
Abstract
Background:
High tibial osteotomy (HTO) is a well-recognized procedure for its effectiveness in treating symptomatic early knee arthritis and malalignment. Although there are numerous systematic reviews evaluating the management and outcomes after HTO, there are few investigations on complications of this procedure.
Purpose:
To systematically review the literature to determine the incidence of intraoperative and postoperative complications associated with medial opening wedge and lateral closing wedge HTOs.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The Cochrane Database of Systematic Reviews, PubMed, Embase, and MEDLINE databases were queried for studies reporting complications associated with HTO with or without concomitant procedures. Data including patient characteristics, procedure type, concomitant procedures, follow-up time, and postoperative imaging were extracted. Rates of intra- and postoperative complications, reoperations, and conversion to arthroplasty were recorded.
Results:
A total of 71 studies were included for analysis, comprising 7836 patients. The overall intraoperative complication rate during HTO was 5.5% (range, 0%-29.3%), and the overall postoperative complication rate was 6.9% (range, 0%-26.6%). The most common intraoperative complication was lateral hinge fracture (incidence, 9.1%; range, 0%-30.4%) in medially based HTOs and peroneal nerve injury in laterally based HTOs (incidence, 3.2%; range, 0%-8.7%). The overall incidence of neurovascular injury after medially or laterally based HTOs was 1.1% (range, 0%-18.9%). The most common postoperative complication was superficial infection (incidence, 2.2%; range, 0%-13%). Of the included studies, 62 included postoperative radiographic analysis, and among those, the incidence of nonunion was 1.9% (range, 0%-15.5%), loss of correction was 1.2% (range, 0%-34.3%), and implant failure was 1.0% (range, 0%-10.2%). Among studies reporting revision surgeries, the overall reoperation rate was 15.5% (range, 0%-70.7%), with the most common type of reoperation being hardware removal (incidence, 10.0%; range, 0%-60%).
Conclusion:
Intraoperatively, medially based HTOs are associated with a 1 in 11 risk of lateral hinge fracture and laterally based HTOs with a 1 in 30 risk of peroneal nerve injury. Postoperative complication rates in the range of 10% to 15% can be expected, including infection (2.9%), loss of correction (1.2%), and nonunion (1.9%). Patients should also be counseled that the reoperation rate is approximately 15%, with hardware removal being the most common procedure.
Modulation of the weightbearing axis of the lower extremity through osteotomies of the proximal tibia is a viable technique used to treat isolated unicompartmental osteoarthritis of the knee in young, active patients.49,68 Further indications include patients with symptomatic malalignment (with or without co-concomitant cartilage or meniscal pathology) as well as those with ligamentous instability in which coronal, sagittal, or axial alignment correction can confer further stability and reduce stress on soft tissue reconstructions.49,68 The most common forms of high tibial osteotomy (HTO) include medially or laterally based wedge osteotomies.48,58 Dome osteotomies can also be used but are primarily reserved for multiplanar deformities.3,86 By correcting the mechanical axis of the lower extremities and transferring the force away from the affected compartment, HTO has the potential to relieve pain, improve function, and potentially modulate the natural history of joint degeneration.
Despite recent advances in technique and fixation, HTO is performed relatively infrequently in part because of specific patient selection criteria and because the surgical alternatives (unicondylar or total knee arthroplasty) are highly clinically successful.80,82 In addition, the procedure itself is technically challenging, poses a risk of complications, and necessitates a longer recovery time than arthroplasty alternatives.11,38,91 Complications specific to HTO include unintended propagation of the osteotomy into the tibial plateau or opposing metaphysis and peroneal nerve palsy. Other complications include nonunion of the osteotomy with or without implant failure, infection, and deep vein thrombosis. The overall incidence of these complications is difficult to discern from the current literature, as most studies are case series or cohort studies with a low number of patients. Although many reviews have focused on investigating the surgical techniques and outcomes of HTO, there is limited evidence in the literature specifically exploring the complications. This information is critical for both surgeons and patients to understand as the surgical indications for HTO continue to broaden as patient demands for joint-preserving techniques increase.
The purpose of this study was to systematically review the current literature to determine the incidence of intraoperative complications, postoperative complications, and reoperations associated with medial opening wedge and lateral closing wedge HTOs. We hypothesized that the rate of complications related to HTO is high given the complexity and relative infrequency of the procedure.
Methods
This study was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. The Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, PubMed, Embase, and MEDLINE were queried in April 2021 for literature reporting on HTO, either opening wedge or closing wedge with or without concomitant procedures. Database queries were performed using the following Boolean search terms: (“High tibial osteotomy” OR “Tibia osteotomy” OR “knee osteotomy”) AND (“outcomes” OR “complications”).
All studies, regardless of level of evidence, were included if they explicitly reported complications after an HTO with or without concomitant procedures. Articles were excluded if they did not explicitly report on the incidence and specific type of complication that occurred during or after the surgery or if the study was limited in scope and only reported on a single complication. Two investigators (V.C.B.R., R.N.P.) screened search results first by title, then by abstract, and last by full text. Further assessment of inclusion and exclusion criteria was applied to these full-text articles.
Relevant data from the studies, including publication information, level of evidence, population characteristics, type of surgery, concomitant procedures, radiographic evaluation, complications, and follow-up time, were extracted and recorded in a customized spreadsheet. Intraoperative complications, including lateral hinge fractures, popliteal artery injury, and peroneal nerve injury, were recorded. Lateral hinge fractures were defined by authors’ recognition (either intraoperatively or early postoperatively) of radiographically visible cortical disruption of the lateral proximal tibia (after medial opening wedge HTOs). 84 These fractures include extension of the osteotomy line within the proximal tibiofibular joint, propagation distal to the proximal tibiofibular joint, and propagation into the articular portion the proximal tibial plateau. 84 Postoperative complications, including superficial and deep infections, wound dehiscence, deep vein thrombosis, compartment syndrome, pain syndrome (defined as having pain for a prolonged period and/or to a higher degree than normal postoperative pain), range of motion deficit (defined as any report of failure to adequate return to baseline), nonunion, hematoma, implant failure, loss of correction, and revision fixation, were recorded. If other postoperative complications were reported, they were recorded as “miscellaneous other.” Hardware removal and conversion to total knee arthroplasty were also recorded but not included as “complications.” Although concomitant procedures and multiligament reconstructions were included, complications specifically attributed to these concomitant procedures by the authors of the original article were not included in this review.
The primary outcome measures were the rates of overall and specific types of complications. The rate of complication was calculated using weighted averages. Only studies that explicitly reported on the rate of reoperation or arthroplasty were used to determine the rates of these outcomes, as many studies may not be designed to assess such outcomes. In addition, only studies where postoperative radiographic analysis was performed were used to determine the rate of implant failure, nonunion, and loss of correction, each of which was defined by the authors of the respective studies. Forest plots were used to graphically compare the conversion to arthroplasty rates and effect sizes between studies. Study heterogeneity among those who reported conversion to arthroplasty rates was assessed using the I2 test. Statistical analysis was performed with R Project for Statistical Computing software (RStudio software, Version 4.1.2; R Foundation for Statistical Computing).
Results
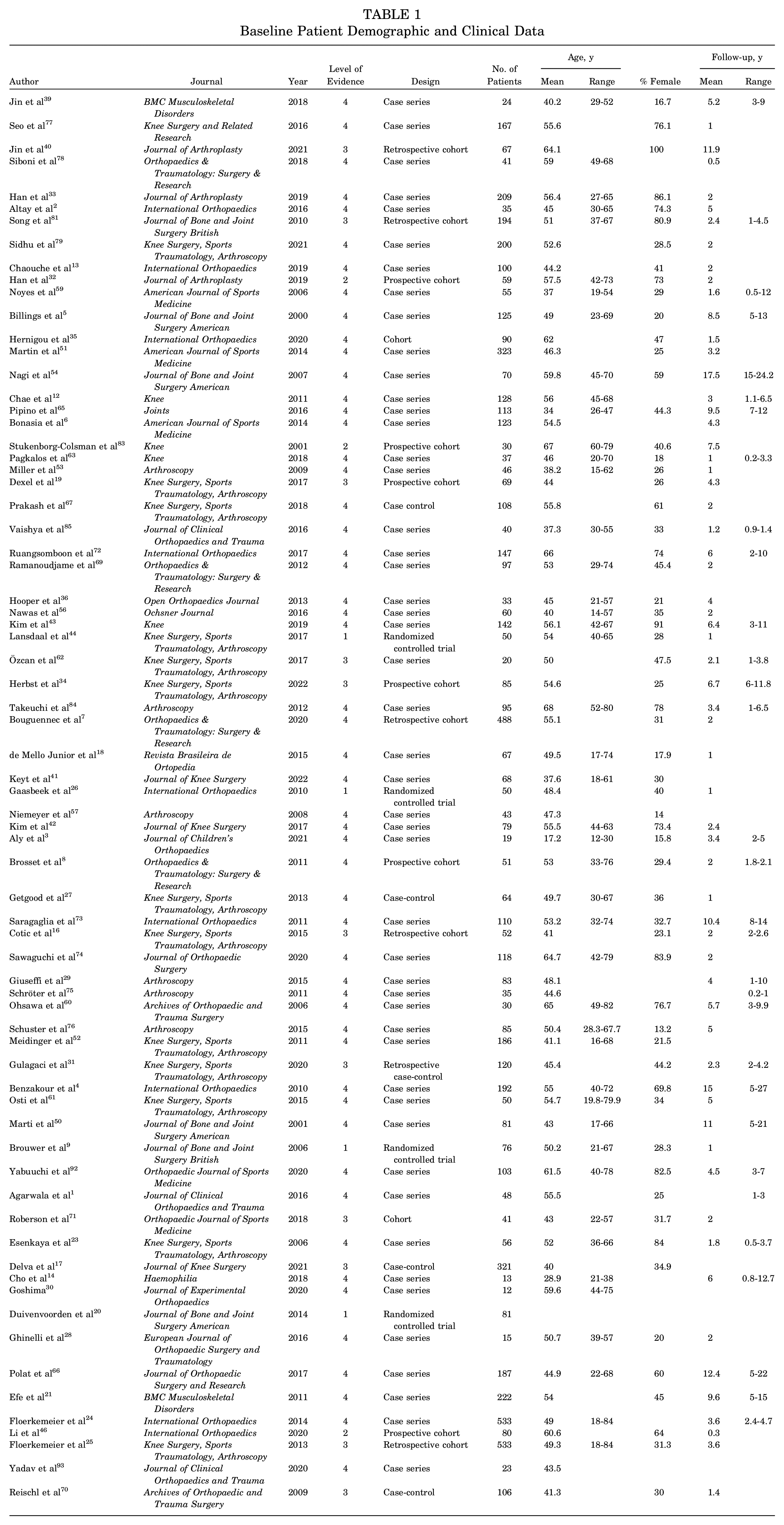
A total of 71 studies were identified for inclusion after database query. ∥ Study design, level of evidence, number of patients, sex, age, and follow-up were recorded and are presented in Table 1. The review included 7836 HTOs: 7337 medial opening wedge osteotomies and 499 lateral closing wedge osteotomies. The mean age of included patients was 50.4 ± 9.0 years, and 39.7% of patients were female. The average follow-up was 3.9 years (0.5-17.5 years). Forty nine of the included studies were cases series, 13 were cohort studies, 5 were case-control studies, and 4 were randomized controlled trials. Level of evidence ranged from Sackett 1 to 4. 10
Baseline Patient Demographic and Clinical Data
The overall intraoperative complication rate was 5.5% (range, 0%-29.3%) (Table 2). Intraoperative complications were seen in 5.6% of medial opening wedge osteotomies and 5.2% of lateral closing wedge osteotomies. The most common complication in medially based HTOs was lateral hinge fracture with an incidence of 9.1% (range, 0%-30.4%). There was a 1.1% incidence of neurovascular injury (range, 0%-18.9%) overall. The incidence of peroneal nerve injury after medial opening wedge HTO was 0.4% (range, 0%-12.7%), and the incidence of peroneal nerve injury after lateral closing wedge HTO was 3.2% (range, 0%-8.7%).
Rate of Individual Complications a
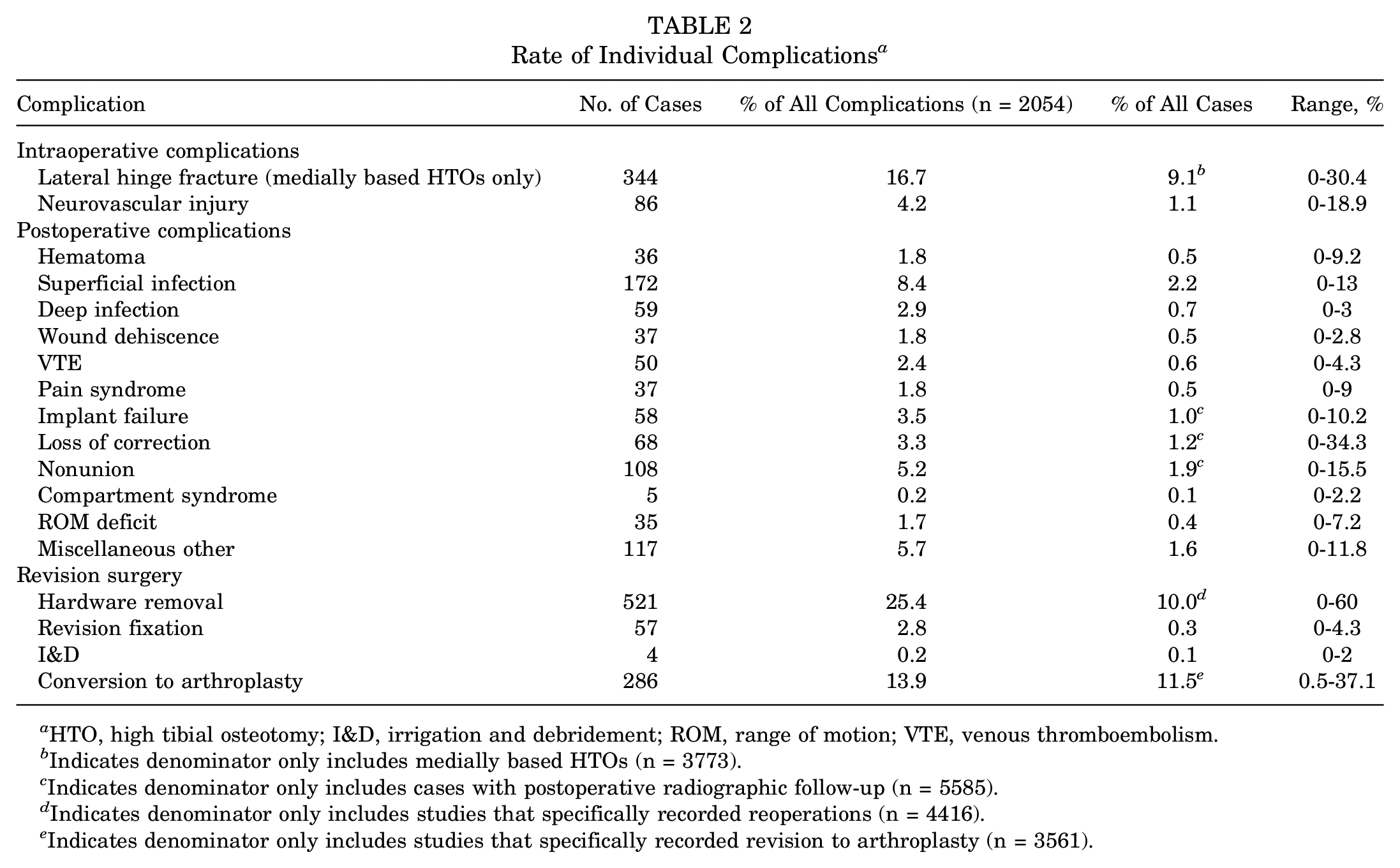
HTO, high tibial osteotomy; I&D, irrigation and debridement; ROM, range of motion; VTE, venous thromboembolism.
Indicates denominator only includes medially based HTOs (n = 3773).
Indicates denominator only includes cases with postoperative radiographic follow-up (n = 5585).
Indicates denominator only includes studies that specifically recorded reoperations (n = 4416).
Indicates denominator only includes studies that specifically recorded revision to arthroplasty (n = 3561).
The postoperative complication rate (not including nonunion, loss of correction, or implant failure) was 6.9% (range, 0%-26.6%). The rate of postoperative complications was 6.6% (range, 0%-36.7%) in medial opening wedge osteotomy and 7.0% (range, 0%-47.8%) in lateral closing wedge osteotomy. Superficial infections were more common than deep infections (2.2% [range, 0%-13%] vs 0.7% [range, 0%-3%]). Pain syndrome had an incidence of 0.5% (range, 0%-9%) and range of motion deficit had an incidence of 0.4% (range, 0%-7.2%). Other complications included postoperative hematoma (0.5%; range, 0%-9.2%), wound dehiscence (0.5%; range, 0%-2.8%), revision fixation (0.3%; range, 0%-4.3%), and venous thromboembolism (0.6%; range, 0%-4.3%). The overall incidence of compartment syndrome was 0.1% (range, 0%-2.2%). Miscellaneous other complications were seen with an incidence of 1.6% (range, 0%-11.8%).
Sixty-two of the included studies reported on postoperative radiographic follow-up, which included 5585 cases. The average follow-up was 3.8 years (range, 0.5-17.5 years). The total incidence of nonunion was 1.9% (range, 0%-15.5%). The incidence of nonunion was 1.7% (range, 0%-12.2%) for medial opening wedge osteotomy and 4.1% (range, 0%-15.5%) for lateral closing wedge osteotomy. The total incidence of loss of correction was 1.2% (range, 0%-34.3%). The incidence of loss of correction was 1.2% (range, 0%-34.3%) for medial opening wedge osteotomy and 0.5% (range, 0%-1.9%) for lateral closing wedge osteotomy. The incidence of implant failure was 1.0% (range, 0%-10.2%). The incidence of implant failure was 1.1% (range, 0%-10.2%) for medial opening wedge osteotomy and was 0.2% (range, 0%-1.0%) for lateral closing wedge osteotomy. When accounting for nonunion, loss of correction, and implant failure, the cumulative incidence of all postoperative complications was 11.4%.
Thirty-five studies specifically recorded reoperations and included 4416 cases (4274 medial opening wedge osteotomies and 142 lateral closing wedge osteotomies). Among these studies, the overall reoperation rate was 15.5% (range, 0%-70.7%). The rate of reoperation was 15.1% (range, 0%-70.7%) for medial opening wedge osteotomy and 25.1% (range, 0%-82.2%) for lateral closing wedge osteotomy. The most common type of reoperation was hardware removal, with a rate of 10.0% (range, 0%-60%). Hardware removal was seen at a rate of 9.7% (range, 0%-54.5%) after medial opening wedge osteotomy and 19.0% (range, 0%-60%) after lateral closing wedge osteotomy.
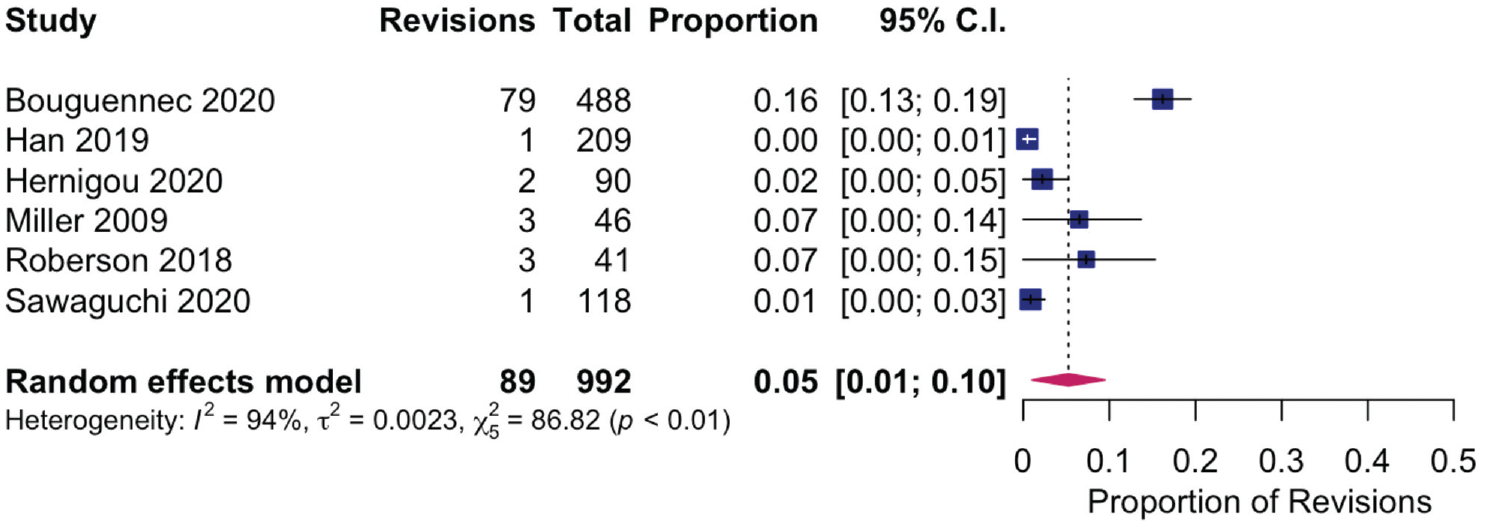
Thirty-one studies specifically recorded revision to arthroplasty (total knee arthroplasty or unicompartmental arthroplasty) and included 3561 cases. The average follow-up among these was 5.2 years (range, 1-17.5 years). The rate of revision arthroplasty in this subgroup was 11.5% (range, 0.5%-37.1%). The incidence of conversion to arthroplasty was 9.9% (range, 0%-33.3%) in opening wedge HTO and 24.4% (range, 0%-32.8%) in closing wedge HTO. Studies explicitly mentioning subsequent arthroplasty were included in an assessment of heterogeneity comparing the rate of conversion of arthroplasty after HTO (Figure 1).
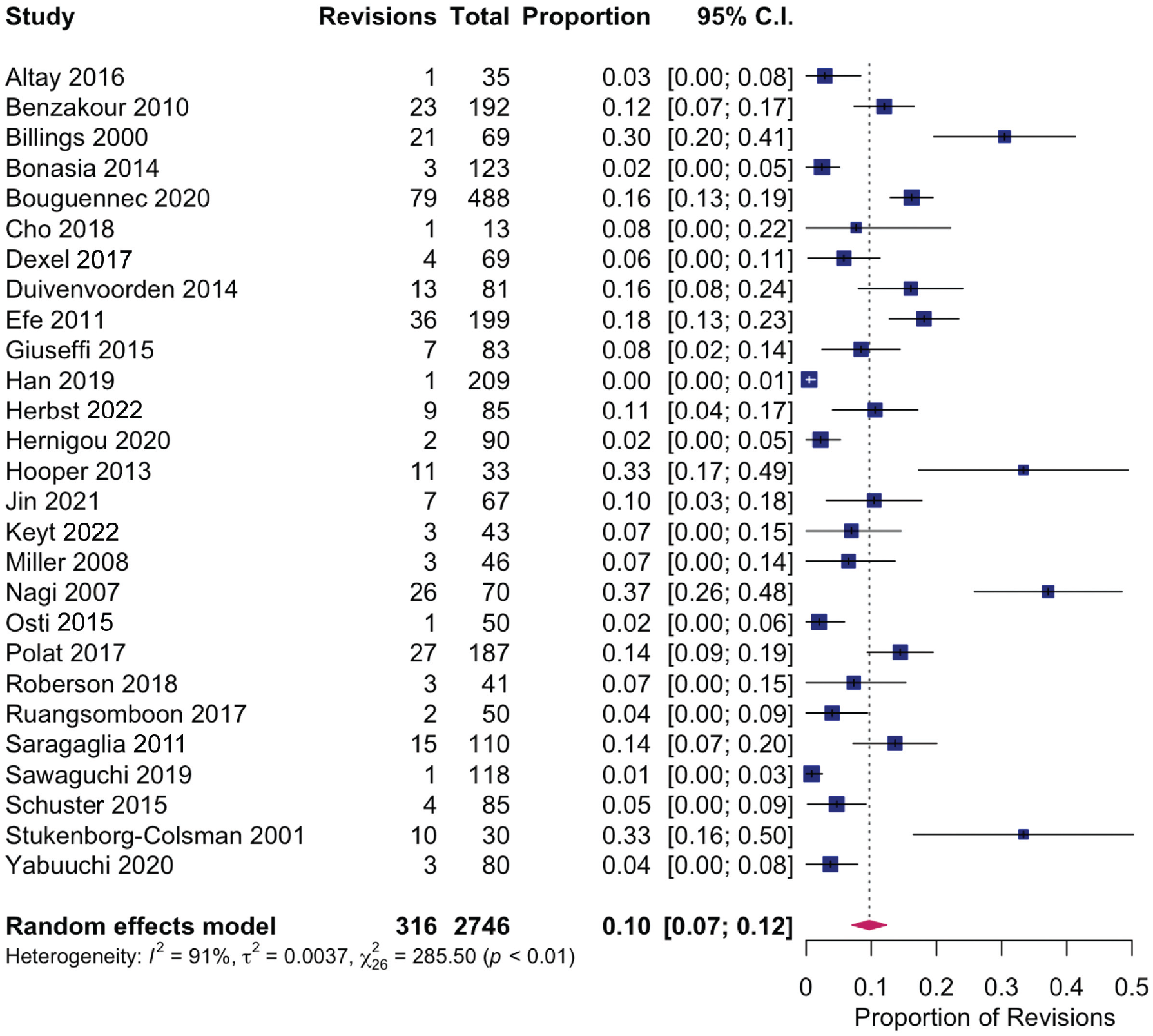
Assessment of heterogeneity for the rate of conversion to arthroplasty after high tibial osteotomy.
Effect sizes varied significantly among the included studies (0.0%-37.1%), leading to a high degree of heterogeneity (I2 = 90.9%). Studies were stratified based on average time of final follow-up >2 years or ≤2 years. There were 21 studies with a follow-up >2 years. In these studies, conversion rate was 2% to 37.1% (I2 = 84.4%) (Figure 2). There were 6 studies with a follow-up of ≤2 years. In these studies, conversion rate was 0.0% to 7.3% (I2 = 94.2%) (Figure 3).
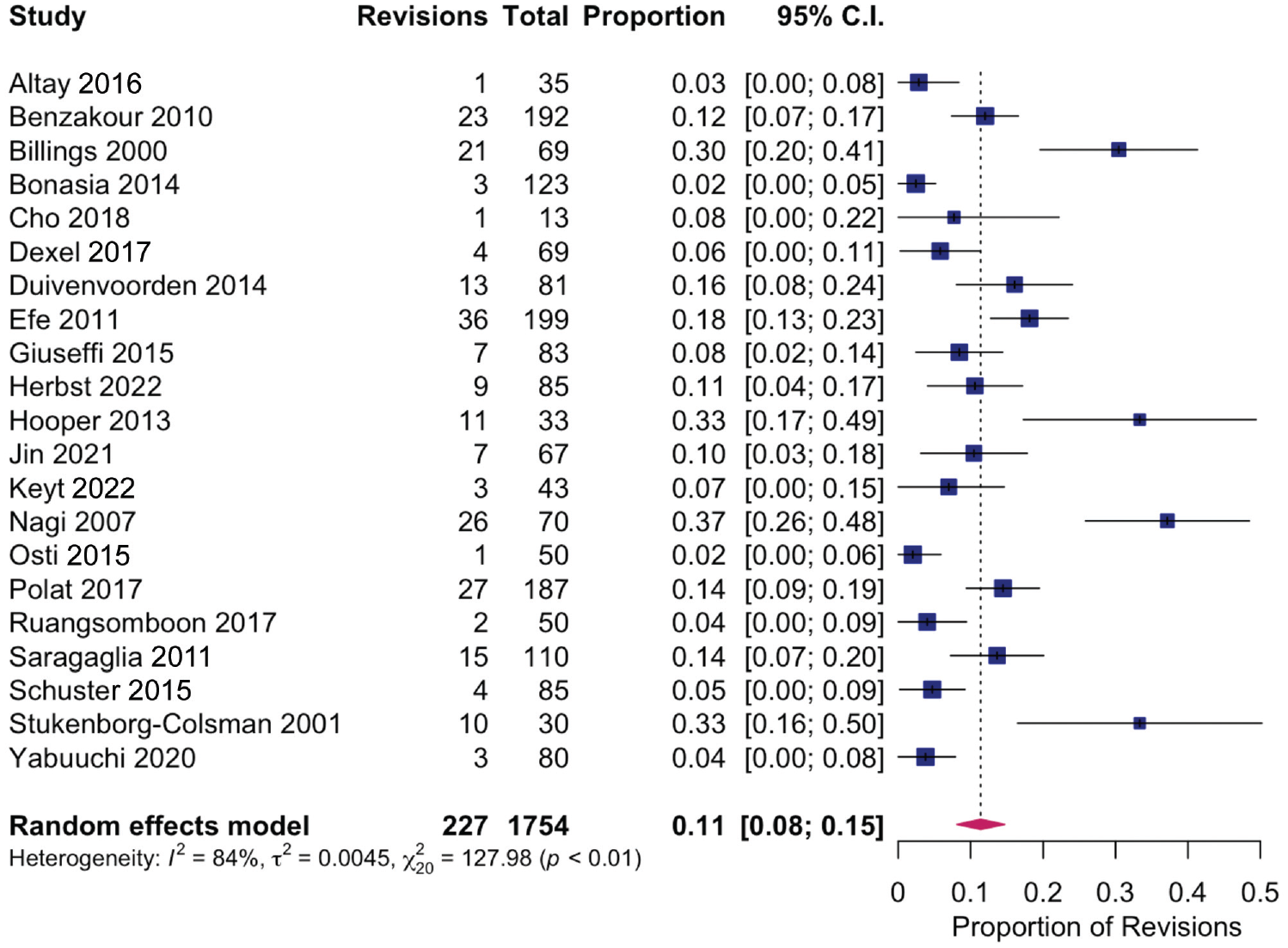
Assessment of heterogeneity for conversion to arthroplasty after high tibial osteotomy in studies with >2 years of follow-up.
Assessment of heterogeneity for conversion to arthroplasty after high tibial osteotomy in studies with ≤2 years of follow-up.
Discussion
In this review, we report an intraoperative complication rate of 5.5% and a postoperative complication rate of 11.4% after HTO. The most common intraoperative complication was lateral hinge fracture in medially based HTOs (9.1%) and peroneal nerve injury in laterally based HTOs (3.2%). The most common postoperative complications were infection (2.9%) and nonunion (1.9%). Nonunion was more commonly seen in lateral closing wedge osteotomies (4.1%) than in medial opening wedge osteotomies (1.7%). Reoperation was common. In studies explicitly reporting reoperation, there was an overall reoperation rate of 15.5%, with hardware removal being the leading cause of reoperation. In studies explicitly mentioning arthroplasty, the rate of conversion to arthroplasty was 11.5%.
Lateral hinge fractures occurred commonly in medial-based osteotomies (9.1% of cases). In fact, lateral hinge fractures were the most common complication overall, representing 16.7% of all complications seen in the included studies. Lateral hinge fractures may lead to worse outcomes, as they can cause increased micromotion at the osteotomy site or even result in gross instability of the proximal tibia. 15 This may predispose the patient to loss of correction, overcorrection, and/or nonunion of the osteotomy and thus may change rehabilitation protocols or necessitate additional lateral stabilization. However, it must be noted that not all lateral hinge fractures destabilize the osteotomy, and there is debate about which of these fractures do create increased instability. 55 Regardless, many studies have looked into the predictive factors for lateral hinge fracture.15,32,45,55 Perhaps intuitively, the most consistent risk factor for lateral hinge fracture is an increased opening distance of the osteotomy. 15 Technical steps to minimize the risk of this complication, especially during high correction angles, are critical for successful patient outcomes and avoiding revision surgery.
Other intraoperative complications were less common. The rate of neurovascular injury was low (1.1%). This is similar to rates previously reported by Woodacre et al. 90 Of the neurovascular complications seen, there were only 2 reported cases of injury to the popliteal artery, both of which required repair by a vascular surgeon with an autologous vascular graft.12,65 Peroneal nerve injury had a higher incidence after lateral closing wedge HTO (3.2%) than medial opening wedge HTO (0.4%). Kim et al 43 specifically studied lateral lower leg numbness after medial opening wedge HTO and reported a rate of 51.5% of lateral numbness at 6 weeks postoperatively and 12.7% at final follow-up, which is attributed to injury to the infrapatellar branch of the saphenous nerve during a medial-based osteotomy. We did not pick up this rate of sensory disturbances in our study, which may be explained by an underreporting of lateral leg numbness due to the tolerability and often transient nature of the symptoms. Considering the findings of Kim et al, 43 it may be reasonable to assume that transient paresthesia or neurapraxia is more common than we saw in our review and may be an underreported complication that should be discussed with patients preoperatively.
Postoperative complications were frequent, with an incidence of 11.4% overall. Infection was the most common postoperative complication, with an incidence of 2.9%. Notably, most of these were superficial infections (2.2%). Deep infections were seen in <1% of all cases (0.7%), although it should be noted there was no standard definition of what constituted a deep (vs superficial) infection. Risk factors for postoperative infection after HTO have been shown to be largely the same factors for surgical-site infection commonly reported in orthopaedic procedures—namely, smoking, older age, and diabetes mellitus.47,70 Use of an oblique incision over a vertical incision has also been shown to be associated with a higher postoperative infection rate. 68 The overall modest deep infection rate identified could be the result of the fact that HTOs are often performed in younger healthy individuals compared with arthroplasty counterparts. Regardless, in the context of identifiable risk factors, careful patient selection is critical.
Following infection, nonunion was the next most common postoperative complication, with an incidence of 1.9% among the 62 studies that specifically documented postoperative imaging. Patient factors such as tobacco use and diabetes mellitus have been associated with an increased risk of nonunion after HTO.87,92 Numerous studies have also found a correlation between body mass index and the rate of nonunion.52,69,78 van Houten et al 87 found that using the Radiographic Union Score for Tibial Fractures score at 6 weeks and 3 months after surgery can be used to predict nonunion after HTO, analogous to its accepted use in tibial fractures. Importantly, there is some controversy about whether medial opening wedge osteotomy is associated with a higher rate of nonunion than lateral closing wedge osteotomy. Some reports suggest that medial opening wedge osteotomy has a higher rate of nonunion than lateral closing wedge osteotomy and several more modern studies have called this finding into question.8,22,52,86,89 Consistent with the later studies, our review saw only minor differences in rates of nonunion, which most likely are not clinically significant. Unfortunately, a true statistical analysis of this difference could not be explored because of the baseline heterogeneity of methods between studies. Despite minimal difference in the rates of nonunion between medial opening wedge and lateral closing wedge osteotomy, 48% of surgeons report increased rate of nonunion as a potential drawback to medial opening wedge HTO, highlighting the need for information on this complication. 89
The incidence of reoperation among studies reporting this complication was 15.5%. The most common cause of reoperation was hardware removal, with an incidence of 10%. Revision to arthroplasty was seen in 11.5% of cases in studies specifically reporting on rates of revision arthroplasty. There was significant heterogeneity in the rate of conversion to arthroplasty across studies (I2 = 90.9%). Notably, there was significant variation in the follow-up time of the studies reviewed in this review, and when analysis was performed to account for these different rates of follow-up, heterogeneity was decreased (ie, there was greater agreement between studies). This may indicate that the rate of revision arthroplasty reported is artificially low given that long-term studies have shown the clinical success of HTO decreases over time, and significant deterioration in function after HTO ultimately may lead to arthroplasty. Survival data show that more than half of HTOs done for medial-based joint degeneration remain effective at 7 to 10 years, which leads to the argument that HTO may be beneficial for patients with early-onset medial compartment knee osteoarthritis, whose young age puts them at risk for exceeding the life span of a total knee arthroplasty if they did not have a procedure to delay arthroplasty.37,64,88 Ultimately, our study confirms that HTO has significant revision rates, but the survival of HTOs, using conversion to arthroplasty as an endpoint, is out of the scope of this review. Nonetheless, in the context of previous literature, HTO may successfully postpone arthroplasty for several years in appropriately selected candidates, and more research is needed to better understand these timelines and risks for early failure.
This review’s findings must be taken in the context of its limitations. Of the 71 studies included, 50 were case series and only 4 were randomized controlled trials. This highlights the need for higher-quality studies on complications, reoperations, and revisions after HTO. Given the high proportion of retrospective cases series, selection bias may have influenced some of the results. The studies included were limited by their sample size. We were unable to perform a meta-analysis because of the lack of homogeneity, and thus a systematic review was the best method to synthesize the current literature. In addition, we saw significant heterogeneity in study methodology, study hypothesis, and outcome reporting across the studies, making critical review of the data challenging. Moreover, the heterogeneous nature of the hypotheses of the studies makes it possible that the number of reported complications is artificially deflated because not every complication experienced was reported in every study. To address this, we performed subgroup analysis on major complications to analyze studies specifically reporting on each given complication.
Conclusion
Intraoperatively, medially based HTOs are associated with a 1 in 11 risk of lateral hinge fracture and laterally based HTOs with a 1 in 30 risk of peroneal nerve injury. Postoperative complication rates in the range of 10% to 15% can be expected, including infection (2.9%), loss of correction (1.2%), and nonunion (1.9%). Patients should also be counseled that the reoperation rate is approximately 15%, with hardware removal being the most common procedure.
Footnotes
Submitted June 16, 2022; accepted October 17, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.E.M. has received consulting fees from Arthrex and hospitality payments from Encore Medical, Medical Device Business Services, and Smith & Nephew. S.P.R. has received consulting fees from Globus Medical and Medical Device Business Services, speaking fees from Synthes GmbH, and royalties from Globus Medical. J.D. has received grants from Arthrex and Acumed; support for education from Arthrex, Smith & Nephew, and Synthes; and consulting fees from DJO. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.