
Abstract
Background
Few studies have examined which patients with migraine might be responders for mind-body interventions. Thus, we examined whether certain baseline mindfulness traits and interest in physical exercise might predict response to treatment.
Methods
This is a planned exploratory analysis of a phase 2 randomized controlled study (N = 50; 25 per arm) comparing a 6-week physical therapist (PT)-delivered biofeedback-assisted relaxation (BAR) program vs. an Enhanced Usual Care (EUC) migraine self-management program (diary tracking and emailed migraine-related educational materials). We conducted moderation analyses to determine whether the Multidimensional Assessment of Interoceptive Awareness (MAIA), Difficulties in Emotion Regulation Scale (DERS) and Physical Activity Enjoyment Scale (PACES) at baseline influenced the effect of BAR on migraine-related outcomes (Migraine-Specific Quality of Life Role Function Restrictive (MSQv2.1-RFR) and Migraine-Related Disability (MIDAS)) at 6 months.
Results
Among the n = 40 participants (BAR = 19; EUC = 21), the majority were female (95%), non-Hispanic (77.5%) and white (67.5%). Mean (SD) age was 45.6 (11.2) years. For the MAIA Not-Worrying subscale, BAR produced the greatest improvement in 6-month MSQv2.1-RFR scores among participants with low baseline Not-Worrying scores (those who tended to worry about bodily sensations/discomfort more) (BAR = 77.1 ± 6.6 vs. EUC = 48.9 ± 5.0; p = 0.002, g = 4.75). The benefit diminished at average levels (p = 0.060, g = 2.72) and was absent at high baseline Not-Worrying (p = 0.528, g = −0.91). For the MAIA Self-Regulation subscale, BAR was most effective among those low in baseline self-regulation (BAR = 71.7 ± 5.3 vs. EUC = 44.3 ± 7.2; p = 0.004, g = 4.27). The DERS total score showed that BAR demonstrated little benefit among participants with better baseline emotion regulation (i.e. lower DERS score; p = 0.907, g = 0.17) but was more effective as baseline emotion regulation difficulties increased, showing a moderate benefit at average levels (BAR = 69.2 ± 4.2 vs. EUC = 55.8 ± 4.0, p = 0.027, g = 3.25) and a large, significant difference at high levels (BAR = 70.6 ± 6.3 vs. EUC = 44.7 ± 5.7; p = 0.004, g = 4.22). The PACES total score indicated that BAR benefits were strongest among those with low (BAR = 76.1 ± 7.0 vs. EUC = 47.1 ± 5.3, p = 0.002, g = 4.60) to average (BAR = 71.2 ± 4.2 vs. EUC = 58.6 ± 4.0, p = 0.035, g = 3.07) enjoyment of physical activity.
Conclusions
We found subgroups of individuals with migraine who may be better responders to PT-delivered BAR, specifically those who tend to worry more about bodily sensations (lower MAIA Not-Worrying score), those with low self-regulation (lower MAIA Self-Regulation score), those with worse emotion regulation (higher DERS score) and those with lower levels of physical activity enjoyment (lower PACES score) at baseline. This may help us determine who may benefit most from BAR.
Trial Registration
ClinicalTrials.gov Identifier: NCT06077812.
This is a visual representation of the abstract.
Introduction
Migraine is the second most disabling condition worldwide, measured in Disability Adjusted Life Years (DALYs). 1 In the USA, over 47 million Americans are affected by migraine. 2 Research has shown that the best treatment for migraine involves both medication and behavioral therapy.3,4 Furthermore, some patients with migraine either prefer or need non-pharmacologic treatment due to contraindicated medications, pregnancy, 5 comorbidities, 6 cost 7 or intolerance. 8 In prior qualitative studies, patients have reported interest in non-pharmacologic treatments as a holistic approach for migraine management, 9 for reduction of symptoms and to maintain overall health. 10 Despite Grade A evidence for non-pharmacologic migraine treatments,11–14 they remain vastly underutilized among patients with migraine. 15 Multiple studies have examined external barriers to the use of non-pharmacologic treatments for migraine, such as difficulty finding trained providers, time to partake in the treatment, limited insurance coverage and mental health stigma,15–17 and a few studies have implemented behavioral techniques such as motivational interviewing to try to overcome barriers for their use.18,19 One mind-body study found that response to mindfulness-based cognitive therapy, measured by headache/migraine disability scores, was influenced by baseline migraine frequency as defined by episodic vs. chronic migraine. 20 While this is valuable insight for clinicians, few other studies have examined whether intrinsic characteristics affect clinical outcomes for non-pharmacologic treatments for migraine.
Biofeedback is another non-pharmacologic intervention with demonstrated efficacy for improving migraine frequency, severity, and disability compared to waitlist controls. 21 Incorporating relaxation training with biofeedback may provide additional support for migraine prevention. 22 Additionally, biofeedback 21 and relaxation training 23 may improve anxiety. Elevated levels of anxiety and stress may contribute to onset and severity of migraine, especially when not well-managed.24–26 Deficits in emotion regulation, comprising the ability to manage negative emotions, thoughts and feelings, have been associated with higher levels of pain perception, pain catastrophizing, pain-related disability,27,28 and elevated levels of anxiety and stress,29,30 including in individuals with migraine. 31 Discomfort and distress associated with bodily sensations are also implicated in pain perception 32 and anxiety, 33 and are elevated in those with migraine.34,35
The biopsychosocial model takes all of these factors into account by recognizing that pain conditions are beyond biological factors and also have influence from social, lifestyle and psychological factors. 36 The biopsychosocial model has recently been applied to migraine, where migraine management is considered a multi-layered model with an intermediate level encompassing education and non-pharmacologic approaches. 36 Behavioral therapies may help with stress management and enhancing self-efficacy, thus potentially boosting the effectiveness of pharmacologic interventions when combined. 36 Behavioral therapies have also been found to reduce pain catastrophizing and increase coping strategies for migraine management. 37 Specifically, biofeedback interventions may be especially useful to target difficulties coping with stress-related factors associated with migraine onset and severity. However, little is known about clinical and psychosocial predictors of response to these interventions.
Given the ongoing need to better understand who might be responders for mind–body interventions among individuals with migraine, we conducted exploratory analyses of physical therapist (PT)-delivered biofeedback-assisted relaxation (BAR) for migraine prevention to examine whether certain baseline mindfulness traits and interest in physical exercise might predict response to treatment. This insight might guide the direction of provider recommendations for non-pharmacologic treatments.
Methods
This is a planned exploratory analysis of a NYU Langone Health Institutional Review Board approved study to determine whether baseline psychological characteristics or attitudes towards exercise influenced the effect of biofeedback on migraine outcomes. All participants completed electronic informed consent via REDCap(38,39) during the enrollment session. In brief, we conducted a phase 2 randomized controlled trial (N = 50; 25 per arm) to compare a 6-week in-person PT-delivered BAR program vs. a remote migraine self-management program. We followed the relevant CONSORT reporting guidelines.(40)
Recruitment
MyChart messages (https://www.mychart.org) were sent (via NYU Langone Health DataCore) to potentially eligible patients who visited a headache specialist or neurologist at NYU Langone Health within the last year and had an International Classification of Diseases (ICD)-10 code of migraine. As a second recruitment method, the study team screened patients of five NYU Langone Health headache specialists and neurologists who predominantly treat patients with headache and called or emailed potentially eligible patients to determine their interest in the study. Those who expressed interest in the study and met study eligibility criteria were scheduled for a virtual baseline enrollment visit with the study coordinator between November 2023 and May 2024.
Inclusion criteria
Inclusion criteria included English-speaking, aged 18–65 years old, with an ICD-10 code of migraine and meeting at a minimum International Classification of Headache Disorders, 3rd edition, criteria for probable migraine, 41 headaches have been present for at least a year, has not begun a new migraine preventive medication in the last month, agreement to not make any changes to preventive medication until 3 months after enrollment in the study (participants were informed that they could make changes to acute medications, if needed), and self-reported headache days between 4 and 29 headache days a month (thus including those who typically receive preventive therapies for migraine but excluding continuous headache). To account for potential medication confounds, we recorded changes in preventive and acute medications reported by participants.
Exclusion criteria
Exclusion criteria included use of cognitive behavioral therapy, biofeedback or other relaxation therapies for migraine within the last year, self-reported medication overuse headache, alcohol or other substance use disorder (self-reported or documented in their medical record), current use of barbiturates or opioids, and a score of > 15 on the Patient Health Questionnaire (PHQ)-8 (because there may be a necessity for more intense psychological interventions targeted for depression, a cut off of 15 was chosen since it is a conservative score on the PHQ-9 with moderately severe depressive symptoms). We also excluded those with a diagnosis of heart attack, coronary heart disease, stroke and/or diabetes mellitus type I or II because these conditions already lessen heart rate variability and we wanted to first examine whether heart rate variability biofeedback delivered by PTs might be feasible, acceptable and effective in healthy people with migraine. 42 Finally, we excluded those who were pregnant (because migraine outcomes can be affected by hormonal fluctuations in pregnancy), unable or unwilling to participate in a study with written or audio-taped materials, and other physical limitations that may interfere with participation in the standard biofeedback protocol used in this study.
Enrollment and intervention
Once consented, participants were randomly assigned into either the in-person biofeedback (BAR) arm (n = 25) or the enhanced usual care (EUC) remote migraine-self management program arm (n = 25). Randomization was stratified by gender (male, female, non-binary, other gender, or prefer not to answer) and age (< 40 years or ≥ 40 years). A statistician created the randomization list (including variable blocks with sizes of four or six used within strata), which the study team uploaded into REDCap to randomize participants into either arm. The study team informed participants that they would receive a migraine self-management program that was either in-person or remote, but participants were blinded to the type of intervention delivered (biofeedback). For those in the BAR arm, a six-session (∼45 min per session) in-person biofeedback protocol was delivered by two PTs at Dynamic Sports Physical Therapy in New York, NY. In brief, the biofeedback techniques introduced throughout the sessions included Progressive Muscle Relaxation with the Thought Technology ProComp5 (https://thoughttechnology.com), assessment of optimal breathing rate using resonance frequency evaluation, thermal biofeedback including hand warming visualization, paced breathing, postural exercises and breathing exercises using the HeartMath Inner Balance Sensor device (https://www.heartmath.co.uk) (if time permitted). Participants in the EUC arm received migraine-related educational material from the American Migraine Foundation. (43–45) Participants in both arms completed a headache diary. The study length was 6 months.
Measures
Measures were examined at baseline and at the 6-month follow-up to evaluate change over time in migraine-related outcomes. Baseline assessments included demographic, clinical and psychological characteristics, as well as attitudes towards exercise. The measures included are outlined below.
Migraine measures
The Migraine-Specific Quality of Life Questionnaire Version 2.1 (MSQv2.1) is a validated,46,47 migraine-specific instrument used to assess the impact of migraine on health-related quality of life during the previous 4 weeks. It comprises three domains: Role Function Restrictive (RFR), Role Function Preventive (RFP) and Emotional Function (EF). Scores for each domain range from 1 to 6 and are rescaled to a 0–100 scale, with higher scores representing better migraine-specific quality of life. 46 The RFR domain reflects limitations in performing daily activities due to migraine and is considered the most sensitive to change, where 8 points is the established clinically meaningful change. 48
The Migraine Disability Assessment (MIDAS) Questionnaire consists of a five-item scale and is used to measure migraine disability during the last 3 months.49–52 It assesses the number of days of missed or reduced productivity in work or school, household chores, and family, social or leisure activities due to headache. The total MIDAS score is calculated by summing the five items, yielding a continuous measure of disability, with higher scores representing greater migraine-related disability. A reduction of 5 or more points is considered a clinically meaningful change in MIDAS. 53
Baseline psychological measures
The Multidimensional Assessment of Interoceptive Awareness, version 2 (MAIA) is a self-reported, 32-item trait questionnaire designed to measure multiple dimensions of subjective interoceptive awareness, meaning how individuals notice, interpret and respond to internal bodily sensations. 54 Items are rated on a six-point Likert scale ranging from 0 ‘never’ to 5 ‘always’ (range 0–160), with higher scores reflecting greater interoceptive awareness and more adaptive mind–body integration. The questionnaire provides measures for eight dimensions; Noticing (awareness of one's sensations), Not-Distracting (tendency to not distract from bodily discomfort), Not-Worrying (tendency to not worry or feel emotional distress related to bodily discomfort), Attention Regulation (ability to attend to one's bodily sensations), Emotional Awareness (noticing how bodily sensations are connected to emotional states), Self-Regulation (ability to regulate distress related to bodily sensations), Body Listening (listening to one's body/sensations) and Trusting (trusting one's body as safe).
The Difficulties in Emotion Regulation Scale (DERS) is a 36-item self-report measure that assesses emotion regulation difficulties in total and across six domains: Nonacceptance of Emotional Responses (not accepting emotional distress or experiencing shame related to emotions), Goals (challenges engaging in goal-directed behavior during experiences of distress), Impulse (impulse control difficulties with experiences of negative emotions), Awareness (difficulties acknowledging emotions), Strategies (limited ability to utilize emotion regulation strategies during distress) and Clarity (limited understanding of emotions being experienced). 55 Items are rated with a five-point scale, where higher scores indicate greater difficulty regulating emotions (range 36–180).
Baseline attitudes towards exercise measure
The Physical Activity Enjoyment Scale (PACES) is an 18-item self-report measure that evaluates affective enjoyment of physical activity. 56 Items are rated on a seven-point scale anchored by opposing descriptors (e.g. ‘I find it pleasurable to I find it unpleasurable’). Higher total scores indicate greater enjoyment and positive affective responses to exercise (range 18–126). As our BAR protocol involved physical exercises, we measured physical activity enjoyment to understand how this may be associated with response. Previous research finds that discomfort with body-related sensations is associated with lower levels of physical activity enjoyment, 57 including in those with probable migraine. 58
Statistical analysis
Because this study was designed as a pilot investigation to evaluate feasibility and estimate preliminary treatment effects, a formal power-based sample size calculation was not performed. Consistent with recommendations for pilot randomized studies 59 and several methodological papers that support sample sizes in roughly this range for pilot studies,59–61 a minimum of 20 participants per group was targeted to provide stable estimates of variability and effect sizes for future adequately powered trials. To account for potential attrition, the target enrollment was increased by five participants per group.
Baseline differences on demographic characteristics and other measures between the BAR and EUC arms were examined. In our primary analysis, we assessed MIDAS and MSQv2.1 at baseline and 6 months, as well as change from baseline to 6 months, to understand longitudinal differences between groups.
Categorical variables were analyzed using chi-squared tests. Continuous variables with approximately normal distributions were summarized as means and standard deviations and compared between arms using independent samples t tests. Variables that were non-normally distributed were summarized using medians and interquartile ranges (IQRs) and were compared using Mann–Whitney U tests. Group differences at baseline and 6-month follow-up, as well as 6-month change scores from baseline, were examined using these same procedures. Effect sizes for modest sample sizes were calculated using Hedges’ g for t tests and the rank-biserial correlation (r) for non-parametric comparisons. p < 0.05 (two-tailed) was considered statistically different.
Modeling approach
We report moderation analyses examining whether baseline psychological characteristics influenced the effect of biofeedback on migraine outcomes measured at the 6-month follow-up compared to baseline. All analyses were performed using SPSS, version 30.0 (IBM Corp.).
The MSQv2.1-RFR moderation models were estimated using general linear models. Separate moderation models were performed for each baseline measure of interest (i.e. MAIA subscales, DERS total, and PACES total). Each model included the 6-month MSQv2.1-RFR score as the dependent variable, baseline MSQv2.1-RFR score and the baseline psychometric score as covariates, treatment arm (BAR vs. EUC) as the predictor, and the treatment × baseline covariate interaction term to test the moderation effect. A statistically significant interaction term (p < 0.05) indicated that the baseline measure moderated the effect of treatment on the 6-month MSQv2.1-RFR score. For measures with significant interactions, estimated marginal means (EMMs) were computed at low (−1 SD), mean and high (+1 SD) levels of the moderator to illustrate simple effects, and effect sizes were quantified using Hedges’ g.
Because MIDAS scores were right skewed and count-like, generalized linear models with negative binomial distribution and log link were utilized to model 6-month MIDAS outcomes. These models included the same covariates and interactions as the MSQv2.1 RFR models.
All models were estimated among participants with complete 6-month follow-up data (n = 40). Model residuals and distributional assumptions were examined to ensure adequate fit.
Results
As shown in Figure 1, three BAR participants withdrew (two withdrew prior to completing a BAR session and the third withdrew after completing one BAR session) and therefore did not have follow-up data. Three additional BAR participants did not complete the 6-month follow-up questionnaire. Four EUC participants did not complete the 6-month follow-up questionnaire.
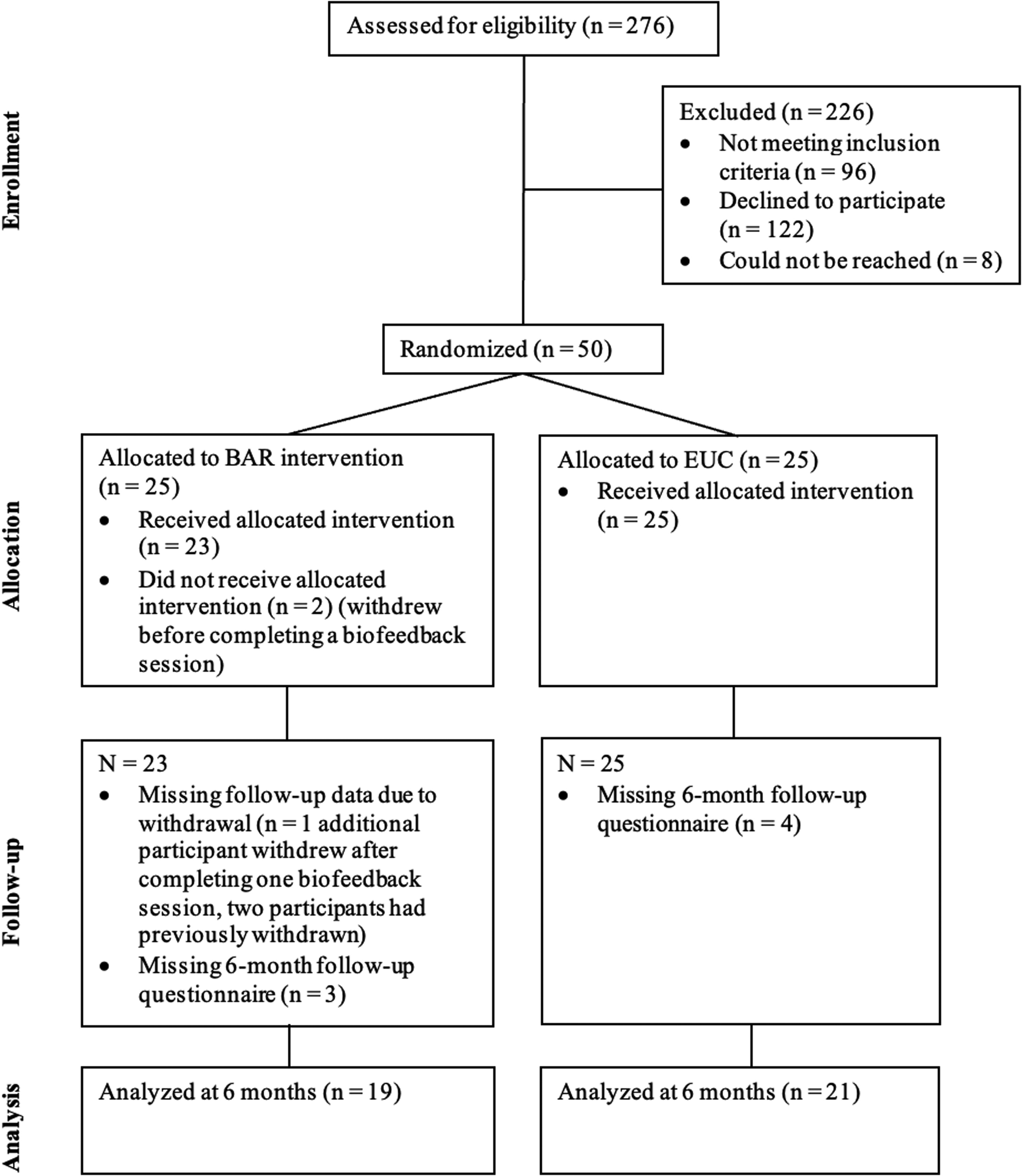
Diagram outlining the flow of participants in the biofeedback-assisted relaxation (BAR) and enhanced usual care (EUC) arms.
Baseline characteristics
Among the n = 40 participants (BAR = 19; EUC = 21) the majority were female (95%), non-Hispanic (77.5%) and white (67.5%) (Table 1). Arms did not differ significantly by gender, ethnicity, or race (all p > 0.05). The mean (SD) age of participants was 45.6 (11.2) years, with no statistically significant difference between the BAR and EUC arms (p = 0.487). Age of first headache (14.6 ± 8.5 years) and age at migraine diagnosis (27.4 ± 12.3 years) were also comparable between arms (both p > 0.05).
Demographic, headache characteristics and outcomes.
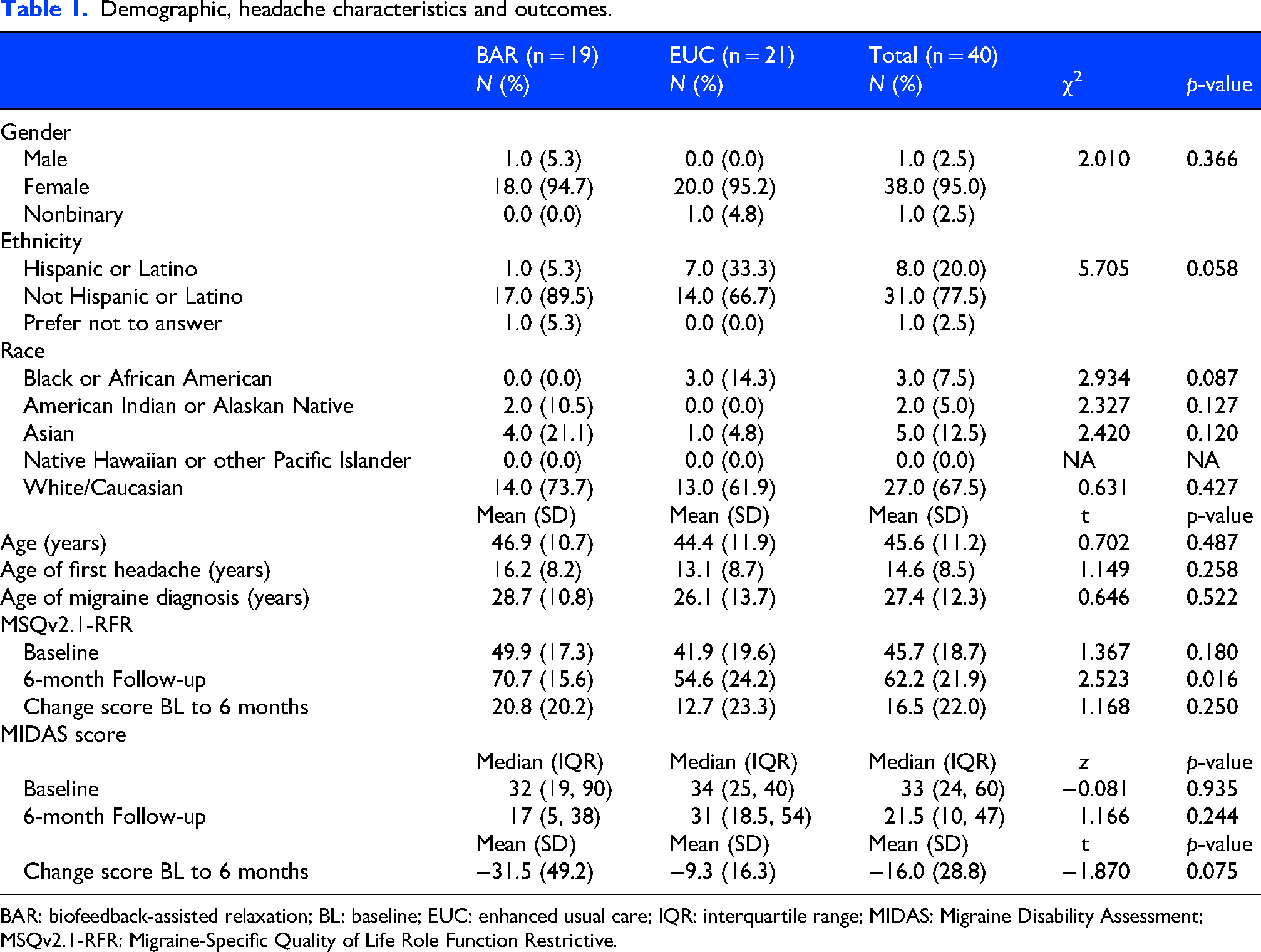
BAR: biofeedback-assisted relaxation; BL: baseline; EUC: enhanced usual care; IQR: interquartile range; MIDAS: Migraine Disability Assessment; MSQv2.1-RFR: Migraine-Specific Quality of Life Role Function Restrictive.
At baseline, MSQv2.1-RFR scores were similar between arms (BAR = 49.9 ± 17.3; EUC = 41.9 ± 19.6; t = 1.37, p = 0.180, g = 0.42) (Table 1). In our primary analysis, we found that, by 6 months, MSQv2.1-RFR scores were significantly higher among participants in the BAR arm (70.7 ± 15.6) compared to the EUC arm (54.6 ± 24.2; t = 2.52, p = 0.016, g = 0.76) (Table 1). The mean change in MSQv2.1-RFR from baseline to 6 months was higher in the BAR arm (20.8 ± 20.2 vs. 12.7 ± 23.3), although this difference did not reach statistical significance (t = 1.17, p = 0.250, g = 0.36) (Table 1).
Baseline MIDAS scores were similar between arms (median = 32 (IQR 19–90) vs. 34 (IQR 25–40); z = −0.08, p = 0.935, r = −0.01) (Table 1). At 6 months, both arms improved, with median MIDAS scores of 17 (IQR 5–38) in the BAR arm and 31 (IQR 18.5–54) in the EUC arm (z = 1.17, p = 0.244, r = 0.18) (Table 1). The mean reduction in MIDAS from baseline to 6 months was greater in the BAR arm (−31.5 ± 49.2) than in the EUC arm (−9.3 ± 16.3), showing a trend toward greater improvement (t = −1.87, p = 0.075, g = −0.61) (Table 1).
Baseline psychometric scores did not differ significantly between arms (Table 2). Overall, baseline characteristics were well balanced, and participants in the BAR arm demonstrated larger improvements in both functional quality of life and headache-related disability over 6 months.
Baseline psychometric measure scores.

BAR: biofeedback-assisted relaxation; DERS: Difficulties in Emotion Regulation Scale; EUC: enhanced usual care; MAIA: Multidimensional Assessment of Interoceptive Awareness; PACES: Physical Activity Enjoyment Scale.
Moderation analyses: Interaction effects
Moderation analyses were conducted to examine whether baseline characteristics (interoceptive awareness (MAIA), emotion regulation (DERS), physical activity enjoyment (PACES)) influenced the effect of BAR on 6-month migraine outcomes (Table 3). Across the baseline measures, four significant treatment × baseline interactions were observed for MSQv2.1-RFR: MAIA Not-Worrying (p = 0.008), MAIA Self-Regulation (p = 0.038), DERS total (p = 0.043), and PACES total (p = 0.009). No significant interaction terms were detected for the MIDAS outcome (all p > 0.05).
Interaction terms (treatment × baseline psychological measure) predicting 6-month MSQv2.1-RFR and MIDAS.
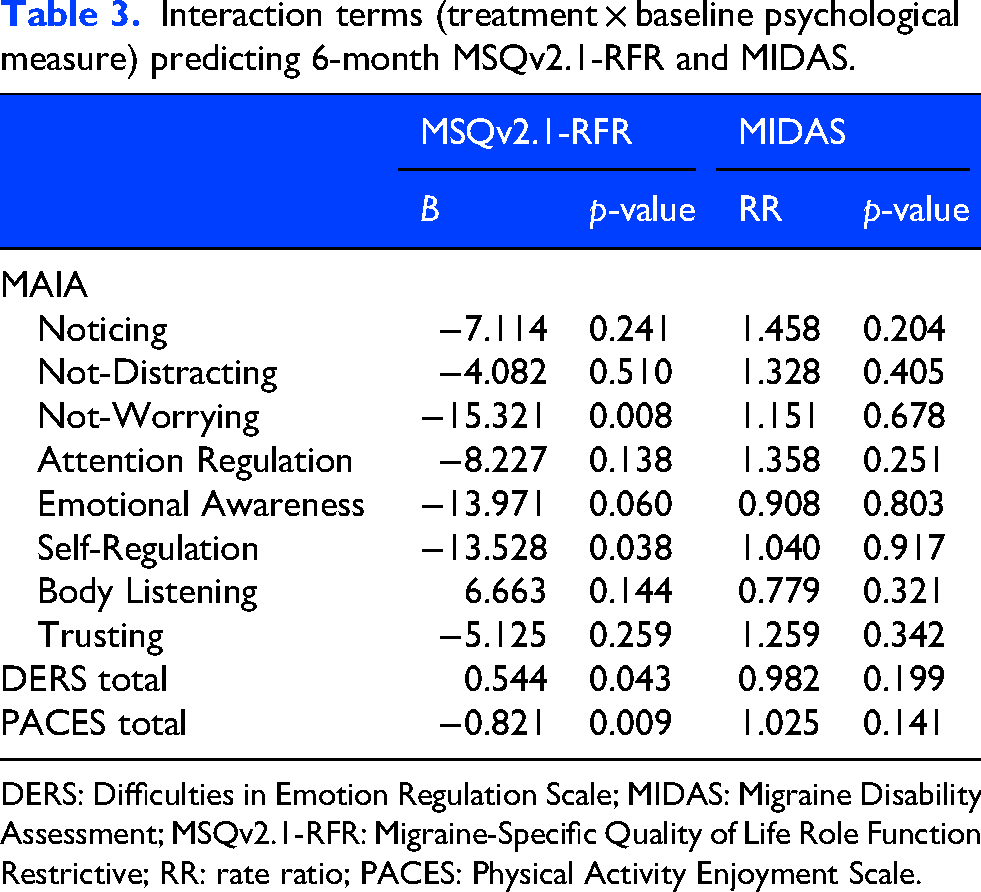
DERS: Difficulties in Emotion Regulation Scale; MIDAS: Migraine Disability Assessment; MSQv2.1-RFR: Migraine-Specific Quality of Life Role Function Restrictive; RR: rate ratio; PACES: Physical Activity Enjoyment Scale.
Moderation effects: Estimated marginal means
To interpret the significant interaction effects, EMMs of 6-month MSQv2.1-RFR scores were examined at low (−1 SD), mean, and high (+1 SD) levels of each significant baseline measure (Table 4). Because these estimates reflect model-adjusted simple effects within subgroups, the resulting standardized effect sizes are larger than those observed in overall between-group comparisons and should be interpreted accordingly.
Estimated marginal means of 6-month MSQv2.1-RFR by treatment arm at low, mean, and high baseline psychometric scores for significant moderators.
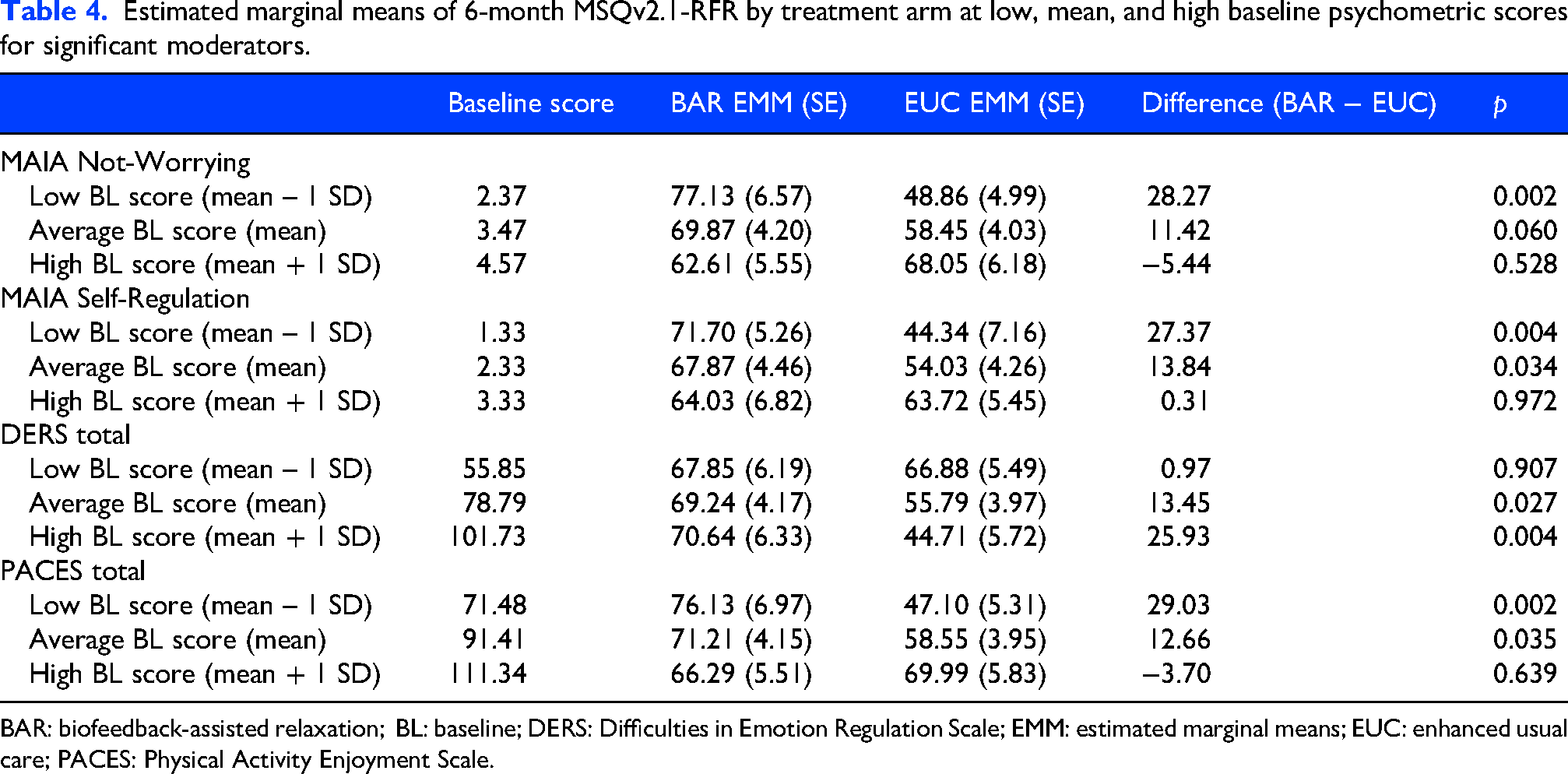
BAR: biofeedback-assisted relaxation; BL: baseline; DERS: Difficulties in Emotion Regulation Scale; EMM: estimated marginal means; EUC: enhanced usual care; PACES: Physical Activity Enjoyment Scale.
Moderation model for MAIA
For the MAIA Not-Worrying subscale, BAR produced the greatest improvement in 6-month MSQv2.1-RFR scores among participants with low baseline Not-Worrying scores (those who tended to worry about bodily sensations/discomfort more) (BAR = 77.1 ± 6.6 vs. EUC = 48.9 ± 5.0; p = 0.002, g = 4.75). The benefit diminished at average levels (p = 0.060, g = 2.72) and was absent at high baseline Not-Worrying (p = 0.528, g = −0.91).
A similar pattern was observed for the MAIA Self-Regulation subscale: BAR was most effective among those who had low baseline self-regulation scores (BAR = 71.7 ± 5.3 vs. EUC = 44.3 ± 7.2; p = 0.004, g = 4.27), with the group difference decreasing at average levels (BAR = 67.9 ± 4.5 vs. EUC = 54.0 ± 4.26; p = 0.034, g = 3.11) and disappearing at high levels (p = 0.972, g = 0.05).
Moderation model for DERS
The DERS total score showed a similar pattern: BAR demonstrated little benefit among participants with better baseline emotion regulation (i.e. lower DERS scores; p = 0.907, g = 0.17) but became increasingly effective as baseline emotion regulation difficulties increased, showing a moderate benefit at average levels (BAR = 69.2 ± 4.2 vs. EUC = 55.8 ± 4.0, p = 0.027, g = 3.25) and a large, significant difference at high levels (BAR = 70.6 ± 6.3 vs. EUC = 44.7 ± 5.7; p = 0.004, g = 4.22).
Moderation model for PACES
Finally, the PACES total score indicated that BAR benefits were strongest among those with low (BAR = 76.1 ± 7.0 vs. EUC = 47.1 ± 5.3, p = 0.002, g = 4.60) to average (BAR = 71.2 ± 4.2 vs. EUC = 58.6 ± 4.0, p = 0.035, g = 3.07) enjoyment of physical activity and were absent at high baseline physical activity enjoyment levels (p = 0.639, g = −0.64).
Discussion
In this study, we found subsets of individuals who may be better responders to PT-delivered BAR according to baseline characteristics. These included individuals who tended to worry more about bodily sensations (MAIA Not-Worrying subscale), those who had low baseline self-regulation (MAIA Self-Regulation subscale) and those with worse emotion regulation (DERS total) and lower levels of physical activity enjoyment (PACES total) at baseline. In individuals with better baseline emotion and self-regulation, less discomfort with bodily sensations and higher levels of physical activity enjoyment, the benefit in migraine-specific quality of life lessened. Based on our analysis of baseline characteristics and responders to biofeedback, biofeedback may enhance one's understanding of how to regulate the body's autonomic responses.
Aligning with previous research, our biofeedback intervention, which included relaxation training, resulted in a trend towards improved migraine-related disability and possibly quality of life.21,22 Our intervention included specific strategies targeting management of autonomic physiological arousal (i.e. fight or flight response), such as progressive muscle relaxation and paced breathing. These techniques can be helpful tools for managing stress and anxiety,62,63 which may help reduce frequency and severity of migraine.26,64 In particular, the techniques may be especially beneficial for those with poorer emotion regulation, like the responders in our sample, who may not have the existing skills to manage emotional responses to stress, thus leaving them vulnerable to subsequent migraine onset. Indeed, targeting emotion regulation improves stress reactivity,65,66 with some indication that this may be applicable to those with migraine.67,68
Our study also found that biofeedback may be particularly beneficial to those with elevated baseline levels of worry about bodily sensations. Individuals who are highly distressed by bodily sensations may have a tendency to interpret physiological cues as threatening, including interpreting them as potential triggers of migraine. 69 For these individuals, biofeedback interventions may facilitate corrective interoceptive learning by allowing them to engage with physiological sensations in a ‘safe’ context thus creating new learning that not all physiological sensations are indications of danger. Accordingly, biofeedback has been associated with changes in interoceptive awareness, 70 cognitive reappraisals regarding physiological sensations, 71 and improved sense of control and self-efficacy in the context of bodily sensations. 72
Individuals who report discomfort with bodily sensations may also be more likely to avoid physical activity, which can induce the feared bodily sensations (e.g. increased heart rate, changes in breathing rate and sweating). For example, those with high anxiety sensitivity tend to report exercise as less enjoyable 57 and tend to avoid exercise,73,74 including those with probable migraine. 58 However, for individuals who begin exercise programs of moderate to vigorous intensity, anxiety sensitivity improves, 75 showing that engaging with the physiological sensations in a relatively safe context may produce improvement and more enjoyment of physical activity as a whole. In our sample, those with lower physical activity enjoyment had greater response to BAR. This may be due to cultivating new types of activity in the BAR-related exercises that allowed for enjoying physical activity differently than previously. Those who already enjoyed physical activity may have different conceptualizations of what constitutes ‘exercise’ thus making the BAR-related exercises less useful overall.
Furthermore, as the BAR intervention may have improved physiological stress responses and reduced fear of bodily sensations, it may also have inadvertently improved physical activity enjoyment and reduced physical activity avoidance. Physical activity has evidence for migraine prevention as an alternative to daily preventive medication. 76 Non-pharmacologic treatments such as relaxation, strength training, and aerobic exercise have been found to be effective in reducing migraine burden. Specifically, prior studies that evaluated aerobic endurance training for migraine found improvements in the intensity, frequency and duration of migraine and overall patient wellbeing.76–79 A systematic review and network meta-analysis found that strength training exercise regimens and high intensity aerobic exercise have the highest efficacy in reducing the burden of migraine, 80 even greater than that of topiramate, a level A evidence-based migraine preventive treatment. One study also showed comparable efficacy between 40 min of aerobic exercise three times a week, a recorded relaxation program and topiramate for migraine prevention. 76 Although exercise may be an effective intervention for improving migraine, some individuals may find it challenging to engage with regular exercise, especially if they tend to worry about pain or triggers related to headaches. Biofeedback can be an initial gateway intervention to help reduce these barriers. Other strategies could be highlighting and encouraging attending to the immediate affective benefits (e.g. stress reduction) of exercise. Indeed, interventions focusing on affective benefits (e.g. stress reduction or mood enhancement) promote better long-term adherence to exercise and mental and physical health outcomes than those focused on health benefits alone.81–84
Strengths
This is one of the few studies that begins to assess moderation effects of biofeedback. Clinically, these results may be utilized to determine which patients with migraine might be best referred for biofeedback.
Limitations
This was a single site study. Demographically, participants were primarily younger, female and from the New York area. Results may not be generalizable to the broader population, including individuals living outside of urban areas. Given the limited sample size and the number of statistical tests performed, some significant interactions may have occurred by chance (type I error) therefore, these findings should be viewed as exploratory and hypothesis-generating.
Conclusions
Clinically, our study suggests some initial predictors of individuals who may receive the most benefit from biofeedback interventions for migraine. The profile of responders seems consistent with those who may be more vulnerable to migraine triggered by stress or anxiety and who have minimal emotion regulation skills to effectively manage such stressors. Teaching body-focused skills to regulate physiological stress, improving self-efficacy to manage stress and reducing worry or negative cognitions related to potential triggers/stress may be particularly effective for this subgroup of individuals with migraine. Individuals with migraine related to other causes may still benefit from biofeedback, but might also be better candidates for other interventions, such as cognitive behavioral therapy, aerobic exercise, devices or medications.
Clinical implications
Specific subgroups of individuals with migraine may respond better to biofeedback (i.e. improvements in Migraine-Specific Quality of Life Role Function Restrictive (MSQv2.1-RFR)) based on baseline characteristics (i.e. mindfulness traits and interest in physical exercise).
Providers may utilize standardized questionnaires to determine if a patient with migraine may respond well to biofeedback.
Footnotes
Consent to participate
All participants completed electronic informed consent via REDCap during the enrollment session.
Ethical considerations
This is a planned exploratory analysis of a NYU Langone Health Institutional Review Board approved study to determine whether baseline psychological characteristics or attitudes towards exercise influenced the effect of biofeedback on migraine outcomes.
Author contributions
KLS contributed to the Conceptualization, Writing – Original Draft, and Writing – Review & Editing. JD contributed to the Investigation, Data Curation, Writing – Original Draft, Writing – Review & Editing, and Visualization. RCB contributed to the Formal analysis, Writing – Original Draft, Writing – Review & Editing, and Visualization. KMF contributed to the Formal analysis, Writing – Original Draft, Writing – Review & Editing, and Visualization. MTM contributed to the Conceptualization, Methodology, Supervision, Project administration, Funding acquisition, Writing – Original Draft, and Writing –- Review & Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The current study was funded by the NYU Langone Health Interdisciplinary Pain Research Program (IPRP's) pilot project award.
Declaration of conflicting interests
KLS receives grant funding from the National Institutes of Health and Brain and Behavior Research Foundation and is an Associate Editor of Mental Health and Physical Activity. RCB has received personal compensation in the range $50,000–$99,999 for serving as a Consultant for MIST Research. KMF has received research support from Abbvie and has received research support from NYU Langone Health, University of SC – Irvine, and AESARA. MTM has received research support from the NIH. MTM contributed to developing intellectual property being used in this study that is co-owned by NYU and IRODY. If the research is successful, NYU and IRODY may benefit from the outcome. JD has no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Anonymized data not published within this article will be made available by request from any qualified investigator per NYU Langone Health Data Sharing Policies.