
Abstract
Pregnancy is marked by visible bodily changes such as weight gain. Guided by objectification theory, this study aimed to test whether gestational body mass gain—an indicator of visible bodily transformation—is associated with perceived interpersonal objectification experiences that position one's body as an object of appearance-based evaluation. These experiences may, in turn, be related to greater self-objectification, which may subsequently correlate with poorer mental health (i.e., depressive symptoms, disordered eating, and sexual dysfunction). The sample included 399 heterosexual, cisgender pregnant women in their second to third trimester who had not previously given birth (Mage = 29.97, range = 19–48). As predicted, path analysis revealed that greater gestational body mass gain was associated with perceived interpersonal objectification, which in turn was related to self-objectification, which then was directly associated with all three mental health outcomes. The association between self-objectification and disordered eating was indirectly explained through body shame and interoceptive awareness, while self-objectification's association with sexual dysfunction was indirectly explained through interoceptive awareness. These findings support the applicability of objectification theory to pregnancy, underscoring the need to reduce weight and appearance-focused practices and foster health-oriented perceptions of pregnant bodies. Finally, findings highlight the importance of public health efforts to normalize pregnancy-related body mass changes.
In Western societies, women's physical appearance continues to be emphasized over their competencies, emotions, and intellect, reinforcing a narrow definition of women's social value (Bordo, 2023). Women are often erotically, socially, and economically rewarded for conforming to cultural beauty ideals through enhanced social approval and advantages in the labor market, thereby reinforcing idealized notions of femininity (Kukkonen et al., 2024; Yetsenga et al., 2024). Objectification theory offers a framework for understanding how cultural norms that position women as objects of visual and sexual value contribute to their experiences of sexual objectification and self-objectification, ultimately affecting their mental health (Fredrickson & Roberts, 1997). Despite calls for greater inclusivity to examine whether associations among the theory's core constructs differ across different life stages, most empirical investigations grounded in objectification theory have remained narrowly focused on college-aged women (for reviews see Beech et al., 2020; Jones & Griffiths, 2015; Ward et al., 2023). The current study responds to this call by examining the applicability of the theory during the transition to motherhood, which is a period of life that has received relatively little attention in the objectification literature (Beech et al., 2020). Based on the appearance-based nature of sexual objectification and the visible appearance changes often occurring in pregnancy, we explored how gestational weight gain might contribute to experiences of interpersonal sexual objectification and its consequences among pregnant first-time mothers.
Sexual Objectification and Self-Objectification
Sexual objectification is understood as a process occurring when women are regarded primarily as bodies meant to provide use or pleasure for others (Fredrickson & Roberts, 1997). That is, when women are reduced to their bodies’ appearance and their subjectivity is ignored, they are evaluated only based on their body's attractiveness, as if their appearance can fully represent who they are. Sexual objectification takes multiple forms and occurs through two main distinct pathways: objectifying environments and objectifying interpersonal experiences (Roberts et al., 2018). Objectifying environments refers to passive exposure to a sexually objectifying culture; for example, through the portrayal of women's bodies as sexual objects in mass social media and pornographic content (Karsay et al., 2019; Vandenbosch & Eggermont, 2015). Objectifying interpersonal experiences occur at the interpersonal level and include both compliments as well as negative comments regarding one's body (particularly regarding appearance and weight), evaluative gazes, and unwanted sexual advances (e.g., Kahalon et al., 2022; Kozee et al., 2007). These interpersonal objectifying experiences precede self-objectification, whereby individuals internalize the objectifying attitude encountered in interpersonal contexts and come to view themselves as objects meant to be looked at and evaluated based on their appearance and bodily attractiveness, rather than their body functionality or intrinsic qualities (Fredrickson & Roberts, 1997)
Antecedents of Objectification and Self-Objectification During Pregnancy
Pregnancy is a period marked by rapid uncontrolled physical changes, including weight gain, shifts in body shape (e.g., thickening of the waist, widening of the hips, the appearance of a “baby bump”), and skin transformations, such as stretch marks and melanin deposition (Cunningham, 2014). These significant bodily changes that occur during a healthy pregnancy are highly visible, making pregnancy a unique context for studying perceived social attention to one's body. In addition, and critically to the present research, such changes may expose women to interactions or situations that emphasize their appearance, which can further increase their self-objectification. Indeed, qualitative research indicates that pregnant women frequently receive body-related messages, which most often focus on weight gain (Harrison et al., 2019; Rodgers et al., 2024), suggesting that manifestations of interpersonal objectification during pregnancy mainly involves appearance-focused remarks rather than overt sexualized attention. These messages may come from various sources within their interpersonal environment, including friends, family members, medical professionals, and even strangers (Harrison et al., 2019; Rodgers et al., 2024). Such messages can include positive comments that emphasize the idea that pregnancy enhances the woman's appearance, such as complimenting a woman on her beautiful belly or “just the right” amount of weight gain (Harrison et al., 2019; Neiterman & Fox, 2017; Rodgers et al., 2024). They can also include more negative comments that imply bloating or undesired appearance shifts, such as excessive weight gain or increased body size (e.g., “that's a big baby”) as well as pressure to control weight (Rodgers et al., 2024). Some women noted that these messages provoked heightened body image concerns and preoccupation with appearance during their pregnancy (Neiterman & Fox, 2017; Rodgers et al., 2024). Whether positive or negative in tone, these objectifying experiences center women's appearance, which may lead them to focus on their appearance rather on their body experience and functionality, possibly increasing their self-objectification (Fredrickson & Roberts, 1997). We proposed that greater visible pregnancy-associated body changes (operationalized as body mass gain relative to a woman's pre-pregnancy composition) would be associated with more objectifying experiences.
Consequences of Self-Objectification During Pregnancy
In the initial conceptualization of objectification theory, self-objectification was posited to place women at greater risk for negative mental health outcomes (Fredrickson & Roberts, 1997). This assertion has been supported by empirical evidence, primarily among samples of young women, which revealed that self-objectification is associated with depression, disordered eating, and sexual dysfunction and dissatisfaction (for reviews see Jones & Griffiths, 2015; Kahalon & Klein, 2025; Schaefer & Thompson, 2018). The few studies on self-objectification conducted among pregnant women illustrate that body surveillance, a behavioral indicator of self-objectification, is associated with depression (Brock et al., 2021; Rubin & Steinberg, 2011), disordered eating (Barnhart et al., 2024), and sexual dissatisfaction (Brock et al., 2021).
The Indirect Association Between Self-Objectification and Mental Health Outcomes During Pregnancy
Objectification theory originally proposed four mechanisms that mediate the affect of self-objectification on adverse mental health outcomes: appearance anxiety, disrupted flow experience, body shame, and reduced interoceptive awareness (Fredrickson & Roberts, 1997). Subsequent research has expanded this framework by identifying additional mechanisms that are particularly relevant for specific outcomes (e.g., Calogero et al., 2021; Kahalon et al., 2024b). In the present study, we focused on two of these previously supported mechanisms: body shame and interoceptive awareness. As discussed below, theory and empirical work suggest that these constructs are particularly relevant in the context of pregnancy and when predicting mental health outcomes specifically.
Body shame includes negative emotional response that arises when individuals perceive their bodies as falling short of cultural appearance standards (McKinley & Hyde, 1996). In the general population, body shame is a well-established mediator in the association from self-objectification to depression and disordered eating (Jones & Griffiths, 2015; Tiggemann, 2011); however, findings regarding sexual dysfunction are less common and inconsistent (for review, see Kahalon & Klein, 2025). During pregnancy, women often undergo a process of reevaluating their body image, which may damage their feelings toward their body (Linde et al., 2022; Watson et al., 2015) and may result in body shame. There is tentative evidence suggesting a role of body shame in the association between self-objectification and disordered eating during pregnancy (Barnhart et al., 2024). Specifically, Barnhart et al. (2024) found that body surveillance was positively associated with body shame among pregnant women, which in turn was associated with disordered eating. However, self-objectification and body-surveillance are distinct constructs (Calogero, 2011); therefore, further evidence is needed to support the association between self-objectification and body shame during pregnancy.
The second hypothesized mediator we examined in this study, interoceptive awareness, refers to one's subjective awareness of internal bodily states, such as hunger, fullness, and heart rhythm (Mehling, 2016). Although less studied than body shame, interoceptive awareness has been shown to explain the indirect associations from self-objectification and body shame to depression and disordered eating (Myers & Crowther, 2008; Peat & Muehlenkamp, 2011; Zheng & Sun, 2017). However, studies examining the role of interoceptive awareness as a mediator between self-objectification and sexual dysfunction are limited (Calogero et al., 2021; Kahalon et al., 2024b). It is plausible that interoceptive processes play a particularly important role during pregnancy. Pregnancy characteristics, such as increased hunger and cardiac output, nausea, and fetal movements (Cunningham, 2014), may heighten attention to internal cues, which may in turn contribute to higher levels of interoceptive awareness during pregnancy (Solorzano et al., 2022). Despite this plausible mechanism, the role of interceptive awareness in the association between self-objectification and mental health outcomes has not yet been examined among pregnant women. This gap provides a rationale for including interoceptive awareness as a proposed mediator in the present study.
Sociocultural Context
All participants in the current study were recruited from Israel. Notably, Israel is characterized by strong pronatalist norms, with a cultural emphasis on family ethos, fertility, and motherhood. At the policy level, reproductive healthcare is provided within a public healthcare system with universal coverage, ensuring broad access to prenatal and reproductive services. Fertility treatments, including in vitro fertilization, are publicly funded and widely available through the national health system (Birenbaum-Carmeli, 2016). Termination of pregnancy is legally regulated and requires approval from a multidisciplinary committee; however, abortion services are generally accessible in practice, with approval rates exceeding 99.8% among individuals who apply (Israeli Central Bureau of Statistics, 2025b).
The Present Study
The present cross-sectional study aimed to test the applicability of objectification theory to pregnancy. Consistent with objectification theory, and based on the premise that more visibly pronounced bodily changes during pregnancy may increase vulnerability to interpersonal objectification, our predictions were as follows:
Method
This study is part of a larger longitudinal project examining individuals during the transition to motherhood. Here we report the data collected during pregnancy. Below, we report how we determined all data exclusions, sample size, and measures in the study, consistent with reporting standards for quantitative research (Appelbaum et al., 2018). This study's design and its analysis were not pre-registered. All research materials are available on the Open Science Framework (OSF) in appendix: https://osf.io/g5pe9/?view_only = c343c41bd737471f8a9b470b30b45483
Participants
This study was open to the participation of pregnant individuals of all genders who met the following inclusion criteria: (a) at or beyond 22 weeks of gestation, (b) no prior live births 1 , and (c) being sexually active during the completion of study questionnaires. These criteria were selected based on evidence illustrating that most expectant mothers experience visible bodily changes at this stage of pregnancy (criteria a; Cunningham, 2014), that the association between sexually objectifying messages and self-objectification is higher among pregnant women with no previous live births in comparison to those with one or more previous live births (criteria b) (Hopper & Aubrey, 2013), and that the assessment of sexual dysfunction requires current sexual activity to yield interpretable results (criteria c). A priori power analysis was conducted using a Monte Carlo simulation in Mplus (Version 8.9) to estimate the minimum sample size required for the path analysis. The model included eight observed variables and thirteen direct paths, with standardized path coefficients set at .25 to reflect small-to-medium effect size. Based on 1,000 replications, maximum likelihood estimation, and the assumption of multivariate normality, a sample size of approximately 390 participants was required to achieve 80% power at a 0.05 significance level.
The initial sample included 525 pregnant individuals who were identified as cisgender women. Following missing data analysis and application of the analytic inclusion criteria (see Analytical Approach section), the final sample included 399 Israeli women, aged between 19 and 48 years (M = 29.97, SD = 4.14), between 22 to 41.5 weeks of gestation (M = 28.98, SD = 5.09). Regarding education, 26 (6.5%) reported a high school diploma as their highest level of attainment, 29 (7.3%) had completed professional studies, 191 (47.9%) held a bachelor's degree, 126 (31.6%) had a master's degree, and 27 (6.8%) had a PhD. Socioeconomic status was reported as below average by 23 (5.8%), average by 230 (57.6%), and above average by 146 (36.6%). Regarding religious affiliation, the majority of participants identified as Jewish (377; 94.5%), with the remaining participants identifying as Muslim (3, 0.7%), Christian (5, 1.3%), Druze (9, 2.2%), or other (5, 1.3%). In terms of religiosity, 72 (18%) identified as religious, 102 (25.6%) as traditional, 218 (54.6%) as secular, and the remaining 7 (1.8%) as other.
Procedure
Upon receiving ethical approval from the Institution Review Board of Bar-Ilan University (approval number IRB 10-2023), we recruited pregnant individuals of all genders through convenience sampling via notices posted on social media platforms, including Facebook and WhatsApp groups discussing pregnancy and stakeholder groups focused on pregnancy or maternal health. Additional recruitment channels included postings in general social media communities for young women (WhatsApp group, mailing lists) and snowballing outreach. A screening questionnaire was administered to determine eligibility (“are you currently pregnant at or beyond 22 weeks? enter the exact gestational week”; “have you previously given birth?”). Those who met inclusion criteria subsequently received a personal email with a link to the study questionnaires. The participants provided digital informed consent prior to completing the study questionnaires via the Qualtrics platform (Provo, UT). Questionnaires were partially randomized: predictors first, mediators second, and dependent variables last, with randomized order within each category. The participants were compensated with a 10 USD voucher for their time.
Measures
Participants completed the following measures in Hebrew. All measures, except those previously translated in past research, were translated into Hebrew and then back translated into English by two researchers independently. Any discrepancies were resolved through discussion until an agreement was reached.
Gestational Body Mass Gain
Participants provided their height, pre-pregnancy and current weight (kg) from which body mass indexes (BMI, kg/m2) were calculated. Self-reported weight data have been shown to exhibit high agreement (r = .98) with measured weight among pregnant women (Shin et al., 2014). Gestational body mass gain was calculated by dividing participant's current BMI by their pre-pregnancy BMI. BMI was used, rather than absolute weight, to capture changes in body shape/size which are accounted for by individual differences in height. Thus, BMI may reflect proportional body changes that are more likely to be noticeable to others. Moreover, BMI gain was considered a more relevant indicator than gestational BMI alone, as it captures the relative and likely noticeable body changes over the course of pregnancy rather than the absolute body size at a single time point.
Interpersonal Objectification
Interpersonal objectification was assessed using an adapted version of the Interpersonal Sexual Objectification Scale (ISOS; Kozee et al., 2007). The ISOS is a 15-item self-report questionnaire assessing objectifying experiences encountered in daily life over the past few weeks, including both body evaluations and unwanted explicit sexual advances. Respondents rated the frequency of these experiences on a 5-point Likert scale ranging from 1 (never) to 5 (almost always). For the purpose of this study, the ISOS was adapted to better reflect interpersonal objectification during pregnancy, primarily through appearance-focused interactions concerning body shape and weight, rather than overtly sexualized attention and harassment. Items focusing on explicit sexual harassment and overt objectification (e.g., “How often has someone grabbed or pinched one of your private body areas against your will?”) were excluded from the original instrument, as these are less commonly reported during pregnancy compared to subtler forms of objectification such as staring at a pregnant body (Harrison et al., 2019; Rodgers et al., 2024). Including such experiences could also pose ethical concerns for pregnant individuals with a history of sexual trauma, as completing these items may have elicited distress (Ullman et al., 2010). Moreover, one item (“How often have you overheard inappropriate sexual comments made about your body?”) was revised to represent a general comment rather than a sexual comment, removing the explicit sexual reference in the original (“How often have you overheard inappropriate comments made about your body?”). Finally, one item was added (e.g., “How often have people you known made comments about your changing body”) to capture objectifying experiences that are unique to pregnancy (Rodgers et al., 2024).
Exploratory factor analysis with maximum likelihood extraction with direct oblimin rotation was conducted to examine the underlying factor structure of this revised eight-item scale (delta = 0). Parallel analysis was used with the scree plot to determine the number of factors to retain. Items with a primary factor loading greater than .50 and no cross-loading greater than .30 were retained (Tabachnick & Fidell, 2007). The Kaiser– Meyer–Olkin (KMO) measure of sampling adequacy was .85 (item-level KMOs = .807–.892), and Bartlett's test of sphericity was statistically significant, χ2(28) = 1447.51, p < .001, indicating that the data were appropriate for factor analysis. Parallel analysis supported retention of a single factor including all items, as the first observed eigenvalue (4.17) exceeded the mean and 95th percentile of simulated eigenvalues, while subsequent eigenvalues (1.04, 0.79, 0.66) did not, supporting a unidimensional solution. Velicer's minimum average partial test suggested a minimum at m = 6, indicating a higher number of factors; however, given the strong evidence from the parallel analysis and the large drop between the first and second eigenvalues, a one-factor solution was retained. Communalities for the retained items further supported this decision, indicating that most items shared substantial variance with the extracted factor (h2= .39–.80). Item loadings on the single factor ranged from .57 to .84, with all items loading in the moderate-to-high range. The adapted scale, including full factor loadings, communalities, item-total correlations, eigenvalues, and parallel analysis results are reported in Tables A1–A2 of the OSF Appendix. The adapted ISOS demonstrated evidence of good internal consistency (Cronbach's α = .87) and evidence of convergent validity. As theoretically expected, higher interpersonal objectification experiences were associated with greater self-objectification (r = .29, p < .001) and body shame (r = .26, p < .001).
Self-Objectification
Self-objectification was assessed using the Self-Objectification Beliefs and Behaviours Scale (SOBBS, Lindner & Tantleff-Dunn, 2017; translated by Kahalon et al., 2024a). This self-report questionnaire consists of 14 items assessing the extent to which women perceive themselves as a sexual object. Respondents rated their agreement with each item on a 5-point scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The scale comprises two subscales: the first reflects the internalization of an observer's perspective on the body (“I often think about how my body must look to others”), and the second reflects the tendency to treat the body as representative of the self, including placing greater emphasis on appearance than on function or internal experiences (“My body is what gives me value to other people”). A total score, representing the overall construct, was computed by averaging across items, with higher scores indicating greater self-objectification. The SOBBS has demonstrated evidence of excellent reliability (α = .91) and validity among college student samples (Lindner & Tantleff-Dunn, 2017) and was previously used among post-partum women (Choma et al., 2024). In the current study's sample, we found evidence of excellent internal consistency, α = .90.
Body Shame
Body shame was assessed using the Body Shame subscale of the Objectified Body Consciousness Scale (OBCS; McKinley & Hyde, 1996). This self-report subscale consists of 8 items assessing the degree to which women feel shame about their bodies when their bodies do not conform to sociocultural ideals (“I feel ashamed of myself when I haven’t made the effort to look my best”). Respondents rated their agreement with each item on a 7-point scale, ranging from 1 (strongly disagree) to 7 (strongly agree). An average score was calculated, with higher scores indicating higher levels of body shame. In the original validation, the Body Shame subscale of the OBCS demonstrated evidence of acceptable reliability (α = .75) and validity among young and middle-aged women (McKinley & Hyde, 1996); it has been previously used among pregnant women and demonstrated good internal consistency (McDonald's ω = .90, 95% CI [.88, .92]) as well as a significant correlation with disordered eating (r = .52, p < .001), as theoretically expected (Barnhart et al., 2024). In the current study's sample, we found evidence of acceptable internal consistency, α = .76.
Interoceptive Awareness
Interoceptive awareness was assessed using the Body Awareness subscale of the Scale of Body Connection (SBC; Price & Thompson, 2007). This subscale consists of 12 items assessing the perceived attention to bodily sensations and signals and bodily responses to emotions (i.e., aware of body changes when angry, aware of changes in breathing, take cues from body; “I notice how my body changes when I am angry”). For the purposes of this study, one item was deleted as it reflected awareness of emotional states rather than bodily sensations (“I notice my emotional response to caring touch”). Respondents rated the frequency of each item on a 5-point scale, ranging from 1 (not at all) to 5 (all the time). An average score was calculated, with higher scores indicating greater interoceptive awareness. A confirmatory factor analysis supported the single-factor structure of the revised Body Awareness subscale used in the current study, indicating adequate fit (CFI = .923, TLI = .900, RMSEA = .095, SRMR = .052). All standardized loadings were significant (p < .001) and ranged from .53 to .79. In the current study's sample, we found evidence of excellent internal consistency, α = .89.
Prenatal Depression
Prenatal depressive symptoms were assessed using the Edinburgh Peri and Postnatal Depression Scale (EPDS; Cox et al., 1987; translated and validated by Kandel-Katznelson et al., 2000). This self-report questionnaire consists of 10 items, assessing the frequency of depressive symptoms experienced over the past seven days (“I have blamed myself unnecessarily when things went wrong”). Respondents rated each item on a 4-point scale ranging from 0 (never/not at all) to 3 (often/quite a lot/most of the time). A sum score was calculated, with higher scores indicating greater severity of depressive symptoms. A score ≥ 13 is considered in the clinical range of probable depression. The EPDS has demonstrated evidence of good reliability, validity, and clinical sensitivity among pregnant women (Park & Kim, 2023). The translated version demonstrated evidence of good reliability, α = .84 (Kandel-Katznelson et al., 2000). In the current study's sample, we found evidence of good internal consistency, α = .86.
Disordered Eating
Disordered eating was assessed using the Eating Attitudes Test (EAT-26; Garner et al., 1982; translated and validated by Koslowsky et al., 1992). This self-report questionnaire consists of 26 items, assessing the frequency of feelings and behaviors associated with disordered eating (“I avoid eating when I am hungry”). Respondents rated the frequency of each feeling/behavior on a 6-point scale, ranging from 0 (never) to 5 (always). According to the EAT-26 guidelines, the ratings are then recorded to a 4-point scale (i.e., “never”, “rarely” and “sometimes” are coded as 0, “often” as 1, “usually” as 2 and “always” as 3 (reversed for item 26). A sum score was calculated, with higher scores indicating greater disordered eating symptoms and attitudes. A score ≥ 20 is considered in the clinical range of eating disorders (Garner et al., 1982). The translated version of the EAT-26 had demonstrated evidence of good reliability (α = .83) and criterion validity, as scores were significantly associated with measures of body image and weight (Koslowsky et al., 1992). In the current study's sample, we found evidence of good internal consistency, α = .84.
Sexual Dysfunction
Sexual dysfunction was assessed using the Female Sexual Function Index (FSFI; Rosen et al., 2000; translated and validated by Yulevitch et al., 2013). This self-report questionnaire consists of 19 items, assessing the following domains: desire, arousal, lubrication, orgasm, sexual satisfaction, and pain during sexual activity (“how often did you feel sexual desire or interest”). Respondents rated each domain relating to their sexual activity in the last month on a 5-point scale, ranging from 1 (very low or not at all) to 5 (very high). The pain during intercourse domain is scored on the same scale, only that it also includes the option 0, which indicates no experience of penetrative sex. A sum score was calculated, where lower scores indicated a higher level of sexual dysfunction. For convenience and readability, we recorded the values such that the higher scores indicated higher sexual dysfunction. The FSFI has demonstrated evidence of good reliability and validity among adult women of all ages (Neijenhuijs et al., 2019). The translated version demonstrated evidence of good internal consistency, α = .82 (Yulevitch et al., 2013). In the current study's sample, we found evidence of excellent internal consistency, α = .93.
Analytical Approach
Analytic Sample
Seven participants who reported being in a lesbian relationship were excluded from the main analyses. This is because evidence suggests that self-objectification differs between women attracted to men and those who are attracted to women or other genders (Kahalon et al., 2024a). Although separate analyses for this group were not feasible due to the small number of complete cases, we conducted supplementary analyses that included these participants in the larger sample and report the results of those analyses below.
Missing data analysis revealed that 78.5% of participants completed all questionnaires or had less than 10% missing data. Missing data was primarily due to early dropout, resulting in partial completion of the study measures. Specifically, 9.8% of the participants provided data on only one variable in the model, 2.4% on two variables, 4.1% on three variables, and 5.1% on four variables (pre-pregnancy and gestational BMI, objectification, self-objectification, and body shame, respectively). Because participants with incomplete data contributed very limited information, listwise deletion was employed to ensure that included participants had adequate data coverage across study variables.
Statistical Analyses
Descriptive statistics were conducted using IBM SPSS version 30. For all analyses, p < 0.05 was considered statistically significant. Pearson's correlation coefficients were calculated to explore the associations among all study variables as well as possible confounds. Path analysis was performed using the AMOS 28.0 version, with maximum likelihood estimation, to examine the theoretical model (Figure 1). The final model included only significant paths. Model fit was assessed through commonly used indices and criteria: Chi-square/df < 3, Confirmatory Fit Index (CFI) and Tucker-Lewis Index (TLI) values greater than 0.90; Root-Mean-Square Error of Approximation (RMSEA) less than 0.06 and Standardized Root Mean Square Residual less than 0.081 (SRMR; Hu & Bentler, 1999; Kline, 2015). Indirect effects were tested using bootstrapping with 5,000 resamples and bias-corrected 95% confidence intervals. Inspection of the residuals indicated that they met the assumptions of normality and linearity.
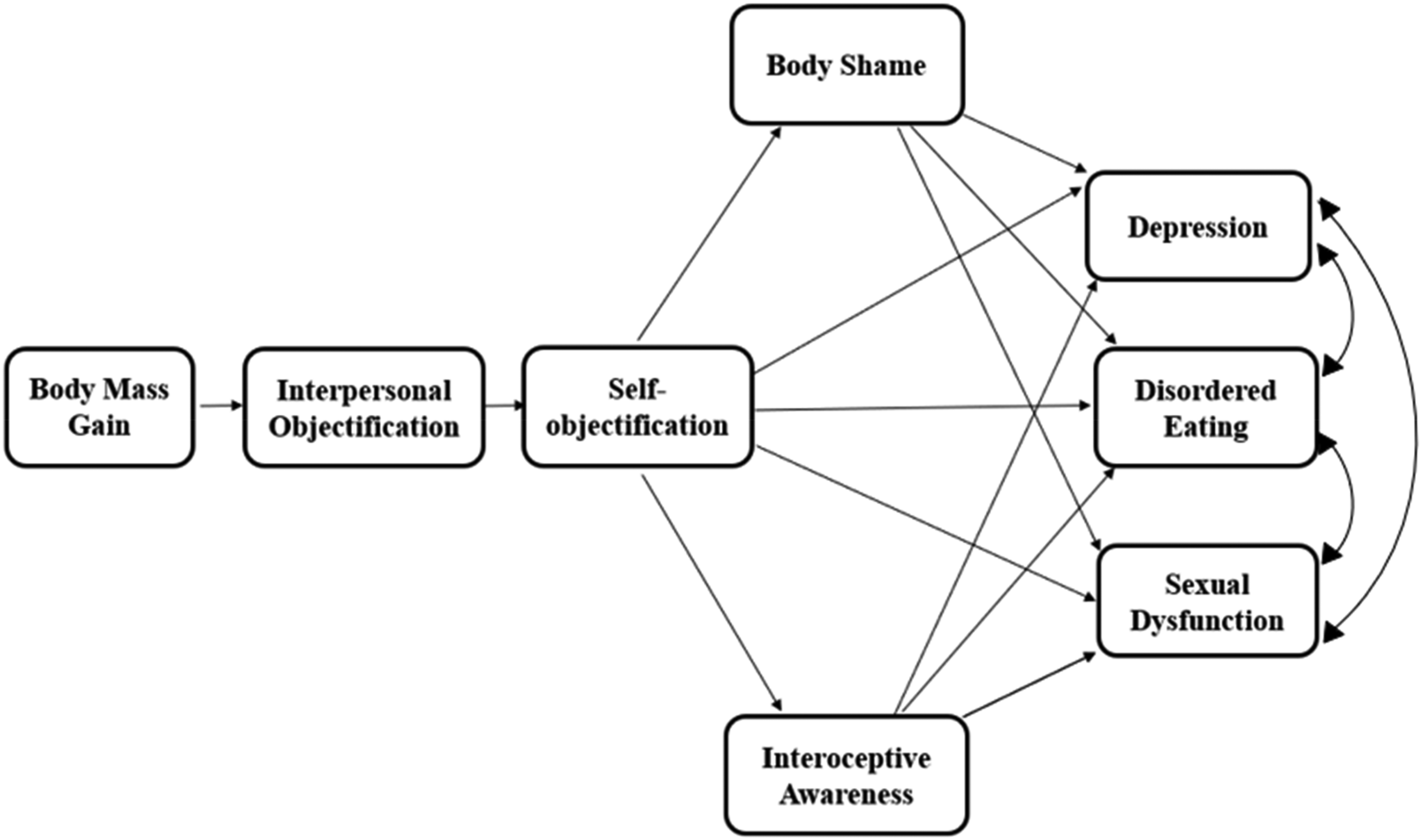
The conceptual model.
Results
Table 1 summarizes the descriptive statistics and correlations among the study variables. As can be seen in Table 1, gestational body mass gain was positively associated with interpersonal objectification, which was positively associated with self-objectification. In addition, significant correlations were found between self-objectification and the mediators offered by objectification theory (i.e., body shame, interoceptive awareness) as well as with all the mental health outcomes: depression, disordered eating and sexual dysfunction. Notably, gestational BMI was not correlated with interpersonal objectification, supporting our conceptualization that relative changes in body shape/size (i.e., body mass change) during pregnancy, rather than absolute gestational BMI, better capture the visible bodily transformations that may elicit objectifying experiences.
Means, Standard Deviations, and Correlations of Study Variables.
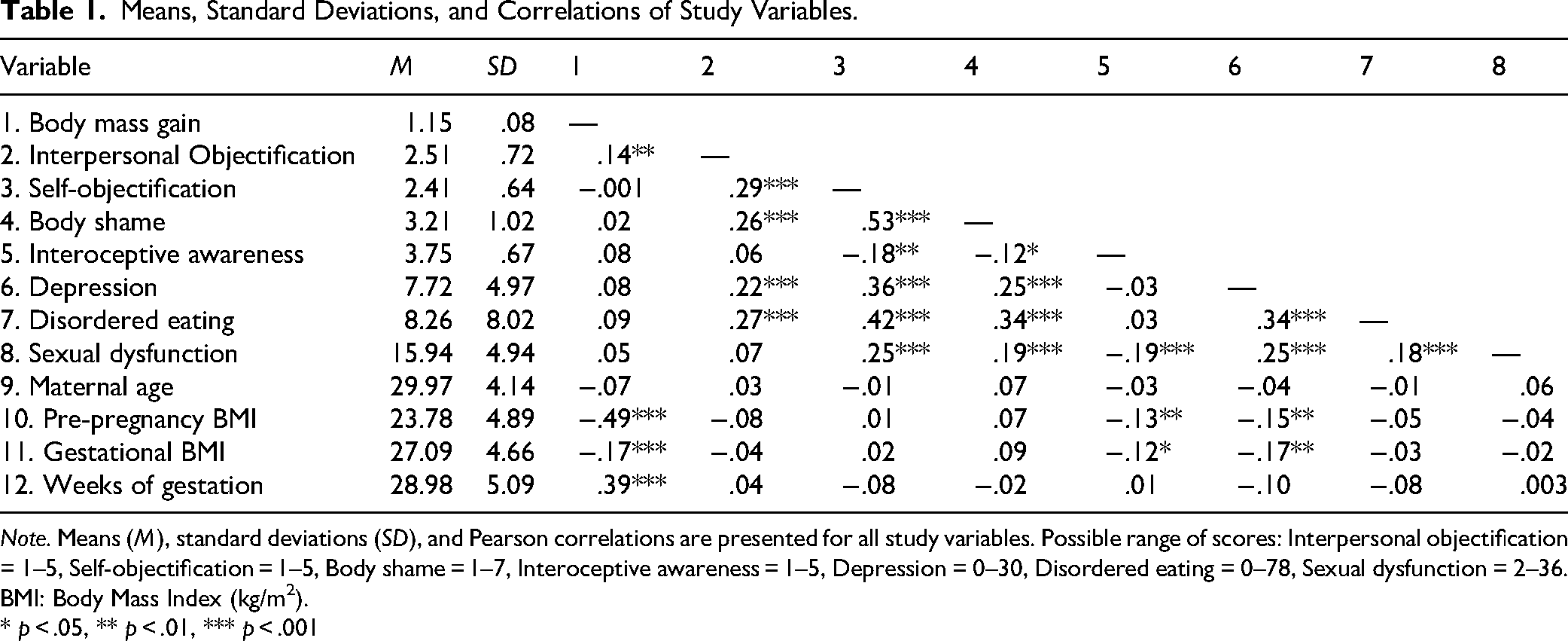
Note. Means (M), standard deviations (SD), and Pearson correlations are presented for all study variables. Possible range of scores: Interpersonal objectification = 1–5, Self-objectification = 1–5, Body shame = 1–7, Interoceptive awareness = 1–5, Depression = 0–30, Disordered eating = 0–78, Sexual dysfunction = 2–36.
BMI: Body Mass Index (kg/m2).
* p < .05, ** p < .01, *** p < .001
Considering the non-significant correlations between maternal age and weeks of gestation 2 and the dependent variables in the model, they were not controlled in the subsequent analyses. Although pre-pregnancy BMI and gestational BMI were significantly correlated with some of the mediators and the dependent variable in the model, they were not included as covariates given that they were already inherently accounted for in the computation of gestational body mass gain. Moreover, collinearity diagnostics confirmed high multicollinearity between pre-pregnancy BMI and gestational body mass gain (tolerance = .75; VIF = 1.33; condition index = 43.45), and between gestational BMI and gestational body mass gain (tolerance = .97; VIF = 1.03; condition index = 36.73).
Figure 2 shows the results of the path analysis (including standardized path coefficients), exploring the serial mediation effect from gestational body mass gain to mental health outcomes via interpersonal objectification, self-objectification, body shame, and interoceptive awareness. Only significant coefficients are presented. Detailed results of the indirect paths are presented in Table 2. The model demonstrated adequate model fit to the data, χ 2 (16) = 37.353, p = .002, CFI = .948, TLI = .909, NFI = .915, RMSEA = .058, and SRMR = .05.
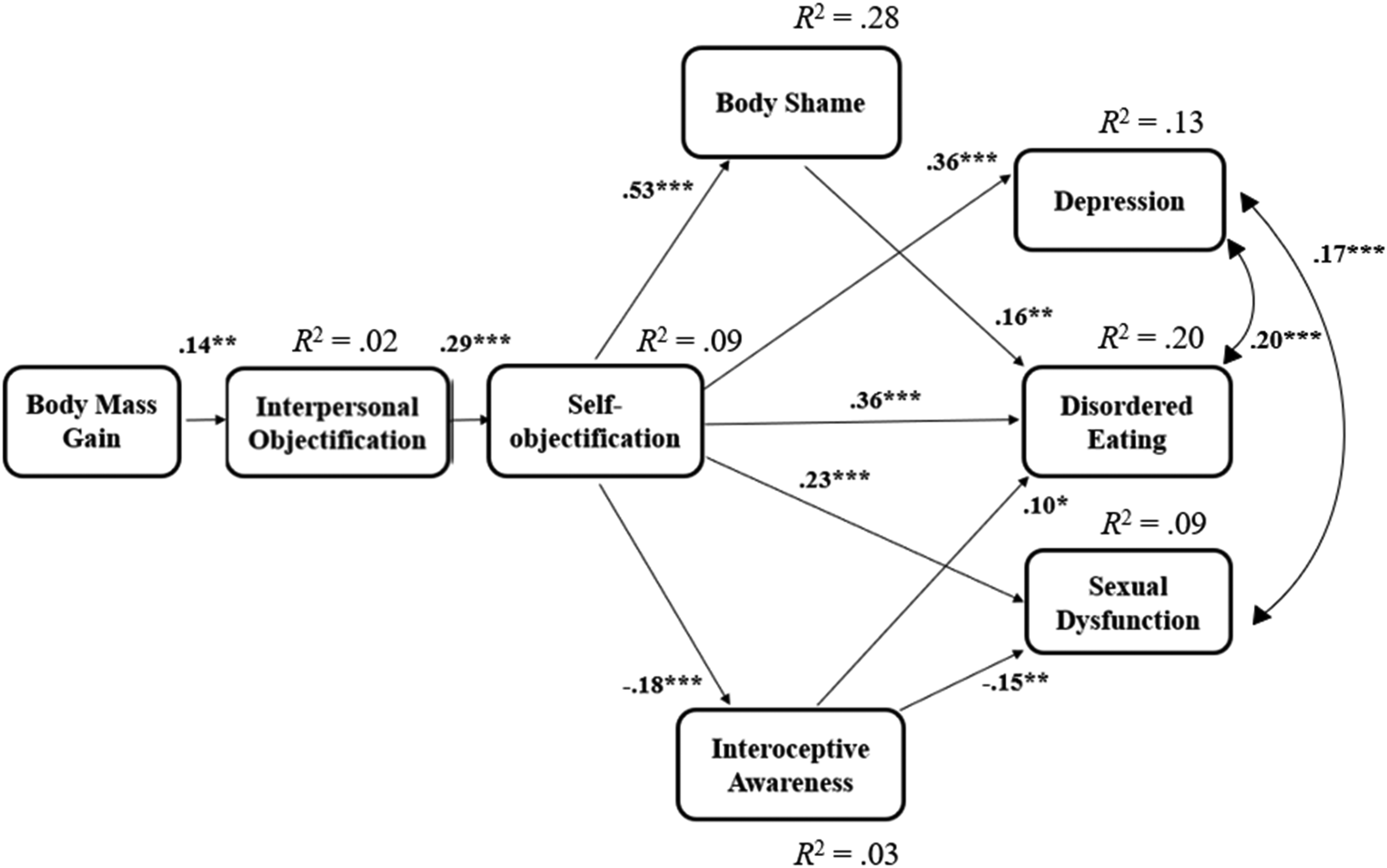
Path analysis of gestational body mass gain and mediating effects of interpersonal objectification, self-objectification, body shame and interoceptive awareness on mental health outcomes.
Summary of Indirect Relations.
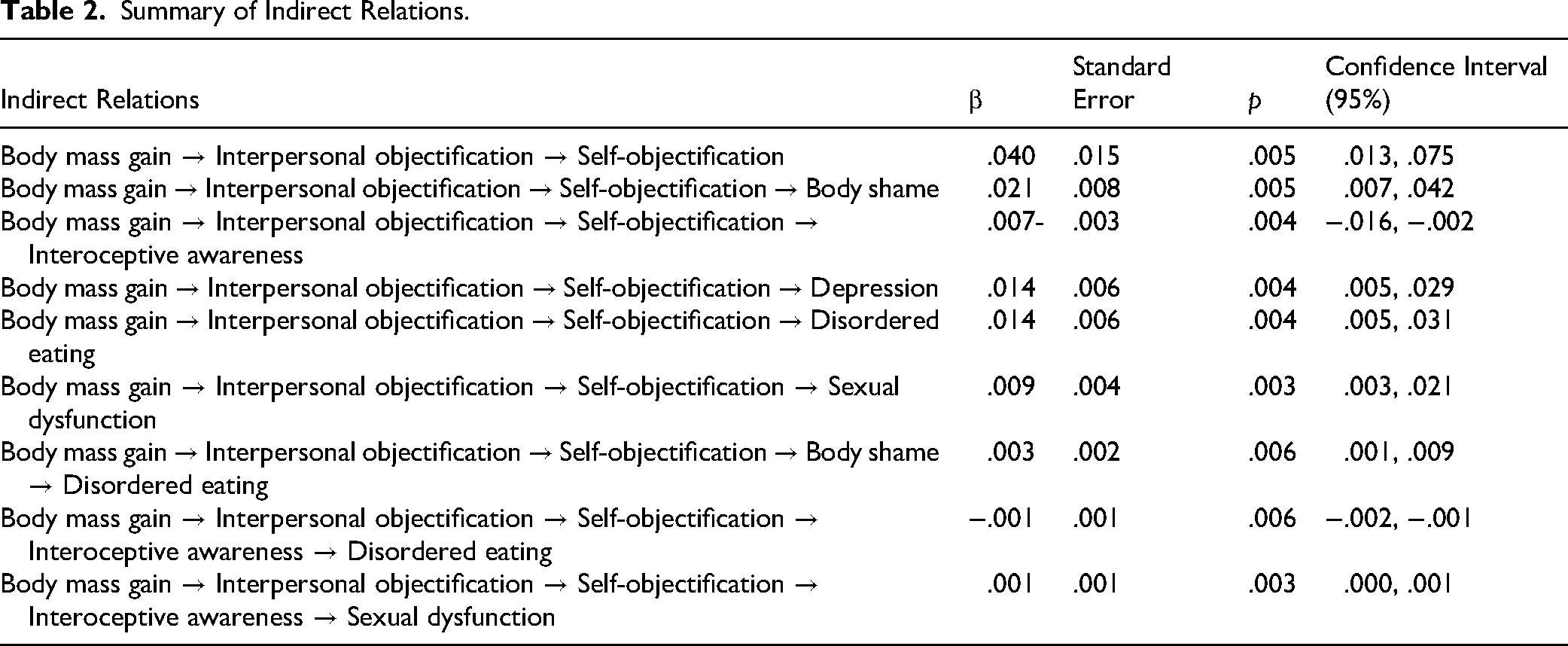
As can be seen in Figure 2 and Table 2, body mass gain was positively associated with interpersonal objectification, which in turn was positively associated with self-objectification. Self-objectification, in turn, was directly associated with depression, disordered eating, and sexual dysfunction, supporting H1. In addition, self-objectification was associated with body shame and interoceptive awareness, which in turn were related to the mental health outcomes. However, the indirect relations varied between the different outcomes, only partially supporting H2. Body shame only partially explained the indirect association between self-objectification and disordered eating, but it did not explain the indirect associations from self-objectification to depression or sexual dysfunction. Similarly, interoceptive awareness only explained the indirect association from self-objectification to disordered eating and sexual dysfunction, but not depression. Notably, when the model was re-estimated including women in lesbian relationships (n = 7), the results did not change meaningfully: all associations remained statistically significant (ps < .02), and the overall pattern of results was unchanged. Full details are available in the OSF appendix
Discussion
The present study examined the applicability of objectification theory among pregnant first-time mothers, focusing on the associations among gestational body mass gain, interpersonal sexual objectification, self-objectification, and mental health outcomes. The results supported the prediction that gestational body mass gain is associated with objectifying interpersonal experiences among pregnant women. Furthermore, consistent with objectification theory, findings supported indirect associations from interpersonal objectification to adverse mental health outcomes via self-objectification, body shame, and lower interoceptive awareness.
Objectification During Pregnancy
The current study supports the applicability of objectification theory to pregnancy, extending the growing literature on objectification processes among pregnant women (Barnhart et al., 2024; Brock et al., 2021; Rubin & Steinberg, 2011). Specifically, the findings highlight pregnancy-related factors (i.e., gestational body mass gain and perceived exposure to interpersonal objectification) that can foster greater self-objectification during pregnancy. In the general population, the link between interpersonal- and self-objectification has received empirical support (Calogero & Jost, 2011; Calogero et al., 2021; Szymanski, 2020), although relatively little research has examined this association among pregnant women. Among cisgender, heterosexual pregnant women, preliminary evidence has suggested an association between the interpersonal experience of humanization by one's partner and low levels of body surveillance (Brock et al., 2021); yet, the sources of interpersonal objectification remain understudied (Roberts et al., 2018; Ward et al., 2023). The present results suggest that pregnancy may heighten women's exposure to appearance-based scrutiny and the internalization of external body evaluations. The visible changes of the pregnant body (as operationalized by gestational body mass gain in this study) may increase susceptibility to objectifying experiences. This external attention to one's body, whether overt or subtle, can encourage women to adopt an outsider's perspective on their bodies, thus fostering self-objectification. Yet, given the correlational nature of this study, it is unclear whether increased body mass gain directly elicits more objectifying experiences, or whether pregnant women who are aware of their body mass gain become more sensitive/attentive to such feedback. In either case, in a sociocultural context that emphasizes appearance over the functional meaning of bodily changes, normative biological changes such as weight gain during pregnancy may indirectly contribute to self-objectification and its associated psychological risks.
Considering the broader sociocultural context in which this study was conducted may further illuminate the factors contributing to the objectification of pregnant bodies. The current findings are embedded within the Israeli context, which is characterized by pronatalist values alongside relatively supportive reproductive health policies (Birenbaum-Carmeli, 2016). Israel's fertility rate is relatively high compared with other high-income countries, with women having on average about 2.9–3.1 children over their lifetimes (Israeli Central Bureau of Statistics, 2025b). These fertility rates imply that Israeli society highly values and facilitates reproduction. Such contexts may intensify instrumental views of the pregnant body as a means for reproduction and childbearing, rendering pregnancy a highly monitored bodily state that may amplify objectification processes. At the same time, access to reproductive healthcare and the legal availability of abortion suggests that participants in the present sample were likely pregnant by choice and not constrained by restrictive abortion legislation (Birenbaum-Carmeli, 2016; Israeli Central Bureau of Statistics, 2025a, 2025b). In less pronatalist sociocultural contexts, or in contexts where abortion is heavily restricted or inaccessible, objectifying processes during pregnancy may be expressed differently and the associations observed in the present study may vary in strength or operate through different psychological pathways. Cross-cultural investigations are therefore needed to examine whether similar patterns of associations emerge across diverse contexts.
Similar to the current study's results, Frederick et al. (2022) found that individuals from the general population with higher BMI also reported greater interpersonal objectification from peers and family (operationalized as perceived pressure to improve appearance and shape, decrease body fat, and look thinner). Nevertheless, it is important to note that in the current study, the observed association between gestational body mass gain and interpersonal objectification was weak. The measure used for interpersonal objectification in the current study (i.e., ISOS) was not originally developed for use with pregnant women, and therefore may not fully capture pregnancy-specific objectification experiences. For example, some pregnant women experience unsolicited touching of their belly and implicit social regulation of their bodies from close others, strangers, and healthcare providers. Such social regulations may include comments regarding pregnant women's eating, weight, physical activity, and the “maternal” shape of their bodies (Hodgkinson et al., 2014; Rodgers et al., 2024). We did not include these forms of objectification in the measure used, and therefore future research may examine such pregnancy-related objectifying experiences.
Contrary to this study, which did not detect an association between gestational body mass gain and self-objectification, Frederick et al. (2022) found an association between BMI and internalization of societal appearance standards. These differences might stem from self-objectification and internalization of appearance ideals being related albeit distinct constructs that are influenced by different factors. Another possible explanation is the unique nature of pregnancy-related body mass gain that may carry a more complex cultural meaning that differs from typical body mass. During pregnancy, body mass gain is often viewed as a positive symbol for a healthy pregnancy and consistent with maternal expectations (“eating for two”; Criss et al., 2016). However, increases in body mass during pregnancy, beyond the baby bump, may also be perceived as negative (Vanstone et al., 2017). This complex and potentially conflicting set of meanings may weaken the association between BMI and self-objectification in the context of pregnancy; however, further study is needed on the topic.
Implications for Mental Health
Our results indicate that self-objectification is directly associated with depressive symptoms, disordered eating, and sexual dysfunction, suggesting that pregnant women with greater self-objectification may be more prone to experience depressive symptoms, disordered eating behaviors, and sexual difficulties. Documenting these associations during pregnancy is important, given that reduced maternal mental health can negatively impact birth outcomes, short- and long-term fetal outcomes, and family well-being (Accortt et al., 2015; Daescu et al., 2023; Milembamane et al., 2023).
The findings regarding depression and disordered eating are congruent with evidence documenting an association with body surveillance, which is a distinct yet related construct to self-objectification (see Calogero & Jost, 2011) among young, non-pregnant, cisgender heterosexual women (for review see Jones & Griffiths, 2015; for meta-analysis see Schaefer & Thompson, 2018) and among pregnant women (Barnhart et al., 2024; Brock et al., 2021; Rubin & Steinberg, 2011). However, the findings regarding sexual dysfunction are particularly novel in the context of a pregnant population. As far as we know, this is the first study to establish this association during pregnancy (for a review, see Kahalon & Klein, 2025).
When considering the model as a whole, disordered eating emerged as the outcome with the most explained variance, aligning with findings from research that examined all three mental health outcomes among non-pregnant, cisgender, heterosexual women (Calogero et al., 2021; Tiggemann & Williams, 2012). This pattern of results may reflect a broader limitation of objectification theory, which has been more effective in explaining disordered eating, but may be less robust in accounting for other mental health outcomes. Moreover, self-objectification showed the strongest relations to all three mental health outcomes (depression, disordered eating, and sexual dysfunction), emphasizing its role in shaping mental health outcomes during pregnancy. However, given the relatively low explained variance of depression and sexual dysfunction, the findings suggest that additional pathways and mechanisms may be involved in these associations, which were not fully captured in the current study.
Tiggemann (2011) asserted that most empirical tests of objectification theory have treated the three mental health outcomes (depression, disordered eating, sexual dysfunction) in isolation. They argued that, since these mental health adversities are often comorbid and may stem from shared self-objectification processes, a more statistically and theoretically valid test of the theory would involve examining whether self-objectification accounts for the intercorrelations among these outcomes. Importantly, models that incorporate all three outcomes are rare and have primarily been tested with young women whose age is consistent with the beauty ideal portrayed in media (Calogero et al., 2021; Tiggemann & Williams, 2012). In the context of these intercorrelations, it is noteworthy that although depression, disordered eating, and sexual dysfunction were positively correlated at the bivariate level (Table 1), these associations were reduced or no longer significant in the path model (Figure 2) once interpersonal objectification, self-objectification, and its consequences (body shame and interoceptive awareness) were controlled. This analytic distinction suggests that the bulk of the shared variance between the mental health outcomes observed in the simple correlations can be explained by objectification-related processes.
The Indirect Relation Between Self-Objectification and Mental Health Outcomes
The results revealed that the association between self-objectification and disordered eating was partially explained by both body shame and interoceptive awareness, and the association with sexual dysfunction was partially explained by interoceptive awareness. However, the association between self-objectification and depression was not explained by either body shame or interoceptive awareness. Taken together, these results provide only partial support for the theoretical pathways proposed in the original objectification theory (Fredrickson & Roberts, 1997). Moreover, contrary to body shame, the findings regarding the indirect role of interoceptive awareness slightly diverge from earlier studies among non-pregnant women that have tested the full model proposed by objectification theory (Calogero et al., 2021; Tiggemann & Williams, 2012). Specifically, these previous studies found that interoceptive awareness only indirectly explained the effect of self-objectification on depressive symptoms (Calogero et al., 2021; Tiggemann & Williams, 2012), which was not observed in the current study. These inconsistencies may be related to the current study's sample (i.e., pregnant women), and specifically to interoceptive awareness associated with gestation (Solorzano et al., 2022), possibly changing pre-pregnancy existing associations with self-objectification, depression, or sexual functioning. Another explanation may be that the measure used for interoceptive awareness in the current study (i.e., SBC) captures general interoceptive awareness, rather than specific pregnancy-related experiences, such as fetal movements.
Similarly, the indirect effect from interoceptive awareness to sexual dysfunction, also rarely observed in non-pregnant samples (Calogero et al., 2021; Tiggemann & Williams, 2012), may be attributed to pregnancy-specific process. For instance, bodily sensations like pain, fatigue, or fetal movement during pregnancy interfere with sexual activity (Araújo et al., 2012). Overall, the findings suggest that certain psychological mechanisms may be more relevant for specific outcomes than others and that self-objectification may operate differently during pregnancy.
Practice Implications
These findings have several implications for clinical practice. First, mental health professionals and healthcare providers should consider how bodily changes may be associated with perceived interpersonal objectification and self-objectification during pregnancy, and how these, in turn, may affect mental health. Training programs for professionals could integrate awareness of objectification processes, which would allow professionals to recognize and address subtle forms of objectification that may be harmful. Moreover, attention and sensitivity should guide medical and casual commentary on pregnant women's bodies, as such messages may inadvertently contribute to perceived interpersonal objectification. Unless medically relevant, healthcare providers are encouraged to use supportive, non-appearance-focused language and to frame body mass changes as normative and functional, rather than aesthetic problems. Such approaches can foster healthy perceptions of pregnant bodies.
At a broader societal level, it is crucial to normalize the physical changes associated with pregnancy in a culture that emphasizes physical attractiveness. Public health campaigns, media literacy programs, and informed interventions can play a role in reshaping societal attitudes and associated behaviors towards promoting healthier perceptions of pregnant bodies. Advocacy efforts are needed to counter cultural messages that overemphasize appearance during pregnancy. Together, these efforts may help create a social environment in which objectification is reduced and a healthier perception of pregnant bodies is promoted.
Limitations and Future Research
Several limitations need to be considered. First, the study relied on a convenience sample of heterosexual, highly educated, pregnant, cisgender women from average to above-average socioeconomic backgrounds, which may limit the generalizability of the findings. It is important to acknowledge that pregnancy is also experienced by non-cisgender transgender men and non-binary individuals, who may also encounter objectification related to childbearing. Future research should extend the scope of objectification theory to include individuals with other gender identities, whose lived experiences may also be shaped by appearance-based expectations during pregnancy. Future studies may benefit from targeted recruitment through community health centers, clinics, or organizations serving under-resourced populations to ensure more inclusive sampling.
A second limitation concerns the variables examined. This study focused on body mass-related appearance changes; however, pregnancy can also entail other appearance-related changes that can lead to different forms of appearance focus (e.g., positive culturally constructed commentary such as “pregnancy glow”). Future research may examine how such experiences influence women's bodily experiences and psychological outcomes during pregnancy. Moreover, this study included only two proposed mediators (body shame, interoceptive awareness) in the examined model; however additional mediators may also be relevant during pregnancy (e.g., appearance anxiety) and should be considered in future research.
A third limitation concerns our use of a BMI-based indicator of gestational body mass gain. We chose this measure to account for individual differences in height that affect the visibility and appearance associated with weight gains. However, it should be noted that BMI is an imperfect index that may misclassify women with higher muscle mass, atypical proportions, or distinct body compositions (Wu et al., 2024) and may not accurately reflect individuals of color, as racial and ethnic groups differ in body composition and fat distribution at the same BMI (Heymsfield et al., 2016). Moreover, gestational weight gain reflects multiple physiological processes (e.g., fetus, placenta, fluid, and blood volume) that BMI cannot distinguish. Future research should use precise markers, such as gestational weight gain charts or clinical indicators, that can provide complementary insights.
Fourth, the cross-sectional design precludes any conclusions about causality. Although associations were observed among body mass gain, objectifying experiences, self-objectification, and mental health outcomes, the directionality of these associations remains unclear. Future studies should adopt prospective longitudinal designs to establish temporal associations among the study variables, as well as to explore the trajectory of sexual objectification (both environmental and interpersonal), self-objectification, and related constructs before, during, and after pregnancy. Specifically, it may be worthwhile to investigate different sources of interpersonal objectification (e.g., partners, family members, healthcare providers, strangers) and their potentially unique effects on pregnant women's psychological experiences. Relatedly, additional research may examine how social media representations of baby bump photos, pregnancy fitness, and “yummy mummy” ideals shape sense of self and pressure to perform femininity.
Finally, measurement-related limitations must also be considered. First, the applied measures were all developed in English with U.S. samples, and only some of them underwent validation for the population sampled in the current study. Because the constructs they assessed may be culture-specific, the measures may introduce measurement bias. An additional limitation concerns the differing timeframes of the mental health outcome measures which may have introduced variability and affected the comparability of the measures and the observed associations. The measures of interpersonal objectification (i.e., ISOS) and interoceptive awareness (i.e., SBC) were adapted for the current study, and their psychometric properties have not been fully validated in pregnant populations. In addition, the study did not assess or control for the participants’ frequency of involvement in sexual activity, which may be reduced during pregnancy. The study also did not assess participants’ self-objectification, body shame, interoceptive awareness, or mental health prior to pregnancy. It is possible that for some women, pregnancy merely amplifies long-standing patterns of self-objectification and body shame concerns developed earlier in life (Rodgers et al., 2024). As a result, it is difficult to determine whether the observed findings reflect pregnancy-related changes or pre-existing individual differences.
Conclusions
This study underscores the relevance and applicability of objectification theory in the context of pregnancy. The findings shed light on a potential source of perceived interpersonal objectification during this period by demonstrating how elevated body mass gain was associated with perceived interpersonal objectification, which in turn was associated with heightened self-objectification. By examining all proposed mental health outcomes of objectification theory within a single model, this study offers a comprehensive contribution to existing literature. The structural model provided support for objectification theory's relevance to pregnant women's experiences, particularly in explaining disordered eating behaviors. In contrast, the model explained relatively little variance in depressive symptoms and sexual dysfunction, suggesting that the proposed mediators (body shame and interoceptive awareness) may not fully capture the pathways linking self-objectification to these outcomes. Notably, self-objectification itself emerged as a robust correlate across all three mental health outcomes, reaffirming its central role in understanding the psychological experiences of pregnant women.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Israeli Science Foundation, (grant number 795/23), awarder to Rotem Kahalon.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.