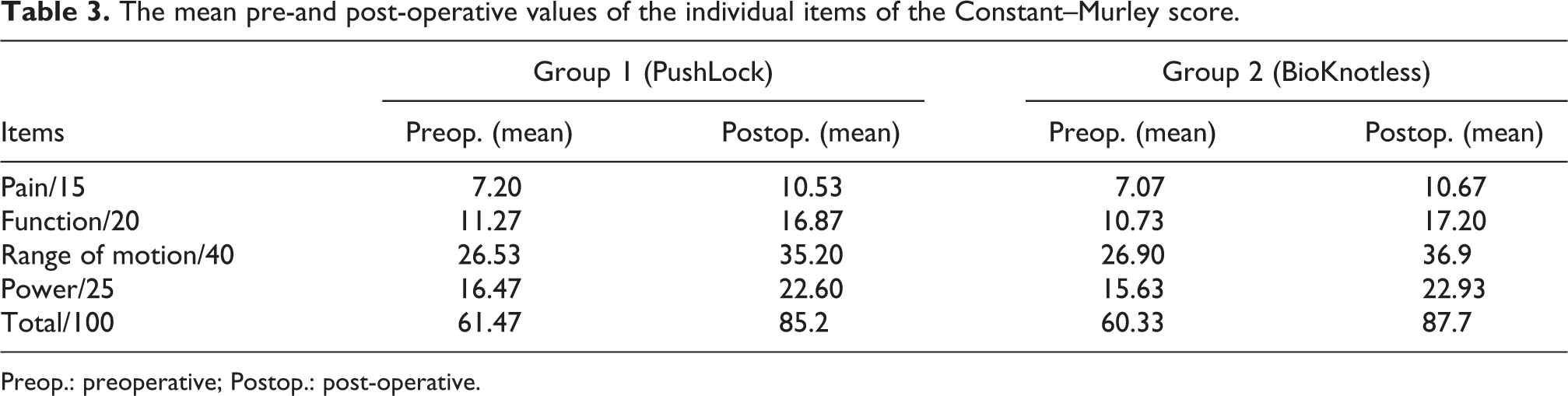
Preop.: preoperative; Postop.: post-operative.
Discussion
The challenge of ABR using traditional suture anchors (TSAs) is to tie consistent, good quality knots. KSA obviates the need for knot tying, which saves operative time. 16 There is also concern for the added height associated with TSA fixation, which has been supported by a case report of knot-induced glenoid erosion after an arthroscopic fixation SLAP repair procedure. 17,18 KSA has lower profile and offers more consistent tensioning as loop security is controlled by the depth of anchor insertion. 19 Both TSA and KSA have been shown to provide a stable anchor construct that withstands cyclic mechanical loading in vitro. 12 Slabaugh and colleagues found that KSA was as effective as TSA in tensioning the AIGHL and thereby in restoring the labral height. 20 Clinical studies comparing ABR using TSA and KSA have generally revealed comparable outcomes in terms of functional outcomes, recurrence of instability, return to pre-injury level and restriction of range of motion, in particular ER. 21 –24 Some studies have reported superior outcomes using KSA, but the difference in these series did not reach statistical significance. 23,24
Absorbable anchors were introduced to reduce the complications of implant loosening, migration and articular damage. With absorption over time, they minimise the interference with further revision surgery. Their radiolucent nature also minimises interference with MRI. Although they provide the necessary initial stability with comparable pull-out strength to metallic anchors, their mechanical characteristics decline with time due to degradation. 13 They are also associated with undesired biological responses such as osteolysis, synovitis and chondrolysis. 25
The first generation of absorbable anchors showed pronounced biological response and loss of primary stability due to rapid absorption. These were composed of polyglycolic acid (PGA) which takes 3–4 months for degradation.
26
The problem of rapid absorption was solved by replacing the PGA with poly-
Both PushLock and BioKnotless KSAs were included in the results of this study. The BioKnotless is an absorbable KSA composed of PLLA, whereas the PushLock is a permanent type composed of PEEK. 10 When comparing the mechanical strength, Peters and colleagues reported a significantly higher rate of re-dislocation and prolonged impairments in mobility and function when using an absorbable KSA compared to the permanent counterpart. 27 In a biomechanical study by Khoo and colleagues, the authors demonstrated a significantly weaker BioKnotless repair when compared to repairs with other three anchor systems, including the PushLock. 28 They also demonstrated the importance of the suture material, as the most common site and mode of failure was the suture pull-through the capsule rather than suture failure. The type of suture material in the BioKnotless is a braided suture, Panacryl or Ethibond, whereas in the PushLock, the suture is a fibre wire. When considering the biological reactions, the use of BioKnotless was associated with significant lower levels of cell proliferation and relatively high level of cell mortality compared to non-absorbable anchors, including the PushLock. 28 This is similar to the findings illustrated in other studies which cited poor labral healing, osteolysis, synovitis and chondrolysis as consequences of using absorbable anchors. 25,27 Whether these will affect clinical outcome will be another topic of study.
There is a paucity of literature comparing the long-term outcomes of Bankart repair using absorbable and permanent KSA. Thal and colleagues found no differences in re-dislocation rate or clinical outcomes when they compared metallic KSA with the BioKnotless. 29 Our findings also displayed comparable outcomes in both KSA groups at the mid term; however, long-term follow-up is warranted before definitive conclusions are made. Some newer designs include a combination of a bioabsorbable polymer and a bioceramic such as porous calcium phosphate. This combination allows for partial absorption and breakdown into calcium and phosphate substrates which provide a biological habitat for in vivo bone formation. In a prospective study by Randelli and colleagues, the authors demonstrated excellent clinical and radiological outcomes of the Bankart repair at a mean of 29 months; the anchors were made of 70% polylactic co-glycolide and 30% β-tricalcium phosphate. 30 In a more recent study, Sugaya and colleagues reported similar promising outcomes of the Bankart repair at a mean of 2 years using a similar biocomposite anchor. 31
Of the entire cohort, approximately 85% of the patients in our series had excellent outcomes and could return to their pre-injury level of functioning, which is comparable to that reported by Hayashida and colleagues (87%). 19 Likewise, there was 2° to 3° loss of ER in our series, which is consistent with the results of other series. 11,21 –23 Recent ABR studies reported recurrence rates between 4% and 11%; our finding of a 9.4% recurrence rate is in concert with these reports. 8,24,32 KSA failure due to migration, loosening, insufficiency or breakage has been reported. 29 We had few incidents of intraoperative anchor breakage of both types without any noticeable predilection for either. Most incidents of breakage occurred for anchors inserted early in our experience. Inappropriate under-drilling of the anchor hole, which is not described by the manufacturer, was the cause of breakage of some anchors in our series. We therefore avoided such off-label use in later procedures.
We acknowledge several limitations of the present study. First, it was retrospective in nature, with the inherent inaccuracies; however, data were prospectively collected. Second, the number of groups being compared was relatively small. Finally, although being a single-surgeon cohort reduces confounders, it more importantly limits the generalisability of our conclusion. Larger, multicentre prospective studies with long-term follow-up are warranted.
Conclusion
ABR for recurrent AGHI using a permanent or absorbable KSA offers comparable successful outcomes without a statistically significant difference.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.