
Abstract
Background
Diffusion tensor imaging (DTI) may demonstrate microstructural changes in diseased trigeminal nerves. Few prognostic indicators for long-term pain freedom after microvascular decompression (MVD) of the trigeminal nerve have been identified. The present study aimed to determine whether microstructural changes from DTI are present in the trigeminal nerve of patients with classical trigeminal neuralgia (cTN) due to arterial compression or deformation and whether they may be used to predict surgical success.
Methods
Patients with a diagnosis of cTN due to arterial compression or deformation that underwent MVD from October 2013 until December 2020, with high resolution 3T magnetic resonance imaging DTI, and over two years of post-surgical follow-up were included in this study. The microstructural metrics of the symptomatic and asymptomatic trigeminal nerve were compared using a paired, two-sided Student’s t-test. Differences between the microstructural metrics of the symptomatic nerve between treatment responders and treatment non-responders were assessed using Welch's t-test due to unequal variances and/or unequal sample sizes.
Results
Eighty-eight patients met inclusion criteria and were analyzed. There was no significant difference in fractional anisotropy (FA) (p = 0.3658), mean diffusivity (MD) (p = 0.1734) and radial diffusivity (RD) (p = 0.6586) between the symptomatic and asymptomatic nerve. There was a significant difference in AD (p = 0.0186). However, after the sequential modified Bonferroni correction, the difference in AD no longer reached significance. There was no significant difference in FA (p = 0.7556), MD (p = 0.8915), RD (p = 0.4324) and AD (p = 0.9918) in the symptomatic nerve between the treatment responders and non-responders.
Conclusions
DTI may not reliably predict outcomes of microvascular decompression in patients with cTN due to arterial compression or deformation.
This is a visual representation of the abstract.
Introduction
Trigeminal neuralgia (TN) is a clinical diagnosis defined by the International Headache Society as severe, electric shock-like, stabbing, shooting or sharp facial pain lasting from a fraction of a second to two minutes in the distribution of one or more branches of the trigeminal nerve (1). Classical TN (cTN) is a subtype of TN that is characterized by the previous clinical characteristics with demonstration of neurovascular compression (NVC) on magnetic resonance imaging (MRI) or during surgery. Microvascular decompression (MVD) of the trigeminal nerve is an effective treatment for TN (2). Predictors of surgical success (long-term pain freedom) have been identified and include response to medication (i.e. ox/carbamazepine), degree of NVC and symptom type (i.e. purely paroxysmal, concomitant continuous pain and/or neuropathy) (3–6). Diffusion tensor imaging (DTI) can be used to measure microstructural changes in white matter (7,8). Microstructural metrics measured from DTI include: fractional anisotropy (FA) is defined as the degree of diffusion along the nerve, axial diffusivity (AD) is defined as the magnitude of diffusion parallel to the nerve, mean diffusivity (MD) is defined as the magnitude of water diffusion in a space and radial diffusivity (RD) is defined as the magnitude of diffusion perpendicular to the nerve. Previous reports have demonstrated microstructural changes in the trigeminal nerve in patients with TN (9–11).
Several studies have identified differences in microstructural metrics between patients who respond to MVD and patients who do not (12,13). Historically, patients with more severe compression of the trigeminal nerve respond better to MVD (14). Severe vascular compression may cause increased white matter damage. If increasing degrees of NVC severity result in greater white matter damage, patients who respond to MVD should have decreased FA and AD and increased MD and RD (12,13). To our knowledge, no previous studies using DTI in TN have specifically studied patients with cTN due to only arterial compression or deformation.
The present study aimed to determine whether microstructural changes from DTI are present in the trigeminal nerve of patients with cTN due to arterial compression or deformation whether they may be used to predict surgical success.
Methods
Patient selection
We retrospectively reviewed a prospectively collected database on patients who underwent MVD to treat pain in the trigeminal nerve distribution from October 2013 until December 2020. Institutional review board approval was obtained.
Patients were excluded if they did not undergo a 3T MRI scan prior to surgery, had a prior ipsilateral procedure for TN (i.e. MVD, open partial sensory rhizotomy, stereotactic radiosurgery of the trigeminal nerve, percutaneous glycerol rhizolysis, percutaneous balloon compression or percutaneous radiofrequency ablation of the trigeminal ganglion), did not have a DTI FOCUS sequence, had trigeminal neuropathic pain, concomitant continuous pain, or did not have an artery causing compression or deformation of the trigeminal nerve. Patients were also excluded if the entry point of the trigeminal nerve into the pons could not be visualized bilaterally on the DTI sequence. Patients with less than two years of follow-up after MVD were excluded.
Classical TN (cTN) was defined as recurrent paroxysms of severe, electric shock-like, stabbing, shooting pain in the distribution of one of the branches of the trigeminal nerve, lasting under two minutes, which is triggered by innocuous stimuli with demonstration of neurovascular compression with morphological changes in the trigeminal nerve root on pre-operative MRI (1,15,16). To evaluate the utility of DTI in a homogeneous cohort, only patients with International Classification of Headache Disorders, 3rd edition (ICHD-3) classification of 13.1.1.1.1 with arterial compression or deformation of the trigeminal nerve were selected.
Pre-operative MRIs were read by two independent neuroradiologists (KT and MH) who were blinded to the side of TN. Each MRI was analyzed for the type of compression, degree of compression and responsible vessel. Neurovascular compression or deformation was defined as deformation or deviation of the trigeminal nerve due to an artery.
Clinical characteristics
Demographic and preoperative clinical characteristics were collected including age, sex, laterality of TN, pre-operative duration of disease, response to medication and symptom description.
MRI scan acquisition
The MRI examinations were completed on a 3-T MR scanner (GE Healthcare) prior to MVD (17). The protocol consists of sagittal T1, axial fluid-attenuated inversion recovery and diffusion-weighted imaging sequences of the entire brain with multiplanar thin-section steady-state free precession images through the cranial nerves The parameters used for the sagittal T1 sequences were: TR/TE, 600/default to minimum; slice thickness, 5 mm; gap, 1 mm; field of view (FOV), 22 cm; and matrix, 256 × 192. Axial imaging parameters were: TR/TE, 2200/150; slice thickness, 5 mm; gap, 1 mm; FOV, 22 cm; and matrix, 256 × 192. Steady-state free precession sequences were obtained with the parameters: TR/TE, default to minimum; flip angle, 65°; slice thickness, 1 mm; matrix, 384 × 256; number of excitations, 2; and FOV, 18–20 cm. DTI images were acquired with a reduced field of view diffusion imaging (18,19) in 21 directions with b = 800 s/mm2, slice thickness of 3 mm, repetition time of 4000 msec, echo time of 65 msec, flip angle of 90˚, matrix size of 160 × 80, and a FOV, 22 × 11 cm.
Operative technique
In the lateral decubitus position, a retromastoid craniectomy measuring approximately 1.5 × 2 cm was created. Copious cerebrospinal fluid was drained from the cerebellar medullary cistern to allow cerebellar relaxation. Exposure of the trigeminal nerve from the root entry point into the pons to the porus trigeminus was obtained. Microvascular decompression was performed throughout the length of the centrally myelinated portion of the trigeminal nerve. The dura was closed in a watertight manner and a calcium phosphate cement cranioplasty was performed.
Clinical follow-up and outcome
Pain status, complications and subsequent procedures were recorded by the neurosurgical team for each patient within seven days of the procedure and again at follow-up appointments or phone calls. Patients were categorized according to pain level at last follow-up: pain-free without medication, pain-free with medication, some pain relief and no pain relief. Treatment responders were defined as patients who were pain-free without medications at last follow-up. Treatment non-responders were defined as patients that had pain or required medications to be pain-free at last follow-up.
DTI processing
ExploreDTI software (https://www.exploredti.com) was used to correct for signal drift correction using a low-degree polynomial fit. An automatic background masking approach was applied in ExploreDTI to increase the specificity of the sampled area of the trigeminal nerve. Gibbs ringing, subject motion and eddy currents were also corrected for using ExploreDTI software. Bilateral regions of interest were manually drawn by a single author who was blinded to the symptomatic side and treatment response on axial slices of the FA color map. The region-of-interest (ROI) covered the entire portion of the visible trigeminal nerve from the entry point of the nerve into the pons (Figure 1(A)). The location of the ROI is demonstrated in Figure 1(B). Average FA, MD, AD and RD were measured from an ROI on each side.

Demonstration of diffusion tensor imaging color (online)/ black and white (print) map with cisternal segment of the (A) trigeminal nerve and (B) region-of-interest.
Volume measurement
Trigeminal nerve volume was assessed on 3T T2-weighted FIESTA images using ITK-SNAP (http://www.itksnap.org) (20). Manual segmentation of the trigeminal nerve was conducted from the entry of the nerve into the pons to the start of Meckel's cave. The Polygon Mode tool was used to trace the trigeminal nerve on axial images slice-by-slice and the volume was calculated using ITK-SNAP.
Microstructural analysis
Microstructural metrics (FA, MD, AD and RD) were compared between the symptomatic and asymptomatic trigeminal nerves. Microstructural metrics of the symptomatic trigeminal nerves were also compared between treatment responders and non-responders. The volumes of symptomatic and asymptomatic trigeminal nerves from the root entry point to the porus trigeminus were calculated using ITK-SNAP (20).
Statistical analysis
The microstructural metrics of the symptomatic and asymptomatic trigeminal nerve were compared using a paired, two-sided Student’s t-test. The volume of the symptomatic and asymptomatic trigeminal nerves was compared using a paired, two-sided Student’s t-test. Differences between the microstructural metrics of the symptomatic nerve between treatment responders and treatment non-responders were assessed using Welch's t-test due to unequal variances and/or unequal sample sizes. To avoid false discovery of a significant p-value with multiple testing, we utilized the sequential modified Bonferroni false discovery rate correction for the four DTI metrics in each of the two analyses. All values are reported as the mean ± SEM. q < 0.05 was considered statistically significant (i.e. false discover rate adjusted p-value). Analysis of covariance was used to assess how the microstructural metrics (FA, MD, RD and AD) differed between treatment responders and non-responders when controlling for the volume of the symptomatic trigeminal nerve. Normality of the data was assessed using histograms and QQ plots. Fisher's exact test was used to determine whether the rate of patients with long-term pain-freedom without medication differed by pre-operative disease duration. All statistics were performed in SPSS, version 29 (IBM Corp.) and R, version 2024.04.2 (R Core Team).
Results
Three hundred and sixty patients were evaluated for eligibility (Figure 2). Ninety-six were confirmed eligible. Forty-one patients did not undergo a pre-operative 3T MRI, 44 patients had a prior ipsilateral procedure (MVD or ablative procedure), 22 patients did not have a DTI FOCUS sequence performed, 21 patients had trigeminal neuropathy or concomitant continuous pain, and 136 patients had simple contact by an artery or vein, no contact by an artery, or deformation by a vein. Upon imaging analysis, eight patients did not have a visible root entry point bilaterally on DTI. All patients had at least two years of follow-up. Eighty-eight patients underwent final analysis.

Exclusion and inclusion criteria of study. DTI = diffusion tensor imaging; MRI = magnetic resonance imaging; REP = root entry point.
Patient demographics and clinical characteristics
Half of the patients were women (50%) and the average age at surgery was 65 years (Table 1). Right-sided TN was more common (56.8%). Most patients responded to ox/carbamazepine (89.8%). Pre-operative disease duration of less than 24 months (40%) and 25–48 months (40%) were the largest groups. Mean disease duration was 48.8 months.
Demographics and clinical characteristics.
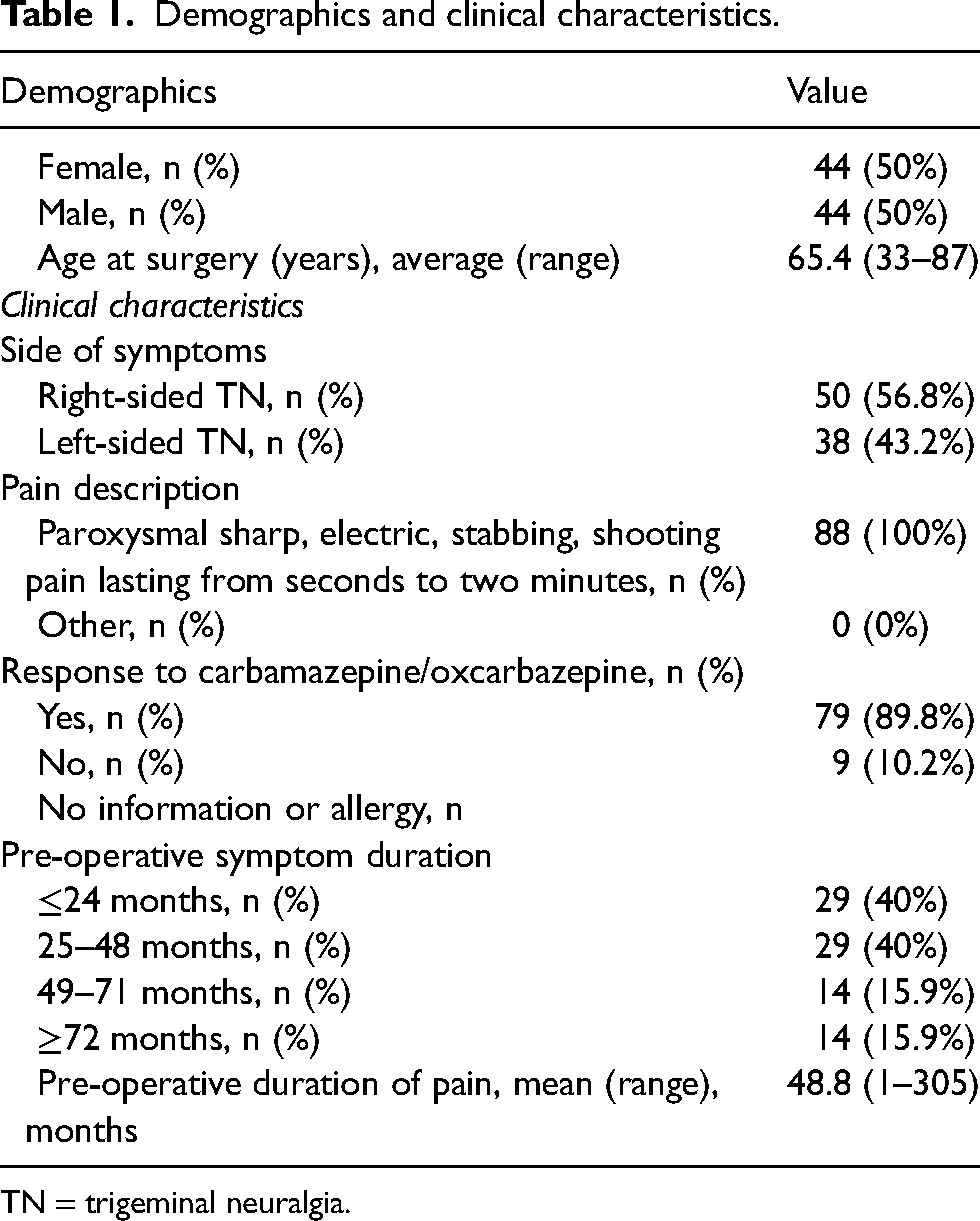
TN = trigeminal neuralgia.
Outcomes
At an average follow-up of 46.2 months, 84.1% of patients were treatment responders (pain-free without medications). Of treatment non-responders (15.9%), 3.4% of patients were pain-free with medications, 6.8% of patients had some pain relief and 5.7% had no pain relief. When patients were stratified by pre-operative pain duration, the rates of pain freedom at long-term follow-up for patients with less than 24 months of pain, 25–48 months of pain, 49–71 months of pain and greater than 72 months of pain were 79.3, 93.1, 85.7 and 78.6% respectively (Table 2). There was no significant difference in the rate of pain freedom between groups (p = 0.43).
Long-term pain status after microvascular decompression.

*Fisher's exact test showed no statistically significant difference in long-term pain freedom rates between pre-operative disease duration groups.
F/U = follow-up.
Volume
Volumes of the trigeminal nerves appear to be relatively normally distributed with perhaps mild right skew on both the symptomatic and asymptomatic side (see supplementary material, Figures S1 and S2). There was no significant difference (p = 0.0763) between the volume of the affected trigeminal nerve (mean = 47.99 mm3) and the volume of the unaffected trigeminal nerve (mean = 51.52 mm3).
Microstructural differences between symptomatic and asymptomatic nerves
There was no significant difference in FA (p = 0.3658), MD (p = 0.1734) and RD (p = 0.6586) between the symptomatic and asymptomatic nerve (Figure 3). Table 3 shows averages and standard deviations of the microstructural metrics. There was a significant difference in AD (p = 0.0186). However, after the sequential modified Bonferroni correction the difference in AD no longer reached significance. As shown in the supplementary material (Figures S1 and S2), all four microstructural metrics (i.e. FA, MD, RD and AD) appear to be normally distributed on both the affected and unaffected sides.

Comparison of fractional anisotropy, mean diffusivity, radial diffusivity and axial diffusivity between affected trigeminal nerve and unaffected trigeminal nerve.
Average microstructural metrics in symptomatic and asymptomatic nerve.

AD = axial diffusivity; FA = fractional anisotropy; MD = mean diffusivity; RD = radial diffusivity.
Microstructural differences of symptomatic nerve between treatment responders versus treatment non-responders
There was no significant difference in FA (p = 0.7556), MD (p = 0.8915), RD (p = 0.4324) and AD (p = 0.9918) between the symptomatic nerve between the treatment responders and non-responders (Figure 4). Table 4 shows averages and standard deviations of the microstructural metrics. When controlling for volume, there was no significant difference in FA (p = 0.3436), MD (p = 0.3108), RD (p = 0.2258) and AD (p = 0.4711) between the symptomatic nerve between the treatment responders and non-responders.

Comparison of fractional anisotropy, mean diffusivity, radial diffusivity and axial diffusivity between treatment responders and treatment non-responders.
Average microstructural metrics in symptomatic and asymptomatic nerve.

AD = axial diffusivity; FA = fractional anisotropy; MD = mean diffusivity; RD = radial diffusivity.
Discussion
The present study demonstrates that DTI does not reliably differentiate diseased and healthy trigeminal nerves in patients with classical TN due to arterial compression/deformation. A lack of reproducibility presents a challenge for using DTI as a pre-operative prognostic marker of surgical success with MVD.
It is certainly possible, as others have shown (11,13), that DTI may be useful in other subpopulations of patients with TN, but, in this homogenous cohort of patients with cTN due to arterial compression/deformity, utilizing these techniques, the utility of DTI was low.
Several studies have demonstrated changes in microstructural metrics in trigeminal nerves effected by TN (9,10,21–24). Our imaging protocol utilized 20 diffusion directions, with b = 800, and a nerve-specific protocol. Previous studies have ranged between 15–32 diffusion directions with b = 800 or 1000. Several of these studies use whole brain imaging (22,23), whereas a few use nerve specific imaging (21,24). Preliminary published data show that nerve specific protocols may be better at assessing microstructural metrics in the trigeminal nerve than whole-brain imaging (25). The 3 mm slice thickness used for DTI images in the present study is noteworthy. Although many groups have used a slice thickness of 1–2 mm (21–24), others have found statistically significant differences between affected and unaffected nerves using a 3 mm slice thickness (26). It is possible that our slice thickness may have a slightly lower sensitivity to detect microstructural changes. Therefore, despite our study being among the largest published on DTI in patients with TN (9–13,21–24,26), some of the power to detect microstructural differences may be lost due to the slice thickness. Additionally, stratifying patients based on subtype of TN during analysis is important. Trigeminal nerves in patients with cTN may have smaller volumes due to more significant compression, which may influence microstructural metrics. To our knowledge, this study is the largest study comparing DTI microstructural metrics between diseased and health trigeminal nerves in a homogenous cohort of patients with cTN.
Even with adequate decompression of the trigeminal nerve during MVD, there are a subset of patients that continue to have pain or eventually have pain recurrence. Numerous papers have studied predictors (e.g. response to medication, degree of neurovascular compression, pain character) of MVD failure (3–6). Utilization of DTI has been identified as a potential objective measure for predicting post-operative outcomes in TN. However, our study demonstrates that we may not be close to reliably using DTI to predict MVD outcomes, especially if microstructural metrics are not consistently altered in affected trigeminal nerves.
Extraction of microstructural metrics from the trigeminal nerve is inherently limited by partial volume effects. Due to the small size of the nerve and the surrounding cerebrospinal fluid, it is difficult to only capture signal from the trigeminal nerve in the region of interest. Furthermore, the more severe compression seen in classical TN, as compared to idiopathic TN, may decrease the volume of the trigeminal nerve and increase the susceptibility to partial volume effects. The appropriate location to draw the region-of-interest has been debated. Studies have drawn the ROI on the brainstem (13,27), whereas others have focused on the trigeminal nerve between the root exit zone and the foramen ovale (10). Current evidence suggests that compression along the centrally myelinated portion of the trigeminal nerve may be responsible for cases of cTN (28,29). Therefore, in our series, we drew our ROI from the root exit zone of the trigeminal nerve into the pons to the presumed entrance of the trigeminal nerve into the foramen ovale (i.e. where the nerve is no longer visible).
Although we did not specifically examine the effect of ROI shape or size on diffusion metrics, we attempted to follow the generally accepted principle that ROIs targeted to only include nerve tissue yield the most reliable microstructural metrics (30). A study specifically examining the effect of ROI size and shape on microstructural measurements of the trigeminal nerve is an interesting future direction.
In our experience, performing MVD on patients over 65 years of age has historically been avoided due to safety and efficacy concerns. However, studies have shown that performing MVDs in older patients, even over 75 years old, is both safe and effective (31). Therefore, our cohort may be older than other cohorts undergoing MVD, but it may be more indicative of the overall population of patients with TN because our practice does not exclude older patients from receiving surgery.
With respect to pre-operative pain duration, the average disease duration of approximately four years prior to surgical intervention in this cohort may be shorter than the larger population of patients with TN. Disease duration has been shown in several studies to impact long-term outcomes of TN (2,32,33). It is possible that longer disease duration may cause more demyelination, though this remains speculative. In the present study, disease duration was not found to predict outcomes.
Several other limitations of the present study are worth noting. The sample size may limit our ability to detect true differences in the microstructure of the nerve. The retrospective nature of the study may indirectly affect the primary findings, specifically by introducing recall bias. As noted above, slice thickness for acquisition of DTI images is a limitation of the present study. Data concerning specific distributions of facial pain were unavailable for this cohort, thus limiting our ability to make definitive claims about this cohort’s representation of the broader TN population. The background masking approach applied during DTI processing increases the specificity of the results, but it resulted in the exclusion of eight patients from the study cohort due to lack of visualization of the trigeminal nerve on the FA color map, which may limit the generalizability of the results.
To more accurately determine whether DTI can be utilized to identify the affected trigeminal nerve, and also as a prognostic indicator, a prospective study with a nerve-specific, thin-sliced MRI protocol is necessary.
Conclusions
DTI may not reliably predict outcomes of microvascular decompression in patients with cTN due to arterial compression or deformation.
Diffusion tensor imaging may not reliably differentiate diseased and healthy trigeminal nerves in people with cTN due to arterial compression or deformation. DTI may not be a prognostic indicator for pain relief after microvascular decompression for people with cTN.
Supplemental Material
sj-jpg-1-cep-10.1177_03331024251322505 - Supplemental material for An analysis of diffusion tensor imaging in classical trigeminal neuralgia
Supplemental material, sj-jpg-1-cep-10.1177_03331024251322505 for An analysis of diffusion tensor imaging in classical trigeminal neuralgia by Margaret Tugend, Colby T. Joncas, Katie Traylor, Marion A. Hughes and Raymond F. Sekula in Cephalalgia
Supplemental Material
sj-jpg-2-cep-10.1177_03331024251322505 - Supplemental material for An analysis of diffusion tensor imaging in classical trigeminal neuralgia
Supplemental material, sj-jpg-2-cep-10.1177_03331024251322505 for An analysis of diffusion tensor imaging in classical trigeminal neuralgia by Margaret Tugend, Colby T. Joncas, Katie Traylor, Marion A. Hughes and Raymond F. Sekula in Cephalalgia
Footnotes
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
Retrospectively reviewed a prospectively collected database on patients that underwent MVD to treat pain in the trigeminal nerve distribution from October 2013 until December 2020. Institutional review board approval was obtained.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.