
Abstract
Objective
To estimate the prevalence, burden and current treatment of disabling primary headaches in a large sample of the Greek population aged 18–70 years old.
Methods
This is an observational descriptive study, with cross-sectional design performed by quantitative computer-assisted telephone interviews, using a validated 37-item questionnaire for headaches. The prevalence, burden, and current treatment of primary headaches (ICHD-3) were recorded along with participants’ treatment preferences.
Results
Out of 10,008 interviewed participants, 1197 (12.0%) reported headaches affecting performance. The annual prevalence of migraine was 8.1% (95% confidence interval, 7.6–8.7, corresponding to 0.6 million Greeks), of chronic migraine 1.0% (95% confidence interval, 0.8–1.2, corresponding to 0.1 million), and of tension-type headache 3.8% (95% confidence interval, 3.4–4.2, corresponding to 0.3 million). The participants with headaches reported 0.5 headache-induced lost workdays per month (corresponding to 5.8 million lost workdays annually) and reductions in performance on 2.8 workdays per month (corresponding to 30.9 million workdays annually). In all, 43.4% of headache participants felt bad/ashamed because of headaches and 21.9% sought professional treatment, most often from a private neurologist. 83.8% of headache participants had never taken pharmacological prophylaxis, and only 5.5% were currently under preventative treatment. For both prophylactic and acute treatment, headache participants prefer oral medication to injection or stimulation devices.
Conclusion
More than 10% of the Greek adult population up to 70 years old experience disabling headaches, causing a dramatic work loss. More than 80% of these have never taken pharmacological prophylaxis. Thus, enriching the quality of life of people with headaches relies crucially on expanding awareness about headaches and their treatment.
Introduction
There is neither a recent epidemiological study about headaches in Greece, nor a large scale one. Two decades ago, a research group used structured face-to-face interviews to study headache prevalence in three different groups: A sample of 3501 inhabitants representing the Greek population aged 15 to 75 years old (1), 588 medical students of the National and Kapodistrian University of Athens (2) and 449 monks of Mt. Athos (3), applying the 1988 International Headache Society diagnostic criteria (4). In the late 1990s, another epidemiological study interviewed 4000 children, aged 4–15 years, to estimate the migraine prevalence in schoolchildren (5). Since then, no other study has been conducted in either the adult population or any particular Greek subpopulation. Nevertheless, the diagnostic criteria for headache disorders have changed twice (6,7), while new treatments with biological agents and neurostimulation devices are under investigation or already in use against migraine and cluster headache (8,9). In this context, it would be particularly interesting to investigate the impact of the headaches of the patients on their daily lives, their willingness for therapeutic interventions and their treatment preferences.
The present study aimed to investigate the prevalence and burden of selected disabling primary headache disorders, as well as the treatment preferences of people suffering from headache in a large sample of the Greek adult population.
Methods
This is an observational descriptive survey, in the form of computer-assisted telephone interviews (CATI), with cross-sectional design. Overall, we planned to conduct a target number around 10,000 interviews, corresponding to 1.4‰ of the Greek population, on a representative sample of the Greek population in terms of gender, age, and area, based on the most recent census (10). We did not perform a formal sample size calculation. Specifically, participants should be males and females aged between 18 and 70 years old, and a representative sample of the 7.4 million inhabitants within this age range. The sampling process was based on random pickup of a phone number from a large database of 97,083 phone numbers (Figure 1). These were representative of the population of Greece (from all 13 regions) in terms of gender, age, and area, based on the most recent census (10). Specifically, we used stratified random sampling: We created subgroups (quotas) based on gender, age range, and region, and set a specific target of complete interviews by a trained interviewer for each subgroup, so that the volume of each stratum in the target sample of 10,000 would be proportional to the corresponding subgroup in the population of Greece. Thus, randomisation was ensured (Supplemental Tables e-1 and e-2), and post-stratification was not applied. The sampling process was random (respondents were asked to provide their gender, age, and region during the survey). As the survey progressed and quotas were gradually filled, we kept looking for respondents matching only the still-incomplete quotas. However, within each subgroup, sampling was random. For instance, if hypothetically at some point the target number was reached for females but not for males, fieldwork continued; if a woman answered, the interview stopped when she informed the interviewer about her gender. In such cases, the interviewer asked if anyone else was in the house, who could possibly take part in the survey (without specifying gender/age requirements).
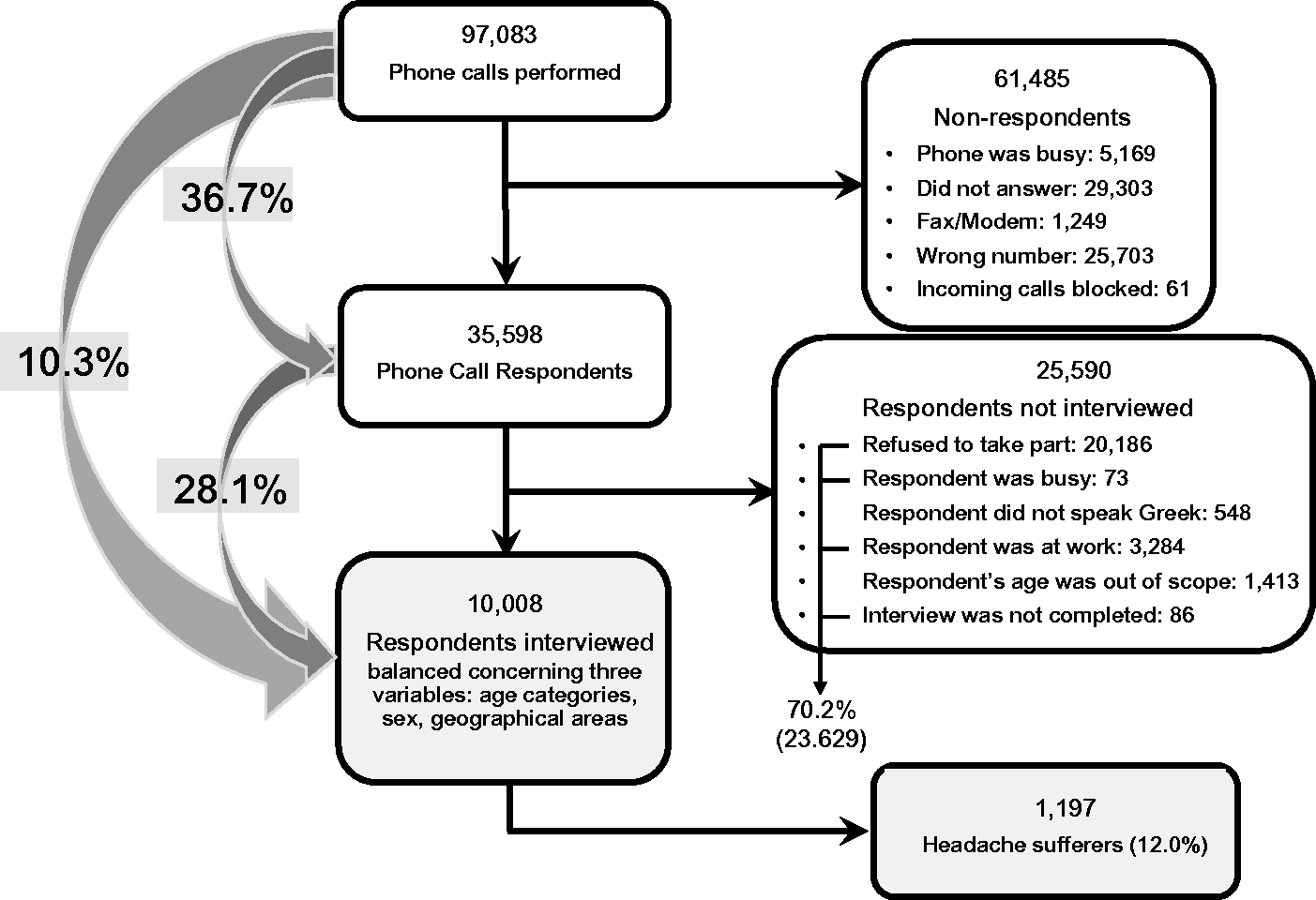
Study flowchart. During the random sampling process the respondents were asked to provide their gender, age, and region. While the survey was progressing, and quotas were gradually filled, we kept looking for respondents matching only the still incomplete quotas.
We prepared a 37-item questionnaire for the survey (Supplemental Table e-4). Apart from the diagnostic and demographic questions, the questionnaire included questions for headache burden, current headache treatments, headache health services and treatment preferences. The screening question was “Do you suffer from headaches that affect your performance and which occurred at least once in the year prior to this survey?”. We developed an automatic algorithm for the diagnosis of migraine, tension-type headache (TTH) and cluster headache (CH) according to the ICHD-3 beta diagnostic criteria (11). The interviewers were neither trained for diagnosing other primary headaches nor for coexistent headache disorders. To assess the sensitivity and specificity of the instrument (questionnaire and diagnostic algorithm), we delivered 150 questionnaires to outpatients diagnosed with primary headaches in pre-study work at the authors’ workplaces. Subsequently, we compared the diagnoses based on these questionnaires to the clinical diagnosis (expert’s opinion following the ICHD-3 beta). In total, we collected 145 questionnaires. Cross tabulating these data, we estimated the sensitivity and specificity of the questionnaire for migraine/probable migraine, TTH/probable TTH and cluster headache/probable cluster headache. We stratified the participants into four social classes based on their occupation and education (class 1, higher education and white-collar occupation; class 4, lower or no education and unskilled or low skilled work) following the Hellenic Statistical Authority. (ELSTAT) recommendations (10). We did not include income in the demographics because of missing data. Missing workdays, as well as workdays with reduced performance and missing family or social obligations, all due to headaches, were reported as average days per month in the preceding 3 months. In addition to the ICHD-3 migraine subtypes, we have subclassified episodic migraine into high (≥8 days and less than 15 days/month) and low frequency (less than 8 days/month) for reasons related to possible indications of reimbursement for the new anti-migraine treatments by the Greek regulators.
The study was carried out by Ipsos Opinion S.A. on behalf of the Hellenic Headache Society, between 22 May 2017 and 27 June 2017.
Standard protocol approvals
The Hellenic Data Protection Authority approved the study protocol and questionnaire used (No 1363/2017), according to the General Data Protection Regulation (GDPR) (EU) 2016. No additional approval from an ethics committee was considered necessary. A verbal informed consent was obtained from every interviewee.
Statistics
We used a binary multiple logistic regression model (MLogR) with stepwise selection. The headache type was the outcome variable while the demographic variables (gender, age group, social class, geographical areas) were the predictors. We used another binary MLogR to evaluate the demographic variables as predictors for pharmacological prophylaxis intake (yes–no). In addition, we used a multinomial MLogR to assess demographics as a predictor for the participant with headache preferences for prophylactic treatment. We performed one-way ANOVA to examine the differentiation of each of the dependent continuous variables (headache frequency, workdays lost per month and days with reduced performance per month) among headache types, followed by Scheffe’s test for post-hoc comparisons. Subsequently, we applied multiple linear regression (MLinR) with stepwise selection for each of the same dependent variables, designating the demographic data of the participants with headache and the use of pharmacological prophylaxis (yes–no) as independent variables. We also used the χ2 test to compare the prevalence of the headache types to each demographic variable, but also to compare the rate of participants with headache under pharmacological prophylaxis and the rates of their treatment preferences to each of the headache types. Missing data were sparse and random and therefore pairwise deletion was applied for basic statistics (descriptive, simple regression, correlation, non-parametric), while listwise deletion was applied for logistic or multivariate regression. Regarding the cases of multiple comparisons, Scheffe’s test was used whenever an ANOVA statistic was performed. Since the vast majority of comparisons of the rest of statistical procedures resulted in p-values either greater than 0.5 or less than or equal to 0.02 (and in many cases less than 0.001) we did not proceed to further corrections for multiple comparisons. Finally, for multicollinearity, the variance inflation factor (VIF) was applied using values > 5 as a cut-off point for variable removal from the model. When the variables were nominal, dummy variables were constructed and the VIF rule was applied again. The statistical analysis was carried out with IBM SPSS Statistics for Windows v24.0 (IBM Corp., Armonk, NY, USA).
Results
From 97,083 phone calls, 35,598 people responded and from these responders, 23,629 did not participate (excluding those outside the age range and those not speaking Greek), representing 70.2% of respondents. A full interview was obtained by 10,008 participants (Figure 1).
The sensitivity and specificity of the questionnaire for migraine/probable migraine, TTH/probable TTH and cluster headache/probable cluster headache were calculated to be 90.1% and 60.0%, 94.3% and 42.9%, 92.4 and 74.6% respectively; positive predictive values were 91.9%, 42.9% and 89.8%, respectively.
The total number of participants who reported having headaches affecting the performance of their daily activities in the past year was 1197/10,008 (12.0%; 95% CI: 11.3–12.6%) (Table 1) corresponding to 0.9 million individuals (95% CI 0.8–0.9) out of 7.4 million individuals of the total national population aged 18–70. 8.1% (95% CI: 7.6–8.7) of the respondents fulfilled the criteria for migraine/probable migraine (corresponding to 0.6 million people), 1.0% (95% CI: 0.8–1.2) for CM/probable CM (0.1 million), 3.8% (95% CI: 3.4–4.2) for TTH/probable TTH (corresponding to 0.3 million), and 0.04% (95% CI: 0.0–0.1) for cluster headache/probable CH (corresponding to 3000 patients) (Figure 2, Tables 1 and 2). In all, 84.3% of them reported at least one headache attack per month (mean 1.4, 95% CI: 0.8–2.1) (Table 3 and Supplemental Table e-3).
Demographics of headache patients.

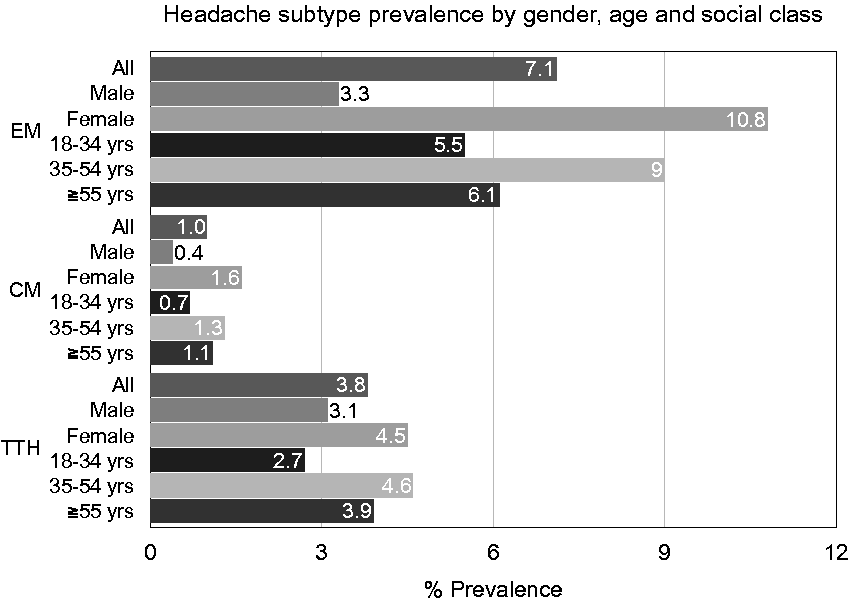
The one-year prevalence of disabling headaches by headache type, age, and gender.
One-year prevalence of primary headache subtypes in a representative sample of 10,008 Greek inhabitants aged 17–70 years.

Note: High frequency episodic migraine ≥8 days with headache/month; low frequency episodic migraine < 8 days with headache/month.
Headache attack frequency by headache subtype.
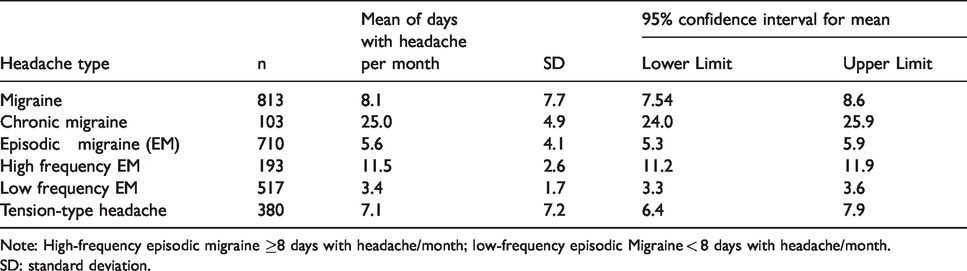
Note: High-frequency episodic migraine ≥8 days with headache/month; low-frequency episodic Migraine < 8 days with headache/month.
SD: standard deviation.
Headache characteristics
The average duration of a headache was 14.1 ± 15.3 h without using painkillers. TTH had a shorter average duration than migraine (10.4 vs. 16.0 h, respectively, p < 0.001). The average lifetime duration of headaches in participants with headache was 11.8 ± 10.3 years (12.8 and 9.7 for migraine and TTH participants, respectively, p < 0.001). The majority of them (84.2%) reported at least one headache attack per month (mean 1.4, 95% CI: 0.8–2.1) (Table 3 and Supplemental Table e-2), while the migraineurs typically experienced eight headache days per month (mean: 8.1, 95% CI: 7.5–8.6). The mean patient-reported headache intensity was 7.2 ± 1.5 on an 11-point scale from 0 (not at all intense) to 10 (extremely intense). Specifically, extremely intense headaches (a 9 or 10 on the scale) were reported by 10.0% of the sample. They were more common in migraine (12.6%) than TTH patients (4.7%). In all, 53.2% of the participants with headache had first-degree relatives with a history of headaches (migraine 59.3% vs. 40.5% TTH).
Headache burden
Missing workdays due to headaches were reported by 16.4% of the headache participants overall, 19.7% for migraine and 9.5% for TTH, averaging 0.5 missed workdays per month (0.7 for migraine and 0.3 for TTH) corresponding to 5.8 million lost workdays annually in the total population of headache participants. In all, 53.2% of headache participants reported reduced work performance caused by headaches. This occurred on 2.8 days per month on average (3.2 and 2.0 days for migraine and TTH, respectively), corresponding to 30.9 million workdays with reduced performance annually (Figures 3–5). Most headache participants (56.2% overall, 64.3% for migraine and 39.0% for TTH) reported that headaches prevented them from responding to their social or family obligations at least 1 day per month, while missing such obligations was documented for 2.5 days per month on average (3.0 and 1.4 for migraine and TTH, respectively). The mean number of days with reduced performance was notably differentiated between CM, EM and TTH (p < 0.001). Scheffe’s post-hoc comparison test showed that the number of days with reduced performance was higher in CM than in EM (p < 0.001) and TTH participants (p < 0.001), but it was not different between TTH and EM (p > 0.05). In all, 43.4% of respondents with headache (47.5% for migraine and 34.7% for TTH) had experienced shame or other reported negative feelings due to headaches.

Working days lost (absenteeism) due to headache.

Working days with reduced productivity (presenteeism).
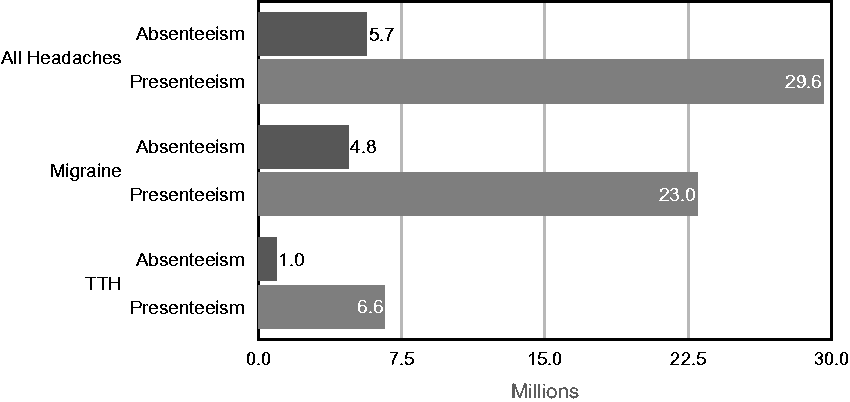
Estimated millions of annual workdays lost or with reduced activity due to headache in Greece.
Headache treatment
Approximately one-fifth of headache participants (21.9%) reported they were willing to seek professional treatment. In all, 71.0% of them visited clinicians working in private practice instead of a hospital (29.0%). A total of 83.8% reported not having used any prophylactic treatments so far. In all, 5.5% of participants with headache mentioned current usage (n = 66/1197) (Table 4). The proportion of participants with headache taking prophylactic treatment was higher in CM than EM participants. A total of 88.1% of the headache participants reported that they were taking a symptomatic treatment of at least one dose weekly (90.7% and 82.6% for migraine and TTH, respectively). They reported an average of 3.7 pills on a weekly basis (4.1 for migraine and 2.9 for TTH) including painkillers (82.8%), non-steroidal anti-inflammatory drugs (NSAIDs, 18.8%) and other oral medications, (e.g. triptans, 5.2%). A total of 11.5% of headache participants (13.3% for migraineurs and 7.6% for TTH sufferers) had tried alternative headache treatments, including six who had tried acupuncture (6.0%), and homeopathy (5.2%). Interestingly, 61.6% of the sample had participated in a spiritual type of ritual to remove the evil eye, while the percentage of those attributing some of their headache attacks to the evil eye was smaller (40.1%).
Rate (%) of Prophylactic treatment intake for each Headache type.
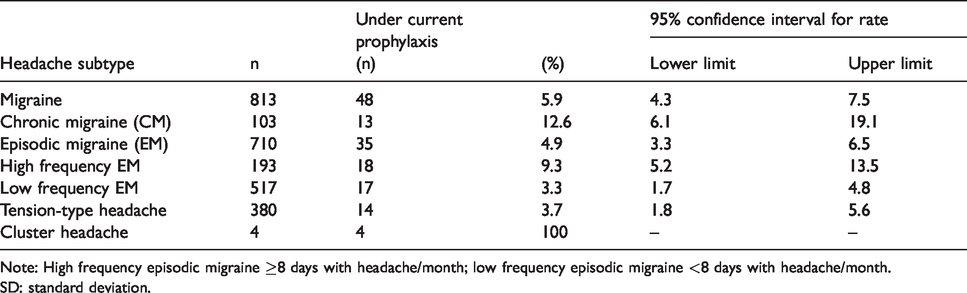
Note: High frequency episodic migraine ≥8 days with headache/month; low frequency episodic migraine <8 days with headache/month.
SD: standard deviation.
Treatment preferences
A total of 61.2% of headache participants prioritised safety over effectiveness regarding prophylactic treatment. This preference was related to previous usage of prophylactic treatment (62.2% of migraineurs who never used prophylactic treatment prioritised safety, in contrast to 47.9% of migraineurs who were familiar with prophylactic treatment, p < 0.05). In all, 52.1% of migraineurs in this last group prioritised effectiveness, p < 0.05). The overall quitting prophylactic medication due to adverse effects was 8.0% (9.2% for migraine and 5.5% for TTH). Headache participants preferred oral to parenteral medication (e.g. injection), especially for acute treatment (85.9% for oral medication vs. 8.0% for injection, p < 0.001). For prophylactic treatment, 50.8% opted for everyday oral medication, as opposed to 18.5% (p < 0.001) for monthly injection, whereas 2.0% selected both. Migraineurs displayed an increased numerical preference for prophylaxis with monthly injection (21.7%) as opposed to TTH participants (11.8%), but this difference was not significant (p > 0.05). Comparing traditional headache treatments (oral medication and injection) to a stimulation device revealed that headache participants tended to favour the former over the latter for both prophylactic treatment (69.1% for traditional methods vs. 14.3% for stimulation device, p < 0.001) and acute treatment (76.7% and 13.3% for traditional methods and stimulation device, respectively, p < 0.001). Notably, the participants with headache reported that they would be willing to spend on average €21.0 ± 8.8 per month, out of their own pockets for headache treatment.
Gender effects
Both migraine and TTH participants were more likely to be female (77.0% and 59.5% respectively). The prevalence of CM was approximately four times higher among females (OR 3.9, p < 0.001) and similarly, the prevalence of EM, three times higher (odds ratio (OR) 3.6, p < 0.001). MLinR did not reveal any other significant difference. Gender effects on treatment preferences were detected. Male participants with headache favoured a stimulation device slightly more than females (17.6% vs. 13.0%, p > 0.05) in prophylactic treatments. In acute headache treatment, the latter seemed to prefer traditional medications (injectables or orally administered) slightly more than males (78.4% vs. 72.4%, p > 0.05). Males displayed willingness to spend more money than females for headache treatment (€25.8 ± 60.1 vs. €19.1 ± 28.9 per month on average, p > 0.05).
Age effects
The prevalence of both EM and TTH was significantly higher in the 35–54 age group (OR 1.6 and 1.7, p < 0.001), but the mean headache frequency in TTH participants was lower in this age group than in others (p < 0.01). The proportion of headache participants who had taken prophylactic treatment for EM increased with age (p < 0.02). MLinR did not reveal any other significant difference. The youngest age group (18–34) reported experiencing extremely intense headaches (10/10) less often than the remaining age groups (4.1% for ages 18–34 vs. 12.4% and 11.3% for ages 35–54 [p < 0.01] and 55–70 [p < 0.01] respectively). Older headache participants (55–70 years old) appeared unwilling to spend any money for headache treatment. Experiencing reduced work performance due to headaches at least once a month was numerically more common among adults under 55 (58.0%) than those 55 or older (38.2%) (p > 0.05). The 55–70 age group was slightly more likely to seek professional treatment (27.6%) than younger participants with headaches (p > 0.05). A total of 1.7% of individuals with headaches aged 18–34 had taken prophylactic treatment, as opposed to 5.6% and 7.8% for ages 35–54 and 55–70, respectively (p < 0.02). Older headache participants reported a higher weekly average of days taking oral pain-relief medication (2.8 days) compared to those aged 18–34 (2.4 days) or 35–54 (2.5 days) (p > 0.05 for each of the comparisons).
Social class effects
Lower social class participants with headaches suffering from TTH had higher mean headache frequency than the rest (mean headache days per month: 9.3, 95% CI: 7.3–11.3, p < 0.02). Among participants with EM, the lowest social class group showed a higher number of workdays lost (mean: 0.9, 95% CI: 0.5–1.3, p < 0.002) or reduced performance (mean: 3.8, 95% CI: 2.6–5.0, p < 0.02) than the other groups. We did not detect any other notable effect of social class on headache frequency, characteristics and treatment preferences.
Discussion
This survey revealed that the 1-year prevalence of disabling primary headaches in the Greek adult population aged 18–70 years is 12.0%, corresponding to 0.9 million adults. In contrast, the annual prevalence of primary headaches in Europe has been estimated to be higher than 50% (12). This vast discrepancy may be attributed mainly to our screening question, asking for headaches affecting performance only. In addition, a low mean annual prevalence rate in Greece, namely 29%, was also reported 20 years ago (1). Thus, both reasons may contribute, with different weights, to the final finding.
Migraine/probable migraine is the most common primary disabling headache disorder (8.1%), followed by TTH/probable TTH (3.8%). In the majority of European countries, the 1-year prevalence of all types of migraine is around 15% (12–19), while globally it is 14% (20). The crude prevalence of migraine in France is 8.2% (standardised 7.9%) (21), while another nationwide study in France reported it to be 11.2% for strict migraine and 10.1% for probable migraine (22). The annual migraine prevalence among adolescents in Norway is as low as 7% (23). In this study, the lower than Europe’s prevalence of migraine may rather be attributed to the combination of the screening question (limiting the headaches to those affecting performance), the inherent impreciseness, at individual level, to ascertain this change in performance, and at population level, the 70.2% of attrition bias during the process of survey. For TTH, the 3.8% 1-year prevalence in Greece is the lowest in Europe (12,16,18,20,23,24). The 60% sensitivity of our questionnaire for TTH diagnosis, but mainly our screening question focusing only on disabling headaches, may both contribute to the low prevalence found in the present study.
The present survey recorded a 1.0% annual CM/probable CM prevalence, corresponding to 0.2 million people in Greece. This estimation lies within the global prevalence range of 1–2% (25). However, in a large number of epidemiological studies, CM is grouped with other frequent headaches under the umbrella term chronic daily headache or chronic headache, including, along with CM, chronic TTH, new daily persistent headache and hemicrania continua. The annual prevalence of chronic headache has been reported to be 4% in Europe (12) and 3% globally (20). Similarly, the national prevalence in Croatia has been estimated to be 2.4% (26), in Turkey 3.3% (18), and in the Netherlands 3.7% (27). Usually, the contribution of chronic headache prevalence is near the global level of 1–2%, like in Turkey, where the prevalence of CM and chronic headache is 1.8% and 3.3% respectively (18). Nevertheless, in Norway, the chronic headache prevalence has been estimated to be 2.9%, but CM and probable CM contributed only the tiny prevalence of 0.01% and 0.1 respectively (28).
In the present study, the 1-year prevalence of cluster headache/probable CH was only 0.04% (four cases out of 10,008). The lifetime prevalence in Europe has been estimated at 0.2–0.3% (12). Similarly, the 1-year prevalence was 0.4% in Estonia (24), 0.1% in Germany (29), 0.1% in the Republic of Georgia (30), 0.2% in Sweden (31), 0.3% in Italy (32) and 0.3% in Denmark (33). Our sample of the adult population was sufficiently large and the validated questionnaire administered for the diagnosis was accurate enough to detect almost all participants with cluster headache. Thus, we may be confident enough that the annual prevalence of cluster headache in Greece is about 40 cases per 100,000 of adults, aged 18–70 years old.
Comparing the present survey to the older one (1), we may observe the lower prevalence rate of headaches in general because of the different methodology used, especially due to investigating headaches in general and not only the disabling ones as in the present study, and despite the suffering of the majority of Greeks from the consequences of the financial crisis (34). Notably, 0.9 million of Greek people with headache miss 0.5 workdays monthly (corresponding to 5.8 million lost workdays annually), while facing 2.8 days of reduced productivity every month (corresponding to 30.9 million workdays with reduced performance annually). Absenteeism and presenteeism of migraineurs were summed up into the relatively low number of 3.9 days monthly, in comparison to the mean 8.1 days per month with disabling headaches. It seems that not all migraine attacks were severe enough to affect their primary daily activities and nearly half of them (four out of eight) were just bothersome, affecting only the minor doings of the day. In comparison to the Eurolight survey, the absenteeism and the reduced productivity at work in Greece are close to the incidence reported in France or Lithuania, and fairly lower than other European countries; for example, Austria, Germany, Netherlands, Italy, Spain and Luxembourg (35). Because all headaches reported in this survey were disabling, the presenteeism rates (3.3 days) were high in relation to the monthly mean headache frequency (8 days) reported.
Importantly, 43.4% of headache participants had experienced shame or other negative feelings due to headaches at work or home. This probably occurs due to the inability of their colleagues at work or even their closest relatives to understand the pain severity and its influence on their productivity and behaviour. Thus, their real health status is frequently misunderstood and they are stigmatised as inefficient workers or work avoiders. That is probably one of the main reasons why migraine is underestimated in Greek society.
Only 21.9% of headache participants with headache had sought medical consultation and the majority of them (71.0%) had preferred to seek professional consultation in the private sector instead of a hospital. The main reasons for this preference may be related to the long delays for hospital appointments and the financial affordability of private professionals for the majority of Greeks. Although headache attacks were disabling among all headache participants, only 5.5% were under prophylactic treatment. Even more embarrassing is the finding that only a limited proportion of participants with CM (12.6%) were under prophylactic treatment. This is a blow to the quality of health care in Greece and requires a large awareness campaign for both citizens and health professionals. The use of prophylactic treatment for migraine is very low in Europe, generally. This is embarrassing, since migraine was ranked second among the diseases leading to lost years lived with disability (YLDs) (36). In the Eurolight project, a questionnaire-based survey in 10 European countries recorded that only 1.6–6.4% of migraineurs eligible for prophylaxis had received one treatment, and only Spain was an outlier with 13.7% (37).
Most participants with headache prioritised safety over effectiveness regarding prophylactic treatment, which should be oral rather than injectable. Nevertheless, the prioritisation of safety is mainly a preference of participants with headache who are naïve to prophylactic treatment and is reversed in favour of effectiveness in the subgroup of participants with headache who had already been exposed to prophylaxis. This finding is consistent with our previous epidemiological study concerning patients’ preferences (38). In this study, all data had been collected through interviews in headache centres and most headache patients had already been exposed to prophylactic treatment. In the same study, most patients (62.8%) had opted for external neurostimulation devices for migraine prophylaxis, and 67.1% for their use as acute treatment. This finding has not been replicated in the present study. The ranking of preferred therapies remained the same even when comparing subgroup pairs, like treatment-naïve participants with headache versus those on prophylaxis. The reverse finding concerning neurostimulation devices in the previous study may be attributed to the insufficient information offered by the interviewing physicians, since they were not experienced enough to offer specific details, given the limited availability of a single device type available in the Greek market. This perhaps resulted in an involuntary exaggeration of the privileges of this kind of therapy that possibly affected participants with headache preferences.
A surprising point was that 61.6% of headache participants participated in a specific spiritual type of rituals in order to remove the evil eye, considering it as the cause of at least some of their headaches. This is a common belief among Greeks, usually related to mild and moderate headache or flu-like symptoms, but not for more serious conditions like hemiplegia, seizures, or loss of consciousness. Originally, this was a pagan belief that was later partially embraced by Christianity.
Strengths of the study
This is the largest population-based epidemiological survey in Greece aiming to estimate the prevalence of medically selected disabling primary headache disorders. In addition, the burden of disabling headaches with treatment preferences were evaluated. So far, and to the best of our knowledge, no other similar survey covering all three aspects has been published recently in the field of headache. Importantly, to corroborate the headache diagnosis, the structured interview used for this survey was pre-evaluated for its specificity and sensitivity of the diagnosis according to the ICHD-3 beta criteria, although the evaluation was performed in out-patients.
Limitations of the study
The survey was deliberately restricted to participants with headaches impairing their daily life. Including performance in the screening question inevitably led to a decreased sensitivity of the questionnaire to detect TTH, since it is by definition mild to moderate and its prevalence is ultimately underestimated in the present study. This led to the paradoxical finding of TTH having a lower prevalence than migraine. Furthermore, rare primary headaches that highly affect performance, such as paroxysmal hemicrania, hemicrania continua, SUNCT, nummular headache or new daily persistent headache, were neglected or not evaluated. However, the principal aim of the study was to estimate the selected disabling primary headaches in the Greek adult population. It was accepted that several cases with mild, non-disabling headaches would be missed, since it is only the moderate to severe ones that usually affect performance in the vast majority of participants with headache. Given that among primary headaches TTH may be by definition mild to moderate, its prevalence is ultimately underestimated in the present study. Another limitation refers to the specificity for migraine, TTH and cluster headache in the pre-screening 37-item questionnaire, which was low although the sensitivity was high. As noted, this questionnaire was validated in the clinic and not in the general population where the survey was performed. It is highly probable that the main biases reported earlier in discussion, concerning migraine and TTH, may also have underestimated the burden of headaches. In addition, the influence of headaches on work and social life performance was assessed by self-reporting of the participants with headache and not by any relevant questionnaire, such as MIDAS. The 70.2% of non-participating respondents may have affected the representativeness of the sample, despite the balance achieved concerning age, gender and region. Even more, based on the automatic algorithm only one diagnosis could be made, therefore cases with more than one headache disorder were classified into the most predominant headache type. Finally, the tools used in the present study were different from those used in the “lifting the burden studies”, thus limiting the comparability of our findings to the countries where these tools were applied.
Conclusions
More than one out of ten Greeks aged 18 – 70 years old suffer from disabling headaches that need medical care and cause a dramatic loss in productivity. Notably, more than 80% of these people have never taken pharmacological prophylaxis, raising questions about headache awareness. Education of people with headaches and their environment, along with the reorganisation of headache services, may improve the appreciation, recognition, and management of headaches in Greece.
Public health relevance
The annual prevalence of primary headaches affecting performance of Greek people aged 18– 70 is 12.0%, corresponding to 885,040 persons. Headache-induced absenteeism amounts to 5.8 million lost workdays annually (0.5 per month) and presenteeism to 30.9 million workdays annually with reduced performance (2.8 days per month). The majority of participants with headache (56.2%) failed to respond to their social or family obligations at least 1 day per month and 2.5 days per month on average. In addition, 43.4% of them had experienced shame or other negative feelings due to their headaches. Despite the huge burden of headaches, 83.8% of the participants with headache had never taken pharmacological prophylaxis, and only 5.5% were currently under preventative treatment. The willingness to spend money out of their pockets is limited to an average €21.0 ± 8.8 per month. Regarding preferences for prophylactic treatment, 50.8% of participants with headaches opted for everyday oral medication, 18.5% for monthly injection and 14.3% for stimulation devices.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102421989630 - Supplemental material for A population-based survey for disabling headaches in Greece: Prevalence, burden and treatment preferences
Supplemental material, sj-pdf-1-cep-10.1177_0333102421989630 for A population-based survey for disabling headaches in Greece: Prevalence, burden and treatment preferences by Theodoros S Constantinidis, Chryssa Arvaniti, Nikolaos Fakas, Jobst Rudolf, Evangelos Kouremenos, Ermioni Giannouli and Dimos D Mitsikostas on behalf of the Hellenic Headache Society in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TSC, CA, NF, JR, EK and EG report no disclosures. DDM received research support, speaking fees and travel grants from Allergan and Novartis, relevant to the present study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was designed by the Hellenic Headache Society and was conducted on its behalf by Ipsos Opinion S.A. Company. The study was supported by unrestricted research grants from Novartis Hellas and Allergan Hellas.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.