
Abstract
Aim
Primary headache disorders such as migraine and tension-type headache are highly prevalent in military populations and may severely impact operational performance and readiness. Despite this, data from many European armed forces are lacking. This study investigates headache phenotypes, diagnosis, treatment and functional impairment in active-duty personnel of a major European military organization.
Methods
This cross-sectional cohort study utilized an anonymous 33-item online questionnaire distributed across military medical centers in Germany between May and July 2023. The survey assessed demographics, headache types according to the International Classification of Headache Disorders, 3rd edition (ICHD-3), diagnostic awareness, treatment history and headache-related disability using the Migraine Disability Assessment Score (MIDAS).
Results
Of the 1189 participants, 914 (77%) completed the survey. Among them, 839 (94.9%) reported experiencing headaches in the past 12 months. Based on ICHD-3 criteria, 227 individuals (27.1%) met the complete set of criteria for migraine, while 246 (29.2%) were classified as probable migraine. Tension-type headache was reported by 222 respondents (26.5%), and cluster headache was resported by 34 (4.1%). Notably, 61.4% of participants had never received a formal diagnosis and only 38.6% had ever sought medical care for their headaches. Functional impairment was substantial: 63.8% reported losing at least one workday in the past three months due to headache. Among those with migraine, an average of 3.9 workdays per month were lost. Despite this burden, only 27.3% of individuals with migraine had ever used preventive medication.
Conclusions
Primary headache disorders are common, underdiagnosed and inadequately treated in this military population, leading to significant functional and operational impairment. Our findings underscore the urgent need for improved screening, diagnosis and evidence-based treatment strategies in uniformed health systems. The results may inform similar efforts in other military and high-demand occupational settings.
This is a visual representation of the abstract.
Keywords
Introduction
Headache disorders disproportionately affect individuals in their most active years, posing a challenge to workforce sustainability and operational readiness in demanding environments such as the military (1–3). In Germany, the 12-month prevalence for all types of headache is approximately 60%, with migraine ranging between 6.8% and 16%, tension-type headache (TTH) between 12.5% and 19.9%, and cluster headache between 0.1% and 0.2%, depending on the study (4–9). When including individuals who fulfill only three of the four International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria (10), the one-year prevalence of migraine increases to 28.4% in women and 18.0% in men, while TTH affects 28.2% of women and 21.8% of men (11).
Migraine and other headache disorders primarily affect young adults, with the highest prevalence found in the fourth decade of life (6,11,12). Globally, migraine is the second most common neurological cause of years lived with disability, second only to stroke (3,13). It is the second leading cause of disability across all ages and sexes worldwide and the leading cause of disability in young women (13,14).
Headaches also pose a significant health concern in military settings. As early as during the Vietnam War, headache and migraine were frequently reported by soldiers and documented by neurologists deployed in combat zones (15). A study investigating the prevalence and impact of migraine on Reserve Officer Training Corps cadets in the US Army found a migraine prevalence of 18%, with 14% in men and 31% in women (16). Similarly, a study conducted among US soldiers returning from Iraq revealed higher-than-expected rates of migraine and other headache types, especially in a predominantly young male cohort (17).
US soldiers exposed to combat situations were significantly more likely to develop headaches post-deployment (18). Headache occurrence was associated with female sex, younger age, lower rank and comorbidities such as anxiety disorders, depression, post-traumatic stress disorder (PTSD) and other pain syndromes. A strong association between migraine, combat exposure, PTSD and physical injury has been reported (19).
Neurological disorders, including headaches, are among the most common causes of medical evacuation from combat zones, ranking third after musculoskeletal disorders and combat injuries (20). The most frequently diagnosed headache types among US soldiers evacuated from Iraq between 2004 and 2009 were post-traumatic headache (34.1%), migraine (30.0%) and TTH (11.4%). When soldiers were evacuated primarily due to headache, they were twice as likely not to return to duty in the combat zone. Predictors of poor outcomes included physical injuries and comorbid psychiatric disorders (20,21).
Headaches are also common and disabling in the British Armed Forces, where severe headaches are strongly associated with PTSD, psychological distress and multiple somatic complaints (22).
The Bundeswehr is the unified armed forces of Germany, comprising around 183,000 active-duty soldiers and supported by a network of approximately 1000 military and civilian medical facilities, including five military hospitals. Its medical service (“Zentraler Sanitätsdienst”) provides comprehensive healthcare to personnel during training, deployment and rehabilitation, both domestically and abroad. To date, data on headache disorders in the active-duty personnel of the German Bundeswehr are lacking. Specific information on headache types, treatment approaches and service-related consequences is unavailable. While international military studies highlight headache burden, no such data exist for the German Bundeswehr, necessitating targeted research. Therefore, the present study aims to investigate the impact, diagnostic awareness, treatment strategies, and operational impact of headache disorders in active-duty Bundeswehr personnel.
Methods
Ethical approval and data protection
This project was approved as a special military medical research initiative by the Medical Service Command of the German armed forces (Project ID: 48K3-S-33 2323). The study protocol was reviewed and approved by the Ethics Committee of Kiel University (Reference: D 453/23). Participation was voluntary. This study adhered to the principles of the Declaration of Helsinki (1964) and its subsequent revisions. At the beginning of the online questionnaire, participants were informed that data collection would be anonymous and that withdrawal after submission would not be possible.
Study design and population
This was a cross-sectional cohort study conducted using an anonymous online questionnaire. The aim was to assess headache phenotypes, treatment strategies, access to care and the impact of headache disorders on duty performance in active-duty German armed forces personnel. The survey was conducted between 15 May and 31 July 2023.
All active-duty military personnel aged 18–65 years were eligible to participate. Recruitment was carried out via flyers distributed to sven regional medical support centers, 120 military medical clinics and 10 satellite medical facilities across Germany. The flyers contained a QR code linking to the survey and were accompanied by an explanatory letter. The local medical personnel were asked to display and distribute the materials to local departments. Reminder emails with the flyer were sent after seven and nine weeks to encourage participation. The response or rejection rate from each center was not systematically tracked; therefore, precise numbers on non-participation cannot be provided.
Questionnaire content
The questionnaire included 33 items. Initial questions collected demographic information including age, sex, military status, rank category, service branch or organizational department, federal state of the military department and days of deployment abroad in the past 12 months. Participants were then asked whether they had ever experienced headaches and whether they had suffered from headaches in the previous 12 months. A negative response to either question terminated the survey.
Participants reporting headaches in the previous 12 months were further asked about the number of headache days in the past 30 days. Phenomenological descriptions of migraine, TTH and cluster headache (based on ICHD-3 criteria) were presented, and participants were asked to indicate which types they experienced and how often. Multiple headache types could be selected.
Subsequent sections addressed previous medical care, headache diagnoses, the use of acute treatments and preventive medications. The final question was an open-response item allowing participants to comment on perceived deficits in care or to suggest improvements for the treatment of headache and migraine in the military context.
To ensure content validity, the questionnaire was reviewed by a panel of clinical experts in neurology, headache medicine and military healthcare. The experts assessed each item for clinical relevance, clarity, and alignment with the ICHD-3. Minor adjustments were made based on their feedback to improve comprehensibility and diagnostic accuracy.
Data analysis
Only fully completed questionnaires were included in the analysis. Demographic data and headache prevalence (lifetime, 12 months and one month) were first assessed. Subsequent analyses were restricted to participants who reported headaches in the past 12 months. Reported headache types were classified according to the ICHD-3. If diagnostic criteria were not sufficiently met, headache type was classified as “unspecified”.
Headache-related disability was measured using the Migraine Disability Assessment Score (MIDAS), which quantifies functional impairment over the previous three months (23). Healthcare utilization was also evaluated, including medical consultations, received headache diagnoses, and use of acute and preventive pharmacologic therapies.
Bias and missing data
The characteristics of individuals who did not participate could not be assessed. Incomplete questionnaires were excluded to maintain the reliability and interpretability of the data, particularly with respect to diagnostic classification according to ICHD-3 criteria and the calculation of MIDAS scores. Partial datasets may introduce bias or limit comparability across key variables. Given the large overall sample size and high completion rate, the exclusion of incomplete entries is unlikely to have compromised the representativeness or validity of the findings.
Statistical analysis
All data analyzed in this study were collected and exported as Excel (Microsoft Corp.) files from the online survey platform Questionstar (https://www.questionstar.de), which was used to distribute the questionnaire and compile responses. Descriptive statistics are provided as means for continuous variables, and as counts and percentages for categorical variables. Analyses were based on available (non-missing) data. All statistical analyses were performed using Prism, version 9 (GraphPad Software Inc.) and RStudio (Posit PBC).
Results
Demographic data
In total, 1189 service members participated in this study, of whom 914 (77%) completed the questionnaire in full. The study flow diagram and the distribution of headache phenotypes are shown in Figure 1. Figure 2 illustrates the distribution by sex, age groups, military status, rank categories, service branches and organizational departments, as well as days of military deployment abroad in the past year and the federal states where participants were stationed.

Study flow diagram and distribution of headache phenotypes.

Demographic characteristics of the study population. (a) Gender distribution and (b) age structure of the overall cohort. (c) Type of service engagement and (d) distribution across different rank groups. (e) The branches of the armed forces and organizational units to which participants belonged. (f) The number of deployment days in the past year. NCO = non-commissioned officer.
Table 1 provides an overview of the demographic characteristics of the various subgroups and the distribution of headache features. Of the participants, 578 (63.2%) were male, 333 (36.5%) were female and three (0.3%) identified as non-binary. The median age was 35 years. Approximately one-third of participants were between 26 and 35 years old (36.0%; n = 329), another third were between 36 and 45 years old (30.4%; n = 278), and the remainder were distributed as follows: 18–25 years (16.1%; n = 147), 46–55 years (14.2%; n = 130) and 56–65 years (3.3%; n = 30).
Overview of the characteristics of the study population.
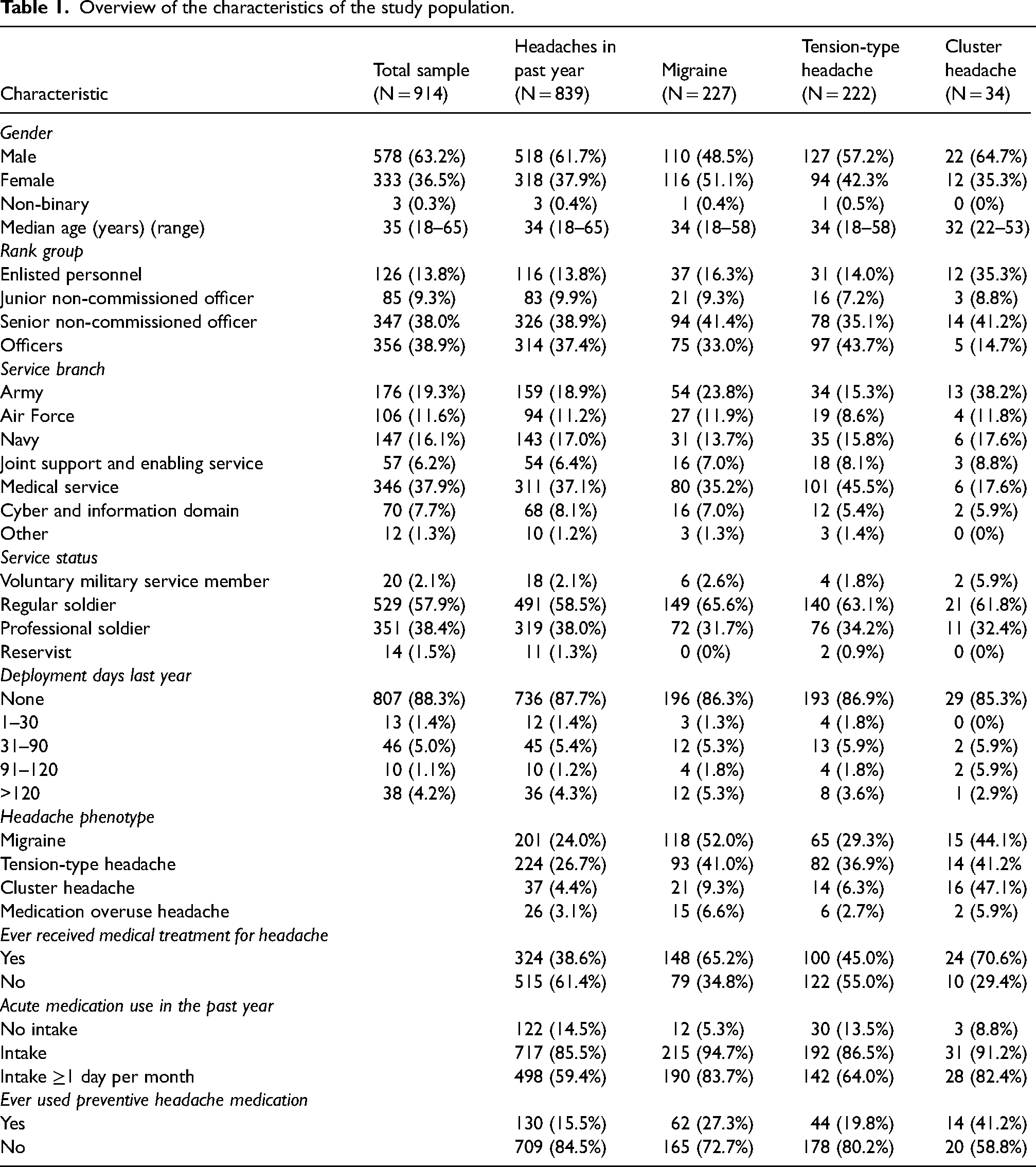
Most participants were regular soldiers (57.9%; n = 529), while professional soldiers made up 38.4% (n = 351). Only a small number of participants were voluntary military service members (2.2%; n = 20) or reservists (1.5%; n = 14).
With regard to rank categories, officers represented 38.9% (n = 356), senior non-commissioned officers made up to 38.0% (n = 347), junior non-commissioned officers accounted for 9.3% (n = 85) and enlisted personnel accounted for 13.8% (n = 126).
Participants were affiliated with various service branches and organizational departments. The Medical Service was the most represented, accounting for 37.9% (n = 346), followed by the Army (19.3%; n = 176), the Navy (16.1%; n = 147) and the Air Force (11.6%; n = 106). The Cyber and Information Domain Service comprised 7.7% (n = 70), and the Joint Support Service comprised 6.2% (n = 57).
While nearly all federal states and some departments abroad were represented, almost two-thirds of the participants were stationed in three federal states: Baden-Württemberg (24.6%; n = 225), Bavaria (20.6%; n = 188) and Schleswig-Holstein (19.1%; n = 175).
Only a small proportion of participants had been deployed abroad in the previous 12 months (11.7%; n = 107). Among these, 13 participants (1.4%) reported up to 30 deployment days, 46 (5.0%) between 31 and 90 days, 10 (1.1%) between 91 and 120 days, and 38 participants (4.2%) reported more than 120 deployment days in the past year.
Headaches among members of the German armed forces
Of the 914 participants, 30 individuals (3.3%) reported never having experienced a headache. Among the remaining 884 participants, 839 (94.9%) reported having suffered from headaches in the past 12 months (Figure 3). Of these, 518 (61.7%) were male, 318 (37.9%) were female and three (0.4%) identified as non-binary.

Some 94.4% of the study participants reported experiencing headaches within the past 12 months. In total, 776 participants had at least one headache day in the past month. In total, 5316 headache days were reported by participants over the past 30 days.
Among the 839 participants who reported headaches in the past year, 776 (92.5%) experienced at least one headache day in the past 30 days. The specific details are as follows:
35.6% (n = 299) reported 1–3 headache days; 28.5% (n = 239) reported 4–7 headache days; 16.4% (n = 138) reported 8–14 headache days; 11.9% (n = 100) reported 15 or more headache days in the past month;
Daily headaches within the past year were reported by 18 participants (2.1%).
Among the 807 participants who were not deployed abroad, 736 (91.2%) reported headaches in the past 12 months. Of these, 196 participants (24.3%) met the diagnostic criteria for migraine. In contrast, among the 107 participants who had been deployed abroad during the past year, 103 (96.3%) reported headaches in the past 12 months and 31 (29.0%) met the criteria for migraine.
Of the 48 participants who reported more than 90 days of foreign deployment within the past year, 46 (95.8%) experienced headaches and 16 (33.3%) met the criteria for migraine.
Clinical characteristics
Among the 839 participants who reported experiencing headaches in the past 12 months, 227 (27.1%) met the ICHD-3 criteria for migraine. An additional 246 participants (29.2%) fulfilled all but one of the diagnostic criteria and were classified as having probable migraine. Together, migraine and probable migraine accounted for more than half (56.4%; n = 473) of all reported headache cases. The gender-specific distribution of migraine and probable migraine is summarized in Table 2.
Gender distribution and frequency of migraine and probable migraine among participants.
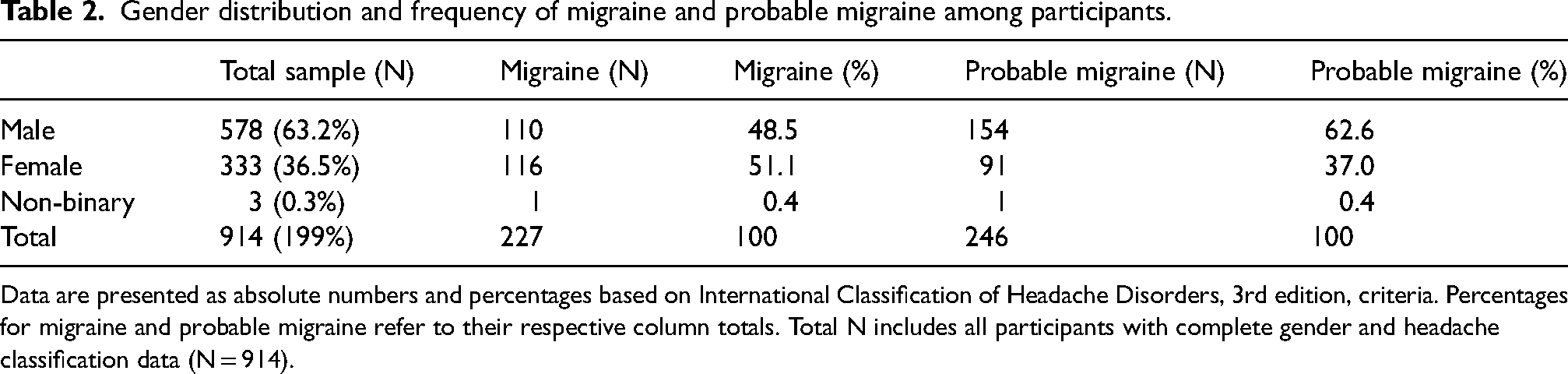
Data are presented as absolute numbers and percentages based on International Classification of Headache Disorders, 3rd edition, criteria. Percentages for migraine and probable migraine refer to their respective column totals. Total N includes all participants with complete gender and headache classification data (N = 914).
TTH was reported by 222 participants (26.5%) and 34 participants (4.1%) met the criteria for cluster headache. Multiple diagnoses were noted: 148 participants met the criteria for both migraine/probable migraine and TTH; 29 participants met the criteria for migraine/probable migraine and cluster headache; and 13 met the criteria for TTH and cluster headache. Eleven participants met the criteria for all three headache types. Additionally, 289 participants (34.4%) reported experiencing other headache types not covered by the three primary ICHD-3 categories.
Awareness of headache diagnosis
Figure 4 illustrates participants’ awareness of their headache diagnoses. Overall, 61% of respondents had no prior knowledge of their specific headache type. Among those who experienced headaches in the past year, 39% had received a formal diagnosis (migraine, TTH and/or cluster headache) prior to the survey. For all three headache types, significant discrepancies were observed between ICHD-3-based classifications and previously assigned clinical diagnoses (Figure 4).

Diagnosis of different headache types. (a) In 39% of participants who had experienced headaches within the past 12 months, a prior medical diagnosis of a headache disorder (migraine, tension-type headache and/or cluster headache) had already been established. For the different headache types, comprising migraine (b), tension-type headache (c) and cluster headache (d), notable discrepancies were observed between the classifications made in our study based on International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria and the diagnoses previously assigned due to medical consultation.
Migraine
Of all participants who experienced headaches in the past 12 months, 227 fulfilled the diagnostic criteria for migraine (Figure 5). Of these, 51.1% (n = 116) were female and 48.4% (n = 110) were male. Only 52.0% (n = 118) had previously received a migraine diagnosis. The remaining 48.0% (n = 109) met all of the diagnostic criteria but had never been diagnosed. Conversely, 83 participants reported having been diagnosed with migraine but did not meet all the diagnostic criteria in the survey. Among them, 59 met two of the three criteria (probable migraine), 19 met only one criterion and five met none.
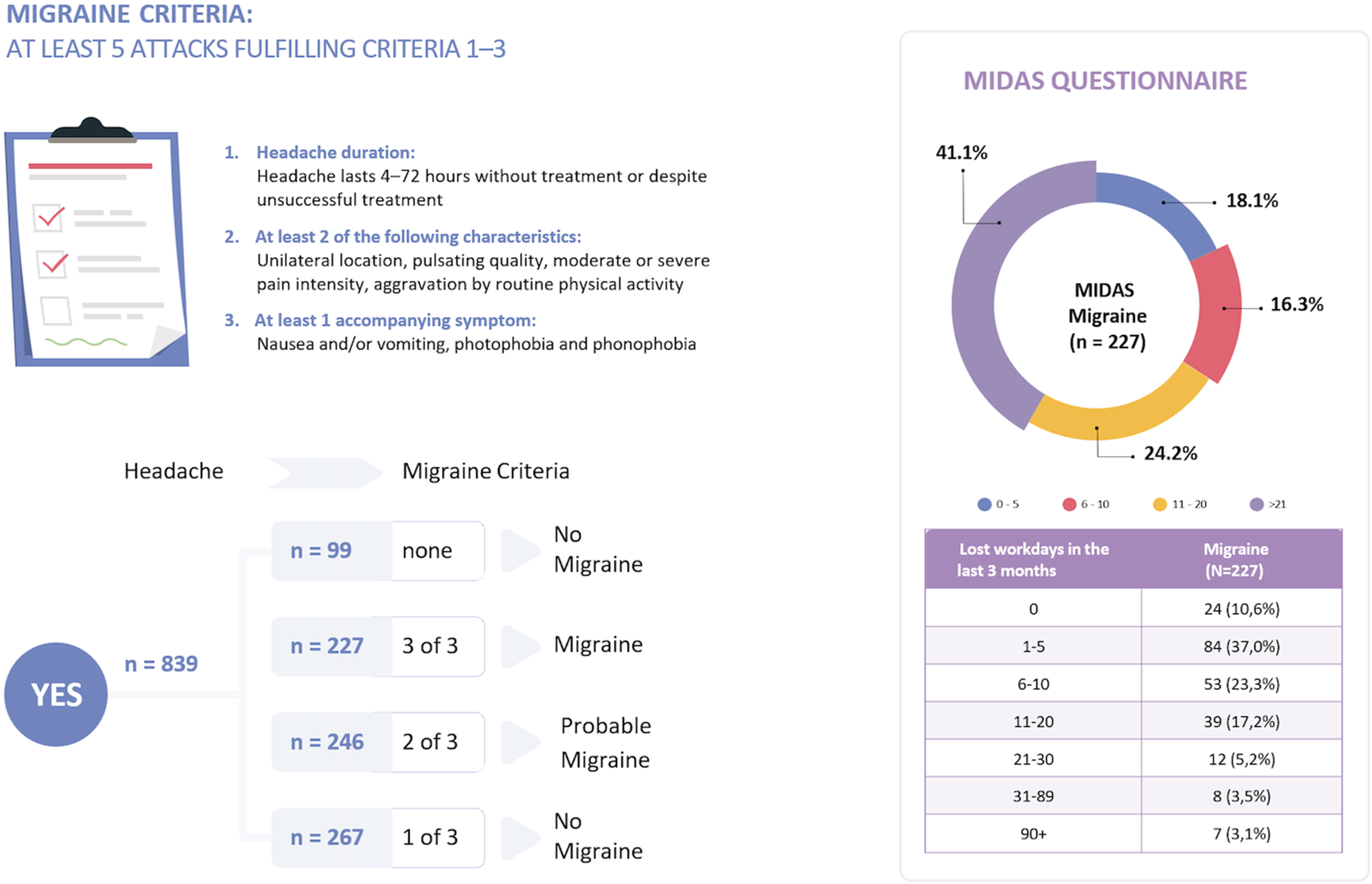
Diagnosis and impact of migraine. Classification as migraine, probable migraine or no migraine based on the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria. The impact of migraine is depicted using the MIDAS score and the number of workdays lost over the past three months. MIDAS = Migraine Disability Assessment Score.
Only a portion of those participants meeting diagnostic criteria for migraine had sought medical care. Medical consultation was highest (89.8%; n = 106) among those with matching clinical and ICHD-3 diagnoses. In contrast, only 38.5% (n = 42) of those with undiagnosed but criteria-confirming migraine had received medical care. Among those diagnosed without meeting the criteria, 66.6% (n = 16) had sought treatment (Figure 4(b)).
Tension-type headache
In total, 222 participants met all ICHD-3 criteria for TTH (Figure 6). Among them, 42.3% (n = 94) were female and 57.2% (n = 127) male. A prior diagnosis of TTH had been made in 36.9% (n = 82); the remaining 63.1% (n = 140) had never been diagnosed, despite meeting all the criteria. Conversely, 142 participants reported having been previously diagnosed with TTH but did not meet all of the diagnostic criteria in the survey.

Diagnosis and impact of tension-type headache. Classification based on International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria. In total, 222 participants met the diagnostic criteria for tension-type headache, with two-thirds of them simultaneously fulfilling the criteria for migraine or probable migraine. To assess the specific impact of tension-type headache, only the 74 participants with a “pure” tension-type headache (i.e. without overlapping migraine diagnosis) were included in the analysis. MIDAS = Migraine Disability Assessment Score.
Medical consultation rates followed similar patterns: 74.4% (n = 61) of those with confirmed diagnoses had received medical care versus 28.0% (n = 39) of the undiagnosed participants meeting the criteria. Among those diagnosed without fulfilling all three criteria, 76.1% (n = 108) had received care (Figure 4(c)).
Cluster headache
In total, 34 participants met all of the diagnostic criteria for cluster headache (Figure 7), including 12 women (35.3%) and 22 men (64.7%). Of these, 16 (47.1%) had previously been diagnosed, while 18 (52.9%) met all the criteria without having received a diagnosis. Additionally, 21 participants reported a prior cluster headache diagnosis but did not meet all of the criteria in this survey.

Diagnosis and impact of cluster headache. In total, 34 participants met the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria for cluster headache based on the survey responses. The assessment of disability was restricted to those participants who fully met all diagnostic criteria for cluster headache, had already received a formal diagnosis, and had previously sought medical treatment for their headache condition. MIDAS = Migraine Disability Assessment Score.
Among those with matching diagnoses, nearly all (94.0%; n = 15) had received medical care. Among undiagnosed but criteria-fulfilling participants, only 50.0% (n = 9) had sought treatment. Among those diagnosed without fulfilling all criteria, 81.0% (n = 17) had received care (Figure 4(d)).
Headache-related impairment
In total, participants lost 5258 workdays over the three-month period, equivalent to an average of 2.1 days per person per month. MIDAS by headache type and gender are presented in Table 3. More than one-third of the participants reported moderate-to-severe disability, with a higher prevalence among women.
Migraine Disability Assessment Score (MIDAS) by headache type and gender.

MIDAS grading: 0–5 = little or no disability; 6–10 = mild disability; 11–20 = moderate disability; 21+ = severe disability.
Among all 839 participants who experienced headaches in the past 12 months, 118 (14.1%) reported having missed work on at least one day due to headaches within the past three months. The majority (n = 94) reported missing 1–5 workdays, while 14 missed 6–10 days and 10 missed more than 10 days. Three participants reported being continuously unable to work due to headaches.
In addition, 528 participants (62.9%) reported a reduction in work performance of at least 50% on one or more days within the past three months. Nearly half of all respondents (49.7%; n = 417) reported reduced productivity on up to 10 days. An additional 72 participants (8.6%) reported such an impairment on 10–20 days, 39 (4.6%) on more than 20 days and eight participants reported daily work capacity impairment.
When combining days of complete work loss with days of ≥50% productivity reduction, 63.8% (n = 535) of the participants experienced at least one day of work-related impairment due to headache within the past three months. Specifically, 35.3% (n = 296) reported 1–5 affected days, 13.3% (n = 112) reported 6–10 days, 9.5% (n = 80) reported 11–20 days, 2.4% (n = 20) reported 21–30 days and 2.2% (n = 18) reported 31–89 days. Nine participants (1.1%) reported 90 affected days, consistent with continuous impairment or total inability to work.
Migraine-related impairment
Of the 227 participants who met all diagnostic criteria for migraine in our survey, 18.1% (n = 41) reported little to no disability, 16.3% (n = 37) reported mild disability, 24.2% (n = 55) reported moderate disability and 41.4% (n = 94) reported severe disability due to their headaches as assessed by the MIDAS questionnaire.
Of the participants, 203 (89.4%) reported the loss of at least one workday due to headaches within the past three months.
Among the respondents, 203 (89.4%) reported at least one workday lost due to headaches within the preceding three months. Of these, 66 individuals (32.5%) reported more than 10 days of work loss and seven participants reported daily impairment or complete inability to work (Figure 5). In total, this subgroup accounted for 2659 lost workdays over the three-month period, corresponding to an average of 3.9 days lost per person per month.
Tension-type headache-related impairment
Due to diagnostic overlap, impairment was assessed only in the 74 participants who exclusively met the TTH criteria. Among them, 70.3% (n = 52) reported little or no impairment, and 14.9% (n = 11) reported mild, 9.5% (n = 7) reported moderate and 5.4% (n = 4) reported severe disability (Figure 6).
Cluster headache-related impairment
To assess impairment, only 15 participants (11 men and four women) with a cluster headache diagnosis, fulfillment of the ICHD-3 criteria and prior medical treatment were included. Among them, 26.6% (n = 4) reported little or no disability, and 6.6% (n = 1) reported mild, 13.3% (n = 2) reported moderate and 53.3% (n = 8) reported severe disability (Figure 7).
Medical care and treatment
Figure 8 provides an overview of previously received headache-related medical care. Of 839 participants, 324 (38.6%) had sought medical attention. Medical consultations correlated with headache frequency and severity. Among the 100 participants with chronic headaches (≥15 days per month), 57% (n = 57) had received medical care. Of 227 migraine cases, 65.2% (n = 148) had sought treatment. Among 139 participants with four or more migraine days per month, 67.6% (n = 94) had received care. Among 94 participants with severe impairment according to MIDAS, 75.5% (n = 71) had received treatment.

Medical care of individuals with headache. (a) Treatments received and medical specialties consulted due to headache. (b) The majority of participants (85.2%) had previously used medication for acute headache treatment. (c) Only a small proportion (15.6%) had used pharmacological prophylaxis for headache.
Most medical visits were to military physicians (84.0%; n = 272). Fewer involved referral to a military neurologic outpatient clinic (41.7%; n = 135), civilian neurologists (26.5%; n = 86) or physical therapists (33.3%; n = 108). Hospital emergency visits were reported by 12.0% (n = 39).
Of 839 participants, 717 (85.5%) had used acute headache medication in the past year. Among them, 69.5% (n = 498) used medication at least once per month, with 58.8% (n = 422) using it fewer than 10 days per month. Frequent use (≥10 days per month) was reported by 10.6% (n = 76) and daily use was reported by 0.7% (n = 5).
Among 227 migraine participants, 215 (94.7%) had used acute medication. Ibuprofen was the most common (80.5%; n = 173), followed by acetaminophen (36.7%; n = 79), triptans (32.6%; n = 70) and metamizole (32.6%; n = 70). Aspirin (19.1%; n = 41) and Thomapyrin (10.7%; n = 23) were also used. Opioids such as tilidine (3.3%; n = 7) and tramadol (1.4%; n = 3) were rarely used.
Of 839 participants, 130 (15.5%) had used preventive medication. Among 100 participants with chronic headaches, only 24 (24%) had used preventive therapy. Among 201 participants previously diagnosed with migraine, 35.8% (n = 72) had used prophylactic medication. Among 227 participants meeting the diagnostic criteria, 27.3% (n = 62) had also done so. Of the 139 participants reporting four or more migraine days/month, 33.8% (n = 47) had used prevention. Of the 94 participants with severe disability according to their MIDASs, 38.3% (n = 36) had used preventive medication.
Suggestions for improving care
The final open-ended question on improving headache care in the German Armed Forces was answered by 284 participants (33.8%). In total, 415 suggestions were collected and categorized (Table 4). The most common issue (20.2%; n = 57) was a call for military physicians and medical staff to take headache disorders more seriously. Another 13.8% (n = 39) requested more thorough evaluation and diagnostics. Additional concerns included reducing bureaucracy with respect to medication prescriptions, sick leave and referrals to specialists. Approximately 10% of responses (each) emphasized access to physical training and wellness programs, workplace adjustments (e.g. tele day, reduced workload, reduced screen time) and better information and education, respectively. Other responses called for improved medical training (8.9%), greater awareness among superior officers (6.7%), and improved access to both acute and preventive therapies (6.0%).
Suggestions for improving the care of service members with headache disorders in the German armed forces (Bundeswehr).

Discussion
To our knowledge, this is the first systematic study to examine the occurrence of primary headache disorders, diagnostic awareness, treatment approaches and the impact of headaches on military service among active-duty personnel in the German armed forces. Headaches are among the most common neurological conditions worldwide, affecting particularly young adults, who comprise the core age group of active military personnel. This study was not designed to assess prevalence based on a representative sample; instead, the aim was to use a large sample in a cross-sectional analysis to examine headache phenotypes, prior diagnoses, treatment and potential service-related impairments among affected individuals.
The use of an anonymous online questionnaire was chosen to maximize accessibility, ensure participant anonymity and increase response rates across geographically dispersed units of the Bundeswehr. Given the sensitive nature of health-related disclosures, particularly in a military setting where concerns about stigma or career impact may inhibit reporting, an online, self-administered format likely encouraged more honest and complete responses compared to in-person interviews. Additionally, this method allowed for efficient large-scale data collection within a limited time frame and resource constraints. Further psychometric evaluation, including assessments of internal consistency, construct validity and test-retest reliability, was not part of the current study design but is planned for future research to strengthen the instrument's methodological rigor.
The specific headache types analyzed were migraine (27.1%), TTH (26.5%) and cluster headache (4.1%). Migraine and probable migraine accounted for 56.4% of all reported headaches. In 61% of cases, no prior diagnosis had been made. Only 38.6% had received any form of medical care. The disability related to headaches was substantial: migraine patients reported an average of 3.9 lost workdays per month. Nevertheless, only 27.3% had ever used preventive medication.
In the present study, a high proportion of participants with headache symptoms were classified as having probable migraine. With 246 cases, this accounted for more than half of the migraine-like headache cases (246 out of 473), corresponding to approximately 52%. This finding is consistent with results from population-based surveys such as the Eurolight study (24) and the Global Burden of Disease Initiative (3,13), which have similarly reported that 30–50% of individuals with migraine symptoms do not fully meet the diagnostic criteria of the ICHD-3 (10) and are therefore classified as having probable migraine.
Especially in non-clinical cohorts such as military populations, where standardized medical diagnoses are rarely available and history-taking is often retrospective, a higher proportion of probable migraine is to be expected. This may result from incomplete recall of symptom features (e.g. attack duration, accompanying symptoms) or from limitations in documentation. Nonetheless, studies have shown that the disease burden of probable migraine is often comparable to that of diagnosed migraine, particularly with regard to functional impairment, medication use, and inability to perform duty (25,26).
Another notable finding is the nearly equal distribution of migraine among male and female participants in the sample (110 males vs. 116 females). This contrasts markedly with civilian population-based data, where the gender ratio for migraine typically approximates 3:1 (female:male). In military cohorts, however, a higher proportion of affected males has repeatedly been described, possibly due to selection and exposure factors. Potential causes include occupation-specific stressors, physical and psychological strain, and possibly lower willingness to seek medical care, leading to underdiagnosis and a higher proportion of cases falling under the category of probable migraine (16,17,27,28). Overall, the data suggest that probable migraine represents a relevant and frequent headache phenotype in the military context, which should be specifically addressed in both diagnostic and therapeutic strategies. The observed gender distribution further suggests possible differences in access to diagnosis or in symptom perception, which warrant further investigation.
The rate of previously established medical diagnoses was particularly low in migraine: nearly half (48%) of those meeting all of the diagnostic criteria had never been diagnosed. Similar findings have been reported in other military populations, including the US and UK armed forces, where high rates of undiagnosed migraine and significant operational limitations have also been observed (17,29).
While we reported an average of 3.9 workdays lost due to headache among affected individuals, this number should be interpreted in light of the distributional data presented in the Results. Most respondents reported only 1–5 lost days, whereas a small subgroup accounted for disproportionately high values, including continuous work disability. This skewed distribution underscores the heterogeneity of headache-related functional impairment in the sample.
Despite the high disease burden, only 27.3% of those affected by migraine had ever received prophylactic medication. Among those with chronic migraine (≥15 headache days per month), this number shrank to beneath 25%. This appears low, considering that a significant proportion of individuals met eligibility criteria based on headache frequency and disability scores (HIT-6 and MIDAS). According to German and international guidelines, preventive therapy is recommended for patients experiencing ≥4 migraine days per month and/or substantial impairment in quality of life or daily functioning (30–35). The discrepancy between treatment need and actual prescription highlights a potential gap in care, particularly in settings where access to specialized headache care may be limited. This underlines the importance of improving identification and management of candidates for preventive treatment among military personnel. This treatment gap points to deficiencies in guideline-based care and highlights the need for better training of medical personnel, as well as improved education for those affected.
The impact on military service is substantial. MIDASs showed that over one-third of respondents experienced moderate-to-severe disability, with a particularly high burden among female service members. These functional limitations have implications for operational readiness, long-term health and duty assignment.
Free-text responses highlighted structural and organizational shortcomings, including a lack of recognition of the disease burden by medical personnel, limited access to appropriate diagnostics and treatment, and bureaucratic obstacles. The frequent use of over-the-counter analgesics (particularly ibuprofen and acetaminophen) rather than migraine-specific agents such as triptans indicates suboptimal pharmacologic strategies.
Our findings indicate that primary headache disorders are prevalent across all service branches in the German Bundeswehr and are associated with significant undertreatment. The resulting impact on duty performance and operational readiness is considerable. The data underscore the necessity of adopting a systematic approach to headache care within the German armed forces.
Similar results have been reported in studies from other countries. Earlier analyses of headaches in military personnel have mainly focused on post-traumatic headache following traumatic brain injury (TBI). A systematic review analyzed the phenotype of post-traumatic headache following mild TBI in military personnel (36). Based on eight studies, migraine-like headaches emerged as the most frequent subtype with a prevalence of 33–92%.
In a retrospective study of soldiers with mild TBI, migraine was the most common headache diagnosis (in 60% of cases) after concussion (37). However, it was not the migraine diagnosis itself, but rather the headache characteristics (and, in particular, continuous pain) that were most predictive of adverse occupational outcomes, including discharge from service. Soldiers with persistent headaches were much less likely to remain in active duty, regardless of whether their headaches were diagnosed as migraine, trigeminal autonomic cephalalgias or other forms. The study in question emphasized that in military contexts, the duration and severity of post-traumatic migraine symptoms are more critical to service fitness than the specific diagnosis.
A retrospective study examined the course and impact of migraine among 159 US Air Force pilots and 44 flight surgeons with aeromedical certification (38). The most common forms of migraine were migraine with aura and isolated aura without headache. In total, 62% identified personal triggers, primarily sleep disturbances, stress, diet, caffeine and hormonal factors, especially in women, and 91% of affected individuals remained flight-qualified over time. These findings support the need for nuanced treatment strategies to ensure flight safety and preserve operational capacity.
A military referral center study found that depression in patients with headache and migraine was more strongly associated with a loss of productivity and duty impairment than headache severity itself (39). The study in question revealed a significant gap in recognizing and treating comorbid depression in headache patients, underlining its economic and functional relevance.
A retrospective analysis of medical disqualifications in US Army helicopter pilots found that migraine was among the most frequent causes of permanent flight disqualification, second only to depression and ahead of PTSD (40). Although many diagnoses allowed for conditional waivers, such as for spinal or neurologic disorders, migraine carried a higher risk of permanent disqualification. This underscores migraine's unique relevance to flight medical assessment and its potential career consequences. In the case of military pilots, functional impairment due to migraine must be considered in light of aviation medicine regulations. Even infrequent migraine attacks, particularly those with aura, can result in temporary or permanent flight disqualification, regardless of overall work capacity. This mechanism of restriction differs fundamentally from that affecting ground-based personnel, where limitations are more often tied to headache frequency and functional disability. International aeromedical guidelines recognize the risks associated with sudden neurological symptoms in aircrew and typically classify migraine with aura as disqualifying unless proven to be reliably controlled and non-impairing (41).
A Canadian study on the mental and physical health of active-duty soldiers found that migraine, along with other chronic pain conditions, was common and strongly associated with psychiatric disorders such as PTSD, depression and anxiety (42). These findings demonstrate that migraine must, in the military context, be viewed not as an isolated condition but as one closely intertwined with psychological burden and service fitness.
A large-scale study of more than 1.2 million Israeli military conscripts (1998–2013) found a significant association between anxiety disorders and migraine, as well as other somatic disorders with similar symptoms (e.g. irritable bowel syndrome, asthma) (43). Migraine was more frequent in individuals with diagnosed anxiety disorders. The findings emphasize that migraine in the military should not be viewed in isolation because it is closely linked with psychological stress. This is especially relevant for frontline diagnostic efforts by military physicians, aiding in avoiding misdiagnoses and in addressing both mental and physical causes appropriately.
A two-year analysis of 1368 admissions to the British field hospital Camp Bastion (Afghanistan) identified migraine as one of the ten most common diagnoses, accounting for 1.8% of all cases (44). It ranked higher than cardiovascular conditions such as myocardial infarction and thrombosis. Although average stays were short (mean 1.6 days), this study highlights that migraine is a relevant condition even in operational settings, underlining the importance of headache diagnostics and care, even in deployment zones, for both mission readiness and service member quality of life.
Another study examined the link between combat deployment and migraine onset among US soldiers using data from the National Longitudinal Study of Adolescent Health (19). Soldiers deployed to combat zones with enemy contact had a significantly higher risk of developing migraine than those deployed to peaceful areas. About 40–45% of the association between combat exposure and migraine could be explained by deployment-related sleep disturbance, psychological stress, and physical injury. These findings indicate that migraine in military settings is heavily influenced by operational stress and underscore the need for preventive and psychological support interventions for combat-exposed soldiers.
A study of 154,548 US servicewomen deployed one to three times to Iraq or Afghanistan found that migraine was among the most commonly diagnosed conditions post-deployment, especially in those with multiple deployments (27). Migraine prevalence increased modestly with the number of deployments, similar to PTSD and musculoskeletal disorders. The strongest predictor for post-deployment migraine was a pre-deployment migraine diagnosis. Longer deployments increased the risk, whereas longer dwell times between deployments did not clearly reduce it. These findings suggest that shorter deployments (e.g. <9 months) may reduce the long-term migraine and health burden in servicewomen.
Another study found that 20% of US soldiers with deployment-related concussion experienced chronic daily headache (CDH), a rate that is four to five times higher than in the general population (45). Two-thirds of CDH cases met the criteria for chronic migraine, often starting within one week of trauma. CDH was not linked to the number of concussions or cognitive deficits but was strongly associated with PTSD symptoms; 41% of CDH patients screened positive for PTSD. These findings suggest that psychological trauma plays a key role in migraine chronification following TBI in military contexts. These findings are consistent with the concept of post-traumatic headache as defined in the ICHD-3, particularly in the context of persistent headache following mild TBI. The described constellation underscores the complex interaction between physical and psychological trauma in the chronification of headache disorders among military personnel.
A long-term analysis showed that, between 1998 and 2010, both the incidence and prevalence of migraine and other headache syndromes increased steadily among active-duty US soldiers (29). Outpatient consultations related to headaches also rose markedly. Gender differences were striking; in 2010, 3.9% of male soldiers and 11.3% of female soldiers sought outpatient care for headaches. Women were also more likely to receive intensive treatment; among those diagnosed with migraine, 6% of women and 3% of men had more than ten outpatient visits. For other headache types, this rate was below 1%. These data highlight the growing importance of migraine in military medicine, particularly among women, and the associated need for expanded care. Migraine is not only prevalent, but also a resource-intensive condition within the armed forces.
A prospective study investigated 985 soldiers evacuated from Iraq and Afghanistan between 2004 and 2009 due to headaches (46). Migraine was the second most frequent diagnosis (30%), following post-concussive headache (34.1%). The overall return-to-duty (RTD) rate was only 33.6%. RTD rates were particularly low for TBI-related headache subtypes such as post-concussive headache, cervicogenic headache and occipital neuralgia. By contrast, soldiers with tension-type headache had the highest RTD rate at nearly 50%. Key negative predictors for RTD included aura, TBI, opioid or beta-blocker use, and psychiatric comorbidities, often seen in migraine patients. These findings illustrate that migraine is a major cause of mission loss and requires targeted diagnostics and individualized therapy in operational settings.
A large population-based study from the Millennium Cohort Study analyzed over 77,000 US soldiers and reservists regarding the onset of migraine and other headache disorders in relation to foreign deployment and combat experience (18). At baseline, 6.9% of men and 20.9% of women reported a physician-diagnosed migraine. Other severe or distressing headache types were also more common in women. Combat deployment significantly increased the risk of new-onset headaches, including migraine, for both sexes (men: odds ratio = 1.72; women: odds ratio = 1.84). In contrast, non-combat overseas deployments did not elevate risk. These findings reinforce the link between migraine, combat-related stress and psychological burden. Early detection, prevention and targeted intervention are essential, particularly for combat-exposed personnel.
Another large study examined migraine frequency and impact among US soldiers following a one-year combat deployment during Operation Iraqi Freedom (17). Within 10 days of return, 19% met the criteria for migraine and 17% for probable migraine. Migraine patients reported an average of 3.1 headache days per month, a mean attack duration of 5.2 hours, and 2.4 duty-impairing headache days per month. Over three months, they made 490 headache-related medical visits, which is far more than those with probable migraine (90 visits). Three months post-deployment, average headache days rose to 5.3 per month and 36% had high migraine-related disability (MIDAS grade 3 or 4). Despite the burden, only 4% used triptans, while 75% relied on OTC medications. The data reveal that migraine is common, impactful and undertreated among returning troops, and it often persists post-deployment, underscoring substantial care and intervention needs.
A study of US Army officer candidates (n = 741 of 1389 invited) found that 18% met the criteria for definite migraine: 14% of men and 31% of women (16). However, only 10% had been previously diagnosed and only 3% had received triptan treatment. During the five-week training program, male participants averaged 0.7 migraine attacks per month and females averaged 1.4. Eight percent reported impaired training performance due to migraine, resulting in 63 missed or limited training days. Risk factors for reduced performance included a pre-existing diagnosis, positive screening and higher pre-training frequency. The findings underscore the need for better diagnosis and treatment of migraine in military training.
A retrospective study of permanent medical disqualifications in US Air Force pilots and navigators (1995–1999) found migraine to be among the top neurological causes, alongside coronary artery disease, hypertension, back pain, disc disorders, diabetes and substance or alcohol misuse (47). These results emphasize migraine's relevance for flight safety assessments.
Limitations
The present study has several limitations. Participation was voluntary, which may have introduced a selection bias toward more symptomatic individuals. In addition, the sample is not representative of the entire Bundeswehr, limiting generalizability. Patients with cluster headache experience a particularly high level of suffering, which may have led to a disproportionately high motivation to participate. This could further contribute to the observed overrepresentation of cluster headache cases. As the sample is not representative, no valid conclusions can be drawn regarding prevalence. A substantial proportion of respondents were medical personnel, which reflects a potential access or selection bias. These individuals may have greater health literacy, better access to medical information and a higher likelihood of self-management or self-diagnosis. As such, their participation may not reflect the general burden or treatment behavior among the broader military population. The prevalence of medication overuse headache may be underestimated in this study because diagnosis was based on self-reported intake frequency and not confirmed by clinical evaluation. Underreporting, misclassification, or lack of awareness among participants could have contributed to underestimation of the true medication overuse headache burden. Headache classification was based on self-reported symptomatology using a questionnaire rather than clinical evaluation by a physician, which may affect diagnostic accuracy. While the questionnaire was reviewed by clinical experts to ensure content validity, further psychometric validation, such as construct validity, internal consistency (e.g. Cronbach's alpha) and test–retest reliability, was not performed and should be addressed in future research.
Despite these limitations, the study has notable strengths, including a large sample size, demographic diversity, and the use of established and widely accepted instruments (ICHD-3 criteria, MIDAS score). The findings provide important initial insights into the burden of headache disorders in the Bundeswehr and offer a foundation for further targeted research and healthcare improvements in military populations.
Conclusions
Primary headaches, and especially migraine, are widespread in military service, significantly underdiagnosed and undertreated. The resulting disability substantially impairs duty performance and operational readiness. The findings highlight an urgent need for the following measures:
Enhanced training and awareness among medical personnel. Integration of standardized headache screening tools. Systematic diagnosis based on international standards (ICHD-3). Guideline-compliant pharmacologic therapy including prophylaxis. Development of nationally standardized treatment pathways. Structured care models within the Bundeswehr.
Targeted improvements in diagnosis, treatment and prevention can reduce functional losses and help maintain long-term operational capability. Headache disorders should be recognized as a relevant military health issue and be integrated accordingly into care planning. These steps are essential to ensuring appropriate and effective care for service members suffering from headaches, with the goal of maintaining operational readiness and sustainably improving their quality of life.
Key findings
In a large cross-sectional survey of 914 German active-duty military personnel, 56.4% met diagnostic criteria for migraine or probable migraine.
Despite significant disability (mean 3.9 lost workdays per month in migraine), only 27.3% had ever received preventive treatment.
61% of all participants had never received a formal headache diagnosis, despite fulfilling ICHD-3 criteria.
Headache-related impairment affected over 60% of respondents, with clear negative implications for operational readiness.
Military healthcare structures currently lack systematic headache screening, diagnosis, and evidence-based treatment pathways.
Footnotes
Acknowledgements
We thank the participants of the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Author contributions
CHG and UM contributed to the design and conceptualization of the study, performed the statistical analysis, interpreted the results and wrote the first draft of the manuscript. AH, KHK, HW and AC contributed to the interpretation and analysis of the data. HG contributed to the design and conceptualization of the study, was involved in co-writing the manuscript and supervised the project. All authors reviewed and approved the final version of the manuscript submitted for publication.
Ethical statement
This project was approved as a special military medical research initiative by the Medical Service Command of the German armed forces (Project ID: 48K3-S-33 2323). The study protocol was reviewed and approved by the Ethics Committee of Kiel University (Reference: D 453/23). Participation was voluntary. This study adhered to the principles of the Declaration of Helsinki (1964) and its subsequent revisions.