
Abstract
Background:
After posterior cruciate ligament reconstruction (PCLR), functional deficits at the knee can persist. It remains unclear if neighboring joints compensate for the knee during demanding activities of daily living.
Purpose:
To assess long-term alterations in lower limb mechanics in patients after PCLR.
Study Design:
Descriptive laboratory study.
Methods:
A total of 28 patients who had undergone single-bundle unilateral isolated or combined PCLR performed stair navigation, squat, sit-to-stand, and stand-to-sit tasks at 8.2 ± 2.2 years after surgery. Motion capture and force plates were used to collect kinematic and kinetic data. Then, 3-dimensional hip, knee, and ankle kinematic data of the reconstructed limb were compared with those of the contralateral limb using statistical parametric mapping.
Results:
Side-to-side differences at the knee were primarily found during upward-driven movements at 8 years after surgery. The reconstructed knee exhibited lower internal rotation during the initial loading phase of stair ascent versus the contralateral knee (P = .005). During the sit-to-stand task, higher flexion angles during the midcycle (P = .017) and lower external rotation angles (P = .049) were found in the reconstructed knee; sagittal knee (P = .001) and hip (P = .016) moments were lower in the reconstructed limb than the contralateral limb. In downward-driven movements, side-to-side differences were minimal at the knee but prominent at the ankle and hip: during stair descent, the reconstructed ankle exhibited lower dorsiflexion and lower external rotation during the midcycle versus the contralateral ankle (P = .006 and P = .040, respectively). Frontal hip moments in the reconstructed limb were higher than those in the contralateral limb during the stand-to-sit task (P = .010); during squats, sagittal hip angles in the reconstructed limb were higher than those in the contralateral limb (P < .001).
Conclusion:
Patients after PCLR exhibited compensations at the hip and ankle during downward-driven movements, such as stair descent, squats, and stand-to-sit. Conversely, residual long-term side-to-side differences at the knee were detected during upward-driven movements such as stair ascent and sit-to-stand.
Clinical Relevance:
After PCLR, side-to-side differences in biomechanical function were activity-dependent and occurred either at the knee or neighboring joints. When referring to the contralateral limb to assess knee function in the reconstructed limb, concentric, upward-driven movements should be prioritized. Compensations at the hip and ankle during downward-driven movements lead to biases in long-term functional assessments.
The posterior cruciate ligament (PCL) stabilizes the knee by restricting posterior tibial translation. 2 A PCL injury alters joint stability and mechanical loading, 6 particularly during demanding activities of daily living (ADLs) such as stair ascent. 15 PCL reconstruction (PCLR), combined with posterolateral corner stabilization, 26 is typically indicated to improve patient outcomes and passive knee stability 1 and to restore native joint biomechanics. 45 However, the biomechanics of the knee after PCLR during ADLs remain poorly understood.
Investigations of in vivo knee biomechanics after PCLR are scarce. Earlier studies have examined knee joint kinematics, forces, moments, and muscle activity during gait in unilateral isolated and combined PCL injuries.5,18,42 Yet, gait may be inappropriate for identifying side-to-side functional differences at the knee15,39 because patients after PCLR exhibit bilateral gait symmetry that differs from that of healthy controls. 5 As a result, investigations of comparatively more biomechanically challenging ADLs may be better suited to identify within-patient differences in lower limb biomechanics.
Demanding activities can produce higher forces directly at the knee joint, require a larger knee range of motion, or necessitate greater involvement of the quadriceps and hamstring muscles. Stair navigation is a common ADL that leads to peak contact loads in the knee joint that are multiples higher compared with level walking.8,43 Conversely, squatting requires greater demands from the quadriceps and hamstring muscles compared with gait, 11 as rising from and sitting down in a chair require a larger range of motion at the knee. 3 Hip and ankle motion can greatly influence knee biomechanics during challenging ADLs because of the biarticular nature of the hamstring, gastrocnemius, and rectus femoris muscles.7,16,24,28 Although many of these ADLs similarly increase demands across the entire limb, the majority of investigations of both PCL-reconstructed and PCL-deficient knees have focused solely on knee joint biomechanics, neglecting proximal and distal joints of the lower limb chain. By limiting the focus to the knee, compensations at the hip and ankle are not adequately addressed. 5
Thus, the aim of this work was to determine whether side-to-side differences in the biomechanics of the knee, ankle, and hip exist at 8 years after the reconstruction of unilateral isolated and combined PCL injuries during high-demand ADLs. To achieve this, we analyzed lower limb kinematic data of a PCLR cohort for 5 ADLs: squat, stair ascent, stair descent, sit-to-stand, and stand-to-sit. Lower limb joint moments were also examined for the squat, sit-to-stand, and stand-to-sit tasks. Because these ADLs are more demanding than gait, we hypothesized that these ADLs would result in long-term bilateral differences in knee joint biomechanics after PCLR. Furthermore, based on previous studies,15,29 we hypothesized that both the stair ascent and the squat tasks would result in compensations at the hip and ankle after PCLR, resulting in side-to-side differences at these joints.
Methods
Patient Cohort
The initial study cohort included 49 patients identified from our medical center database, who had available clinical and motion analysis data at a minimum of 2 years after surgery and had undergone PCLR at our orthopaedic clinic (Figure 1). All protocols for the study were approved by the local ethics committee, and all participants provided written informed consent before enrollment. Patients were recruited consecutively between 2012 and 2013 and were included in the study according to the following criteria: 25 to 60 years of age at the time of recruitment and having undergone primary, unilateral reconstructive surgery for a PCL tear using a single-bundle (anterolateral bundle) technique. 22 Patients were included in this PCLR cohort if the procedure was isolated PCLR or PCLR combined with anterior cruciate ligament (ACL) reconstruction and/or reconstruction of the posterolateral corner.
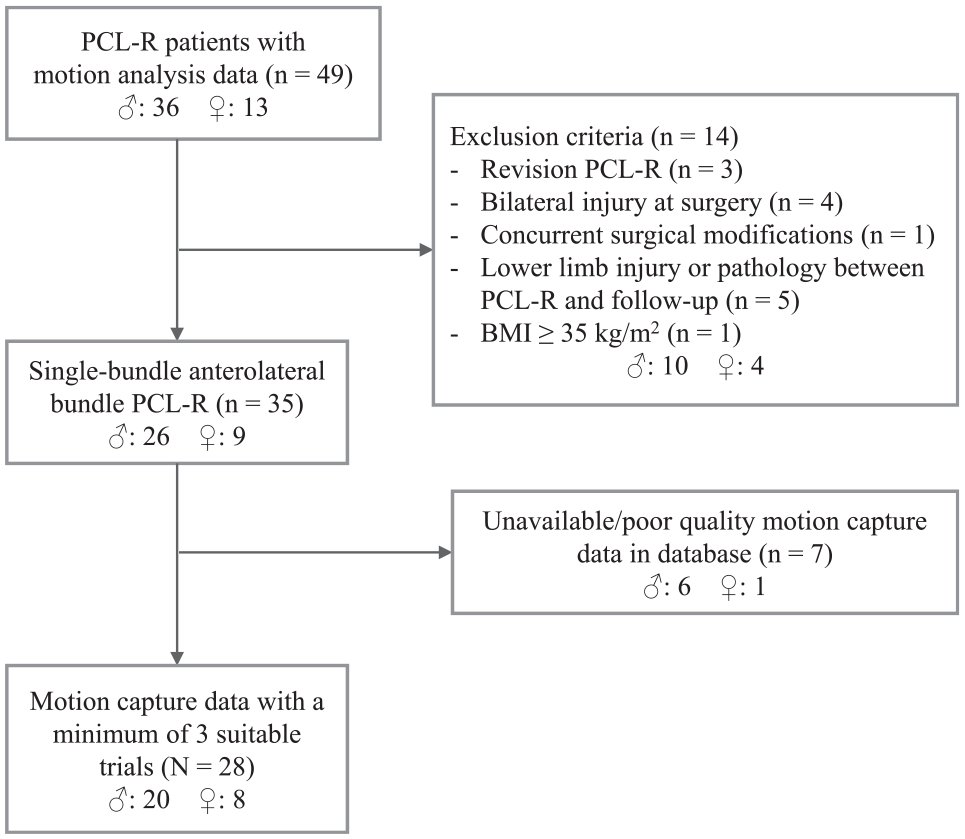
Flowchart describing the inclusion of study patients. BMI, body mass index; PCL-R, posterior cruciate ligament reconstruction.
Exclusion criteria were as follows: bilateral PCL injuries, revision PCLR, concurrent surgical modifications during PCLR such as lateral collateral ligament refixation, other lower limb injuries or abnormalities between surgery and the time of motion capture/data collection, and a body mass index ≥35 kg/m2. Furthermore, patients were excluded from the study if motion capture data from fewer than 3 suitable trials were available for analysis for all ADLs.
Surgical Technique
All patients underwent primary, unilateral PCLR performed by a single surgeon using a conventional tibial tunnel and single-incision femoral technique. 22 Hybrid tibial fixation was used with suture backup, and maximal pretension was applied manually with the knee in 60° to 80° of flexion. A 5-strand semitendinosus and gracilis tendon autograft from the ipsilateral knee was the primary graft used. The modified Larson technique using the contralateral semitendinosus tendon was used to stabilize the posterolateral corner via 2 small incisions. 25 If the primary graft choice was not feasible, fresh-frozen allograft tissue from the local clinic tissue bank was used instead (n = 1). When needed, an anatomic single-bundle technique using a femoral tunnel drilled via the anteromedial portal was used for ACL reconstruction. Fixation was performed with a biodegradable interference screw using contralateral tissue from either a 4-fold gracilis tendon autograft or an allograft.
Rehabilitation
The primary rehabilitative goal for the initial 10 weeks after surgery was to minimize knee swelling and to improve knee range of motion. The knee was immobilized for the first 6 weeks with a posterior tibial support splint (Medi), with gradual passive flexion mobilization performed with the patient in a prone position. Assistive crutches were also used with an initial recommendation of 15 kg of toe-touch weightbearing on the ipsilateral limb, with a gradual increase in applied loads as tolerated until crutch disuse at 6 weeks. After 6 weeks, knee joint mobilization beyond 90° of flexion was allowed. From 10 weeks after surgery, quadriceps strengthening exercises were permitted. Active hamstring contractions were disallowed until after 16 weeks.
Clinical Assessment
A total of 28 patients were analyzed in this study (Table 1). The PCL tears were either isolated or combined with tears of other structures, such as the ACL and posterolateral corner (Table 1). The mechanisms of injury included sporting activity, motor vehicle accident, ADLs, and unreported (Table 1). Furthermore, patients completed the International Knee Documentation Committee (IKDC) form to assess their subjective knee status with regard to symptoms, function, and participation in sports. 19 A minimum IKDC score of 0 indicates a high prevalence of knee symptoms and low levels of function and sports activity, and a maximum IKDC score of 100 indicates limited knee symptoms and high levels of function and sports activity.
Patient Characteristics a
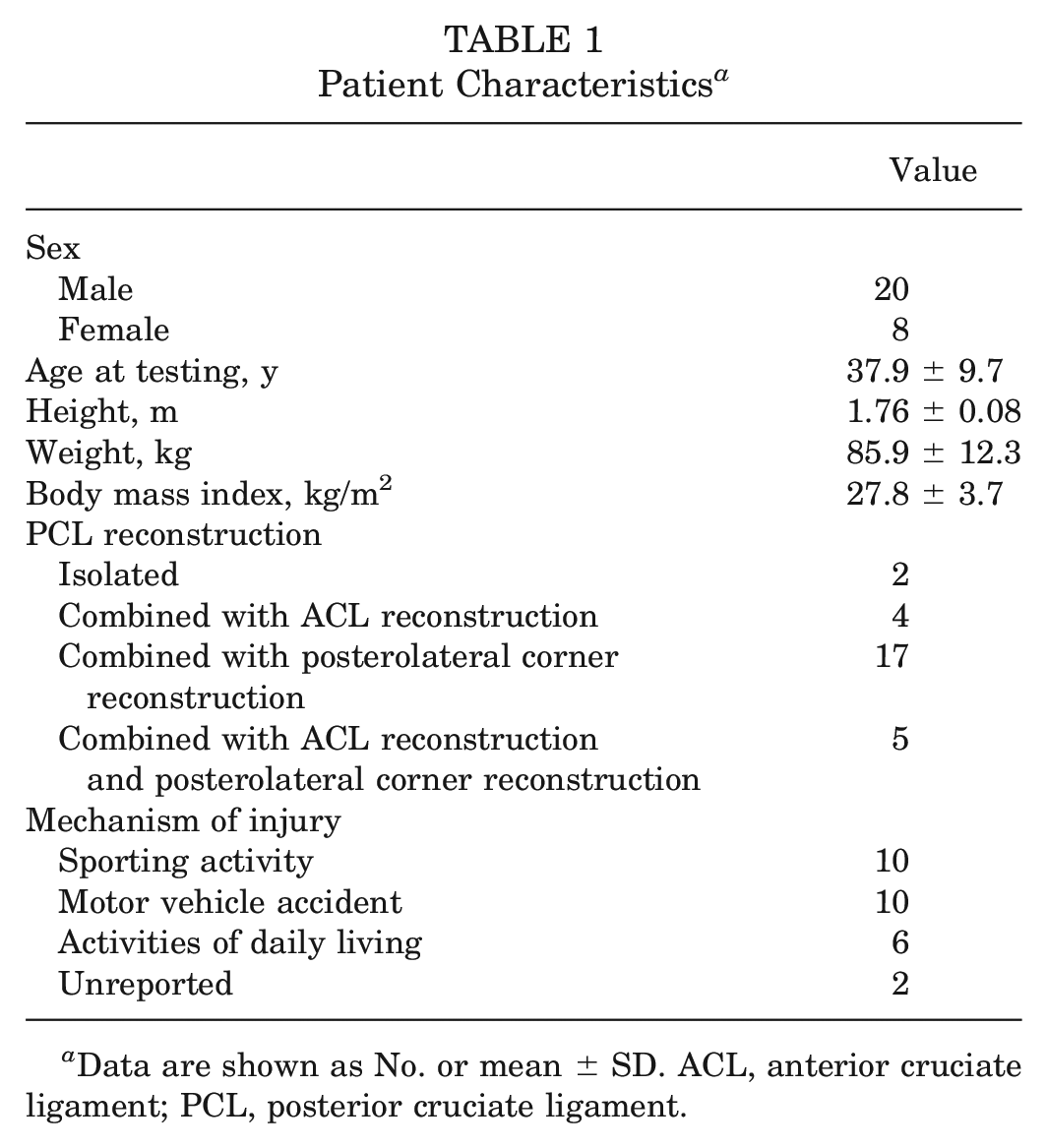
Data are shown as No. or mean ± SD. ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
Biomechanical Assessment
Patients underwent a biomechanical assessment at a mean 8.2 ± 2.2 years after surgery. Patients donned tight-fitting shorts and tops to maximize access to the lower limbs for marker placement. Lower limb joint kinematic data were assessed using 52 reflective markers placed on bony and segment landmarks according to a standardized protocol. 41 Then, 3-dimensional marker trajectories during movement trials were recorded using 10 infrared cameras operating at 120 Hz (T20S; Vicon). Kinematic data were collected for 5 different movements: stair ascent, stair descent, squat, rising from a seated position in a chair to a standing position (“sit-to-stand”), and sitting down into a chair from a standing position (“stand-to-sit”). Ground-reaction forces were recorded synchronously with 2 force plates at 960 Hz (BP400600; AMTI) during the squat, sit-to-stand, and stand-to-sit tasks. All tasks were performed barefoot and at a self-selected pace. A minimum of 3 successful trials were conducted for each task.
Stair ascent and descent were performed on a custom-made 4-step staircase. Patients ascended and descended the staircase, pausing at the top landing and avoiding the use of a safety handrail. All tasks were initiated from a standing position, with the lead leg alternating between trials. Stair ascent movement cycles started with contact of the index foot on the first step and ended with contact of that same foot on the third step; stair descent movement cycles started with foot contact on the third step and ended with contact of the same foot on the first step (Figure 2).
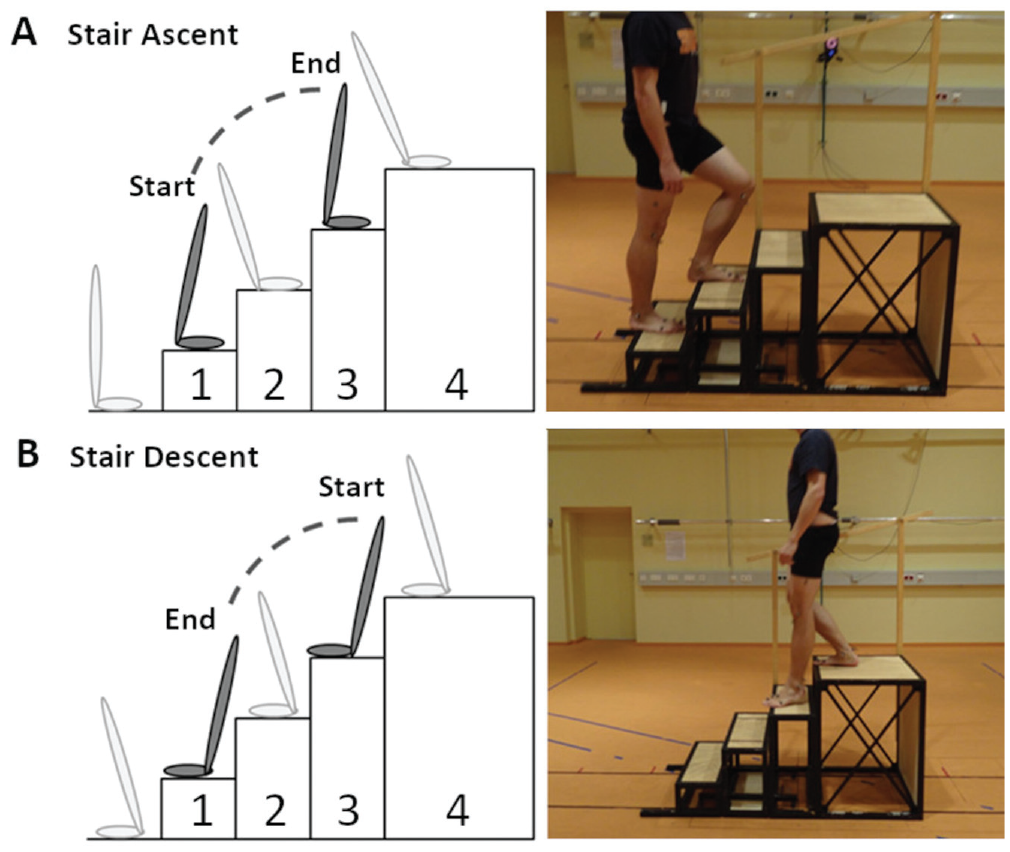
Depiction of movement cycles relevant for (A) stair ascent and (B) stair descent on a custom-built staircase (right column). (A) Stair ascent cycles were defined from 0% to 100%, beginning with contact of the index foot on the first step and ending at contact of that same foot on the third step. (B) Stair descent cycles were defined between 0% and 100%, starting with contact of the index foot on the third step and ending with contact of that same foot on the first step.
Squats were performed from an upright position with feet flat on the floor and shoulder-width apart, with arms extended anteriorly. Patients squatted to their lowest attainable depth and ascended to the starting position. Squat movement cycles began at the initiation of knee flexion from a standing position and finished once the patient reached a standing position, with the cessation of knee extension. Both the sit-to-stand and stand-to-sit tasks were performed at a self-selected pace with a chair at a seat height of 44 cm and without armrests. Stand-to-sit movement cycles began at the initiation of knee flexion from standing and ended once hip extension was unchanged at the point of pelvic retroversion. Sit-to-stand movement cycles started once hip flexion began with pelvic anteversion and ended once the patient was in a standing position, with the cessation of knee extension.
Motion capture data were filtered using a second-order low-pass Butterworth bidirectional filter (6-Hz cutoff). Next, 3-dimensional lower limb joint angles were calculated using a floating axis coordinate system 47 in which lower limb joint external moments were determined using inverse dynamics. 46 Although marker-based joint kinematics can deviate from true skeletal motion as previously reported for the knee,4,27 the resulting angles and moments across the hip, knee, and ankle have demonstrated acceptable measurement errors. 13 For each trial, waveforms were normalized to 100% of the respective movement cycles. These time-normalized waveforms were generated for hip, knee, and ankle angles as well as external moments during the squat, sit-to-stand, and stand-to-sit tasks.
Statistical Analysis
For each patient, mean waveforms were calculated for each parameter in MATLAB (R2018; MathWorks). All waveforms were tested for normality before analysis within the statistical parametric mapping (SPM) library. 14 To perform within-patient comparisons between parameters of the reconstructed and contralateral limbs, the paired t test was applied for the waveforms of normally distributed parameters using SPM. 14 For parameters that did not satisfy normality, the repeated-measures Shapiro-Wilk test was applied using statistical nonparametric mapping (SnPM). All SPM and SnPM analyses were conducted in MATLAB using open-source spm1d (Version M.0.4.5; www.spm1d.org), with an alpha level of .05. Specific details outlining SPM have been reported previously.14,31 SPM allows for the consideration of the entire time series as well as the identification of time regions in the waveform where the independent variable has significant effects and where a critical threshold is exceeded. 14 When periods of significance were identified for a given activity and parameter, the maximum difference between the waveforms within this given time region was calculated for each patient, with group means and 95% CIs of the maximum differences reported. Negative values indicated that the given parameter was lower for the reconstructed limb than for the contralateral limb; positive values indicated that the given parameter was higher for the reconstructed limb than for the contralateral limb.
Results
Patient-Reported Outcomes
Patients reported some knee symptoms and functional limitations, as demonstrated by a mean IKDC score of 75.5 ± 15.8.
Stair Ascent
Significant differences during all tasks are summarized in Table 2. For stair ascent (n = 28), internal rotation was lower for the reconstructed knee at 5% to 11% of the movement cycle (P = .005). No kinematic differences were found in the other planes of motion at the knee. Additionally, no differences between the reconstructed and contralateral hips and ankles were identified during stair ascent.
Differences Between Reconstructed and Contralateral Limbs During Activities of Daily Living
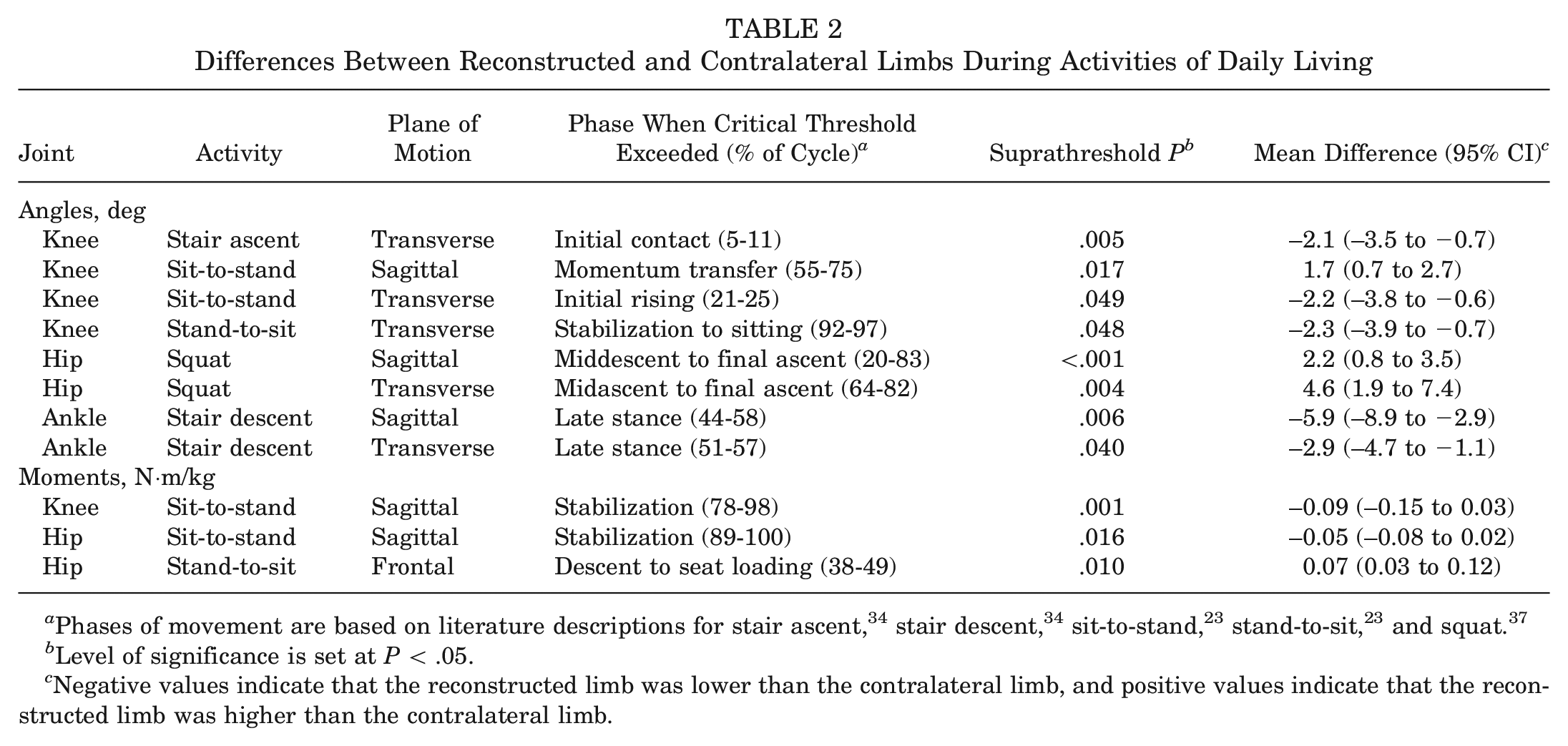
Phases of movement are based on literature descriptions for stair ascent, 34 stair descent, 34 sit-to-stand, 23 stand-to-sit, 23 and squat. 37
Level of significance is set at P < .05.
Negative values indicate that the reconstructed limb was lower than the contralateral limb, and positive values indicate that the reconstructed limb was higher than the contralateral limb.
Stair Descent
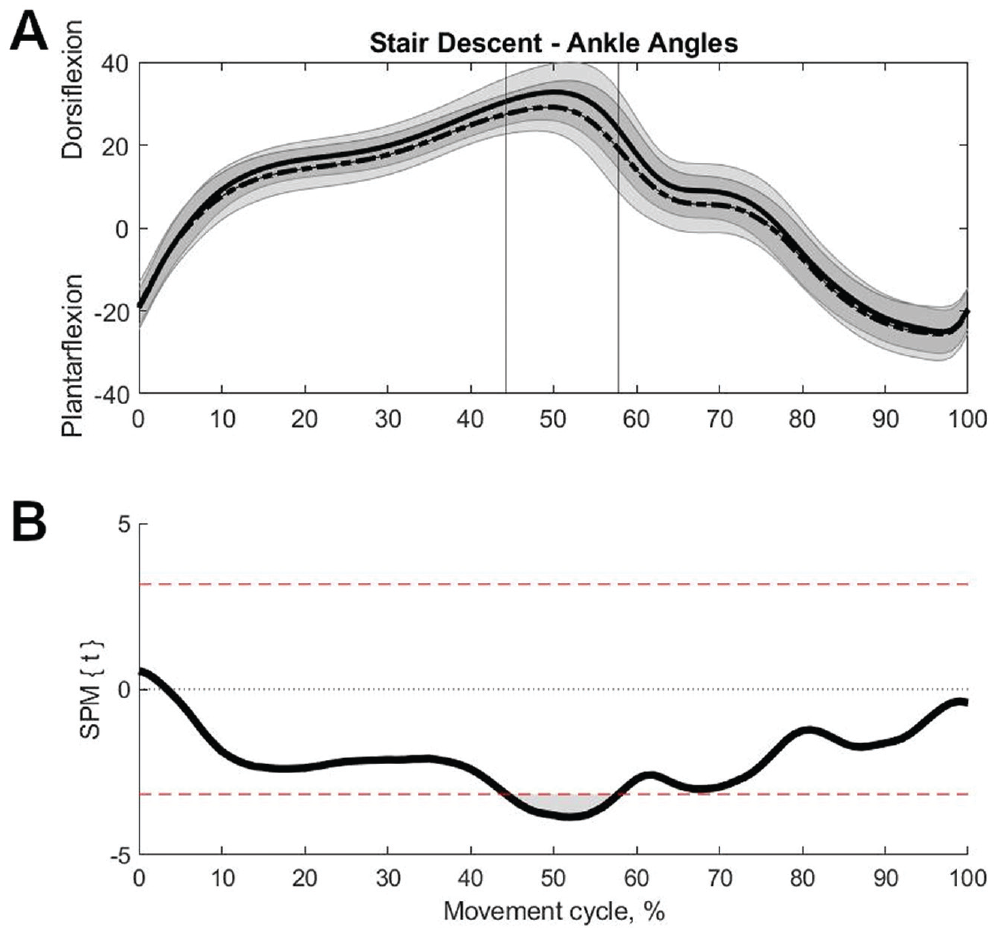
For stair descent (n = 28), the reconstructed limb exhibited lower dorsiflexion from 44% to 58% of the movement cycle (P = .006) (Figure 3) and lower external rotation at the ankle from 51% to 57% of the movement cycle (P = .040) compared with the contralateral limb. No further differences in ankle kinematics, and no differences in knee and hip kinematics, were found between the reconstructed and contralateral limbs during stair descent.
(A) Mean with SD (shaded area) sagittal ankle angles of the posterior cruciate ligament (PCL)–reconstructed (dashed line) and contralateral (solid line) limbs as well as (B) resultant statistical parametric mapping (SPM) test values for 0% to 100% of the stair descent movement cycle. Top and bottom dashed lines in (B) correspond to 95% CI threshold values of t* = ±3.17, beyond which curves significantly differ. Vertical lines in (A) at 44% to 58% of the movement cycle correspond to the shaded areas identified as significantly lower for the PCL-reconstructed ankle compared with the contralateral ankle (P = .006) in (B).
Sit-to-Stand
For sit-to-stand (n = 18), the reconstructed knee exhibited higher flexion angles from 55% to 75% (P = .017) and lower external rotation angles from 21% to 25% (P = .049) of the movement cycle than the contralateral knee. These were the only side-to-side differences found in lower limb kinematics; knee angles in the frontal plane, and all angles of the hip and ankle, were found to be similar. Regarding joint moments, side-to-side differences were identified toward the end of the movement cycle. Both sagittal knee moments (78%-98% of the cycle; P = .001) and sagittal hip moments (89%-100% of the cycle; P = .016) were lower for the reconstructed limb than the contralateral limb. No differences in moments were identified in the other planes of motion at the knee and hip or in any plane at the ankle.
Stand-to-Sit
For stand-to-sit (n = 21), the reconstructed knee exhibited lower external rotation angles than the contralateral knee at 92% to 97% of the cycle (P = .048). Also, frontal hip moments for the reconstructed limb were higher compared with the contralateral limb at 38% to 49% of the cycle (P = .010). No differences were found for other joint moments or for any kinematic parameters.
Squats
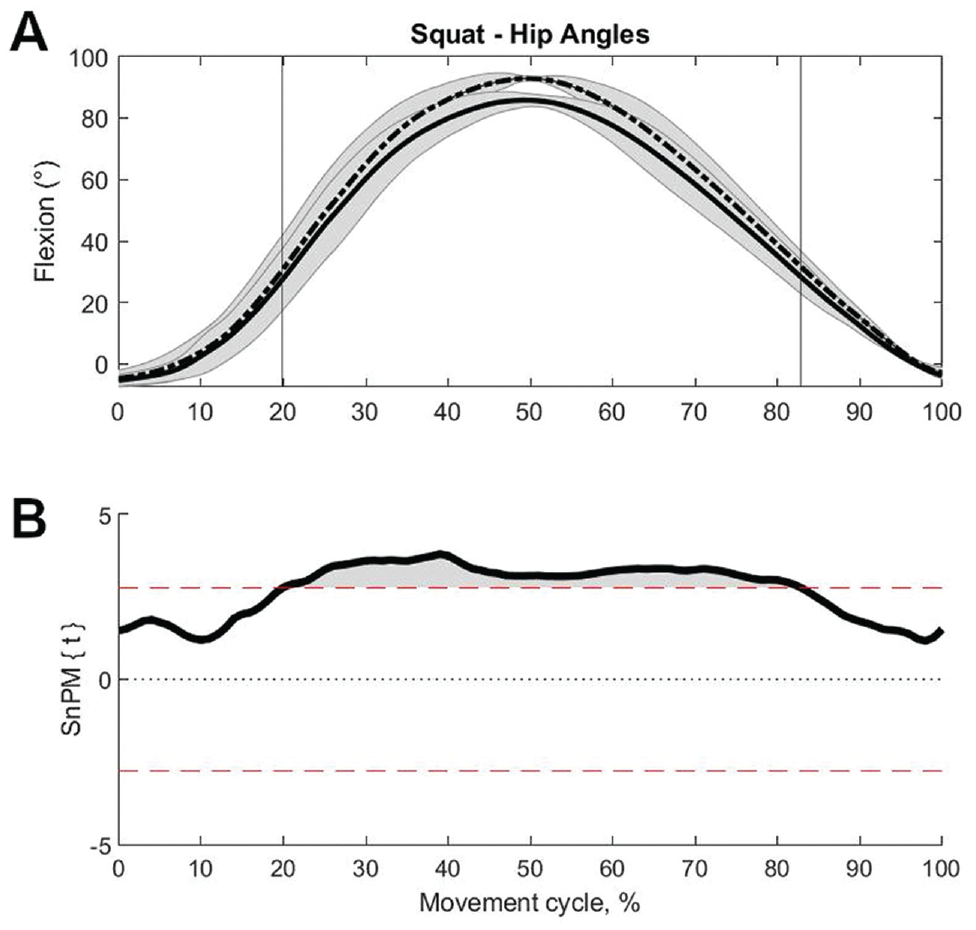
For squats (n = 19), the sagittal hip angle was higher in the reconstructed limb compared with the contralateral limb between 20% and 83% of the cycle (P < .001) (Figure 4). Furthermore, during the ascending portion, the transverse hip angle was higher in the reconstructed limb compared with the contralateral limb between 64% and 82% of the cycle (P = .004). No further differences were found in kinematics and moments between limbs.
(A) Mean with SD (shaded area) sagittal hip angles of the posterior cruciate ligament (PCL)–reconstructed (dashed line) and contralateral (solid line) limbs as well as (B) resultant statistical nonparametric mapping (SnPM) test values for 0% to 100% of the squat movement cycle. Top and bottom dashed lines in (B) indicate 95% CI threshold values of t* = ±2.77, beyond which curves significantly differ. Vertical lines in (A) at 20% to 83% of the movement cycle correspond to the shaded areas identified as significantly higher for the PCL-reconstructed hip versus the contralateral hip (P < .001) in (B).
Discussion
To our knowledge, this is the first long-term in vivo biomechanical analysis of patients after PCLR while performing various ADLs that elicit different demands on the lower limb joints compared with gait. Our first hypothesis was partially supported. The stair ascent and sit-to-stand tasks exhibited primary side-to-side differences in the transverse and sagittal planes of the knee, respectively. Our second hypothesis was also partially supported. Side-to-side differences between the reconstructed and contralateral limbs were identified only at the ankle during stair descent and exclusively at the hip for both the stand-to-sit and the squat tasks. These collective findings highlight the importance of the activity used to assess knee function when referring to the contralateral limb. These results imply that compensatory biomechanics exhibited distal and proximal to the reconstructed knee were activity-dependent.
In particular, movements performed in a downward-driven direction—stair descent, stand-to-sit, and squats—resulted only in side-to-side differences distal and proximal to the knee. These movements are dominated by eccentric muscle actions, which enable controlled lowering of the body. Stair descent, 30 stand-to-sit, 21 and the descending portion of the squat 44 all involve eccentric activation of the quadriceps muscle. During stair descent, the reconstructed ankle exhibited lower dorsiflexion angles than the contralateral ankle from 44% to 58% of midstance. At this time of double-leg support, forward propulsion occurs with controlled dorsiflexion30,34 and knee flexion, weight is transferred to the opposite limb, and plantarflexor muscles are minimally activated. 38 Limited dorsiflexion can reduce forward progression of the tibia when stepping down, resulting in hip and knee kinematics that deviate from uninjured populations. 35 Here, when using the contralateral limb as a reference, there were minimal differences at the hip and knee after PCLR. However, this does not necessarily indicate that these parameters are comparable with those of uninjured persons, as observed in gait after PCLR. 5 As a result, this ankle-dominant compensation in this particular PCLR population was only apparent during stair descent, which is an open-chain downward movement.
On the other hand, closed-chain downward movements implicated hip-dominant compensation on the reconstructed limb. During stand-to-sit, the reconstructed limb exhibited higher frontal moments at the hip compared with the contralateral limb at 38% to 49% of middescent. During this movement, the gluteal and hamstring muscles are activated, with support from the quadriceps and gastrocnemius muscles. 3 Considering that quadriceps atrophy has been previously observed after a PCL injury, 9 gluteal muscles may possibly compensate for limited quadriceps function after a PCL injury, 42 although this speculation could not be confirmed in this study because of the lack of electromyographic data. A similar observation was observed during the squat: sagittal angles were higher in the reconstructed hip compared with the contralateral hip between 20% and 83% of the movement cycle, with no differences found at the knee. Additional analysis of the sagittal angles across all joints during the squat yielded no significant differences between the reconstructed and contralateral limbs. These results are in contrast to previous results in patients at 3 years after a PCL injury, with side-to-side differences in knee extension moments during downward squats. 29 Patients after PCLR 29 and ACL reconstruction 36 compensate at the hip during squats, with patients having undergone PCLR additionally compensating at the ankle. 29 However, these differences may be caused by variations in both treatment and injury types, as previous studies investigated only isolated PCL injuries, whereas the PCLR cohort investigated here included both isolated and combined PCL injuries. Notably, the majority of patients analyzed here (n = 22) underwent stabilization of the posterolateral corner, which was achieved using an autograft from the contralateral semitendinosus tendon. Potential limited contributions from this muscle on the contralateral limb may have also affected these measurements but cannot be confirmed within the scope of this study.
Side-to-side differences between the reconstructed and contralateral knees were often identified in upward movements that are dominated by concentric contraction of the quadriceps muscle, but not exclusively. During stair ascent, the reconstructed knee exhibited less internal rotation during initial loading of the limb at 5% to 11% of the movement cycle. Previous fluoroscopic results in patients after PCLR during stair ascent, however, found no significant differences in transverse-plane kinematics but did identify posterior subluxation in the early stance. 15 The results here are also in contrast to findings in patients after ACL reconstruction, who compensate at the hip during the stair ascent 17 and lateral step-up tasks, 10 with the latter activity also leading to compensation at the ankle. During sit-to-stand, the reconstructed knee demonstrated higher flexion angles during midascent at 55% to 75% of the movement cycle and exhibited reduced sagittal moments at 78% to 98% of the movement cycle. The sit-to-stand task additionally exhibited reduced sagittal hip moments for the reconstructed limb between 89% and 100% of the movement cycle. In contrast to the other upward movements, during the ascent portion of the squat, the only side-to-side differences were identified at the hip, with the reconstructed hip having a higher transverse angle than the contralateral hip between 64% and 82% of the cycle. Considering that the descent portion of the squat directly preceding this yielded no differences at the knee and only differences at the hip, this likely forms a basis as to why no differences were identified during this movement. Both the stair ascent and the sit-to-stand tasks are, in comparison, independent movements. These upward movements combine knee flexion with increased demands on the knee extensor muscles, 30 which can result in shear forces at the joint 40 and thus support soft tissue such as the reconstructed PCL.
The mean IKDC score of 75.5 ± 15.8 indicated that patients still exhibited some knee-related symptoms that affected function in daily life and participation in sports. For the more challenging ADLs investigated in this study, not all movements resulted in differences in knee biomechanics. In particular, activities that involved downward movements identified compensations at the hip and ankle, which ultimately resulted in apparent functional symmetry at the knee.
The present study has some limitations. First, a healthy, uninjured control group was not included for comparison with the patients who underwent PCLR. Although the focus of this study was to examine side-to-side differences within the investigated cohort, previous PCLR 5 and PCL-deficient 20 analyses have demonstrated that patients exhibit altered biomechanics after PCL surgery/injuries compared with healthy controls. Second, the included cohort was relatively heterogeneous. Because of the nature of the injuries sustained, most patients underwent the reconstruction of neighboring structures such as the posterolateral corner and ACL in addition to the PCL. The graft type also varied between patients because the primary graft choice was not always feasible. As a result, interpretations of these results regarding the effect of surgery on lower limb biomechanics during demanding ADLs are limited. Third, joint moments could not be calculated for stair navigation trials because of the lack of force plates on the stairs. Electromyography could have provided additional information about muscle activity, but such measurements were unavailable and were beyond the scope of this investigation. Fourth, this investigation was limited to ADLs. These included activities that could be plausibly performed by all participants without difficulty, and the ability to perform these activities should not require particular fitness or motor skills. Although more high-demand activities such as running and cutting movements could induce larger side-to-side differences in joint biomechanics, increased activity intensity has been linked to increased measurement errors, 27 particularly in the frontal and rotational planes. 4 Fifth, the small sample size may have precluded the detection of significant differences (ie, increased type II error rate). Sixth, multiple comparisons may have inflated the type I error rate, but adjustments (eg, Bonferroni) in SPM can be overly conservative.32,33 Finally, it was unknown whether patients developed knee osteoarthritis, as this condition could alter or affect lower limb biomechanics. 12
In addition, some significant side-to-side differences identified by paired SPM tests only occurred during a short phase of the cycle; for example, for stand-to-sit, transverse knee angles were found to be significantly different between 92% and 97% of the movement cycle (P = .048). Although SPM advantageously allows entire waveforms to be objectively compared, and thus excludes biases caused by only examining certain temporal aspects of a time series, the use of SPM can also identify statistical differences that may not be clinically relevant or easily interpretable.
Conclusion
Patients after PCLR exhibited long-term side-to-side differences with compensatory consequences at the hip and ankle during the stair descent, squat, and stand-to-sit tasks. On the other hand, persistent side-to-side differences at the knee were identified during stair ascent and sit-to-stand. These results suggest that, depending on the selected activity, side-to-side comparisons of only knee biomechanics after PCLR may not be indicative of overall functional deficits during demanding ADLs, as they have not included the recognition of possible compensatory adaptations that occur in the ipsilateral ankle and hip.
Footnotes
Acknowledgements
The authors thank Leonie Krahl, Yanlin Zhong, Julia Ohde, and Teresa Benert for their assistance in data collection and processing, as well as the study participants for making this work possible.
Submitted April 26, 2023; accepted February 29, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.N.D. has received consulting fees from Pluristem, DePuy Synthes, Implantec, Implantcast, and Stryker; has grants or grants pending with Pluristem, DePuy Synthes, Implantec, Implantcast, Smith & Nephew, Stryker, and Zimmer; and has patents (planned, pending, or issued) with Pluristem and B&C for work unrelated to this particular study. T.M.J. has received support for education and hospitality payments from Smith & Nephew, Richard Wolf, and DJO Global. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.