
Abstract
Background:
Distal tibial allograft (DTA) reconstruction for glenoid bone loss is nonanatomic, as it does not match the glenoid radius of curvature (ROC) in the anterior-posterior (AP) plane. The dorsal articular portion of the distal radius has not been previously described as an allograft reconstruction option for glenoid bone loss.
Purpose:
To evaluate distal radius fresh-frozen allograft (DRA) as a potential match for glenoid reconstruction.
Study Design:
Controlled laboratory study.
Methods:
Eighteen fresh-frozen human cadaveric specimens—including 6 shoulder, 6 wrist, and 6 tibia specimens—were used. The ROC and the graft length were measured in the superior-inferior (SI) plane. A 30% defect was created in all glenoid specimens, and both DTAs and DRAs were harvested to assess graft fit after fixation. Computed tomography analysis was used to assess bony ROC and bone mineral density (BMD).
Results:
The cadaveric specimens had a mean age of 77 years. The mean SI glenoid length was 39.7 mm compared with 36.8 mm for the DRA and 30 mm for the DTA. The ROC in the SI plane was 29 ± 5.3 mm for the glenoid, 37.8 ± 4.9 mm for the DRA, and 24 ± 3.7 mm for the DTA. In the AP plane, the ROC was 39.6 ± 6.6 mm for the glenoid, 30.4 ± 18.6 mm for the DRA, and 126.3 ± 9.5 mm for the DTA. On computed tomography analysis, the ROC in the SI plane was 30.4 ± 1.5 mm for the glenoid, 30.3 ± 5.6 mm for the DRA, and 24.5 ± 9.4 mm for the DTA. In the AP plane, the ROC was 30.8 ± 2 mm for the glenoid, 19.1 ± 2.3 mm for the DRA, and 46.7 ± 21.7 mm for the DTA. The BMD was 226.3 ± 79 Hounsfield units (HU) for the glenoid, 228.5 ± 94.7 HU for the DRA, 235 ± 96.2 HU for the coracoid process, and 235.1 ± 84.6 HU for the DTA.
Conclusion:
Compared with the DTA, the DRA had a greater mean graft length in the SI plane, providing utilization in cases of larger bony defects; the DRA has a more acute ROC in the AP plane (closer to that of the glenoid), providing a greater potential buttress to anterior humeral translation. Compared with currently utilized grafts, the DRA BMD was not significantly diminished. This study presents the DRA as a novel allograft reconstruction option in the setting of anterior glenoid bone loss; further biomechanical and clinical investigation is indicated.
Glenoid bone loss in the setting of recurrent shoulder instability remains a challenging surgical problem. The bony foundation of the glenoid and the surrounding soft tissue is critically compromised in a way that destabilizes the shoulder joint and renders it susceptible to subsequent dislocation and subluxation events. 2 Surgical management revolves around bony augmentation utilizing allogenic or autologous grafts.3,7,15 Graft options for glenoid bone augmentation have been adequately explored in the literature, with each graft option entailing several clinical implications on the presenting patients and their therapeutic outcomes.3,7,14,15
The Latarjet procedure—transfer of the coracoid process for glenoid augmentation—has been well established in the literature and remains the preferred autograft reconstruction option by many surgeons.3,8,9 However, significant variance in patient coracoid anatomy exists. 11 Therefore, the Latarjet procedure cannot accommodate every bony defect, especially in severe glenoid bone loss. This often necessitates bigger grafts for reconstruction. The iliac crest is another described autograft option with good outcomes in shoulder surgery literature.14,15 However, the invasiveness and morbidity of the graft harvesting process remain a limitation for this procedure. 14
Provencher et al 18 first introduced the distal tibial allograft (DTA) as a potential allograft reconstruction option in cases of glenoid bone loss, and there has been biomechanical investigation to support its use.1,6 Clinically, DTA reconstruction has shown good mid term outcomes, even in cases of revision of failed Latarjet procedures.17-19 Although the procedure has many benefits, its ability to reconstruct the glenoid geometry is variable, with 14% of grafts being morphologically unacceptable. 16 Utilizing a computed tomography (CT) model of cadaveric specimens, Willemot et al 20 showed that the DTA performed well in the coronal reconstruction of the glenoid radius of curvature (ROC) but did not perform well in the reconstruction of the axial plane glenoid ROC. 20 Their study identified glenoid allografts to be the most reliable option to accurately reconstruct native glenoid geometry when compared with the distal tibia or the coracoid process. Still, these grafts are costly and often not available in most surgical health care systems. 20
Exploring novel graft options is of pivotal importance, especially when considering the supply limitations and potential financial constraints of currently available allograft options. To our knowledge, no previous work has evaluated and described the utilization of the dorsal articular portion of the distal radius as an allograft reconstruction option for recurrent instability in the setting of glenoid bone loss. This study aimed to evaluate the use of distal radius fresh-frozen allograft (DRA) as a potential match for glenoid reconstruction by assessing the ROC of the graft and the bone mineral density (BMD). The DTA was utilized as the primary comparison group with cadaveric and CT analysis. We hypothesized that the dorsal articular portion of the distal radius would provide a viable allograft reconstruction option with a ROC that matches the ROC of the native glenoid and a BMD similar to that of the currently described grafts.
Methods
Study Design
This was a cadaveric study exploring the utility of the distal radius as a novel osteochondral allograft option in glenoid bone loss. Eighteen fresh-frozen human cadaveric specimens—including 6 shoulder, 6 wrist, and 6 tibia specimens—were utilized in our study. Characteristics of cadaveric specimens were recorded. All specimens were dissected free of all soft tissues except for the glenoid labrum of the shoulder and dorsal wrist ligaments of the distal radius. All anatomic specimen dissections, graft measurements, and surgical reconstructions were performed by 2 fellowship-trained shoulder surgeons (A.Z.K. and J.A.A.).
Cadaveric Reconstruction and Assessment
Digital calipers were used to measure the anterior-posterior (AP) and superior-inferior (SI) diameters of the glenoid with the labrum attached. Dimensions were taken based on viewing the glenoid en face as a clock, with the superior portion of the glenoid equivalent to 12 o’clock. Diameters were measured from 12 o’clock to 6 o’clock and from 3 o’clock to 9 o’clock. The ROC for each specimen was independently measured by each surgeon in both the SI and AP planes using a digital radius gauge. The graft length in the SI plane was also assessed. A 30% defect was then created in all glenoid specimens, and the distal tibia and distal radius grafts were harvested and prepared for grafting (Figure 1).
A 30% defect was created in all glenoid specimens for later incorporation of distal radius and distal tibia grafts.
The harvested distal radius and distal tibia grafts were labeled and numbered. A computer-based random number generator was used to assign a graft type to each defected shoulder specimen. Glenoid reconstruction was conducted using 2 cannulated screws. The concordance of the ROC of distal radius grafts, distal tibia grafts, and glenoid specimens was assessed qualitatively using inspection of the resultant cadaveric construct and evaluation of anatomic reconstruction.
CT Analysis
CT scans were obtained for all specimens before dissection to confirm the absence of osteoarthritis, significant joint deformity, or evidence of previous surgical procedures. Two independent physicians (A.Z.K. and M.Y.F.) conducted CT imaging analysis. They calculated the ROC of the distal radius grafts, distal tibia grafts, and glenoid specimens before the procedure to assess anatomic concordance. The ROC was evaluated using the “3D Ball” configuration of the Region of Interest tool on Osirix DICOM Viewer software (Figure 2). Each evaluating physician recorded 5 ROC values for the distal radius specimens based on 5 CT cuts—coronal dorsal, coronal volar, sagittal radial, sagittal middle (between radial and ulnar), and sagittal ulnar. Similarly, 5 ROC values were recorded for distal tibia specimens based on 5 CT cuts—lateral, 1 cm medial to lateral, anterior, middle (between AP), and posterior cuts. For the glenoid, 6 ROC values were obtained based on 6 CT cuts—axillary superior, axillary middle (between superior and inferior), axillary inferior, coronal anterior, coronal middle (between anterior and posterior), and coronal posterior. The mean of the values obtained from both physicians were calculated, used, and reported as the ROC in the SI and AP planes.
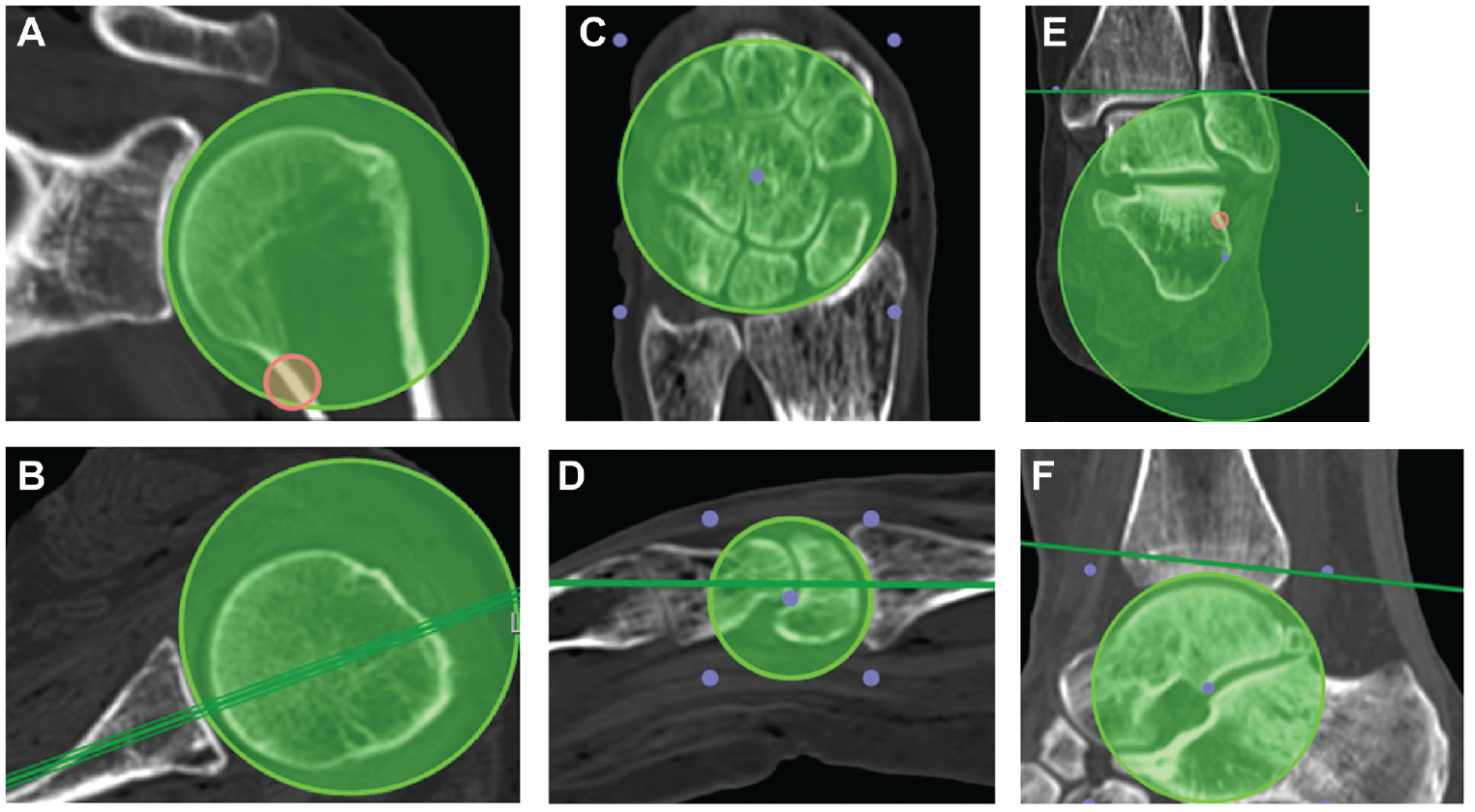
Example of the CT ROC analysis of the glenoid in the (A) coronal and (B) axial planes; the distal radius in the (C) coronal and (D) sagittal planes; and the distal tibia in the (E) coronal and (F) sagittal planes. CT, computed tomography; ROC, radius of curvature.
The BMD of the distal radius grafts, the distal tibia grafts, the coracoid processes native to the cadaveric glenoids, and the cadaveric glenoids were also evaluated and reported. Using a previously described methodology, we calculated the BMD using the “Closed Polygon” tool configuration of the Region of Interest tool on the Osirix DICOM Viewer software. 4 Each evaluating physician calculated 3 BMD measurements of different cuts for the distal radius, distal tibia, coracoid process, and native glenoid of each specimen. Values were reported in Hounsfield Units (HU). The mean BMD measurements obtained from both authors were calculated and reported.
Statistical Analysis
Standard descriptive statistics were utilized to calculate means within each group and calculate standard deviations (Microsoft Excel).
Results
A total of 6 glenoid, 6 distal tibia, and 6 distal radius specimens were obtained for cadaveric analysis. All specimens were left sided. Descriptive data of included specimens is presented in Table 1. The mean SI graft length of the glenoid was 39.7 mm—compared with 36.8 mm for the distal radius and 30 mm for the distal tibia (Table 2A).
Descriptive Data of Glenoid, Distal Radius, and Distal Tibia Specimens a
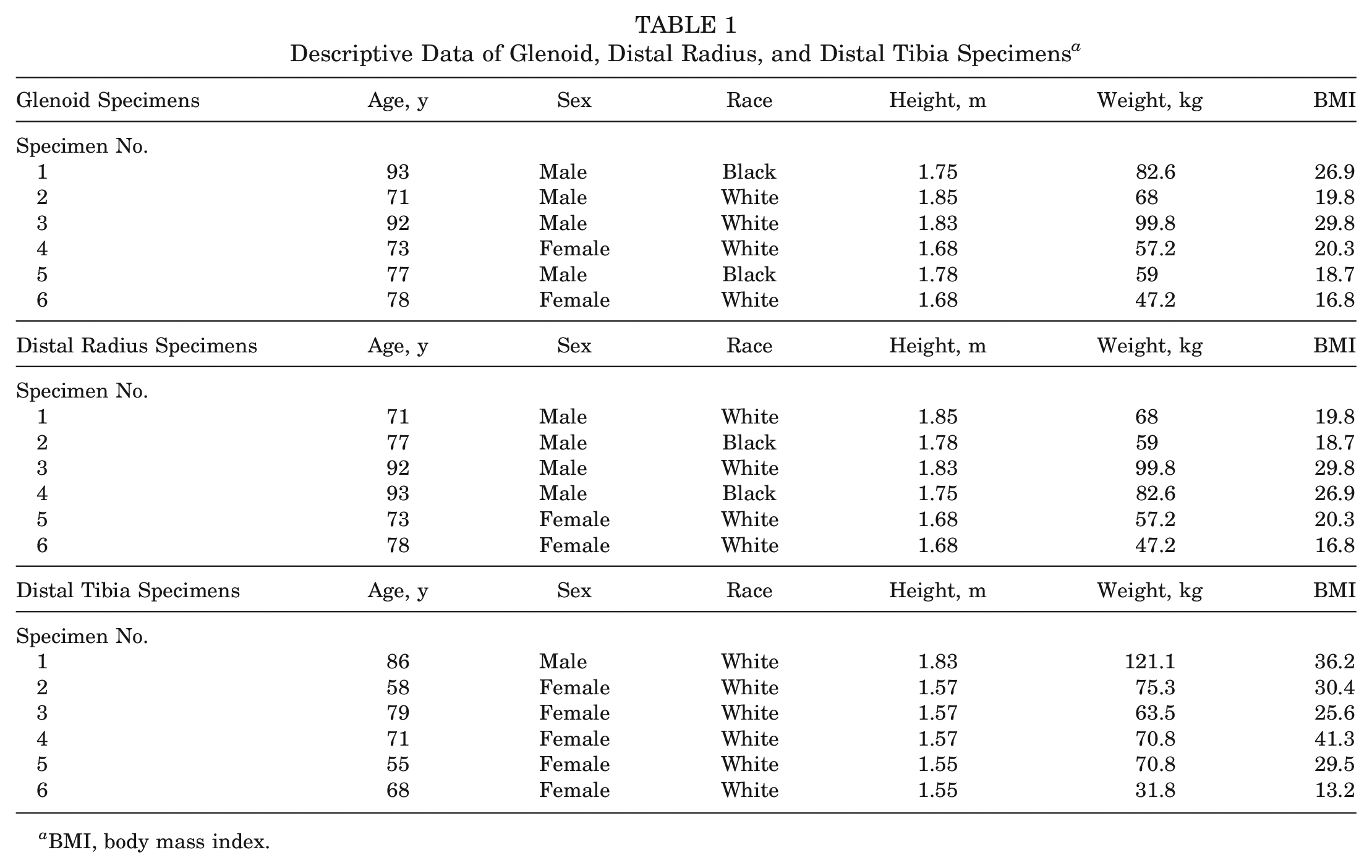
BMI, body mass index.
Mean Cadaveric Measurements of Specimen Length a
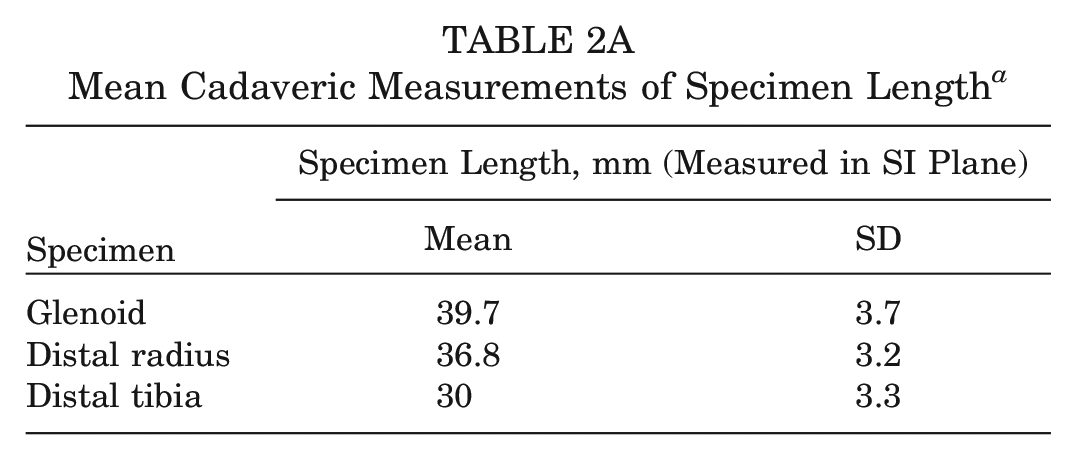
SI, superior-inferior.
The mean ROC in the SI plane was 29 ± 5.3 mm for the glenoid—compared with 37.8 ± 4.9 mm for the distal radius and 24 ± 3.7 mm for the distal tibia. In the AP plane, the mean ROC was 39.6 ± 6.6 mm for the glenoid—compared with 30.4 ± 18.6 mm for the distal radius and 126.3 ± 9.5 mm for the distal tibia (Table 2B).
Mean Cadaveric Measurements of Specimen ROC a
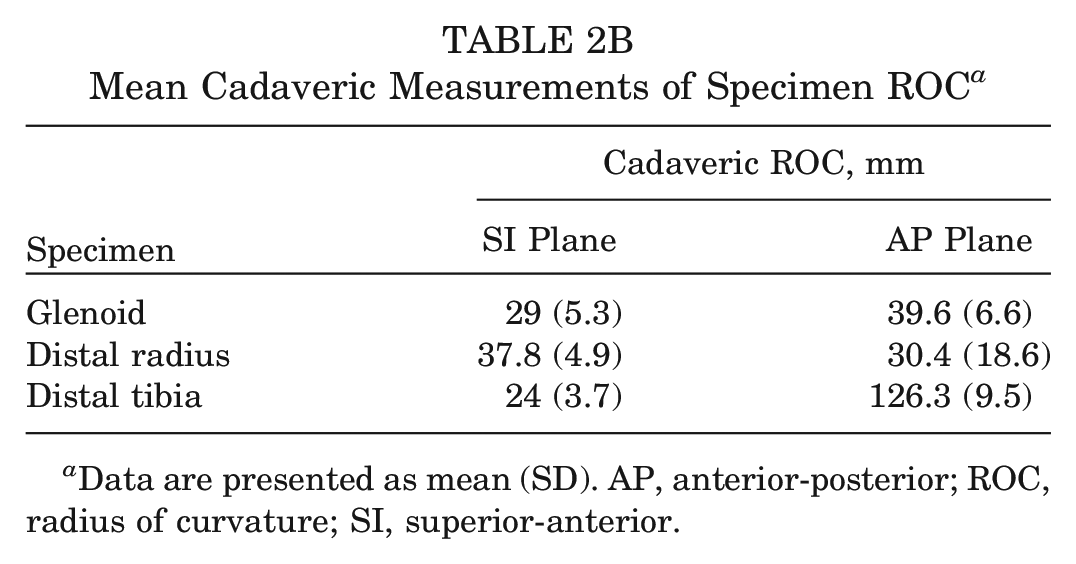
Data are presented as mean (SD). AP, anterior-posterior; ROC, radius of curvature; SI, superior-anterior.
On CT analysis, the mean ROC in the SI plane was 30.4 ± 1.5 mm for the glenoid—compared with 30.3 ± 5.6 mm for the distal radius and 24.5 ± 9.4 mm for the distal tibia. In the AP plane, the mean ROC for the glenoid was 30.8 ± 2 mm—compared with 19.1 ± 2.3 mm for the distal radius and 46.7 ± 21.7 mm for the distal tibia (Table 3).
Mean CT Measurements of ROC a
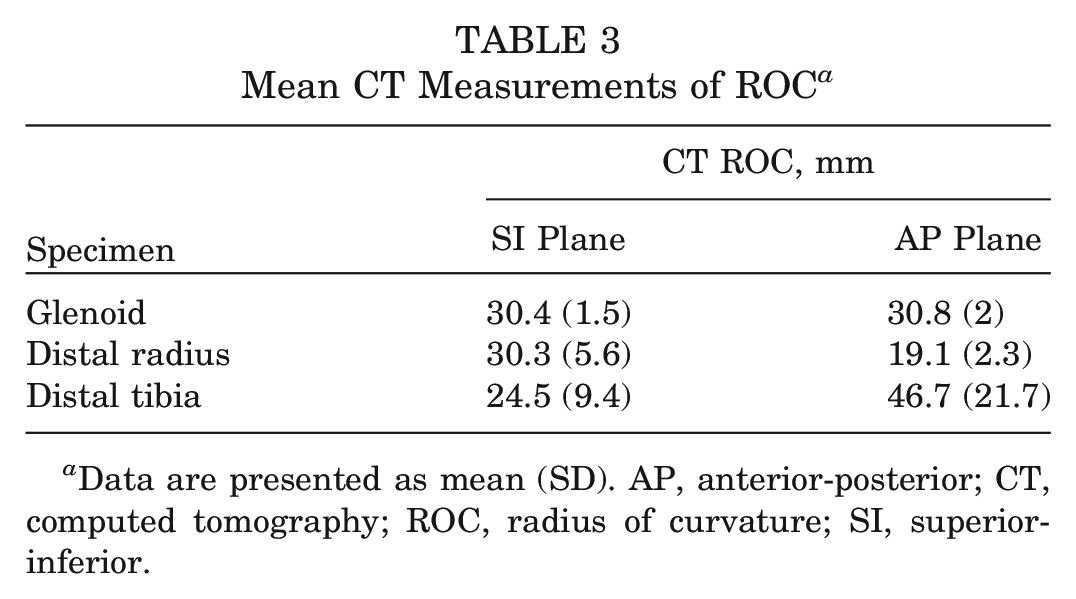
Data are presented as mean (SD). AP, anterior-posterior; CT, computed tomography; ROC, radius of curvature; SI, superior-inferior.
The mean BMD was highest in the distal tibia, measuring 235.1 ± 84.6 HU. The coracoid process followed this at a mean BMD of 235 ± 96.2 HU. The distal radius had the next highest mean BMD of 228.5 ± 94.7 HU. This was last followed by the native glenoid with a mean BMD of 226.3 ± 79.0 HU (Table 4).
Mean CT Measurements of BMD a
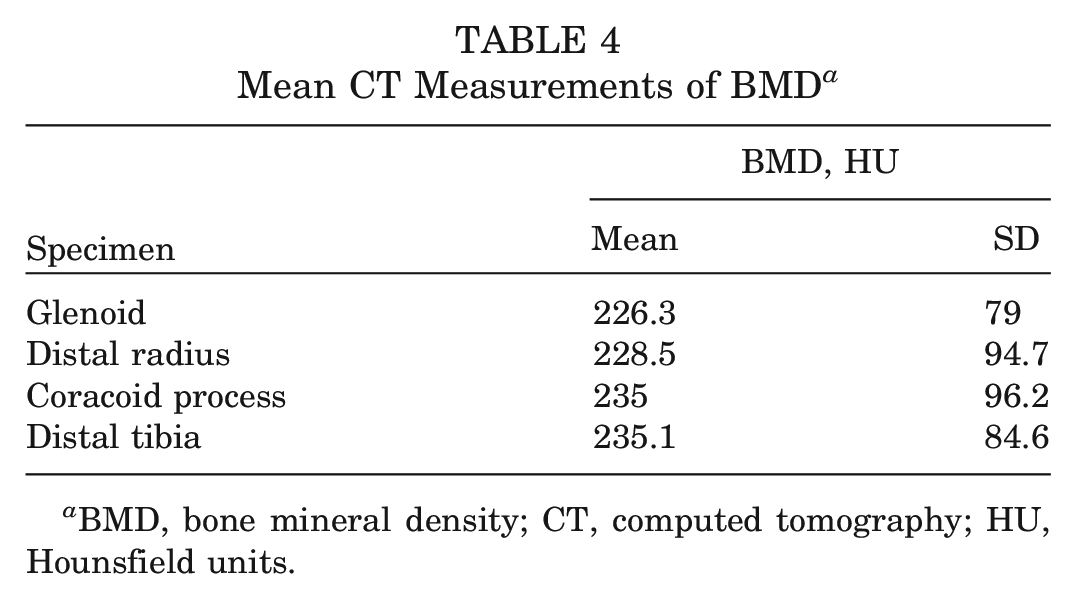
BMD, bone mineral density; CT, computed tomography; HU, Hounsfield units.
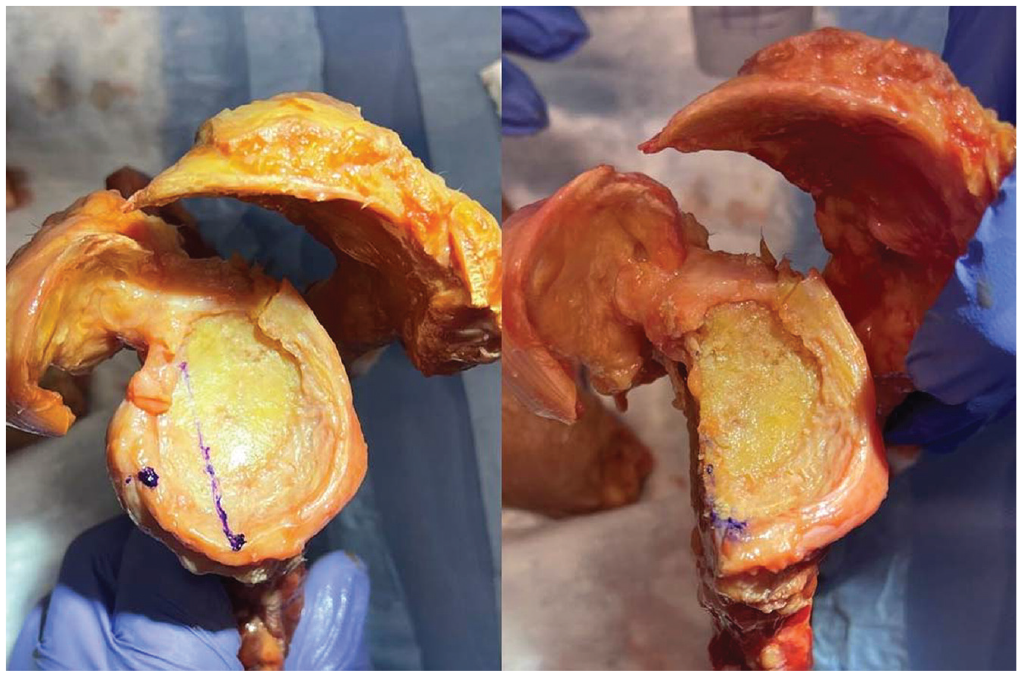
Three glenoids were reconstructed using DTAs, and 3 glenoids were reconstructed using DRAs. The qualitative cadaveric assessment showed better anatomic concordance in the DRA specimens, demonstrating better ROC, similar morphological features, and smoother integration into the native cadaveric glenoid (Figure 2). DTA specimens showed lower levels of anatomic concordance with the glenoid in the axial plane based on subjective cadaveric assessment (Figure 3).
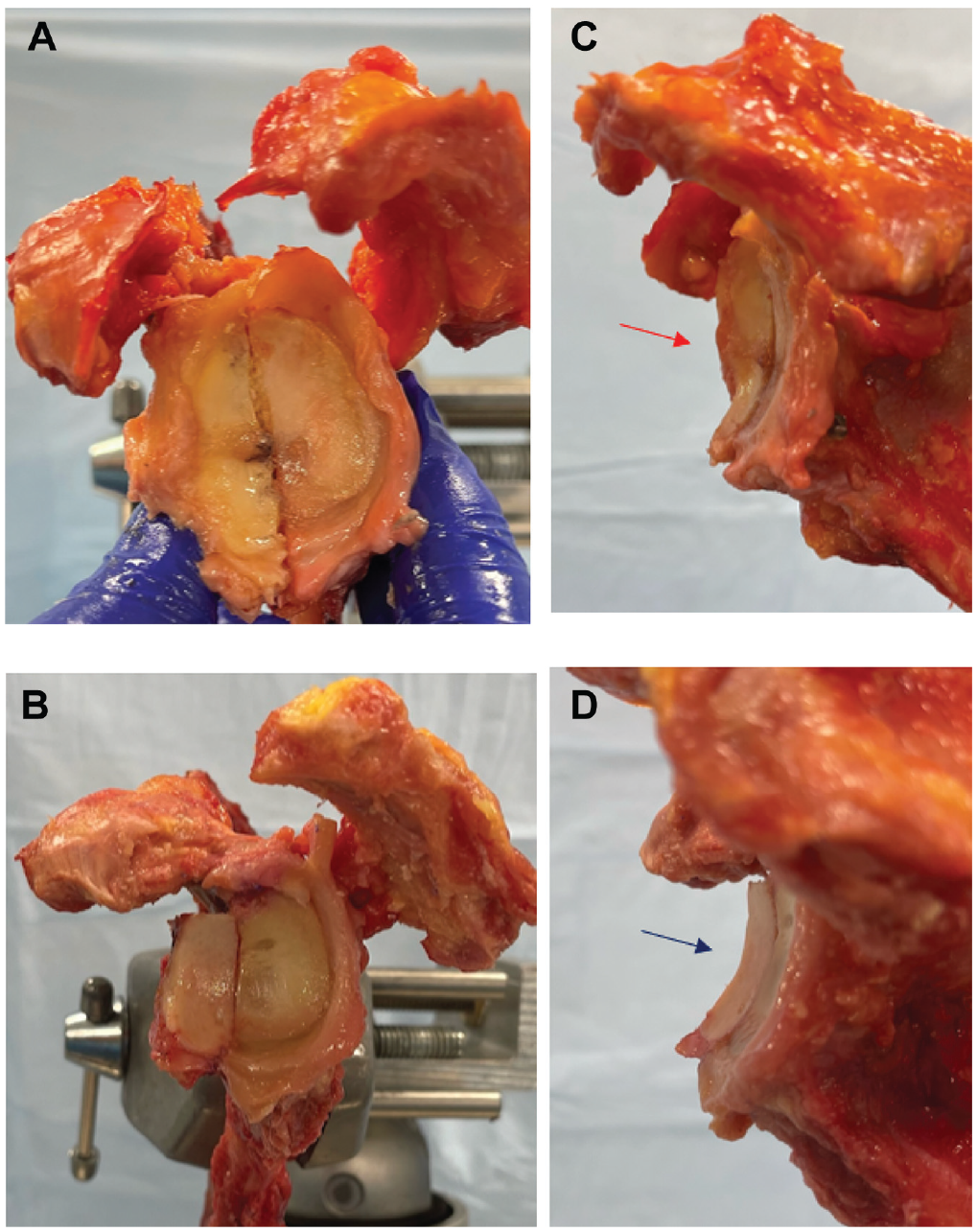
(A) The 30% glenoid defect created for each sample. After the distal radius or the DTA was harvested, it was fixed to the glenoid with 2 cannulated screws. (A) The SI plane and (C) the AP plane demonstrate the DRA. The DTA is demonstrated in the (B) SI plane and the (D) AP plane. The red arrow in the image C denotes the more acute ROC of the dorsal distal radius in the AP plane when compared with the DTA (blue arrow in image D). AP, anterior-posterior; DRA, distal radius allograft; DTA, distal tibial allograft; ROC, radius of curvature; SI, superior-inferior.
Discussion
This study presents the distal radius as a novel allograft reconstruction option for patients with critical anterior glenoid bone loss in recurrent glenohumeral instability. This study describes the utilization of the entirety of the dorsal articular surface—including both the scaphoid and lunate fossa—of the distal radius for glenoid reconstruction. Compared with the DTA, the distal radius had a greater graft length in the SI plane. This suggests a potential role for the distal radius as a reconstructive option in cases of more significant glenoid bone loss.
Another significant finding of this study was the difference in the AP plane ROC between graft options. The distal tibia has a ROC that matches the native glenoid closely in the SI plane but has a much larger ROC (comparatively flat) in the AP plane. Therefore, while it can reconstruct the native glenoid in the superior to inferior plane, it does not reconstruct the native anterior glenoid rim (Figure 3D). Our study’s findings are consistent with previous literature.5,6,20 Willemot et al 20 tested multiple graft reconstruction options. They showed that the distal tibia was a close match to the native glenoid with regard to coronal ROC, but of the multiple graft options they tested, it had the worst ROC match in the axial plane. This articular incongruity could potentiate earlier progression of osteoarthritis. In contrast, this study showed the dorsal articular surface of the distal radius to have a more acute ROC in the AP plane (closer to that of the glenoid), providing the ability to reconstruct the anterior glenoid rim better and potentially creating a greater buttress against anterior humeral translation. In the reconstructed specimens, we were able to qualitatively appreciate a better anterior buttress, as demonstrated in Figure 2. Furthermore, the DRA has the potential to employ the dorsal radiocarpal ligaments, if preserved with the allograft specimen, to perform an anterior capsular soft tissue reconstruction in addition to the allograft bony reconstruction.
One potential area of concern for these authors going into the present investigation was the strength and bone density of a potential DRA. The distal tibia is a more significant weightbearing articular surface compared with the distal radius, which we hypothesized would give the DRA a less significant BMD when compared with a DTA or even a coracoid autograft. This was the motivation behind the evaluation and comparison of graft BMD in this study. Interestingly, there was not a significant difference in the BMD found between graft options (235.1 HU for the distal tibia compared with 235 HU for the coracoid and 228.5 HU for the distal radius) on CT analysis. These were all a close match to the native glenoid at 226.3 HU. Another consideration is that with the DRA option, the dorsal distal radius cortex will be preserved, which should add to anterior bone support and ultimate screw purchase. In harvesting the DTA, the first cut often made is to flatten the incisura fibularis. 12 The concavity of the incisura is highly variable, ranging from a crescentic shape to flat 13 ; therefore, significant cortical bone from the anterior graft could end up being removed based on the anatomy of the tibial allograft utilized.
Given the fresh-frozen allograft supply and cost constraints, the exploration of additional graft options is an important area of investigation. This study presents a novel allograft option for consideration. Decker et al 5 performed a CT analysis evaluating the distal tibia ROC compared with the native glenoid and the humeral head. They found that when randomly pairing samples, there was a ROC match of the distal tibia to the native glenoid in only 22% of cases. This finding highlights the significant variation in human anatomy and, consequently, allograft match availability, further demonstrating the need to have additional graft options available to reconstructive shoulder surgeons.
There are limitations to this study. This was a cadaveric analysis to assess the anatomic feasibility and utility of the distal radius as a potential allograft option for glenoid reconstruction. Based on our data and initial findings, we believe that this graft option has great potential for future clinical use. However, we recommend further biomechanical and clinical testing, which is in progress. We utilized calipers to assess the ROC of each sample. By utilizing these calipers, an assumption of each articular surface being a perfect sphere is made. In reality, there is some variance across each joint surface at different topographical locations. 10 To account for this variation, each reviewer took multiple measurements across different contact points for each sample and averaged them to give the data presented in this work. Furthermore, as noted by this study and previous work mentioned above, significant variation in allograft anatomy exists. We utilized 18 cadaveric specimens for this study based on the precedent set from previous literature. We used 1 donor source in North America; therefore, these averages may not be generalizable to all patient populations. Finally, the ages of the cadaveric specimens generally differed from those of the patient population that would benefit from this procedure. As such, the BMD results may not accurately represent the clinical situation.
Conclusion
Compared with the DTA, the DRA had a greater mean graft length in the SI plane, providing utilization in cases of larger bony defects; the DRA has a more acute ROC in the AP plane (closer to that of the glenoid), providing a greater potential buttress to anterior humeral translation. Compared with currently utilized grafts, the DRA BMD was not significantly diminished. This study presents the DRA as a novel allograft reconstruction option in the setting of anterior glenoid bone loss. However, further biomechanical and clinical investigation is recommended.
Footnotes
Submitted May 8, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Stryker Inc supplied financial support for performing the study without having any input on data analysis or manuscript preparation. A.Z.K. has received support for education from Arthrex, Medical Device Business Services, and Elite Orthopedics and hospitality payments from Stryker and Exactech. J.A.A. has received research support from Arthrex, Lima, Orthofix, Zimmer, and Department of Defense; consulting fees from Bioventus, DJ Orthopedics, Enovis, Globus Medical, Stryker, and Zimmer; royalties from DJ Orthopedics, Enovis, Globus Medical, OsteoCentric Technologies, Smith & Nephew, Stryker, and Zimmer; and publishing royalties from SLACK and Wolters Kluwer Health and Lippincott Williams & Wilkins. He is a board or committee member for Pacira, Orthobullets, and Shoulder 360 and holds stock or stock options in Aevumed, OBERD, Orthobullets, Atreon, OTS Medical, Restore 3D, and Shoulder JAM. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.