
Abstract
Background:
Having simple and reliable validated outcome measures is vital to conducting high-quality outcomes research in the field of orthopaedic surgery. Activity level is a key prognostic variable for patients with sports injuries. There is a paucity of such activity scales for children and adolescents who are otherwise healthy and athletically active. In addition to frequency and intensity of athletic activity, level of play and coach/trainer supervision are important variables unique to children and adolescents that are not captured in available adult scoring systems.
Purpose:
To create and validate a concise and comprehensive activity rating scale for athletically active children and adolescents 10 to 18 years of age.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
Item generation was performed with a panel of orthopaedic surgeons and adolescent athletes. Item reduction, pilot testing and scale refinement resulted in a final 8-item instrument, the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS). Existing methods were used to determine reliability and validation. The Flesch-Kincaid score was calculated at a 6.6th-grade reading level (approximately 13 years old); therefore, although all subjects provided their own answers, parents were allowed to assist children younger than 13 years with reading the questionnaire.
Results:
Scale reliability was excellent (test-retest reliability, intraclass correlation coefficient = 0.91; internal consistency, Cronbach alpha = .914), and there were no floor or ceiling effects. There was also robust construct validity: Convergent validity testing revealed positive correlations between the HSS Pedi-FABS and level of competition in athletic activity, number of reported hours of athletic activity per week, and existing comparable adult and pediatric scales. Discriminant validity was shown with age, body mass index, and type of sport as measured by the Daniel scale.
Conclusion:
The 8-item HSS Pedi-FABS can be used to reliably and accurately evaluate activity level as a prognostic variable for clinical research studies. It is a simple, reliable, and valid metric to assess activity in children and adolescents 10 to 18 years of age. This instrument will lead to better evaluation of posttreatment outcomes and patient-reported activity for child and adolescent athletes.
More than 30 million children in the United States participate in organized sports programs, 1 and more than 3.5 million children age 14 and younger receive medical treatment for sports injuries each year. 54 Treatment algorithms for these children are largely developed by use of results from clinical outcomes research evaluating the effect of an intervention on recovery from injury. Activity level is known to be a key prognostic variable for active patients with musculoskeletal injuries. ¶ Therefore, having reliable, validated, and simple activity level measures is vital to conducting high-quality outcomes research in the fields of orthopaedic surgery, sports medicine, and rehabilitation.
Within the realm of pediatric orthopaedic surgery, existing rating scales are largely geared toward children with marked disability (eg, the Gross Motor Function Classification System for use in children with cerebral palsy). 51 The few scales that do measure a broader range of functional activity are long, time consuming, and specific to activity, sport, and/or joint.26,33 Lengthy global activity measurements may lead to questionnaire fatigue, 6 and activity-specific questionnaires may incorporate cultural and regional biases,44,62 thus decreasing their global validity. In the adult literature, multiple joint-specific upper extremity, # lower extremity, ** and quality of life41,47,48,61,65-67 functional metrics are currently used; however, many items in these instruments do not pertain to children.
Because the existing sport activity scales were developed for adults and may lack specificity for children, a child- and adolescent-specific activity scale is critically needed (1) to enable objective assessment of activity level in children and (2) to provide a prognostic variable for outcomes research within the field of pediatric sports medicine. The goal of this study is to develop and validate an activity rating scale for active children and adolescents aged 10 to 18 for use in clinical research.
Materials and Methods
This study was approved by the hospital institutional review board, and consent or refusal did not affect patient care in any way.
In preparation for item generation and scale validation, a formal search of PubMed and Ovid/Medline was performed to locate any existing pediatric or adolescent activity scales. A search strategy was used that included the following terms and Boolean operators: “(activity OR scale OR questionnaire OR outcome) AND (pediatric OR adolescent).” Additionally, medical subject headings (MeSH terms) were included in the search to include hierarchically organized search terms. For example, this search included the term “outcome scale,” which in turn includes 10 subject headings such as “outcome assessment,” “outcome studies,” “outcomes research,” and “patient outcomes.” Further, 2 recently published systematic reviews evaluating existing patient-reported outcome measures in orthopaedic surgery were evaluated.56,57 After joint- and sport-specific scales were eliminated, as well as scales targeted at children with disabilities, only the Physical Activity Questionnaire for Older Children (PAQ-C) and Physical Activity Questionnaire for Adolescents (PAQ-A) remained.
Four groups of patients were used in completion of this study, all of whom met inclusion criteria of our target cohort: healthy active adolescents 10 to 18 years old. These 4 groups consisted of the item generation group (n = 20), the item reduction group (n = 20), the pilot testing/interview group (n = 20), and the validation group (n = 51). Sports played by each participant group are listed in Table 1.
Sports Participation by Each Group of Included Subjects a
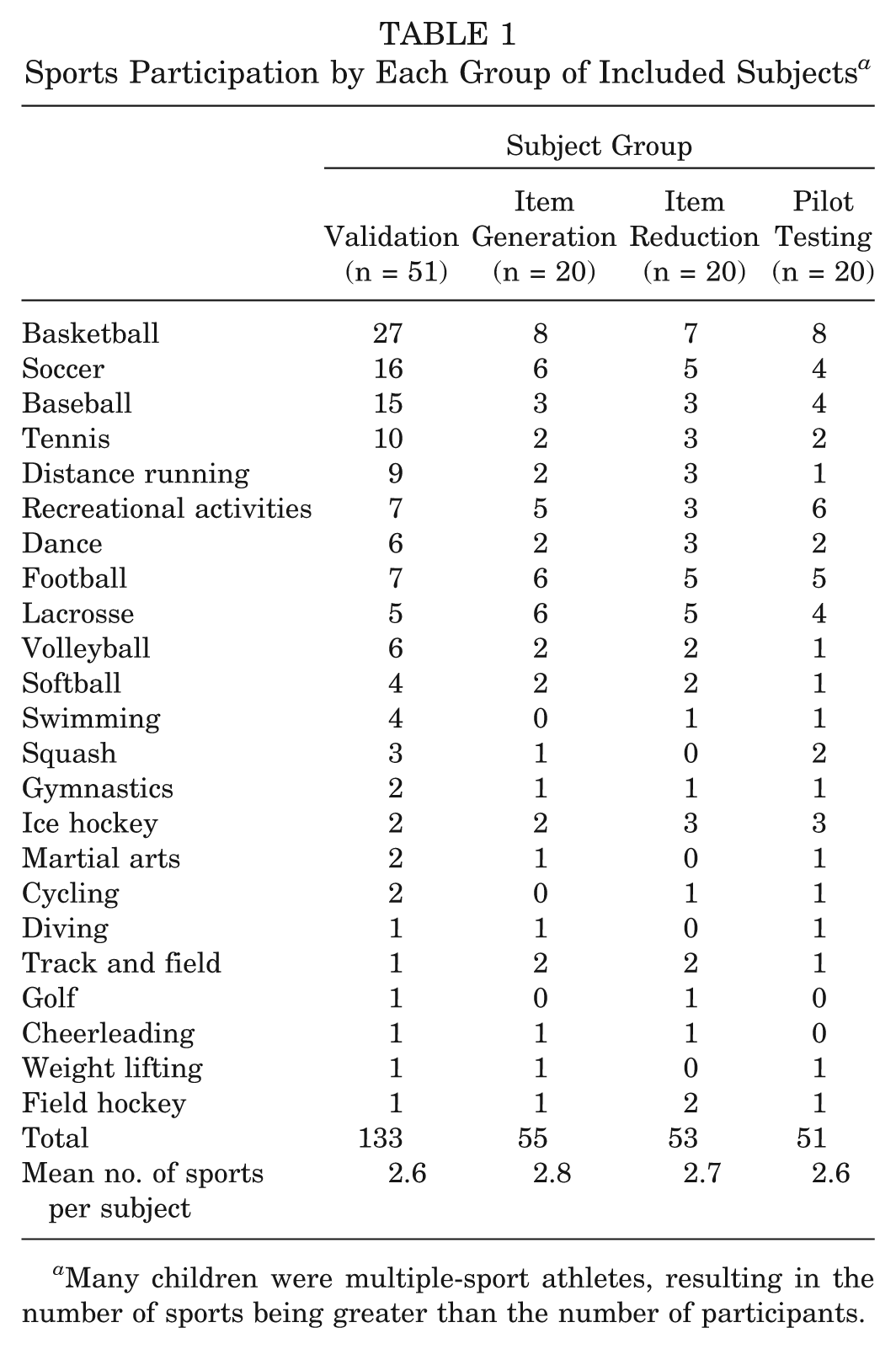
Many children were multiple-sport athletes, resulting in the number of sports being greater than the number of participants.
Item Generation
To identify relevant items for inclusion in the scale, a panel of fellowship-trained orthopaedic surgeons (2 pediatric, 1 sports medicine) were consulted to generate a list of items, and the aforementioned validated scales were reviewed for potentially relevant items. Because the scale was intended for patients aged 10 to 18, twenty adolescent athletes 10 to 18 years old (the item generation group) were also separately surveyed to determine what activity items were important to them; surveys continued until no new responses were generated. These children and adolescents (10 male and 10 female participants; mean age, 14.8 ± 1.8 years) were varsity and junior varsity athletes at area junior high and high schools. Their sports participation is shown in Table 1. Items identified by the surgeons and the subjects were compiled into a list of 13 items after duplicates were eliminated.
Item Reduction
A separate cohort of 20 active children and adolescents (the item reduction group) ages 10 to 18 was asked to score the importance and frequency of each item on a 10-point scale. These children and adolescents (10 male and 10 female participants; mean age, 14.9 ± 2.1 years) were varsity and junior varsity athletes at area junior high and high schools. Their sports participation is shown in Table 1. These scores were summed, averaged, and ranked to select items having the greatest clinical relevance to the population of interest. 43 Running, cutting, decelerating, and pivoting were each independently identified as a highly relevant item, in addition to 4 items measuring duration, endurance, supervision, and level of competition, leaving a total of 8 items. The original clinicians involved in the original item generation evaluated clinical sensibility after item reduction to ensure that the final item set was relevant to both practitioners and subjects. 19
Several design and scoring schemata were considered. A multi-item scale was deemed to be most appropriate to eliminate concerns surrounding validity of hierarchically ranked scoring systems. 68 A concise 8-item Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) was created with a goal of facilitating rapid completion to minimize patient burden. The instructions specifically ask the subject about activity during a 1-month window so that the instrument is stable in the face of day-to-day variation in activity but sensitive enough to monitor change over time. Further, 1-month reporting minimizes the chances of underestimation of activity level in the event that a child misses 1 week of organized athletic activity because of school or family vacation.
Pilot Testing
The HSS Pedi-FABS was pilot tested through pilot questionnaire administration and a series of interviews in a separate cohort of 20 children (the pilot testing group) to solicit feedback regarding item understanding, language, wording, layout, and ease of completion. This allowed for the identification of potential sources of error that may decrease reliability and validity of the scale, and it was performed in children and adolescents (10 male and 10 female; mean age, 14.7 ± 1.9 years old) who were varsity and junior varsity athletes at area junior high and high schools. Their sports participation is shown in Table 1. After we modified the language, layout, and formatting using the pilot testing results to ensure understanding and ease of use, the HSS Pedi-FABS was finalized when no further ambiguity remained (Figure 1; see Appendix 1, available online at http://ajsm.sagepub.com/supplemental). The Flesch-Kincaid score 27 of the final instrument was calculated at a 6.6th-grade reading level (approximately 13 years old). All subjects provided their own answers; however, parents were allowed to assist children who were younger than 13 years with reading the questionnaires, if necessary.
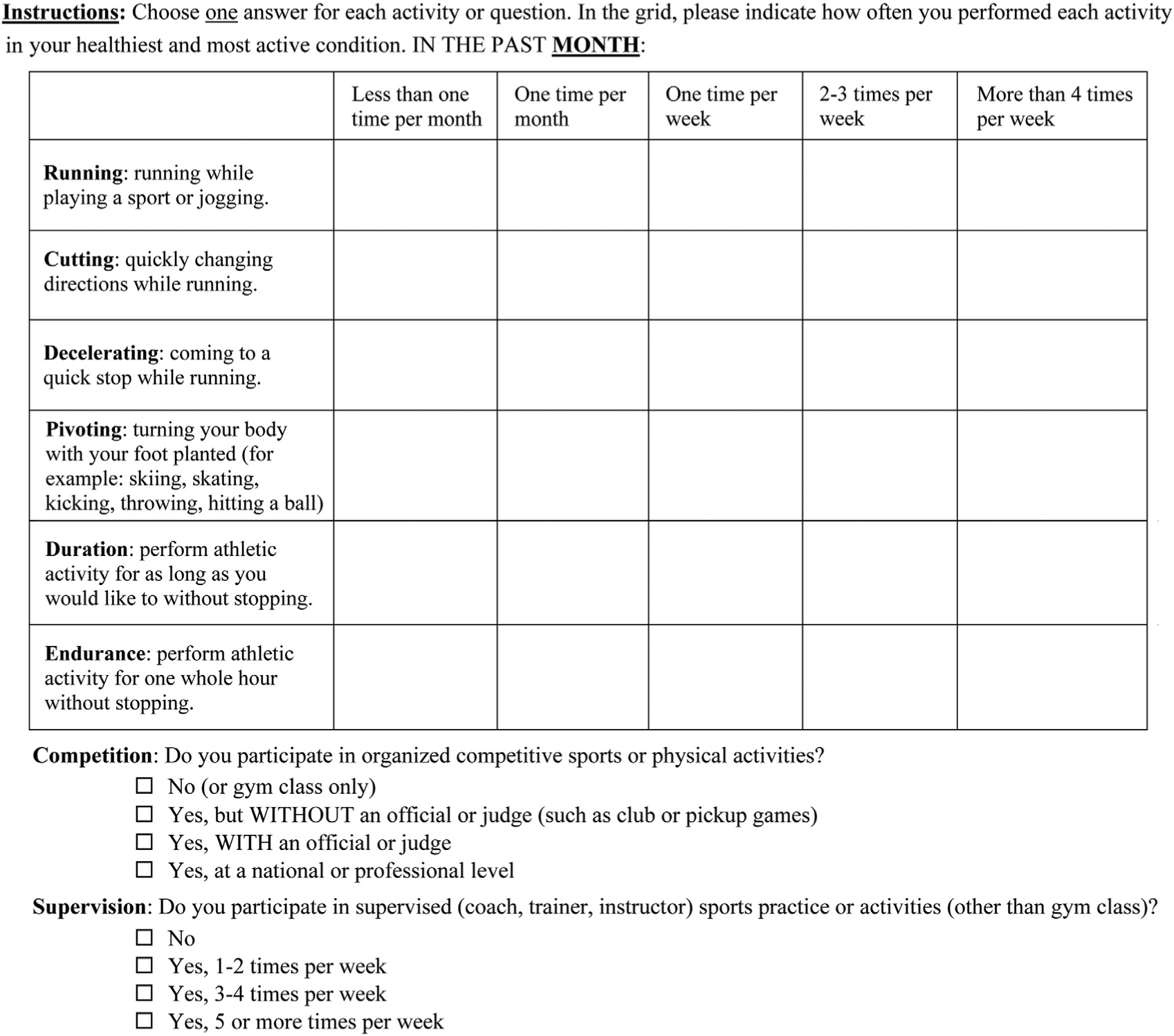
The Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS). Scoring is performed by adding points from each question for total possible score range from 0 to 30 points. For questions regarding running, cutting, decelerating, pivoting, duration, and endurance, each question is worth 0, 1, 2, 3, or 4 points. For the questions about competition and supervision, each question is worth 0, 1, 2, or 3 points. A scoring legend is shown in Appendix 1, available online.
Validation
A total of 51 English-speaking children ages 10 to 18 years who were healthy (no chronic disease or active health condition other than seasonal allergies) and were involved in at least 1 organized athletic or physical activity (school and/or community based) were evaluated (the validation group). Subjects recruited were patients from the pediatric orthopaedic clinic who were seen for minor complaints as well as healthy children who were also present in the waiting room (eg, patients’ friends and siblings). Parental consent was obtained for children younger than 18 years in addition to subject assent.
Construct validity was assessed through evaluation of the HSS Pedi-FABS for both convergent and discriminant validity by use of widely accepted methods.14,60 In this process, existing scales and demographic variables were considered a priori for either convergent or discriminant validity testing. Convergent validity was evaluated by comparing scores on the HSS Pedi-FABS to existing adult outcome measures in the orthopaedic sports literature (Tegner, Marx, Noyes)44,50,62 and the Pediatric Activity Questionnaire (PAQ-A or PAQ-C based on child’s age). 26 Although the adult scales are not validated in children specifically, they are helpful in providing construct validity by comparing scores with the HSS Pedi-FABS through regression analysis.9,11,14,60 As a further assessment of convergent validity, HSS Pedi-FABS scores were compared with subject-reported and parent-confirmed highest level of competition and hours of organized athletic activity per week currently and in peak athletic season.
Discriminant (divergent) validity was assessed between the HSS Pedi-FABS and those variables that were hypothesized a priori to lack any significant correlation. In active children, these included age and body mass index (BMI). Linear regression modeling was used for these analyses. The Daniel scale, 12 a 3-point scale that analyzes only the type of sport played and does not account for level of participation, frequency, or multiple sports, was also used for discriminant validity testing. It was hypothesized not to correlate with a scale designed to measure activity level, particularly in children and adolescents in whom type of sport may not be as meaningful as in adults. Construct validity is ensured in the event that there are significant correlations between the HSS Pedi-FABS and those measures of convergent validity, and there is an absence of significant correlation with those variables tested for discriminant validity,9,11,14,60 for at least 75% of the tested hypotheses in at least 50 subjects. 63
Face validity of the final HSS Pedi-FABS was ensured by clinicians before initiation of the validation phase. Criterion validity could not be evaluated because there is currently no accepted reference standard measurement tool for pediatric sport activity level quantification.
Reliability
Reliability of the HSS Pedi-FABS was evaluated using 2 complementary methods: test-retest reliability and internal consistency. Sample size calculation in previous methods indicated that at least 40 subjects are required for reliability testing. 16 All 51 subjects who participated in the validation phase (the validation group) were included in internal consistency reliability testing. At a predetermined interval after first completion, these subjects were contacted and completed the HSS Pedi-FABS again.3,15 Additionally, they were asked whether their condition had changed in any way. Those who replied “no change” (41 subjects) were included in the final test-retest reliability analysis.
Readability
Readability of the HSS Pedi-FABS was assessed by use of Flesch-Kincaid grade level analysis. 27
Floor and Ceiling Effects
Scales that yield continuous scores were assessed for floor and ceiling effects. A floor or ceiling effect was considered to be present if more than 15% of respondents scored the lowest or highest possible score, respectively.46,63
Statistical Methods
Statistical analyses were performed by members of the research team with advanced training in epidemiology and biostatistics using SAS Software version 9.2 (SAS Institute, Inc, Cary, North Carolina). Sample size was derived from previously validated methods.16,44 Spearman rank correlations were calculated to evaluate associations between the HSS Pedi-FABS and the Tegner, Marx, Noyes, and PAQ. In analysis of the Daniel scale, which is a 3-point categorization score, the Kruskal-Wallis test was used. Test-retest reliability was assessed with the intraclass correlation coefficient (ICC) (2,1). Internal consistency was evaluated with Cronbach alpha. All analyses were 2-tailed and used P = .05 as the threshold for statistical significance.
Results
Organized sports participation (Table 1) and demographic characteristics of the validation group (Table 2) were recorded. Subjects included 32 children age 10 to 18 (mean age, 14.4 ± 2.0 years) who presented to a pediatric orthopaedic surgeon with a minor complaint that they reported did not affect their activity level: mild hip pain (n = 2), scoliosis screening with curves less than 20° (n = 7), mild back pain (n = 5), healthy during follow-up visit (n = 5), mild foot/ankle pain (n = 3), mild knee pain (n = 5), tendonitis (n = 1), and minor small bone fracture (eg, phalanges) (n = 4). An additional 19 healthy friends or relatives who accompanied the patients in the waiting room were included in the study as well. Item and total scores on the HSS Pedi-FABS are displayed in Table 3. Overall score distribution on the HSS Pedi-FABS is displayed in Figure 2.
Demographic and Activity Responses for the Validation Group (n = 51) a
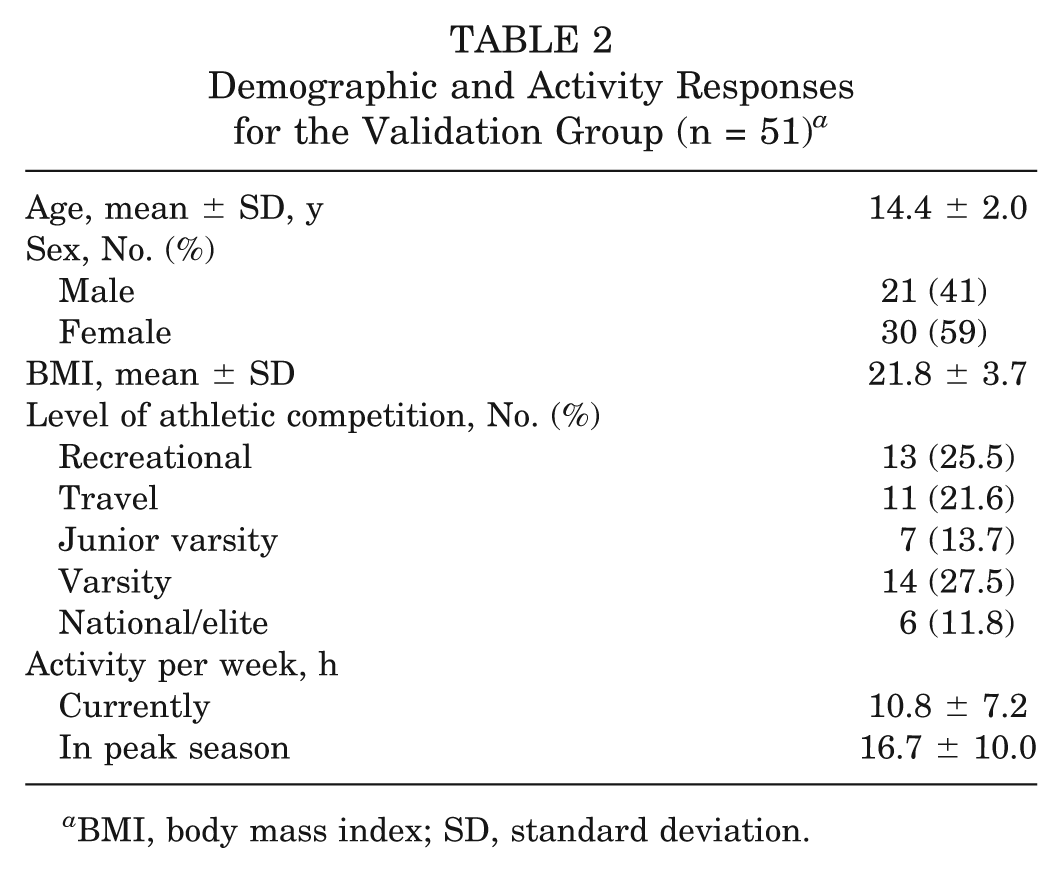
BMI, body mass index; SD, standard deviation.
Item Responses for the HSS Pedi-FABS in the Validation Group (n = 51) a
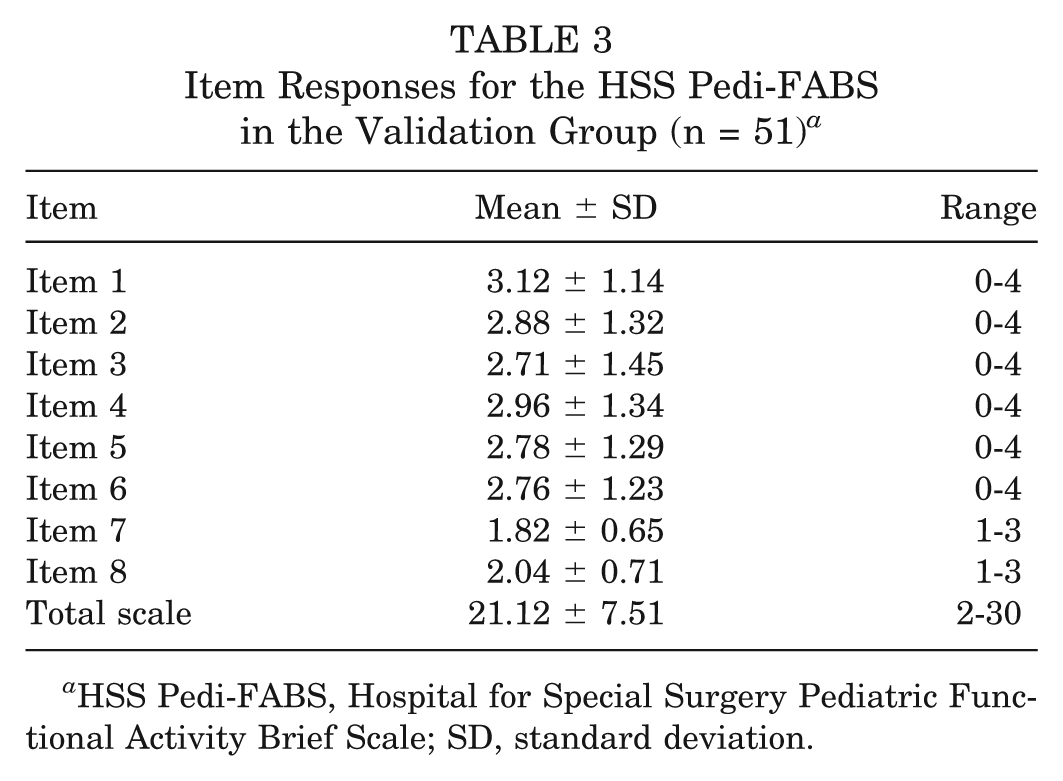
HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale; SD, standard deviation.
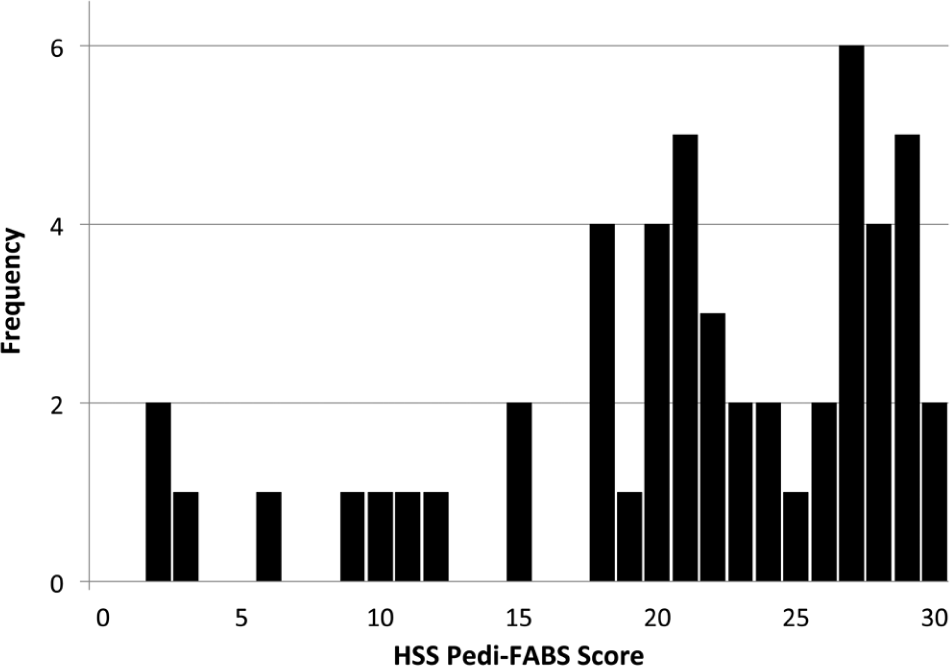
Distribution of scores of 51 subjects in the validation group who completed the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS). Although there is a slight negative skew, the subject cohort consisted of active children.
Validation Results
Fifty-one subjects completed the HSS Pedi-FABS for validation. Statistically significant positive correlations were noted between the HSS Pedi-FABS and existing adult and pediatric scales: Tegner (r = 0.44, P = .001), Marx (r = 0.51, P = .0001), Noyes-Sports (r = 0.30, P = .03), Noyes-Functional (r = 0.44, P = .001), and PAQ (r = 0.60, P < .001). Additionally, level of competition (r = 0.56, P < .001), hours per week of current athletic activity (r = 0.62, P < .001), and hours per week of athletic activity during peak season (r = 0.62, P < .001) all showed statistically significant correlation to the HSS Pedi-FABS.
Of the variables evaluated for discriminant validity, age and BMI showed no significant associations with the HSS Pedi-FABS. Further, there was no significant association between the HSS Pedi-FABS and the Daniel scale; mean scores for each of the 3 Daniel scale categories were nearly identical (21.1, 21.7, and 20.2 for categories 1, 2, and 3, respectively). Therefore, all of the a priori validation hypotheses were demonstrated.
Reliability Results
All 51 subjects were used to evaluate the HSS Pedi-FABS for internal consistency reliability, resulting in a Cronbach alpha of .914. Forty-one subjects of the original validation group answered “no change” when asked whether there were any changes in their condition, and they were therefore eligible for inclusion in test-retest reliability calculation. Test-retest reliability of the HSS Pedi-FABS was excellent (ICC = 0.91). The test-retest interval averaged 7 days (range, 4-14 days).
Floor and Ceiling Effects
Ceiling effects were noted in the 3 continuous adult measures (Table 4; see Appendix 2, available online). No ceiling effect was present in the HSS Pedi-FABS. No floor effects were seen in any scale.
Scores, Floor, and Ceiling Effects for Each of the Continuous-Measure Activity Scales Studied a
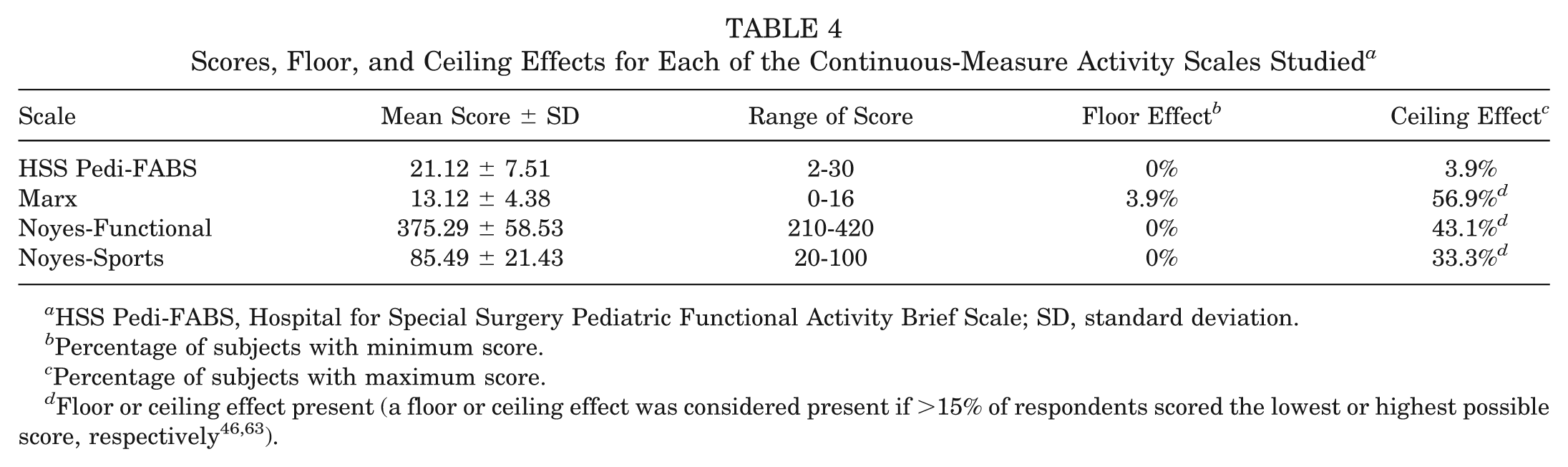
HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale; SD, standard deviation.
Percentage of subjects with minimum score.
Percentage of subjects with maximum score.
Discussion
This study demonstrated that the 8-item HSS Pedi-FABS has robust construct validity (both convergent as well as discriminant), demonstrates reliability in both test-retest and internal consistency reliability calculations, and lacks floor and ceiling effects when administered to a target cohort of athletically active adolescents age 10 to 18 years. This rigorous development and validation and the simplicity (only 8 items) of the instrument make it ideal for clinical activity assessment and quantification in this age group and confer potential for widespread application in clinical outcomes research in pediatric orthopaedic surgery, sports medicine, and rehabilitation.
A formal literature search conducted in preparation for this study yielded a dearth of potential pediatric self-reported activity questionnaires, despite a burgeoning interest in pediatric sports medicine outcomes. Existing pediatric questionnaires measured disability; were parent-reported, lengthy, or specific to a single condition or joint; or consisted of only a small activity component within the overall score. For example, Kocher et al 33 successfully validated a pediatric International Knee Document Committee (Pedi-IKDC) evaluation in children and adolescents, which is knee-specific. Although this metric has proven useful for pediatric and adolescent sports research on conditions of the knee, it is not designed to measure global athletic activity. Use of the Pedi-IKDC is therefore limited in conditions of the spine, hip, ankle, or foot and in long bone fracture. Another scale, the Child Health Questionnaire (CHQ), is a family of generic quality of life instruments that are validated in children 5 to 18 years old. This scale, however, consists of parent-reporting and is designed to assess quality of life; it does not specifically address physical activity.
In evaluation of the HSS Pedi-FABS, evidence of construct validity was robust. In addition to demonstrating both convergent and discriminant validity, the positive correlations in the 0.3-0.6 range indicate that although there is a statistically significant correlation, the activity measured by our construct differs from that of existing scales. Unlike adults, in whom activity level generally decreases with age, 44 children maintain their activity level as they progress through adolescence. Furthermore, in active children, differences in BMI may be attributable to differences in muscle mass, adiposity, or both. Although decreased activity may lead to larger increases in BMI over time during adolescence, 5 cross-sectional associations between BMI and activity in active children are not known. Therefore, both provided data for discriminant validity testing, and this lack of association between age or BMI and the HSS Pedi-FABS allows for use of the scale longitudinally, with changes over time representing the patient’s condition rather than changes in age or body habitus. Furthermore, because the Daniel scale is a 3-point scale that analyzes only type of sport played (1, jumping and pivoting sports; 2, lateral motion sports; 3, other sports such as running and swimming) and does not account for level of participation, frequency, or multiple sports, it too provided an excellent comparison for discriminant validity testing. Although sport type may be meaningful in understanding activity level in adults, similar differences in active children and adolescents may be inconsequential.
In contrast to some of the existing adult metrics, the HSS Pedi-FABS did not demonstrate a ceiling effect, confirming that existing sport activity scales developed for adults lack specificity for children. Whereas the adult activity metrics evaluate frequency and various sport maneuvers to quantify activity, this is not always appropriate in children. For instance, a 35-year-old athlete who runs 5 times per week is likely to have higher activity than one who runs once per week. However, children tend to be more active than adults. An adolescent athlete who runs 5 times per week at varsity track practice is very different than an otherwise sedentary adolescent who may report running 5 times per week while playing outside with friends. The HSS Pedi-FABS accounts for these differences with items that factor level of competition, endurance, and level of supervision of sport activity by coaches and trainers. By appraising these unique items, the HSS Pedi-FABS avoids the ceiling effect otherwise noted when existing adult scales are used to test children (Figure 2 and Table 4; see Appendix 2, available online).
The HSS Pedi-FABS has some advantages over existing pediatric scales as well. Other pediatric scales are lengthy, and the simplicity and brevity of our 8-item scale provide an advantage. In addition to decreasing burden on patients and parents, these qualities minimize the potential for questionnaire fatigue and will likely increase completion compliance for clinical outcome studies. Limiting questionnaire length subsequently maximizes patient/subject retention and minimizes loss of clinical research data points. Finally, the HSS Pedi-FABS is not sport- or joint-specific and therefore is a more generalizable measure of global athletic activity.
One difficulty during development was choosing an acceptable grade reading level for the scale, given the wide range of normal scholastic developmental variation in this target age group. Readability of the scale before validation was evaluated and noted to be at a 6.6th-grade level. This was deemed acceptable because the scale could be read and understood by most children in the target population yet still provide enough detail to create a robust construct. Additionally, the scale is written well below the national average literacy level (8th grade), thereby making the scale accessible to those parents who assisted the younger children who required reading help. 37 Further, although parents helped their children read the scale as needed, the children provided their own answers. Developing and validating the scale in younger children affords applicability to this important younger demographic, who have been the subject of recent interest in sports injuries (eg, ACL rupture, 18 osteochondritis dissecans, and patellar instability) and surgical intervention. Although the influence of parental reading assistance is unclear, the results indicate that this scale is reliable and valid in these younger children as well.
Although this novel activity scale has many advantages, there are some limitations to its use. In subjects who are predominantly active in sports that do not require running, cutting, decelerating, and pivoting (eg, swimming, diving), these 4 items may give an overall score that underestimates activity level. However, for the vast majority of sports and activities, this score is applicable. Even for those sports in which these maneuvers may be less applicable, endurance and level of competition and supervision may be quantified, extending use of the scale when cohorts of athletes within these unique sports are compared. Despite these limitations, there are clear advantages to this activity scale. These include simplicity, validity, excellent reliability, and lack of the ceiling effect that exists with currently available adult metrics. Although the current study establishes this scale as a reliable and valid measure of activity that is suitable for use as a prognostic variable in clinical research, one limitation is the lack of responsiveness data. Research is underway to determine responsiveness of the scale to further understand how changes in activity over time correspond to clinical change. Furthermore, replication of this work in different cohorts and populations would increase generalizability and allow for cross-cultural comparisons of activity level.
In conclusion, the 8-item HSS Pedi-FABS is a simple, reliable, and valid metric to assess activity in children and adolescents 10 to 18 years old. It is a valuable tool for objective assessment of activity in children and adolescents and for evaluation of activity level as a prognostic variable for clinical research studies in pediatric orthopaedic sports medicine. By using this instrument for child and adolescent athletes, investigators can better evaluate outcomes after treatment.
Footnotes
Acknowledgements
The authors acknowledge the following individuals for their assistance with this manuscript: Lawrence H. Yang, PhD, assistant professor of epidemiology, Joseph L. Mailman School of Public Health of Columbia University; Sophia Li, Columbia University; and K. Durham Weeks, MD, Hospital for Special Surgery.
Presented at the 39th annual meeting of the AOSSM, Chicago, Illinois, July 2013.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from the Louis and Rachel Rudin Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.