
Abstract
Background:
It remains unclear how posterior cruciate ligament (PCL) reconstruction influences long-term lower extremity joint biomechanics.
Purpose:
To determine whether patients who underwent PCL reconstruction exhibited long-term alterations in lower limb gait mechanics.
Study Design:
Controlled laboratory study.
Methods:
A total of 26 patients underwent gait analyses at 8.2 ± 2.6 years after primary unilateral PCL reconstruction. Sex- and age-matched healthy controls were analyzed for comparison. Gait data were collected using motion capture and force plates. Hip, knee, and ankle angles and moments were compared during initial contact, early stance, and late stance for the reconstructed and uninjured contralateral limbs of patients who underwent PCL reconstruction (PCL group) as well as the limbs of healthy control participants (CON group).
Results:
No side-to-side kinematic differences were noted between the reconstructed and contralateral limbs of the PCL group; some trivial differences were noted in knee and hip moments. However, major differences between the PCL and CON groups occurred at the knee. Reconstructed and contralateral limbs of the PCL group exhibited larger knee flexion angles during initial contact (Δ = 7.0° [P < .001] and Δ = 6.9° [P < .001], respectively), early stance (Δ = 5.8° [P = .003] and Δ = 6.7° [P < .001], respectively), and late stance (Δ = 7.9° [P < .001] and Δ = 8.0° [P < .001], respectively) compared with the CON group. During early stance, contralateral limbs of the PCL group displayed larger knee flexion moments (Δ = 0.20 N·m/kg; P = .014) compared with the CON group, and both reconstructed (Δ = 0.05 N·m/kg; P = .027) and contralateral (Δ = 0.07 N·m/kg; P = .001) limbs of the PCL group exhibited larger knee external rotation moments compared with the CON group. During late stance, reconstructed and contralateral limbs of the PCL group exhibited smaller knee extension moments (Δ = 0.24 N·m/kg [P < .001] and Δ = 0.26 N·m/kg [P < .001], respectively) and knee internal rotation moments (Δ = 0.06 N·m/kg [P < .001] and Δ = 0.06 N·m/kg [P < .001], respectively) compared with the CON group. No discrepancies were observed at the hip; minimal differences were noted in sagittal-plane ankle mechanics.
Conclusion:
Patients who underwent PCL reconstruction generally exhibited bilateral gait symmetry at 8 years after surgery. However, they exhibited important biomechanical deviations in both knees compared with healthy controls. These modifications likely reflect adaptive gait strategies to protect the PCL after reconstruction.
Clinical Relevance:
Long-term follow-up analyses of patients who underwent PCL reconstruction should not use the uninjured contralateral limb as a “healthy” reference, as it also exhibits mechanical differences compared with controls. Results could inform the development of neuromuscular and strength training programs targeting the restoration of knee biomechanics similar to healthy controls to prevent early-onset degeneration that is frequently associated with altered biomechanics.
The posterior cruciate ligament (PCL) is the main restraint to posterior tibial translation 36 and, with the structures of the posterolateral corner, plays a secondary role in limiting axial rotation.7,36 The PCL is understudied compared with its counterpart, the anterior cruciate ligament (ACL), likely because of its lower injury incidence: ACL injuries account for approximately 45% to 60% of all knee ligament injuries, while PCL injuries account for only approximately 4%. 3 Up to 95% of PCL tears occur in combination with other ligament tears, mainly structures of the posterolateral corner. 36 PCL deficiency has several ramifications, including increased knee laxity and altered mechanical loading. 7 PCL-deficient knees often exhibit higher contact forces in the medial compartment, a finding associated with a higher incidence of articular cartilage degeneration. 7
Reconstructive surgery is often indicated for combined PCL injuries. 52 Surgery aims to improve patient outcomes, counteract knee instability, and restore natural knee biomechanics, with the end goal of preventing long-term joint degeneration. 52 Patients have reported favorable long-term outcomes after PCL reconstruction, including high function and low symptom levels as well as a satisfactory return to daily activities.35,52 Conversely, initial improvements in posterior tibial translation tend to degrade over time. 19 Furthermore, long-term radiographic23,51 and semiquantitative magnetic resonance imaging–based 20 results have shown that many patients undergo degenerative changes after PCL reconstruction, irrespective of posterior tibial stability. This evidence suggests that PCL reconstruction may neither restore normal biomechanics nor prevent the development of abnormal biomechanics in the long term, or the extent of joint damage at the time of injury may have caused irreparable cartilage damage and ensuing degenerative changes, regardless of surgery. Nonetheless, little research has evaluated whether knee mechanics during everyday activities are restored after PCL reconstruction.23,32,47 Such work is warranted, as ample data suggest that ambulatory mechanics are implicated in the development of knee osteoarthritis.1,4,13
Few studies have assessed gait mechanics after PCL reconstruction.23,47 No side-to-side differences were noted in spatiotemporal, kinematic, or kinetic parameters of 10 patients at 3.3 years after PCL reconstruction. 47 Conversely, knees with multiple reconstructed ligaments (including the PCL and posterolateral corner in most cases) had smaller sagittal-plane range of motion than unmatched healthy control knees, as well as smaller external knee flexion moments compared with uninjured contralateral knees, at 3 years after surgery. 23 While insightful, previous studies had pitfalls that precluded a comprehensive understanding of long-term gait changes after PCL reconstruction. First, mechanics were analyzed only for the knee in the sagittal plane. Patients with reconstructed cruciate ligaments can exhibit altered movement patterns at the hip and ankle,12,38,43 and discrepancies can arise in the frontal and transverse planes.17,32,43 Second, reconstructed limbs were compared with uninjured contralateral limbs or limbs from unmatched controls; uninjured contralateral limbs of patients who underwent PCL reconstruction have not been compared with limbs from matched controls. While asymmetries can appear in the early stages after knee surgery, symmetrical gait is typically restored after several years.5,6,11,43,55 Yet, a comparison of the reconstructed and contralateral limbs of patients who underwent PCL reconstruction—to each other and to sex- and age-matched controls—is required for a systematic and robust evaluation of potential gait asymmetries in longitudinal studies. Lastly, previous work had follow-up times of <3.5 years after surgery. Longer follow-ups are needed to adequately characterize long-term adaptations after PCL reconstruction.
This study aimed to determine whether patients who underwent PCL reconstruction exhibited long-term alterations in lower limb joint kinematics and kinetics during self-paced level walking. It was hypothesized that no differences would be observed between the reconstructed and uninjured contralateral limbs of patients at a minimum of 2.5 years after PCL reconstruction. It was also hypothesized that patients who underwent PCL reconstruction would display biomechanical alterations in all 3 lower extremity joints and planes of motion compared with a healthy control group.
Methods
This cross-sectional analysis was performed on a subset of data from a larger cohort study. Previous publications have used data from the same patients included in the current study.10,19-21 This study was approved by our institution’s research ethics board (EA2/055/10). Participants provided written informed consent before their involvement in the study.
Participants
The larger cohort consisted of 66 patients who had previously undergone PCL reconstruction at our institution’s orthopaedic clinic. Of these 66 patients, 49 underwent gait analyses between 2012 and 2013. For the current analysis, inclusion criteria were the following: 20-60 years of age at the time of recruitment and having undergone primary unilateral reconstructive surgery for a PCL tear (isolated or combined with other ligament tears) using the anterolateral bundle technique 25 at least 2 years before study enrollment. Exclusion criteria were the following: PCL revision surgery, use of a different surgical technique (eg, double-bundle), bilateral knee involvement at the time of PCL injury, previous injury/surgery to either lower limb, known ipsilateral (hip, ankle) or contralateral (hip, knee, ankle) musculoskeletal conditions (eg, femoroacetabular impingement, tendinopathy, osteoarthritis), body mass index (BMI) ≥35, and unavailable gait data (ie, poor data quality, no healthy control match). Ultimately, data were analyzed for 26 patients (Figure 1), for whom the mechanisms of knee injuries were as follows: sporting activities (n = 9), motor vehicle accidents (n = 11), and activities of daily living (n = 6).
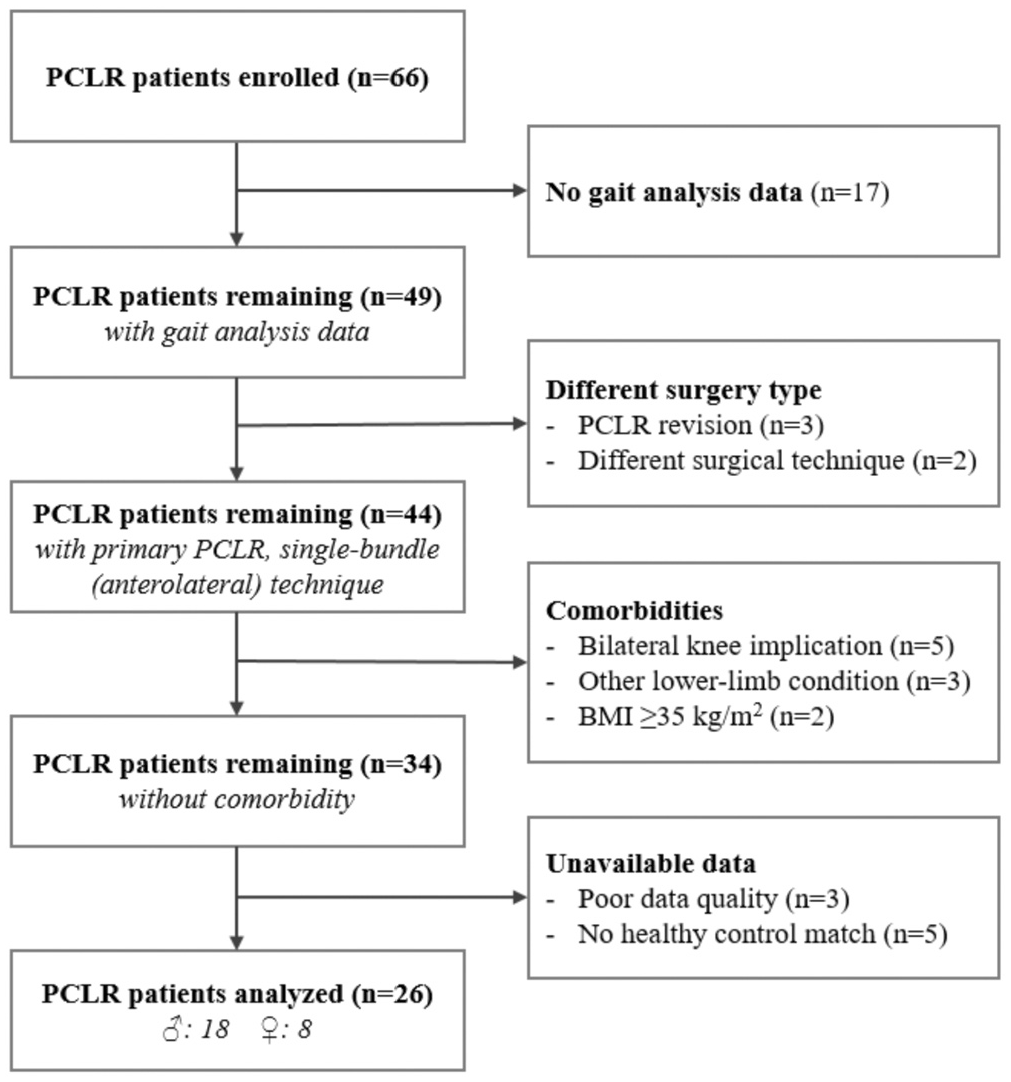
Flowchart describing the inclusion of patients who had undergone posterior cruciate ligament (PCL) reconstruction. A total of 66 patients were enrolled. Patients were excluded for the following reasons: no gait analysis data, different surgery type, comorbidities, and unavailable data. The final analysis included data from 26 patients.
In addition, a control group was created for comparison using participants who underwent the same experimental protocol. The control group, which was recruited from the university campus and local community, consisted of sex- and age-matched (to within 5 years) participants with no previous lower limb injury/surgery and no known lower extremity conditions.
At the time of study enrollment, demographic characteristics were recorded, including sex, age, height, weight, and BMI. Patients who underwent PCL reconstruction also completed the International Knee Documentation Committee (IKDC) subjective knee form, 24 a measure of knee status with respect to symptoms, function, and sports activities. Scores from the individual items are summed and transformed to a scale that ranges from 0 to 100, with higher scores representing fewer symptoms and higher levels of function. In addition, static laxity was evaluated in both knees. Posterior tibial translation was assessed using conventional stress radiographs at 90° of knee flexion. With the patient lying on the side, a posteriorly directed force of 150 N was applied to the tibial tuberosity using a stress device (GA II stress device; Telos). 26 The absolute posterior tibial translation for the reconstructed knee and the side-to-side difference in posterior tibial translation were determined. Moreover, posterolateral knee laxity was assessed using the dial test at 30° and 90° of knee flexion. With the patient in a prone position, a maximal external rotation force was applied to the lower leg by the clinician, and the foot-thigh angle (ie, external tibial rotation) was measured with a goniometer 27 ; side-to-side differences were determined.
Surgical Technique and Postoperative Care
All patients underwent unilateral primary reconstruction for a PCL tear that was either isolated (n = 3) or combined with other structures: PCL + posterolateral corner (n = 15), PCL + ACL (n = 3), and PCL + ACL + posterolateral corner (n = 5). The mean time between the PCL injury and reconstruction was 3.1 ± 5.3 years. All surgical procedures were performed by the same orthopaedic surgeon using the same protocol. 25 Arthroscopically assisted single-bundle (anterolateral) PCL reconstruction was performed using the conventional tibial tunnel technique and femoral single-incision technique with biodegradable interference fit fixation. Hybrid fixation with suture backup was used at the tibial site. A maximum manual pretension was applied at approximately 60° to 80° of knee flexion. The primary graft choice was a 5-strand semitendinosus and gracilis tendon autograft from the ipsilateral knee. Posterolateral corner stabilization was performed with the modified Larson technique via 2 miniature incisions using the contralateral semitendinosus tendon. 31 In select cases (eg, refusal of contralateral graft harvest), and depending on availability, a fresh-frozen allograft obtained from our medical center’s tissue bank was used (n = 6). If required, ACL reconstruction was performed using an anatomic single-bundle technique with the femoral tunnel drilled via the anteromedial portal as well as biodegradable interference screw fixation of a 4-fold contralateral gracilis tendon autograft or allograft.
Standard postoperative care, structured around the stages of tissue healing, was prescribed. For the first 8 to 10 weeks, the aim of postoperative management was to reduce swelling and effusion and increase knee range of motion. During this time, the knee was immobilized in a straight posterior tibial support splint (Medi) for 6 weeks, allowing gradual passive mobilization into flexion with the patient in a prone position. Crutches were used, as tolerated, for 6 weeks. Toe-touch ambulation (maximum of 15 kg) was recommended for the initial weeks, with a gradual increase in weightbearing over time according to symptom severity. Mobilization of the knee beyond 90° of flexion was permitted after the sixth week. As of the tenth week, patients could progress to quadriceps strengthening exercise; active hamstring contractions were prohibited for 16 weeks.
Biomechanical Assessment
For the PCL reconstruction patients, gait analyses were performed at 8.2 ± 2.6 years (mean ± SD) after PCL reconstruction to assess lower extremity joint biomechanics. Participants wore skin-tight shorts and a t-shirt. Overall, 52 retroreflective markers (6 on the pelvis, 9 per thigh, 10 per shank, and 4 per foot) were affixed onto the lower extremities of participants according to a standardized protocol. 45 Three-dimensional marker trajectories were recorded at 120 Hz with 10 infrared cameras (T20S; Vicon). Ground-reaction forces were recorded synchronously at 960 Hz with 2 side-by-side floor-embedded force plates (BP400600; AMTI) that were not visible to the participants (Appendix Figure A1).
A static reference trial, with the participant standing in the anatomic position, was recorded to determine segment lengths and joint centers. After practicing walking in the laboratory, participants executed barefoot walking trials at a natural self-selected speed over a 10-m walkway. Data collection continued until 3 successful trials, during which each foot landed fully on distinct force plates, were captured.
Gait data were processed and analyzed using commercial software (Visual 3D; C-Motion). Participant-specific link-segment models were created based on marker data from the static trial. A second-order low-pass Butterworth bidirectional filter with a 6-Hz cut-off was applied to marker and force plate data. 40 Using marker-based kinematic reconstruction, lower extremity joint angles were calculated for the sagittal, frontal, and transverse planes in a 3-dimensional floating axis coordinate system. 54 External lower extremity joint moments were determined in the same coordinate system using inverse dynamics. 53
For each trial, time-normalized waveforms were generated for hip, knee, and ankle angles as well as external moments during the stance phase of gait (ie, heel strike to toe-off). Joint angles were expressed in degrees; joint moments were expressed as normalized to body weight (N·m/kg). The outcome measurements of interest were the angle and moment values for the hip, knee, and ankle joints in each of the 3 planes of motion at initial contact (angles only); the peak values near the time of the maximum knee flexion angle/moment during the first half of the stance phase (“early stance”); and the peak values near the time of the minimum knee flexion angle/moment during the second half of the stance phase (“late stance”). To eliminate ambiguity in selecting peak values, the local maximum or minimum values nearest to 25% and 75% of the stance phase were extracted. Sagittal-plane excursions during early stance and late stance were also analyzed. Furthermore, spatiotemporal parameters were computed, including step length, stride length, step time, stride time, stance time, swing time, gait speed, and cadence. All measurements were obtained for 3 gait trials and then averaged. These outcome variables have demonstrated acceptable measurement error. 15
For patients who underwent PCL reconstruction (PCL group), data from the reconstructed and uninjured contralateral limbs were analyzed separately; for healthy control participants (CON group), data from the left and right limbs were averaged to eliminate the effects of limb dominancy and contralateral differences and yield a single set of representative measurements.
Statistical Analysis
Descriptive statistics for the PCL and CON groups were computed as means ± SDs for continuous data and counts for categorical data and were compared using a 2-tailed independent t test. Data for reconstructed and contralateral limbs of the PCL group were compared using a 2-tailed paired-samples t test. Data for reconstructed and contralateral limbs of the PCL group were compared with the CON group using 1-way analysis of variance and the post hoc Tukey test when significant. A statistical significance threshold of α = 0.05 was used for all tests. To characterize the magnitude of statistically significant differences, standardized effect sizes were determined using the Cohen d (mean difference between groups / pooled SD). Effect sizes of 0.2-0.49, 0.5-0.79, and ≥0.8 indicated small, moderate, and large effects, respectively. 9
To ensure the appropriateness of statistical analyses, requisite assumptions for the t test and analysis of variance were verified. Specifically, normality was confirmed using histograms and the Shapiro-Wilk test, while the homogeneity of variance was confirmed using the Breusch-Pagan test. In a few instances, data were determined to be heteroscedastic; therefore, robust error estimates were used. Data were also scrutinized for outliers using box plots. Ultimately, all observations were deemed physiologically plausible and thus were retained for analysis. All analyses were conducted using Stata (Version 13.1; StataCorp).
Results
The PCL and CON groups were not different in terms of sex, age, and height; however, the PCL group had a greater body mass and BMI (Table 1). On average, the PCL group had an IKDC score of 74.1 ± 16.2 points. Static knee laxity measurements for the PCL group were as follows: absolute posterior tibial translation for the reconstructed knee of 8.0 ± 3.5 mm; side-to-side difference in posterior tibial translation of 4.7 ± 4.4 mm (mean ± SD); and side-to-side difference in external tibial rotation (dial test) of ≤5° (n = 14), 6°-10° (n = 11), and 11°-19° (n = 1) at 30° of knee flexion and of ≤5° (n = 12), 6°-10° (n = 12), and 11°-19° (n = 2) at 90° of knee flexion.
Demographic Data of Participants a
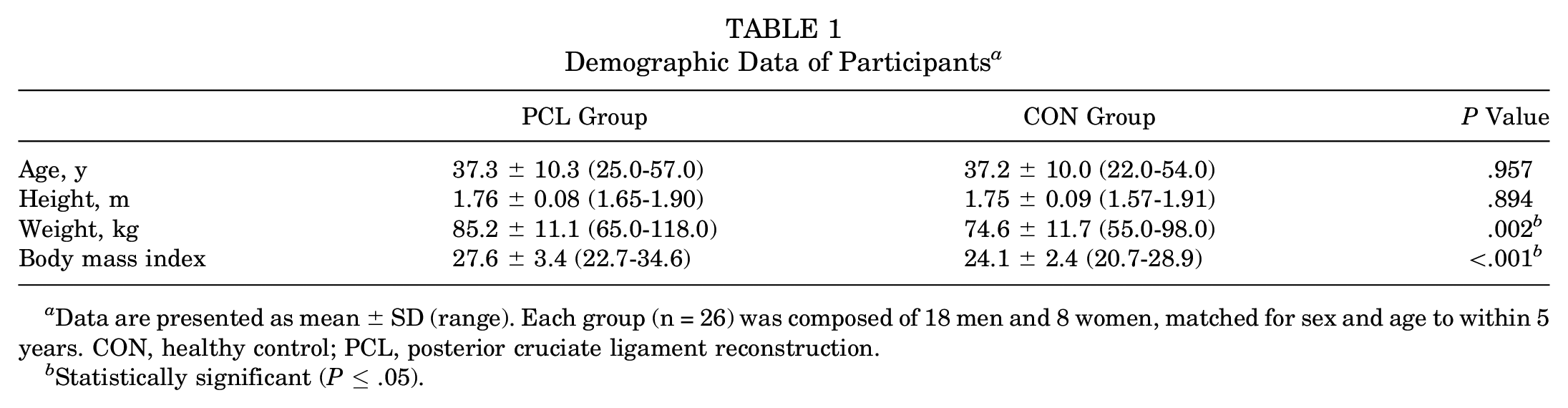
Data are presented as mean ± SD (range). Each group (n = 26) was composed of 18 men and 8 women, matched for sex and age to within 5 years. CON, healthy control; PCL, posterior cruciate ligament reconstruction.
Statistically significant (P≤ .05).
Overall, no differences were noted between reconstructed and contralateral limbs of the PCL group as well as the CON group with respect to spatiotemporal parameters (Table 2).
Spatiotemporal Results During Gait at a Self-Selected Speed a
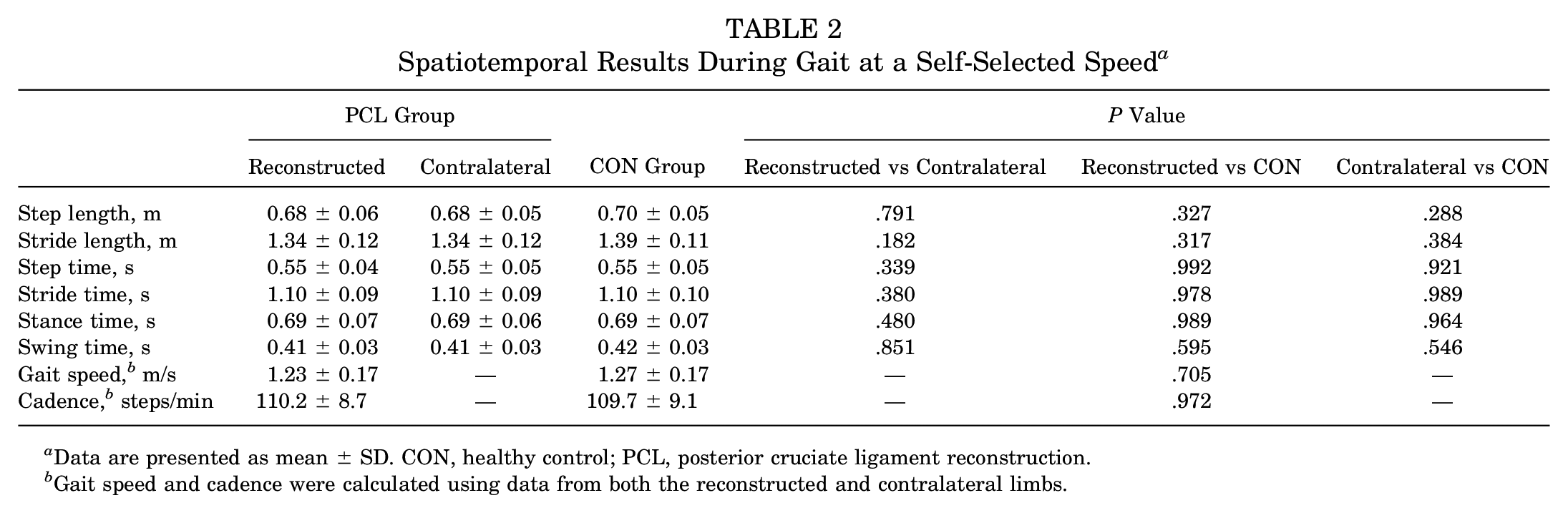
Data are presented as mean ± SD. CON, healthy control; PCL, posterior cruciate ligament reconstruction.
Gait speed and cadence were calculated using data from both the reconstructed and contralateral limbs.
Regarding joint kinematics, no differences were observed between reconstructed and contralateral limbs of the PCL group for any parameter (P > .05). Reconstructed and contralateral limbs of the PCL group exhibited larger knee flexion angles during initial contact (Δ = 7.0° [P < .001; d = 1.49] and Δ = 6.9° [P < .001; d = 1.41], respectively), early stance (Δ = 5.8° [P = .003; d = 0.96] and Δ = 6.7° [P < .001; d = 1.08], respectively), and late stance (Δ = 7.9° [P < .001; d = 1.58] and Δ = 8.0° [P < .001; d = 1.59], respectively) compared with the CON group (Table 3 and Figure 2). Contralateral limbs of the PCL group displayed larger ankle dorsiflexion angles at initial contact compared with the CON group (Δ = 3.0°; P = .026; d = 0.77). In addition, reconstructed (Δ = 1.7°; P = .009; d = 0.85) and contralateral (Δ = 1.9°; P = .004; d = 0.93) limbs of the PCL group had smaller sagittal-plane ankle excursions during early stance compared with the CON group. No between-group differences were observed for hip angles (P > .05). Hip and ankle angles are provided in Appendix Table A1.
Knee Angles (in Degrees) During Initial Contact, Early Stance, and Late Stance a
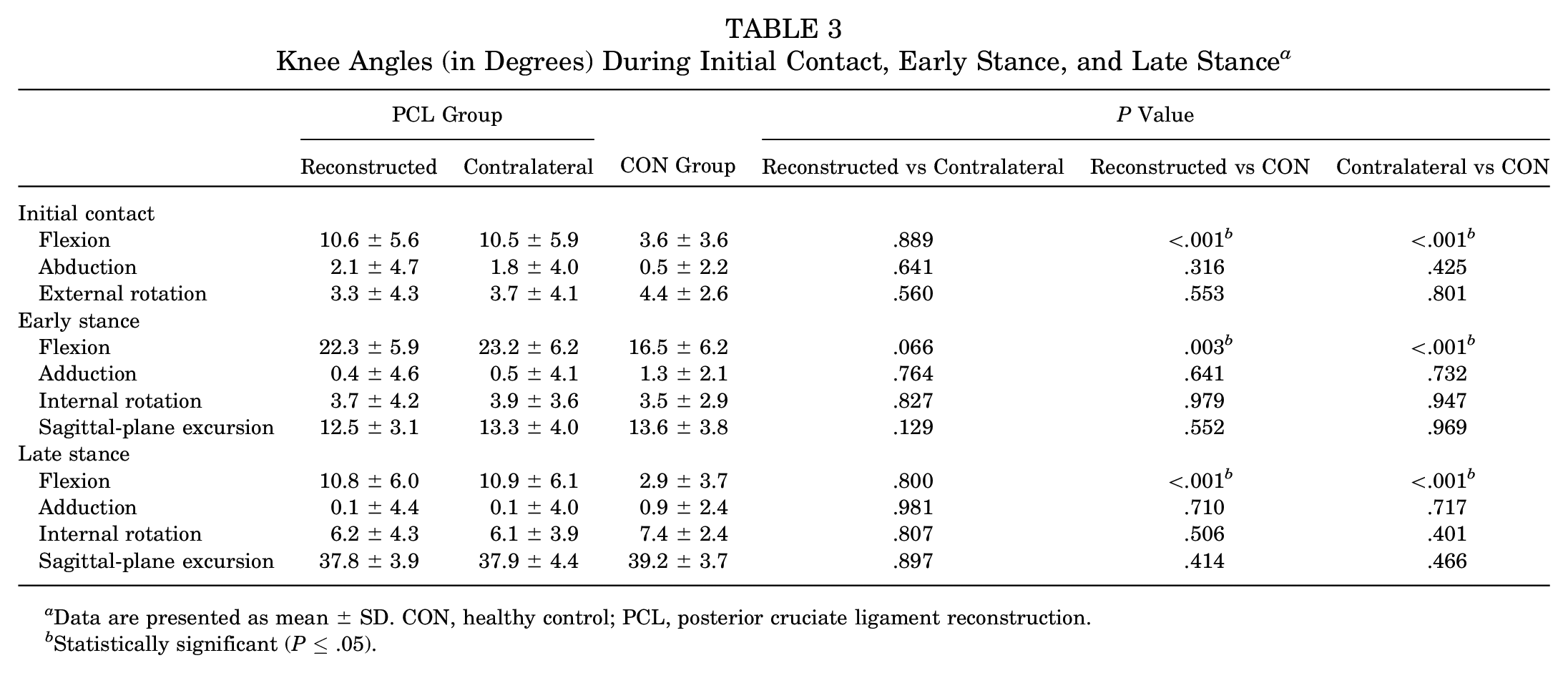
Data are presented as mean ± SD. CON, healthy control; PCL, posterior cruciate ligament reconstruction.
Statistically significant (P≤ .05).
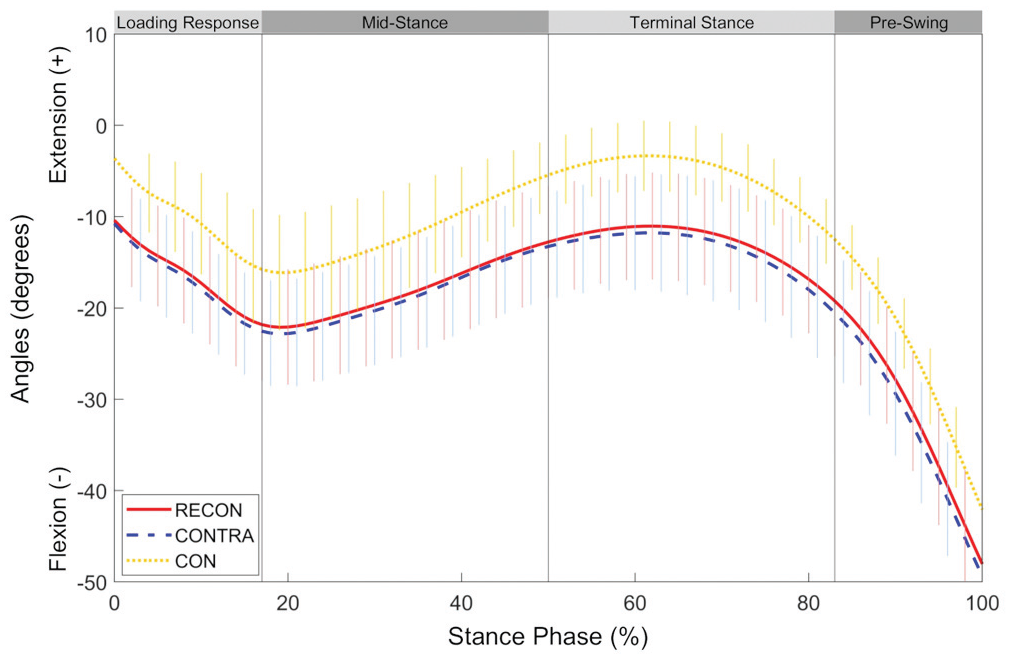
Ensemble mean (±SD) curves for knee flexion-extension angles during the stance phase of gait for the reconstructed (RECON) and uninjured contralateral (CONTRA) limbs of the posterior cruciate ligament (PCL) group as well as the average of left and right limbs of the control group (CON).
Concerning joint kinetics, some side-to-side differences were noted in the PCL group: reconstructed limbs exhibited smaller peak knee flexion moments (Δ = 0.05 N·m/kg; P = .047; d = 0.21) and smaller peak knee external rotation moments (Δ = 0.02 N·m/kg; P = .035; d = 0.29) during early stance (Table 4) as well as smaller peak hip extension moments (Δ = 0.05 N·m/kg; P = .008; d = 0.23) during late stance (Appendix Table A2) compared with contralateral limbs. No side-to-side differences were seen for ankle moments (P > .05). Several kinetic differences were observed between the PCL and CON groups. During early stance, contralateral limbs of the PCL group displayed larger peak knee flexion moments compared with the CON group (Δ = 0.20 N·m/kg; P = .014; d = 0.75), and both reconstructed (Δ = 0.05 N·m/kg; P = .027; d = 0.82) and contralateral (Δ = 0.07 N·m/kg; P = .001; d = 1.15) limbs of the PCL group exhibited larger peak knee external rotation moments compared with the CON group. During late stance, reconstructed and contralateral limbs of the PCL group exhibited smaller peak knee extension moments (Δ = 0.24 N·m/kg [P < .001; d = 1.82] and Δ = 0.26 N·m/kg [P < .001; d = 1.98], respectively) (Figure 3) and smaller peak knee internal rotation moments (Δ = 0.06 N·m/kg [P < .001; d = 1.50] and Δ = 0.06 N·m/kg [P < .001; d = 1.50], respectively) (Figure 4) compared with the CON group. Furthermore, reconstructed limbs of the PCL group displayed smaller peak ankle dorsiflexion moments during late stance compared with the CON group (Δ = 0.10 N·m/kg; P = .022; d = 0.78). No differences in hip moments were observed between the PCL and CON groups (P > .05). Hip and ankle moments are provided in Appendix Table A2.
Knee Moments (in N·m/kg) During Early Stance and Late Stance a
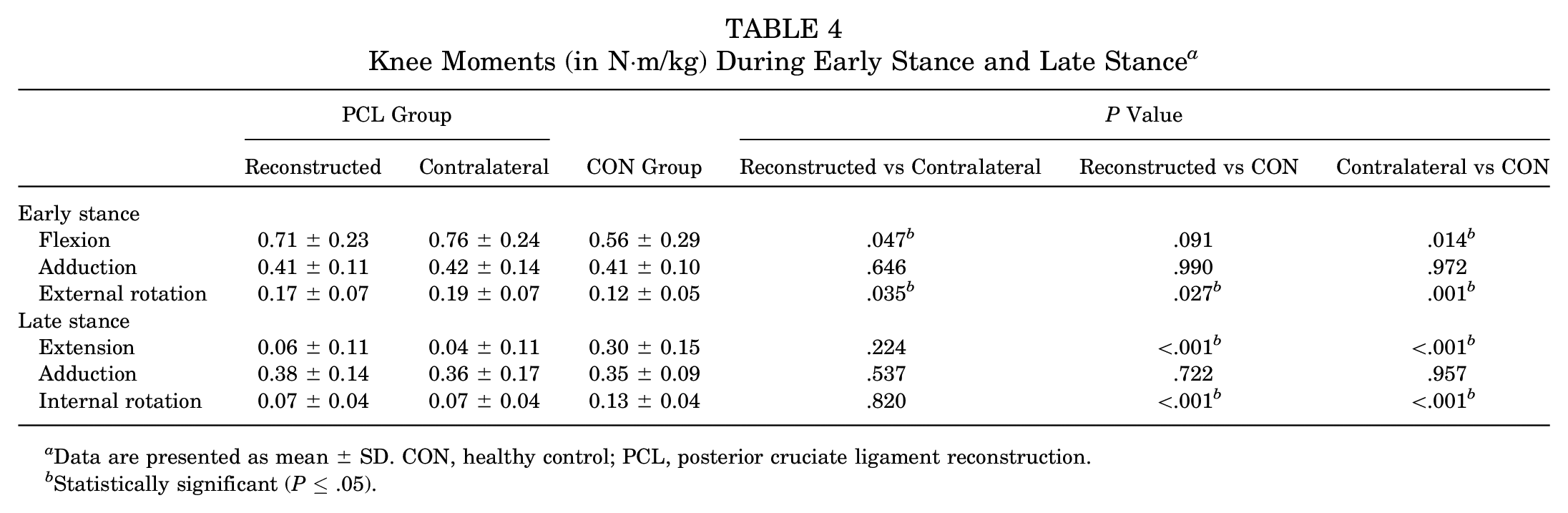
Data are presented as mean ± SD. CON, healthy control; PCL, posterior cruciate ligament reconstruction.
Statistically significant (P≤ .05).
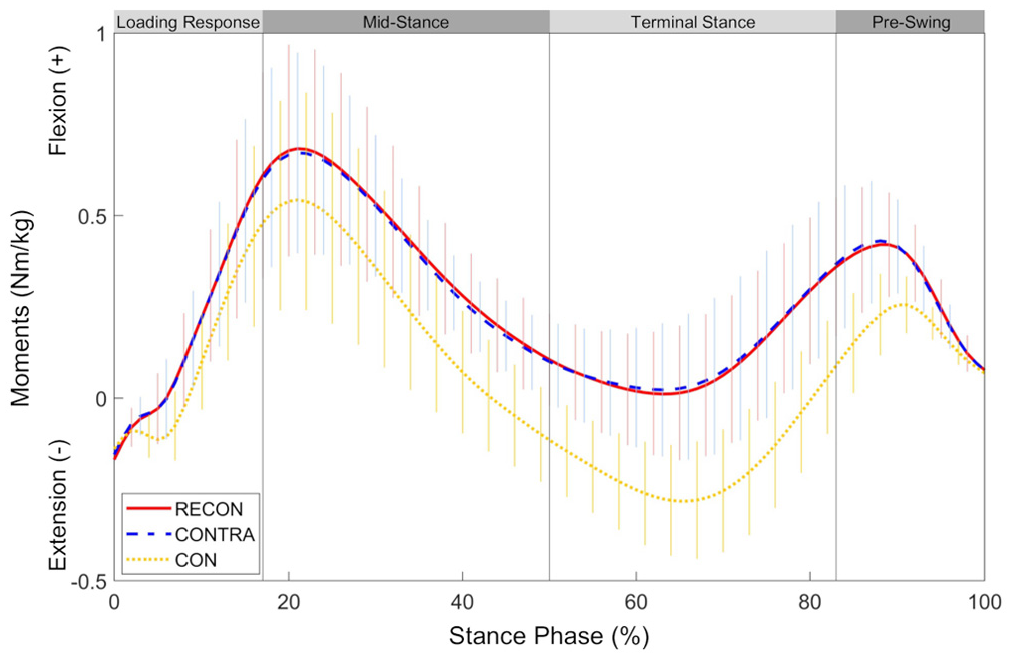
Ensemble mean (±SD) curves for external knee flexion-extension moments during the stance phase of gait for the reconstructed (RECON) and uninjured contralateral (CONTRA) limbs of the posterior cruciate ligament (PCL) group as well as the average of left and right limbs of the control group (CON).
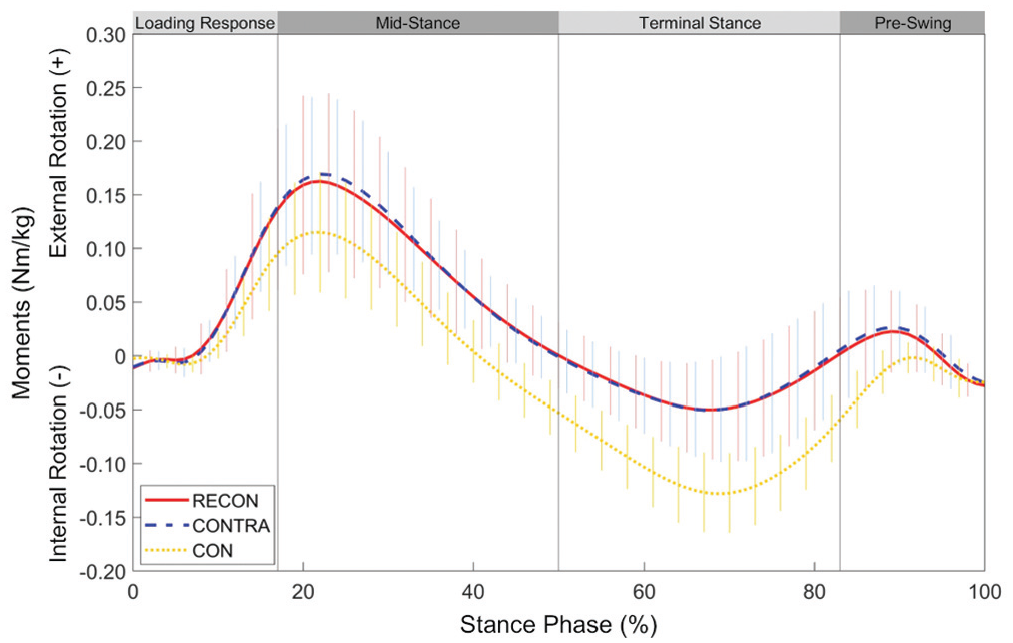
Ensemble mean (±SD) curves for external knee external-internal rotation moments during the stance phase of gait for the reconstructed (RECON) and uninjured contralateral (CONTRA) limbs of the posterior cruciate ligament (PCL) group as well as the average of left and right limbs of the control group (CON).
Discussion
This work provides novel data with regard to the long-term consequences of unilateral reconstruction of isolated and combined PCL injuries on gait mechanics. No side-to-side differences were noted between reconstructed and contralateral limbs of the PCL group for any of the spatiotemporal or kinematic parameters; trivial differences were observed for knee and hip moments. Overall, bilateral gait symmetry seemed to be established after PCL reconstruction. Furthermore, important differences in knee mechanics were noted between the PCL and CON groups: compared with the CON group, both knees of the PCL group exhibited altered mechanics in the sagittal and transverse planes. In contrast, no between-group discrepancies were noted at the hip; some were noted at the ankle in the sagittal plane, but these were deemed of secondary importance. These findings suggest that patients who have undergone PCL reconstruction develop long-term biomechanical adaptations that are similar in both the reconstructed and uninjured contralateral knees, with minor (and potentially trivial) alterations at other lower extremity joints. These modifications likely reflect adaptive strategies to protect the PCL during ambulation. Nonetheless, longitudinal studies are required to confirm the effect of surgery on restoring normal gait biomechanics or preventing the development of abnormal biomechanics over time.
The current work found no side-to-side differences in the PCL group for any of the spatiotemporal or kinematic parameters. The finding of a lack of differences between limbs in the PCL group align with those from previous investigations of self-paced walking in patients at 4 years after untreated unilateral isolated PCL injuries 17 as well as in patients approximately 3 years after unilateral isolated PCL or multiple knee ligament reconstruction.23,47 Conversely, some side-to-side kinetic differences were observed. Notably, reconstructed limbs of the PCL group displayed smaller peak knee flexion moments during early stance compared with contralateral limbs, corroborating findings previously reported in patients at 3 years after unilateral multiple knee ligament reconstruction. 23 While the aforementioned study observed a 19% side-to-side difference in peak knee flexion moments, the present analysis noted only a 7% difference. This discrepancy is likely explained by the heterogeneity of the injured structures between samples: in the study by Hart et al, 23 only 80% of patients underwent PCL reconstruction, and most (20/25) also had ACL involvement; in the current study, 100% of patients underwent PCL reconstruction, and only about a third (8/26) also had ACL involvement. Moreover, in the current analysis, reconstructed limbs of the PCL group displayed smaller peak knee external rotation moments during early stance, likely attributable to the smaller knee flexion moments, as well as smaller peak hip extension moments during late stance compared with contralateral limbs. However, it should be noted that these discrepancies, which ranged between 0.02 and 0.05 N·m/kg with small effect sizes (d < 0.30), were likely trivial. Overall, it seems that symmetrical gait was achieved in the long term after PCL reconstruction. These results are in agreement with evidence showing that patients who undergo surgical treatment for unilateral musculoskeletal knee conditions (eg, ACL reconstruction, total knee arthroplasty) tend to re-establish a relatively symmetrical gait over time.5,6,43,55 Whether symmetrical gait represents a successful outcome remains unclear. Restored symmetry may reflect improved symptoms and functional recovery after cruciate ligament reconstruction. 33 However, despite the attainment of bilateral symmetry, both knees in the PCL group displayed important mechanical deviations compared with the CON group, suggesting adaptations in the uninjured contralateral limb to resemble more closely the aberrant biomechanics of the PCL-reconstructed limb. Deviations from normal joint biomechanics could disrupt tissue homeostasis, promoting degenerative changes 2 ; however, such conclusions are beyond the scope of the current analysis.
Both reconstructed and contralateral limbs of the PCL group exhibited important kinematic and kinetic deviations at the knee compared with the CON group; these differences occurred mainly in the sagittal plane. Deviations from healthy controls in sagittal-plane angles and moments have been noted previously in knees that have undergone ACL or multiple ligament reconstruction,23,43 with the variability likely reflective of the affected joint structures. In the current study, both reconstructed and contralateral limbs of the PCL group exhibited larger knee flexion angles during initial contact, early stance, and late stance compared with the CON group. While the PCL and CON groups had the same sagittal-plane knee excursions, the PCL group sustained greater knee flexion throughout stance, a feature reflected by the results of the discrete data analysis and illustrated in Figure 2. In addition, contralateral limbs of the PCL group displayed larger peak knee flexion moments during early stance compared with the CON group; reconstructed limbs of the PCL group did not (P = .091) likely because of the small abovementioned side-to-side difference for this parameter. Also, both reconstructed and contralateral limbs of the PCL group had smaller peak knee extension moments during late stance compared with the CON group. Together, these data indicate that the PCL group generally sustained greater knee flexion moments throughout the stance phase (as illustrated in Figure 3). Interestingly, previous reports have coined the term “knee extensor dominant gait” to denote walking with sustained larger knee flexion angles and larger external knee flexion moments.29,42 An external knee flexion moment is balanced by an equal but opposite net internal extension moment and indicates that the sagittal-plane moment is dominated by the quadriceps. Accordingly, one possible explanation for the larger knee flexion moments in the PCL group could be a greater quadriceps effort (or less hamstring effort) throughout stance 29 ; however, electromyography and/or muscle strength data are required to confirm this notion. Alternatively, these findings may reflect an ingrained kinematic strategy learned over several years after injury/surgery. As kinetic parameters are directly associated with measured kinematics, greater knee flexion moments may simply be the consequence of greater knee flexion angles. 37 These biomechanical alterations may represent an adaptive strategy to reduce hamstring-induced stress on the PCL and secondary restraints to posterior tibial translation. Conversely, higher knee flexion angles and moments persisting longitudinally after PCL reconstruction may represent important parameters involved in the development of knee osteoarthritis,8,13,14,22,46 although future work is required to confirm this speculation. A comparison to healthy age- and sex-matched controls should be considered the gold standard for the evaluation of gait mechanics after a surgical intervention, as we have shown that there are significant differences between patients who have undergone PCL reconstruction and healthy controls that remain undetected when only the uninjured contralateral limb is used for comparison.
The current study also noted discrepancies in transverse-plane knee moments. Both reconstructed and contralateral limbs of the PCL group displayed larger peak knee external rotation moments during early stance and smaller peak knee internal rotation moments during late stance compared with the CON group. These findings align with those from ACL-reconstructed knees, which displayed altered rotational moments compared with the knees of healthy controls. 43 As depicted in Figure 4 and supported by the results of the discrete peak analysis, the PCL group generally sustained higher knee external rotation moments throughout the stance phase. Such alterations in knee rotational moments can be partly attributed to modified knee flexion-extension angles and moments. For instance, it has been proposed that patients with PCL and posterolateral instability walk with more knee flexion to avoid terminal extension, which would accentuate external tibial rotation through the screw-home mechanism and increase stress on the compromised joint structures.16,47 Avoidance of terminal extension would result in smaller internal rotation moments (balanced by external rotator muscles) required for external tibial rotation.
No discrepancies were noted in frontal-plane knee biomechanics in the PCL group. This finding was unexpected, as results from in vitro studies showed that PCL-sectioned knees (with and without sectioning of other ligaments) exhibited increased varus instability as well as increased joint contact force in the medial compartment, 7 features typically attributed to alterations in frontal-plane knee biomechanics. 49 In addition, ACL-reconstructed knees have shown altered mechanics (ie, knee adduction angles and external knee adduction moments) after surgery. 43 Nonetheless, our findings are in agreement with clinical studies, which have demonstrated no significant knee abduction-adduction instability with PCL deficiency. 7 Discrepancies in study findings are likely caused by several factors. For example, cadaveric studies cannot replicate the neuromuscular contribution to joint stability that occurs in in vivo conditions, and mechanical alterations exhibited by patients who have undergone ACL reconstruction may represent adaptive strategies unique to the specific joint structures involved.
Seemingly, PCL reconstruction had very little long-term effects on gait mechanics at lower extremity joints other than the knee; some exceptions occurred at the ankle, which were deemed of secondary importance. Both reconstructed and contralateral limbs of the PCL group had smaller sagittal-plane ankle excursions during early stance, which were likely caused by the larger knee flexion angles that occurred simultaneously. In addition, contralateral limbs of the PCL group displayed larger ankle dorsiflexion angles at initial contact compared with the CON group, whereas reconstructed limbs of the PCL group exhibited smaller peak ankle dorsiflexion moments during late stance compared with the CON group. An in-depth interpretation of these unilateral differences is challenging; however, these were probably influenced by the major biomechanical differences at the knee and/or minor variations across all joints of the kinetic chain.
Between-group differences in knee mechanics observed in the current study are likely not caused by dissimilarities in demographics or spatiotemporal parameters. The PCL and CON groups were not different in terms of sex, age, and height; however, the PCL group was heavier. In this analysis, body weight was intentionally not controlled for: an increase in body weight is a typical occurrence in patients who have undergone knee surgery 39 and represents an important feature of such musculoskeletal conditions. In the current study, the CON group was of “normal weight” (BMI = 24.1 ± 2.4), while the PCL group was “overweight” (BMI = 27.6 ± 3.4). While obese patients (BMI >30) typically exhibit altered knee mechanics during gait compared with normal weight patients, such differences have not been observed between normal weight and overweight persons. 41 Nonetheless, because body weight directly influences gait mechanics, future work should confirm this speculation by comparing groups that are also matched for weight. Furthermore, knee angles and moments during gait can be affected by spatiotemporal parameters (eg, gait speed, stride length)18,34; yet, these characteristics were not different between groups. In contrast, alterations in sagittal- and transverse-plane knee mechanics observed in the PCL group may be the result of altered knee muscle function partly due to the surgical procedure itself. The semitendinosus and gracilis tendons were the main tissues harvested for joint reconstruction. Both the semitendinosus and gracilis muscles contribute to knee flexion and internal rotation of the leg.28,50 Accordingly, harvesting these tendons could disrupt tissue integrity and natural joint function. 48 Yet, it is doubtful that long-term alterations in knee mechanics were caused by muscle weakness due to tendon harvesting, as tendon regrowth and the recovery of functional biomechanical properties are mainly restored with time (>2 years after surgery). 44
This study had some limitations. First, because of the nature of the injuries, most patients underwent operative treatment not only for the PCL but also for other implicated joint structures (eg, posterolateral corner, ACL). This resulted in a more heterogeneous group and restricted the inferences that could be made regarding the effects of surgery on gait mechanics. Second, patients were not assessed for evidence of degenerative joint changes, a common occurrence after PCL reconstruction that could influence lower limb joint biomechanics. 30 Third, specific details about patient rehabilitation, including exercise prescription and compliance, were unknown. Thus, the potential effects of rehabilitation and knee muscle strengthening on recovery and gait outcomes could not be elucidated. Fourth, neither electromyography nor muscle strength measurements were acquired; therefore, it could not be ascertained whether gait differences in patients who underwent PCL reconstruction resulted from altered muscle activation or muscle weakness. Fifth, multiplicity may have inflated the type I error rate. Finally, results from this study can only be generalized to patients who have undergone primary unilateral PCL reconstruction using the anterolateral bundle technique.
In conclusion, patients with unilateral isolated or mixed injuries exhibited symmetrical gait at 8 years after PCL reconstruction; however, bilateral mechanical alterations were observed in comparison to gait in healthy controls. These gait modifications, predominantly in the sagittal and transverse planes at the knee, likely reflect adaptive strategies to protect the PCL.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211017147 – Supplemental material for Gait Adaptations at 8 Years After Reconstruction of Unilateral Isolated and Combined Posterior Cruciate Ligament Injuries
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211017147 for Gait Adaptations at 8 Years After Reconstruction of Unilateral Isolated and Combined Posterior Cruciate Ligament Injuries by Nicholas M. Brisson, Alison N. Agres, Tobias M. Jung and Georg N. Duda in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Leonie Krahl, Yanlin Zhong, Julia Ohde, and Teresa Benert for their assistance in data collection and processing as well as the study participants for making this study possible.
Submitted March 5, 2020; accepted February 1, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was directly funded by the German Research Foundation (DFG; DU 298/25-1) and the German Federal Ministry of Education and Research (BMBF; OVERLOAD-PrevOP, 01 EC1408A). T.J. has received education support from Smith & Nephew, Richard Wolf, and DJO Global. G.N.D. has received consultancy fees from Pluristem Therapeutics, DePuy Synthes, ImplanTec, Implantcast, and Stryker; has received grants or grants pending from Pluristem Therapeutics, DePuy Synthes, ImplanTec, Implantcast, Smith & Nephew, Stryker, and Zimmer; and has patents (planned, pending, or issued) with Pluristem Therapeutics and B&C for work unrelated to this particular study. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.