
Abstract
Background/Aim
Persistent idiopathic facial pain (PIFP) is a rare condition with a lifetime prevalence of approximately 0.03%. It is characterized by persistent daily facial pain without identifiable cause and presents diagnostic and therapeutic challenges due to unknown pathophysiology, symptom overlap with other painful disorders, and limited evidence-based treatments. The aim of this Delphi study was to establish international consensus-derived guidelines for the management of patients with PIFP.
Methods
A three-round Delphi study was conducted with 16 international pain experts, each with ≥10 years of clinical experience in pain management and extensive peer-reviewed publications. The first round involved open-ended questions, and the qualitative data were analyzed using systematic text condensation, resulting in a quantitative questionnaire with 42 statements. Subsequent rounds employed Likert-scale responses to these statements. Consensus was defined as ≥80% agreement or disagreement. In addition, if 11–12 (68–75 percent) out of the 16 experts agreed or disagreed, consensus was not reached, but a majority was considered to have a particular opinion.
Results
Consensus was reached in 35 out of the 42 statements (83%), emphasizing multidisciplinary collaboration and avoidance of invasive procedures in the treatment of PIFP. In an additional three statements (7%) a majority of the experts agreed with each other. In four statements (10%), no consensus or majority was reached. Pharmacological treatments, including tricyclic antidepressants, serotonin-norepinephrine reuptake inhibitors, and gabapentinoids, may be considered; however, opioids should generally be avoided in the treatment of PIFP. Patient education and behavioral therapies are important interventions, and the most important measure of therapeutic success is improved quality of life
Conclusion
The present Delphi study has established internationally derived consensus guidelines and recommendations for the evaluation and comprehensive management of patients with PIFP. This is a first step in gathering knowledge for future evidence-based guidelines and more specific treatment recommendations. These international expert consensus guidelines recommend a multi- or interdisciplinary approach in managing PIFP, avoiding invasive interventions and prioritizing patient-centered outcomes.
Keywords
Introduction
Pain in the head and face is very common in the general population. Its classification has evolved substantially in the past few years, especially with regard to chronic pain. The International Classification of Headache Disorders (ICHD) has undergone several adjustments since its initial publication (1), and the first version of the International Classification of Orofacial Pain (ICOP) was introduced in 2020 (2) as a collaborative effort between dentists and physicians. ICOP is aligned with the International Classification of Diseases 11 (ICD-11) section on chronic pain (3–5) and the category “Chronic primary headache or orofacial pain” (6).
Orofacial pain (OFP) is per definition confined to the oral cavity and/or face (2) and is distinguished from headaches by anatomical boundaries (7–9). In clinical settings, the distinction between OFP and headache is sometimes unclear due to complex referral patterns. Significant differences in the prevalence of OFP have been reported, depending on factors such as the population studied, study duration, and geographical location (10). Nevertheless, OFP is common, affecting approximately 16–22% of the population (10,11) and it has a major impact on the quality of life (QoL) of those affected, often resulting in impaired sleep and mood and considerable disability (7,12). Dental pain is the most common OFP followed by pain associated with temporomandibular disorders (TMD) (10,11).
The term “atypical facial pain” as a diagnosis was updated in the 3rd edition of ICHD in 2018 and has since been referred to as “persistent idiopathic facial pain” (PIFP) (9). This term was recognized in 2020 with the introduction of the ICOP (2). This pain condition is defined as a “persistent facial pain, with variable features, recurring daily for more than 2 h per day for more than three months, in the absence of clinical neurological deficit or preceding causative event” (2). PIFP is a rare orofacial pain condition with a lifetime prevalence of approximately 0.03% and should not be confused with persistent idiopathic dentoalveolar pain (PIDAP), which presents with pain perceived to be within the intraoral tissues (2). The diagnosis is reserved for cases where no other condition can explain the pain (13,14). The majority of patients with PIFP are women (15) and they often report a diffuse, dull, aching, or nagging pain that is not confined to the neuroanatomic distribution of a specific peripheral nerve, which distinguishes it clinically from peripheral neuropathic pain. The pain can be both deep and superficial (2) and has been described as refractory to therapy and persisting for long periods of time, often many years (15).
The pathophysiology of PIFP remains unknown. It has been suggested that this pain condition may involve a disproportionate response to mild injury (13), and functional imaging points toward central sensitization (16). It may also be considered a nociplastic type of pain that arises from altered nociceptive function and aberrant activities in the central nervous system (17–19). There is no established protocol for the management of patients suffering from PIFP. Although many different treatment regimens have been proposed, the lack of high-quality randomized controlled studies limits evidence-based treatment decisions (13). Still, as with many other chronic pain conditions, a multimodal therapeutic approach has been recommended (13,20,21), ideally provided in an interdisciplinary or transdisciplinary fashion with a joint treatment plan.
In the absence of scientific evidence, healthcare providers must rely on clinical experience to be able to make decisions concerning patient management. The collective experience of colleagues, summarized into a consensus, is considered more valuable than the experience of a single individual (22,23).
The aim of this Delphi study was to establish international consensus-derived guidelines for the management of patients with PIFP.
Methods
The study protocol was registered on Researchweb Region Uppsala and publicly presented in the Uppsala Public Dental Health Service's 2022 Odontology Research Report. The classical Delphi consensus method was used in this study (24). One of the advantages of the Delphi method over other consensus techniques is that it maintains anonymity among the experts, eliminating the potential social influence on beliefs and opinions that can occur when people meet face-to-face (25).
The experts were identified through three approaches: the Orofacial Pain Classification Committee responsible for ICOP (2); a narrative literature review of publications in the field of PIFP; and pain specialists whose expertise, according to the lead authors, was considered an important contribution to the project. Eighteen international pain experts were invited to participate in this Delphi study. An expert was defined as a researcher with identifiable peer-reviewed publications and at least 10 years of clinical experience in the management of pain patients. The mean total number of peer-reviewed publications of our expert panel was 226 (range: 45–608). Before being included in the study, the experts received written information about the study. The experts did not receive financial compensation for their participation. However, they were informed prior to accepting that their involvement in the study would include an invitation to serve as co-authors. Two experts declined to participate due to time constraints. Sixteen experts from three of the six WHO regions were included in the expert panel (Table 1). The expert panel comprised the following specialties: neurology, neurosurgery, neurophysiology, headache medicine, pain management, orofacial pain, endodontics, oral and maxillofacial surgery, and oral medicine. The three leading authors (EL, PA and TG) did not participate as members of the expert panel. The first author (EL) is an orofacial pain and jaw function specialist and PhD with experience in orofacial pain, qualitative research, and Delphi methodology. The second author (PA) is an orofacial pain and jaw function specialist and professor in orofacial pain and jaw function with research experience in various areas of orofacial pain. The last author (TG) is an anesthesiologist, pain physician and professor emeritus in clinical pain research, with experience in several areas of pain medicine.
Demographic and professional characteristics of pain experts in the Delphi panel.

The Delphi process comprised three rounds, which were conducted in English. For the
Open-ended questions (Round 1).

The qualitative part of this study resulted in a second quantitative questionnaire of 42 statements, which was e-mailed to the experts (second round). In this
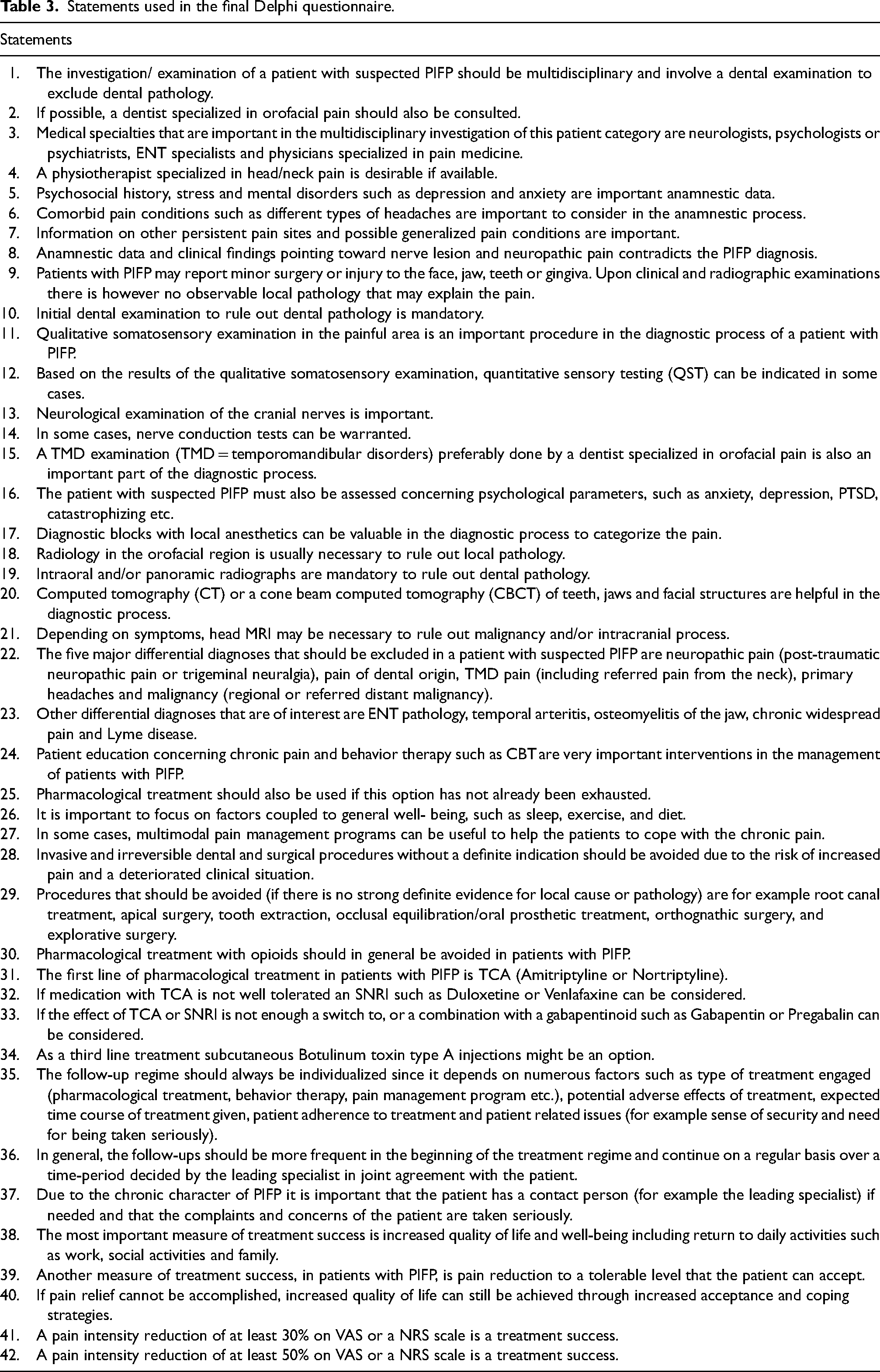
The experts then received a refined questionnaire containing 42 statements (Table 3) for the
Statements used in the final Delphi questionnaire.
Statistical analysis
The results are presented as frequencies and percentages.
Ethical considerations
All experts were informed about the study and that participation was voluntary. Anonymity in a Delphi study allows the participants to express their true opinions without any social influence of other participants. Still, in order to ensure a high response rate and efficient communication, the first author (EL) needed to know the identity of the experts and consequently complete anonymity could not be achieved. The goal of consensus is stated early in the research process, and the method has previously been criticized for putting pressure on participants and making them feel compelled to align their opinions with a shared group understanding (27). Due to voluntary participation and anonymity among experts, the risk of exerting pressure on any participant was considered minimal. Communication with the regional ethical review board confirmed that this study did not require a formal ethical approval.
Results
The present study began in July 2022, and the Delphi process was completed in late June 2023. A summary of the results and a first draft of the manuscript were prepared and presented in October 2024. Post-study discussions were initiated and concluded in March 2025, and joint manuscript writing continued until May 2025. There were no deviations from the study protocol.
During the analysis of the qualitative data in the first questionnaire (first round) four main themes were identified.
The first theme
The results corresponding to each statement in the quantitative questionnaire are presented in Table 4. The response rate was 100% in all rounds. After the third round, one expert made a minor correction in one specific statement, which did not affect the results. The experts reached consensus in 35 out of the 42 statements (83%); in an additional three statements (7%) a majority of the experts agreed with each other. In four statements (10%), no consensus or majority was reached. There was a high degree of consensus already after Round 2. When evaluating response stability among the statements that reached consensus, only Statement 42 failed to show agreement in both Rounds 2 and 3 - it reached consensus only in the final round (Round 3).
Frequency of answers (n) by 16 pain experts on each of the 42 statements in the final Delphi questionnaire (Table 2).

Majority = 11–12 out of 16 pain experts either agreed or disagreed with the statement. Consensus = ≥13 out of 16 pain experts either agreed or disagreed with the statement.
There was consensus among the experts that the diagnostic process in patients with suspected PIFP should be multidisciplinary and include a dental examination and if possible, a consultation with a dentist specialized in orofacial pain (100% agreement). Neurologists, psychologists or psychiatrists, otolaryngologists and physicians specialized in pain medicine were also considered significant specialties in the diagnosis of PIFP (100% agreement). The majority of experts also agreed (75% agreement) that a physiotherapist specialized in head/neck pain is desirable in the evaluation of these patients.
Information about possible generalized pain, comorbid pain conditions and exclusion of the five major differential diagnoses, i.e., neuropathic pain, pain of dental origin, TMD pain (including referred pain from the neck), primary headaches and malignancy were found to be important in the clinical assessment (100% agreement).
Patients with PIFP may have a history of minor surgery or trauma to the face, jaw, teeth or gingiva. However, it is crucial to note that if radiographic examination, anamnestic data and clinical observations suggest local pathology, such as nerve damage and neuropathic pain (characterized by features such as a relevant temporal relationship between the trauma and the onset of pain, as well as somatosensory abnormalities), this would be inconsistent with a diagnosis of PIFP (94% agreement). Although not part of the Delphi process, the post-study discussions revealed that the experts relied on ICOP when considering diagnostic criteria for patients with PIFP.
Computed tomography (CT) or cone-beam computed tomography (CBCT) of the teeth, jaws and facial structures is recommended (81% agreement) and, depending on symptoms, head MRI may also be necessary (88% agreement). These examinations serve to rule out some main differential diagnoses that would require a different treatment regimen.
In terms of management, invasive and irreversible dental and surgical procedures (such as tooth extraction, surgical exploration, or root canal treatment) to treat persistent idiopathic facial pain should be avoided because of the risk of increased pain (100% agreement). However, if another condition (such as periapical periodontitis) explains part of the current pain, dental or surgical interventions may, of course, be indicated, even in patients with PIFP. The expert panel concluded that pharmacological management with tricyclic antidepressants (TCAs), serotonin-norepinephrine reuptake inhibitor (SNRIs) and gabapentinoids is indicated if this option has not already been exhausted. In general, the experts recommended avoiding opioids when treating patients with PIFP (94% agreement). In some cases, multidisciplinary or interdisciplinary pain management programs can be useful (100% agreement). Management should also include factors associated with general well-being, such as sleep and exercise (94% agreement).
Follow-ups should always be individualized and based on several factors such as the type and duration of therapy, potential adverse effects, patient adherence, the presence of comorbid pain conditions, the individual's general health, and other patient-related issues (100% agreement). The most important measure of therapeutic success is improved QoL and well-being (94% agreement). Pain assessment is commonly included in most QoL instruments.
Recommendations for the management of PIFP patients are summarized in Table 5.
Management of persistent idiopathic facial pain – recommendations.

Experience-based opinions, derived from the current Delphi process.
Discussion
The present Delphi study has established international consensus-derived guidelines and recommendations for the evaluation and overall management of patients with PIFP.
Like chronic pain in other regions of the body, orofacial pain can be secondary to another disease or disorder in the orofacial region, or it can be a health condition in its own right (i.e., chronic primary pain) (3). Pain of dental origin (dentoalveolar pain) is the most common type of OFP, followed by TMD pain (11,28). Toothache is most often a secondary pain that requires management of the underlying dental disease. To rule out pain originating in the dental pulp or periapical tissues, consultation with a dentist specialized in Endodontics may thus be helpful. Tooth pain is commonly inflammatory in nature, but it can sometimes be mimicked by primary headache (neurovascular in origin), neuropathic pain or idiopathic pain (28–30).
Examination and collaborative management
In the post-study discussions, it became evident that the experts relied on ICOP when diagnosing PIFP. As mentioned in the introduction, ICOP represents the most recent classification of PIFP and provides a clear, systematic framework that helps healthcare providers to diagnose PIFP and rule out other causes of orofacial pain - such as dental, neuropathic, or TMD pain (2). Therefore, ICOP can be recommended for its standardized approach, which reduces variability in diagnosis and facilitates better communication between healthcare providers. The main difference between ICOP and ICHD-3 is that the latter considers “atypical odontalgia” a possible variant of PIFP and groups both conditions under a single entity, whereas ICOP distinguishes between the two, classifying them separately as PIFP and PIDAP (previously referred to as atypical odontalgia). A comparison of the definitions of PIFP in ICOP (2020) and ICHD-3 (2018) is presented in Table 6.
Comparison of persistent idiopathic facial pain (PIFP) definitions in ICHD-3 (2018) and ICOP (2020).
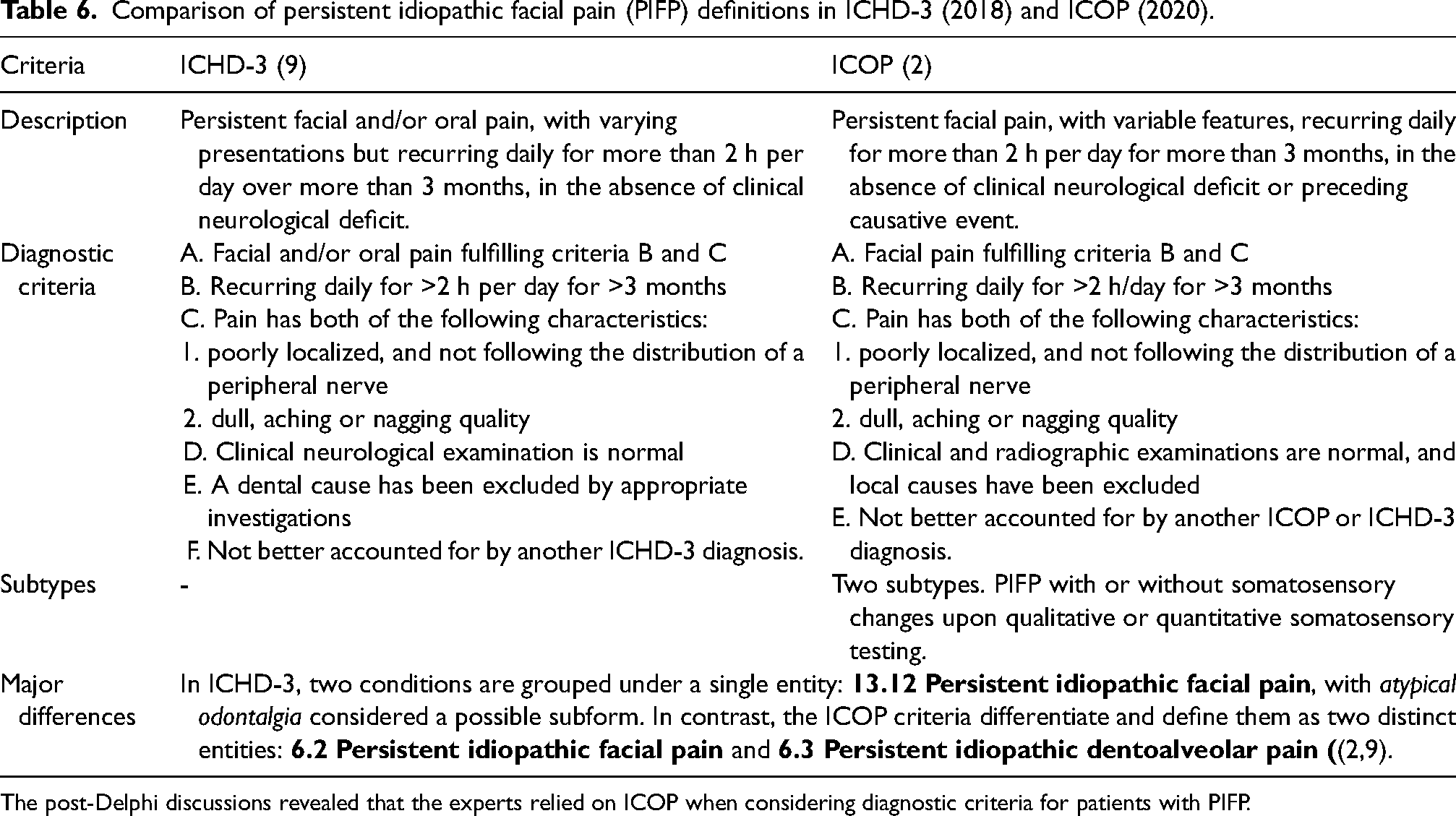
The post-Delphi discussions revealed that the experts relied on ICOP when considering diagnostic criteria for patients with PIFP.
Since the most common OFP must be ruled out first, the expert panel concluded (100% agreement) that a dental examination to rule out dental pathology is mandatory. If possible, a dentist specializing in OFP should also be consulted to exclude TMD pain and other related OFP conditions. Primary headache disorders—specifically migraine and trigeminal autonomic cephalalgias—can present as facial pain, and in rare cases, as isolated facial pain, which makes diagnosis challenging. Targeted interventions for these disorders, such as treatment with triptans, anti-CGRP medications, calcium channel blockers, indomethacin, and anti-epileptics such as lamotrigine, may therefore play an important role in the diagnostic work-up of patients presenting with complex facial pain (31–33).
Different forms of neuropathic pain are important differential diagnoses for PIFP. In many cases of trigeminal neuralgia, patients experience continuous facial pain between paroxysmal attacks, making the exclusion of this condition a necessary part of the diagnostic process for patients with suspected PIFP (15,34). In this Delphi study, pain of dental origin, TMD pain (including referred pain from the neck), primary headaches, neuropathic pain, and malignancy were identified as the five major differential diagnoses for PIFP (100% agreement). One of the guiding principles in both ICOP and ICHD-3 is that all other potential sources of pain must be excluded before a diagnosis of PIFP can be established (2,9).
A multidisciplinary and biopsychosocial approach has been proposed for the assessment and management of many different chronic pain conditions (35–37). Several studies have shown that multidisciplinary multimodal pain management, in which clinicians from various specialties work independently although sharing responsibility for decision-making and pain care, can significantly reduce pain in patients suffering from chronic pain conditions such as non-specific low back pain (35), fibromyalgia (38), and TMD pain (39). Pain management using a multidisciplinary approach has also been found to reduce catastrophizing, self-reported disability, and depression (40), as well as improve physical functioning and facilitate return to work for patients (41,42). Several studies have shown that multimodal pain rehabilitation is superior to standard care in reducing pain and disability in chronic primary pain patients (35,43–45). These findings emphasize the need to integrate different therapeutic approaches in the management of more complex pain conditions to achieve improved outcomes, which is consistent with the findings in our study. An important component of multidisciplinary pain management is early diagnosis and individualized evidence-based therapy (37). Still, it is unclear which component of multimodal interventions - such as education, exercise, or medication – provides the most significant therapeutic effect (36).
Interdisciplinary pain management involves collaboration between caregivers, working together across fields of expertise and sharing therapy approaches. Transdisciplinary pain management, on the other hand, involves not only interdisciplinary collaboration among different caregivers but also the involvement of patients, patient advocacy groups and health care payers, for example health insurance providers (21). The purpose of the transdisciplinary collaboration is to find common ground in values, therapy protocols and new health care structures across the different parts of pain care. It is considered optimal in terms of both clinical effectiveness and economic sustainability (21).
There are significant diagnostic and therapeutic challenges in the management of patients with PIFP. The expert panel in our study recommends a multidisciplinary evaluation (100% agreement) and, in some cases, a multimodal pain management program for these patients (100% agreement). This underscores the importance of key healthcare providers working together in a coordinated manner. This collaborative approach, in which general dentists/endodontists, dentists specialized in orofacial pain, neurologists, psychologists or psychiatrists, otolaryngologists, and physicians specialized in pain medicine working together in a coordinated manner (46), is critical to managing the complexity of PIFP. Unfortunately, such multidisciplinary or interdisciplinary settings are not always available in clinical practice, often resulting in unidisciplinary pain management.
In the evaluation of pain patients, diagnostic blocks with local anesthetics can be of significant value. Blocking nociceptive signals from the periphery can provide important information about the origin and pathways of pain (47). Thus, diagnostic blocks can help differentiate between peripheral, central and referred pain, as well as distinguish between somatic and visceral pain (48). In the orofacial region, peripheral nerve blocks may be used to target the maxillary and mandibular nerves, along with their branches such as the infraorbital, inferior alveolar, auriculotemporal, and masseteric nerves. They can also be administered in specific anatomical areas, such as intra-articularly in the temporomandibular joint (TMJ) and intramuscularly in the masseter and temporal muscles (49). The expert panel concluded (88% agreement) that diagnostic blocks can be valuable in the diagnosis of patients with suspected PIFP.
Somatosensory testing may be important in the evaluation and diagnosis of pain, particularly neuropathic pain. A rigorous system of quantitative sensory testing (QST) has been proposed by the German Research Network on Neuropathic Pain (DFNS) (50,51) and also implemented in the orofacial region (52,53). The expert panel in our study found no consensus concerning the clinical value of using QST in patients with PIFP. The full battery of tests in QST is usually found only in few specialized centers and is not accessible to general practitioners. The expert panel recommended (88% agreement) the more accessible Qualitative Sensory Testing (QualST) which has been suggested for clinical use (54). Nerve conduction testing for motor and sensory nerves may hypothetically provide guidance on, for example, the type of neuropathy (55). Electrophysiological studies, such as blink reflex, masseter inhibitory reflex and trigeminal somatosensory evoked potential examination, have been suggested in the assessment of trigeminal neuropathy (56–59). Still, peripheral nerves supplying the orofacial region are difficult to access for nerve conduction studies. In the present Delphi study, no consensus was found regarding the use of nerve conduction studies in patients with PIFP.
In patients with PIFP, more advanced radiographic techniques such as CBCT, CT or MRI may be needed to exclude differential diagnoses (60). CBCT or CT are particularly useful when facial pain may be related to dental pathology, such as periapical abscesses; sinus disease; or bone-related conditions, such as osteomyelitis, maxillofacial tumors, and TMJ bony changes like degenerative joint disease. In contrast, MRI is better suited for assessing neurovascular structures and soft tissue. It is especially useful for detecting trigeminal nerve pathology, such as neurovascular compression, as well as intracranial conditions, including tumors and multiple sclerosis. MRI can also identify TMJ inflammation and various soft tissue abnormalities (61,62). Ögütcen-Toller et al. (63) suggested that all patients with “atypical facial pain” should undergo MRI because of the risk of intracranial and extracranial lesions.
The expert panel in our study agreed (81% agreement) that CT or CBCT is necessary to rule out local pathology and that MRI may be necessary (88% agreement) to rule out malignancy and/or intracranial processes in patients with PIFP. There was no consensus on the need for intraoral and/or panoramic radiographs in the evaluation of PIFP patients. One could speculate that because patients with PIFP often have had their pain for a very long time, dental examinations including intraoral and panoramic radiographs were often performed early in the process. Furthermore, there was strong consensus (100%) that a dental examination should be conducted in these patients, and intraoral radiographs are generally included as part of a standard dental assessment.
Therapy
Local blocks to specific nerves (49) or peripheral nerve ganglia (64) have been suggested as therapeutic options for many different orofacial pain conditions. However, the evidence of their long-term efficacy remains limited (49). The off-label use of botulinum toxin type A (BTX-A) for pain management, such as TMD related myalgia (65–70) and peripheral neuropathic pain (71), has increased over time, although the evidence for its efficacy remains weak. A review of PIDAP (72), which is thought to be an anatomical variant of PIFP (73), stated that case reports have shown that BTX-A may be a viable therapy. In a randomized controlled trial, Jamtøy et al. (74) investigated the efficacy of BTX-A injection into the sphenopalatine ganglion (SPG) in patients with PIFP. They found no short-term pain reduction compared to placebo (74). In the present Delphi study, there was no consensus or majority opinion supporting the use of BTX-A in PIFP patients, suggesting that it is premature to recommend this therapy.
There is an agreement in the literature that idiopathic orofacial pain, including PIFP, should not be subjected to invasive irreversible surgical interventions because of the risk of aggravating the pain (13,75–77). In our study there was a strong consensus (100% agreement) that invasive and irreversible dental and surgical procedures with the aim of treating the pain should be avoided in PIFP patients unless there is another verified and clear indication for such a procedure. This is an important clinical recommendation and is similar to treatment guidelines for chronic primary low-back pain, which also discourage surgery (78,79). Unfortunately, before PIFP patients reach specialist services, many have undergone irreversible therapies in an attempt to find a “cure” (13,80–82).
Pharmacological therapy with TCAs (83,84), SNRIs (83–86), pregabalin (83,85) and gabapentin (83,87) has been recommended for various chronic pain conditions. These pharmacologic agents have also been suggested in patients with PIFP, although the evidence is sparse (13). There are many patient-specific factors, such as concomitant medication, certain medical conditions etc., that may influence the choice of pharmacologic therapy. In the present study, the majority of experts (69% agreement) recommended TCA as a first-line drug. The frequency of side-effects has been reported to be high with TCA medication (88). If TCA is not suitable or well-tolerated by a patient, the expert panel recommended (81% agreement) that an SNRI should be considered. If the effect of TCA or SNRI is insufficient, a switch to, or a combination with a gabapentinoid such as gabapentin or pregabalin can be considered (81% agreement). Dosing regimens in PIFP patients were not within the scope of the present Delphi study. However, there are some evidence-based recommendations for dosing regimens to manage neuropathic pain that may be considered (81,83,89).
Due to the risk of side effects and addiction associated with long-term opioid use (78,90), non-opioid medications are often preferred in the management of non-cancer chronic pain (91). Notably, the expert panel in our study recommended (94% agreement) that opioids should be avoided in the management of PIFP.
The expert panel in our study concluded (96% agreement) that it is also important to focus on factors related to general well-being, such as sleep and exercise, in patients with PIFP. There is evidence to suggest that these factors are important in the management of chronic primary pain (92–96), whereas data on PIFP remains sparse. An association between sleep and pain has been established, and poor sleep has been shown to adversely affect pain management (92). It has been suggested that interventions targeting sleep disturbances and fatigue may increase effectiveness of interdisciplinary pain programs (93). Still, the relationship between sleep and PIFP is unknown (13). The majority of PIFP patients do not experience pain-related awakenings (97) and report that their sleep is pain-free (98). Long-term physical exercise can reduce pain in many different chronic pain conditions, although the pain response may differ between different diagnoses (94–96).
Follow-ups and therapeutic success
Non-adherence can be a major problem in medical therapy and results in substantial health care costs (99). Arrangements for convenient follow-up visits and improved patient-provider communication are thought to increase adherence to prescribed therapies (100). Trust between caregiver and patient is also very important to improve therapeutic outcomes (101). In PIFP patients the expert panel recommended (100% agreement) frequent initial follow-up visits and a patient-specific contact person to build trust and increase patient adherence.
It is important to assess the therapeutic effect in order to adequately evaluate whether a therapy is beneficial in the inpatient setting (102). Farrar et al. (102) suggested that a 30% reduction in pain intensity on a numerical rating scale (NRS) is a clinically relevant outcome in chronic pain patients receiving pregabalin. Others have used 50% (or greater) reduction in pain as an outcome variable for analgesic efficacy (103). According to our expert panel, another measure of therapeutic success in these patients is when pain is reduced to a tolerable level (100% agreement). Although pain intensity is often chosen as the primary outcome variable in pain research, other outcome variables such as pain-related disability, quality of life, psychological impact, and patient satisfaction are also important. IMMPACT (the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials) recommends the following domains are recommended in the evaluation of chronic pain management: pain intensity, global improvement, symptoms and adverse events, participant disposition, emotional and physical functioning (104). In ICD-11, severity is assessed in three dimensions: intensity, distress and disability (6). These dimensions can be assessed using NRS or questionnaires (105). Quality of life encompasses several domains, including health, spiritual well-being, and social and psychological functioning. Pain intensity and self-efficacy are important predictors of QoL in patients suffering from chronic pain (106). Chronic pain is a common cause of long-term sick leave and disability (107). Sick leave is a major economic burden for both society and the individual, and return to work is therefore crucial (108). The expert panel reached a consensus (94% agreement) that the most critical measures of therapeutic success in patients with PIFP are improved QoL and well-being including return to daily activities.
Methodological concerns
In both medicine and dentistry, there are contrasting attitudes towards opinions derived from experts and their clinical experience. The scientific value of “consensus opinion of experts” has been ranked very low (109). Still, clinical experience is very important in the application of research evidence to specific patients (110) and in areas such as the management of patients with PIFP, where evidence is inadequate or even non-existent (111).
The term “expert” in a Delphi study and the fact that a particular selected group represents a valid “expert opinion” have been criticized (112). In this study, an expert was defined as a researcher with identifiable peer-reviewed publications and at least 10 years of clinical experience in the management of pain patients. Although the selection of experts was subjected to bias, it is important to remember that they were chosen for a specific purpose - to share their knowledge, experience and opinions on a specific topic.
Our panel had a majority of European experts and covered three of the six WHO regions. This regional bias should be considered when interpreting the results. The composition and size of an expert panel depend on the desired perspective. For a broad view, a heterogeneous group — including researchers, clinicians, patients, public members, and administrators — is ideal. For more specific issues, such as management of rare pain conditions like PIFP, a homogeneous panel of specialists is preferable. Panel size recommendations for a homogenous group vary in the literature: Manyara et al. (113) suggest 20–30, while Clayton et al. (114) recommends 15–30 for homogeneous panels. Although a large number of experts (30–50) may improve replicability and provide more representative data, it may also result in a large data set and subsequent complex data analysis. Delphi studies can be conducted with as few as 10–15 experts and still be effective (115). Our panel of 16 participants is at the lower end and may warrant some criticism.
Percentage agreement is the most common method for defining consensus in a Delphi study. Various thresholds have been suggested: Loughlin and Moore (116) proposed 51%, Sumsion (117) recommended 70%, and Green et al. (118) suggested 80% agreement for consensus to be met. In our study, we set the consensus threshold at 80% agreement or disagreement. If 65–70% agreement or disagreement was reached, the second threshold majority was met. Even when consensus is reached or a majority of experts agree on an issue, it is important to emphasize that this does not necessarily mean that the “absolute truth” or “correct belief” has been established.
The original Delphi method includes four rounds, but some authors recommend two or three rounds (27,112). Besides achieving consensus, the stability of responses between multiple rounds is a measure used to determine whether or not additional rounds should be used (119). Too few rounds may not yield meaningful data. On the other hand, too many rounds may lead to sample fatigue and a decrease in response rates (27,120). In this study, three rounds were required to achieve either consensus or response stability between the rounds. Stability between rounds is an inherent aspect of the Delphi process, whether there is consensus, majority agreement, or bipolarity (121). In this study, the Delphi process was concluded when either consensus was reached or stability in responses across rounds was demonstrated. This stopping criterion may, in theory, result in a lack of response stability in cases where consensus is achieved. A high degree of consensus was already observed after Round 2. When evaluating response stability among the statements that reached consensus, only Statement 42 failed to demonstrate consensus in both Rounds 2 and 3 — it reached consensus only in the final round (Round 3). A fourth round was not conducted solely due to the lack of response stability in Statement 42. Additionally, after Round 3, the experts were given a final opportunity to review their responses in the third questionnaire and correct any input errors. As noted in the results, only one expert made a minor correction to a specific statement. This correction did not affect the outcome in terms of consensus classification (Consensus, Majority, or No Consensus). While this opportunity to review and correct input in Round 3 did not constitute an additional fourth round (i.e., it did not include free-text comments, controlled feedback, etc.), it may still have implications when discussing response stability, as the expert panel participants were evidently satisfied with their answers.
Notably, this study achieved a 100% response rate, which is ideal. The Delphi method has been criticized for lack of reliability and validity (27,112). However, studies suggest that the method has acceptable reliability (122) and content validity (123). Due to the size of the expert panel, the geographic distribution, and the strict criteria used to define an expert, we believe that our panel is representative of a group of international pain experts, and therefore we can expect the results to have content validity. Several of the synthesized statements were general in nature. Anonymity in the Delphi methodology can be seen as a limitation in terms of depth and nuance, but it is also one of the method's greatest strengths — allowing for independent input free from group dynamics or dominant voices (24). In the post-study discussion, it was concluded that further research is needed to develop more specific and nuanced treatment recommendations, particularly in the area of pharmacological treatment.
Conclusion
In conclusion, this Delphi study has established international expert-based consensus guidelines and recommendations for the evaluation and management of patients with PIFP (Table 5), which reinforce several earlier recommendations reported in the literature (13,124,125). The recommendations emphasize the importance of interdisciplinary collaboration in the examination and management of these patients, involving coordinated efforts among general dentists or endodontists, dentists specialized in orofacial pain, neurologists, psychologists or psychiatrists, otolaryngologists, and physicians specialized in pain medicine. Therapeutically, invasive and irreversible dental and surgical procedures to treat PIFP should be avoided because of the risk of increased pain. Pharmacological management with TCAs, SNRIs, and gabapentinoids may be considered, provided that these options have not already been exhausted. Finally, the most important measure of therapeutic success is reduction of pain to a level considered acceptable by the patient and improved quality of life.
Supplemental Material
sj-docx-1-cep-10.1177_03331024251399927 - Supplemental material for Management of persistent idiopathic facial pain (PIFP) – An international Delphi study
Supplemental material, sj-docx-1-cep-10.1177_03331024251399927 for Management of persistent idiopathic facial pain (PIFP) – An international Delphi study by Erik Lindfors, Per Alstergren, Rafael Benoliel, Paulo Conti, Justin Durham, Jean-Paul Goulet, Osamu Komiyama, Thomas List, Arne May, Dimos-Dimitrios Mitsikostas, Donald R. Nixdorf, Maria Pigg, Tara Renton, Gunnar Skagerberg, Peter Svensson, Rolf-Detlef Treede, Jens Christoph Türp, Joanna M. Zakrzewska and Torsten Gordh in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024251399927 - Supplemental material for Management of persistent idiopathic facial pain (PIFP) – An international Delphi study
Supplemental material, sj-docx-2-cep-10.1177_03331024251399927 for Management of persistent idiopathic facial pain (PIFP) – An international Delphi study by Erik Lindfors, Per Alstergren, Rafael Benoliel, Paulo Conti, Justin Durham, Jean-Paul Goulet, Osamu Komiyama, Thomas List, Arne May, Dimos-Dimitrios Mitsikostas, Donald R. Nixdorf, Maria Pigg, Tara Renton, Gunnar Skagerberg, Peter Svensson, Rolf-Detlef Treede, Jens Christoph Türp, Joanna M. Zakrzewska and Torsten Gordh in Cephalalgia
Footnotes
Acknowledgment
ChatGPT (OpenAI) was used for minor language polishing to enhance the clarity and readability of the manuscript.
Author contributions
EL was responsible for the conceptualization of the study. The three lead authors (EL, PA, and TG) developed a questionnaire consisting of ten open-ended questions focused on the management of PIFP, which was sent to sixteen experts in the Delphi panel (Round 1). The free-text responses from this questionnaire were analyzed by the lead authors resulting in a second, quantitative questionnaire that was again sent to the expert panel (Round 2 and 3). After the third round, the study was closed, and the results were analyzed and extensively discussed by all authors, including both the expert panel and the lead authors. All authors contributed to editing, reviewing, and approving the final manuscript for submission.
Consent to participate
Before being included in the study, the experts received written information about the study.
Data availability statement
All data generated during this study are included in this published article. To ensure transparency regarding the qualitative part of the study, supplementary information with supporting quotes for each statement can be found in Online Supplemental Appendix A. Additional supplementary material, describing the development of the statements between Rounds 2 and 3, is provided in Online Supplemental Appendix B. Further data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Public Dental Health Service, Uppsala, Sweden (grant number FTVLUL-984093 and FTVLUL-991859).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.