
Abstract
Access to medication abortion—the use of medications rather than a surgical procedure for pregnancy termination—is an essential reproductive healthcare service. Following the overturn of Roe v. Wade and federal abortion protections in the United States, medication abortion and telemedicine for abortion are increasingly vital. Black, Latinx, and lower-income women in the United States already experience disproportionate barriers to abortion care and interpersonal and structural violence—interconnected, social systems that police bodily autonomy. This current study examined qualitative data from a larger community-led, reproductive justice project on medication abortion perspectives among Black and Latinx women in a large, urban center in Georgia. We used thematic analysis to examine interviews (N = 82) with key informants (n = 20) and interviews (n = 32) and focus groups (n = 30) with Black and Latinx women ages 18–51 years. Four violence-related themes were identified: (a) sexual assault and intimate partner violence as reasons for abortion; (b) reproductive coercion by partners and family members; (c) reproductive coercion by predominantly White providers; and (d) abortion bans, the legacy of enslavement, immigration enforcement, and poverty as structural violence. Shifting family planning care to be patient- and community-centered, in conjunction with policy advocacy to change oppressive systems, is critical.
Keywords
Safety and abortion are inherently intertwined components of reproductive autonomy: eradicating violence necessitates access to the full spectrum of reproductive health care including abortion, and improving equitable access to patient-centered abortion care requires careful attention to violence at all socioecological levels. Between 6% and 22% of abortion patients experience intimate partner violence (IPV; i.e., psychological, physical, and/or sexual violence by an intimate partner). The experience of IPV significantly increases the odds of unintended pregnancy and abortion (Pallitto et al., 2013) as survivors of IPV are more likely to experience sexual violence and reproductive coercion, including contraceptive sabotage, pressure to become and stay pregnant, and occasionally, although less commonly, pressure to have an unwanted abortion (Chibber et al., 2014; Samankasikorn et al., 2019). Moreover, being denied a wanted abortion is associated with an increased likelihood of still experiencing violence from the partner involved in the pregnancy two and a half years later (Roberts et al., 2014). Further, approximately 15% of rapes lead to pregnancy each year (Basile et al., 2022), and 1% of abortion patients report their pregnancy is the result of rape and <0.5% due to incest (Kirkman et al., 2009; Roberts et al., 2014; Saftlas et al., 2010).
There are also significant racial/ethnic and economic inequities in both abortion access and violence victimization. Women 1 of color and those living on lower incomes are more likely to experience IPV, sexual violence, and reproductive coercion (Bryant-Davis et al., 2010; Chamberlain & Levenson, 2013; Samankasikorn et al., 2019; West, 2004). At the same time, women of color and women living on lower incomes are both more likely to need abortion care—in part due to racialized poverty—and are more likely to experience barriers to wanted abortions (Dehlendorf et al., 2013; Dehlendorf & Weitz, 2011; Mosley, Ayala, Jah, Hailstorks, Hairston, Dixon Diallo et al., 2022; Thompson, Young et al., 2022). For those communities, reproductive autonomy—that is, “individuals’ ability to be fully empowered agents in their reproductive needs and decisions and to access reproductive health services without interference or coercion” (Senderowicz & Higgins, 2020, p. 147)—is highly constrained by restrictive abortion policies (e.g., state-level abortion bans, preclusion of federal abortion funding due to the Hyde amendment) and austere social divestment (e.g., limited or nonexistent social safety net; Rice et al., 2021; Thompson, Young et al., 2022).
Traditionally, the reproductive rights movement, particularly in the United States (U.S.), has centered White middle-class women and focused on legal access to abortion and contraception, much to the detriment of communities marginalized by racism and classism (Luna & Luker, 2013; Ross, 2006). Communities of color and lower-income communities have long been the targets of population control and eugenic policies and culture including coerced and forced sterilizations (Harris & Wolfe, 2014; Luna & Luker, 2013; Roberts, 1997; Ross, 2006; Schoen, 2006). The reproductive justice theory and social movement, founded by Black U.S. women in response to the White-centric reproductive rights movement, uses a human rights (rather than a legal rights) approach and emphasizes the rights to have children, to not have children, to raise children in safe and supportive environments, and to do so with bodily autonomy free of violence and coercion from individuals or the state (Asian Communities for Reproductive Justice, 2005; Luna & Luker, 2013; Ross, 2006; Ross et al., 2017; Ross & Solinger, 2017). In the reproductive justice framework, abortion and contraception are equally valued as paid parental leave, antipoverty initiatives, and prison abolition. Furthermore, reproductive justice leaders have championed the need for community-led research in the realm of family planning to infuse this holistic human rights paradigm, uplift Black and other marginalized voices, and to apply an intersectional lens that considers not only gender discrimination but also simultaneously inequities based on race, ethnicity, class, and other social axes (Mosley, Ayala, Jah, Hailstorks, Dixon Diallo et al., 2022; Mosley, Ayala, Jah, Hailstorks, Hairston et al., 2022; Rice et al., 2021; Thompson, Northcraft et al., 2022). Reproductive justice applies a socioecological approach that emphasizes structural and political determinants of reproductive and community health (Crear-Perry et al., 2021). Therefore, a reproductive justice investigation of abortion and violence shifts focus from only interpersonal violence to also include structural violence, which Farmer (2004, p. 323) defined as “the social machinery of oppression” (e.g., racism, sexism, classism) that “constricts the agency of its victims” through social policies, norms, and institutions at the macro-level. In addition to maintaining oppression and inequities, structural violence can create interpersonal violence including normalizing power inequities that excuse violence—such as the hypersexualization of Black women that is then used to excuse their sexual violence experiences—and the absence or elimination of social programs that directly and indirectly prevent and respond to violence—such as lack of resource investment in communities affected by violence (Montesanti & Thurston, 2015).
Access to the full spectrum of reproductive health services is a prerequisite of reproductive justice, and this includes surgical abortion as well as medication abortion—the use of medications (typically mifepristone and misoprostol) for pregnancy termination. Following the U.S. Supreme Court decision to overturn Roe v. Wade and federal abortion protections, medication abortion and telemedicine for abortion are increasingly vital as access to surgical abortion severely declines in the wake of state-level abortion bans (now effective in 13 of the nation's 50 states; Center for Reproductive Rights, 2022). Emerging research on medication abortion access has indicated there are stark disparities by region, race/ethnicity, and socioeconomic status (Allsworth, 2022; Mosley, Ayala, Jah, Hailstorks, Hairston et al., 2022; Thompson, Young et al., 2022). Moreover, given the historical and ongoing inequities, it is imperative to employ a reproductive justice and human rights approach to family planning research, although there is a dearth of community-engaged research at the intersection of violence and abortion care, particularly medication abortion. To address these gaps, the study team conducted the Georgia Medication Abortion (GAMA) project using a community-led reproductive justice approach to explore Black and Latinx
2
women's perspectives of and experiences with medication abortion in Georgia. For the analyses presented in this study, more specifically, the team analyzed violence-related data from the GAMA project to answer:
How do Black and Latinx women describe experiences of interpersonal violence, including reproductive coercion, in the context of medication abortion? What are the roles of structural violence in access to medication abortion for Black and Latinx women?
Method
Approach and Setting
The GAMA project employed a critical research paradigm (Mash, 2014; Wiener, 2022)—specifically adhering to the tenets and methodologies of community-engaged participatory action research and intersectional reproductive justice research (see Mosley, Redd et al., 2022 for more details about this paradigm). The project was led by Black and Latinx women at SisterLove, a Black-led, reproductive justice and HIV organization in Georgia. It was supported and guided by academic researchers as well as a Community Advisory Board (CAB) comprised of eight Black and Latinx women, abortion providers, religious leaders, and leaders from Black and Latinx community organizations including Caminar Latino which works on education, support, and prevention around violence in the Latinx community. The CAB helped refine the study's research questions, develop data collection instruments, recruit participants, review preliminary results, and disseminate findings in the community (including a psychoeducational video), through publications, and at conferences and workshops. This study was set in a large, urban area of Georgia, a highly diverse 29-county urban center in the Southeastern U.S., where abortion is highly restricted (Mosley, Ayala, Jah, Hailstorks, Dixon Diallo et al., 2022) and rates of intimate partner, sexual, and community violence are high—particularly during COVID-19 (Atlanta Police Department, 2022; Evans et al., 2021; Fox 5 Atlanta Digital Team, 2022; Stevens, 2022). All study procedures were approved by Emory University's Institutional Review Board in January 2019.
Data Collection
For the GAMA study, the research team collected data from April 2019 to December 2020 through 20 key informant interviews, 32 in-depth interviews with Black (n = 16) and Latinx (n = 16) women, and six focus groups with Black (n = 4, 4, and 5) and Latinx (n = 8, 5, and 4) women. Interviews and focus groups were conducted either in English, Spanish, or a combination of the two languages, based on the preference of the participant(s). Key informants were defined as abortion providers broadly—including three physicians, three front desk receptionists, two nurses, two health educators, and two clinic administrators (n = 12)—and leaders of Black (n = 4) and Latinx (n = 4) community-based organizations. They were recruited through the CAB, emails to local abortion clinics, and emails to other Black and Latinx community-based organizations partnering with SisterLove on this and other projects. Black and Latinx women were also recruited for the community member interviews and focus groups through a community-based recruitment strategy including partnerships with community-based organizations and abortion clinics, social media, radio ads, and flyers in community settings including hair and nail salons, commercial centers, and university student lounges.
The interview and focus groups guides have been previously published (Mosley, Ayala, Jah, Hailstorks, Hairston et al., 2022). Briefly, the key informant interviews with abortion providers explored their experiences serving Black and Latinx abortion patients including medication abortion, barriers and facilitators of medication abortion among Black and Latinx communities, policy determinants of abortion access, and integration of medication abortion education and services into other existing health and social services. Key informant interviews with community-based organization leaders explored their organization, services provided, communities served, knowledge of medication abortion, community discourse and attitudes around medication abortion, barriers and facilitators of medication abortion including stigma, medication abortion and self-managed stories, policy determinants of abortion access, and integration of medication abortion into their community-based services. Focus groups with Black and Latinx women (i.e., community members) then explored knowledge and language of medication abortion, barriers and facilitators of medication abortion, social networks and support, attitudes and social norms toward medication abortion including stigma, and ideal ways for people to learn about and access medication abortion. In-depth interviews explored topics very similar to the focus groups, but they inquired about personal experiences with medication abortion and stories of self-managed abortion. Due to the sensitive nature of personal experiences with abortion, these questions were limited to individual interviews. Because interviews and focus groups with Black and Latinx community members primarily referenced their own experiences or the experiences of close friends, while key informants discussed observed experiences of Black and Latinx women, the results present key informants’ data separately and combined data from community members’ individual interviews and focus groups.
Analysis
Interviews and focus group discussions were audio recorded, transcribed, and (if needed) translated into English verbatim for qualitative data analysis. Transcripts were then thematically analyzed using iterative and team-based memo-ing, coding, and diagramming. The analytic team included two Black and Latinx women in leadership positions at SisterLove, one White female academic researcher who co-led the study, one Black female OBGYN abortion provider (also a Co-Investigator on the study), and 13 Black and Latinx Master of Public Health student interns. Following the Sort, Sift, Think, Shift protocol (Maietta et al., 2021), which draws from qualitative traditions of narrative analysis, phenomenology, and grounded theory, and using Dedoose qualitative software, the team (1) created memos for each interview including a list of important topics; (2) compiled the list of important topics—a combination of both deductive and inductive—into a preliminary codebook; (3) used the codebook to horizontally code across the transcripts, where each transcript was analyzed by two coders who met to reconcile and come to 100% agreement (i.e., they coded independently and then met in real time to discuss discrepancies in their coding until they reached consensus for all codes across the entire transcript; any ongoing discrepancies were discussed in the weekly team meetings; all final coding decisions were made by the two SisterLove leaders); (4) developed analytic memos for each code; (5) investigated code co-occurrence where two topics commonly intersected using matrices; (6) explored group differences in codes such as by race/ethnicity using matrices; and (7) developed higher level themes from connections among the codes and group differences using diagramming and group discussion.
Violence—including sexual violence, IPV, and abortion restrictions as structural violence—inductively emerged as an important topic during Step 1 of analysis and was then integrated into the codebook as an inductive code, explored through an analytic memo and group difference analyses, and then led to higher level themes, which became the basis of this manuscript. Interpersonal violence—such as sexual assault, reproductive coercion, and IPV—and structural violence are interconnected and both involve deliberate harm to others; however, within structural violence, harm occurs due to unequal distribution of power and is integrated into the larger norms, procedures, and policies of society to maintain inequity (Rylko-Bauer & Farmer, 2016). Consistent with this literature, participant statements were coded as consistent with structural violence if the statement referred to harm that was disproportionately experienced by a marginalized group or groups and was the result of large-scale social processes, rather than interactions between individuals. Notably, in line with the critical research paradigms of intersectional reproductive justice and community-based participatory action research, the team employed intersectionality (Crenshaw, 1989; Ross et al., 2017) and knowledge justice (Smith & Millspaugh, 2015) epistemology in the analysis. For example, the intersectional positionality of each research participant (e.g., race, ethnicity, and economic background) was used to contextualize and interpret their speech, while structural factors including abortion policy were interrogated as they construed differential effects according to each participant's intersectional identities and experience of social privilege and oppression. Moreover, the analysis focused on participants’ own interpretation and description of their subjective experiences (i.e., not objective “facts”)—thus creating community-based knowledge about medication abortion and challenging traditional paradigms of knowledge being controlled by physicians or other highly privileged groups.
Positionality and Reflexivity
The current study on medication abortion among Black and Latinx women in Georgia is led by SisterLove, in close partnership with Black and Latinx women, Black and Latinx community-based organizations, and abortion providers serving those communities. The study was originally conceptualized by a Black Latinx lawyer ([SA], a leader at SisterLove) with support from the Director of SisterLove (DDD, a Founding Mother of reproductive justice). The study director (ZJ) was a Black Latinx public health professional, and she was supported by a diverse team of Black and/or Latinx public health students. Data collection was conducted by the study director, student interns, the second author (SA), and the last author (EAM). The study was supported by academic researchers from Emory University, specifically two non-Latinx White women (KSH and EAM) and one non-Latinx Black OBGYN abortion provider (TH), who received reproductive justice training from SisterLove and provided ongoing training in qualitative data collection, positionality and reflexivity, and analysis. As such, the study team largely reflected the Black and Latinx communities upon which this research is focused. After each interview and focus group, the facilitator completed a debrief form including prompts for reflexivity about one's personal experiences, assumptions, and how those might have influenced the participant interaction and the researchers’ interpretations of the data. Quarterly CAB meetings provided regular opportunities for reflexivity by the study team, especially our unique insider–outsider position as researchers and community members (Newman et al., 2011; Dwyer & Buckle, 2009). Finally, this manuscript's first author (ECN) is a non-Latinx White psychologist who researches violence, including racial/ethnic and economic disparities, from a reproductive justice perspective.
Results
Of the 82 socioeconomically diverse, predominantly Black and/or Latinx women (see Table 1 for demographics) in the study, most discussed issues related to interpersonal and structural violence and medication abortion and abortion access in general. The larger study focused on medication abortion in general, thus discussions on the role of interpersonal and structural violence in medication abortion and abortion care overall were unprompted. Four themes were identified: (a) sexual violence and IPV as reasons for abortion; (b) reproductive coercion by partners and family members to maintain or terminate a pregnancy; and (c) reproductive coercion by predominantly White providers regarding birth control and denying access to medication abortion; (d) restrictions such as abortion bans, immigration enforcement, and poverty as structural violence. We have provided demographic information pertaining to racial identity, Latinx identity, and age for participants’ direct quotes from individual interviews. Demographic data were collected from focus group participants in the aggregate, but individual demographic information cannot be linked to specific quotes from focus group participants.
Demographics of the Georgia Medication Abortion Project Including Key Informant Interviews, In-Depth Interviews, and Focus Groups.
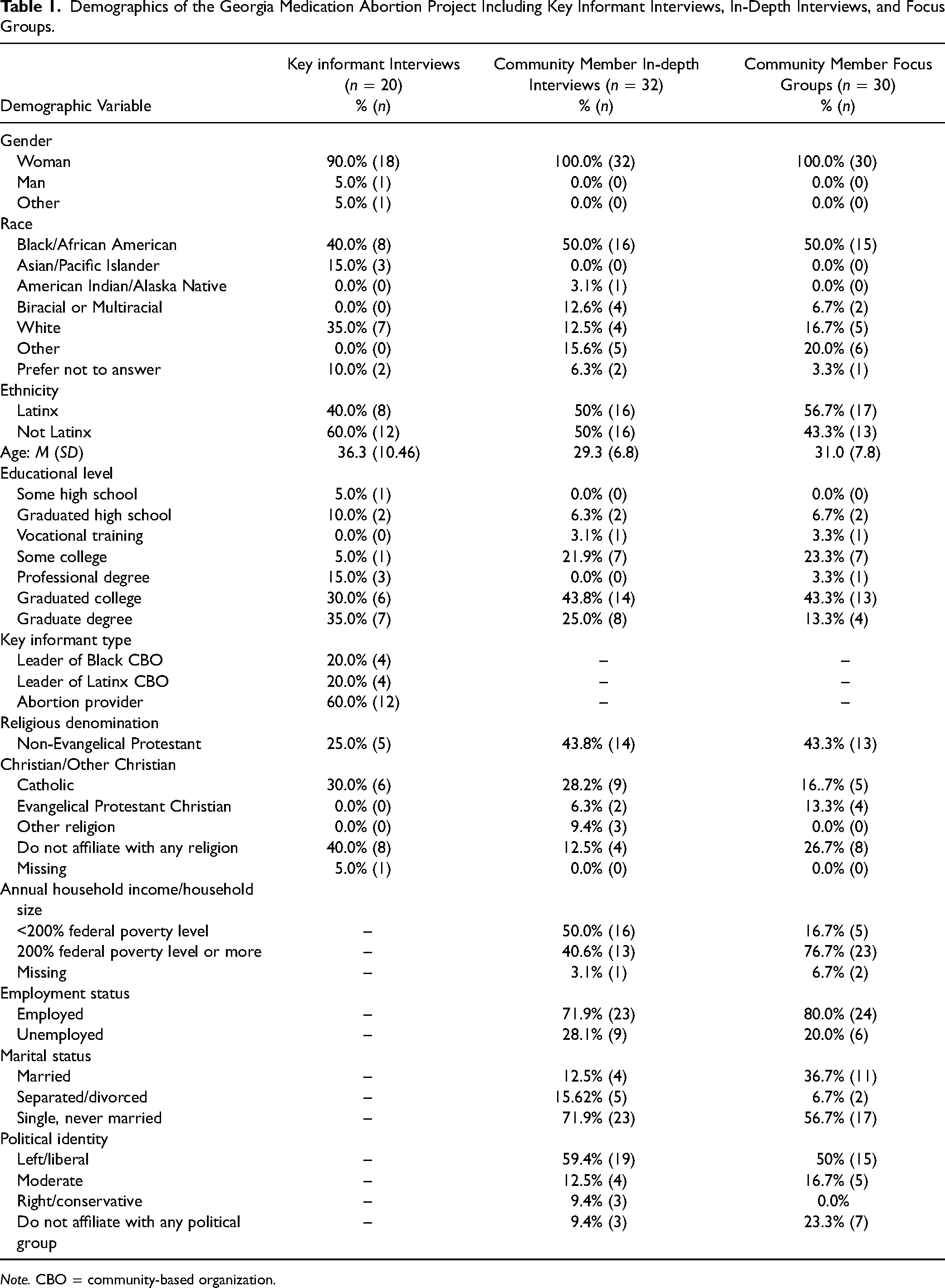
Note. CBO = community-based organization.
Theme 1: Sexual Assault and IPV as Reasons for Abortion
Key Informants
Abortion in the context of sexual assault and IPV was discussed by nine key informants as part of the landscape of abortion care. Although sexual assault and IPV were not directly asked about by interviewers, when providing examples of women who seek abortion services within their clinics, five of the 12 key informants who worked as abortion providers (physicians, nurses, receptionists, administrators, health educators) spontaneously referenced patients who had been raped or were experiencing IPV as reasons for their abortions. Four of the eight community leaders also referenced sexual assault and IPV as contexts in which abortion services were necessary. One Latinx community-based organization leader stated that she herself was in a relationship that contained IPV. She then stated, “this is why I was so distressed as I was going to have another baby in that circumstance, and that is why I thought about [abortion]” (White, Latinx, 53 years old). She added that the perception of abortion as acceptable when it is the result of sexual assault or IPV is found within members of the Latinx community. She added that abortion remains very stigmatized in Latinx communities and “the only time abortion is mentioned is when it is related to domestic violence.” Similarly, one Black community-based organization leader noted that while abortion is negatively perceived and stigmatized within many religious institutions (which influences individual attitudes), there is the presence of “some churches that will feel that you should have an abortion if you are raped” (Black, non-Latinx, 35 years old).
Community Members
When discussing perceptions of abortion, including medication abortion, multiple community members emphasized abortion in response to rape or sexual assault was “an option [women] need to have” (Black, non-Latinx, 42 years old). Overwhelmingly, these viewpoints did not vary based upon the participants’ personal identification as being in support of or against abortion. In an interview, one community member indicated that she advocated for the option of abortion to the family of a rape survivor she knew, stating, “I was like, ‘she's very young, and she was raped by this older man.’ She could terminate the pregnancy” (White, Latinx, 26 years old). Two community members within a focus group comprised of Latinx community members empathized with those who were pregnant due to rape, with one referencing her own attempted rape and how distressing it would be to discover she was pregnant. One member of a different focus group comprised of Black community members indicated she had known friends who became pregnant as a result of rape, and another reflected on how she would respond in that situation, stating, “I can’t really say that should I be in that situation that I would keep the baby. I can’t honestly say it, because I’d be so emotionally wrecked.” Another community member expressed concern about the welfare of a child who was the product of rape, stating “the child is a product of rape, how is its mother going to treat it, because it was something that she did not expect, and it was an event that she would want to forget. And who knows how the mother would react to the child” (White, Latinx, 30 years old). Several referenced family members or friends whom they consider “pro-life,” however, noted that those family members or friends “definitely understand the situation if the person was sexually assaulted” (Black, non-Latinx, 22 years old), suggesting participants believed this viewpoint (i.e., rape as a reason for abortion) to be relatively common. One community member in a focus group noted that she also understood abortion in cases of IPV (White, Latinx, 28 years old) to which other members agreed.
Theme 2: Reproductive Coercion by Family/Partner to Maintain or Terminate a Pregnancy
Key Informants
Multiple key informants discussed witnessing reproductive coercion in which a patient's partner, family, or community attempted to leverage power to influence the decision to maintain or terminate a pregnancy. Broadly, one abortion provider noted that a partner's views and threats to not contribute financially to an abortion prevent patients from accessing abortion (Black, non-Latinx, 29 years old). Another abortion provider described a scenario where a patient, who was currently in a violent relationship, scheduled an abortion appointment to occur when her partner thought she would be at work, and as the appointment was lengthier than she anticipated, the patient began to panic out of fear he would find out. Speaking generally about reproductive coercion, one community leader stated if “you don’t want to raise children in this relationship, so you’re terrified, but your significant other or whomever is beating you wants you to have the baby, it's not like you’re going to be able do what you need” (Black, non-Latinx, 35 years old). In contrast, one community-based leader (White, Latinx, 28 years old) noted that community members who do outreach regarding domestic violence observed a woman whose partner attempted to “forced [her] into [an abortion]…as another way to try and control her.” She added that once it became clear that her partner had forced her to come to the clinic, and the woman did not understand what was occurring, the procedure was halted (White, Latinx, 32 years old). Another community-based leader described coercion and abuse from the parents of a pregnant woman and stated that the parents beat the woman almost every day in hopes of inducing a spontaneous abortion.
Several leaders noted that reproductive coercion also occurs through gender and relationship socialization within communities, and they emphasized Latinx communities. One community leader (Race Not Indicated, Latinx, 39 years old) highlighted power dynamics may occur at home and she has observed husbands saying, “no she cannot take [birth control].” She added that community workers commonly observe “men being in charge of the reproductive lives of their wives, and controlling how many kids they wanna have.” She added that when conducting workshops, women ask if their husbands would be aware of their chosen birth control method, with the connotation of wanting to hide this from their husbands (Race Not Indicated, Latinx, 39 years old). Another Latinx leader (White, Latinx, 53 years old) stated that “we are still rooted in many ideas that we bring from the family that they do not change…[abortion] will be frowned upon by families, the family will not see it well, or the community will not see it.” She added that abortion is linked to larger ideas about gender socialization: “We see [family, community, and religion] influencing when domestic violence is happening. Telling [women] he is your cross, you looked for him, stay with him, you have to endure it, to be there, I think those things influence [abortion]” (White, Latinx, 53 years old).
Community Members
One community member explicitly referenced reproductive coercion by a partner, with one highlighting the role of power and control at the center of coercion. She indicated that she had an abortion because she became pregnant after her boyfriend tampered with a condom. She stated that when she told him that she was devastated to be pregnant, “he revealed to me later that he had poked a hole in the condom because he didn’t want me to leave. He thought that I was going to respond like, ‘oh this is how much you love me?’” (Black, Latinx, 41 years old). She stated that he continued to pressure her not to get an abortion, such as telling her he had dreams of the fetus telling him not to kill it. The same woman later referenced a friend who had two abortions, and when she had planned to continue her third pregnancy, her boyfriend stated that she needed to have an abortion. Several community members noted that if someone was experiencing IPV, obtaining an abortion would be challenging because of the violent partner's power and influence.
Theme 3: Reproductive Coercion by Predominantly White Providers
Key Informants
Three key informants discussed power and medical racism within abortion care, access to different types of abortion care, and reproductive coercion. One abortion provider (Black, non-Latinx, 46 years old) noted that a physician may believe one form of abortion care is the best in a certain circumstance, and “use their power position.” She indicated, “if that physician, depending on how he or she looks at it, determines the best option is medication abortion…they’re in the power position to disseminate that information in a way that could influence her.” One abortion provider noted that this applies to birth control and referenced, Some of our staff who were working in clinics were seeing people during counseling being asked if they wanted to have an IUD put in, and [discussing] research happening to get it put in for free, or there was grant funding where they could get it put in for free, but if people wanted it removed they would have to pay for that, and so it was just like, if they were able to get it in for free, why can’t they have it removed for free…We have to [remember] like these racist notions about family planning aren’t okay, and people have to be able to do what they want for themselves and their body. (Black, non-Latinx, 29 years old).
Community Members
When asked what may contribute to difficulties accessing abortion services, one community member stated, “Medical racism. I feel like doctors feeling like they can persuade women or not listening to women's voices when they’re talking about what their body needs” (Black, non-Latinx, 22 years old). None of the community members described occurrences in which providers attempted to convince patients to have an abortion, but rather providers did not universally provide comprehensive information about the types of abortion. Persons presenting for care perceived that options were not discussed in a manner that afforded them the opportunity to review all available methods of termination to determine which best fit their needs at the time. One Black, Latinx woman in a focus group described her medication abortion after a “Caucasian male doctor [told] me, ‘hey your pregnancy is not viable, you need to take this.’” She indicated feeling that she did not receive information on it, and feeling bullied and dehumanized. One community member noted that doctors may “choose for you” regarding what type of abortion service (Black, non-Latinx, 27 years old). She reflected on her own abortion experience and stated that she did not receive information on the different types of abortion. She indicated that they provided some cursory information on medication abortion (vs. surgical abortion); however, “they kind of almost decided for me or it was like a forced decision, but they’ll just [say], ‘Oh well you’re probably going to want this so let's just do that’” (Black, non-Latinx, 27 years old). She stated that she later researched the different options and would have preferred a medication abortion in contrast to a surgical abortion. Notably, another participant commented that the nurse practitioner did not give the option of medication abortion, but she did not mind that because she felt the nurse thought it would be a faster experience (Black, non-Latinx, 41 years old).
Several women reported reproductive coercion and medical racism regarding birth control. One participant stated: I also feel that I was also rushed into then getting this birth control shot that I didn’t fully consent to on the day of my abortion. I feel like all that really messed with my body… I don’t know if I felt forced more so like I didn’t fully consent to it. It felt almost like a punishment. Like, “Let's make sure we shoot you up, so it doesn’t happen to you.” Even not knowing, I would have wanted to read up more on the shot because I’ve never had a birth control shot before. And understanding the history of it, the ways in which its been used to sterilize Black women, etc. I just wanted to know the dosage, all those little details. It was hard for me to just ask for because I was already overwhelmed by going through [my abortion]. It was this secondary thing that I was like, maybe just got to get through this too. (Black, non-Latinx, 24 years old)
Theme 4: Abortion Bans, Poverty, Legacy of Slavery, and Immigration Enforcement as Structural Violence
Key Informants
Overwhelmingly, providers and community organization leaders indicated that policies to restrict and ban abortions—including Georgia's (at the time) injuncted 6-week gestational age limit—disproportionately affect Black and Latinx communities, with several noting this was purposeful. One provider noted, “it's (Georgia's new abortion law) going to impact the people that get abortions and because the majority who get abortions are lower income and people of color, then it's going to disproportionately affect them because they are the ones with access issues” (Black, non-Latinx, 34 years old).
Providers and community organizers noted that gestational bans—especially Georgia's (at the time) impending 6-week limit, 24 h waiting periods, and multiple ultrasounds create obstacles for all people. However, they also noted that abortion procedures are expensive and often require multiple appointments, which increase the costs due to transportation and time off work. Thus, these restrictions intersect with the barriers that Black and Latinx pregnant individuals face, including the disproportion likelihood of living in poverty and lacking insurance, to create even greater obstacles to access care. One provider noted that patients will need to save money for both the procedure and logistics, which delays care to the point where they may be unable to get an abortion because they are past the state-imposed, previable, gestational limit. Overall, when discussing barriers to abortion care for Black individuals, one leader indicated, “basically all the things that make life harder for Black people in this country will be playing out why accessing abortion is harder for them” (White, non-Latinx, 27 years old). Two providers noted that Black women are vulnerable to several gynecological risk factors, such as fibroids and conditions that influence menstrual cycle regularity, which influences how early one may notice they are pregnant. One provider noted the percentage of birth complications among Black and Latinx women and added that policy makers consider this disparity when making these abortion restrictions and bans, suggesting they are purposefully imposing these restrictions and bans to worsen Black and Latinx birth complications. One community leader also noted that White women are more likely to have the resources to travel to another state to obtain abortion care, and an abortion provider noted that White woman are also more likely to be provided with resources, such as pain medications, or have preexisting resources, such as a comfortable home environment, to cope with any discomfort of medication abortion.
When discussing barriers to abortion care for Black women, several providers and community organizers referenced the lack of healthcare services for Black communities and legacy of genocide and slavery. One community leader stated, “particularly in the South, because we have this legacy of slavery, Jim Crow, and everything, we know that there is a disproportionate number of healthcare services available to people of color, period” (Black, non-Latinx, 41 years old). Two community leaders noted that there is also uncertainty regarding the use of medication abortion because it is new. One leader noted, “we’re always comfortable with what's familiar, so when they look at it, they are just like, ‘oh my god that's just another way to get rid of our generation. That's just another way to annihilate us.’” (Black, non-Latinx, 49 years old). Two providers discussed the origins of abortion access and family planning in eugenics, and one provider referenced the Tuskegee Syphilis Study, noting that it resulted in many Black women becoming sterile (due to contracting syphilis from their husbands, who participated in the study and were denied treatment by the research team).
When discussing barriers to care for Latinx women, providers and community leaders overwhelmingly referenced immigration enforcement as a barrier to care—“fear of raids. Fear of being detained. Taken, you know, away from their families and children. Because it has happened” (Race Not Indicated, Latinx, 39 years old). One provider noted that Latinx women are not able to cross state lines to access abortion care or will decline abortion funds because they are fearful this will be discovered by immigration enforcement, and two community organizers heard women express fears that abortion care could influence the immigration process. One provider noted that “there is a sense that people are disposable” within the work environments that Latinx people are often in, which are often low-paying, do not offer time off, and do not facilitate accessing any form of medical care (White, non-Latinx, 47 years old). One provider noted that the intersection of structural violence through immigration intersected with IPV for a woman who was 26 weeks pregnant and delayed care. Providers and community organizers also noted that the lack of Spanish-speaking services is a barrier to care, as several indicated they employ interpreters, but often feel that it is less ideal than having Spanish-speaking staff.
Community Members
Community members discussed the intersection of racism, classism, and misogyny as factors that contribute to the lack of access to abortion services. Several participants and individuals within two focus groups noted that Black and Latinx communities are more likely to experience poverty and are less likely to have health insurance that covers abortion care. They stated this impedes one's ability to access abortion care, with one participant noting, “a lot of time race or socioeconomic class is impacted by race too because the racism and the ways in which capitalism play together to keep people suppressed” (Black, non-Latinx, 24 years old). Several participants noted that women of color experience this institutional oppression along with misogyny in response to seeking abortion care, noting, “we’re taught that your life has to go a certain way…if you do become pregnant, it's like, ‘this is the life for you…people just expect women to have kids, especially women of color” (Race Not Indicated, Latinx, 26 years old). One community member stated that the politics of abortion—specifically the 6-week gestational age limit that had been passed but not yet enacted in Georgia—are “shaped around White supremacy, how capitalist or neo-capitalist ideas of, ‘I can tell you what to do with your body.’ Like this is something that I control. We control land, we can control property, we can control your body” (Black, non-Latinx, 22 years old). Similar to providers and community organizers, several participants and individuals in focus groups discussed the legacy of slavery and sexual violence that contribute to the lack of access to abortion for Black women: In the Black community specifically, I think we’re especially suffering with the lack of education, lack of knowledge because of sexual trauma we’ve collectively experienced as a race in America. We have a problem talking about sex…We need to start talking about it. We need to start talking about the trauma that happens so we can get over it. Rape during slavery happened, and not just to women. It happened to men as well. (Black, non-Latinx, 41 years old)
Within both interviews and focus groups, community members discussed experiences of racism and misogyny within the medical field, which they believed contributed to stigma regarding abortion. Several women noted that lack of access to overall medical care is a barrier for many Black and Latinx people, with several community members specifying that for abortion care that “if you can’t find a clinic or there's no Black folks there, it makes it more difficult because the medical field is racist just like the rest of the world” (Black, non-Latinx, 24 years old). Several individuals in interviews and one focus group also discussed experiences of feeling judged as part of the “hypersexualization of Black women and girls” within their interactions with providers (Black, non-Latinx, 24 years old). One community member indicated that judgment within the medical field interacts with abortion policies, such that the questions providers are required to ask (i.e., “Are you sure?” “Come back in 24 h and let's see if you are still…if you wanna go through with this”) create barriers in which women change their minds “because they are like, ‘I don’t want to deal with that scrutiny again and that judgment’ because they probably do feel judged” (Race Not Indicated, Latinx, 26 years old). Finally, one focus group and three community members in interviews discussed the lack of access to abortion care within private insurance companies and OBGYN practices contributes to the stigma and lack of access to abortion care.
Discussion
In the current study, we used qualitative data from a larger reproductive justice study on medication abortion among Black and Latinx women in Georgia to examine the intersection of interpersonal and structural violence and abortion among key informants and community members. One advantage of a structural violence framework is it highlights how macro-level violence, which is often invisible, intersects with other forms of violence, which are more readily visible, to cause disproportionate harm to certain groups and maintains inequity (Rylko-Bauer & Farmer, 2016). Our study attempts to center the experiences of Black and Latinx individuals, who are disproportionately impacted by abortion bans, including increased risk of maternal mortality (Stevenson, 2021). It is notable that the larger study did not intend to investigate violence and abortion; the spontaneous mention of interpersonal violence as well as the injustice, inequity, and suffering that characterize structural violence potentially suggests that abortion bans, racism, and violence are inextricably linked. Overall, the current findings reflect the deleterious outcomes that interpersonal and structural violence has upon the autonomy of Black and Latinx pregnant individuals, which are made all the more chilling in the knowledge that they will likely worsen following the recent Dobbs v. Jackson ruling that eliminated constitutional protections for abortion. Although our data collection (April 2019–December 2020) was finished before the Dobbs decision, our team was in the field conducting interviews and focus groups while Georgia lawmakers were debating and passing HB 481, which outlawed abortion after embryonic cardiac activity (around 6 weeks since last menstrual period). In this way, our data foreshadowed how Black and Latinx communities would be impacted by the later Dobbs decision.
Results from interviews and focus groups contribute to the growing data regarding sexual assault, IPV, and abortion. Several community key informants and community members discussed cases where women sought abortion services following rape or in the context of IPV, including reproductive coercion, which were reflected in our first and second themes. Among those who gave birth in the last 9 months, Black and Latinx individuals and individuals living in poverty are more likely to experience IPV and Black women are most likely to experience reproductive coercion, illustrating the interaction of structural and interpersonal violence (Samankasikorn et al., 2019). Importantly, women in IPV relationships are more likely to seek abortions later in pregnancy than those not in such relationships (Foster & Kimport, 2013). It is notable that regardless of personal opinion on the ethics of abortion, participants indicated abortion care to be necessary in cases of rape or incest. This perspective is consistent with national trends (Blazina, 2022). Black and/or Latinx women have reported community beliefs about abortion inform personal attitudes, such as spiritual traditions, historical and ongoing reproductive coercion and injustice perpetrated against women of color, and familial expectations regarding parenting if one becomes pregnant (Brown et al., 2022; Holman et al., 2020), and these beliefs were echoed by some participants. Similar to the extant research, despite these socialization experiences, overwhelmingly key informants and community members described sexual assault and IPV is reasons for abortion.
Numerous key informants and community members disclosed experiences of medical racism (specifically, obstetric racism) and coercion within provider–patient relationships informed by racism and classism (Davis, 2019; SisterSong et al., 2014). None of the key informants or community members said that providers attempted to influence a patient's decision to terminate a pregnancy. However, several community members and key informants described experiences of reproductive coercion or judgment from providers, who were overwhelmingly White, regarding the types of abortion procedures and initiating birth control immediately. Both key informants and community members connected these experiences to forced sterilization, eugenics, and experimentation perpetrated against people of color. Physician-centered perinatal and reproductive health care models emphasize clinical health risk mitigation and members of such teams, which comprise the majority of the U.S. medical system, are trained through institutional learning (Julian et al., 2020). Because the U.S. medical system is entangled with other institutions of structural violence and has perpetrated violence against communities of color, medical racism and coercion are part of those systems (Prather et al., 2018). Some of the interactions with providers are consistent with implicit pressure, which refers to subtle practices such as the imbalanced provision of information, minimization of side effects, and/or changes in affect or tone of voice that indicate a provider's implied favored or preferred contraceptive outcome or termination procedure (Gomez & Wapman, 2017). Providers’ biases regarding Black and Latinx individuals may interact with implicit pressure and result in different contraception options and counseling for Black and Latinx women in contrast to White women (Dehlendorf et al., 2010; Gomez & Wapman, 2017). Providers may not intend to exert this subtle or “under-the-surface” pressure; however, the impact is still felt. In addition to constraining immediate reproductive autonomy, implicit pressure is associated with later discontinuation of contraception and reluctance toward contraception (Gomez & Wapman, 2017), and individual racism and discrimination within reproductive care services have contributed to women delaying care (Oakley et al., 2018; Thompson, Young et al., 2022). Thus, medical obstetric racism and coercion by providers are compounding the barriers to abortion access and violence Black and Latinx pregnant individuals experience.
Multiple links between interpersonal violence and abortion care have been established (Basile et al., 2022; Miller et al., 2021), including pregnancy in the context of rape or incest and the association between early interpersonal trauma (e.g., childhood sexual abuse) and negative reproductive health outcomes including unwanted pregnancy. Research has also demonstrated that being denied a wanted abortion increases the likelihood of physical violence from the male-involved partner two and a half years after an unwanted pregnancy (Roberts et al., 2014). We extend this evidence and argue that to consider the link between violence and abortion care exclusively as one related to interpersonal violence perpetuates a tendency within the social sciences to focus on the individual and ignore the broader social context (Rylko-Bauer & Farmer, 2016). Because structural violence is built into the mechanisms through which societies function, it is normalized (Farmer, 2004). Many individuals view racism, poverty, immigration policies, and abortion restrictions/bans as natural outgrowths of legitimate systems, rather than violence. Given violence involves deliberate harm inflicted upon others, it is challenging to frame the persistence and creation of norms, procedures, and policies—including abortion restrictions/bans—that result in disproportionate harm to oppressed communities as anything other than violence, particularly since it is clear from the outset that harm will occur. For example, there is extensive scientific data and historical precedent to indicate that restricting abortion will exacerbate poverty and maternal mortality, particularly for Black women (Drife, 2010; Foster et al., 2018; Stevenson, 2021), and yet these policies have been and are continuing to be enacted.
Sexual assault and IPV are linked to structural factors—including gender inequity, racism, and poverty—such that social institutions’ construction of gender and race ascribe less value and less body autonomy to those socialized as female, of racial/ethnic minoritized status, and/or of lower socioeconomic status (Montesanti & Thurston, 2015). Structural violence begets interpersonal violence against women by normalizing gender-based power differentials such that sexual assault and IPV are seen as valid or excusable because women are perceived as expendable or deserving of violence. Further, the intersection of racism and gender-based power differentials facilitates and excuses violence against women of color in particular. Structural violence through the unequal distribution of resources, abandonment of the social safety net, and lack of economic opportunities exacerbates interpersonal violence when women must remain in violent relationships due to a lack of financial and support resources (Montesanti & Thurston, 2015). Further, structural violence via mass incarceration and police brutality beget and exacerbate sexual assault when women of color, particularly Black women, are less likely to report to law enforcement and are more likely to be considered “uncooperative” by police and receive a less thorough response from the criminal justice system (Long & Ullman, 2013).
Structural violence operates directly in opposition to reproductive justice (i.e., “the human right to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities” with bodily autonomy free of coercion; Ross & Solinger, 2017, p. 9). Key informants and community members expressed that poverty, racism, immigration enforcement, and the legacy of slavery, which is conceptualized as part of structural violence, all contribute to a lack of access to abortion care for Black and Latinx individuals. Consistent with other research (Thompson, Northcraft et al., 2022), the role of poverty was emphasized as a crucial variable that influences access to abortion care, particularly in the context of abortion bans and restrictions (that effectively function as bans). Because Black and Latinx communities are more likely to experience poverty than White communities (Baker et al., 2022), poverty is a central way in which abortion bans disproportionately affect Black and Latinx people. Notably, lack of access to abortion care increases the likelihood that Black and Latinx individuals will remain in poverty (Foster et al., 2018). Participants identified violent immigration enforcement, exclusively discussed as it affects Latinx communities, to be another barrier to abortion access as fear of immigration enforcement deters pregnant individuals from traveling out of state or engaging in medical services of any kind, including abortion services. Multiple key informants and community members also expressed that long-standing, socially embedded, and normalized racism and misogyny toward Black women creates barriers to abortion access, including stereotypes and stigma that create a “no win” situation when Black women are making pregnancy-related decisions. Several participants traced this stigma to the legacy of slavery, including systemic sexual violence and forced birth and sterilization by enslavers. Several participants noted that while poverty influences every group, the unique and intersecting oppressions of Black and Latinx women, including the likelihood of living in poverty, create barriers that maintain inequity through lack of access to abortion care.
Limitations and Future Directions
The current study's results must be taken in context with its limitations. The study's community members were Black and Latinx women, thus results may not generalize to those of different races and ethnicities. The community members were cisgender women; thus results may differ for transgender and gender-expansive individuals, who experience transantagonism within reproductive healthcare, including abortion care (Moseson et al., 2021). The study did not collect data on participants’ sexual orientation, and future studies should seek to examine violence and abortion care across the intersections of race and sexuality, particularly given the disproportionate interpersonal and structural violence experienced by sexual minoritized individuals of color (Long & Ullman, 2013). The sample was also exclusively recruited from a large, urban area in the Southern U.S.; thus, the experiences may not generalize to Black and Latinx individuals living in rural areas or in different geographic locations, all of which have differing abortion access. Some of the experiences described by participants are reflected in literature on accessing and experiencing reproductive healthcare (Thompson, Young et al., 2022), reflecting a long-standing pattern of the effects of structural and interpersonal violence on reproductive health among Black and Latinx women. Further, the majority of community members reported they had obtained a college degree or higher and/or were employed, thus the findings may not reflect those with different educational attainment and/or lower levels of income. Although this does not suggest the participants do not have experience or cannot speak to the impact of poverty, future research exclusively centering on those experiencing economic inequity is needed. However, in the context of structural barriers, there is documented evidence that demonstrates disparities in the care that Black and Latinx women receive, in spite of greater educational attainment and living above the poverty level (for a review, see Taylor, 2020). Finally, the current study did not assess the political affiliation of key informants. This background may have provided important context as to the generalizability of the findings. As the effect of abortion bans unfolds within the U.S., future research should continue to examine the impact of abortion bans and restrictions on Black and Latinx individuals across intersecting identities (e.g., gender, class, sexuality, ability, political affiliation, and religiosity) through a variety of methodologies, including both qualitative and quantitative research. Given the perpetuation of violence by researchers against communities of color, which was highlighted by several participants, it is critical that such research be grounded in a reproductive justice framework and community-led research.
Practice Implications
These results suggest a number of clinical and policy implications. Given the frequency with which key informants and community members discussed interpersonal and structural violence and abortion care, reproductive health providers should familiarize themselves with trauma-informed care across reproductive health services to ensure they are not compounding the trauma experiences of their patients (Cahill & Doyle, 2021; Tillman, 2020). Trauma-informed care also includes the elimination of barriers to care and clinicians are critical to building accessible health systems (Wycoff & Matone, 2019); providers should continue working toward addressing barriers within their clinics, such as offering services and paperwork in multiple languages. Clinics should also consider the effects of their models of care on individual patients and communities and move toward community-informed perinatal and reproductive health care models, which emphasize awareness of the history of reproductive health within the U.S., collaborative community partnerships, multidisciplinary teams, and pursuit of social justice (Julian et al., 2020). Changing inequitable power dynamics through models of care and prompting individual accountability toward bias may also prevent implicit pressure by providers.
Although the current study carries implications for the individual actions of providers and clinics, ultimately the policies created and enacted within the environment wield tremendous power in the lives of those seeking abortion care. Given that abortion is a safe, common, and integral part of reproductive health care (Raymond & Grimes, 2012) and a critical component for reproductive justice, we strongly encourage health care providers, community members, and policy makers to work tirelessly toward equitable abortion care access. Although the current study suggested that most individuals support abortion in the case of sexual assault, sexual assault and incest exceptions to abortion bans are not sufficient (Davis et al., 2023). Reporting requirements regarding rape or incest exception present a barrier to abortion care (Kacanek et al., 2010). Individuals may choose not to report a rape or instance of incest for myriad reasons, including fear of not being believed, threatened repercussions from the perpetrator, family, or friends, and being overwhelmed and isolated in a confusing legal system (Campbell, 2008; Slatton & Richard, 2020). Some abortion providers fear “it will be as if [these exceptions] didn’t exist” because of confusion and concern on the part of victims and providers as to what a report of sexual assault or incest will necessitate or trigger (Messerly, 2022). These barriers may be particularly burdensome for those who have experienced intimate partner sexual violence, which remains underreported (Bagwell-Gray et al., 2015). Notably, these exceptions do not include exceptions for those experiencing IPV, which key informants identified as a reason for seeking abortion care. Thus, to ensure that sexual assault and IPV survivors have access to abortion, abortion must be accessible for all, rather than reserved for only certain circumstances.
Although the current study emphasizes abortion care within a reproductive justice framework, reproductive justice emphasizes an inclusive conceptualization of body autonomy and centers on the voices of those most constrained in the machinery of oppression (Ross, 2006). As such, a reproductive justice framework is also relevant for those who do not support abortion. Thus advocacy for abortion access is not sufficient and must include policy changes to promote investment in communities and divestment from the carceral state and current policing policies, supportive employment policies for pregnant and parenting individuals, their partners, and communities, and environmental protections to promote healthy pregnancies and childhoods.
Conclusion
This qualitative investigation of Black and Latinx individuals’ perspectives on and experiences of violence and abortion care illuminates the intersection of interpersonal and structural violence. Overall, both key informants and community members discussed links between sexual assault and IPV as reasons for and barriers to receiving abortion care, while also highlighting the context of structural violence. It is the hope that this study informs future research and policy advocacy that is led by people of color to transform the current landscape of abortion care into true reproductive justice.
Footnotes
Authors’ Note
The authors would like to acknowledge all members of the CAB for their leadership and contributions to the Georgia Medication Abortion project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Georgia Medication Abortion Project was funded by the Society of Family Planning Research Fund and the Center for Reproductive Health Research in the Southeast through grants from an Anonymous Foundation and the Collaborative for Gender + Reproductive Equity, a sponsored project of Rockefeller Philanthropy Advisors.