
Abstract
Background:
Previous studies evaluating the outcomes of hip arthroscopy for patients with global acetabular overcoverage and focal superolateral acetabular overcoverage suffer from short-term follow-up and inconsistent radiographic criteria when defining these subpopulations of patients with femoroacetabular impingement syndrome (FAIS).
Purpose:
To evaluate the intermediate-term postoperative outcomes for patients with FAIS in the setting of global acetabular overcoverage, lateral acetabular overcoverage, and normal acetabular coverage.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients undergoing hip arthroscopy for FAIS were enrolled in a prospective cohort study, and those with a minimum follow-up of 5 years were included in this analysis. Patients were grouped based on type of acetabular coverage: global overcoverage (lateral center-edge angle [LCEA] ≥40°, with coxa profunda), lateral overcoverage (LCEA ≥40°, without coxa profunda), and no overcoverage (LCEA <40°). Functional outcomes (modified Harris Hip Score and Nonarthritic Hip Score) and failure of primary hip arthroscopy were compared between groups.
Results:
In total, 94 patients (mean age, 41.9 ± 14.2 years) were included with a mean follow-up duration of 6.1 ± 0.9 years. Of these patients, 40.4% had no acetabular overcoverage, 36.2% had lateral overcoverage, and 23.4% had global overcoverage. There was no difference between groups with respect to percentage of patients who underwent reoperation for either revision arthroscopy or conversion to total hip arthroplasty (28.9% for the normal acetabular coverage group, 29.4% for the lateral overcoverage group, and 31.8% for the global overcoverage group; P = .971). Among patients for whom primary hip arthroscopy did not fail, there was no difference in 5-year functional outcomes between groups. Postoperative LCEA >40° (β = −13.3; 95% CI, –24.1 to −2.6; P = .016), female sex (β = −14.5; 95% CI, –22.7 to −6.2; P = .001), and higher body mass index (β = −1.9; 95% CI, –2.8 to −1.0; P < .001) were associated with worse intermediate-term hip function in terms of modified Harris Hip Score.
Conclusion:
There was no difference in functional outcomes or rate of reoperation at a minimum of 5 years postoperatively between those with global acetabular overcoverage, those with regional lateral overcoverage, and those with normal acetabular coverage. Provided that an appropriate acetabuloplasty is performed, there is no evidence to suggest that global acetabular overcoverage portends a worse prognosis than other FAIS subtypes.
Keywords
Femoroacetabular impingement syndrome (FAIS) is the pathological articulation of an abnormally aspherical femoral head and/or an overhanging acetabulum resulting in pain and additional symptoms with hip range of motion. 26 A variety of intra- and extra-articular bony and soft tissue lesions have been associated with FAIS, including, but not limited to, subspine overgrowth, chondral delamination, labrum pathology, and capsular changes ultimately leading to degenerative joint disease and hip osteoarthritis if left unaddressed over the long term. ‡ Hip arthroscopy has become the mainstay of operative FAIS management with overall favorable outcomes in terms of patient-reported functional status, revision procedure rates, and conversion to total hip arthroplasty (THA). Recent studies have described some of the radiographic and intraoperative factors that are associated with varying levels of postoperative functional outcomes across the spectrum of FAIS.2,11,26,29-31,33,34
The presence of excessive acetabular overcoverage of the femoral head in the setting of FAIS has historically been associated with inferior outcomes after hip arthroscopy, previously requiring open surgical hip dislocation to properly address the pathology. 16 More recently, the use of improved arthroscopic techniques has been shown to yield acceptable clinical results without the morbidity associated with open surgical dislocation.9,10,22,25 However, the conclusions that can be drawn from existing studies are limited by the heterogeneous radiographic criteria that have been used to define this subpopulation of patients with FAIS. Although some analyses have diagnosed acetabular overcoverage based on an increased lateral center-edge angle (LCEA) >35° or >40° regardless of other morphologic features, others require additional criteria of concomitant coxa profunda or rotrusion acetabuli.9,10,22,23,32
The purpose of this study was to compare intermediate-term reoperation rates and functional outcomes after hip arthroscopy between patients with global acetabular overcoverage, lateral acetabular overcoverage, and normal acetabular coverage. We hypothesized that there would be no evidence to suggest an effect of the type of acetabular overcoverage on failure rates or functional outcomes.
Methods
Patient Selection
Beginning in 2012, patients undergoing hip arthroscopy with the senior author (T.Y.) of this study were prospectively enrolled in a cohort study of patients with FAIS. All patients provided consent for study participation as outlined by the approved institutional review board protocol (IRB Protocol i15-00058). FAIS was diagnosed clinically using relevant patient history, physical examination signs (eg, Patrick test and anterior impingement test), and radiologic findings. Patients underwent anteroposterior (AP) supine, 45° Dunn, and 90° Dunn view radiographs to assess bony hip pathology, while additional soft tissue pathology and chondrolabral lesions were characterized using magnetic resonance imaging or magnetic resonance arthrography.
Patients were included in the analysis if they underwent primary hip arthroscopy for symptomatic FAIS and had a minimum of 5 years of postoperative follow-up data. To compare the functional outcomes between different types of acetabular overcoverage, the patients were categorized into 1 of 3 groups. Patients with both LCEA ≥40° and coxa profunda (ie, medialization of the medial wall of the acetabulum beyond the ilioischial line on AP pelvis radiographs) were defined as having global acetabular overcoverage (Figure 1). Patients with LCEA ≥40° but no coxa profunda were defined as having lateral acetabular overcoverage. Patients with LCEA <40° and no coxa profunda were defined as having no acetabular overcoverage.
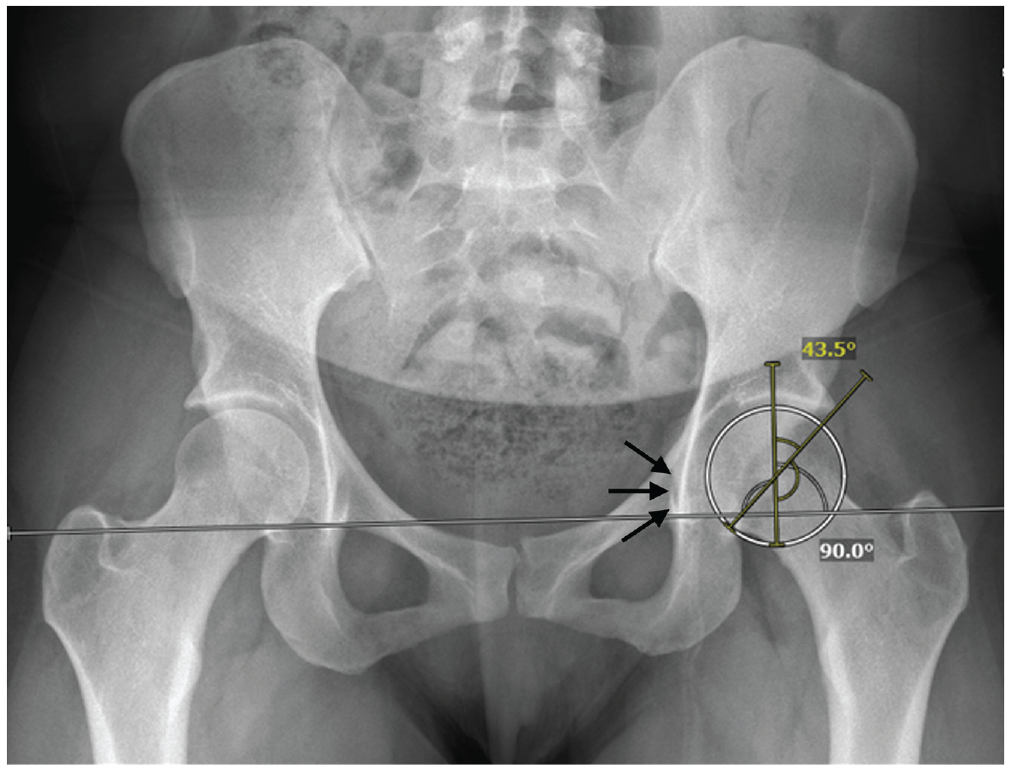
Preoperative pelvis radiograph obtained in a patient with global acetabular overcoverage as demonstrated by elevated lateral center-edge angle and coxa profunda (arrows).
Exclusion criteria consisted of patients undergoing bilateral hip arthroscopy, Tönnis grade >1, joint space narrowing with <2 mm remaining joint space, pediatric patients (<15 years of age), history of rheumatological disease, history of slipped capital femoral epiphysis, and previous ipsilateral hip surgery.
Surgical Technique and Postoperative Recovery Protocol
Under anesthesia, midanterior and anterolateral portals were made as previously described to perform initial diagnostic hip arthroscopy.2,3,19 Fluoroscopy was used to perform periacetabular or femoral osteochondroplasties for pincer and cam lesions, respectively. Labral tears were repaired when possible. For tear patterns that were not amenable to repair, labral debridement was performed. No patients in this cohort underwent labral reconstruction during the primary hip arthroscopy. Any loose bodies were removed. The horizontal interportal capsulotomy was closed with a standard repair at the end of each case. All patients received postoperative hip abduction bracing that limited hyperextension and external rotation immediately after surgery. Patients were flatfoot weightbearing with crutches for the first month. Postoperative antibiotics (cefalexin, 500 mg twice daily), deep vein thrombosis chemoprophylaxis (aspirin, 81 mg daily), and heterotopic ossification prophylaxis (celecoxib, 200 mg daily) were administered.
Patient-Reported Outcomes
The Nonarthritic Hip Score (NAHS) and modified Harris Hip Score (mHHS) were measured preoperatively and then postoperatively at 3 months, 6 months, 1 year, 2 years, and 5 years. The primary outcome of this study was the difference in patient-reported hip function as measured by mHHS and NAHS between acetabular coverage groups at the time of final follow-up for those patients for whom primary arthroscopy did not fail. The secondary outcome was failure of primary hip arthroscopy as defined by requiring either revision hip arthroscopy or THA during the study period. When relevant, mHHS was evaluated on the basis of minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS) achievement rates with 8 points for the MCID threshold and 74 points for thre PASS threshold, as previously published. 5
Statistical Analysis
A priori sample size calculation was performed to evaluate the number of patients needed to detect a difference in mHHS of 11.4 points at the time of final follow-up, which represents the intermediate-term MCID for this functional score based on a previous investigation. 5 For a 1-way analysis of variance (ANOVA), based on an anticipated effect size of f = 0.4 (corresponding to a difference in means equivalent to the MCID), α = 0.05, and 1 –β = 0.8, a total sample size of 66 patients was needed.
Cox proportional hazards regression was used to evaluate the risk of primary arthroscopy failure over time. The differences in mHHS and NAHS at the time of final follow-up for those patients who did not require reoperation during the study period were compared between groups using ANOVA and multiple comparison tests as necessary. The differences in mHHS and NAHS were also evaluated using linear mixed-effects models, which included the fixed effects of type of acetabular overcoverage, postoperative LCEA >40°, age, sex, body mass index (BMI), and time from surgery, as well as by patient random effect. Multiple linear regression models were used to evaluate the factors associated with patient-reported functional status at the time of final follow-up. All statistical comparisons were deemed significant at P < .05. Analysis was performed using R (R Foundation for Statistical Computing).
Results
Patient Cohort
Of the 131 patients who underwent primary hip arthroscopy for FAIS, 94 patients (71.8%) had follow-up of at least 5 years postoperatively and were included in the analysis (Figure 2). The mean age of the overall cohort was 41.9 ± 14.2 years, and there was a mean follow-up duration of 6.1 ± 0.9 years. Of the included patients, 38 (40.4%) had no acetabular overcoverage, 34 (36.2%) had lateral acetabular overcoverage but no global overcoverage, and 22 (23.4%) had global overcoverage. Patients in the lateral overcoverage group had a greater mean age than patients in the no-overcoverage group (47.2 ± 14.0 years vs 37.9 ± 11.8 years; P = .018). Otherwise, baseline patient demographics were similar (Table 1).
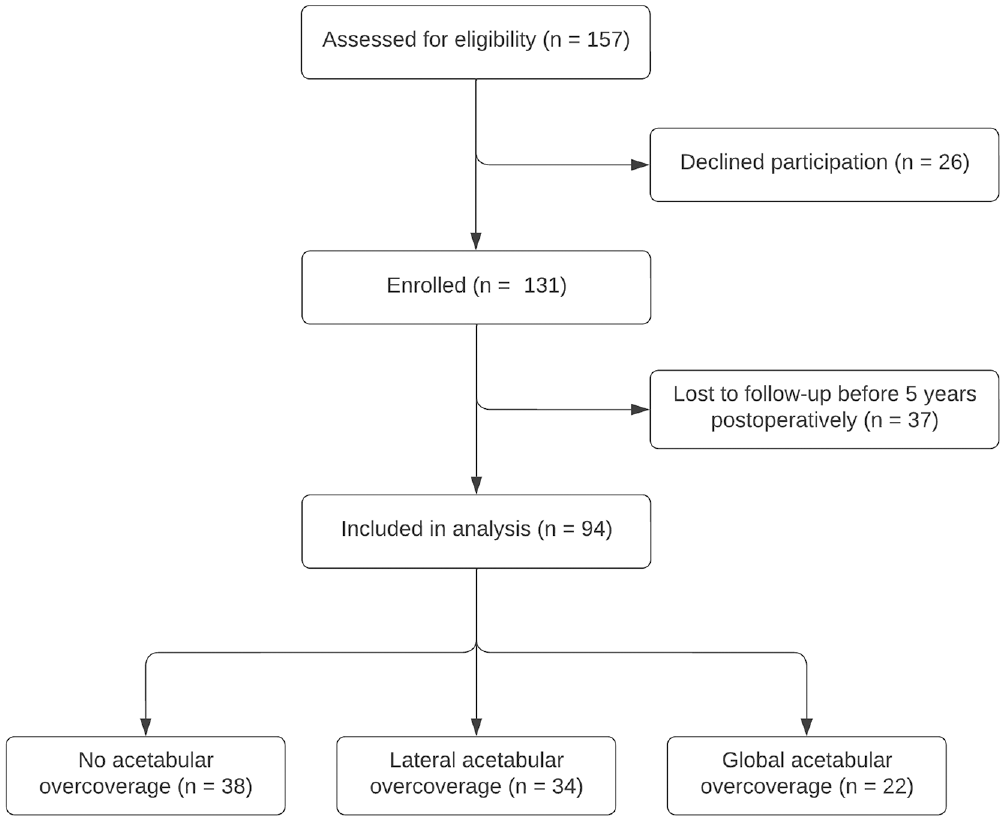
Flowchart of patients included in the analysis.
Comparison of Demographic Variables, Radiographic Measurements, Operative Factors, and Postoperative Outcomes Between Patients With No Acetabular Overcoverage, Lateral Acetabular Overcoverage, and Global Acetabular Overcoverage a
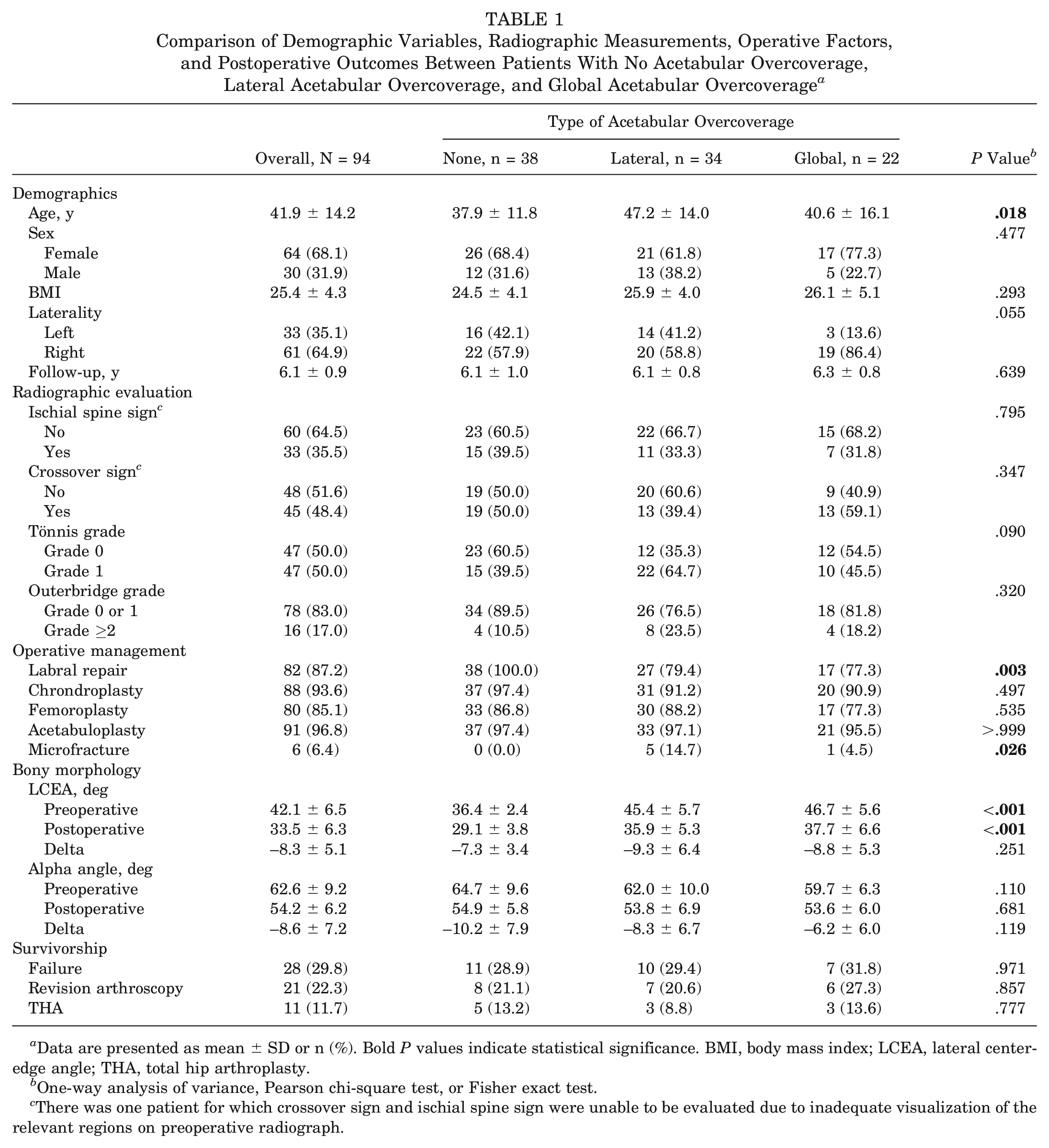
Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance. BMI, body mass index; LCEA, lateral center-edge angle; THA, total hip arthroplasty.
One-way analysis of variance, Pearson chi-square test, or Fisher exact test.
There was one patient for which crossover sign and ischial spine sign were unable to be evaluated due to inadequate visualization of the relevant regions on preoperative radiograph.
Patients in the no-overcoverage group had a lower LCEA both preoperatively and postoperatively. There was no difference in preoperative or postoperative alpha angle between groups (Table 1). A significantly greater percentage of patients with no acetabular overcoverage underwent labral repair (100.0%) compared with patients with lateral overcoverage (79.4%; P = .004) and global overcoverage (77.3%; P = .005).
Preoperative Hip Function
Overall, patients demonstrated poor hip function preoperatively based on mHHS (mean score, 44.2 ± 12.0 for all patients) and NAHS (mean score, 48.4 ± 13.7 for all patients). Patients with no acetabular overcoverage had a greater baseline mHHS than patients with lateral overcoverage (48.2 ± 11.6 vs 40.6 ± 11.6; P = .009), although the difference in means was slightly less than the reported MCID of 8 points for mHHS. There was no baseline difference in mHHS between the no-overcoverage group and the global overcoverage group (43.1 ± 12.5; P = .144), or between the global overcoverage group and the lateral overcoverage group (P = .476). Similarly, there were no differences in preoperative NAHS between any of the 3 groups (P = .069).
Failure of Primary Hip Arthroscopy
A total of 28 patients (29.8%) experienced failure of the primary hip arthroscopy and underwent reoperation by the time of final follow-up. There was no difference in percentage of patients for whom primary arthroscopy failed between the acetabular overcoverage groups (P = .971). At a mean of 2.0 ± 1.6 years after the initial surgery, 21 patients (22.3%) underwent revision arthroscopy. Among the patients who underwent revision arthroscopy, 3 (14.3%) underwent revision labral debridement, 5 (23.8%) underwent labral reconstruction, and 13 (61.9%) underwent revision labral repair. All patients underwent additional bony resection during revision arthroscopy. There was no difference between groups with respect to the proportion of patients who underwent revision arthroscopy (P = .857) or time to revision arthroscopy (P = .847). Eleven patients (11.7%) underwent THA at a mean of 3.2 ± 2.7 years after primary hip arthroscopy. There was no difference between groups with respect to the proportion of patients who underwent THA (P = .777) or time to THA (P = .234).
Overall, 87.2% of the included patients underwent labral repair at the time of primary hip arthroscopy. A significantly greater percentage of patients with no acetabular overcoverage underwent labral repair compared with patients with both lateral and global overcoverage (100.0% vs 79.4% vs 77.3%, respectively; P = .003). Among patients who underwent labral repair, 25.6% underwent reoperation by the time of final follow-up, compared with 58.3% of patients who underwent labral debridement alone and did not undergo labral repair during the primary surgery (P = .038). Based on Cox proportional hazards regression, labral repair at the time of primary hip arthroscopy was associated with a significantly lower risk of failure (hazard ratio [HR], 0.33; 95% CI, 0.12-0.86; P = .023), while the type of acetabular overcoverage was not significantly associated with the risk of failure (lateral overcoverage: HR, 0.77; 95% CI, 0.30-1.98; P = .588; global overcoverage: HR, 0.77; 95% CI, 0.28-2.17; P = .626) (Figure 3).
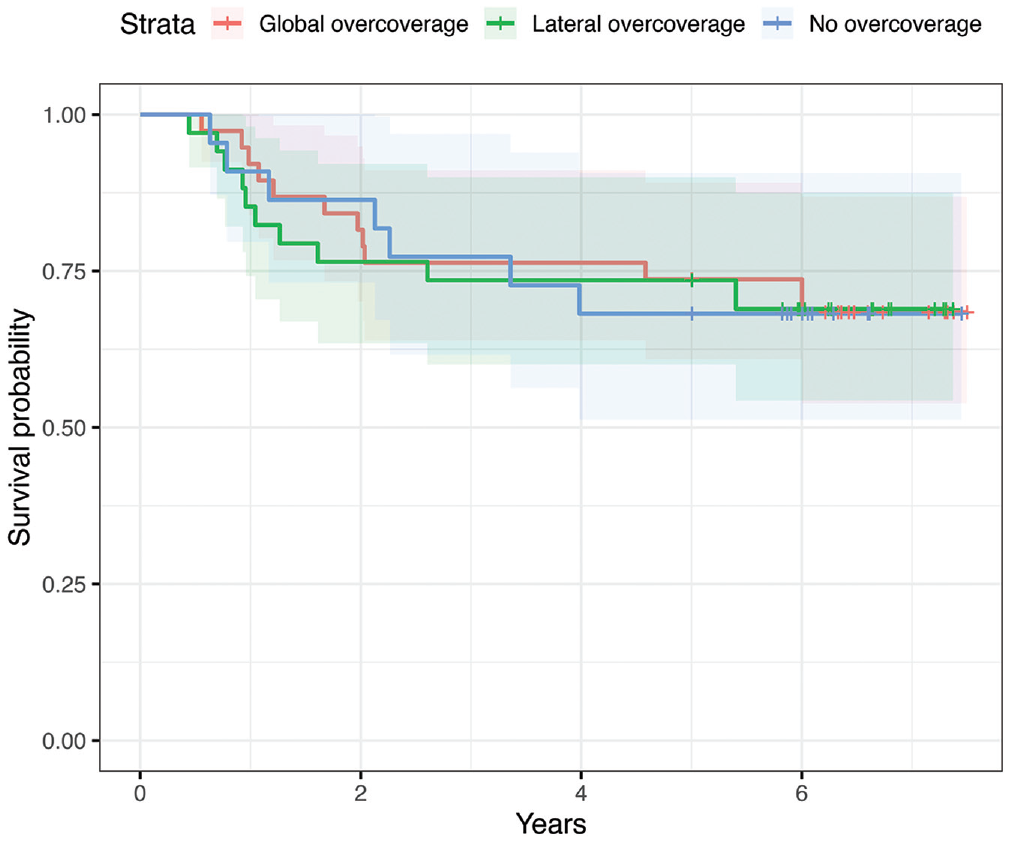
Survival of primary hip arthroscopy over time based on type of acetabular overcoverage.
Intermediate-Term Functional Outcomes
Among patients who did not undergo reoperation during the study period (70.2% of the overall cohort), the differences in patient-reported functional status at the time of final follow-up were compared between groups. At a minimum of 5 years postoperatively, there was no difference in mHHS between patients with global acetabular overcoverage, patients with lateral overcoverage, and patients with no overcoverage (79.2 ± 24.6 vs 84.2 ± 15.8 vs 83.5 ± 12.4; P = .647). Similarly, there was no difference in NAHS between groups at a minimum of 5 years postoperatively (85.0 ± 23.2 vs 88.3 ± 17.5 vs 89.0 ± 15.2; P = .783).
Overall, the mean mHHS increased quickly from the time of surgery until 6 months postoperatively and then continued to increase at a slower rate until reaching a maximum at 2 years postoperatively. From 2 to 5 years postoperatively, the mHHS decreased by a mean of 9.6 points, slightly more than the reported MCID, to a final follow-up score of 83.2 ± 16.9. Despite the worsening of mHHS between 2 and 5 years after surgery, the mean 5-year mHHS remained above the reported PASS score of 74 and was similar to the functional status achieved at 1 year postoperatively (Figure 4). Of those for whom primary surgery did not fail, 78.8% reported an mHHS above the PASS score at 5 years postoperatively. Based on a linear mixed-effects model, the type of acetabular overcoverage did not have a significant effect on mHHS.
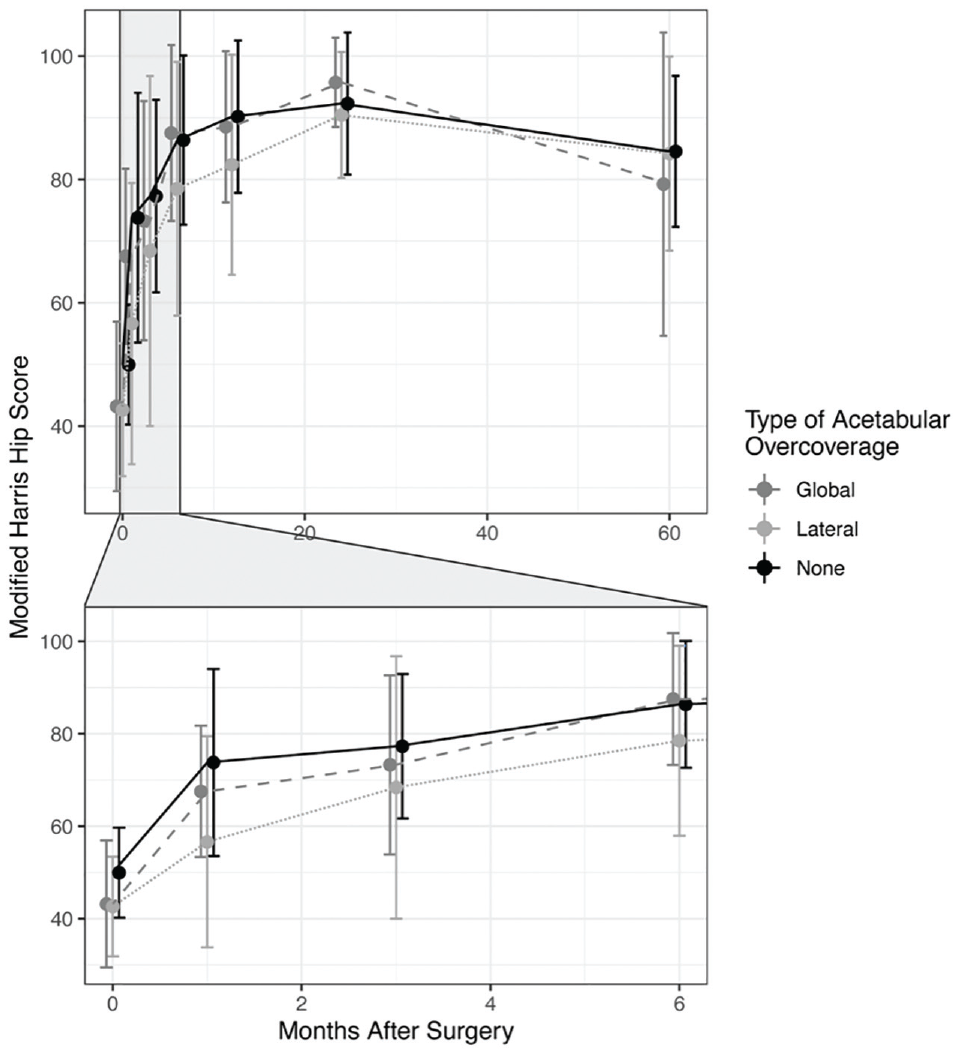
Change in modified Harris Hip Score from preoperative baseline to 5 years postoperatively based on type of acetabular overcoverage.
The mean NAHS increased after surgery until 1 year postoperatively and then remained stable at the 2- and 5-year follow-up time points. The final intermediate-term NAHS was 88.1 ± 17.8 for the overall cohort, representing a maintained functional status above the reported PASS score (Figure 5). Again, the type of acetabular overcoverage did not have a significant effect on NAHS based on a linear mixed-effects model consisting of patients who did not require reoperation after primary hip arthroscopy.
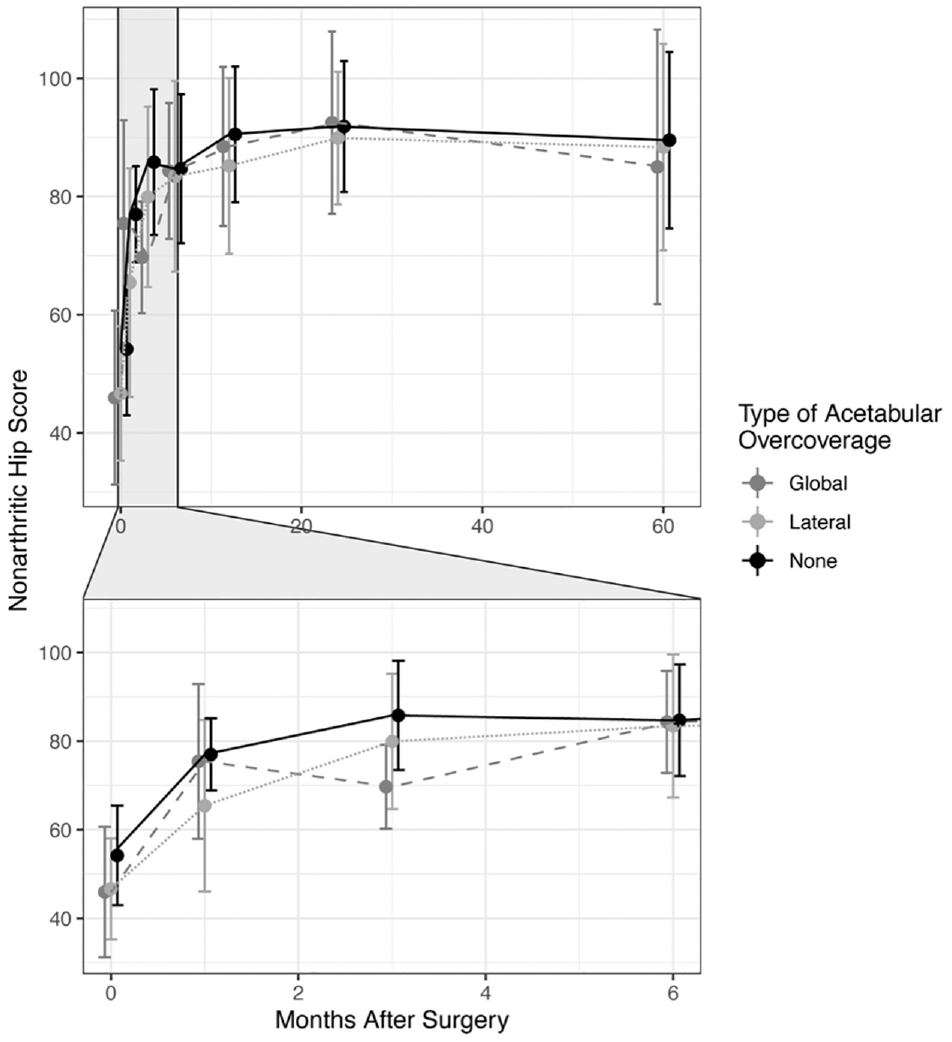
Change in Nonarthritic Hip Score from preoperative baseline to 5 years postoperatively based on type of acetabular overcoverage.
Multiple linear regression models were developed to evaluate the factors associated with subjective functional status at a minimum of 5 years postoperatively in the subset of patients for whom primary surgery did not fail. Postoperative LCEA >40°, female sex, and higher BMI were associated with worse intermediate-term hip function (both mHHS and NAHS) when controlling for age and preoperative mHHS. The type of acetabular overcoverage did not have a significant effect on mHHS at final follow-up, provided that patients with global or lateral overcoverage had a sufficient acetabuloplasty to decrease the postoperative LCEA to <40° (Figure 6).
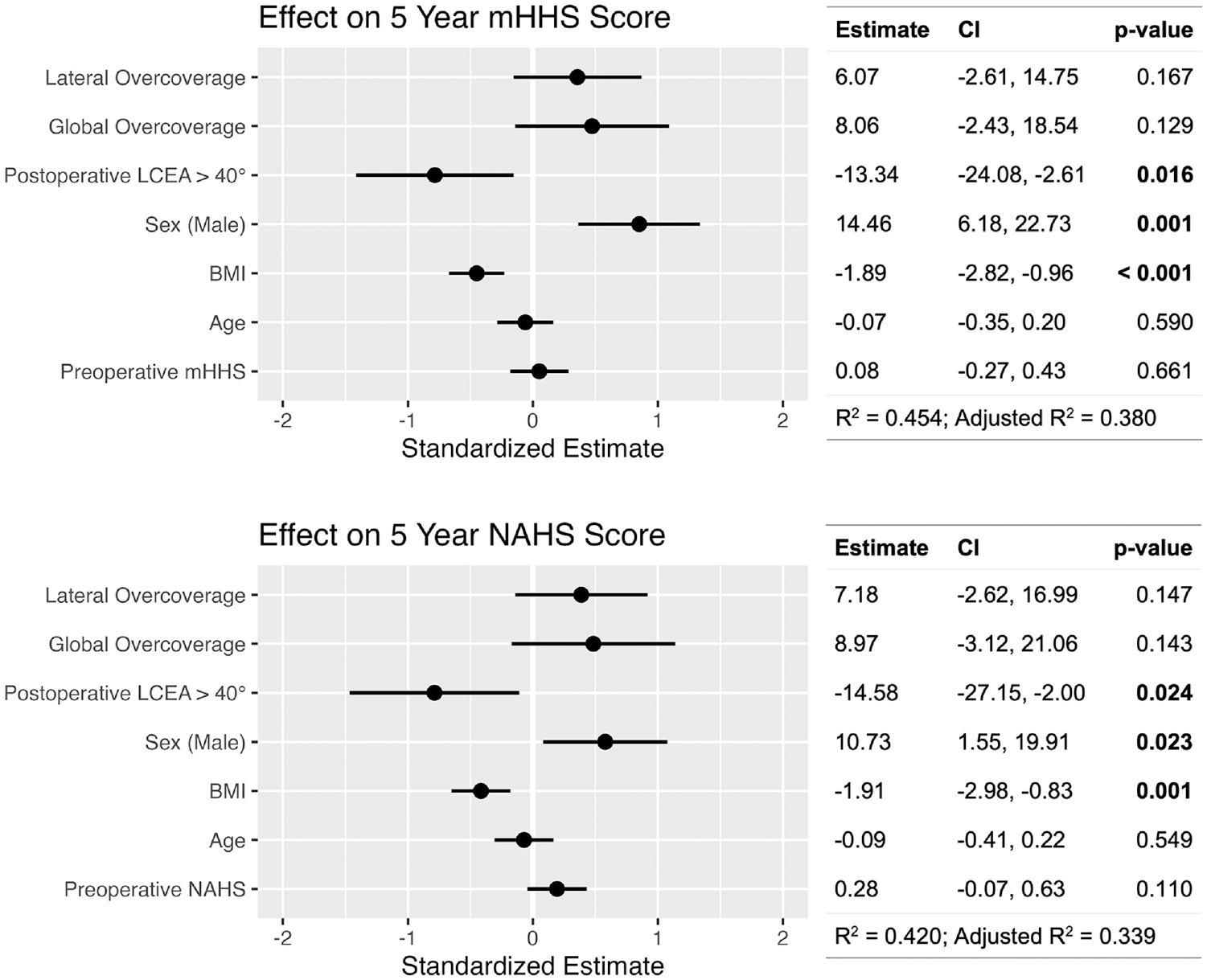
Linear regression models demonstrating the effect of acetabular overcoverage, postoperative lateral center-edge angle, sex, and body mass index (BMI) on 5-year postoperative functional status when controlling for age and preoperative baseline functional status for patients who did not undergo reoperation for failed primary hip arthroscopy. LCEA, lateral center-edge angle; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score.
Discussion
Our results demonstrate that there is no evidence for any difference in intermediate-term postoperative outcomes between patients with global acetabular overcoverage, regional lateral overcoverage, and normal acetabular coverage. The overall cohort demonstrated a rapid improvement in hip function during the first postoperative year. After 1 year, the rate of improvement slowed, but functional status continued to increase until 2 years postoperatively before stabilizing. After 2 years, patients may demonstrate a small decline in hip function over the next several years, although patient-reported outcomes remained high at the 5-year time point. Even though NAHS did not demonstrate the partial drop in functional status between 2 and 5 years postoperatively that was observed with mHHS, the overall trend in patient-reported outcomes over time was similar between the 2 scoring systems. Importantly, the 3 groups demonstrated similar responses to surgery over the 5-year study period. There was no difference in functional outcomes based on the type of acetabular overcoverage, provided that sufficient acetabuloplasty was performed intraoperatively.
Acetabular overcoverage can contribute unique challenges to hip arthroscopy, including difficulties with hip joint distraction, central compartment access, instrument navigation, and appropriate acetabuloplasty. 10 Additionally, overcoverage often portends more complex labral pathology. Maldonado et al 21 suggested that for each additional degree of LCEA, there is a 6% increase in the odds of the need for primary labral reconstruction. Some studies note a connection between obesity and global acetabular overcoverage, further adding to the complexity of addressing this pathology. 35 In both the existing literature and this study, higher BMI was associated with worse intermediate-term outcomes. 17 Because of the additional complexities associated with these cases, severe overcoverage deformities have previously been treated with surgical hip dislocation, although this is becoming less frequent with technical advancements in hip arthroscopy. 24
The effect of global and regional acetabular overcoverage on outcomes after hip arthroscopy remains controversial, likely because of heterogeneity in definition and methodology. In their multicenter cohort of 388 patients, Matsuda et al 25 reported no difference in pre- to postoperative improvement in International Hip Outcome Tool Short Form scores, revision hip arthroscopy, or conversion to THA between patients with overcoverage (LCEA, ≥39°) and those without at a minimum 2-year follow-up. Similarly, at a minimum 5-year follow-up, Maldonado et al 21 reported that there was no significant difference in functional outcomes of 45 patients with LCEA >40° compared with a comparison group of patients with LCEA from 25° to 40°.
However, the studies by Matsuda et al 25 and Maldonado et al 21 must be interpreted within the context of their use of LCEA as the sole criterion to define overcoverage. Elevated LCEA only denotes regional superolateral overcoverage, but cannot be used in isolation to define global acetabular overcoverage. 14 Similarly, coxa profunda in isolation has a poor sensitivity and specificity for global acetabular overcoverage. 6 Rather than using a single overly simplistic radiographic measurement to identify patients with global overcoverage, using a combination of both LCEA >40° and coxa profunda seems to be a more accurate method of diagnosis. 6 Our study defines global overcoverage using both radiographic parameters, and distinguishes it from regional lateral overcoverage.
Two separate 2017 analyses by Chandrasekaran et al9,10 accurately use LCEA and coxa profunda to define global overcoverage. They first evaluated a cohort of 35 patients with global overcoverage treated operatively with a mean follow-up of 2.6 years. They reported a mean improvement of 13.5 ± 17.7 points for mHHS, leading to a mean of 79.3 ± 17.8 points at the time of final follow-up, but they reported that the change in mHHS did not meet the MCID for the functional outcome score. 10 Confusingly, the study that they referenced by Chahal et al 7 is an evaluation of the PASS value for mHHS, not MCID. Furthermore, they reported that the mean mHHS at final follow-up was greater than the PASS value of 74 determined by Chahal et al, and the mean improvement in mHHS was greater than the commonly used MCID values. 5 In a second study, Chandrasekaran et al 9 then compared the outcomes in largely the same cohort of patients with a comparison group consisting of patients with normal LCEA. They reported that the mean change in mHHS from baseline was significantly less for the global overcoverage group than the change from baseline for the comparison group. However, the more meaningful analysis is the direct comparison of postoperative scores between groups, which demonstrated no significant difference. 9
The results of our analysis differ from those of Chandrasekaran et al. 9 On the basis of their data, they concluded that operative management of global acetabular overcoverage can be expected to lead to worse short-term functional improvement compared with FAIS without global overcoverage. However, our results demonstrate that there was no evidence for any difference in short- or intermediate-term functional outcomes between patients with global overcoverage, regional lateral overcoverage, and normal acetabular coverage provided that a sufficient acetabuloplasty was performed. Furthermore, Chandrasekaran et al 9 suggested that patients with global overcoverage are at a greater risk of reoperation after primary hip arthroscopy. Our results demonstrated no difference in the risk of reoperation or conversion to THA between groups. Overall, we did not find evidence that outcomes for patients with global acetabular overcoverage were significantly different than those for patients with regional lateral overcoverage or normal acetabular coverage.
Limitations
The most significant limitation of this study is that 2-dimensional radiographic parameters were used to approximate the complex 3-dimensional morphology of the acetabulum. Although combining the radiographic criteria of LCEA and coxa profunda is more accurate than using either parameter alone, a technique that uses 3-dimensional advanced imaging to characterize acetabular overcoverage would likely be superior. Several methods of 3-dimensional acetabular measurement have been proposed with promising results, but none have reached the point of regular clinical use.18,28 Despite the inherent limitations, evaluation of acetabular morphology based on radiographs continues to be a popular method used by hip surgeons.
There were some baseline differences between the groups. Notably, the proportion of patients who underwent labral repair was greater among those with normal acetabular coverage compared with those with lateral or global overcoverage. This may be the result of chance imbalance—if just 2 of the patients in the normal acetabular coverage group had not undergone labral repair the difference between groups would no longer be statistically significant—or the differences in acetabular anatomy may be associated with labral tear patterns that are more amenable to repair. The effect of labral repair on failure of primary hip arthroscopy was accounted for by including it in the multivariable survival analysis.
None of the patients included in this study underwent labral reconstruction during primary hip arthroscopy, and we were therefore unable to evaluate differences in survival or functional outcomes between labral repair and labral reconstruction. However, given the convincingly beneficial effect of labral repair compared with debridement alone (as demonstrated by the significantly lower risk of failure among patients who underwent labral repair), it is possible that for patients with nonrepairable tears, labral reconstruction may lead to improved outcomes.
The mean age of patients in this cohort who underwent surgery is higher than that in other reports, and the results should be interpreted in this light. Furthermore, mHHS has been shown to have a ceiling effect compared with other outcome scores. The senior author has been collecting mHHS and NAHS data for the last 10 years, and therefore much of his long-term outcome research still relies on these scores.
Conclusion
In this analysis of 94 patients with FAIS who underwent operative management, there was no difference in functional outcomes or rate of reoperation at a minimum of 5 years postoperatively between those with global acetabular overcoverage, those with regional lateral overcoverage, and those with normal acetabular coverage. Provided that an appropriate acetabuloplasty is performed, there is no evidence to suggest that global acetabular overcoverage portends a worse prognosis than other FAIS subtypes.
Footnotes
Submitted April 3, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.Y. has received royalties and consulting fees from Arthrex Inc, and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.