EP.01
MERTK in the rat trigeminal system: a potential novel target for cluster headache?
J Edvinsson1, C Ran2, F Jennysdotter Olofsgård2, A Steinberg2, L Edvinsson1 and A Carmine Belin2
1Lund University, Lund, Sweden
2Karolinska Institutet, Stockholm, Sweden
Introduction: The trigeminal system is key to the pathophysiology of migraine and cluster headache, two primary headache disorders that share many features. Recently, MER proto-oncogene tyrosine kinase (MERTK), a cell surface receptor, was strongly associated with cluster headache through genetic studies. Further, the MERTK ligand galectin-3 has been found to be elevated in serum of migraine patients.
Objective: In this study, MERTK and MERTK ligands were investigated in key tissue to better understand their potential implication in the pathophysiology of primary headache disorders.
Methods: Immunohistochemistry was used to map MERTK and galectin-3 expression in rat trigeminal ganglia. RT-qPCR was used to assess MERTK gene expression in blood, and ELISA immunoassays were used for MERTK ligand quantification in serum from study participants with and without cluster headache.
Results: MERTK gene expression was elevated in blood samples from study participants with cluster headache compared to controls. In addition, MERTK ligand galectin-3 was found at increased concentration in the serum of study participants with cluster headache, whereas the levels of ligands growth arrest specific 6 and protein S unaffected. MERTK and galectin-3 were both expressed in rat trigeminal ganglia. Galectin-3 was primarily localized in smaller neurons and to a lesser extent in C-fibres, while MERTK was found in satellite glia cells and in the outer membrane of Schwann cells. Interestingly, a strong MERTK signal, emanating from Schwann cells, was found in specifically in the region proximal to the nodes of Ranvier.
Conclusion: The overexpression of MERTK and galectin-3 in tissue from study participants with cluster headache, as well as the presence of MERTK in rat peripheral satellite glia cells and Schwann cells in the trigeminal ganglia, further highlights MERTK signalling as an interesting potential future therapeutic target in primary headache.
Figure


EP.02
Changes in work schedule affect headache frequency among Norwegian nurses – a three-year follow-up study
E Kristoffersen1,2, S Waage3,4, S Pallesen3,4 and B Bjorvatn3,5
1Department of General Practice, University Of Oslo, Oslo, Norway
2NorHead, Department of Neurology, Akershus University Hospital, Lørenskog, Norway
3Norwegian Competence Center for Sleep Disorders, Haukeland University Hospital, Bergen, Norway
4Department of Psychosocial Science, University of Bergen, Bergen, Norway
5Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway
Introduction: Night workers are on duty during their biological resting phase and studies suggest that working rotating shifts, multiple night shifts per year and multiple quick returns (defined as shifts with less than 11 hours in-between) per year are associated with shortened sleep, increased risk of sleep disturbances, pain and other health complaints. Short sleep duration and disturbed sleep can trigger headache, and work schedule is therefore hypothesized to affect the risk of headache per se, including the risk of primary headache disorders.
Objectives: The aim of the present study was to explore whether changes in work schedule, number of night shifts, and number of quick returns were related to changes in headache frequencies.
Methods: A longitudinal study with questionnaire data from 2014 (baseline) and 2017 (follow-up) on work schedule (day only, shift work without nights and shift work with nights), number of night shifts, number of quick returns (less than 11 hours in-between shifts) and validated headache diagnoses among 1104 Norwegian nurses. Associations were explored by multivariate regression analyses with adjustment for age, sex, prior headache type, anxiety, depression and change in number of working hours.
Results: The median age at baseline was 37 years (interquartile range 31-43) and 90.5% were female. In the adjusted logistic regression analysis of changed work schedule between baseline and follow-up, changing from night work was associated with increased odds for reversion from headache >1 days/month to no headache at all last year (odds ratio (OR) = 2.77, confidence interval = 1.29–5.95). Changes towards less night shifts (>10) or less quick returns (>10) during the last year were associated with increased odds of reversion of headache to no headache (OR = 2.23, 1.20–4.17 and OR = 1.90, 1.04–3.49, respectively). Only decrease in number of night shifts (>10) during the last year reduced risk of onset of any new headache between baseline and follow-up (OR = 0.39, 0.18–0.84).
Conclusion: Changing from night work and reducing the number of night shifts and quick returns were associated with less headache in this three-year follow-up of Norwegian nurses. This adds to the growing body of evidence that shift work may have direct negative health consequences
EP.03
Clinical features and ICHD diagnoses in patients referred by a rhinologist to headache specialists for prominent craniofacial pain
A Ali1, J Singh, A Saleem and J Craig
1Henry Ford Health
2Michigan State University
Introduction: The majority of patients diagnosed with “sinus headache” are misdiagnosed and mistreated. These patients are often referred to ENT for further evaluation of sinus disease. As of yet, collaboration between rhinologists and headache specialists for evaluation of “sinus headache” has not been studied.
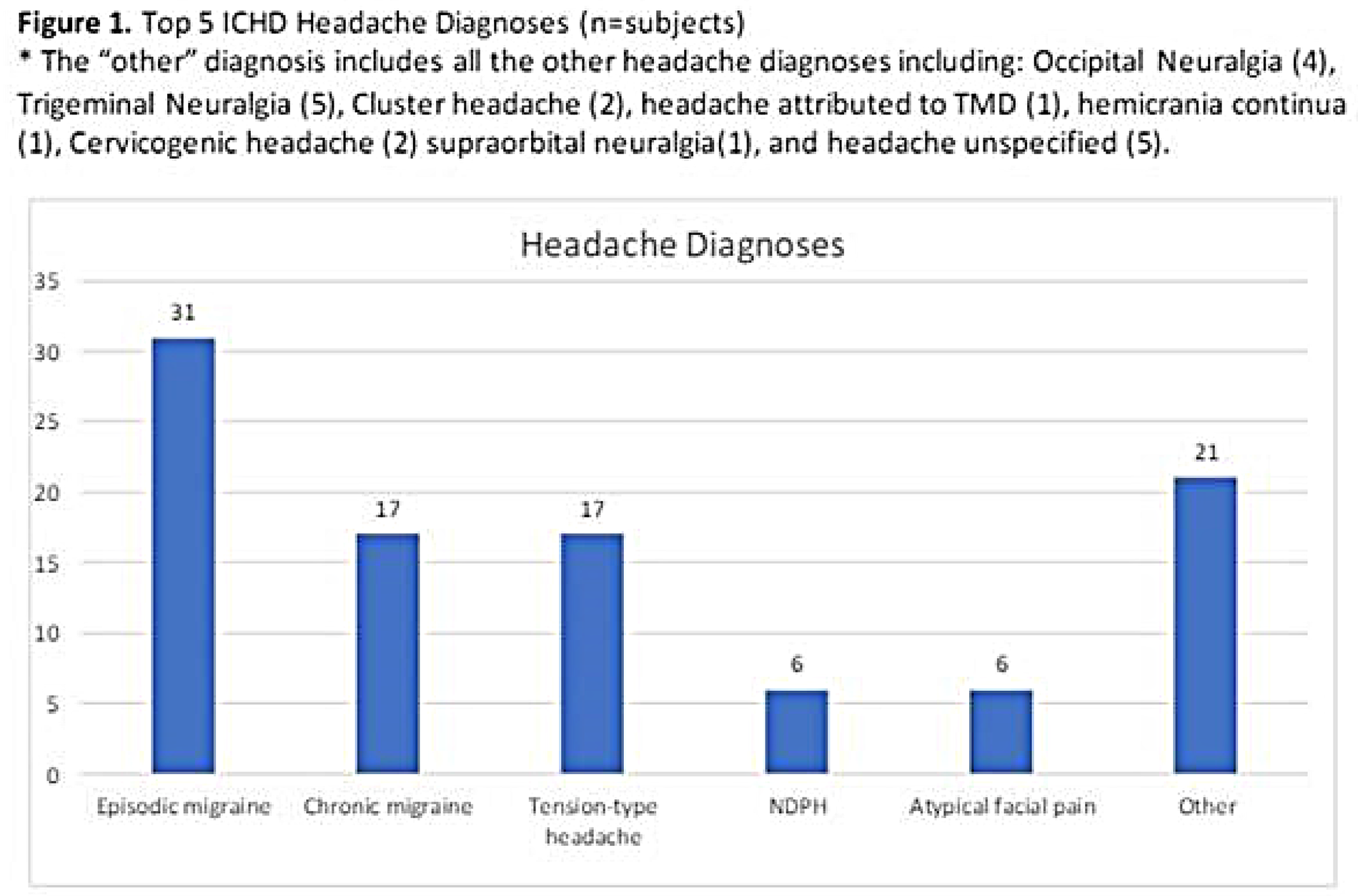
Objective: To report clinical features and ICHD headache diagnoses in patients referred by a rhinologist to headache specialists for prominent craniofacial pain.
Methods: We conducted a retrospective study of patients presenting for craniofacial pain to a rhinologist, who were subsequently referred to a headache specialist for presumed non-sinogenic craniofacial pain. A total of 98 patient charts were reviewed and information including demographics, gender, nasal endoscopy findings, SNOT-22 (Sino-Nasal Outcome Test-22 questionnaire) score, ICHD (International Classification of Headache Disorders) headache diagnosis, and headache characteristics were extracted.
Results: Nasal endoscopy performed in the rhinologist clinic was normal in 92.7% of patients, edema was noted in 5.2% of patients, and mucopurulence in 2% of patients. The majority of the patients described their pain as frontal or frontal-maxillary, dull or throbbing, and moderate to severe. Migraine was the most common final diagnosis in 49.1% of the patients and the second most common diagnosis was tension-type headache in 17.3% of the patients. The remaining patients were diagnosed with 11 additional ICHD diagnoses.
Conclusion: Patients referred from a rhinologist to a headache specialist for non-sinogenic craniofacial are likely to carry a diagnosis of a primary headache disorder, specifically migraine or tension-type headache. Collaboration between specialists may improve diagnostic accuracy and outcomes. Future study is warranted.

EP.04
Colours and intermittence/flickering quality of aura visual symptoms evaluated in a multicentre, cross-sectional study
M Viana1,2, A Hougaard3,4, E Tronvik5,6, I Grøntveit Winnberg5,6, A Ambrosini7, A Perrotta7, T Phu Do3,4,8, M Al-Mahdi Al-Karagholi3, M Fominykh8, S Sihabdeen2, C Gobbi2,9 and C Zecca2,9
1King’s College London, London, United Kingdom
2Neurocenter of Southern Switzerland, Lugano, Switzerland
3Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
4Department of Neurology, St. Olavs Hospital, Trondheim, Norway
5NorHEAD, NTNU, Norwegian University of Science and Technology, Trondheim, Norway
6Headache Clinic, IRCCS Neuromed, Pozzilli, Italy
7Danish Knowledge Center on Headache Disorders, Rigshospitalet Glostrup, Glostrup, Denmark
8IMTEL, Norwegian University of Science and Technology, Trondheim, Norway
9Faculty of Biomedical Sciences, Università della Svizzera Italiana, Lugano, Switzerland
Introduction: Visual symptoms are the most common disturbances of migraine aura. These symptoms can be described systematically by subdividing them into elementary visual symptoms (EVS). Since EVSs are not easy to describe verbally, we developed and tested in a large population of patients a collection of images (n = 27) illustrating the spectrum of migraine aura EVSs (SMAI – Standardized Migraine Aura Iconography - Figure). Indeed, some EVS have also important additional features such as the colours and interremittent/flickering quality. Yet such features have not been considered properly during previous clinical studies on migraine aura with spare exceptions (Crotogino 2001; Queiroz 2011).
Objectives: main objective of this study was to specifically document the colours and intermittence/flickering quality of EVSs.
Methods: Individuals with migraine aura recruited from four tertiary headache centres (in Switzerland, Denmark, Norway and Italy) were invited to complete a web-survey were we tested a set of images representing 25 EVSs. In such survey we also requested information regarding: i) colour of each EVS, which participants could select from a list of 14 options, and ii) the intermittent or flickering quality of these symptoms which we assessed through the following question: “Is it/are they sparkling (like stars or flashing lights) and/or flickering (with rapid movements like the wings of a butterfly)?”.
Results: Two hundred and fifteen participants completed the study (78.9% women, median age 36). They recognised a total of 1645 EVS from our predefined list. The median number of EVS recognised by participants was seven (IQR 4–11). Prevalence of various colours and intermittent/flickering quality are provided in Table. An intermittent/flickering quality was described in most cases in which this aspect was applicable (bright light, zig-zag lines, small bright dots, white dots/round forms, coloured dots, coloured lines, geometrical images, tiny flickering dots, ‘bean-like’ forms, and corona effect). Participants reported specific colours of their EVS where this feature was applicable (zig-zag lines, coloured dots, coloured lines, geometrical images, ‘bean-like’ forms). The most frequently reported colours were generally silver, black, white, and grey. Of non-grayscale colours, yellow was most frequently reported.
Conclusion: For the first time, we systematically examined the occurrence of specific features related to EVSs, such as intermittence/ flickering and colour, in a large population of participants. These characteristics hold clinical relevance due to their distinct and easily detectable nature, with a high frequency of occurrence (59% of cases for intermittence/flickering and 88% for colour).
Figure 1


EP.05
The healthcare burden of migraine in England: a retrospective cohort study using electronic health record data from Clinical Practice Research Datalink (CPRD)
S Collings1, A Patel2, H Gowman2, S Law2, A Ahern1, R Pawinski1, R Wood2 and S Afridi3
1Pfizer Ltd, Tadworth
2Adelphi Real World, Bollington, United Kingdom
3Guy's and St Thomas’ NHS Trust Foundation, London, United Kingdom
Introduction: Migraine costs the United Kingdom National Health Service an estimated £1 billion per year in direct healthcare costs. Poor management of migraine places avoidable burden on patients and the healthcare system, however there is limited evidence available on the health care resource utilisation (HCRU) of migraine patients across England and different healthcare settings.
Objectives: To quantify the healthcare burden (HCRU and associated direct medical costs) of adults with migraine in England and compare with general population controls.
Methods: A retrospective cohort study of adults newly diagnosed with migraine between 1 January 2017 and 31 March 2019, using linked primary and secondary healthcare data (Clinical Practice Research Datalink Aurum [CPRD] and Hospital Episode Statistics [HES]) in England. Migraine cases and general population controls were matched on age, sex, ethnicity, practice region, Index of Multiple Deprivation and baseline comorbidities (depression, cardiovascular disease). All-cause HCRU and migraine-related (primary care prescriptions, general practitioner [GP] appointments, inpatient stays, outpatient visits, accident & emergency [A&E] attendances) and costs were estimated for cases and compared with controls. HCRU (rates, per patient-year [ppy]) and costs (per patient per year [pppy]) were described during a variable 12-month minimum follow-up period, with the study period extending to 31 March 2021. HCRU and costs were reported overall and stratified by geographical region.
Results: A total of 62,143 migraine cases and matched general population controls were identified, of which 76.2% (n = 47,376) were female and the mean [SD] age at index was 39.8 [15.5].
Migraine cases had greater rates [95% CI] of all-cause secondary care interactions than controls (outpatient consultations; cases: 3.0 [2.98, 3.00] versus controls: 1.7 [1.70, 1.71]; A&E attendances; cases: 0.5 [0.53, 0.54] versus controls: 0.3 [0.26, 0.27]; inpatient stays; cases: 0.4 [0.42, 0.42] versus controls: 0.2 [0.24, 0.24]). Total all-cause direct medical costs were numerically higher for cases compared with controls (mean [SD]: £884 [£1,923] versus £654 [£1,595]). All-cause costs attributed to inpatient stays (mean [SD]) (cases: £408 [£1,479]; controls: £245 [£1,122]) accounted for the largest proportion of total medical costs (cases: 46.2%; controls: 37.5%).
Among migraine patients, 69.4% (n = 43,131) had a migraine-related primary care consultation, 14.7% (n = 9,123) required an outpatient consultation, 0.4% (n = 228) A&E attendance and 7.8% (n = 4,869) inpatient stay related to migraine. 15.1% (n = 9,362) of migraine patients saw a neurologist during follow-up.
When observing total all-cause costs in cases by geographical region, costs ranged from (mean [SD]) £783 [£1,603] in the East Midlands to £1,025 [£1857] in the North East. Total all-cause costs of cases in London were £862 [£2,086].
Conclusion: Overall, patients with migraine contribute a larger cost burden on the healthcare system than their matched controls, demonstrated by patients with migraine utilising more expensive secondary care services. Furthermore, all-cause direct medical costs of migraine cases varied substantially between geographical regions, which may suggest inequities in the management of patients with migraine.
EP.06
The use of triptans and other acute treatments for the management of migraine in routine clinical practice in England: a retrospective cohort study using data from Clinical Practice Research Datalink (CPRD)
S Collings1, A Patel2, H Gowman2, S Law2, A Ahern1, R Pawinski1, R Wood2 and S Afridi3
1Pfizer Ltd, Tadworth
2Adelphi Real World, Bollington, United Kingdom
3Guy's and St Thomas’ NHS Trust Foundation, London, United Kingdom
Introduction: In the United Kingdom, migraine is the second leading cause of years lived with disability and optimal management has been indicated as a priority for improving migraine care. Prior to recent approval of calcitonin gene-related peptide (CGRP) inhibitors, acute treatments recommended by the National Institute for Health and Care Excellence (NICE) for primary care management of migraine included triptans, non-steroidal anti-inflammatory drugs (NSAIDs) and analgesics. Despite the availability of prescribing guidelines and an array of treatments, there is a paucity of data on the management of migraine patients with acute treatments (prior to the availability of CGRP inhibitors) in clinical practice, specifically, which acute treatments are being prescribed within primary care and treatment sequencing.
Objectives: To describe patterns in acute treatment use for migraine in primary care in England.
Methods: A retrospective cohort study using linked primary and secondary healthcare data in England (Clinical Practice Research Datalink Aurum [CPRD] and Hospital Episode Statistics [HES]). Adults newly diagnosed with migraine between 01.01.2017 and 31.03.2019 were identified. Medication use was described in primary care only.
Acute treatment patterns (prescribing rates, sequencing) and triptan use in primary care were described during a variable 12-month minimum follow-up period, with the study period extending to 31 March 2020.
Results: A total of 62,205 patients met all eligibility criteria, of which 76.2% (n = 47,420) were female and the mean (SD) age at index was 39.8 (15.5) years.
Triptans (25.7%; n = 15,971) and NSAIDs (15.1%; n = 9,368) were the most commonly prescribed acute treatments during follow-up; opiates were prescribed to 8.7% (n = 5,397). Of the 18.9% (n = 11,780) of patients prescribed at least 2 acute treatments on or following index, a high proportion of patients moved from triptans to opioids (61.8%, n = 7,285) and almost 22% (21.7%; n = 2,556) moved from an opiate to a triptan.
For patients prescribed at least 2 different triptans (n = 1,149; 1.8%), the median time-to-second triptan was 299.0 (IQR 103.0-562.0) days. Following initiation of the second triptan, 17.2% (n = 198/1,149) of patients subsequently cycled back to a previously prescribed triptan, and 14.7% (n = 170/1,149) cycled back to the same triptan and formulation.
A total of 9,362 (15.1%) patients saw a neurologist during follow-up, with a median of 89 days (IQR 1.0-241.0) since diagnosis; of these 16.6% (n = 1,558) were prescribed a triptan prior to their first neurologist consultation during follow-up.
Conclusion: Triptans are the most prescribed acute treatment for migraine; however, the management of migraine appears to include regimens with opioids, counter to NICE recommendations. In addition, many patients had not been prescribed a triptan prior to attending their first neurologist consultation post-migraine diagnosis.
These observations suggest that migraine patients are not being optimally treated in primary care in accordance with local and international best practices, highlighting a need for further guidance and education on the management of migraine in primary care.
EP.07
Women with migraine and non-response to triptans have lower income and income growth than those responding to triptans– a Danish nationwide registry study
M Ashina1, J Hansen2, D Hauberg5, U Lønberg5 and T Steiner1,3,4
1Department of Neurology, Danish Headache Center, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
2Private neurology practice, Slagelse, Denmark
3Department of Neuromedicine and Movement Science, Norwegian University of Science and Technology, Trondheim, Norway
4Division of Brain Sciences, Imperial College London, London, United Kingdom
5Pfizer Denmark, Copenhagen, Denmark
Introduction: Migraine, a neurological disease, negatively impacts education and work performance, a disease-attributed burden that is cumulative over a lifetime. People with migraine who do not respond sufficiently to acute treatments such as triptans are likely to earn less, and see fewer increases in earnings during their working years, than people without migraine. Migraine affects three times more women than men.
Objectives: In this population-based study using data from Danish national registries, we estimated, in women with migraine, the differences in absolute and relative gross annual earnings over time between those with presumed triptan non-response and those with triptan response.
Methods: From the Danish National Prescription Register, we identified all women aged 18-65 years with triptan non-response, defined as having redeemed prescriptions for three or more distinct triptans, but fewer than ten of the last prescribed triptan, between 1998 and 2019 (“non-responders”). Each was matched by year of birth, region of residence and year of first triptan prescription redemption with three women with triptan response, defined as persons redeeming prescriptions for triptans continuously in the study period (“responders”). Annual individual gross income was defined as the total annual salary recorded in the Danish Income Statistics Register. Growth in annual gross income was calculated with year 0 (the year when non-responders discontinued triptan treatment) as the baseline for each group.
Results: We identified 4,275 non-responders and 12,671 responders. At year 0, non-responders had 16% lower average annual gross income than responders (30,416 EUR vs. 35,254 EUR; p < 0.001). Women in both groups had similar growth rates in annual income in years -3 to year 1. In subsequent years, non-responders showed almost no annual income growth until year 6, after which their average income increased until year 10. In comparison, responders showed an approximately linear growth in average annual gross income throughout, until year 10 (Figure 1). Ten years after triptan discontinuation, non-responders earned 31,845 EUR, and responders 40,543 EUR, a difference of 27%; p < 0.001.
Conclusion: Women with triptan non-response had, on average, lower incomes prior to discontinuing triptans and reduced growth in income over the 14-year study period than women with triptan response, a combination resulting in an income gap that was both cumulative and widening. Triptan non-response, usually implying exhaustion of all acute treatment options, is likely to be indicative of poor control of migraine, impeding, first, entry into the workforce and, second, successful career advancement. As women as a group already experience a societally-imposed wage gap compared to men, triptan non-response may impact them more severely. The study highlights the economic impact of inadequately treated migraine on women, and an important and unmet treatment need.
Figure 1

EP.08
A novel model of same day emergency neurology care prevents hospital admissions, reduces unnecessary tests and streamlines care for patients presenting acutely with headache
W Bierrum1, J Spencer1, R Macarimban1, A Shirazi1, A Dethabrew1, I See1, A Chandratheva1, R Simister1, A Alim-Marvasti1 and S Haider1
1Acute neurology service (Neuro-SDEC) UCLH, London, United Kingdom
Introduction: The acute neurology service (neuro-SDEC) at UCLH is a consultant led service embedded within same day emergency care (SDEC) at UCLH. The aim of the service is to provide rapid diagnosis, investigation and treatment for patients presenting with acute neurological conditions such as headache.
Through early specialist input, urgent investigations such as same day MRI and pathways including an IV magnesium pathway for status migrainosus, the service can provide significant benefit to these patients.
To quantify this, a snapshot audit was undertaken from November – December 2023 to review all headache cases seen by the service, as well as all admitted patients that would have been appropriate for neuro-SDEC but were not seen by the service.
Objectives: The audit aimed to evaluate the impact of neuro-SDEC on the management of patients presenting acutely with headache and compare this against the standard model of admitting patients for an inpatient investigations and neurology review.
Methods: Patients were prospectively logged from 27th November to 19th December 2023. All cases seen by neuro-SDEC were scrutinised to assess whether neuro-SDEC review avoided hospital admission, prevented a lumbar puncture and avoided general neurology outpatient referral.
Inpatient ward lists were screened daily to identify admitted patients and each case was reviewed to look at the length of inpatient stay, time to imaging and neurology review, as well as discharge diagnosis and onward referrals.
Results: 52 patients with headache were seen by the SDEC neurology team during the audit period, 48% of these patients would have otherwise been admitted to hospital. 30 general neurology outpatient clinic referrals were avoided and 5 patients avoided having a lumbar puncture. In 61% of cases, the diagnosis changed after the patient was seen by the neurology team.
There were 7 patients admitted to hospital with headache during the study period. These patients had a combined length of stay of 17 bed days. 3 patients had an inpatient MRI with a wait time of 22 hours. The average wait time for inpatient neurology review was 42 hours. 42% of admitted patients underwent a lumbar puncture. Of note, 2 patients were referred to neuro-SDEC to facilitate an earlier discharge from hospital.
Migraine was the most common diagnosis in both groups of patients.
Conclusion: Neuro-SDEC provides an effective alternative model to the standard of care for patients presenting acutely with headache. The service prevents hospital admissions, reduces unnecessary tests such as lumbar puncture and prevents referrals to general neurology outpatients. Having the service available also reduces inpatient length of stay and facilitates earlier discharge from hospital.
Overall, the service benefits patients presenting acutely with headache by enabling prompt diagnosis, investigation and treatment, as well as reducing time spent in hospital and on outpatient waiting lists.
EP.09
Partnering with Pharmacy Teams to Improve Migraine Management
D Watson1, C Duncan1, K Styles1, S Flannery1, R Music2 and L Coyle1
1NHS Grampian, Aberdeen, United Kingdom
2Migraine Trust, London, United Kingdom
Introduction: Migraine affects approximately 1 in 7 people and is the second highest cause of global disability in the general population significantly impacting the quality of life for affected individuals. It is often under recognised, inappropriately managed and medication overuse remains a common issue. A patient survey identified that community pharmacies were the number one place people wished to receive advice. Community pharmacies play a crucial role in supporting patients with migraine. However, there is considerable variation in the skills and knowledge needed to assess, support, and manage migraine cases resulting in potentially inaccurate assessments, improper advice, and suboptimal pharmaceutical management. To address these challenges, a collaborative project between a patient organisation and a health authority aimed to enhance recognition and management of migraine within pharmacy teams.
Objectives: The primary objective was to reduce variation by developing targeted learning resources for pharmacy team members. By improving their skills and knowledge, we aimed to enhance the service provided to patients with migraine. Additionally, we sought to raise public awareness about migraine presentation and available resources, emphasising the role of community pharmacies in supporting migraine management.
Methods: The project involved several key steps:
Needs Assessment: Focus groups and surveys were conducted with people living with migraine and pharmacists to shape the project’s direction.
Resource Development: An interactive online learning module with patient videos was created providing essential information for pharmacy teams.
Training Sessions: Four live training sessions were conducted for pharmacy teams. These sessions covered accurate assessment, effective support, and proper management of migraine cases. A follow up virtual session was held 3 months after the last training session to reinforce knowledge and provide a further opportunity for questions.
Patient Literature: Patient resources linked to a QR code were developed for both pharmacies and GP practices.
Public Awareness Campaign: Radio adverts, billboards, and bus posters were used to raise awareness about migraine and the role of community pharmacies.
Results:
Training Attendance: Attended by 73 pharmacy team members, including 33% of community pharmacists working in the health authority area.
Online Module: 253 engagements
Improved Confidence: Qualitative feedback from pharmacy teams indicated increased confidence in managing people with migraine.
Patient Engagement: A public webinar, during the awareness campaign, had 463 attendees and 416 YouTube views within 24 hours.
Increased Discussions: An initial patient survey, advertised to health authority employees, had 162 responders of whom 14% had discussed migraine with a pharmacist. The survey was sent to all those signed up to the patient webinar; of 59 responding, 53% had discussed migraine with a pharmacist. After the webinar attendees were asked to complete the survey again; of 205 responding 91% expressed willingness to consider such discussions.
Conclusion: Partnering with pharmacy teams enhances migraine management. By providing targeted resources, training, and public awareness campaigns, we can improve patient outcomes. Looking ahead, phase 2 aims to embed these changes and expand the project to other health authorities, fostering a collaborative approach to migraine care.
EP.10
Beyond Genetics: The Role of Familial Comorbidities in Shaping Migraine Phenotypes
T Ozdemir Gultekin1, S Eyupoglu2, E Uluduz3, D Uluduz4 and A Ozge5
1Baskent University Istanbul Hospital, Istanbul, Turkey
2Brain 360, Integrative Brain Health Center, Istanbul, Turkey
3Koc University Medical Faculty, Istanbul, Turkey
4Istanbul University, Cerrahpasa Medical Faculty, Istanbul, Turkey
5Mersin University, School of Medicine, Mersin, Turkey
Objective: Migraine is a highly disabling neurological condition with substantial variability in its clinical presentation. This study aims to explore the influence of familial transmission of comorbid medical conditions on the phenotype of chronic and episodic migraine.
Methods: A total of 500 patients from a private tertiary headache clinic were categorized into episodic and chronic migraine based on the International Classification of Headache Disorders-3 criteria. Data on demographics, clinical symptoms, and familial medical history were collected. Statistical analysis included Chi-square and independent sample t-tests to evaluate the impact of familial comorbidities on migraine types.
Results: Of the participants, 63% were diagnosed with episodic migraine and 37% with chronic migraine. Significant findings included higher rates of medication overuse (63.31%) and allodynia (58.82%) in chronic migraine patients. Notably, patients with a maternal history of hypercholesterolemia showed a higher prevalence of chronic migraine (78.6%), whereas those with both parents affected tended to have episodic migraine. Educational levels are inversely correlated with chronic migraine prevalence, suggesting a socioeconomic influence on migraine chronification.
Conclusion: This study highlights significant associations between familial health conditions and the type of migraine. The findings suggest that maternal transmission of comorbidities, particularly hypercholesterolemia, may influence the development of chronic migraine. These results underscore the importance of considering familial medical history in the management and understanding of migraine.


EP.11
Exploring the Gut-Brain connection: Characterization of the Gut Microbiome in Migraine Patients and Its Impact on Headache Management
C Mugo1, E Church1, R Horniblow1, H Botfield1, S Mollan2, A Sinclair1, L Hill1 and O Grech1
1University of Birmingham, Birmingham, United Kingdom
2Department of Ophthalmology, University Hospitals Birmingham NHS Foundation Trust, UK, Birmingham, United Kingdom
Background: Migraines, characterized by throbbing head pain, may occur with or without aura. While treatments focus on managing symptoms and preventing further episodes, excessive dependence on acute therapies can lead to medication overuse. Therefore, finding non-pharmaceutical treatments which may prevent the development or severity of migraine is of interest. Emerging evidence has suggested there is involvement of the gut-brain axis’ in migraine, where the microbiota may influence brain function via stimulation of the vagus nerve or neurotransmitter release. Conversely, the central nervous system can regulate the gut microbiota through the sympathetic and parasympathetic systems and secretion of neuroendocrine peptides. Migraine is often associated with gastrointestinal disorders, pointing to shared root causes. Diet has been identified as a key trigger for some, with noticeable differences in migraine frequency and severity linked to various dietary patterns.
Objective: We conducted a systematic review which aimed to characterise the gut microbiota of migraine patients and explore the therapeutic benefit of altering the gut phenotype on migraines.
Methods: Embase, PubMed, and the Cochrane Library were systematically queried using specific terms found in titles and/or abstracts, including variations of ‘migraine’ or ‘headache’ and terms related to the gut microbiome such as ‘gastrointestinal microbiome,’ ‘microbiota,’ ‘bacterial flora,’ ‘probiotics,’ ‘prebiotics,’ and ‘Synbiotics.’ The databases were searched since inception to January 29, 2024. Covidence software was employed to filter studies using precise inclusion and exclusion criteria, and the NIH quality assessment tools were used to determine risk of bias. The analysis included data on gut bacterial abundance, exploring its links to migraine risk and clinical features, as well as the effectiveness of Gut Microbiota-Targeted Therapies in individuals with migraines.
Results: Out of the 529 relevant studies identified, 16 studies were included in this review, ranging from ‘Good’ to ‘Poor’ quality. The abundance of 75 bacterial taxa significantly differed between migraineurs and controls. Additionally, 45 bacteria significantly correlated to migraine risk and 5 significantly correlated to migraine clinical characteristics. Studies revealed significant microbial differences between migraine and healthy individuals. Bacteroidetes, Proteobacteria, and Firmicutes phyla groups were notably abundant in migraine patient groups. However, studies presented conflicting findings regarding the abundance of Actinobacteria and Clostridia in relation to increased migraine risk among migraineurs. Synbiotic and synbiotic/probiotic therapies which aimed to target the gut microbiota resulted in significant reductions in migraine frequency, duration, and painkiller consumption. The effectiveness of probiotics in reducing the duration, severity, and frequency of migraines however varied across different studies.
Conclusion: The evidence indicates that individuals with migraines often exhibit altered compositions of the gut microbiome, suggesting a significant biological linkage between gut health and migraine occurrence. This alteration in the gut microbiota not only correlates with increased migraine risk but also impacts clinical manifestations of the condition. Given these findings, targeting the gut microbiome through specific therapies presents a promising avenue for effectively managing and potentially alleviating migraines. By focusing on restoring or modifying the gut microbiome, gut microbiome targeted therapies may reverse the effects of an altered gut microbiome composition in migraineurs.
EP.12
Continuous exposure to sumatriptan enhances neuronal activity within the trigeminal vascular system in rats
M De Felice1, J Hall1 and F Boissonade1
1University Of Sheffield, Sheffield, United Kingdom
Introduction: Migraine is an incapacitating collection of neurological symptoms. Migraine remains poorly understood, despite being the third most common and disabling disease in the world, with a global prevalence of 10%.
Trigeminovascular-mediated central sensitization has been implicated in the development of migraine symptoms. In addition to severe headache these include pain following light touch (cutaneous allodynia, observed in most patients during migraine), and is believed to underlie: the progression of migraine pain; the relative resistance to some medications (including triptans); and critically the transformation from an episodic to a chronic, more disabling disorder known as chronic migraine.
Objectives: Using a clinically-relevant model of migraine that uses continuous sumatriptan administration to induce medication overuse headache and a migraine-like state, we investigated the hypothesis that the appearance of migraine symptoms, such as the development of facial allodynia and increased responses to migraine triggers, are associated with peripheral and central sensitisation of the trigeminovascular system.
Methods: The trigeminal ganglion (TG) and trigeminal nucleus caudalis (TNC) were isolated from rats following subcutaneous infusion with sumatriptan or saline (over a period of 6 days), either on the last day of infusion (day 6) or on day 20 (from the start of infusion). On day 20 a subgroup rats was treated with sodium nitroprusside (a nitric oxide donor known to trigger migraine in humans) prior to tissue collection. Tissues were immunohistochemically labelled using antibodies to identify known biomarkers of neuronal and glial activation and specific cell types (pERK, pp38, Iba-1, GFAP and NeuN).
Results: An increase in biomarker expression was observed in sumatriptan-infused rats in both the TG and TNC at day 6 and day 20. In the TNC, this expression was localised to areas known to be involved in nociceptive processing in migraine. Labelling for pERK and pp38 displayed a shift in expression from neurones (on day 6) to glia (on day 20), implicating a role for both of these cell types in migraine.
Conclusions: Continuous sumatriptan administration causes increased expression of markers of altered excitability in neuronal and glial cells in both the TG and TNC. This suggests that both peripheral and central sensitisation of the rat trigeminovascular system are involved in the pathophysiological mechanism underlying migraine and medication overuse headache pathophysiology.
EP.13
A head to head cohort study on the effiacy and safety of Indomethacin and Ibuprofen for the acute treatment of migraine
C Giannini, S Braca, C Russo, G Cretella, A Stornaiuolo and R De Simone
Introduction: Indomethacin, a non-steroidal anti-inflammatory drug (NSAIDs) which acts by inhibiting both ciclo-oxygenase (COX) and nitric-oxyde synthase (NOS) is extensively used for the treatment of migraine. This coupled mechanism of action could account for an increased therapeutic potential. However, no head-to-head studies have been performed with other NSAIDs for migraine acute treatment. Ibuprofen is an established symptomatic migraine treatment, belonging to the same NSAIDs category while not exerting effects on nitric oxyde pathway. Therefore, we aimed to compare indomethacin and ibuprofen for the treatment of migraine patients.
Methods: This is a prospective observational cohort study comparing the effectiveness and safety of Ibuprofen and Indomethacin. We enrolled 104 consecutive patients who were randomized either to Indomethacin 50 mg or Ibuprofen 600 mg. We evaluated, over 10 migraine attacks, the reduction in pain two hours after drug administration using a visual analog scale (0 = no pain; 10 = highest pain). We also recorded side effects occurrence.
Results: We observed a mean reduction in pain intensity of - 4.39 (IC95% −3.6, − 5.14) in the indomethacin group, which proved significant when compared to the Ibuprofen group (−3.1; IC95% – 2.49, – 3.71) group (p < 0.05). There were no statistically significant differences in terms of mild adverse events between the two groups (p > 0.05).
Conclusion: Our findings suggest that Indomethacin could be more effective than Ibuprofen in treating migraine attacks.
Image 1

EP.14
Cardiovascular and Cerebrovascular Events During Treatment of Migraine with Rimegepant: Analysis of Post-Authorization Safety Data
A Chan1, R Fountaine2, R Pawinski3, G Pixton2 and E Straghan3
1Pfizer Healthcare Ireland, Dublin, Ireland
2Pfizer Research and Development, Groton, USA
3Pfizer Ltd, Tadworth, UK
Introduction: Rimegepant is a small molecule calcitonin gene-related peptide (CGRP) receptor antagonist indicated for the acute treatment of migraine with or without aura, and the preventive treatment of episodic migraine in adults. Rimegepant was approved 27 February 2020 (USA), 25 April 2022 (EU), and is currently approved in 68 countries. All new medicines are required by regulatory agencies such as the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) to have ongoing safety monitoring. Standard routine ongoing pharmacovigilance requirements include periodic safety update reports (PSURs) to monitor the product’s benefit-risk balance. PSURs include post-marketing reports of adverse drug reactions from all countries where rimegepant is licensed, as well as other data sources, such as clinical trials. Post-marketing data include spontaneous sources (serious and non-serious adverse reactions from spontaneous individual case safety reports, including reports from healthcare professionals, patients, scientific literature, and regulatory authorities, irrespective of the causality assessment made by the reporter) and solicited sources (serious adverse reactions from non-interventional studies and solicited reports of serious adverse reactions). Reports of cardiovascular and cerebrovascular events were included in each rimegepant PSUR upon regulatory request.
Objective: This real-world analysis of post-authorization safety data assessed the incidence over time in the occurrence of cardiovascular and cerebrovascular events among individuals taking rimegepant, using post-marketing data obtained from rimegepant PSURs which utilized similar methodology.
Methods: Post-marketing reports of adverse drug reactions categorized as cardiovascular or cerebrovascular were extracted from the four rimegepant 6-monthly PSUR reports covering the 2-year period 27 February 2022 through 26 February 2024. The events were coded using Medical Dictionary for Regulatory Activities (MedDRA) version 25.0 through 26.1 and categorized using Standardized MedDRA Queries (SMQs) for cardiovascular events and cerebrovascular events. Data originating from clinical trials were not included in this analysis.
Results: Exposure to rimegepant was estimated to be 305,632 patients during the first 6-month interval and 35,999 patient-years in the fourth 6-month interval (Table 1). Over the 2-year period, there were 78 patients with cardiovascular events and 27 patients with cerebrovascular events identified from post-marketing data sources (Table 1). Incidence of reported cardiovascular and cerebrovascular events remained stable and very low during the 2-year period.
Conclusions: There was no new safety signal for cardiovascular or cerebrovascular events associated with rimegepant during the 2-year period. Routine pharmacovigilance is ongoing, including a Post Authorization Safety Study in patients with cardiovascular disease. With the favourable cardiovascular and cerebrovascular safety profile, the latest Pharmacovigilance Risk Assessment Committee assessment at EMA has requested monitoring requirements for rimegepant to be eased from bi-annual to annual PSURs, with no need for cardiovascular and cerebrovascular safety data presentation unless the benefit-risk profile changes. Funded by Pfizer.

EP.15
Characteristics of people with migraine using rimegepant in the 2023 U.S. National Health and Wellness Survey
M Lewis1, A Jenkins2, J Cirillo1, K Hygge Blakeman3, L Abraham2, J Brown1 and J Ailani4
1Pfizer, Inc, New York, USA
2Pfizer, Ltd, Tadworth, UK
3Pfizer AB, Stockholm, Sweden
4Department of Neurology, Medstar Georgetown University Hospital, Washington, USA
Introduction: Rimegepant is the only migraine medication indicated for both the acute treatment and prevention of migraine, but little is known regarding real-world rimegepant users. This analysis described the demographic and migraine-associated characteristics of people with migraine (PwM) using rimegepant.
Objectives: To describe characteristics of PwM who reported rimegepant use in the 2023 U.S. National Health and Wellness Survey (NHWS).
Methods: This retrospective, cross-sectional study used data from the 2023 US NHWS (Oracle Life Sciences). NHWS captured patient-reported information on demographic and health information. Adults that self-reported migraine also completed a migraine-specific module capturing detailed migraine treatment and disease characteristics. Those that reported current use of rimegepant were included for this descriptive analysis of demographics, comorbid conditions, migraine frequency and severity, and current treatments. Use of rimegepant as an acute or preventive treatment was not captured in the 2023 survey.
Results: Among 8,439 (weighted sample 29 million) adults in the US who reported having diagnosed migraine, 186 reported current rimegepant use. The mean (standard deviation (SD)) age was 43.2 (13.4) years and 90.9% were female. Additional demographic characteristics showed 72.0% white, 5.9% black, and 14.5% Hispanic race/ethnicity as well as 55.4% married/living with a partner and 56.5% were employed. The majority (57.0%) reported no Charlson comorbidities but 58.1% had ≥1 cardiovascular (CV) risk factors (high blood pressure, high cholesterol, current smoker, type 2 diabetes, obesity), with 33.3% having ≥2 CV risk factors. Additionally, the combined prevalence of specific CV diseases (angina, arrhythmias, heart failure, heart attack, cerebrovascular disease, peripheral vascular disease, and angina) was 19.9%.
Migraine specific measures showed mean (SD) monthly migraine days (MMD) of 6.4 (7.2) with 49.5% of rimegepant users reporting ≥4 MMDs. Among women, 37.3% reported their migraines were associated with their menstrual cycle. Using the Migraine Disability Assessment Test (MIDAS), 44.6% reported severe disability and 33.9% reported mild/moderate disability.
All rimegepant users reported use of both acute and prevention migraine treatments. The most common acute co-treatments reported included non-steroidal anti-inflammatory drugs (23.1%) and triptans (21.5%) as well as prevention agents such calcitonin gene-related peptide monoclonal antibodies (22%) and anti-convulsants (15.1%). Using a 7-item Likert scale, 86.6% of rimegepant users reported being satisfied with their current rimegepant treatment.
Conclusions: Rimegepant users captured in the 2023 US NHWS reported a high rate of treatment satisfaction. The high level of migraine frequency and disability suggests rimegepant users are a relatively severe migraine population. Nearly half of all rimegepant users had pre-existing conditions that may make them inappropriate for acute standards of care (triptans) and more likely to use novel migraine treatments. More data are needed to understand the patient journey in migraine, as well as information on specific use (acute or prevention) of rimegepant.
EP.16
Effectiveness and tolerability of lasmiditan as acute migraine treatment (DART): a real-world multicentric study
G Vaghi1,2, R De Icco1,2, L Iannone3, M Corrado1,2, A Burgalassi3, E De Matteis4, F De Santis4, C Fasano3, E Piella5, M Romozzi6, G Sebastianelli7, G Avino8, S Cevoli9, G Coppola7, G Dalla Volta10, A Granato11, F Boscain12, E Mampreso12, R Ornello4, F Pistoia4, I Rainero13, M Trimboli14, A Russo15, M Valente16, C Vollono17 and C Tassorelli1,2
1Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
2Headache Science & Neurorehabilitation Unit, IRCCS Mondino Foundation, Pavia, Italy
3Headache Centre and Clinical Pharmacology Unit, Careggi University Hospital Florence, Florence, Italy
4Department of Biotechnological and Applied Clinical Sciences, University of L'Aquila, L'Aquila, Italy
5Department of Neurosciences “Rita Levi Montalcini”, University of Torino, Torino, Italy
6UOC Neurologia, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
7Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome Polo Pontino ICOT, Latina,
Italy
8Ospedale di Prato Santo Stefano, Prato, Italy
9IRCCS Istituto delle Scienze Neurologiche Bologna, Bologna, Italy
10Headache Centre of Istituto clinico città di Brescia (gruppo SAN DONATO, Brescia, Italy
11Azienda Ospedaliero-Universitaria di Trieste, Trieste, Italy
12Headache Centre, Neurology - Euganea Health Unit, Padua, Italy
13Headache Center, Department of Neuroscience, University of Torino, Torino, Italy
14Centro Interaziendale Cefalee, Azienda Ospedaliero-Universitaria Renato Dulbecco, Catanzaro, Italy
15Department of Advanced Medical and Surgical Sciences, University of Campania “Luigi Vanvitelli”, Naples, Italy
16Azienda Sanitaria Universitaria Friuli Centrale, Presidio Ospedaliero Santa Maria della Misericordia, Udine, Italy
17Department of Neurosciences, Università Cattolica del Sacro Cuore, Rome, Italy
Introduction: Lasmiditan, a serotonin 5-HT1F receptor agonist, has been recently approved in Italy for the acute migraine treatment.
Objectives: We designed a prospective multicentric study to evaluate lasmiditan effectiveness and tolerability in the real-world setting (NCT05903040).
Methods: We enrolled 55 patients from 13 Italian headache centers: 87.3% females, 45.4 ± 14.4 years, 21.8% (n = 12) with chronic migraine (CM), 9.1 ± 7.2 baseline monthly migraine days. Patients were instructed to treat up to four migraine attacks with lasmiditan 50 mg (20.4%) or 100 mg (79.6%). Using an ad hoc diary, we prospectively collected migraine-attack features every 30 minutes after lasmiditan administration, up to 2 hours (2 h).
Results: Preliminary analyses were conducted on 38 first-treated attacks (10/38 in a CM patient) and 81 total attacks. When considering all treated attacks, 37% (30/81) of patients rated migraine intensity as severe at lasmiditan intake on a 0-3 rating scale. Pain freedom 2 h post-dose was reported in 42.1% (16/38) of first-treated attacks, and in 40.7% (33/81) of total attacks. The rate of pain freedom was not influenced by timing of lasmiditan intake (p = 0.154), while it was negative influenced by higher baseline pain severity (p = 0.048). Freedom from the most bothersome symptom 2 h post-dose was reported in 44.4% (36/81) of attacks.
All the 38 patients who reported data for the first attack have previously used triptans. When compared to triptan use, 42.10% (16/38) of them declared a better effectiveness of lasmiditan, mainly related to a faster onset of action.
Adverse events were reported in 33 (46.5%) of the total treated attacks and 17 (44.7%) of first treated attacks. They were predominantly: dizziness (n = 12), fatigue (n = 10) and paraesthesia (n = 6). Tolerability was rated as good-to-excellent in 50% of cases.
Conclusion: Our real-world data support lasmiditan effectiveness in the acute treatment of migraine. Adverse events were reported in 46.5% of attacks.
EP.17
Efficacy and Safety of Rimegepant 75 mg for Acute Treatment of Migraine: A Pooled Analysis of 4 Randomized, Placebo-Controlled Trials
S Tepper1, J Pavlovic2, S Yu3, R Lipton2, G Pixton4, Y Zou5, R Fountaine4 and D Semel6
1The New England Institute for Neurology and Headache, Stamford, United States
2Albert Einstein College of Medicine and Montefiore Headache Center, Bronx, United States
3PLA General Hospital, Beijing, China
4Pfizer Inc., Groton, United States
5Pfizer Inc., Shanghai, China
6Pfizer Inc., New York, United States
Introduction: Rimegepant is an oral small molecule calcitonin gene-related peptide receptor antagonist approved for acute treatment of migraine (with and without aura) and preventive treatment of episodic migraine in adults.
Objective: To summarize the efficacy and safety of rimegepant for acute treatment of migraine using pooled data from four randomized, placebo-controlled trials (NCT03235479, NCT03237845, NCT03461757, NCT04574362).
Methods: Participants were aged ≥18 years and had a ≥ 1-year history of migraine, 2–8 migraine attacks of moderate or severe pain intensity per month, and attacks lasting 4–72 h if untreated. Participants were provided a single dose of rimegepant 75 mg or placebo to treat a single migraine attack of moderate or severe pain intensity within the next 45 days. Preventive migraine medications were permitted if dosing was stable for ≥3 months prior to screening. Rescue medication (aspirin, ibuprofen, acetaminophen up to 1,000 mg/day, NSAIDs, antiemetics, or baclofen) was allowed 2 hours post-dose. Standard-of-care migraine treatments were allowed 48 hours post-dose. Co-primary endpoints at 2 hours post-dose were pain freedom and freedom from the most bothersome symptom (MBS). Secondary endpoints were pain relief at 2 hours post-dose, return to normal function at 2 hours post-dose (among those with disability at migraine onset), use of rescue medication within 24 hours post-dose, and sustained pain freedom from 2–24 and 2–48 hours post-dose. These secondary endpoints were chosen since they were key secondary endpoints in the most recently completed study of rimegepant for acute treatment of migraine (NCT04574362). Treatment comparisons utilized Mantel-Haenszel risk estimation with stratification by study and prophylactic migraine medication use randomization stratum (sustained pain freedom endpoints used stratification only by study); p values are nominal. On-treatment adverse events (AEs) were also assessed.
Results: Overall, 4,895 participants received rimegepant (N = 2,439) or placebo (N = 2,456). For the co-primary endpoints, the proportion of participants with pain freedom 2 hours post-dose (20.0% vs 11.8%; p < 0.0001) and MBS freedom 2 hours post-dose (40.2% vs 29.2%; p < 0.0001) was higher in the rimegepant group than in the placebo group (Table). Rimegepant was also superior to placebo on secondary endpoints of pain relief at 2 hours post-dose (60.3% vs 45.1%; p < 0.0001), return to normal function at 2 hours post-dose (33.5% vs 21.1%; p < 0.0001), rescue medication use within 24 hours post-dose (15.5% vs 28.9%; p < 0.0001), sustained pain freedom from 2–24 hours post-dose (14.5% vs 7.1%; p < 0.0001), and sustained pain freedom from 2–48 hours post-dose (12.6% vs 6.4%; p < 0.0001). AEs were reported in 11.1% and 9.6% of participants in the rimegepant and placebo groups, respectively. The only AE reported in >1% of participants was nausea (rimegepant = 1.4%, placebo = 1.3%). Severe AEs occurred in 0.3% and 0.1% of participants in the rimegepant and placebo groups, respectively. Serious AEs occurred in 0.1% of participants in both groups; none were deemed related to study treatment.
Conclusions: In this pooled analysis of four randomized placebo-controlled trials, a single dose of rimegepant 75 mg demonstrated efficacy and a favorable safety profile for the acute treatment of a migraine attack with moderate or severe pain.

EP.18
Long-term safety and discontinuation for rimegepant versus triptans: A matching-adjusted indirect comparison
L Powell1, C de Brún1, B Rogula1, A Jenkins2, J Atkinson2 and L Abraham2
1Broadstreet HEOR, Vancouver, Canada
2Pfizer Ltd, Tadworth, United Kingdom
Introduction: Rimegepant 75 mg (Nurtec), an oral calcitonin gene-related peptide antagonist, was approved for the acute treatment of migraine with or without aura in adults in China in January 2024 (many countries also have a preventive indication). In China, triptans are the most relevant comparator to rimegepant for the acute treatment of migraine. Although efficacy may be similar, rimegepant could offer tolerability and safety advantages. However, comparative evidence on the long-term safety and tolerability of as needed (PRN) rimegepant versus triptans is lacking.
Objectives: The aim of this analysis was to compare discontinuation and adverse events (AEs) over 12-months of open-label PRN use for rimegepant and triptan-treated subjects using a matching-adjusted indirect comparison (MAIC).
Methods: Triptan open label extension or long-term safety trials were identified from the literature. Comparability to the PRN arms of the rimegepant trial (NCT03266588) was assessed with respect to patient characteristics, outcome definitions, and data availability.
A zolmitriptan long-term study (Cady et al., 1998) was selected based on the number of baseline covariates reported and similar safety outcome definitions; however, this study had variable duration of follow up due to early termination.
MAIC was performed in accordance with recommendations from the National Institute for Health and Care Excellence (NICE) Decision Support Unit (DSU), derived from the publication by Signorovitch et al. (2012). Proportions of categorical fields and means of continuous fields were matched. Individual patient data from BHV3000-201 were weighted to match the baseline covariates in the Cady et al. (1998) population (age, sex, history of aura, duration of migraine history, monthly migraine days, use of concomitant migraine preventive medications). Outcomes measured were discontinuation over 12 months (overall and due to AEs or lack of efficacy), and AEs (reported in both studies: dizziness, somnolence, paresthesia, nausea, and asthenia). For each outcome, odds ratios (ORs), relative risks, and risk differences (RDs) were estimated, with 95% confidence intervals (CIs).
Results: After MAIC weighting, the effective sample size of the rimegepant patients was 383.2 (25.3% of the original sample size), and their aggregate baseline characteristics matched those of the zolmitriptan population. Rimegepant was associated with a statistically significant lower risk of overall discontinuation than zolmitriptan (31.1% vs. 36.7%, OR: 0.8 [95%CI: 0.7, 0.9]; Table 1). Patients were less likely to discontinue rimegepant compared to zolmitriptan due to the following non-trial specific reasons: AEs (OR = 0.3 [0.2, 0.5]) and lack of efficacy (OR = 0.3 [0.2, 0.4]).
Compared to zolmitriptan, rimegepant patients had a reduced risk of experiencing all the following AEs: dizziness, somnolence, paresthesia, nausea, and asthenia. Though the most frequently experienced of these AEs for rimegepant was nausea (3.2%), the risk was still less than with zolmitriptan (15%; RD: −11.8 [−13.6, −10.0]).
Conclusion: Despite the bias against rimegepant due to shorter follow-up in the zolmitriptan study, these results suggest patients were less likely to discontinue rimegepant than zolmitriptan, both due to AEs or lack of efficacy, and also less likely to experience AEs of dizziness, somnolence, paresthesia, nausea, or asthenia over 12-months of PRN use.

EP.19
Rimegepant for the Acute Treatment of Migraine: A Phase 3, Multicenter, Open-label, Long-term Safety Study in Adults from China
S Yu1, L Ma2, Q Zhong2 and X Han2
1Chinese PLA General Hospital, Beijing, China
2Pfizer (China) Research and Development Co Ltd, China
Introduction: Rimegepant orally disintegrating tablet (ODT) is an oral small-molecule calcitonin gene-related peptide receptor antagonist for the acute treatment of migraine. Here we report the results of a phase 3, multicenter, open-label, single arm study to assess the long-term safety and tolerability of rimegepant 75 mg ODT for the treatment of acute migraine in Chinese adults (NCT05371652).
Objectives: The primary objective was to evaluate the long-term safety and tolerability of 75 mg Rimegepant ODT. Secondary objectives were to evaluate the number of migraine days and severity of migraine attacks during long-term treatment (LTT) with rimegepant ODT, relative to the Observation Period (OP).
Methods: Eligible participants had at least 1 year history of migraine (with or without aura) and a history of 6–18 moderate to severe migraine attacks per month ≤3 months prior to the screening visit, and ≥6 qualified migraine days during the OP. After the 30-day OP, participants could take rimegepant as needed (PRN, maximum of 1 tablet per day), at the onset of mild to severe migraine attack. The treatment phase of the study was 52 weeks.
Results: Of 330 screened adults, 241 were enrolled. Of the enrolled adults, 240 (99.6%) were treated, and 208 (86.3%) completed the study. Participants had a mean (SD) age of 39.1 (11.0) years and 192 (80.0%) were female. Mean age at migraine onset was 27.3 (9.7) years and all participants had experienced migraine for no less than 1 year prior to screening. The median (Q1, Q3) average rimegepant dose during LTT was 4.6 (3.1, 7.1) tablets per month. A total of 203 (84.6%) participants reported at least one treatment emergent adverse event (TEAE) during LTT, of which, 46 (19.2%) were evaluated by the investigator as being related to rimegepant. One participant experienced a TEAE of CTCAE grade ≥3, which was evaluated by the investigator as being related to rimegepant. There were no rimegepant-related serious AEs and no rimegepant-related TEAEs that led to treatment interruption or discontinuation. Most abnormal laboratory parameters were of Grade 1-2. For all migraine attacks, the mean reduction from the OP in the number of monthly migraine days (MMDs) was observed as early as the first 4 weeks (−1.7 [95% CI −2.2, −1.2]) with a trend of continued reduction over time to Month 11 (−5.7 [95% CI −6.3, −5.1]), followed with a plateau through Month 13. The mean monthly reduction across LTT was −4.4 (95% CI −4.9, −3.9) days.
Conclusions: Rimegepant demonstrated a favorable safety profile and was well tolerated in Chinese participants during the long-term acute treatment of migraine. In the manner of PRN use, reduction in the number of MMDs was observed as early as the first 4 weeks and continued to improve for 11 months with a maintained reduction through to the end of LTT.
EP.20
Treatment outcomes in people with migraine receiving rimegepant or triptans: a descriptive analysis from a real-world survey
L Abraham1, J Brown2, K Hygge-Blakeman3, F Dai2, J Jackson4, W Whitton4, S Barlow4 and L Hancock4
1Pfizer R&D UK Ltd, Tadworth, United Kingdom
2Pfizer, Inc., New York, United States of America
3Pfizer AB., Stockholm, Sweden
4Adelphi Real World, Bollington, United Kingdom
Introduction: Despite their wide usage as a first line prescription therapy for acute migraine treatment, for some PwM triptans are associated with clinical issues including cardiovascular (CV) contraindications, medication overuse headache, tolerability concerns, and insufficient efficacy. Rimegepant, an oral, calcitonin gene-related peptide receptor antagonist, is the only therapy approved for acute and preventive treatment of migraine. This analysis uses real-world data to assesses patients treated with rimegepant or triptans, presenting demographics, migraine-associated characteristics, and treatment outcomes.
Objective: To assess treatment outcomes of people with migraine (PwM) who use rimegepant or triptans to treat migraine attacks.
Methods: Patient and physician data were drawn from the Adelphi Migraine Disease Specific Programme (DSP)™, a real-world, cross-sectional survey with retrospective data collection of physicians and their consulting adult PwM in the USA, conducted in 2022. Physicians provided treatment practice data for the next 10 consecutively consulting PwM, including patient demographics, clinical characteristics, migraine treatments, reasons for treatment choice and treatment satisfaction. Patients provided data on consistency of response, treatment optimization, satisfaction and willingness to continue using treatment. To be included in this analysis, patients were receiving either rimegepant or a triptan as acute monotherapy.
Results: A total of 91 rimegepant and 437 triptan acute monotherapy users were included, of which patient-reported data was available for 29 and 103 rimegepant and triptan patients, respectively. Of the rimegepant users, n = 50 had received a triptan as their previous line of treatment.
Physician-reported consistency, defined as achieving pain freedom within 2 hours on more than half of occasions, was 73% for rimegepant users and 57% for triptan users. Patient-reported consistency of response, defined as achieving pain freedom within 2 hours for 4 or 5 out of 5 attacks, was 76% for rimegepant users and 63% for triptan users.
Almost nine out of ten patients receiving rimegepant (87%), and 62% of patients receiving a triptan, reported treatment optimization as defined by an MTOQ score >24.
For rimegepant users, 95% of physicians and 97% of patients reported satisfaction (extremely satisfied/satisfied) with current acute treatment. For triptan users, 87% of physicians and 78% of patients reported satisfaction with current acute treatment. Furthermore, 59% of rimegepant users, and 22% of triptan users, reported being ‘extremely satisfied’ (Figure 1); nearly all patients across groups reported a willingness to continue taking their prescribed acute treatment.
Physician-reported reasons for choosing rimegepant or triptans included pain freedom at 2 hours (78% and 50%), rapid return to function (67% and 46%), prolonged pain relief (44% and 27%), no need for a second dose (33% and 9%), efficacy in patients who had failed prior acute medications (51% and 14%), lower risk of medication overuse headache (44% and 9%), and suitable for patients with CV risk factors (34% and 3%).
Conclusions: Patients prescribed rimegepant monotherapy reported high satisfaction, response consistency, and treatment optimization. Physicians reported rapid return to function, durability of effect, and safety profile as key reasons for prescribing rimegepant. These data provide real-world evidence of the holistic value of rimegepant for the acute treatment of migraine.

EP.21
To describe the radiological features of patients with headache as a presenting symptom of neurosarcoidosis
A Ali1, S Mahmood, Y Sallowm1, L Schultz1 and M Cerghet1,2
1Henry Ford Health
2Michigan State University School of Medicine
Objective: To describe the radiological features of patients with headache as a presenting symptom of neurosarcoidosis.
Introduction: Neurologic complications occur in approximately 5%-10% of patients with sarcoidosis, and approximately 50% of these patients have neurologic deficits at the time sarcoidosis is first diagnosed. A wide spectrum of central and peripheral nervous system clinical manifestations may be observed, including cranial nerve palsies, sensory and/or motor deficits, and headache. MRI results in patients with neurosarcoidosis may include abnormal contrast enhancement, structural masses, and demyelinating lesions.
Methods: This single center retrospective cohort study assessed patients who were diagnosed with neurosarcoidosis in an urban tertiary care center between 1995 and 2016. We included patients who had MRI results at the time of diagnosis. Patients were divided into two groups based on presence or absence of headache as a presenting symptom. The MRI result of meningeal contrast enhancement was reviewed.
Results: Of the 110 patients analyzed, 30 (27.3%) had an initial presenting symptom of headache while 80 (72.7%) did not. Patients with headache had a higher proportion of meningeal contrast enhancement on MRI (66.7% (20/30) vs 25.0% (20/80); p < 0.001) and leptomeningeal involvement (53.3% (16/30) vs 7.5% (6/80), p < 0.001) compared to patients with no headache. Although they had a lower proportion of spinal cord localization (13.8% (4/29) vs 34.2% (26/76), p = 0.038) and intraparenchymal CNS involvement (16.7% (5/30) vs 51.3% (41/80), p = 0.001) compared to patients with no headache.
Conclusion: Patients with neurosarcoidosis who present with headache as an initial symptom had a higher proportion of meningeal contrast enhancement seen by MRI than patients who present with other neurological symptoms. This suggests a clinico-radiologic link between headache and meningeal disruption in patients with neurosarcoidosis.

EP.22
Evaluation of the effectiveness of external stimulation of the trigeminal nerve in the treatment of chronic tension-type headache
D Turakulova1, E Mirdjuraev and L Shadmanova
1Center for the development of professional qualification of medical workers, Tashkent, Uzbekistan
Background and Aims: Chronic tension-type headache (CTTH) represents a significant global health burden, affecting individuals across diverse demographic groups and exerting substantial socioeconomic impacts. Muscular factors play a significant role in the pathophysiology of CTTH. Additionally, psychological factors, such as stress, anxiety, and depression, are commonly associated with CTTH and may contribute to its pathophysiology. The aim of this study was to evaluate the effectiveness of external trigeminal nerve stimulation using the Cefaly device (CEFALY Technology, Belgium) in the treatment of CTTH with a focus on muscle relaxation and stress relief.
Methods: A prospective study was conducted involving patients aged 18–60 diagnosed with CTTH, as per the International Classification of Headache Disorders-3 (ICHD-3) criteria. Participants were divided into two groups: one receiving standard pharmacological treatment alone (n = 56) and another receiving pharmacological treatment combined with therapy using a Cefaly device (n = 56). The intervention group underwent 40-minute therapy sessions with the Cefaly device three times a week for 8 weeks. Validated questionnaires, such as the Headache Impact Test (HIT-6) and the Perceived Stress Scale (PSS), were utilized to assess reductions in headache severity, medication consumption, and improvements in quality of life and psychoemotional well-being. Statistical analyses, including descriptive and inferential statistics, were employed to compare outcomes between the two groups, adjusting for potential confounders.
Result: The study included 112 participants with CTTH, evenly divided into two groups: standard pharmacological treatment alone (n = 56) and pharmacological treatment combined with therapy using a Cefaly device (n = 56). After 8 weeks of treatment, the combination treatment group showed a significant reduction in headache severity compared to the standard treatment group (p < 0.05). Medication consumption for headache management also decreased significantly in the combination treatment group (p < 0.05). Additionally, participants in the combination treatment group reported greater improvements in quality of life, as evidenced by significantly lower scores on the Headache Impact Test (HIT-6) (p < 0.05) and reduced perceived stress levels measured by the Perceived Stress Scale (PSS) (p < 0.05). Statistical analysis was performed using paired t-tests or Wilcoxon signed-rank tests for within-group comparisons and independent t-tests or Mann-Whitney U tests for between-group comparisons. Adjustments for potential confounders were made using multivariate regression analysis.
Conclusion: These findings highlight the potential of adjunctive therapy with Cefaly devices to enhance treatment outcomes and alleviate the burden of CTTH on affected individuals. Further research is warranted to explore the long-term effects and mechanisms underlying the observed benefits, as well as to optimize treatment protocols for maximal efficacy and patient satisfaction. Nonetheless, our study underscores the importance of adopting a multimodal approach to headache management, incorporating both pharmacological and non-pharmacological interventions to improve patient outcomes and quality of life.
EP.23
10 year outcome on patients receiving onabotulinumtoxinA therapy for CM prophylaxis. A real-life data on 436 patients from Hull (UK) headache clinic
F Ahmed1,2,3, R Khan1, S Dorsey1,3, H Delrosario1 and M Khalil3
1Hull University Teaching Hospitals Nhs Trust, Hull, United Kingdom
2Hull York Medical School, Hull, United Kingdom
3Spire Hospital Hull and East Riding, Hull, United Kingdom
Background: CM is defined as headaches on > 15 days/month for > 3 months of which > 8 days meet criteria for migraine with or without aura or respond to migraine-specific treatment, affects 2% of the general population and is the most disabling form of the disorder with substantial impact on quality of life. OnabotulinumtoxinA (Botox) has been used as preventive therapy for Chronic Migraine (CM) since 2010. In the UK, it is used in adult patients with CM provided patient had failed at least three first line therapies and medication overuse is addressed.
Objective: We report ten year outcome on a large cohort of patients treated with onabotulinumtoxinA at the Hull headache clinic (UK)
Methods: Adult patients receiving OnabotulinumtoxinA for CM at the Hull Migraine Clinic (UK) were followed up prospectively. All patients had tried and failed at least one preventive therapy. OnabotulinumtoxinA was delivered as per the PREEMPT study protocol. Patients were asked to maintain a headache diary at least a month prior to and continuously after receiving onabotulinumtoxinA. Data was extracted for headache days (HD), migraine days (MD), headache-free days (FD), analgesic consumption including triptan and HIT 6 at every visit and one month following treatment. 10 year outcome is extracted for patients who commenced treatment between July 2010 and April 2014. NICE and Hull criteria were applied to evaluate responder. The treatment was stopped if the patient did not respond to first two cycles (negative stopping rule) or if patient stopped responding to any two consecutive cycles at subsequent visits (resistance) or if the patient had achieved < 8 days of headaches for any three consecutive months (positive stopping rule) and recommenced if the monthly headache days exceeded ten/month for at least three months following stoppage. Patients with medication overuse were included in the audit.
Results: 437 patients (360F 77 M) aged 45 (range 14-79) were audited. 425 (97.2%) had failed three treatments. 262 (222F 40 M) responded and continued to cycle 3. 175 (145F 30 M) stopped as per negative rule.
At 10 year follow up 82 (31.2%) patients were still on treatment of whom 47 never stopped treatment while 35 did stop at some stage and restarted. 38(14.5%) patients became refractory after an initial response and commenced other treatments including the CGRP MAB. 42 (16%) switched to CGRP MAB though they were still getting good response. 8 stopped due to pregnancy. 21 were lost to follow up. 71 (27.1%) remained in remission of which 38 commenced CGRP MAB for episodic migraine.
Conclusion: We report 10 year outcome data on a large cohort of patients receiving onabotulinumtoxinA therapy for CM at the Hull headache clinic. Some patients still prefer onabotulinumtoxinA in spite of availability of new therapies.
EP.24
Average steps per day as marker of treatment response in adults with chronic migraine
F Jantzen1, B Chaudhry1, S Younis1, I Nørgaard1, C Cullum1, T Do1, D Beier1 and F Amin1
1Danish Headache Center, Copenhagen, Denmark
Background: Physical activity can worsen migraine, leading to reduced activity levels in adults with chronic migraine. This study has investigated the change in average steps per day, as a surrogate marker of physical activity, in adults with chronic migraine successfully treated with monoclonal antibodies against calcitonin gene-related peptide or its receptor.
Methods: Data were obtained from adults with chronic migraine, who were classified as responders to preventive treatment with monoclonal antibodies. The primary endpoint was the difference in mean number of steps per day between the 3-months prior to treatment initiation and the first 3-months after treatment initiation. The secondary endpoint was the correlation between the change in steps per day and the change in monthly migraine days.
Results: Twenty-two (20 females) participants were enrolled with a median age of 48.5 years. The median number of steps per day increased from 4,421 at baseline to 5,241 after treatment (P = 0.039). We found a positive correlation between the increase in steps per day and the treatment response (P = 0.013).
Conclusions: Increase in physical activity, based on steps per day, positively correlated with treatment response to monoclonal antibodies. Automatically registered data on daily step count might be used to monitor physical activity as a response to preventive treatment in adults with chronic migraine.
EP.25
Blood pressure in migraine patients undergoing treatment with CGRP monoclonal antibodies in patients with migraine: a systematic review and practical recommendations
B van der Arend1, F van Welie1, M Olsen3, J Versijpt4, A Maassen van den Brink2 and G Terwindt1
1Leiden University Medical Center, Leiden, Netherlands
2Erasmus MC, Rotterdam, Netherlands
3Holbæk Hospital, Holbæk, Denmark
4University Hospital Brussels, Brussels, Belgium
Background: Monoclonal antibodies targeting Calcitonin Gene-Related Peptide or the CGRP-receptor have revolutionized the prevention of migraine. Despite their effectiveness, worries have surfaced regarding potential unwanted cardiovascular effects linked to CGRP's vasodilation function, suggesting a potential influence on blood pressure (BP).
Methods: Studies were systematically retrieved from PubMed, CDSR, WoS, MEDLINE, and EMBASE up to 1 May 2024. We focused on randomized controlled trials and observational cohort or case-control studies examining the impact of anti-CGRP-mAbs compared to control treatments on BP in patients with migraine. Two reviewers independently conducted study selection, data extraction, and risk of bias assessment.
Results: The literature search yielded 693 articles. After removing duplicates and conducting screening, 22 full-text articles were evaluated with only four studies meeting the inclusion criteria. Among these, only one study had a low risk of bias and reported elevated BP following initiation of anti-CGRP-mAb treatment.
Conclusions and recommendations: Despite the current limited evidence, clinicians are urged to monitor BP of migraine patients undergoing treatment with anti-CGRP-mAbs. The dearth of evidence seems to be linked to a continuing lack of awareness regarding the increased risk of cardiovascular events in migraine. It is advisable to prioritize (remote) BP monitoring to ensure intervention if needed.
Figure


EP.26
Comprehensive Assessment of Erenumab Efficacy in Participants with High Frequency Episodic Migraine with at Least One Previously Failed Preventive Treatment: the EMBRACE Study
G da Silva Lima1, R Rao2, G Szabó3, S Szklener4, C Tassorelli1, A Khodavirdi1, M Chehrenama1, A Bhatia1, Y Zhu1 and D Dodick6,7
1Amgen Inc., Thousand Oaks, USA
2Azienda Socio Sanitaria Teritoriale Spedali Civili di Brescia, Brescia, Italy
3Óbudai Egészségügyi Centrum, Budapest, Hungary
4NZOZ Neuromed M i M Nastaj Spolka Partnerska, Poland
5IRCCS Fondazione C Mondino, Italy
6Department of Neurology, Mayo Clinic, Scottsdale, US
7Atria Academy of Science and Medicine, New York, US
Introduction: Monthly migraine day (MMD) has been used to define migraine classification, clinical management of migraine, and efficacy of preventive treatment. MMD reduction though often associated with improvements of migraine-related impairments, only partially captures therapeutic benefit of migraine treatments.
Objective: EMBRACE study evaluated impact of erenumab 140 mg once monthly on other aspects of migraine including pain, functional impairment, and non-ictal burden in patients with high-frequency episodic migraine (HFEM).
Methods: EMBRACE (NCT04252742), a phase 4, double-blind, randomized, placebo-controlled, global study enrolled patients aged ≥18 years with HFEM, defined as an average of ≥ 7 to < 15 migraine days and < 15 headache days per month, with at least one previous treatment failure.
Primary endpoint was change from baseline in mean monthly hours of at least moderate headache pain intensity over months 1, 2, and 3. Secondary endpoints included change from baseline in mean monthly function domain score as measured by the Migraine Functional Impact Questionnaire (MFIQ) (4 domains), average duration of at least moderate pain intensity during qualifying migraine attacks, and mean monthly average peak migraine pain intensity as assessed by the 11-point Numeric Rating Scale (NRS) over months 1, 2, and 3. Safety endpoints included treatment-emergent adverse events (TEAE), fatal AEs, serious AEs (SAEs), AEs leading to investigational product (IP) discontinuation, most common AEs, and events of interest.
Results: 512 participants were randomized with 510 receiving either erenumab 140 mg (n = 254) or placebo (n = 256) monthly. Demographics and baseline characteristics were balanced. Erenumab was superior to placebo in reducing: duration of moderate or severe headache pain intensity (p-value < 0.001); migraine functional impact in the 4 MFIQ domains (p-value < 0.001); and duration of migraine pain of at least moderate intensity in migraine attacks (p-value = 0.013) and in reducing peak migraine pain intensity (p-value = 0.011).
Overall incidences of TEAEs were higher for erenumab compared to placebo (19.3% vs. 14.8%). Grade 3 AE incidence was 1.6% for erenumab and 1.2% for placebo. Incidence of AEs leading to IP discontinuation was the same (0.4%) in both groups. No grade 4 or 5 (deaths) AEs were reported. SAEs were observed only in placebo (n = 2 [0.8%]). Most frequent events of interest were constipation (erenumab = 3.1%, placebo = 1.6%) and COVID-19 (erenumab = 2.0%, placebo = 2.7%).
Conclusions: EMBRACE represents a novel approach demonstrating the extent of therapeutic impact that effective migraine preventive treatments can have on migraine burden. In this trial, participants treated with erenumab reported spending significantly fewer hours with a headache of moderate or severe pain intensity every month while also experiencing significantly lower impact of migraine on usual activities and measures of physical, social and emotional functioning. Additionally, EMBRACE provided confirmatory evidence to support that erenumab treatment produces an enduring impact on residual migraine attacks with remaining events being less painful overall as measured by the significant reduction in average peak pain intensity per attack and average time spent with a moderate-to-severe headache on remaining recorded attacks as compared to placebo. No new safety events were identified.
EP.27
Efficacy and safety of erenumab in adults with medication overuse headache (MOH) over 1-year: Results from the chronic migraine (CM)-MOH trial final analysis
S Tepper1, D Dodick2, M Lanteri-Minet3,4, D Dolezil5, R Gil-Gouveia6,7, C Lucas8, K Piasecka-Stryczynska9, G Szabó10, D Mikol11, M Chehrenama11, Z Liu11 and G da Silva Lima11
1The New England Institute for Neurology and Headache, Stamford, USA
2Department of Neurology, Mayo Clinic, Scottsdale, USA
3Pain Department and FHU InovPain, Centre Hospitalier Universitaire de Nice-Côte Azur and University, France
4Inserm U1107, Neuro-Dol, Université Clermont Auvergne, Clermont-Ferrand, France
5Prague Headache Center, DADO MEDICAL sro, Prague, Czech Republic
6Neurology Department, Hospital da Luz, Luz Saude, Portugal
7Center for Interdisciplinary Research in Health, Universidade Católica Portuguesa, Lisboa, Portugal
8Department of Pain, CHU Lille, France
9Department of Neurology, Poznan University of Medical Sciences, Poznan, Poland
10Óbudai Egészségügyi Centrum, Budapest, Hungary
11Amgen Inc., Thousand Oaks, USA
Introduction: Erenumab (namely 140 mg) demonstrated superiority over placebo in inducing MOH remission in participants with CM-MOH over a 24-week double-blind treatment period (DBTP) (OR [95% CI]: 2.01 [1.33, 3.05]; P < 0.001 for 140 mg; OR [95% CI]: 1.37 [0.92, 2.05]; P = 0.13 for 70 mg). Erenumab treatment demonstrated higher rates of acute headache medication day (AHMD) reduction and sustained MOH remission.
Objective: To report results of exploratory endpoints from open-label treatment period (OLTP) for participants (non-opioid treated) who were part of the primary analysis.
Methods: This phase 4, randomized, double-blind, placebo-controlled study (NCT03971071) recruited adults with CM for ≥12 months, concomitant diagnosis of MOH, and history of ≥1 treatment failure. Participants were separated into non-opioid and opioid treated cohorts, then randomized 1:1:1 to erenumab 140 mg, 70 mg, or placebo once monthly for 24 weeks. Participants successfully completing DBTP had an opportunity to receive erenumab 70 mg or 140 mg during a 28-week OLTP.
Exploratory endpoints included MOH relapse at year 1 in participants achieving MOH remission at month 6 of DBTP and treated with erenumab throughout study, absence of MOH at end of study for all OLTP participants, sustained absence of MOH over 1 year for participants treated with erenumab throughout study, and change from baseline in mean monthly AHMD, monthly migraine days (MMD), and MHD of at least moderate pain intensity for all OLTP participants. Safety endpoints were AEs and changes in vital signs.
Results: 552 of 584 participants (94.5%) entered OLTP and received at least one dose of erenumab. Baseline demographics and disease characteristics remained balanced. Mean (SD) monthly AHMD was 18.8 (4.2), MMD was 18.8 (4.6), and MHD with at least moderate pain intensity was 19.4 (4.7) days at baseline. Most overused medication was triptans (69.4%). At end of study, absence of MOH was observed in 75.5% and 69.0% in erenumab 140 mg and 70 mg, respectively. Only 3 in each erenumab dose group (2.6%) were observed to have returned to MOH diagnosis at end of study. Sustained absence of MOH remission was achieved by 68.8% and 60.5% in erenumab 140 mg and 70 mg, respectively. At 1 year, mean (SD) change in monthly AHMD from baseline was –11.7 (5.7) for erenumab 140 mg, and –10.5 (6.5) for erenumab 70 mg. Mean (SD) change in MMD from baseline to 1 year was –11.5 (6.3) for erenumab 140 mg, and –10.0 (6.8) for erenumab 70 mg. Change in MHD of at least moderate pain intensity to 1 year was −12.0 (6.6) for erenumab 140 mg, and –10.6 (7.0) for erenumab 70 mg. In average, these changes signify a move from initial CM-MOH at baseline to a pattern consistent with episodic migraine without medication overuse. AEs were consistent with erenumab known safety profile.
Conclusions: Erenumab treatment was associated with high rates of MOH remission at end of year 1 and sustained MOH remission over 1 year. Treatment effect during OLTP was consistent regardless of having received erenumab or placebo during DBTP.
EP.28
Efficacy of Anti-CGRP mAbs in migraine: a comparative analysis between overweight and normal-weight populations
G Cretella1, C Russo1, S Braca1, A Stornaiuolo1, A Miele1, C Giannini1 and R De simone1
1Department of Neuroscience, Reproductive Sciences and Odontostomatology, University Of Naples Federico II, Napoli, Italy
Introduction: Migraine and excess weight share a relationship not yet fully understood. Moreover, the Body Mass Index (BMI) has been positively correlated with the frequency of migraine attacks. Anti-CGRP monoclonal antibodies (mABs) hold a pivotal role in targeting peripheral mediators in migraine treatments. Consequently, this study endeavors to assess the efficacy of mABs in a population characterized by excess weight compared to a normal weight control group.
Methods: We enrolled 120 chronic migraine patients treated with anti-CGRP mAbs divided into two groups according to BMI (BMI > 25 and <25). Over a time period of 12 months, we recorded mean monthly headache, BMI, midas, headache intensity and acute medication intake every three months.
Results: A monthly migraine frequency of 22+-7 days was found in the control group and 20+-7 days in the group of overweight patients before starting treatment. At month 12, an average of 9.5+-8.6 and 8.8+-7.0 days were found, respectively. Preliminary analysis of the data reveals a decrease in the monthly frequency of migraine in both the overweight patient group and the control group (p < 0.001). When comparing the difference in the decrease, it does not appear statistically significant (p = 0.6). Further analyses are still in progress.
Conclusion: The current analysis reveals that antibody treatment retains efficacy in the overweight population in the same way as in the normal-weight group. There are limited data in literature on the use of CGRP inhibitor monoclonal antibodies in individuals who are overweight/obese and further studies are needed to better understand efficacy in this patient population.
EP.29
Efficacy of Fremanezumab Treatment for Migraine Prevention in Patients with Migraine and Major Depressive Disorder: Results from the Open-Label Extension of the UNITE Study
R Lipton1, V Ramirez Campos2, Z Roth-Ben Arie3, M Ortega4, P Barbanti5,6, M Galic7 and D Mitsikostas8
1Departments Of Neurology, Psychiatry And Behavioral Sciences, Albert Einstein College Of Medicine, New York, USA
2Teva Branded Pharmaceutical Products R&D, Inc., West Chester, USA
3Teva Pharmaceutical Industries Ltd., Tel Aviv, Israel
4Teva Pharmaceutical Industries Ltd., Parsippany, USA
5Headache and Pain Unit, IRCCS San Raffaele, Rome, Italy
6San Raffaele University, Rome, Italy
7Teva-Pharma, Produtos Farmacêuticos, Lda., Porto Salvo, Portugal
8Department of First Neurology, Aeginition Hospital, National and Kapodistrian University of Athens, Athens, Greece
Introduction: Migraine and major depressive disorder are frequently comorbid. The 12-week, double-blind, placebo-controlled period (DBPC) of the UNITE study (NCT0401284) showed that fremanezumab, a humanised monoclonal antibody that targets calcitonin gene-related peptide, reduced monthly migraine days (MMD) and depressive symptom scores in patients with migraine and depression versus placebo.
Objectives: To report the longer-term efficacy and safety data, including the impact on disability and major depressive disorder outcomes, from the open-label extension (OLE) of UNITE.
Methods: UNITE was a 28-week, Phase 4, double-blind, placebo-controlled, parallel-group study, which included a 28-day screening period, 12-week DBPC and 12-week OLE. Adults with episodic or chronic migraine (EM, CM), a history of major depressive disorder according to the Diagnostic and Statistical Manual of Mental Disorders criteria ≥12 months prior to screening and active symptoms of depression (defined as a Patient Health Questionnaire-9 [PHQ-9] score of ≥10 at screening) were enrolled in the study. Following screening, eligible patients were randomised 1:1 to monthly fremanezumab (225 mg) or matched placebo. After 12 weeks, all completers were invited to enter the OLE where they received quarterly fremanezumab (675 mg) in either the fremanezumab-fremanezumab or placebo-fremanezumab group. Key exploratory endpoints assessed in the OLE included mean change from baseline to Week 24 in MMD, Hamilton Depression Rating Scale-17 (HAM-D 17) score, 6-Item Headache Impact Test (HIT-6) disability score, Clinical Global Impression of Severity of Illness (CGI-S) rating and PHQ-9 score. Safety was measured through adverse events (AEs).
Results: In total, 330/353 patients entered the OLE (EM, 47%; mean age, 43.3 years; 289 [88%] female). Mean change from baseline in MMD at Week 12 was –5.4 for fremanezumab and –3.4 for placebo. At Week 24, mean change from baseline in MMD was –6.9 for the fremanezumab-fremanezumab group and –7.0 for the placebo-fremanezumab group (Figure 1). Mean change from baseline in HAM-D 17 score for the fremanezumab-fremanezumab and placebo-fremanezumab groups was –6.8 and –5.4 at Week 12 and –7.6 and –8.4 at Week 24, respectively. Clinically meaningful reductions in HIT-6, CGI-S and PHQ-9 scores were observed at Week 24 in both treatment groups. In the OLE, 60 (18%) patients reported ≥1 AE. The most common AEs were infections and infestations (17 [5%]); one mild event of constipation was reported. Three (<1%) patients reported ≥1 serious AE (all in the placebo-fremanezumab group). No patients in the OLE discontinued the study due to an AE.
Conclusions: Despite the complex treatment history of this high-risk population, patients with migraine and major depressive disorder experienced sustained reductions in MMD, disability and depressive symptom scores over the OLE, suggesting that fremanezumab may reduce the symptoms and cumulative burden of both diseases. Notable reductions in these exploratory endpoints in patients who switched from placebo to fremanezumab, and in those who switched from monthly to quarterly fremanezumab dosing schedules, highlight the efficacy of both dosing regimens for migraine prevention, with safety outcomes consistent with that of the DBPC and pivotal fremanezumab randomised controlled trials.

EP.30
Efficacy Outcomes from a Phase 3, Randomised, Double-Blind, Placebo-Controlled Study of Fremanezumab for the Preventive Treatment of Migraine in Chinese Adults
S Yu1, S Barash2, G Chen3, G Yiu2, J Bryson2, Y Carmeli Schwartz4, Z Roth-Ben Arie4, M Benedek-Segal4 and X Ning2
1Department of Neurology, Chinese PLA General Hospital, Beijing, China
2Teva Branded Pharmaceutical Products R&D, Inc., West Chester, USA
3Teva Pharmaceutical Information Consulting (Shanghai) Co., Ltd., Beijing, China
4Teva Pharmaceutical Industries Ltd., Tel Aviv, Israel
Introduction: Fremanezumab, a humanised monoclonal antibody that selectively targets calcitonin gene-related peptide, is approved for the preventive treatment of migraine in adults in the United States (US) and Europe. While clinical care guidelines in China are similar to those of the US and Europe in their support of a stratified approach to migraine treatment (accounting for attack severity, treatment side effects, and previous treatment response), there are currently no preventive treatments with a primary indication for migraine available in China.
Objectives: This study aims to demonstrate the efficacy and safety of monthly and quarterly doses of fremanezumab in Chinese adults with episodic and chronic migraine (EM, CM).
Methods: This multicentre, parallel-group, Phase 3 study consisted of a 4-week baseline period, 12-week double-blind period (DBP), 12-week open-label extension (OLE) period, and 3-month follow-up period. Eligible participants were 18–70 years of age, with a diagnosis of EM or CM with onset at ≤50 years of age, ≥ 4 monthly migraine days (MMD), and a ≥ 12-month history of migraine prior to screening. Exclusion criteria included use of medications containing barbiturates or opioids on ≥4 days during the baseline period or an intervention or device for migraine during the two months prior to screening. Participants were randomised 1:1:2 to receive 225 mg monthly or 675 mg quarterly (with placebo at Week 4 and 8) fremanezumab, or matched monthly placebo for 12 weeks. During the OLE, all participants received monthly fremanezumab. The primary endpoint was mean change from baseline in MMD during the DBP. Secondary endpoints assessed included mean change from baseline in migraine days during the first four weeks of treatment, mean change from baseline in days with acute medication use, the proportion of participants achieving ≥50% reduction in MMD, and mean change from baseline in monthly headache days (MHD) of at least moderate severity. A hierarchical testing procedure was implemented according to the predetermined sequence.
Results: In total, 361/454 screened participants (placebo, n = 182; all fremanezumab [monthly and quarterly dosing], n = 179) were included in the efficacy analysis. The mean change from baseline in MMD during the DBP was –4.6 for fremanezumab versus –2.8 for placebo (p < 0.0001); mean change from baseline in MMD at each timepoint is shown in Figure 1. The reduction in migraine days in the first four weeks of treatment was significantly greater with fremanezumab versus placebo (–4.5 vs. –2.2; p < 0.0001), as was the reduction in days of acute medication use during the DBP (–3.0 vs. –1.1; p < 0.0001). In total, 58% of participants in the fremanezumab group achieved ≥50% reduction in MMD during the DBP compared with 35% of participants in the placebo group (p < 0.0001). Least squares mean change from baseline in MHD was greater for participants receiving fremanezumab versus placebo (–4.5 vs. –2.4; p < 0.0001).
Conclusions: All primary and secondary endpoints were met according to prespecified hierarchical analysis, with results comparable to studies of fremanezumab in diverse populations, including those of different ethnicities. These results support the use of fremanezumab for migraine prevention in Chinese adults with migraine.

EP.31
Impact of Atogepant on Long-term Response Rates and Migraine-Specific Quality of Life in Migraine Prevention: Interim Analysis of a Phase 3, Multicenter, Open-label, 156-Week Extension Study
P Goadsby1,2, D Holle-Lee3, C Tassorelli4,5, S Cho6, M He7, P Gandhi7, K Carr7, B Dabruzzo7, J Smith7 and S Ashina8,9,10
1NIHR King's Clinical Research Facility, King's College London, London, United Kingdom
2Department of Neurology, University of California, Los Angeles, United States of America
3Department of Neurology, West German Headache and Vertigo Center Essen, University of Essen, Essen, Germany
4Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
5Headache Science & Neurorehabilitation Centre, IRCCS C. Mondino Foundation, Pavia, Italy
6Department of Neurology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
7AbbVie, North Chicago, United States of America
8BIDMC Comprehensive Headache Center, Beth Israel Deaconess Medical Center, Boston, United States of America
9Department of Neurology and Department of Anesthesia, Critical Care and Pain Medicine, Harvard Medical School, Boston, United States of America
10Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
Introduction: Atogepant is an oral calcitonin gene-related peptide receptor antagonist approved for the preventive treatment of migraine. ELEVATE and PROGRESS were phase 3, randomized, double-blind, placebo-controlled trials evaluating atogepant for the preventive treatment of episodic migraine (EM) in participants who had previously been failed by 2-4 classes of conventional oral preventive treatments (ELEVATE), or the preventive treatment of chronic migraine (CM, PROGRESS).
Objectives: Evaluate long-term response rates and migraine-specific quality of life across the first year of atogepant treatment in an open-label extension study enrolling participants with EM and a history of prior preventive treatment failures, or CM.
Methods: This interim analysis (September 14, 2023) of the open-label, 156-week, long-term safety extension study evaluated atogepant 60 mg once daily for the preventive treatment of EM or CM in participants who completed ELEVATE or PROGRESS, respectively. The long-term safety, tolerability, and efficacy of atogepant in participants completing Week 48 or early termination was evaluated. The proportion of participants reporting ≥50%, ≥ 75%, and 100% improvement (reduction) in monthly migraine days (MMDs) from the baseline period of the lead-in study was assessed at weeks 13-16, 29-32, and 45-48 using eDiary collection during these 4-week intervals. The migraine-specific quality of life questionnaire (MSQ v2.1) was completed during clinic visits at weeks 12, 20, 28, 36, 44, and 52. The role function-restrictive (RFR) domain of the MSQ measures how often migraine impacts function related to daily social and work-related activities. All data presented are from participants in the protocol defined modified Intent-to-Treat (mITT; Full Analysis Set) population.
Results: Of the 595 participants who received ≥1 dose of study intervention, 524 had ≥1 evaluable 4-week period of post-baseline data (ELEVATE, n = 240; PROGRESS, n = 284) and were included. Of participants, 50.5% (265/524) enrolled directly from the conclusion of the double-blind treatment period (at week 7 of the lead-in study), while the remaining participants were enrolled following a 4-week safety period, or later. Among participants, 70.0% (73.5% [ELEVATE], 67.0% [PROGRESS]) achieved a reduction of ≥50% in MMDs at weeks 13-16 and similar rates were observed up to 48 weeks (figure 1). Participants who were direct rollovers from visit 7 of the lead-in study had similar ≥50% response rates to the full mITT population. At weeks 13-16, 43.9% and 18.1% of participants reported ≥75% and 100% improvement from lead-in baseline, respectively, that was maintained through week 48. At lead-in study baseline, RFR domain scores in participants recruited from ELEVATE (43.09) were similar to those from PROGRESS (40.73), and indicative of severe impairment (table 1). At week 12, participants reported an improvement of 34.79 (37.63 [ELEVATE], 32.43 [PROGRESS]) that was consistent through week 52. As previously reported for this study, the overall safety results were consistent with the known safety profile of atogepant.
Conclusion: Improvements from lead-in baseline study were observed at weeks 13–16 for ≥ 50%, ≥ 75%, and 100% response rates, and at week 12 for the RFR domain of the MSQ v2.1. These improvements were sustained over weeks 48 (response rates) and 52 (RFR).


EP.32
Impact of Fremanezumab Cessation and Reinitiation in Migraine Management: PEARL Study 4th Interim Analysis
D Mitsikostas1, M Ashina2,3, F Mohammad Amin1,4, P Kokturk5, C Schankin6, G Sahin7, P Pozo-Rosich8, P Dorman9, T Nežádal10, I Pavão Martins11, M Sumelahti12, V Ramirez Campos13, X Ning13, H Akcicek5 and C Tassorelli14,15
1Department of First Neurology, Aeginition Hospital, National and Kapodistrian University of Athens, Athens, Greece
2Department of Neurology, Danish Headache Center, Copenhagen University Hospital – Rigshospitalet Glostrup, Copenhagen, Denmark
3Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
4Department of Neurorehabilitation/Traumatic Brain Injury, Rigshospitalet Glostrup, University of Copenhagen, Copenhagen, Denmark
5Teva Netherlands B.V., Amsterdam, Netherlands
6Department of Neurology, Inselspital, University Hospital Bern, University of Bern, Bern, Switzerland
7Department of Clinical Sciences of Lund, Lund University, Skåneuro Neurology Clinic, Lund, Sweden
8Headache Unit & Research Group, Vall d’Hebron Hospital & Research Institute, Universitat Autonoma de Barcelona, Barcelona, Spain
9The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, United Kingdom
10Institute of Neuropsychiatric Care, First Faculty of Medicine, Charles University, Prague, Czech Republic
11Centro de Estudos Egas Moniz, Faculty of Medicine, University of Lisbon, Lisbon, Portugal
12Faculty of Medicine and Health Technology, University of Tampere, Tampere, Finland
13Teva Branded Pharmaceutical Products R&D, Inc., West Chester, USA
14Department of Brain & Behavioral Sciences, University of Pavia, Pavia, Italy
15IRCCS C. Mondino Foundation, Pavia, Italy
Introduction: Despite recent updates to the guidelines, some reimbursement authorities still mandate a pause in preventive treatment with calcitonin gene-related peptide (CGRP) pathway monoclonal antibodies (mAbs) after one year of continuous use. However, migraine symptoms frequently return following treatment cessation and treatment effectiveness can be reduced upon reinitiation.
Objectives: This fourth interim subanalysis of the PEARL study explored the impact of fremanezumab cessation and reinitiation on monthly migraine days (MMD).
Methods: PEARL (EUPAS35111) is a Phase 4 study evaluating the real-world effectiveness of fremanezumab in adults with episodic or chronic migraine (EM, CM). The fourth interim analysis was conducted when all participants completed ≥12 months of treatment.
Results: Of 220 participants with documented cessation of fremanezumab, 98 stopped treatment for reimbursement and 192 reinitiated after a mean (standard deviation, SD) period of 2.6 (2.0) months (Table 1). Over 40% of participants experienced worsening of migraine (≥50% increase in MMD from the time of cessation) at Months 1 and 2 after the time of cessation (Month 1: Total, 41.3% [74/179], EM, 54.5% [36/66], CM, 33.6% [38/113]; Month 2: Total, 41.8% [66/158], EM, 53.7% [29/54], CM, 35.6% [37/104]). Mean MMD decreased after reinitiation but remained higher than before cessation (Figure 1). The proportion of participants achieving ≥50% reduction in MMD at Month 1 and Month 3, respectively, was 49.0% and 58.9% in the first treatment period (before cessation) versus 35.7% and 45.5% in the second treatment period (after reinitiation).
Conclusion: Post-fremanezumab cessation, a notable rise in MMD was observed, with reduced effectiveness upon reinitiation. This challenges the rationale behind mandated treatment pauses, underscoring the need for individualised patient management strategies.


EP.33
Long-term improvements following >=50% migraine response in eptinezumab-treated patients with migraine
M Ashina1,2, S Awad3, X Lee3, L Boserup3, B Sperling3, A Ettrup3, R Lipton4 and J Ailani5
1Department of Neurology, Danish Headache Center, Copenhagen University Hospital- Rigshospitalet, Copenhagen, Denmark
2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
3H. Lundbeck A/S, Copenhagen, Denmark
4Department of Neurology, Albert Einstein College of Medicine, Bronx, United States
5Department of Neurology, Georgetown University Hospital, Washington, United States
Introduction: The DELIVER trial examined long-term (72-week) patient response to eptinezumab preventive treatment. For eptinezumab-treated patients demonstrating an initial migraine response (i.e., response over the placebo-controlled period, Weeks 1–12), changes from baseline in monthly migraine days (MMDs), 6-item Headache Impact Test (HIT-6) total score, presenteeism, and percentage of severe migraine attacks are reported.
Objectives: To evaluate long-term improvements in patients who experienced ≥50% migraine response with the first dose of eptinezumab, a population likely to continue eptinezumab treatment in clinical practice.
Methods: DELIVER included adults with migraine and 2–4 prior preventive migraine treatment failures, with the long-term population (n = 865) including those completing the 24-week placebo-controlled period and continuing into the 48-week dose-blinded extension period. Post hoc analysis followed eptinezumab-treated patients with a ≥ 50% reduction in MMDs (i.e., ≥ 50% migraine response) during the first dosing interval (Weeks 1–12) across subsequent 12-week dosing intervals for the duration of the 72-week trial.
Results: Over Weeks 1–12, 123/286 (43.0%, 100 mg) and 141/282 (50.0%, 300 mg) eptinezumab-treated patients in the long-term full analysis set experienced ≥50% migraine response. Eptinezumab-treated patients with initial ≥50% migraine response showed sustained reductions in migraine frequency, with mean reductions of 7.8 (100 mg) and 8.1 (300 mg) MMDs over Weeks 1–12 and 8.2 (100 mg) and 8.6 (300 mg) over Weeks 61–72. Also shown were sustained improvements from baseline in headache-related impact (HIT-6 total score: baseline 66.1–66.5; reduction 13.3–15.1 [Week 12] and 14.1–15.9 [Week 72]); presenteeism-affected working time (baseline 52.2–52.4%; reduction 35.7–37.8% [Week 12] and 34.7–35.4% [Week 72]); and percentage of severe migraine attacks (baseline 45.0–47.9%; reduction 28.7–29.5% [Weeks 1–12] and 29.6–33.4% [Weeks 61–72]).
Conclusion: Patients with ≥50% migraine response following one eptinezumab dose (100 mg or 300 mg) experienced improvements over Weeks 1–12 that were maintained over 72 weeks in MMDs, headache-related impact, presenteeism, and percentage of severe migraine attacks.
EP.34
Long-Term Safety, Tolerability, and Efficacy of Atogepant for the Preventive Treatment of Migraine: Interim Analysis of a Phase 3, Multicenter, Open-Label, 156-Week Long-Term Safety Extension Study
S Ashina1, M Ashina2, D Holle-Lee3, C Tassorelli4, S Cho5, M He6, R de Abreu Ferreira6, J Smith7, K Pfleeger7 and J Trugman6
1BIDMC Comprehensive Headache Center, Beth Israel Deaconess Medical Center, Boston, MA, USA; Department of Neurology and Department of Anesthesia, Critical Care and Pain Medicine, Harvard Medical School, Boston, MA, USA; Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; Department of Neurology, Danish Headache Center, Copenhagen University Hospital - Rigshospitalet, Copenhagen
3Department of Neurology, West German Headache and Vertigo Center Essen, University of Essen, Essen, Germany
4Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy; Headache Science & Neurorehabilitation Centre, IRCCS C. Mondino Foundation, Pavia, Italy
5Department of Neurology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
6AbbVie, Madison, USA
7AbbVie, North Chicago, USA
Introduction: Atogepant is an oral calcitonin gene-related peptide receptor antagonist approved for the preventive treatment of migraine. ELEVATE and PROGRESS were phase 3, randomized, double-blind, placebo-controlled trials evaluating atogepant for the preventive treatment of episodic migraine (EM) in participants with an inadequate response to 2–4 classes of conventional oral preventive treatment (ELEVATE), and for the preventive treatment of chronic migraine (CM) (PROGRESS).
Objective: Evaluate the long-term safety and efficacy of atogepant for the preventive treatment of migraine.
Methods: This interim analysis (September 14, 2023) of the open-label, 156-week, long-term safety extension study evaluated atogepant 60 mg once daily for the preventive treatment of EM or CM in participants who completed ELEVATE or PROGRESS, respectively. The long-term safety, tolerability, and efficacy of atogepant in participants completing Week 48 or early termination was evaluated. Efficacy was assessed during the first 48 weeks.
Results: The safety population in this interim analysis included 595 participants (ELEVATE, n = 270; PROGRESS, n = 325). Mean duration of atogepant exposure was 496.5 days. Treatment-emergent adverse events (TEAEs) occurred in 79.0% of participants; most were mild/moderate and not related to atogepant. Common TEAEs (≥5%) were COVID-19 (28.7%), nasopharyngitis (10.9%), and constipation (8.2%). One death attributed to asphyxia by housefire was observed. Other serious TEAEs occurred in 5.5% of participants and were not related to atogepant. TEAEs leading to discontinuation occurred in 5.9% of participants. ALT/AST ≥3 x ULN occurred in 2 participants; none met Hy’s Law. Least square mean change from baseline in monthly migraine days was −5.5 (ELEVATE) and -10.9 (PROGRESS) at Weeks 13–16 and was sustained over 48 weeks. Similar outcomes were observed for monthly headache days and monthly acute medication use days.
Conclusions: The overall safety results were consistent with the known safety profile of atogepant. No new safety signals were identified. Improvements in efficacy outcomes were sustained over 48 weeks.
EP.36
Safety Outcomes from a Phase 3, Randomised, Double-Blind, Placebo-Controlled Study of Fremanezumab for the Preventive Treatment of Migraine in Chinese Adults
S Yu1, S Barash2, G Chen3, G Yiu2, J Bryson2, Y Kessler4, Y Carmeli Schwartz4, Z Roth-Ben Arie4, M Benedek-Segal4 and X Ning2
1Department of Neurology, Chinese PLA General Hospital, Beijing, China
2Teva Branded Pharmaceutical Products R&D, Inc., West Chester, USA
3Teva Pharmaceutical Information Consulting (Shanghai) Co., Ltd., Beijing, China
4Teva Pharmaceutical Industries Ltd., Tel Aviv, Israel
Introduction: The favourable safety profile of fremanezumab, a humanised monoclonal antibody that selectively targets calcitonin gene-related peptide, has been demonstrated in multiple Phase 3 trials, including in individuals with difficult-to-treat migraine. As a result, fremanezumab is approved as a preventive migraine treatment in Europe, the United States, and many other countries. In China, migraine treatment guidelines recommend the use of preventive medications that are not developed specifically for migraine, such as antiepileptics and beta blockers, and that are often associated with significant adverse events (AEs). Thus, there remains an unmet need for well tolerated and efficacious preventive treatments for individuals with migraine in China.
Objectives: This study aims to demonstrate the efficacy and safety of monthly and quarterly doses of fremanezumab in Chinese adults with episodic and chronic migraine (EM, CM).
Methods: This multicentre, parallel-group, Phase 3 study consisted of a 4-week baseline period, 12-week double-blind treatment period (DBP), 12-week open-label extension (OLE) period, and 3-month follow-up period. Eligible participants were adults (18–70 years) with a diagnosis of EM or CM with onset at ≤50 years of age, ≥ 4 monthly migraine days (MMD), and a ≥ 12-month history of migraine prior to screening. Participants were excluded if they had used medications containing barbiturates or opioids on ≥4 days during the baseline period or an intervention or device for migraine during the two months prior to screening. Participants were randomised 1:1:2 to receive 225 mg monthly or 675 mg quarterly (with placebo at Week 4 and 8) fremanezumab, or matched monthly placebo for 12 weeks. During the OLE, all participants received 225 mg monthly fremanezumab. The primary endpoint was mean change from baseline in MMD during the DBP, and safety was assessed through adverse event reporting, clinical laboratory test results and electrocardiogram findings.
Results: Of the 454 screened participants, 361 (placebo, n = 182; fremanezumab, n = 179 [monthly, n = 90; quarterly, n = 89]) were included in the efficacy analysis and 365 (placebo, n = 183; fremanezumab, n = 182 [n = 91 per dose regimen]) were included in the safety analysis. In total, 97% of participants in the placebo group and 95% across the fremanezumab groups completed DBP. The least squares mean change from baseline in MMD during the DBP was –4.6 for fremanezumab versus –2.8 for placebo (p < 0.0001). The percentages of participants reporting any AE were similar across treatment groups (Table 1); and only administration site reactions occurred more frequently in the fremanezumab groups compared with the placebo group.
Conclusions: The safety and tolerability profile of fremanezumab in Chinese adult participants with migraine was consistent with previous pivotal global studies, with no safety signals observed. These findings suggest fremanezumab may provide an effective and well tolerated preventive migraine treatment option in this population.

EP.37
The Use of Onabotulinumtoxin A for the Treatment of Chronic Migraine During Pregnancy: An American Headache Society Survey Study
A Ali2, J Nofar1, K Hamilton1 and P Mathew3
1Henry Ford Health, Detroit, USA
2Michigan State University College of Human Medicine
3Harvard Medical School
Introduction: The peak prevalence of migraine in women occurs during childbearing age, yet migraine preventative treatment options are limited during pregnancy due to concerns of potential harm to the developing fetus. Onabotulinum toxin type A (OnabotA) is an FDA-approved neurotoxin for the preventative treatment of chronic migraine. Based on available data, OnabotA appears to be safe for use during pregnancy, but there is significant clinician hesitancy in using this therapy during pregnancy. No studies have been conducted to explore physicians’ practices regarding the use of botulinum toxin during pregnancy.
Objective: To survey the clinical practices of headache providers regarding botulinum toxin injections for chronic migraine in pregnancy.
Methods: A 15-question survey exploring physicians’ use of OnabotA for the treatment of chronic migraine was distributed via SurveyMonkey to all members on the American Headache Society (AHS) listserv on September 21, 2021, and was closed on October 29, 2021. The final 4 questions pertained to use during pregnancy. Descriptive analysis was performed.
Results: Of the 1665 members in the AHS listserv, 168 responders (162 from the United States and 6 from Canada) completed the survey (response rate 10.1% [168/1665]).
70 (42%) had used OnabotA during pregnancy
97 (59%) reported continuing use of OnabotA while a patient is actively trying to become pregnant
71 (43%) continued OnabotA treatment into pregnancy
117 (71%) reported that they have or would consider resuming OnabotA treatment during pregnancy should a patient experience refractory headache after discontinuation of the treatment; 48 (29%) reported that they still have not or would not consider restarting OnabotA treatment under those same circumstances
Conclusion: Of the clinicians sampled, a slight majority avoided the use of OnabotA during pregnancy, however have used or considered using OnabotA should the patient develop refractory headache after discontinuation of OnabotA due to pregnancy. Additionally, the majority of clinicians did not discontinue OnabotA while a patient is actively trying to become pregnant. This is in contrast to the general practice of discontinuing medications that are thought to be teratogenic when attempting conception. It is not surprising that clinicians are hesitant to use OnabotA given the limited evidence of its definitive safety during pregnancy. However, the available data has been reassuring, which has resulted in more clinicians using OnabotA during pregnancy. The use of OnabotA for migraine prevention during pregnancy conveys benefits to both the mother and fetus in terms of pain and disability mitigation, and likely also results in improvement of sleep and nutrition. In addition, OnabotA use likely reduces the use of medications, which can at times have negative impacts on the developing fetus. Larger studies investigating long-term outcomes in newborns are necessary to support the safety of OnabotA use during pregnancy. The publication of additional case series and pregnancy registries will be important to increase the use of OnabotA in pregnant women and women who are attempting pregnancy.
Figure

EP.38
STRESS IN RATS INCREASES THE SUSCEPTIBILITY TO MIGRAINE-LIKE ACTIVATION AND SENSITIZATION OF TRIGEMINOCERVICAL NEURONS: INFLUENCE OF SEX
A Salinas Abarca1, R Torres-Granados1, M Romero-Reyes1 and S Akerman1
1Department of Neural and Pain Science, University of Maryland, School of Dentistry, Baltimore, United States
Introduction: Migraine headache is a severe and highly disabling pain condition that significantly affects females more than males. It is thought to be mediated by abnormal activation and sensitization of intracranial meningeal afferent neurons and their central projection to the trigeminocervical complex. Chronic stress affects millions of people worldwide, and it is established that patients with migraine are particularly susceptible to stress as a migraine trigger, although the exact mechanism is unknown.
Objective: To dissect the role of stress and possible sex dimorphism in reducing the threshold to mediate trigeminocervical neuronal migraine-like mechanisms.
Methods: We adapted and combined two migraine-like approaches, stress and a chemical migraine provocative (nitric oxide (NO) donor), to dissect clinically relevant neurophysiological changes within dural-trigeminovascular neurons. We also measured nociceptive periorbital withdrawal thresholds to determine migraine-like outcomes to the stress protocols alone. Rats (male and female) were stressed using either restraint (2 h for four days) or food-fasting (16 h). In restraint-stress rats, physiology studies were delayed until behavioral thresholds were restored to baseline (between 18-22 and 28-32 days, to males and females, respectively). In vivo electrophysiological extracellular recording of dural-responsive trigeminocervical neurons was carried out in naïve or stressed rats, with ongoing and cranial-evoked neuronal responses evaluated to a non-noxious dose of the NO donor, sodium nitroprusside (SNP; 30 µg/kg, IV).
Results: Female rats (n = 12) showed a lower baseline periorbital withdrawal threshold, and restraint stress caused a prolonged but reversible periorbital hypersensitivity that was also significantly prolonged in females. In naïve rats, only in females (n = 7) did the non-noxious dose of SNP mediate activation and sensitization of dural-responsive trigeminocervical Aδ and C-fiber neurons. Further, the electrical activation threshold of intracranial meningeal afferents was also significantly lower. In the stressed/SNP rats (n = 7/group), significant neuronal changes were observed in both sexes. However, responses were significantly exacerbated in stressed females compared to naïve.
Conclusions: These data demonstrate that stress can independently mediate migraine-like periorbital hypersensitivity, indicative of sensitization of dural-trigeminocervical neurons. Both stresses also ‘prime’ the trigeminovascular system, reducing the threshold necessary to mediate a migraine-like response, using a non-noxious dose of a migraine provocative (NO donor). This translates to the increased susceptibility of migraine patients to stress. We also demonstrate clear sex differences in the sensitivity and activation of intracranial meningeal afferents that translate to the sex dimorphism experienced in the clinical setting.
EP.39
TARGETING THE S1P-S1PR1 SIGNALING AXIS IN MIGRAINE-LIKE DURAL-RESPONSIVE TRIGEMINOCERVICAL NEURONS IN RATS
A Salinas Abarca1, M Romero-Reyes1, D Salvemini2 and S Akerman1
1Department of Neural and Pain Science, University of Maryland, School of Dentistry, Baltimore, United States
2Department o0f Pharmacology and Physiology, Saint Louis University, St. Louis, United States
Introduction: Emerging evidence suggests dysregulated neuronal sphingolipid metabolism is linked to various clinical pain states via the over-production of sphingosine-1-phosphate (S1P) in spinal dorsal horn neurons and its selective engagement with S1P receptor 1 (S1PR1). Indeed, functional S1PR1 antagonists, such as ozanimod, which are already approved for the treatment of multiple sclerosis, are effective in preclinical models of persistent spinal-related pain states in preclinical models. However, it is unknown whether activation of the S1P-S1PR1 signaling axis contributes to the development of trigeminovascular sensitization in preclinical models related to migraine.
Objectives: To dissect the role of the S1P-S1PR1 signaling axis in a preclinical model of migraine-related activation and sensitization of trigeminocervical (TCC) neurons and to establish S1PR1 as a novel target for treatment in migraine and related disorders.
Methods: We used in vivo electrophysiological extracellular techniques to record dural-responsive TCC neurons in naïve male and female rats or in a model of trigeminovascular sensitization. Here, restraint stress (2 h/day for 4 days) was used to mediate latent sensitization that was unmasked by administration of a non-noxious dose of the nitric oxide (NO) donor, sodium nitroprusside (30 µg/kg, IV). We evaluated the effects of pretreatment with two functional S1PR1 antagonists, FTY720 (1 mg/kg, IV) and ozanimod (1 mg/kg, IV), and measured ongoing and cranial-evoked neuronal responses over 3 h.
Results: Pretreatment with FTY720 (1 mg/kg, IV, n = 7) and ozanimod (1 mg/kg, IV, n = 7) significantly inhibited ongoing spontaneous neuronal firing and intracranial dural-evoked Aδ and C fiber responses in naïve rats. In addition, ozanimod (n = 7) prevented the prolonged increase in ongoing activity and the neuronal hypersensitivity to intracranial and extracranial innocuous and noxious V1 cutaneous stimulation mediated by restraint stress/SNP.
Conclusions: These data provide preclinical evidence that functional S1PR1 antagonists (ozanimod and FTY720) modulate the trigeminal ganglion-TCC pathway, decreasing the neuronal activity of trigeminovascular neurons in migraine-like models. This supports the participation of the S1P-S1PR1 signaling pathway in mechanisms of activation and sensitization of dural-trigeminovascular neurons related to migraine. These data also establish S1PR1 as a novel and effective target for the treatment of migraine and related disorders.
EP.40
Chronobiology in Migraine: Preliminary results from a Headache Database
U Ashraf1,2,3 and S Tomlinson1,3
1St Vincent's Hospital, Sydney, Australia
2University of New South Wales, Sydney, Australia
3University of Notre Dame Australia, Sydney, Australia
Introduction: The pathophysiology of migraine, a common and disabling neurological disorder, remains incompletely understood. The hypothalamus has been posited to be important in the generation and chronification of migraine attacks based off pre-clinical data as well as neuro-imaging studies and is the primary neurological generator of chronobiological rhythms in the body such as the circadian rhythm for sleep and the menstrual cycle in females. Chronobiological characteristics of migraine may give further insight into the role of the hypothalamus in migraine pathophysiology.
Objective: To identify the prevalence of different chronobiological rhythms in headaches and to characterise migraines with circadian attack rhythm.
Methods: A retrospective cohort study was performed on patients from the Headache Clinic at St Vincent’s Hospital Sydney. Data was collected from the clinical documentation of patients who visited the Headache Clinic since February 2024 and collated onto a secure REDCAP database. Patients with a diagnosis of migraine as per ICHD-3 criteria were included. Statistical significance was calculated using Fisher’s exact test and multivariate analysis performed by binomial logistic regression using XLSTAT.
Chronobiological data was collected by reviewing if the patient tended to have migraines at a particular time of day (classified as a circadian attack rhythm), at multiple particular times of the day (classified as an ultradian attack rhythm) or at specific times of the week, month or year (classified as an infradian attack rhythm).
Results: Of the patients encountered in the Headache Clinic since February 2024, 58 were identified as having a diagnosis of migraine. The number of patients who had high frequency episodic migraine or chronic migraine (HFEM/CM) were 43/58 (74%) and 15/58 (26%) had episodic migraine (EM). Most patients, 46/58 (79%), were female and 12/58 (21%) were male. Table 1 displays data on the prevalence of chronobiological rhythms amongst men, women, patients with EM and patients with HFEM/CM.
39/43 (91%) patients with HFEM/CM had a chronobiological attack rhythm compared to 9/15 (60%) patients with EM (p = 0.014).
6/36 (17%) patients with circadian attack rhythm had premonitory nasal congestion compared to 0/22 patients without circadian attack rhythm (p < 0.001). 10/36 patients with circadian attack rhythm had premonitory anxiety compared to 2/20 patients without circadian attack rhythm (p = 0.012).
Conclusion: Chronobiological attack rhythms are highly prevalent in migraine, regardless of sex, with the most prevalent attack rhythm being circadian. Patients with more frequent migraine are more likely to have a chronobiological attack rhythm compared to patients with less frequent migraine. Patients with circadian attack rhythm were more likely to have premonitory nasal congestion and anxiety, similar to patients with cluster headache.
Given the role of the suprachiasmatic nucleus in the hypothalamus in maintaining circadian rhythmicity and the hormonal role the hypothalamus plays in infradian rhythms such as the menstrual cycle, this data provides clinical evidence of the significant role the hypothalamus plays in migraine pathophysiology. In particular, the higher prevalence of chronobiological attack rhythm in more frequent migraines may suggest increasing hypothalamic activation as migraine becomes more chronic.

EP.41
Differences in cortical gray matter thickness between patients with episodic and chronic migraine
N Imai1, A Moriya1 and E KItamura2
1Department of Neurology and Headache Center, Japanese Red Cross Shizuoka Hospital, Shizuoka, Japan
2Department of Neurology, Kitasato University, Sagamihara, Japan
Introduction: Previously, surface-based morphometric analyses indicated variations in the cortical thickness of patients with migraines.
Objectives: In this study, we explored the differences in cortical gray matter thickness between patients with episodic and chronic migraines.
Methods: Seventy-three migraineurs, including 51 with episodic (44 females; mean age: 39.5 ± 13.1 years) and 22 with chronic migraine (18 females; mean age: 39.0 ± 14.9 years), were analyzed using a 3 T magnetic resonance imager. T1-weighted structural images were acquired using an accelerated sagittal Inversion Recovery–Fast Spoiled Gradient sequence with several sagittal slices. We estimated and compared cortical thickness between patients with episodic and chronic migraines through surface-based morphometry using FreeSurfer software (version 7.4.1; https://surfer.nmr.mgh.harvard.edu). Parameters were compared between headache types using Student's t-test (for data with normal distribution and equal variances), Welch's t-test (for data with normal distribution but unequal variances), and Mann–Whitney’s U-test (for data with non-normally distribution) (Python 3.11.5 packaged by Anaconda, Inc.).
Results: The results revealed significant regional differences in the cortical thickness. In particular, patients with chronic migraine exhibited thinner cortices in the right fusiform gyrus as well as right pars triangularis, and thicker bilateral posterior cingulate cortex compared to those with episodic migraine (Table 1).
Conclusion: These results suggest a potential association of chronic migraine rather than episodic migraine with distinct cortical abnormalities. These variations in cortical thickness across different regions potentially reflect the differential impact of chronic and episodic migraines on brain structure, which is possibly correlated with the frequency and duration of migraine episodes.

EP.42
Effects of over-the-suture scalp stimulation on headache occurrence in humans
K Peng1, A Thieleke1 and A May1
1Department of Systems Neuroscience, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Introduction: Dural nerve endings have been implicated in the pathogenesis of headache. Accumulating evidence in both animal and human models suggests that a proportion of the dural afferents project through the cranial sutures and innervate extracranial tissues, providing a possible link between the extra- and intracranial nociceptive systems and their potential role in headache generation. Furthermore, research is underway to determine whether blockade of sensitisation targeting the suture with botulinumtoxinA would be effective (and more efficient, i.e., at a lower dose) in reducing headache frequency compared to the standard approach. We therefore hypothesise that the suture is an important bridge for the communication between the extra- and intracranial nociceptive systems. Based on this, a direct stimulation of the scalp above the suture (as opposed to the non-suture region) would be more likely to induce dura stimulation, characterised by the presence of headache.
Objectives: Compare the incidence of headache when the scalp is stimulated directly over the sutures with the incidence of headache when the scalp is stimulated over a non-sutured area.
Methods: Two simulation protocols were applied to three independent cohorts of healthy participants: Cohort 1 received a subcutaneous injection of capsaicin solution, while cohorts 2 and 3 received topical electrical stimulation. The study employed a crossover design, and all participants received the stimulation at different scalp sites in randomised order at each appointment, one targeting the suture region (1 cm behind the bregma alone the midline, site A), the others non-suture regions (3 cm lateral to the site A, site B; forehead, site C; occipital region, site D). Cohort 3 was recruited after reviewing the results of cohorts 1 and 2 and with a slightly modified stimulus protocol. Headache occurrence was followed up for 24 hours after the experiment using a standardised protocol.
Results: Headache occurrence did not differ between stimulation sites in either cohort 1 or 2. In cohort 2, there is a trend towards higher headache occurrence at site A compared to site D (P = 0.058). Concerns about overstimulation were raised by the high rate of headache occurrence at both suture and non-suture sites in cohort 2. In cohort 3, a lower stimulation intensity was used and there was a trend for site A to be more likely to induce headache compared to site C (p = 0.067).
Conclusion: The study did not find a statistical difference between sutured and non-sutured sites in the incidence of headache. However, the existence of a trend raises at least two possibilities. First, the stimulation protocol may need to be refined to find the sweet point of the stimulus intensity to differentiate the two sites. Second, as the current study examined healthy controls, the difference may be more pronounced in a patient cohort, such as a migraine cohort. Finally, the differences between a trigeminal and a C2/C3 dermatome (site A vs site D) in headache initiation need further confirmation.
EP.43
Predictors of cranial autonomic symptoms in adults and children with migraine
P Amarasena1, R-J Wilcha1, P Soontrapa3, N Karsan1, K Nagaraj4, C Lastarria Perez5, S Ololade1, P Prabhakar6 and P Goadsby1
1King's College London, London, United Kingdom
2Ghent University Hospital, Ghent, Belgium
3Mahidol University, Thailand
4Swansea University Board, Wales, UK
5Vallesur - Auna Clinic, Arequipa, Peru
6Great Ormond Street Hospital for Children, London, UK
Introduction: Cranial autonomic symptoms (CAS) are well reported in migraine, although little is known about if and how they are predicted by other patient and symptom factors. Advancing this understanding may give insights into migraine neurobiology and therapeutic substrates.
Objectives: We set out to evaluate predictors of the number of CAS reported with migraine in both paediatric and adult clinical cohorts within our clinics.
Methods: Databases of chronic migraine extended phenotypes within the adult Headache service at King’s College Hospital between 2015 and 2020 (n = 622), and within the Children’s Headache Clinic at Great Ormond Street Hospital for Children between 2021 and 2022 (n = 76), were merged for a service evaluation. Patients without information on CAS were excluded. Migraine-associated symptoms were coded as dichotomous variables. Predictors of interest for the number of CAS reported: age, gender, allodynia, aura, baseline headache frequency and number of premonitory symptoms, were analysed within a Poisson regression model (IBM SPSS v 29). P < 0.05 was considered significant.
Results: The total sample size for analysis was n = 489, after excluding missing data . There were no outliers. Patients were aged 5-92 years (median 45, IQR 31-56), and the majority (83%) were female. At least one CAS associated with migraine was present in 74% (median 2, range 0-7, IQR 0-3). Within the regression model, the absence of aura negatively predicted CAS, whereas allodynia, increasing numbers of premonitory symptoms and increasing age positively predicted more CAS (Table).
Conclusions: Cranial autonomic symptoms (CAS) in chronic are common in both paediatric and adult patient groups. In line with our previous data, the reporting of more CAS is positively associated with allodynia. More CAS may present with advancing age, although reporting issues in younger populations should be considered. CAS may be associated with a more enriched migraine phenotype.

EP.44
Predictors of migraine-related allodynia in adults and children
P Amarasena1, R-J Wilcha1, P Soontrapa3, N Karsan1, N Vandenbussche2, K Nagaraj4, C Lastarria Perez5, S Ololade1, P Prabhakar6 and P Goadsby1
1King's College London, London, United Kingdom
2Ghent University Hospital, Ghent, Belgium
3Mahidol University, Thailand
4Swansea University Board, Wales, UK
5Vallesur - Auna Clinic, Arequipa, Peru
6Great Ormond Street Hospital for Children, London, UK
Introduction: Allodynia is a non-canonical symptom of migraine associated with higher disability
Objectives: We aimed to examine detailed phenotypic data from our adult and paediatric clinical cohorts for allodynia predictors in chronic migraine.
Methods: Databases of CM extended phenotypes within the adult Headache service at King’s College Hospital between 2015 and 2020 (n = 622), and within the Children’s Headache Clinic at Great Ormond Street Hospital for Children between 2021 and 2022 (n = 76), were merged for a service evaluation. Patients without information on allodynia were excluded. Migraine-associated symptoms were coded as dichotomous variables. Predictors of interest for the presence of allodynia: gender, vertigo, aura, photophobia, phonophobia and osmophobia, baseline headache frequency, number of premonitory symptoms, presence of cranial autonomic symptoms (CAS) and age categories, were analysed using a binary logistic regression model (IBM SPSS v 29). P < 0.05 was considered significant. Outliers with standardised residuals outside two standard deviations of the mean were excluded from the analysis.
Results: The sample size for analysis was n = 453, after excluding missing data and outliers. Patients were aged 5-92 years (median 45, IQR 31-56), and the majority (83%) were female. Allodynia associated with migraine was present in 59%. Within the regression model, the presence of osmophobia, vertigo, CAS and younger age positively predicted allodynia (Table).
Conclusions: Allodynia in chronic migraine is common in both young children and adults, and may be associated with a more enriched migraine phenotype independent of baseline headache frequency. We have previously reported the association with CAS with allodynia in children. Supportive evidence from adults, as well as the association with other sensory sensitivities alludes to the shared neurobiology of these symptoms.
Table

EP.45
Resting state high-density EEG analysis reveals subcortico-cortical linear and non-linear anomalies in migraine patients during the interictal period
G Sebastianelli1, C Porcaro2, S Gilli1, C Abagnale1, F Casillo1, G Di Lorenzo3 and G Coppola1
1Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Latina, Italy
2Department of Neuroscience (DNS) and Padova Neuroscience Center (PNC), University of Padova, Padova, Italy
3Chair of Psychiatry, Department of Systems Medicine, Tor Vergata University of Rome, Rome, Italy
Introduction: Clinical electrophysiology showed consistent functional changes in the brainstem-thalamus-cortex loop in migraine patients. Anomalies of cortical electroencephalographic (EEG) rhythmic activity, namely a decrease in alpha rhythms and an increase in slow delta-theta rhythms, characterize the migraine patient during the pain-free phase.
Objectives: This study aimed to determine whether these abnormalities are caused by defective linear and non-linear rhythmic pacemaker activity originating from the brainstem and projecting to the thalamus or are solely primary cortical abnormalities.
Methods: Forty-two migraine without aura (MO) patients, specifically during the interictal phase, and 42 healthy volunteers (HVs) underwent an eyes open resting state 64-channel EEG. Using the functional source separation approach (FSS), we employed four ad-hoc spatial functional constraints to isolate brain activity throughout the sensorimotor pathway. Specifically, we focused on extracting brain activity from two subcortical nodes (brainstem and thalamus) and two cortical nodes (primary sensory (S1) and primary motor (M1) areas). For each of the four sensorimotor nodes, we examined specific electrophysiological characteristics, such as spectral features and Higuchi's fractal dimension (FD), a non-linear measure of brain complexity.
Results: Compared to HVs, MO had significantly elevated FD values in the brainstem and thalamus in both the left and right hemispheres. No significant differences in FD values were observed between the two cortical nodes. When comparing MO with HVs, we observed an increase in the delta and a decrease in the alpha power spectral density in all four nodes of the sensorimotor system.
Conclusion: During the interictal periods of migraine patients, there is a disturbance in the linear and non-linear functioning of the brainstem and thalamic subcortical nodes in the sensorimotor system. This disturbance might result in alterations in the rhythmic patterns of the cortex.
EP.46
The Relationship between Premonitory Symptoms and Migraine Triggers: Preliminary results from a Headache Database
U Ashraf1,2,3 and S Tomlinson1,3
1St Vincent's Hospital, Sydney, Australia
2University of New South Wales, Sydney, Australia
3University of Notre Dame Australia, Sydney, Australia
Introduction: Migraine is a debilitating and common neurological disorder with many patients having a premonitory phase, headache phase, and postdrome phase of a migraine attack. Many migraine sufferers identify provoking factors for a migraine attack. The relationship between premonitory symptoms and migraine triggers is incompletely understood, with triggers potentially being conflated in some instances with what are actually premonitory symptoms e.g. a perceived migraine trigger of certain food may in fact reflect premonitory food cravings. The correlation between other combinations of reported triggers and premonitory symptoms have not been extensively explored and may provide further insights into the pathophysiology of the disease.
Objective: To identify an association between triggers and premonitory symptoms to inform neuroanatomical correlates in the hypothalamus.
Methods: A retrospective cohort study was performed on patients from the Headache Clinic at St Vincent’s Hospital Sydney. Data was collected from the clinical documentation of patients who visited the Headache Clinic since February 2024 and collated onto a secure REDCAP database. Patients migraine (ICHD-3 criteria) were included. Statistical significance was calculated by Fisher’s exact test and multivariate analysis by binomial logistic regression using XLSTAT.
Premonitory symptoms were defined as symptoms a patient with migraine experienced 1 hour to 24 hours prior to the headache phase of their migraine attacks.
Migraine triggers were defined as endogenous or exogenous factors that patient identified as increasing their chance of a migraine attack subsequently. Triggers that were screened for were less sleep, excess sleep, reduced stress/relaxation, increased stress, concurrent illness, certain foods, overcast weather, heat, dehydration, seasonal change, flying, physical exertion, missing meals and excess eating.
Results: 58 patients were identified as having a diagnosis of migraine. 43/58 (74%) had high frequency episodic migraine or chronic migraine (HFEM/CM) and 15/58 (26%) had episodic migraine (EM). 46/58 (79%) patients were female and 12/58 (21%) were male.
49/58 (84%) patients reported 3 or more premonitory symptoms. 38/43 (88%) patients with HFEM/CM reported 3 or more premonitory symptoms, compared to 11/15 (73%) patients with EM (p = 0.37).
All patients reported at least one trigger for their migraines. The five most commonly identified triggers were poor sleep in 48/58 (83%) patients, increased psychological stress in 45/58 (78%) patients, heat in 29/58 (50%) patients, physical exertion in 27/58 (47%) patients and dehydration in 27/58 (47%) patients. Table 1 displays the association between premonitory symptoms and triggers.
Conclusion: Certain premonitory symptoms are more likely to occur in conjunction with certain triggers. This lends evidence to the theory that patient-identified triggers may increase activation of certain parts of the hypothalamus (i.e. increased psychological stress increases paraventricular nucleus activation) and premonitory symptoms may arise due to activation of those specific parts of the hypothalamus (i.e. yawning is mediated by the paraventricular nucleus), this is demonstrated in Figure 1. The presence of certain premonitory symptoms on clinical history may therefore have predictive utility in identifying potentially avoidable or modifiable triggers for individual migraine sufferers and provides further insight into the role of the hypothalamus in migraine pathophysiology.


EP.47
Clustering Migraineurs using Functional Connectivity
J Sridhar1, M Babaei1, B Sanjanwala1, D DeSouza1, R Cowan1
1Department of Neurology and Neurological Sciences, Headache and Facial Pain Program, Stanford University, United States of America
Introduction: Migraine is a complex, heterogeneous disorder currently subtyped based solely on clinical symptoms, which may not fully inform effective treatment. Integrating brain function with clinical characteristics may improve our understanding of migraine pathophysiology and optimize treatment strategies.
Objectives: To identify subtypes of individuals with migraine based on resting-state brain functional connectivity using a data-driven approach, and to describe the clinical characteristics of the resulting groups.
Methods: Participants with migraine and healthy controls were recruited for Stanford University's Headache Study. The migraine group was defined according to the International Classification of Headache Disorders (ICHD-3). Participants underwent structural and functional MRI scans using a 3 T GE scanner and reported headache characteristics including frequency and intensity and completed a detailed questionnaire on clinical features. After excluding those with MRI issues and incomplete data, 128 individuals with migraine and 25 controls without migraine were included in the analysis.
Structural scans were pre-processed using FreeSurfer (v7.4.1) and functional scans using fMRIPrep (v23.2.0). This included motion correction, slice-timing correction, alignment to anatomical and frame-wise displacement (FD) estimation. Post-processing with XCP-D (v1.8.6) involved removing initial non-steady volumes, filtering outliers at FD = 0.5, despiking, and bandpass filtering (0.01–0.1 Hz). Regressors included the top five principal components from white matter and cerebrospinal fluid, six motion parameters, and mean global signal. Timeseries were extracted using the Schaefer atlas for 17 networks from 100 regions-of-interest (ROIs). ROIs in the limbic network were excluded due to signal loss. Functional connectivity (FC) for the remaining 15 networks was computed using Pearson’s r and transformed to Fisher’s z. Hierarchical agglomerative clustering was applied to the FC matrices of 128 migraine participants, identifying two optimal clusters via Silhouette scores. Average FC matrices from the control group were used for comparison. Connectivity differences between migraine clusters and controls across networks were assessed with t-tests and corrected for multiple comparisons using False Discovery Rate. Clinical measures were also evaluated for the clusters.
Results: Two distinct clusters of migraine participants were identified based on resting-state brain connectivity. Compared to controls (Fig. 1C), Cluster 1 (n = 12) exhibited a significant increase in connectivity in control and attention networks (Fig. 1B), while Cluster 0 showed no significant differences (Fig. 1A). While there were no statistically significant differences in headache characteristics and clinical measures between the clusters (Table 1), participants in Cluster 1 tended to experience more frequent and intense headaches and had lower depression and anxiety scores compared to those in Cluster 0.
Conclusions: This study identified distinct resting-state FC patterns in a subset of migraine participants that did not correspond to the ICHD-3 binary separation between episodic and chronic migraine but demonstrated no significant links to a specific clinical profile. Cluster 1, a smaller group, needs more data for validation. The relationship between brain networks and symptoms in migraine is complex, and clinical features alone do not fully explain the observed resting-state connectivity. Future clustering approaches will include volumetric and diffusion metrics to better identify migraine subgroups and understand their mechanisms.
Figures 1A, 1B, 1C,1D


EP.48
Contralateral insula and bilateral superior temporal lobes integrate trigeminal somatosensory processing into perceptual determination of pain
K Peng1, J Mehnert1 and A May1
1Department of Systems Neuroscience, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Introduction: Pain, as a subjective experience, transcends the mere activation of the somatosensory system. The so-called pain matrix, comprising somatosensory, insula, and cingulate areas, might be better described as a salience matrix, since its activation pattern does not differ from those observed in non-painful somatosensory, auditory, or visual stimulations. Understanding which region of the brain is determining an incoming sensory input as painful is nevertheless crucial to understanding pain itself. The neuronal process involved may further play an important role in chronic pain conditions, where nociceptive input from the periphery is no longer present. A limited number of studies employing functional neuroimaging have implicated the insula as crucial in pain determination, with the anterior insula being more involved in pain determination while the posterior insula being more involved in pain intensity assessment. However, these studies need replication, and it remains largely unknown whether here the trigeminal nociceptive system functions differently than the extracranial somatosensory system and whether headache disorders like migraine influence this system.
Objectives: We aimed to identify the brain regions responsible for pain determination within a trigeminal nociceptive model.
Methods: Two study cohorts were recruited, a migraine cohort (n = 10) and an age- and sex-matched healthy control cohort (n = 13). Both cohorts underwent functional MRI (fMRI) daily for 7–11 consecutive days to ensure that the migraine cohort would eventually experience migraine attacks. Each day during the experiment, subjects had their forehead electrical pain threshold determined, followed by event-based fMRI using electrical forehead stimulation at the intensity of the day’s pain threshold. The stimulation was repeated 120 times, with the subject rating each trial either as painful or as non-painful.
Results: A total of 85 days of fMRI experiments were recorded in the migraine cohort and 91 days in the healthy control cohort. On average, the migraine cohort perceived 48.1 ± 10.5% of the stimuli as painful, while the control cohort perceived 46.1 ± 10.0% as painful, given the functional definition of a pain threshold of being 50% painful (and 50% non-painful). Both painful and non-painful trials represented the same intensity (at the threshold level) of the incoming stimuli and activated the somatosensory networks, including the ipsilateral spinal trigeminal nucleus, contralateral thalamus. Comparison between painful and non-painful trials revealed greater activation in contralateral anterior and posterior insula as well as in bilateral superior temporal lobes during painful trials independent of the group (healthy controls or migraine patients).
Conclusions: The findings provide evidence that the contralateral insula and bilateral superior temporal lobes integrate incoming trigeminal somatosensory processing into the perceptual decision of pain. This process appears to be similar in both migraine patients and healthy controls.
EP.49
Evaluation of perivascular and extracellular space properties in migraine: a potential index for glymphatic clearance
R Messina1,2, E Pagani2, F Genovese1,2, I Cetta1,2, L Zanandrea1,2, B Colombo2, M Rocca1,2 and M Filippi1,2
1Vita-Salute San Raffaele University, Milan, Italy
2IRCCS San Raffaele Hospital, Milan, Italy
Introduction: The glymphatic system is a network of perivascular spaces (PVS) that facilitates fluid exchange and peptide clearance in the brain.
Objectives: To investigate if glymphatic dysfunction contributes to migraine pathophysiology using a comprehensive approach, and examine its variations between patients studied during the interictal phase and those studied while experiencing headache.
Methods: One hundred twenty migraine patients (95 interictal, 25 with headache) and 52 controls underwent diffusion tensor (DTI) and susceptibility weighted (SWI) magnetic resonance imaging. Using DTI and SWI, we computed the Diffusion Along Perivascular Space (DTI-ALPS) index, reflecting diffusivity in the PVS near the left lateral ventricle. This index serves as a proxy for regional glymphatic function. Based on previous evidence showing an association between glymphatic function and changes within intra/extracellular compartments, we employed neurite orientation dispersion and density imaging to evaluate voxel-wise maps of white and grey matter extracellular (EVF) and intracellular (IVF) volume fraction. Thus, providing a comprehensive insights into the glymphatic system functioning. Age- and sex-adjusted between-group comparisons were run using R, FSL and SPM12 software.
Results: Compared to controls, migraine patients were older (mean age: patients 39 (12), controls 36 (14), p = 0.02) and had a higher proportion of female subjects (female: patients 82, controls 23, p = 0.004). We found no significant differences between patients and controls, neither concerning the DTI-ALPS index nor regarding the white and grey matter EVF and IVF. No differences were even observed between migraine patients studied while experiencing headache and those in the interictal phase.
Conclusion: These results suggest the absence of abnormalities in the PVS and the white and grey matter extracellular compartment, indicating normal functioning of the glymphatic system in people with migraine, both during the interictal and the headache phase.
EP.50
Diagnosis and management of IIH and IIHWOP in chronic headache
K Patwardhan1 and D Kulkarni1
1Neuro one brain and spine center, Miraj, India
2Anil Kulkarni eye hospital, Miraj, India
Introduction: Headache is the second leading cause of disability after stroke. The pseudotumor cerebri syndromes are disorders with raised intracranial pressure and headache. Idiopathic intracranial hypertension is the commonest cause and affects women of childbearing age who are obese. Most of the times they present with papilledema but a subset of these IIH patients do not have papilledema and are termed IIH without papilledema (IIHWOP) by recent classification. It remains to be understood whether the classification and management of IIHWOP is like IIH as both patients are phenotypically similar.
Objectives: To study the prevalence, presentation, and management of IIHWOP in phenotypically classified IIH patients.
Methods: This is a prospective observational study of three years Patients with chronic disabling headache, and with raised ICP were evaluated with lumbar puncture and CSF opening pressure, ophthalmologic evaluation, and Optical Coherence Tomography; MRI brain with venography. CSF drainage was done in all patients with ICP > 250mmH20. IIHWOP was defined according to Friedman's diagnostic criteria. A 6 month follow up study was done.
Results: 36 patients were enrolled. All patients had history of chronic headache and raised ICP on lumbar puncture. Study included 31 females (86.1%) and 5 males (13.9%). Mean age at presentation was 38 ± 6.6 years. Average BMI was 38.2 kg /m2. 22 patients (61%) had CSF opening pressure > 220 mmH2O, 9 patients (39%) had > 280 mmH2O. 19((52.7%) patients had neuroimaging findings suggestive of elevated ICP. Papilledema (Frisen grading) was seen in 33((91.6%) patients. Out of 36, 29 had visual field defects. Three (9.3%) patients met the newly proposed diagnostic criteria by Friedman for IIHWOP. Of the three IIHWOP patients, one had sixth nerve palsy, one had imaging features of raised ICP with enlarged blind spot on field charting and one patient had just transient visual obscuration. Two (5.55%) out of 36 patients had recurrent IIH out of which one was IIHWOP confirmed on repeat LP and CSF pressure testing. All the patients were managed by LP and CSF drainage, mannitol, acetazolamide and topiramate. Weight reduction was the mainstay of treatment.
Conclusions: Majority of patients with IIH present with headache and papilledema. A small subset of patients presents without papilledema termed as IIHWOP. Although IIHWOP is a rare clinical condition it should be considered in patients with chronic refractory headache and CSF pressure testing should be done in appropriate patients. Further evaluation of IIHWOP is needed as both conditions are typically seen in young obese females and respond to the same treatment regimen. Though they do not have papilledema, they tend to have other signs of raised ICP like TVO, sixth nerve palsy and MRI abnormalities. Anatomical differences in optic nerves and the threshold at which papilledema develops may be different in IIHWOP group of patients. Patients of both IIH and IIHWOP can have recurrence. The current nosological position of IIHWOP needs further exploration and research.
Glossary- IIH- Idiopathic intracranial hypertension.
IIHWOP-Idiopathic intracranial hypertension without headache
ICP-Intracranial pressure
LP-CSF-Lumbar puncture cerebrospinal fluid
BMI-body mass index
TVO-transient visual obscuration

MO.01
Efficacy and safety of eptinezumab in patients with episodic cluster headache (ALLEVIATE): A randomized placebo-controlled trial
R Jensen1, S Tepper2, A Charles3, P Goadsby3,4, C Tassorelli5, N Boneva6, A Snoer6, M Josiassen6, C Linander6, A Ettrup6 and B Sperling6
1Danish Headache Center, Department of Neurology, Rigshospitalet-Glostrup, University of Copenhagen, Copenhagen, Denmark
2New England Institute for Neurology and Headache, Stamford, United States
3UCLA Goldberg Migraine Program, Department of Neurology, David Geffen School of Medicine at UCLA, Los Angeles, United States
4NIHR King’s Clinical Research Facility and Headache Group, King’s College London, London, United Kingdom
5Department of Brain and Behavioral Sciences, University of Pavia, National Institute of Neurology C. Mondino Foundation, Pavia, Italy
6H. Lundbeck A/S, Copenhagen, Denmark
Introduction: Episodic cluster headache (eCH) is a highly disabling primary headache disorder consisting of cluster periods (bouts) composed of series of 15–180-minute attacks of excruciating pain occurring near-daily to multiple times daily and attack-free remission periods (≥3 months). Cranial autonomic symptoms and agitation often occur during the attacks. Eptinezumab is a humanized monoclonal antibody directed against calcitonin gene-related peptide and is approved for preventive treatment of migraine.
Objectives: To evaluate the efficacy, safety, and tolerability of eptinezumab in patients with eCH.
Methods: ALLEVIATE (NCT04688775) was an interventional, multi-region, randomized, double-blind, placebo-controlled, delayed-start study. Adults with eCH (based on the International Classification of Headache Disorders, 3rd edition) and a history of cluster period(s) lasting ≥6 weeks were randomized (1:1 ratio) to one of two initial treatments: eptinezumab 400 mg or placebo, administered intravenously. Patients initially receiving placebo received eptinezumab 400 mg at Week 4 and vice versa. This analysis presents the results from the initial 4-week, randomized, placebo-controlled phase. The primary endpoint was the change from baseline in the number of weekly attacks over Weeks 1–2. Additional endpoints included ≥50% reduction from baseline in the number of weekly attacks (“≥50% response”) and Patient Global Impression of Change (PGIC) score (from 1 = very much improved to 7 = very much worse).
Results: A total of 231 patients were enrolled and randomized to receive eptinezumab 400 mg (n = 113) or placebo (n = 118) at baseline. Patients were mostly male (eptinezumab, 76%; placebo, 79%); mean age was 44 years (both arms) and mean time since CH diagnosis was 10.5 (eptinezumab) and 9.5 (placebo) years. At baseline, patients reported a mean of 15.3 (eptinezumab) and 15.7 (placebo) CH attacks per week. The change from baseline in number of weekly attacks over Weeks 1–2 was ‒4.0 with eptinezumab and ‒4.6 with placebo (P = 0.5048). Due to a lack of statistical significance in the primary endpoint, all other P-values are considered descriptive and not controlled for multiplicity. More eptinezumab-treated patients achieved ≥50% response over Weeks 2, 3, and 4 (50.9%, 62.5%, and 66.7%, respectively) compared with placebo (37.3%, 48.3%, 50.5%; P < 0.05). Similarly, mean PGIC scores showed greater improvements with eptinezumab, with mean scores of 2.9 (eptinezumab) versus 3.4 (placebo) at Week 2 (P = 0.0061) and 2.9 (eptinezumab) versus 3.2 (placebo) at week 4 (P = 0.0681). The number of treatment-emergent adverse events (TEAEs) was similar between eptinezumab 400 mg and placebo, and the most commonly reported TEAEs were similar to those observed in previous eptinezumab trials in migraine.
Conclusion: In the placebo-controlled period of the ALLEVIATE study in eCH, eptinezumab did not separate from placebo on the primary endpoint of attack frequency. However, patients treated with eptinezumab demonstrated higher ≥50% responder rates and perceived better disease improvement than patients who received placebo. Eptinezumab was generally well tolerated in patients with eCH, with no new safety signals observed compared to migraine trials with eptinezumab.
MO.02
The effect of an injection with methylprednisolone and lidocaine around the greater occipital nerve on the R2 component of the blink reflex and the clinical response in patients with episodic and chronic cluster headache
W Naber1, P van Tilborg1, R Brandt1, E van Kemenade1, G Terwindt1 and R Fronczek1
1Lumc, Leiden, Netherlands
Objectives: To explore the impact of a Greater Occipital Nerve (GON) injection, containing both an anesthetic and a corticosteroid, on the nociceptive blink reflex; and assess its potential correlation with clinical response, in both episodic and chronic cluster headache.
Methods: In this single-center, prospective cohort study, participants with episodic (n = 17) and chronic cluster headache (n = 16) were followed for 12 weeks post-GON injection with daily headache diaries and blink reflex measurements at four timepoints: 30 minutes before injection and 30 minutes, one week, and four weeks post-injection. The primary outcome was the R2 latency. A secondary outcome was the area under the curve (AUC) of the blink reflex. Primary and secondary outcomes were compared using linear mixed models.
Results: Except for a decrease in the R2 latency ipsilateral to the injection side four weeks after the GON injection, no differences of the R2 latencies were observed. A reduction of both mean attack frequency (MAF) and intensity were seen after treatment with a GON-injection. Lower MAF were observed on week one and week four compared to baseline (1.0 vs. 2.0; 95%CI: 0.90 to 2.36; P < 0.001; 0.4 vs. 2.0; 95%CI: 1.26 to 2.86; P < 0.001). 75.8% (25/33) of participants had ≥30% reduction of their cluster headache attacks and 27.3% (9/33) was attack-free at week four. The AUC increased in week one and four compared to baseline (73363.5 vs. 58445.3 μVms, P = 0.036; 73363.5 vs. 58445.3 μVms; P = 0.006). No correlation between the R2 latencies or AUC and the clinical response were observed.
Conclusion: Although clinically effective, the mechanism of action of a GON-injection in cluster headache remains enigmatic. Our results suggest a more complicated interplay than just an altered sensitivity of the trigeminal system.
Image 1

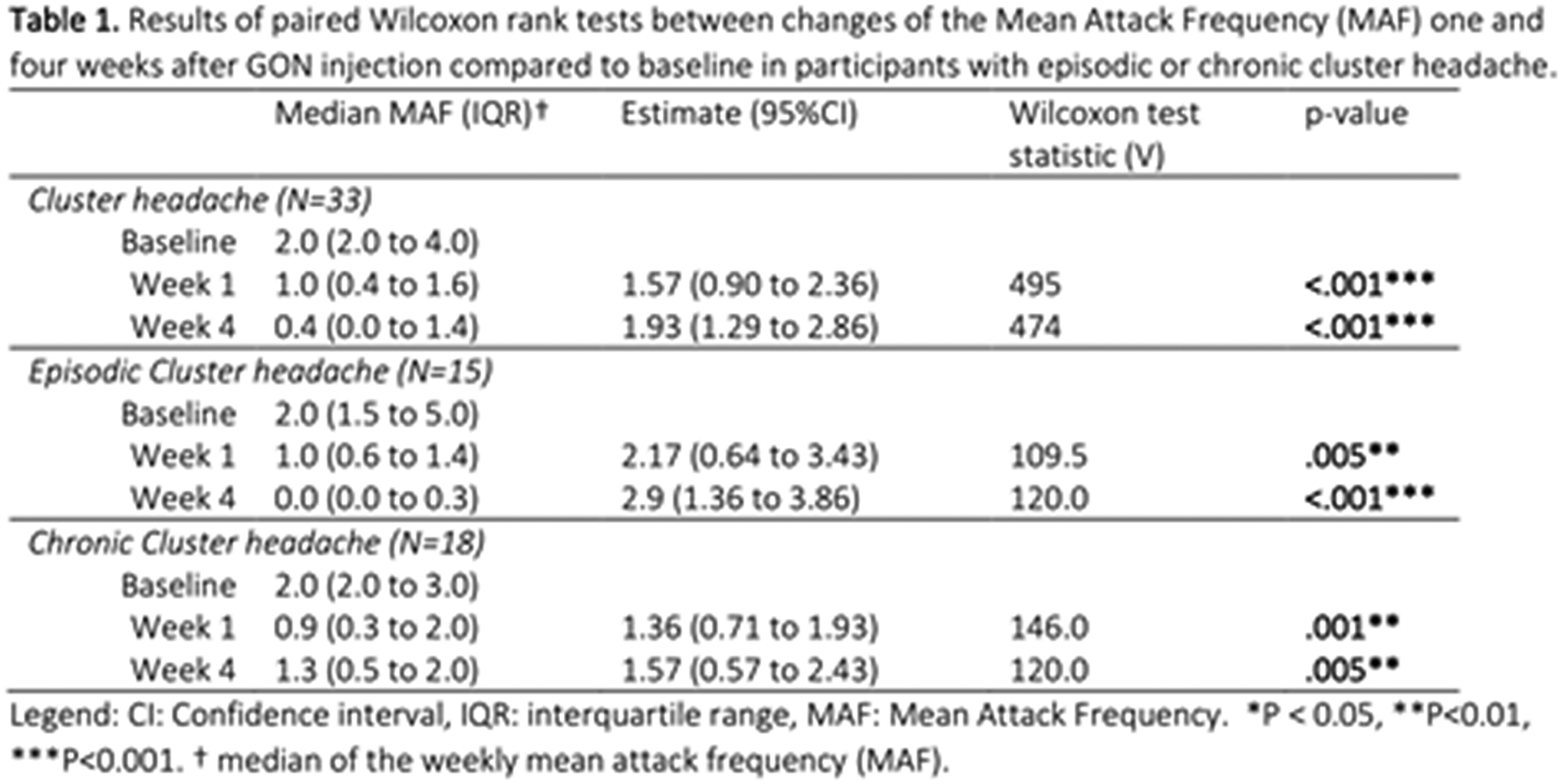
MO.03
Role of specific microRNAs in cluster headache: correlation with disease phenotype and neuropeptide levels
F Cammarota1, R De Icco1,2, F Bighiani1,2, M Corrado1,2, G Vaghi1,2, A Antoniazzi1,2, E Mazzotta1,2, V Grillo1,2, R Greco2, C Demartini1,2, A Zanaboni1,2, M Francavilla1,2, M Allena2, G Sances2 and C Tassorelli1,2
1Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
2Headache Science and Neurorehabilitation Unit, IRCCS Mondino Foundation, Pavia, Italy
Introduction: The role of specific microRNAs was studied in episodic and chronic migraine, but their possible involvement in cluster headache is yet to be elucidated.
Objectives: Our objective is to evaluate the role of specific microRNAs in episodic cluster headache in active phase (AeCH), remission phase (ReCH), chronic cluster headache (cCH), and healthy controls (HCs).
Methods: In this cross-sectional study, we assessed gene expression of miR-382-5p, miR-34a-5p, and miR-155 in peripheral blood mononuclear cells (Relative Quantification). AeCH and cCH patients were assessed outside of an acute cluster headache attack.
Results: We enrolled 18 AeCH (45.7 ± 12.8 years, 14 males, 16.3 ± 9.6 attacks/week), 7 ReCH (48.6 ± 19.8 years, 5 males), 10 cCH (50.1 ± 16.2 years, 9 males, 21.4 ± 18.8 attacks/week), and 14 HCs (45.4 ± 15.2 years, 2 males). miR-382-5p expression was higher in AeCH (1.7 ± 0.8) when compared to ReCH (0.8 ± 0.2) and HCs (0.3 ± 0.1) (p < 0.005 for all comparisons). miR-34a expression was higher in AeCH (1.7 ± 0.4) when compared with ReCH (1.0 ± 0.3), cCH (1.2 ± 0.3) and HCs (0.5 ± 0.2) (p < 0.001 for all comparisons). miR-155 expression was lower in HCs (0.4 ± 0.1) compared to all CH subgroups (p = 0.001 for all comparisons), with no difference among AeCH (1.7 ± 0.5), ReCH (1.3 ± 0.3) and cCH (1.3 ± 0.5).
Conclusion: miR-382-5p, miR-34a-5p and miR-155 expression is increased in cluster headache when compared to HCs. MiR-382-5p and miR-34a-5p were associated with disease activity, being higher in AeCH patients when compared to ReCH. MicroRNAs expression of cCH was in-between active and remission phases of episodic cluster headache patients. Our data supports the role of specific microRNAs in the pathophysiology of different primary headaches.
MO.04
Comparison between spontaneous and triggered premonitory symptoms in CH and migraine
A Gonzalez-Martinez1,2, D Wei2, N Karsan2, K Nagaraj2, H Gosalia2 and P Goadsby1,3
1Hospital Universitario de la Princesa & Instituto de Investigación Sanitaria Princesa (IIS-Princesa), Madrid, Spain
2NIHR King’s Clinical Research Facility and Wolfson SPaRC King’s College London, London, United Kingdom
3Department of Neurology, University of California, Los Angeles, CA, USA
Introduction: Cluster headache (CH) and migraine are both debilitating primary headache disorders often accompanied by premonitory symptoms. To date, the literature on the evaluation of premonitory symptoms in CH is less extensive compared to that on migraine. Additionally, comparisons between spontaneous and triggered premonitory symptoms in these conditions are scarce.
Objectives: This study investigates the prevalence and characteristics of spontaneous and nitroglycerine (NTG) triggered premonitory symptoms in patients with CH and migraine (‘experimental CH cohort’ and ‘experimental M cohort’).
Methods: A comparative study was conducted to investigate the presence, type of premonitory symptoms and agreement between spontaneous and triggered data collected from ‘experimental CH cohort’ and ‘experimental migraine cohort’. The study was performed at a Headache Unit of a tertiary hospital specialized in CH treatment, following a detailed phenotyping of spontaneous CH and migraine premonitory symptoms as per included in our previous work.
Results: A total of 12 patients with CH and 12 age and sex-matched patients with migraine were included in this study. The proportion of spontaneous and NTG-triggered-premonitory neck stiffness, mood changes and yawning among ‘experimental CH cohort’ and ‘experimental migraine cohort’ was similar. The total number of spontaneous premonitory symptoms was higher in the ‘experimental migraine cohort’ compared to ‘experimental CH cohort’ (P-value < 0.001) although there were no differences in the number of premonitory symptoms in the triggered CH cohort compared to the migraine cohort.
Conclusion: These findings highlight the significant presence and similar type of premonitory symptoms in both CH and migraine patients, regardless of the spontaneous or triggered nature of the symptoms. These results suggest that premonitory symptoms in patients with CH and migraine may be influenced by common changes in areas of the brain controlling arousal, cognition, and homeostasis. The study underscores the need for further exploration into the mechanisms behind these premonitory symptoms, which may provide insights into the pathophysiology of CH and migraine, potentially guiding future therapeutic strategies.
MO.05
Effect of invasive vagus nerve stimulation in a patient with both chronic cluster headache and focal epilepsy - A Case Report
P van Tilborg1, A Bosch2, R Thijs1,2 and R Fronczek1,2
1Department of Neurology, Leiden University Medical Centre (LUMC), Leiden, The Netherlands
2Stichting Epilepsie Instellingen Nederland (SEIN), Heemstede, The Netherlands
Introduction: Current treatment options for chronic cluster headache (CCH) are often insufficient. Non-invasive vagus nerve stimulation (nVNS) has been shown to be effective as an acute treatment in episodic cluster headache. However, this effect was not observed in CCH. Two less-controlled studies indicated a potential preventive effect of nVNS in CCH. The effect of invasive vagus nerve stimulation (VNS) has not been studied in CCH.
Objective: To report the clinical effect of an implanted vagus nerve stimulator in a single patient with CCH.
Methods: We report on a 71-year-old male who had been diagnosed with CCH in 1965. The attacks still fulfil the ICHD-3 criteria for cluster headache, presenting as an extreme left-sided orbital stabbing pain accompanied by autonomic symptoms. In the past decade the patient typically suffered one or two CCH attacks per day. He uses nasal or subcutaneous sumatriptan as abortive treatment. He did not tolerate prophylactic medication.
In addition to CCH, he was diagnosed with right frontotemporal focal epilepsy. This was proven using ictal video electroencephalography recording and subsequently treated with cenobamate and pregabaline. In June 2023 a vagus nerve stimulator was implanted as treatment for the refractory epilepsy. Following surgery, the VNS duty cycle was increased per standard treatment protocol for epilepsy. Medication dosages were not altered post-implantation.
Results: Three months following VNS implantation the cluster headache attack frequency had decreased from seven to three attacks per week. Five-months following implantation, only one weekly cluster headache attack remained. This decrease in attack frequency was still present during the last follow-up in May 2024. Interestingly, when the VNS was temporarily deactivated due to an unrelated minor surgery in September 2023, the patient reported an increase in cluster headache attack frequency. Once the VNS was reactivated five days later, the attack frequency decreased again.
Conclusion: In this case, vagus nerve stimulation lead to a considerable decrease in weekly CCH attack frequency. While natural disease course or a placebo effect cannot be excluded, the continued effect almost one year post-surgery in a patient who’s suffered daily attacks since childhood suggests that the decreased weekly attack frequency can at least partly be contributed to vagus nerve stimulation. This is further supported by the change in attack frequency during the temporary deactivation of the VNS. As CCH patients are in need of more treatment options, additional research into the effect of vagus nerve stimulation as preventative treatment for CCH could be beneficial.

MO.06
Analysis of MRI-based microstructural and functional resting-state network correlation: insights into the activity of the hypothalamic-thalamo-cortical network in patients with episodic cluster headache
C Abagnale1, A Di Renzo2, G Giuliani3, G Sebastianelli1, F Casillo1, C Di Lorenzo1, F Caramia3, V Di Piero3 and G Coppola1
1Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Latina, Italy
2IRCCS – Fondazione Bietti, Rome, Italy
3Department of Human Neurosciences, Sapienza University of Rome, Rome, Italy
Introduction: Neuroimaging studies have shown that the hypothalamus and other distant brain regions, belonging to complex cerebral networks, are involved in generating pain in cluster headache (CH). However, the exact relationship between these areas, which may be somewhat dependent or independent, is not yet understood.
Objectives: We searched for differences in resting-state functional connectivity (FC) between brain networks and its relationship with the microstructure of the hypothalamus and the thalamus between episodic CH patients during the bout and healthy controls (HCs).
Methods: We collected 3 T MRI data from 26 patients with CH between attacks and compared them with data from 20 HCs. We collected resting state data among independent component (IC) networks. We calculated fractional anisotropy (FA), mean (MD), axial (AD), and radial (RD) diffusivity values of the hypothalamus and bilateral thalami and correlated them with resting state ICs Z-scores and CH clinical features.
Results: Patients with CH had less FC between the salience network and the left executive control network (ECN) than HCs, but more FC between the default mode network and the right ECN. CH patients showed lower FA and higher MD, AD, and RD microstructural hypothalamic metrics than those of HCs. CH patients had a higher bilateral FA metric of the thalamus than HCs. AD and RD diffusivity metrics of the hypothalamus correlated positively with the duration of disease history. We found no correlations between hypothalamus and thalamus diffusivity metrics and cortical networks’ FC.
Conclusion: The present findings provide the first evidence that abnormal intra-network connectivity at rest, associated with significant differences in thalamic and hypothalamic microstructure, may independently have a role in the pathophysiology of cluster headaches.
MO.07
Efficacy and safety of Lu AG09222 for migraine prevention in patients with 2–4 previous preventive treatment failures: HOPE, an interventional, randomized, double-blind, parallel-group, placebo-controlled phase 2 trial
M Ashina1,2, R Phul3, M Khodaie3, E Löf3 and I Florea3
1Department of Neurology, Danish Headache Center, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
3H. Lundbeck A/S, Copenhagen, Denmark
Introduction: A potential new route for the treatment of migraine is the targeting of pituitary adenylate cyclase-activating polypeptide (PACAP), a signaling molecule believed to play a key role in migraine pathogenesis. Lu AG09222 is a humanized monoclonal antibody targeting the PACAP ligand and may therefore be able to prevent migraine attacks.
Objectives: This proof-of-concept trial of Lu AG09222 (HOPE) was designed to assess the efficacy, safety, and tolerability of a single intravenous infusion of Lu AG09222 for migraine prevention in adults with migraine for whom 2-4 prior preventive treatments failed to benefit.
Methods: HOPE was an interventional, randomized, double-blind, parallel-group, placebo-controlled phase 2 trial (NCT05133323). Participants were adults (18–65 years) diagnosed with migraine (episodic or chronic) and with documented failure of 2–4 previous preventive migraine treatments. The trial consisted of a 4-week double-blind treatment period and an 8-week double-blind follow-up period. Participants recruited from specialist settings in Europe and North America were randomized (2:1:2) to receive a single-dose intravenous infusion of Lu AG09222 high dose, Lu AG09222 low dose, or placebo. The primary efficacy endpoint was the mean change from baseline in the number of monthly migraine days (MMDs) over weeks 1–4 for the high dose of Lu AG09222.
Results: A total of 237 participants were randomized and treated (Lu AG09222 high dose, n = 97; Lu AG09222 low dose, n = 46; placebo, n = 94). Participants were 87.8% female with a mean age of 42.5 years and 16.7 MMDs at baseline. This trial met the primary endpoint: the mean change from baseline over weeks 1–4 in MMDs was −6.2 (standard error [SE] 0.66) with Lu AG09222 high dose and -4.2 (SE 0.67) with placebo, corresponding to a difference from placebo with Lu AG09222 high dose of 2.0 (90% confidence interval: −3.5, −0.6; one-sided p = 0.01). Lu AG09222 was generally well tolerated, with no safety concerns observed in this trial.
Conclusion: This proof-of-concept trial demonstrated that Lu AG09222 can be a potential treatment for migraine prevention. In this trial, Lu AG09222 was well tolerated.
MO.08
Practice variation in United Kingdom (UK) neurology management of episodic migraine
R Khan1, J Bernard2, S Thakerar2, A Williams2 and F Ahmed1
1Hull University Teaching Hospital NHS Trust, Hull, UK
2AbbVie, Maidenhead, UK
Introduction: Migraine is the second leading cause of years lived with disability, however it remains under-diagnosed and not optimally treated in some cases.¹ This piece of research aims to better understand the current standard of practice and explore the variabilities in episodic migraine patient management within the United Kingdom (UK).
Objectives: Assess current UK practices in episodic migraine patient pathway and understand barriers to following latest guidelines in neurology.
Methods: UK neurologists experienced in treating episodic migraine patients participated in a structured online survey between Nov-Dec 2023. Findings were analysed using simple descriptive statistics.
Results: The survey was completed by 74 UK neurologists seeing an average of 79 migraine patients per month. 38% respondents reported more than 60% referrals being inappropriate mainly attributed to lack of effective communication with primary care.
Although majority of respondents refer to the UK National Institute for Health and Care Excellence (NICE) (73%), British Association for the Study of Headache (BASH) (57%) and UK regional (47%) guidelines for their management of episodic migraine, they felt a lack of timely updates, funding constraint and lack of capacity due to staff shortages were the main barriers for implementation.
Majority of respondents were familiar with the newer therapies Calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) (82%) and gepants (74%), but only 30% reported prescribing CGRP mAbs ‘often’ and ‘very often’ to their episodic migraine patients, despite being NICE recommended.
Conclusion: The management of episodic migraine varies regionally in the UK. Despite NICE approval, few eligible patients receive newer therapies. Funding and resource constraint, along with inappropriate referrals from primary care were the main reasons for variability in care.
References
1. NHS. RightCare: Headache & Migraine Toolkit. Optimising a headache and migraine System. December 2019
MO.09
Effectiveness and predictors of response of intravenous dihydroergotamine in the treatment of primary headache disorders – A service evaluation
P Amarasena1,2, F Greenwood2 and P Goadsby1,3,4
1Wolfson Sensory Pain and Regeneration Centre, Institute of Psychiatry, Psychology & Neuroscience, King’s College London, London, United Kingdom
2King's College Hospital, London, United Kingdom
3NIHR-Wellcome Trust King's Clinical Research Facility, King's College London, London, United Kingdom
4Department of Neurology, University of California, Los Angeles, USA
Background: Dihydroergotamine (DHE) has been used to treat headache for nearly eighty years. We aimed to evaluate the effect and predictors of response to our DHE infusion protocol.
Methods: Data including demographics, clinical information, DHE dose, side effects, medications and response to DHE of 160 successive DHE admissions were collected from clinic letters and discharge summaries as part of a service evaluation. The response to DHE was categorized by patients on an ordinal scale: complete, good, partial and nil. Generalized linear logistic regression modelling was employed, with response to DHE as an ordinal dependent variable and a cumulative logit link function, to identify predictors of outcome. Significance level was set at P < 0.05.
Results: Data from 160 hospital admissions for DHE from 131 patients were analysed. Their median age was 47 years and 72.5% were females. Only active primary headaches were considered for analysis: 82 (63%) had migraine, 11 (8%) had cluster headache (CH), 3 (2%) had hemicrania alternans (HA) and 30 (23%) had new daily persistent headache (NDPH), while 5 (4%) had both migraine and CH. The median DHE dose was 11.25 mg.
Of the patients, 47 with migraine (54%), 13 with CH (81%), 10 with NDPH (33%) and 1 (33%) with HA had a response to DHE. The most common adverse effects were nausea (controlled – 45%, uncontrolled – 10%), muscle cramps (47%) and headache exacerbation (16%). A model considering all patients predicted response (X2 = 24.561, P < 0.011). Compared to migraine, DHE was more effective for CH (OR = 4.436, X2 = 6.417, P = 0.011) and less effective for NDPH (OR = 0.344, X2 = 5.616, P = 0.018). The model considering all DHE admissions (X2 = 57.630, P < 0.001) showed absence of nausea was associated with a better outcome than uncontrolled nausea (OR = 6.616, X2 = 7.638, P = 0.006), while muscle cramps predicted a better response (OR = 2.076, X2 = 4.609, P = 0.032).
Conclusion: DHE by infusion over five days is an effective treatment for primary headache disorders, especially for CH. Adequate control of nausea is essential for a better response and muscle cramps may predict a better outcome.
MO.10
Switching from ligand to receptor CGRP-mAb or vice versa in non-responders: A Controlled Cohort Study
N Van Veelen1, B van der Arend1, E Hiele1, E van Zwet1, G Terwindt1
1Leiden University Medical Center, Leiden, Netherlands
2Erasmus MC, Rotterdam, Netherlands
Background: Limited options exist for migraine prevention after stopping anti-calcitonin gene-related peptide monoclonal antibodies. A systematic review examining the benefits of switching between different classes (ligand versus receptor mAb) is essential, alongside well-designed real-world-studies.
Methods: In this controlled cohort study, we included 67 patients, who discontinued their first treatment with erenumab or fremanezumab. Patients (n = 31) switched to another monoclonal antibody class within 3 months, while those in the control group (n = 36) received standard care. Allocation to either group relied largely on the availability of alternate monoclonal antibody treatments, introducing pseudorandom allocation. Changes in monthly migraine days were compared between groups three months post-discontinuation of the first monoclonal antibody or initiation of a different monoclonal antibody class. A multivariate regression model was conducted that accounted for potential confounding factors.
Results: The groups were comparable at baseline and poor treatment response was the main reason for treatment discontinuation of the first monoclonal antibody. The switching cohort experienced a −3.9 monthly migraine days reduction (95% CI [−6.4, −1.3], p = 0.004) versus the control group.
Conclusion: Transitioning to a different anti-calcitonin gene-related peptide monoclonal class yields reduction in monthly migraine days compared to returning to standard care for patients with inadequate initial treatment response.

MO.11
OnabotulinumtoxinA (Botox) for Chronic Migraine during pregnancy; experience from Hull (UK) headache clinic over 12 years
F Ahmed1,2,3, R Khan1, S Dorsey1,3, M Khalil3 and H Delrosario1
1Hull University Teaching Hospitals Nhs Trust, Hull, United Kingdom
2Hull York Medical School, Hull, United Kingdom
3Spire Hospital Hull and East Riding, Hull, United Kingdom
Migraines are common in women of reproductive age and its control may deteriorate although 50-80% experience improvement during pregnancy with a significant reduction in frequency and intensity of their attacks. There is limited evidence demonstrating safety and efficacy of the oral agents during pregnancy with only amitriptyline and low dose propranolol deemed suitable for use. Most women and clinicians, therefore choose to discontinue or avoid preventive medication during pregnancy. Onabotulinumtoxin A has been the established treatment for chronic migraine (CM) in the UK where at least 3 preventive agents have failed although its use in pregnancy has not been fully evaluated.
We report pregnancy outcome in 126 patients with CM exposed to onabotulinumtoxinA during pregnancy.
Patients receiving treatment with onabotulinumtoxinA were asked to report if they were pregnant. They were then appraised about the limited data of safety and were offered to stop or continue treatment after signing an informed consent. The toxin were administered as per PREEMPT protocol. Pregnancy outcome data were collected on all patients for the mode of delivery, birth weight, congenital malformation and any other unexpected outcomes.
126 patients reported pregnancy while on treatment with onabotulinumtoxinA (8-16 weeks) of which 80 received treatment in the first trimester and 46 few weeks before conception. 97 patients chose to continue treatment at three monthly interval while 29 stopped further treatment. Those on treatment continued to show a good response and 20/29 patients relapsed and were given greater occipital nerve block. The remaining 9 remained in remission. After pregnancy 17 /20 resumed onabotulinumtoxinA while the remaining three chose oral prophylaxis. 6/9 patients who remained well during pregnancy relapsed 1–3 months following delivery. 3 chose to resume onabotulinumtoxinA, 3 commenced CGRP MAB.
Of the 97 patients that continued treatment there was 2 miscarriages. Remaining 95 were full term deliveries of which there were 10 forceps and 7 caesareans. One patient with miscarriage continued treatment and conceived twice while on treatment with normal full term deliveries. The other patient had a previous history of miscarriage for which no underlying cause was identified. No fetal malformation was reported. While on toxin, one patient had been pregnant thrice and one twice. Their pregnancies were not considered separately. Of the 29 who stopped treatment there was one miscarriage, 4 forceps and four caesareans mode of delivery.
Based on our experience with 126 pregnant patients with CM over the past 12 years, onabotulinumtoxinA is a safe drug and could be considered a good preventive treatment option for CM during pregnancy.
MO.12
Real-world Switching Rates of Atogepant Are Lower Than CGRP Monoclonal Antibodies (mAbs) in Patients With Migraine Using Claims Database
R Lipton1, P Gandhi2, L Wilson3, S Ayton3, K Umashankar2, M Duan2 and J Ailani4
1Albert Einstein College of Medicine, Bronx, USA
2AbbVie, Madison, USA
3Genesis Research LLC, Hoboken, USA
4MedStar Georgetown University Hospital, Washington, DC, USA
Introduction: CGRP mAbs and atogepant, an oral CGRP antagonist, are approved in the US and EU for the preventive treatment of migraine. Switching treatments is an indicator of unmet treatment needs and associated with incremental direct medical costs.
Objective: To understand the real-world treatment switch rates of atogepant versus calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) using claims data from the United States.
Methods: Adult migraine patients newly initiating atogepant or a CGRP mAb between 10/2022 and 6/2023 were identified from the Merative MarketScan database. The earliest treatment claim was the index date. Patients were excluded if they had ≥1 claim for atogepant, rimegepant, BOTOX for migraine, or a CGRP mAb in the 12 months preceding the index date. A switch was defined by the occurrence of ≥1 claim for a different branded preventive treatment (atogepant, CGRP mAb, or BOTOX) during the 12 months following the index date. Multivariable logistic regression models were used to compare odds of switching between atogepant and CGRP mAbs.
Results: Based on a 12-month follow-up, the study included 641 patients who initiated treatment with atogepant and 3,594 with a CGRP mAb (26 eptinezumab, 1,041 erenumab, 917 fremanezumab, and 1,610 galcanezumab). Baseline demographics and clinical characteristics were comparable across treatments; 37% of atogepant and 42% of CGRP mAb users had a chronic migraine diagnosis. At 12 months follow-up, 13.4% of atogepant users and 21.1% of CGRP mAb users (23.1% eptinezumab, 26.5% erenumab, 19.6% fremanezumab, 18.4% galcanezumab) initiated a different branded preventive. Patients taking CGRP mAbs had significantly higher odds of switching to another branded preventive compared to patients taking atogepant (Odds Ratio 1.72, 95% CI: 1.35, 2.21).
Conclusions: Compared with atogepant users, CGRP mAb users were significantly more likely to switch to another branded preventive treatment within 1 year of treatment initiation.
MO.13
COMPARISON OF EFFICACY AND SAFETY OF MONOCLONAL ANTIBODIES TARGETING CGRP FOR MIGRAINE PREVENTION AND AGE-RELATED SUB-GROUPS ANALYSIS: A 12-MONTHS, MULTICENTER, PROSPECTIVE, REAL-LIFE STUDY
I Cetta1, R Messina1, L Zanandrea1, F Genovese1, S Guerrieri2, B Colombo2, M Filippi1 and Study group I
1Neuroimaging Research Unit, Neurology Unit, Vita-Salute San Raffaele University, IRCCS San Raffaele Scientific Institute, Milan, Italy
2Neurology Unit, IRCCS San Raffaele Scientific Institute, Milan, Italy
Introduction: Limited data exists on the efficacy and safety of anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) for migraine prevention across different age groups. Our previous single-center study demonstrated the effectiveness and safety of three and six months of erenumab in patients over and under 65 years, without significant differences.
Objectives: This study aimed to explore the effect of patients’ age on the efficacy and safety of mAbs targeting the CGRP pathway.
Methods: This was a multicenter, prospective, observational study. Enrollment of migraine patients was conducted as part of the I-GRAINE registry, an Italian multicentric project, involving more than 25 Headache Centers. Patients were categorized into age quartiles, resulting in four subgroups. Clinical data were collected at baseline (T0) and at three (M3), six (M6), and 12 (M12) months, including monthly headache (MHD) and migraine (MMD) days, acute treatment usage in terms of days (AMD) and pills (AMP), HIT-6, MIDAS, NRS, ASC-12 scores, and adverse events (AEs) assessment.
Results: A total of 1890 migraine patients participated in the study, predominantly females (80%) with a median age of 49 years (IQR: 18–80), nine hundred twenty-four (49%) treated with erenumab, five hundred seventy-four (30%) with fremanezumab and three hundred ninety-one (21%) with galcanezumab, only one patient received eptinezumab. Migraine characteristics included chronicity (62%), medication-overuse headache (MOH, 58%) and psychiatric comorbidities (32%). All four age groups exhibited significant improvements in clinical variables at M3, M6, and M12 (p < 0.001), except for ASC-12 score in the oldest age group at six and 12 months after treatment. No statistically significant differences in changes of clinical outcomes emerged over time between groups, except for the variation at M12 in patients aged >57 years, who experienced a greater reduction in MHD (p = 0.022), MMD (p = 0.022) and AMP (p = 0.001) compared to the other groups. AEs occurred in 3% of patients during mAb treatment, with constipation (39%), local reactions (33%), and systemic symptoms (28%) being the most common. AEs predominantly occurred in the first trimester (63%), decreasing to 17% at M12. No statistically significant differences were found among age groups regarding the frequency of AEs (p > 0.05).
Conclusions: This multicentric study is the first to investigate real-life efficacy and safety of CGRP-targeting mAbs across different age groups. Ore results confirm the consistent and sustained effectiveness of mAbs across all ages, particularly in elder patients, and suggest their suitability for older patients with potential contraindications to oral preventive drugs. These findings support clinicians in confidently recommending mAb treatment for advanced-age patients and reinforce the favorable safety profile of these therapies.
O.01
The brainstem locus coeruleus and migraine
V Munday1, I Rosenzweig2 and P Holland1
1Headache Group, Wolfson Sensory, Pain and Regeneration Centre, Institute of Psychiatry, Psychology & Neuroscience, King's College London, London, United Kingdom
2Sleep and Brain Plasticity Centre, Department of Neuroimaging, Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom
Introduction: A bidirectional relationship between migraine and sleep is well documented in the literature; however, the underlying pathophysiological mechanisms remain incompletely understood. There is significant convergence of neural networks involved in the regulation of migraine and sleep/arousal, particularly within the brainstem and hypothalamus. Thus, we hypothesise that understanding of this shared circuitry has the potential to provide insight into the complex relationship between migraine and sleep.
Objective: To investigate the role of the noradrenergic locus coeruleus in migraine-related pain processing and sleep.
Methods: The locus coeruleus was selectively targeted through stereotaxic injection of a canine adenovirus (CAV-PRS-hM3D(Gq)-mCherry) which specifically targets noradrenergic neurons via the PRS promoter. Periorbital sensitivity thresholds were assessed using von Frey filaments before and after chemogenetic activation of noradrenergic neurons via intraperitoneal injection of designer ligands. Subsequently, acute intraperitoneal injection of nitroglycerin was used to induce periorbital sensory hypersensitivity, followed by injection of the chemogenetic activator deschloroclozapine 90 mins later. Periorbital sensitivity thresholds were tested 30 minutes after this in order to assess the potential for activation of noradrenergic neurons to reverse nitroglycerin-evoked sensory hypersensitivity.
Results: Chemogenetic activation of noradrenergic neurons resulted in a significant increase in periorbital sensory thresholds compared to baseline. No significant difference in thresholds was observed following a vehicle injection. However, nitroglycerin decreased periorbital sensory thresholds, an effect that was reversed via activation of locus coeruleus noradrenergic neurons.
Conclusions: The locus coeruleus is a heterogeneous structure that demonstrates differential regulation of migraine-related pain processing. Given its role in the regulation of sleep, further detailed exploration is warranted to uncover divergent and shared neural circuits underpinning the relationship between sleep and migraine.
O.02
BoNT/A targets sensitized TRPV1-positive DRG neurons at therapeutic concentrations
P Syed2, R Gormal2, B Sondergaard1, M Nelson1, R Broide1 and F Meunier2,3
1AbbVie, North Chicago, USA
2Clem Jones Centre for Ageing Dementia Research, Queensland Brain Institute, Brisbane, USA
3School of Biomedical Sciences, The University of Queensland, Brisbane, USA
Introduction: Botulinum neurotoxin type A (BoNT/A) is the active ingredient in onabotulinumtoxinA (onabotA; BOTOX®), which is clinically approved to treat a number of aesthetic and therapeutic indications, including chronic migraine. In cholinergic neurons, BoNT/A inhibits neurotransmission by cleaving SNAP-25 in presynaptic nerve terminals thereby blocking neurotransmitter release. Pre-clinical and clinical studies have indicated that BoNT/A may also be effective in various pain disorders via mechanisms that are less understood. We test the hypothesis that the toxin preferentially targets sensitized sensory neurons, a mechanism that could support its clinical use in alleviating pain including migraine.
Objective: This study aims to characterize the molecular mechanism of BoNT/A interaction with sensitized sensory neurons using rat primary dorsal root ganglion (DRG) neuronal cultures.
Methods: Previous BoNT/A imaging studies have mostly relied on relatively high concentrations (nM) of toxin, or fragments thereof to visualize uptake. To characterise the interaction of toxin with sensory neurons, we used single-molecule super-resolution microscopy, capable of tracking picomolar concentrations of BoNT/A in sensory neurons. Primary DRG neurons were incubated with 100 pM of ATTO647N-labelled enzymatically inactive BoNT/A (exBoNT/A) and imaged using the universal point accumulation imaging in nanoscale topography (uPAINT) technique.
Results: We used a lentivirus-based system to specifically label TRPV1-expressing (+) sensory neurons, thus identifying a subpopulation of neurons involved in pain modulation. We found that following 5-30 min exposure, very small amounts of toxin uptake were detected, and only much longer incubation, up to 24 h, resulted in toxin detection in DRG neurons. Since BoNT/A has been reported to alleviate pain in sensitized conditions, we reasoned that neuronal sensitization might increase the toxin’s uptake. We, therefore, sensitized mature DRG neurons for 72 h with 500 nM Prostaglandin E2 (PGE2) and 50 nM Bradykinin (BK) prior to incubation with 100 pM exBoNT/A. Sensitization increased toxin uptake in a TRPV1 + neurons by ∼3-fold across all tested time points. We further labelled sensitized nerve terminals with FM1-43, a probe taken up by recycling synaptic vesicles in an activity-dependent manner, and commonly used to identify actively firing neuronal terminals. Single neurotoxin molecules were detected in FM1-43-labelled nerve terminals, demonstrating toxin access to pre-synapses responsible for transducing nociceptive signals.
Conclusions: BoNT/A preferentially targets sensitized nociceptive neurons that are implicated in transmitting pain signals. This suggests that sensitization promotes a critical change in the molecular landscape of TRPV1 + neurons, which appears to be conducive to the interaction and internalization of the toxin.
O.03
Disrupted activation of pain networks during attack imagery in patients with episodic migraine
A Perdigão1, I Esteves1, A Fouto1, A Ruiz-Tagle1, G Caetano1, R G. Nunes1, R Gil-Gouveia2,3 and P Figueiredo1
1ISR-Lisboa/LARSyS and Department of Bioengineering, Lisbon, Portugal
2Neurology Department Hospital da Luz Lisboa, Lisbon, Portugal
3Center for Interdisciplinary Research in Health, Universidade Católica Portuguesa, Lisbon, Portugal
Migraine patients present hypersensitivity to pain stimulation, usually accompanied by increased brain activation of pain-processing regions compared to healthy controls. However, studying pain perception linked specifically to spontaneous migraine attacks proves challenging due to the unpredictability of their occurrence. As a result, most neuroimaging studies of pain mechanisms in migraine have been conducted during the interictal phase through the application of painful stimuli or recurred to pharmacological triggering. However, these may not entirely capture the intricate pain experienced by migraine patients during an attack.
In this study, we propose a new attack imagery paradigm aimed to elicit brain activation associated with migraine attacks in patients during a pain-free period, in which patients alternate periods of attack with periods of relief. For comparison, healthy controls perform an equivalent pain imagery task, alternating periods of a non-migraine head pain experience with the respective pain relief. If migraine attack imagery proves able to elicit activation of the underlying brain pain networks, it may provide a powerful, non-invasive tool for research of migraine pain episodes that is more specific than painful stimulation and exempt of pharmacologically induced effects.
We studied a group of 14 patients with episodic migraine without aura in the interictal phase (MIG, F, 34.8 ± 8.5 years) and a group of 15 healthy controls (HC, F, 30.9 ± 6.8 years). Patients / controls executed an attack / pain imagery task, alternating 20 s of attack / pain with 20 s of relief. fMRI data were acquired on a 3 T MRI system using a 64-channel receive head RF coil (Siemens). After pre-processing, fMRI data were analysed using a voxel-wise general linear model (GLM) with the task paradigm as regressor of interest and the motion parameters and outliers as confounds. A group-level mixed-effects analysis was then performed to determine the main effects of pain vs. relief as well as patients vs. controls differences for pain vs. relief. A correlation analysis was conducted to assess the relationship between BOLD signal change and clinical parameters.
Both patients and controls activated brain regions associated with pain, including the precentral, postcentral, supramarginal, and inferior frontal gyri, during the pain relative to the relief periods. However, in contrast with controls, who also activated areas of the medial pain system, namely the anterior cingulate cortex (ACC) and the dorsolateral prefrontal cortex (DLPFC), patients significantly deactivated these areas (Figure 1). Moreover, the level of ACC deactivation increased with attack frequency, although this effect did not survive correction for multiple comparisons. No effects were found for the other clinical parameters.
Overall, our findings provide evidence of aberrant functioning of pain networks in the migraine brain, including the medial pain system, which seem to be correlated with attack frequency. The attack imagery paradigm may represent a promising alternative to studies of pain mechanisms in migraine involving painful stimulation or pharmacological triggering, which is potentially closer to the experience felt during the attack while overcoming some of the limitations associated with studying the attack itself.
Figure 1
Table 1
O.04
Glucagon-like peptide-1 receptor agonists for the treatment of migraine: a pilot prospective observational study in a cohort of obese patients
S Braca1, C Russo1, A Stornaiuolo1, G Cretella1, C Giannini1 and R De Simone1
1University Of Naples “Federico II”, Naples, Italy
Introduction: Migraine, affecting 14.7% of the global population, often lacks effective treatment. Glucagon-like peptide-1 receptor (GLP-1R) agonists, used for diabetes and obesity, control fluid secretion, influencing cerebrospinal fluid (CSF) production in the brain's choroid plexus. Studies show GLP-1R agonists reduce intracranial pressure (ICP) in rodents, surpassing common idiopathic intracranial hypertension (IIH) drugs in effectiveness. Clinical trials have confirmed their ability to lower ICP and improve headache frequency in IIH patients. There is converging evidence that reducing ICP benefits not only IIH patients but may also be beneficial to those with borderline normal CSF pressure, indicating that even isolated intracranial compliance reduction might be crucial in migraine development. Indeed, GLP-1R agonists have also been found to suppress pain pathway sensitization in trigeminal nucleus caudalis.
Objective: This study explores GLP-1R agonists as a novel migraine treatment, focusing on their efficacy in reducing migraine frequency.
Methods: This is a pilot prospective observational cohort study, aiming at evaluating the effectiveness of subcutaneous Liraglutide, 1,2 mg daily, for the treatment of comorbid migraine in obese patients. We enrolled 26 patients with migraine and a concomitant BMI equal or greater than 30 at our tertiary Headache Centre. Exclusion criteria included the presence of papilledema to rule out idiopathic intracranial hypertension. Duration of follow-up was 12 weeks. We assessed mean monthly days with headache by reviewing standardized paper patient headache diaries. The primary outcome of this study was the reduction of mean monthly days with headache after 12 weeks of continuous treatment with Liraglutide. The secondary outcomes were the reduction of BMI, MIDAS score, and the rate of adverse events.
Results: Mean monthly days with headache decreased from a baseline mean of 20.04 ± 6.38 days to 8.81 ± 6.01 days post-treatment. This change was statistically significant with a mean difference of 11.23 days (95% CI: 7.96 to 14.50, p < 0.001). MIDAS score decrased from a baseline mean of 62.58 to 27.23 post-treatment. This reduction was also significant with a mean difference of 35.35 (95% CI: 27.32 to 43.38, p < 0.001). Conversely, BMI decreased slightly from 34.01 to 33.65, and this change was not statistically significant (mean difference = 0.36, 95% CI: -0.02 to 0.74, p = 0.060). The analysis of covariance (ANCOVA) was used to assess whether the change in headache days was influenced by BMI change while controlling for other variables, and the coefficient for changes in BMI was not significant (B = 0.190, p = 0.949), indicating no significant effect of BMI reduction on headache frequency. We recorded mild adverse events in 10 (38%) of patients, all of which of gastro-intestinal nature, mainly regarding nausea and constipation; none of these events determined discontinuation of treatment.
Conclusion: this pilot study suggests that GLP-1 agonists may be a suitable and effective treatment for migraine and that their efficacy is unrelated from weight loss. This may shed new light on migraine physiopathology and its relation with CSF volume and pressure homeostasis.

O.05
Machine learning versus polygenic risk scoring as migraine predictors based on genome-wide genotype data
A Danelakis1,2, B Winsvold2,3, M Bjørk2,4,5, D Giles6, P Nachev6, T Kumelj1,2,7, K Hagen1,2,7, M Matharu6, E Tronvik1,2,7, H Langseth1, A Stubberud1,2,7 and D Nyholt8,9
1Norwegian University of Science and Technology - NTNU, Trondheim, Norway
2Norwegian Centre for Headache Research - NorHead, Trondheim, Norway
3Oslo University Hospital, Oslo, Norway
4University of Bergen, Bergen, Norway
5Haukeland University Hospital, Bergen, Norway
6University College London - UCL, London, England
7Saint Olavs University Hospital, Trondheim, Norway
8International Headache Genetic Consortium - IHGC, Brisbane, Australia
9Queensland University of Technology - QUT, Brisbane, Australia
Introduction: Despite strong patterns of inheritance, the largest Genome-Wide Association Study (GWAS) meta-analysis explains only 11.2% of the migraine heritability. This missing heritability can be partially explained by epistatic interactions where certain variants with low or marginal effects may have larger effects in combination with other variants. Polygenic Risk Scoring (PRS), assuming an additive genetic architecture, can estimate the risk of a disease based on the sum of all risk alleles carried by an individual, but does not model any gene-gene/environment interactions. Therefore, implementing high-dimensional machine learning (ML) models that account for interactive effects could with better precision identify individuals with migraine using genotype data, and help solve the missing heritability issue.
Objectives: (1) Estimate the predictive accuracy of ML in diagnosing migraine versus headache-free controls from genome-wide genotype data; (2) Compare accuracy of both simple and complex ML models with PRS across increasing dimensionalities of genetic input data.
Methods: The study population was participants in the second and third Nord-Trøndelag Health Study, genotyped with three different versions of the Illumina HumanCoreExome microarray. Phenotype was based on validated IHS criteria in questionnaires.
To identify the most relevant variants for the ML models we acquired summary statistics for migraine risk loci and risk variants from the largest available GWAS meta-analysis. The test set was kept unseen during model training. A series of standard ML classification architectures and deep learning models were evaluated and optimized. All models were trained on a training set and performance was continuously evaluated with 10-fold cross validation. The area under the receiver operating characteristics curve (AUC) was used as the main scoring metric for training and optimizing the models. The top performing model for each dataset was finally applied on the held-out test set to quantify out-of-sample performance. To compare the diagnostic accuracy of ML versus PRS and evaluate the effect of the dimensionality of the genotype input data, four different datasets with increasing number of genetic variants were created (108, 7771, 7840, and 140467 variants) PLINK and LDpred2 were used for calculating and evaluating polygenic risk scores. All PRS scores were normalized and 0.5 was used as a decision threshold. PRS was calculated on the same test set as the ML models.
Results: A total of 43197 individuals were included in the modelling. The top performing model for the three datasets with the lowest number of variants was the Light Gradient Boosting Machine classifier with test-set AUCs ranging from 0.630 to 0.637. In the largest dataset, the Multinomial Naive Bayes classifier achieved a cross-validated and out-of-sample test set AUC of 0.85 and 0.88 respectively. PRS scores were statistically significantly inferior to ML for all datasets, achieving an AUC of 0.53 and 0.59 for PLINK and LDPred2, respectively, in the largest dataset.
Conclusions: ML outperform PRS in predicting migraine from genotype. This indicates that interactive effects among variants improve simple additive prediction. With increasing number of variants, simpler ML models perform better since they tackle the “high predictors low samples” problem (“p>>s”) better and avoid overfitting.
O.08
Predictors of migraine-related vertigo in adults and children
N Karsan1, N Vandenbussche2, R-J Wilcha1, P Amarasena1, P Soontrapa3, K Nagaraj4, C Lastarria Perez5, S Ololade1, P Prabhakar6 and P Goadsby1
1King's College London, London, United Kingdom
2Department of Neurology, Ghent University Hospital, Ghent, Belgium
3Mahidol University, Salaya, Thailand
4Department of Neurology, Swansea University Board, Swansea, Wales, UK
5Vallesur - Auna Clinic, Arequipa, Peru
6Department of Neurology, Great Ormond Street Hospital for Children, London, UK
Introduction: Vertigo is a non-canonical, common symptom of migraine. We set out to examine detailed phenotypic data from our adult and paediatric clinical cohorts for predictors of vertigo in chronic migraine (CM).
Methods: Databases of CM extended phenotypes within the adult Headache service at King’s College Hospital between 2015 and 2020 (n = 622), and within the Children’s Headache Clinic at Great Ormond Street Hospital for Children between 2021 and 2022 (n = 76), were merged for a service evaluation. Patients without information on vertigo were excluded. All migraine-associated symptoms were coded as dichotomous variables. Predictors of interest for the presence of vertigo: gender, allodynia, aura, photophobia, phonophobia and osmophobia, baseline headache frequency, number of premonitory symptoms, presence of cranial autonomic symptoms (CAS) and age categories, were analysed using a binary logistic regression model (IBM SPSS v 29). P < 0.05 was considered significant. Outliers were defined as those with standardised residuals outside two standard deviations of the mean.
Results: The total sample size for analysis was n = 457, after excluding missing data and outliers. Patients were aged 5-92 years (median 45, IQR 31-56), and the majority (83%) were female. Vertigo associated with migraine was present in 50%. Within the regression model, the presence of aura and allodynia positively predicted vertigo, and advancing age negatively predicted vertigo (Table).
Conclusions: Vertigo in chronic migraine is common, is present in young children and adults, and may be associated with a more enriched phenotype independent of baseline headache frequency. Future treatment strategies should evaluate the effect on this often under-recognised yet disabling symptom.
Table
O.09
Evaluating a New Migraine Scoring System Against Established Metrics
P Pozo-Rosich1, E Caronna1, E Ruiz De La Torre2, P Goadsby3, M Ashina4, P Irimia5, A Maassen van den Brink6, D Mitsikostas7 and G Terwindt8
1Headache Unit, Neurology Department, Vall d'Hebron University Hospital, Spain
2EMHA, Europe
3NIHR-King’s Clinical Research Facility, King’s College London, UK
4Danish Headache Center, Department of Neurology, Rigshospitalet Glostrup, University of Copenhagen, Denmark
5Department of Neurology, Headache Unit, University Clinic of Navarra, Spain
6Department of Internal Medicine, Erasmus MC Medical Center, Rotterdam, The Netherlands
71st Department of Neurology, Aeginition Hospital, National and Kapodistrian University of Athens, Greece
8Department of Neurology, Leiden University Medical Center, The Netherlands
Introduction: Migraine is a complex neurological disorder characterised by episodic attacks that significantly affect quality of life. Traditional scoring systems such as MIDAS (Migraine Disability Assessment) and HIT-6 (Headache Impact Test) quantify migraine impact but may not sufficiently address all dimensions, such as treatment response, patient understanding, stigma and ease of use for physicians, highlighting the necessity for a new system.
Objectives: To validate a new migraine scoring system that integrates frequency, acute treatment reliability, and pain intensity and benchmark it against MIDAS and HIT-6.
Methods: The European Migraine & Headache Alliance, a patient association umbrella alliance, collaborated with migraine experts to develop a system that differentiates migraine severity, reduces stigma, and simplifies use for general practitioners and patients. The development involved a comprehensive analysis of patient data, focusing on three key indicators: frequency of headache days, reliability of acute treatment, and pain intensity. Variables included monthly headache days, days with mild/moderate/severe intensity, days of acute medication intake (MAMD), and MAMD with good response, alongside scores for MIDAS, HIT-6, and Migraine-Specific Quality-of-Life Questionnaire (MSQ). The process began with the assignment of threshold scores for each indicator based on their severity which were integrated to compute a total score and grouped into four severity levels: Level 1 (scores 1-4), Level 2 (scores 5-6), Level 3 (scores 7-9), and Level 4 (scores 10-15). Comparative analyses were conducted to examine group shifts, observing if and why patients previously categorised under MIDAS or HIT-6 classifications experienced changes in their grouping when using the new scoring system, i.e., does their classification or severity differ and what drives this.
Results: Data from 319 patients, predominantly women (84%), with a median age of fifty, collected in a specialised migraine unit, were analysed. The majority (60%) of patients scored 9 or higher on a 1-15 scale, indicating more severe symptoms with the following distribution across levels: Level 1 (14.1%), Level 2 (12.2%), Level 3 (25.4%), and Level 4 (48.3%). Comparisons with HIT-6 and MIDAS revealed that almost half of the patients remained in consistent groups when transitioning from HIT-6 (48.2%) and MIDAS (46.4%), however, notable changes in categorisation were noted in Levels 2 and 3, i.e., the majority of patients were found to have a different severity in the new system compared to HIT-6 and MIDAS. Furthermore, a significant movement was observed as 8.2% of the patients made a substantial shift, moving from Group 1 in HIT-6 to Level 4 in the new system or vice versa. Following correlation and regression analyses, acute treatment reliability was identified as the primary driver for these changes with pain intensity identified as an additional driver, to a lesser extent.
Conclusion: The new scoring system partially aligns with established metrics while introducing a new way of evaluating migraine severity, highlighting the importance of variables such as treatment reliability and pain intensity as well as frequency. This new scoring system can facilitate tailored management and monitoring of migraine over time, potentially improving alignment with sufferers’ perceptions and enhancing understanding between physicians and patients.
P.01
Burnout and Resilience: A Clinic Based Migraine Study
M Capote1, K Garces1, M Gupta1, E Veledar1 and T Monteith1
1Department of Neurology-Headache Division, University of Miami, Miller School of Medicine, Miami, United Kingdom
Objectives: Migraine is a highly prevalent, chronic neurological disorder, associated with a major psychosocial and economic impact. The migraine brain may be vulnerable to high stress loads and the transformation from episodic to chronic migraine is associated with stressful life events. Prolonged or repeated stress may result in burnout, although the impact in people with migraine is not well understood. The aim of the study is to determine the relationship between burnout, resilience, and features of migraine.
Methods: This is a cross-sectional survey study of participants in the headache clinic with a history of migraine, limited to aged 18-65 years. Participants were recruited via electronic portal messages or in clinic. Participants were consented, and completed a survey via Redcap that contained questions about migraine symptoms, and other medical history, sociodemographic, and validated instruments such as the Oldenburg Burnout Inventory (OBI), the Connor-Davidson Resilience Scale, the Pain Categorizing Scale (PCS), the Headache Impact Test (HIT-6), Migraine-Specific Quality-of-Life Questionnaire (MSQ), the General Anxiety Disorder Assessment (GAD-7), and the Patient Health Questionnaire (PHQ-9).
Results: Of 180 people, 164 were female. Mean age was 45.1(SD ±12.2) years. Migraine occurred less than 15 days (N = 124) and greater than 15 days per month (N = 39, with no gender and age difference between frequency migraine groups. There were significant differences in burnout exhaustion subscales in those with high frequency migraine vs low frequency migraine16.22 vs 18.35, p < 0.04, confirmed with significant differences in PCS and HIT-6 scores for the 2 groups. Indicators of pain catastrophizing, headache impact, and depression were all greater for individuals with chronic than episodic migraine. Low resilience measures were seen across all migraine frequencies, with a trend toward lower resilience with higher frequencies. There was highly significant negative correlation between burnout and resilience, (Spearman r = -0.24193, p = 0.0148).
Conclusion: Migraine is associated with indicators of burnout and low resilience overall. Larger studies are needed to confirm findings, and to determine if this is a trait associated with migraine or a disease characteristic, in which targeting burnout and resilience may have therapeutic benefits.
P.02
Real-world Effectiveness of Anti-CGRP Monoclonal Antibody in Chronic Migraine in Thailand: A Retrospective Study in a Middle-Income Country
P Anukoolwittaya1,2,7,8, A Hiransuthikul1,3, T Pongpitakmetha1,4,7,8, W Rattanawong1,5,8
and S Thanprasertsuk1,6,7,8
1Chulalongkorn Headache and Orofacial Pain (CHOP) Service and Research Group, Division of Neurology, Department of Medicine, King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, Bangkok, Thailand
2Division of Neurology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
3Department of Preventive Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
4Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
5Department of Medicine, Faculty of Medicine, King Mongkut's Institute of Technology Ladkrabang, Bangkok, Thailand
6Department of Physiology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
7Chula Neuroscience Center, King Chulalongkorn Memorial Hospital, Bangkok, Thailand
8Thai Headache Society, The Neurological Society of Thailand, Bangkok, Thailand
Introduction: Monoclonal antibodies targeting the calcitonin gene-related peptide (CGRP mAbs) have demonstrated efficacy and safety in the prophylactic management of chronic migraine (CM), as evidenced by multiple phase 3 clinical trials Since 2019, the European Headache Federation has endorsed CGRP mAbs as first-line therapy, followed by the American Headache Society in 2024. Despite their proven benefits, real-world data on CGRP mAbs in middle-income countries are limited, particularly due to high costs and limited availability of the drug.
Objective: To determine the real-world efficacy of CGRP mAbs in converting CM to EM, as well as their impact on headache frequency and disability scores, among patients with CM, with and without mediation overuse headache (MOH).
Methods: A retrospective study was conducted by systematically reviewing the electronic medical records of patients who attended the headache clinic at King Chulalongkorn Memorial Hospital from January 2019 to September 2023. The study included patients aged 18 years and older, diagnosed with CM according to the International Classification of Headache Disorders, version 3 (ICHD-3), who had used CGRP mAbs for at least 6 months. Kaplan-Meier plots were used to assess the conversion rate to EM and the proportion of those achieving a ≥ 30% reduction in monthly headache days (MHD) compared to baseline. Furthermore, changes in average MHD and the Migraine Disability Assessment (MIDAS) score were examined.
Results: Among the 26 patients diagnosed with CM included in the analysis (median age [IQR] of 35.1 [23.7–50.4] years, with 20 [76.9%] being women), 14 (53.9%) had MOH. The CGRP mAbs used were as follows: 18 (69.2%) received galcanezumab, 7 (26.9%) received erenumab, and 1 (3.9%) received fremanezumab. The conversion rate to EM was 73.6% after 3 months and remained consistent until the last observation at month 6 (Figure). The percentage of patients achieving a ≥ 30% reduction in MHD improved from 73.6% at 3 months to 100% at 6 months post-treatment. Median MHD decreased progressively from baseline (20 [14–28]) to 3 months (15 [7–19]) and 6 months (12.6 [10–14]) after initiating CGRP mAbs. These reductions coincided with decreases in median MIDAS score over time: 30 (5–90) at baseline, 3 (0–24) at month 3, and 0 (0–13) at month 6 post-CGRP mAbs.
Conclusion: CGRP mAbs demonstrated high efficacy in converting CM to EM and achieving a ≥ 30% reduction in MHD among patients. Unfortunately, CGRP mAbs are not covered by universal healthcare coverage or insurance in Thailand, highlighting the need for further investigation into the cost-utility analysis of CGRP mAbs.
Image 1

P.03
Insights from a mixed-methods feasibility RCT assessing digital Cognitive Behavioural Therapy for insomnia in individuals with chronic migraine
X Chan1, B Martin1, A Greenwood1, L Fleming1, J Laverick2, S Whoriskey2, M Ghadiri-Sani3, G Gorrie4, I Morrison5, A Henry6, C Espie7, K Elhadd3 and M Crawford1
1University of Strathclyde, Centre for Sleep Health, Psychological Sciences and Health, Glasgow, United Kingdom
2University of Strathclyde, Mathmatics and Statistics, Glasgow, United Kingdom
3The Walton Centre, Liverpool, United Kingdom
4Queen Elizabeth University Hospital, NHS Greater Glasgow and Clyde, Glasgow, United Kingdom
5Ninewells Hospital, Dundee, United Kingdom
6Big Health, San Francisco, United States
7University of Oxford, Oxford, United Kingdom
Introduction: Difficulties sleeping is a frequent complain in individuals with chronic migraine, and these are hypothesised to be interrelated in a biobehavioural vicious cycle. Given it’s flexibility, it is suggested that digital forms of CBTi (dCBTi) will be more appealing to individuals with chronic migraine, though it remains to be seen whether dCBTi is able to show benefit to insomnia and migraine symptoms. Using a mixed-methods feasibility randomised controlled design, this study will explore the use of dCBTi, and the barriers in the way of conducting a full-scale RCT in a chronic migraine population.
Objectives: Assess 1) treatment effects 2) barriers to conducting a full-scale RCT, and 3) mechanisms underpinning the relationship between insomnia and chronic migraine.
Methods: A 2-arm randomised controlled design was employed to compare a dCBTi treatment and a Sleep Hygiene Education (SHE) control. The interventions each involved 6 weekly, fully-automated online sessions, which participants were provided access to following a 30-day baseline assessment. Symptoms of insomnia and migraine were assessed using the Insomnia Severity Index (ISI) and the Migraine Disability Assessment (MIDAS), respectively, and was assessed at baseline, post-treatment (3 months) and follow-up (6 months after starting treatment). Treatment effects were assessed using paired-t-tests comparing baseline to post-treatment, while regression analyses were used to explore whether decreases in napping behaviour were related to improvements in migraine symptoms, mediated by improvements in insomnia (proposed mechanism). Preliminary blinded analyses are reported at group level but will be available at the time of presentation. Blinded and unblinded semi-structured interviews were conducted after the 3-month assessment or once having finished participation in the study.
Results: Three-hundred and fifty-seven individuals were assessed for eligibility and of those, 90 were randomised. At present 49 participants have completed the study, 33 have dropped out, 2 were ineligible after baseline, and 6 remain active. Preliminary analyses at the overall group level showed a significant decrease in insomnia severity on the ISI (mean difference of 5.6 (t = 6.98, df = 46, p = <0.001)). Although headache frequency did not change (mean difference = 6.1(t = 1.52, df = 39, p = 0.136)), headache severity showed significant improvement (mean difference = 0.93 (t = 3.44, df = 45, p = 0.001)). Qualitative insights from 20 participants across 16 interviews/focus groups indicate that the flexibility afforded by digital interventions was positive. While some found the sleep restriction component of the CBTi challenging given an increased propensity for a migraine attack, others found the treatment effective and relaxing. Regarding SHE, most found the treatment acceptable and accessible, with variation in the level of information previously known/practiced. Overall, most found the daily burden acceptable, but noted that the length of the study was a commitment.
Conclusion: Moderate changes in insomnia symptoms and small changes to migraine severity were found at a group level and preliminary qualitative findings indicate some benefits arising from the use of dCBTi. Full analyses will uncover differences between arms and give insight into challenges in the way of conducting a full-scale RCT.
P.04
MultiHead – work-focused multidisciplinary headache treatment
O Lunder1,2, T Wisløff3,4, K Aaseth1,2, E Kristoffersen1,2,5 and K Vetvik1,2
1Department of Neurology, Akershus University Hospital, Lørenskog, Norway
2NorHead, the Norwegian Headache Research Center, Trondheim, Norway
3Health Services Research Unit, Akershus University Hospital, Lørenskog, Norway
4Intitute of Clinical Medicine, University of Oslo, Oslo, Norway
5Department of General Practice, University of Oslo, Oslo, Norway
MultiHead – work-focused multidisciplinary headache treatment
Introduction: The costs related to lost work days and reduced productivity are high among people with headache. Despite new pharmacological treatments, many patients experience insufficient treatment response. Although available for other chronic pain conditions, multidisciplinary teams are not accessible for headache patients within the public health care system in Norway.
In cooperation with The Norwegian Labor and Welfare Administration we established a multidisciplinary headache clinic for patients who struggle with work absence due to headaches.
Objectives: The objectives of this project are to evaluate the effects of combined pharmacological and non-pharmacological treatment in a multidisciplinary team on headache frequency, health-related quality of life and work participation.
Methods: Patients aged 18-67 years referred to Department of Neurology, Akershus University Hospital, due to headaches, and currently on sick leave or had a history of recurrent sick leave periods were included.
All patients were treated by a team of headache specialists, headache nurses, psychologists, physiotherapists, and senior advisors from the Norwegian Labor and Welfare Administration. The patients were followed-up with structured clinical follow-up and self-administered questionnaires at baseline, and after 3, 6 and 12 months. Between these visits, all patients were offered follow-up based individual needs.
We used Wilcoxon test to compare continuous data and Chi square test for categorical variables from baseline to 12-month follow-up.
Results: 101 patients (87 females) completed the 12 months follow-up. Migraine was the most common diagnosis (n = 84), followed by tension-type headache (n = 14). The majority (n = 84) suffered from chronic headache at baseline, 46 used preventive drugs and 68 had already tried several different non-pharmacological treatments. Half of the patients (n = 52) were currently on sick leave due to headache at baseline.
A significant reduction of headache days from 22.1 (SD 8.1) to 12.4 (19.4) (p < 0.01) per month, days with use of acute medication from 7.7 (SD 7.1) to 4.7 (SD 5.1) (p < 0.01) and Headache Impact Test 6 (HIT-6) scores from 64.8 (SD 4.4) to 59.2 (SD 8.2) (p < 0.01) was observed after 12 months. A ≥ 75% and ≥50% reduction in headache frequency per month was observed in 37% (n = 37) and 52% (n = 52) of the patients.
After 12 months, 50% of those who were on sick leave at baseline returned to work (p < 0.01).
Conclusions: Treatment in a multidisciplinary team had significant effects on headache burden and work participation after one year.
Image 1

P.05
Contemporary Prospective Understanding of Migraine Real-World Evidence (CAPTURE): Baseline Patient-Reported Outcomes
E Leroux1, P Goadsby2, Z Katsarava3, M Lanteri-Minet4, E Tucker5, Y Liu6, J Lam5, H Ha5, L Delahaye7 and P Pozo-Rosich8
1Montreal Neurological Clinic, Montreal, Canada
2NIHR-King’s Clinical Research Facility, King’s College London, UK; University of California, Los Angeles, Los Angeles, USA
3Evangelical Hospital Unna, Unna, Germany
4Pain Department and FHU InovPain, CHU Nice and Côte Azur University, Nice, France; INSERM U1107 Migraine and Trigeminal Pain, Auvergne University, Clermont-Ferrand, France
5AbbVie, Toronto, Canada
6AbbVie, North Chicago, USA
7AbbVie, Rungis, France
8Headache Unit, Neurology Department, Vall d’Hebron University Hospital, Headache and Neurological Pain Research Group, Vall d’Hebron Institute of Research, Universitat Autònoma de Barcelona, Spain
Introduction: CAPTURE is a 2-year, international, prospective, longitudinal study aiming to elevate the understanding of disease burden and treatment patterns among people living with migraine, stratified by headache frequency.
Objective: To describe results of an interim analysis of baseline patient-reported outcome (PRO) data for CAPTURE participants enrolled as of December 2023.
Methods: Adults with migraine diagnosed for >=1 year, aged <50 years at onset, and taking >=1 medication indicated for migraine with >=4 monthly headache days (MHDs) in the prior 3 months were assigned to cohorts based on headache frequency (cohort 1: 4-<8 MHDs; cohort 2: 8-<15 MHDs; cohort 3: >=15 MHDs. Descriptive data for baseline characteristics and patient-reported outcomes (PROs) (Migraine Disability Assessment [MIDAS], Migraine-Specific Quality of Life questionnaire v2.1 [MSQv2.1], Work Productivity and Activity Impairment Questionnaire [WPAI], Headache Impact Test-6, Patient Global Impression–Severity, Hospital Anxiety and Depression Scale, Migraine Interictal Burden Scale) are presented. Endpoints include durations of current/subsequent migraine treatment use and change from baseline of clinical outcomes (eg, MHDs, medication use, PROs).
Results: Among 239 participants (as of December 2023; cohort 1: n = 68; cohort 2: n = 104; cohort 3: n = 67), baseline PROs indicated greater impairment and poorer quality of life with higher MHDs (Table). For cohorts 1, 2, and 3, respectively, baseline mean (SD) MIDAS total scores were 29 (40), 33 (30), and 61 (52); MSQv2.1 Role Function–Restrictive scores were 58.9 (17.5), 53.4 (20.8), and 44.8 (22.0); and WPAI migraine-related impairment was 39.4 (27.2), 40.6 (24.8), and 52.0 (22.8).
Conclusion: Baseline PROs suggest greater disease burden among participants with higher MHD frequency. CAPTURE will provide critical data on migraine disease patterns and the associated burden over time.


P.06
Rimegepant effectiveness and tolerability as an acute migraine treatment (GAINER): a real-world multicentric study
M Corrado1, R De Icco1, L Iannone2, A Burgalassi2, G Vaghi1, E De Matteis3, F De Santis3, C Fasano2, E Piella4, M Romozzi5, G Sebastianelli6, G Avino7, S Cevoli8, G Coppola6, G Dalla Volta9, A Granato10, E Mampreso11, R Ornello3, F Pistoia3, S Sacco3, I Rainero12, M Trimboli13, A Russo14, M Valente15, C Vollono16 and C Tassorelli1
1Department of Brain and Behavioral Sciences, University of Pavia. Headache Science & Neurorehabilitation Center, IRCCS Mondino Foundation, Pavia, Italy
2Headache Centre and Clinical Pharmacology Unit, Careggi University Hospital, Florence, Italy
3Department of Biotechnological and Applied Clinical Sciences, University of L'Aquila, L'Aquila, Italy
4Department of Neurosciences “Rita Levi Montalcini”, University of Torino, Torino, Italy
5UOC Neurologia, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
6Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome Polo Pontino ICOT, Latina, Italy
7Ospedale di Prato Santo Stefano, Prato, Italy
8IRCCS Istituto delle Scienze Neurologiche, Bologna, Italy
9Headache Centre of Istituto clinico città di Brescia (gruppo San Donato), Brescia, Italy
10Azienda Ospedaliero-Universitaria di Trieste, Trieste, Italy
11Headache Centre, Neurology - Euganea Health Unit, Padua, Italy
12Headache Center, Department of Neuroscience, University of Torino, Torino, Italy
13Centro Interaziendale Cefalee, Azienda Ospedaliero-Universitaria Renato Dulbecco, Catanzaro, Italy
14Department of Advanced Medical and Surgical Sciences, University of Campania “Luigi Vanvitelli”, Naples, Italy
15Azienda Sanitaria Universitaria Friuli Centrale, Presidio Ospedaliero Santa Maria della Misericordia, Udine, Italy
16Department of Neurosciences, Università Cattolica del Sacro Cuore, Rome, Italy
Introduction: Rimegepant, a novel oral calcitonin gene-related peptide receptor antagonist, has been recently approved for the acute migraine treatment. While its efficacy has been proven in clinical trials, there are no current data regarding its real-world tolerability and effectiveness.
Objectives: We designed a prospective multicentric study to evaluate rimegepant effectiveness and tolerability in the real-world setting (NCT05903027).
Methods: We enrolled 87 patients (76% females, 44.3 + 11.7 years, 28% with chronic migraine, baseline monthly migraine days 9.4 + 7.8) from 13 Italian headache centers. Patients were instructed to treat up to four migraine attacks with rimegepant 75 mg. Using an ad hoc diary, we prospectively collected migraine-attack features every 30 minutes after rimegepant administration, up to 2 hours (2 h).
Results: Preliminary analyses were conducted on 43 reported first-treated attacks (8/43 in CM patients), and on 91 total attacks. At rimegepant intake, 38.5% of patients rated migraine intensity as severe (3 on a 0–3 rating scale). Pain freedom 2 h post-dose was reported in 58.1% (25/43) of first-treated attacks, and in 53.8% (49/91) of total attacks. The 2 h pain freedom response was not influenced by timing of rimegepant intake (p = 0.204), baseline pain severity (p = 0.171) and the diagnosis of chronic/episodic migraine (p = 0.626). Freedom from the most bothersome symptom 2 h post-dose was reported in 60.4% of attacks. Mild adverse events were reported in 18% total attacks (8/91), namely gastrointestinal discomforts (n = 4), fatigue (n = 2), dizziness (n = 1) and somnolence (n = 2). Tolerability was rated as good-to-excellent in 92.3% cases (84/91).
Conclusion: Our real-world data support rimegepant effectiveness, safety, and tolerability as an acute migraine treatment. In this preliminary analysis, rimegepant effectiveness was not influenced by pain severity and timing of drug intake.
P.07
Two-year outcome of Galcanezumab in refractory chronic migraine patients: Real-world data from the Hull Migraine Clinic, UK
F Ahmed1,2,3, R Khan1, S Dorsey1,3 and H Delrosario1
1Hull University Teaching Hospitals Nhs Trust, Hull, United Kingdom
2Hull York Medical School, Hull, United Kingdom
3Spire Hospital Hull and East Riding, Hull, United Kingdom
Objective: Galcanezumab is licensed as preventive treatment in those with > 4 days of headaches per month. In the UK, NICE has approved its use in episodic and chronic migraine patients who have failed at least three prior treatments. We evaluated two year outcome on patients prescribed Galcanezumab for CM.
Methods: Adult CM patients attending the Hull Migraine clinic were prescribed Galcanezumab and followed up prospectively. Patients maintained a headache diary for at least 1 month prior to and continuously after commencing Galcanezumab. All patients tried and failed at least 6 treatments with 93% failing OnabotulinumtoxinA. We measured monthly headache days (MHD), migraine days (MMD), headache-free days (HFD), analgesia medication (AMD) and triptan days (TD) and Headache Impact Test-6 (HIT6) scores at baseline and monthly during the first three months and subsequently at the 12th and 24th month of treatment. The treatment was discontinued if they had < 30% reduction in either MHD, MMD at the end of first three months. At one year, those that continued were asked to stop treatment for three months if they had < 4 headache days per month for the previous three months and treatment recommenced if any time in the subsequent three months, the headache days went above 4 per month.
Results: 125 patients (98 F, 27 M), mean age 42.5 years (range 21–75), commenced Galcanezumab between January 2022– May 2022. 92 patients (76 F, 16 M) at 3-month follow-up had baseline MHD, MMD and HFD of 27, 17 and 3 days, improving to 15, 6 and 15 days respectively were classed as responders and continued treatment for one year. The remaining 33 patients (22 F, 11 M) stopped treatment due to lack of response. At one year 87 (94.5%) patients (73 F and 14 M) were still getting > 5 days of headaches per month and continued treatment and only 5 (5.5%) patients (3 F, 2 M) were able to stop treatment. All but 1 had to restart therapy as the headache days exceeded > 5 or more in the month following stoppage. 91 patients who continued for two years only 8 were able to stop the treatment. The remaining 83 (90%) have been given treatment for the third year running.
Side effects were observed in 15 (12F 3 M) that included constipation, weight gain and a transient rash at the site of injection.
Conclusion: Even though many patients with CM are reverted to episodic migraine following Galcanezumab therapy, almost all (90%) patients are required to continue treatment for the third year.
P.08
The safety and efficacy of erenumab in migraine patients with cardiovascular risk factors
S Kandapara2, S Broadhurst1 and M Ghadiri-sani1
1The Walton Centre Nhs Trust, Liverpool, UK
2The University of Liverpool, Liverpool, UK
Introduction: Migraine is a common and often debilitating neurological condition impacting 12% of people worldwide, particularly those aged 25-55. The conventional migraine preventatives have been poorly tolerated and often relatively ineffective. Calcitonin Gene Related Peptide (CGRP), has been shown to play a crucial role in the pathophysiology of migraines, leading to the development of CGRP receptor antagonists such as erenumab, as breakthrough treatments.
Although several studies have shown erenumab to be effective, there remains concerns about its safety in patients with cardiovascular risk factors and previous vascular events, limiting its use in these patient groups.
Objective: A retrospective review to assess the safety of erenumab in migraine patients who have comorbid cardiovascular and cerebrovascular disease and risk factors.
Methods: We conducted a retrospective review of our database and patient notes for 480 migraine patients who were prescribed erenumab from June 2021 to January 2024. 69 patients were excluded due to lack of notes and remaining had only started treatment within the preceding 3 months, therefore, no data was yet available.
Therefore, 411 patients were analysed for demographics, cardiovascular risk factors, and treatment outcomes. The primary outcome was the continuation of erenumab therapy, indicating reduction of headache severity and frequency by at least 30% in chronic migraine and 50% improvement in episodic migraine patients.
Results: In total, 250 out of 411 (61%) patients discontinued erenumab, while 39% continued therapy for at least a year.
49 patients out of 411 (12%) had pre-existing cardiovascular risk factors. These included history of cerebral bleeds (13%) and strokes (4%), hypertension (46%), diabetes (28%) and hypercholesterolemia 9%. Among these patients (n = 49), 55% discontinued therapy.
Overall, reasons for discontinuation included lack of efficacy (n = 232), worsening headaches (n = 6), constipation (n = 5), and mood changes (n = 2).
Only one patient discontinued due to exacerbation of hypertension, with no significant adverse cardiovascular outcomes reported.
Conclusion: Our data suggests erenumab is generally well-tolerated and effective in prevention of migraine in patients with cardiovascular risk factors. The isolated hypertension case highlights the need for regular monitoring, but overall safety remains favourable.
At our centre, erenumab is used in highly refractory patients, who have failed at least 3 oral preventatives and in most cases, another anti-CGRP MAB drug, which could explain why only 40% of patients responded to erenumab.
Further studies with larger cohorts and more robust data is needed to explore the safety of anti-CGRP MABs in management of migraine patients with vascular risk factors.

P.09
Three year outcome of Fremanezumab in refractory chronic migraine patients: Real-world data from the Hull Migraine Clinic, UK
F Ahmed1, R Khan1, S Dorsey1,3, H Delrosario1 and M Khalil3
1Hull University Teaching Hospitals Nhs Trust, Hull, United Kingdom
2Hull York Medical School, Hull, United Kingdom
3Spire Hospital Hull and East Riding, Hull, United Kingdom
Objective: Fremanezumab is licensed as preventive treatment in those with > 4 days of headaches per month. In this prospective audit, we evaluate the outcome on Fremanezumab therapy at three years follow up from a tertiary headache clinic in the UK.
Methods: Adult CM patients attending the Hull Migraine clinic were recruited if they were prescribed Fremanezumab for CM prophylaxis and followed up prospectively. Patients maintained a headache diary for at least 1 month prior to and continuously after treatment. All patients tried and failed at least 6 (range 5-11) treatments with 91% failing OnabotulinumtoxinA. We measured monthly headache days (MHD), migraine days (MMD), headache-free days (HFD), analgesia medication (AMD) and triptan days (TD) and Headache Impact Test-6 (HIT6) scores at baseline and monthly during the first three months and subsequently at 12th, 24th and 36 months of treatment. The treatment was discontinued if they had < 30% reduction in either MHD, MMD at the end of first three months. At years one two and three, those that continued were asked to stop treatment for three months if they had < 4 headache days per month for the previous three months and treatment recommenced if any time in the subsequent three months, the headache days went above > 4 per month.
Results: 300 CM patients (221 F, 79 M), mean age 48.6 years (range 21–75), commenced Fremanezumab between November 2020– April 2021. 243 patients (87 F, 56 M) at 3-month follow-up had baseline MHD, MMD and HFD of 28, 17 and 2 days, improving to 15, 6 and 15 days respectively were classed as responders and continued treatment for one year. The remaining 57 patients (34 F, 23 M) stopped treatment due to lack of response. At one year 225 (92.5%) patients (213 F and 12 M) were still getting > 4 days of headaches per month and continued treatment and only 18 (7.5%) patients (12 F, 2 M) were able to stop treatment. All but 3 had to restart therapy as the headache days exceeded > 4 or more in 1-3 months following cessation of therapy. Of 240 (222F 18 F) continued the second year we were able to stop 33 patients (25 F 8 M) who had < 4 days of headache per month in the prior three months. 21 (8.6%) patients stopped as the treatment was no more effective and were commenced other prophylactic therapy. 10 of the 33 relapsed within three months and recommenced treatment. Of the 196 patients given treatment for the third year, 19 achieved remission and 17 (7%) stopped responding and the remaining 160 (65.8%) have been issued the prescription for the 4th year.
Side effects were observed in 41 (30F 11 M) that included constipation, weight gain cold hands and feet and a transient rash at injection site.
Conclusion: The three year real-life follow-up data on Fremanezumab from a tertiary headache clinic shows two third still requiring treatment in year 4 and 1 in 6 became non-responsive following an excellent initial response.
P.10
Retrospective review of safety of galcanezumab in migraine patients with cardiovascular risk factors
S Talukder1, M Deb1, S Broadhurst1 and M Ghadiri-Sani1
1The Walton Centre Nhs Trust, Liverpool, UK
Introduction: Migraine is a common and often debilitating neurological condition impacting 12% of people worldwide, particularly those aged 25-55. The conventional migraine preventatives have been poorly tolerated and often relatively ineffective. Calcitonin Gene Related Peptide (CGRP), has been shown to have a key role in migraine pathophysiology, leading to the development of CGRP receptor antagonists such as galcanezumab as breakthrough treatments.
Although clinical trials and real world evidence has shown galcanezumab to be effective in management of migraine, there remains concerns about it safety in management of patients with co-morbid cardiovascular risk factors thereby, limiting its use in in these cohort of patients.
Objective: A retrospective review to assess the safety of galcanezumab in treating migraine patients with co-morbid vascular risk factors.
Methods: We reviewed our database and the notes for 158 migraine patients who were prescribed galcanezumab from June 2021 to December, 23.
We analysed for demographics, cardiovascular risk factors, and treatment outcomes. The primary outcome was the continuation of galcanezumab in management of migraine, in patients with episodic and chronic migraine, indicating at least 30% and 50% improvement in headache severity and frequency, respectively.
Results: 27 out of the 158 patients on galcanezumab had cardiovascular risk factors. These included hypercholesterolemia (n = 11), hypertension (n = 10), previous strokes (n = 6), diabetes (n = 5) and previous cerebral bleeds (n = 2).
7 patients were over the age of 65, 2 of whom were over the age of 75.
One patient had multiple cardiovascular risk factors including left bundle branch block, heart failure, bilateral pulmonary emboli, Churg strauss vasculitis, Pacemaker in situ diabetes and hypercholestroleamia who has remained on treatment without any exacerbation of underlying conditions.
Among these patients (n = 7), 26% discontinued therapy, all due to inefficacy. 1 patient developed hypertension but decided to continue on treatment while being treated with antihypertensives.
Conclusion: Our data suggests galcanezumab is very well tolerated and effective in prevention of migraine in patients with cardiovascular risk factors. The isolated hypertension case highlights the need for regular monitoring, but overall safety remains favourable.
Based on our data galacanezumab is highly effective (74% response rate), particularly given that it is used in highly refractory patients, who have failed at least 3 oral preventatives and other available anti-CGRP MAB treatments.
Further larger, randomised controlled trials will potentially be needed to explore the safety of galcanezumab in patients with vascular risk factors.
Image 1

P.11
Understanding COVID-Associated Headache: Insights from Patient Studies
Z Akbarkhodjaeva
1
1RSPCSM, Tashkent, Uzbekistan
Background: COVID-19 has been associated with a spectrum of neurological manifestations, including headache, which can significantly impact patients’ well-being and clinical management. This abstract aims to elucidate the characteristics, prevalence, and clinical implications of COVID-associated headache through patient studies.
Materials and Methods: A retrospective analysis was conducted among patients diagnosed with COVID-19 and presenting with headache symptoms at a tertiary healthcare center between March 2020 and December 2021. Demographic data, COVID-19 severity, headache characteristics, and associated symptoms were collected from medical records. Headache phenotypes, including migraine-like, tension-type, and other patterns, were classified based on standardized criteria. Statistical analyses, including descriptive statistics and logistic regression, were performed to identify factors associated with COVID-associated headache.
Results: The study included 300 COVID-19 patients with a mean age of 45 years (SD = 12.6), of whom 55% were female. Headache was reported as a presenting symptom in 40% of cases, with a median duration of 7 days. The predominant headache phenotype was migraine-like (52%), followed by tension-type (30%) and other patterns (18%). Patients with severe COVID-19 illness demonstrated a higher prevalence of headache compared to those with mild or moderate disease (p < 0.05). Notably, headache persisted beyond the acute phase of COVID-19 in 25% of cases, with features suggestive of post-COVID headache syndrome. Logistic regression analysis revealed female gender, younger age, and pre-existing migraine history as significant predictors of COVID-associated headache (p < 0.01).
Conclusion: COVID-associated headache represents a common and clinically relevant manifestation of SARS-CoV-2 infection, with distinct phenotypic characteristics and implications for patient care. Migraine-like features are particularly prevalent among affected individuals, highlighting the need for tailored management strategies targeting migraine-specific mechanisms. Long-term monitoring is warranted to assess the persistence of headache symptoms and the emergence of post-COVID headache syndrome in vulnerable populations. Comprehensive evaluation and multidisciplinary approaches, encompassing neurological, infectious disease, and headache expertise, are essential in addressing COVID-associated headache and optimizing patient outcomes. Further research is needed to elucidate the pathophysiological mechanisms underlying COVID-19-related headache and inform targeted therapeutic interventions.
P.12
Contemporary Prospective Understanding of Migraine Real-World Evidence (CAPTURE): Baseline Migraine Treatment Patterns
C Tassorelli1, M Matharu2, J Ailani3, M Lanteri-Minet4, E Tucker5, J Lam5, Y Liu6, H Ha5, L Delahaye7 and P Pozo-Rosich8
1University of Pavia and C. Mondino Foundation, Pavia, Italy
2Queen Square Institute of Neurology, London, UK
3MedStar, Georgetown University Hospital, Washington, DC, USA
4Pain Department and FHU InovPain, CHU Nice and Côte Azur University, Nice, France; INSERM U1107 Migraine and Trigeminal Pain, Auvergne University, Clermont-Ferrand, France
5AbbVie, Toronto, Canada
6AbbVie, North Chicago, USA
7AbbVie, Rungis, France
8Headache Unit, Neurology Department, Vall d’Hebron University Hospital and Headache and Neurological Pain Research Group, Vall d’Hebron Institute of Research, Universitat Autònoma de Barcelona, Barcelona, Spain
Introduction: Longitudinal data describing the symptom frequency, patient-reported outcomes, and treatment patterns in migraine are currently limited, potentially affecting the care that people experiencing migraine receive. The currently available research has primarily used cross-sectional designs and geographically limited samples, with no assessments of migraine frequency or health care resource utilization, and are generally limited to medication record databases.
Objective: CAPTURE is a 2-year, international, prospective, longitudinal study that aims to elevate understanding of burden of illness, disease course, and treatment patterns among people living with migraine, stratified by headache frequency.
Methods: Adults with migraine diagnosed for >=1 year, aged <50 years at onset, and taking >=1 medication indicated for migraine with >=4 monthly headache days (MHDs) in the 3 months before screening were assigned to cohorts based on MHD frequency (cohort 1: 4-<8; cohort 2: 8-<15; cohort 3: >=15; Figure). Descriptive data for baseline characteristics, including current/prior migraine medications, are presented. Endpoints include change from baseline in MHDs, monthly migraine days, monthly acute medication use days, and patient-reported outcomes across the study period. Durations of current and subsequent migraine treatment use and migraine-related healthcare resource utilisation will also be assessed.
Results: This analysis set (December 2023) included 239 participants (cohort 1: n = 68, 77.6% female; cohort 2: n = 104, 86.1% female; cohort 3: n = 67, 91.9% female; with a mean age of 42.3, 42.6 and 40.8, respectively). In terms of race, most participants across all cohorts were White: 95.5% in Cohort 1, 100% in Cohort 2, and 96.9% in Cohort 3. Cohort 1 had a small representation of Black or African American (1.5%) and Asian (3.0%) individuals, while Cohort 3 included 3.1% American Indian or Alaska Native individuals. Most participants were from Europe, accounting for 77.9%, 76.9%, and 79.1% in Cohorts 1, 2, and 3, respectively. North America was the second-most common region, with 22.1% in Cohort 1, 22.1% in Cohort 2, and 20.9% in Cohort 3. South America was least represented, with only 1.0% of Cohort 2 originating from there. In cohorts 1, 2, and 3, current use of acute migraine medication only was reported for 5.9%, 2.9%, and 0% of participants; preventive medication only for 19.1%, 27.9%, and 32.8%; and both acute and preventive medication for 27.9%, 20.2%, and 26.9%, respectively. Most common current acute medications were triptans and propionic acid derivatives; most common current preventive medications were topiramate, amitriptyline and calcitonin gene–related peptide receptor monoclonal antibodies (Table).
Conclusion: The CAPTURE study will build a large, longitudinal database on migraine treatment patterns in the contemporary era and associated disease trajectories.


P.13
Contemporary Prospective Understanding of Migraine Real-World Evidence (CAPTURE): Baseline Clinical Characteristics
M Ashina1, M Peres2, R Stark3, M Lanteri-Minet4, E Tucker5, Y Liu6, J Lam5, H Ha5, L Delahaye7 and P Pozo-Rosich8
1Department of Neurology, Danish Headache Center, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark; Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
2University of São Paulo, São Paulo, Brazil
3Alfred Hospital and Monash University, Melbourne, Australia
4Pain Department and FHU InovPain, CHU Nice and Côte Azur University, Nice, France; INSERM U1107 Migraine and Trigeminal Pain, Auvergne University, Clermont-Ferrand, France
5AbbVie, Toronto, Canada
6AbbVie, North Chicago, USA
7AbbVie, Rungis, France
8Headache Unit, Neurology Department, Vall d’Hebron University Hospital, and Headache and Neurological Pain Research Group, Vall d’Hebron Institute of Research, Universitat Autònoma de Barcelona, Barcelona, Spain
Introduction: There is insufficient longitudinal evidence describing symptom frequency, impacts on patient-reported outcomes, and contemporary treatment patterns in migraine, which may limit access to care.
Objective: To present interim baseline clinical characteristics for CAPTURE, a 2-year, international, prospective, longitudinal study that aims to enhance understanding of disease burden and treatment patterns among people living with migraine, stratified by headache frequency.
Methods: Adults with >=1-year migraine diagnosis aged <50 years at onset who were taking >=1 medication indicated for migraine and had >=4 monthly headache days (MHDs) in the 3 months before screening were assigned to cohorts based on MHD frequency (cohort 1: 4-<8; cohort 2: 8-<15; cohort 3: >=15; Figure). Descriptive data for baseline demographics and clinical characteristics (migraine duration, MHDs, monthly migraine days [MMDs], monthly acute medication use days, migraine-related comorbidities) are presented. Changes from baseline in MHDs, MMDs, acute medication use days, and patient-reported outcomes across the study period and durations of current and subsequent migraine treatment use will be assessed.
Results: As of December 2023, among the 239 participants (cohort 1: n = 68; cohort 2: n = 104; cohort 3: n = 67), mean age was 42.3, 42.6 and 40.8, respectively, > 95% of participants were White (cohort 1: 95.5%; cohort 2: 100%; cohort 3: 96.9%), > 78% were female (cohort 1: 77.6%; cohort 2: 86.1%; cohort 3: 91.9%), and >77% resided in Europe (cohort 1: 77.9%; cohort 2: 76.9%; cohort 3: 79.1%). North America was the second-most common region, with 22.1% in Cohort 1, 22.1% in Cohort 2, and 20.9% in Cohort 3. Cohort 2 also had 1 participant (1%) from South America. Mean duration of migraine since onset was similar among cohorts (23.0-23.8 years) (Table). Past use of preventive treatments was high (cohort 1, 81.8%; cohort 2, 81.4%; cohort 3, 92.3%). The most prevalent migraine-related comorbidity was hypertension (cohort 1: 4.4%; cohort 2: 7.7%; cohort 3: 9.0%).
Conclusion: CAPTURE aims to provide pivotal data on the longitudinal course of migraine and associated treatment patterns, stratified by headache frequency. This study promises to provide insights for developing tailored treatment approaches for people with migraine.


P.14
Pain profiling in migraine: a systematic review of Quantitative Sensory Testing (QST), Conditioned Pain Modulation (CPM), and Corneal Confocal Microscopy (CCM)
F Van Welie1, A Dahan2, M van Velzen2 and G Terwindt1
1Department of Neurology, Leiden Univerisity Medical Center, Leiden, Netherlands
2Department of Anaesthesiology, Leiden Univerisity Medical Center, Leiden, Netherlands
Introduction: Central sensitization is believed to play a key role in migraine chronification. Managing chronic migraine is challenging, often leading to frequent use of pain medications. Overuse of these treatments can cause central sensitization and increased neuronal excitability. Therefore, understanding the pain modulatory system's role in migraine is crucial.
Objectives: The aim of this systematic review is to identify pain profiling parameters, using Quantitative Sensory Testing (QST), Conditioned Pain Modulation (CPM), and Corneal Confocal Microscopy (CMM), that are reliably different between patients with migraine and healthy controls.
Methods: A comprehensive literature search (up to 1 August 2023) was conducted, which included studies comparing QST, CPM, and CCM parameters between patients with migraine and healthy controls. The quality of the research was assessed using the Newcastle-Ottawa Scale (NOS) for non-randomized studies.
Results: QST studies indicate that migraine patients exhibit lower pressure pain thresholds (PPT), particularly in the trigeminal region. CPM studies suggest a (mild) inhibitory or absent response in migraine patients, not different from controls. High-frequency and chronic migraine patients may exhibit a facilitatory CPM response. With repeated executions of CPM, migraine patients display a diminishing CPM response, a phenomenon not observed in control subjects. CCM investigations in migraine patients revealed conflicting outcomes, likely as a result of small sample sizes and limited characterization of migraine features.
Conclusion: Pain profiling migraine patients varies due to sensory modality, applied methods, anatomical sites, and migraine features. Understanding pain profiling offers insights into migraine pathophysiology, requiring careful selection of parameters and differentiation among migraine subtypes, also considering medication (over)use. Future studies should further determine chronic migraine pain profiles compared to episodic migraine, and study the transition from episodic to chronic migraine, as well as the opposite transformation, as this will provide more insight in the pain mechanisms underlying migraine.
P.15
Early use of erenumab vs non-specific oral migraine preventive medication: Results from the open-label extension of the APPRAISE study
P Pozo-Rosich1,2, D Dolezil3, K Paemeleire4, A Stepien5, P Stude6, J Snellman7, M Arkuszewski7, M Aoun7, C Babanrao Pisal8 and R Gil-Gouveia9
1Headache and Neurological Pain Research Group, Vall d’Hebron Institute of Research (VHIR, Spain
2Neurology Department, Hospital Universitari Vall d’Hebron, Spain
3Headache Center Prague, DADO Medical sro, Czech Republic
4Department of Neurology, Ghent University Hospital, Belgium
5Department of Neurology, Military Institute of Medicine-National Research Institute, Poland
6Neurological Practice Dr Stude, Germany
7Novartis Pharma AG, Switzerland
8Novartis Healthcare Private Limited, India
9Center for Interdisciplinary Research in Health, Portugal
Introduction: The phase 4 APPRAISE study (NCT03927144) demonstrated that earlier use of erenumab provides greater and sustained efficacy, safety and adherence than non-specific oral migraine preventive medications (OMPM) in EM patients with 1 or 2 prior preventive treatment failures.
Objective: To assess the long-term clinical benefit and safety of erenumab (70 or 140 mg) in patients with EM who completed the core phase (CP; screening/baseline periods and 52-week open-label treatment period) of APPRAISE.
Methods: Eligible patients completed the 52-week visit of CP regardless of treatment arm could participate in the open-label extension phase (OLEP) (Figure 1). All patients in OLEP received erenumab; eligibility required patients in the erenumab arm to have benefitted from treatment during CP, while those in the OMPM arm required a treatment switch to erenumab, as determined by the investigator. Erenumab was administered as a monthly subcutaneous injection for up to 52 weeks (contingent on observed continuous benefit). Investigator-reported outcomes on clinical benefit were based on the Clinical Global Impression (CGI) scales. Safety assessments included adverse events (AEs) and serious adverse events (SAEs).
Results: Of 523 patients (84.2%) who completed the CP, 461 (erenumab, n = 343; OMPM, n = 118; as defined by CP randomisation) entered the OLEP and 436 (94.6%) completed the study (erenumab, n = 328 [75.2%]; OMPM, n = 108 [24.8%]). Primary reasons for premature discontinuation of the OLEP were patient decision (2.4%), no longer clinically benefiting (2.0%) and AEs (0.7%). At Week 104, 328/461 patients (71.1%) reported an overall clinical improvement (CGI-Improvement score of ≤3; erenumab, n = 232 [67.6%]; OMPM, n = 96 [81.4%]) and most patients (54.9%) were classified as having marked therapeutic effect without any side effects (CGI-Efficacy index, erenumab, n = 190 [55.4%]; OMPM, n = 63 [53.4%]). The incidence of treatment-emergent AEs (TEAEs) was comparable between treatment arms (erenumab, n = 208 [60.6%]; OMPM, n = 73 [61.9%]), but was overall lower compared with the CP of the study (erenumab, n = 305 [74.8%]; OMPM, n = 157 [76.2%]); AEs were mainly mild or moderate in severity. The overall exposure-adjusted incident rate (EAIR) of TEAEs was 107 per 100 patient years. The most common TEAEs by preferred term were COVID-19, n = 79 (17.1%); study was conducted during the pandemic), nasopharyngitis, n = 38 (8.2%) and constipation, n = 26 (5.6%). The EAIR of constipation was higher in the OMPM arm (16.1 per 100 subject years) than in the erenumab arm (3.1 per 100 patient years). The EAIR of TESAEs was low (3.0 per 100 patient years). A total of 4 (0.9%) patients permanently discontinued the study drug (3 [0.9%] in the erenumab arm and 1 [0.8%] in the OMPM arm). Overall, the EAIR for any AE leading to discontinuation of study treatment was low (0.9 per 100 subject years). No deaths were reported and no new safety signals were observed.
Conclusion: Long-term findings from the OLEP of the APPRAISE study indicate that patients who were treated with erenumab during the CP and those who switched to erenumab during the OLEP demonstrated sustained and consistent clinical benefit with a safety profile consistent with that observed in the CP.
Figure 1

a Treatment discontinuation, when the subject permanently stopped taking study treatment prior to the defined study treatment completion date. Treatment discontinuation did not imply study discontinuation. Every effort was attempted to ensure patients complete the study visit even if treatment was discontinued. Only monotherapy was allowed in either arm. Treatment failure status and decision on whether to switch to a new treatment was checked at every visit and based on investigator and patient's discretion (based on efficacy/tolerability/satisfaction) and not on prespecified cutoffs for certain parameters. Participants who discontinued treatment were monitored according to the protocol. b Core phase included a screening period (up to 2 weeks), baseline period (4 weeks), and an open-label treatment period (52 weeks).
OMPM, oral migraine preventive medication; Pl, principal investigator; SoC, standard of care; TF, treatment failure; W, week.
Pozo-Rosich P, et al. JAMA Neurology. 2024. doi:10.1001/jamaneurol.2024.0368. (Epub ahead of print).
P.16
THE INFLUENCE OF GENDER ON SELF-RATED DISABILITY IN MIGRAINE
M Zaletel1 and G Požlep1
1University Clinical Centre of Ljubljana, Ljubljana, Slovenija
Migraine is a prevalent disorder. The prevalence of migraine is higher in female gender. It is well known that migraine relates to disability and is an important cause of years lived with disability (YLD) among females, 15-49 years. Self-rated disability (SRD) is the subjective perception of disability. It is not clear whether SRD differs between genders. It is expected that SRD would be higher in women.
In our study, we used the European Health Interview Survey (EHIS). The purpose of EHIS was to assess the health status of residents. The survey EHIS (European Health Interview Survey), conducted in 2019, included 9900 adults, aged 15 years or older. Binary logistic regression was used in univariate as well as multivariate analysis. We analyzed self-rated disability (SRD) in both genders.
In migraineurs, SRD significantly relates to absenteeism (OR = 2.86; p < 0.001). In the general population, migraine correlates with SRD (OR = 1.68; p < 0.001) and gender relates to absenteeism (OR = 1.26; p < 0.001). In migraineurs, the association between gender and SRD is not significant (OR = 0.86; p = 0.240). In addition, gender is not associated with absenteeism (OR = 1.14; p = 0.418).
In conclusion, surprisingly, in migraine population gender is not associate with with SRD and absenteeism as well. It seems, that women possess greater copy strategies than men.
P.17
Migraine and osmophobia: preliminary data of a study on memory functions
A Granato1, T Cattaruzza1, T Lombardo1, G Garascia1, L Bartole1 and P Manganotti1
1Neurology Unit, Cattinara University Hospital, Department of Medical, Surgical and Health Sciences, University Of Trieste, Trieste, Italia
Introduction: Migraine is often accompanied by neurovegetative symptoms, such as osmophobia that can be both ictal and interictal. It has been reported that memory and smell share some common cerebral pathways. Memory functions in osmophobic migraineurs have been poorly investigated to date.
Objectives: Aim of the study was to assess memory functions in patients suffering from migraine with osmophobia.
Methods: Migraineurs with ictal or interictal osmophobia referred in a six-month period to the Headache Centre of the University of Trieste were enrolled. Exclusion criteria were chronic migraine, smell and nose pathologies and conditions (e.g uncompensated hypothyroidism, age >50 years, chronic insomnia) or drugs (e.g. antidepressants or antiepileptics for migraine prophylaxis) which could impair memory. Demographic data and characteristics of headache were collected. MoCA test was used for cognitive screening. Then memory, visuospatial ability, attention and executive functions were assessed through Rey Auditory Learning Verbal Test (RALVT), Rey–Osterrieth Complex Figure (ROCF), Multiple Features Target Cancellation (MFTC) and Stroop Color and Word Test (SCWT), respectively.
Results: Sixteen patients were enrolled (14 females, 2 males; mean age 39 ± 9). All of them had a medium-high education level (16 ± 1 years). All patients had ictal and 60% had interictal osmophobia. About half of patients (56%) always tended to avoid smells. The most frequently pejorative or trigger smell was smoke (87% and 50%, respectively). Migraine prophylaxis was used in 60% of cases; 56% improved ictal osmophobia after the assumption of a symptomatic drug. All patients scored within normal limits in the MoCA test. As regards the memory domain, the majority of our sample scored within normal limits in RALVT immediate recall (44% pE4; 13% pE3; 31% pE2), delayed recall (38% pE4; 38% pE3; 6% pE2), delayed recognition (100% pE4) and ROCF delayed recall (75% pE4; 0% pE3; 6% pE2). None of our patients showed any deficit in the visuospatial task, scoring within the upper normal range in ROCF copy (100% pE4). To assess attentive functions, we measured accuracy, false alarms and time of execution in MFTC. Only 2 patients had and accuracy below cutoff points according to educational level (13%<0,869; 88%>0,869), however all the execution times were within the cutoff value, and there were no false alarms. Finally, the SCWT was performed with a good accuracy by most patients (only 6% had pE0 and 19% pE1) and with a speed within normal limits by all of them.
Conclusions: Our sample of migraineurs with osmophobia had a cognitive level within normal range. Isolated deficits in memory (RALVT delayed recall, ROCF delayed recall), attention (MFTC accuracy) and executive functions (SCWT accuracy) were observed only in a small percentage of patients, preserving overall high cognitive performances.
P.18
Understanding Medication Overuse Headache: A Clinical Overview and Statistical Analysis of Patient Cases
Z Akbarkhodjaeva1 and G Rakhimbaeva2
1RSPCSM, Tashkent, Uzbekistan
2Tashkent Medical Academy, Tashkent, Uzbekistan
Background: Medication overuse headache (MOH) presents a substantial challenge in headache management due to its complex etiology and high prevalence rates. This abstract aims to analyze clinical data and statistics pertaining to MOH cases, elucidating demographic trends, medication usage patterns, and treatment outcomes.
Materials and Methods: A retrospective analysis of MOH cases was conducted, utilizing medical records from a tertiary headache clinic spanning a five-year period. Demographic information, headache characteristics, medication usage history, and treatment interventions were collected and analyzed. Statistical methods, including descriptive statistics and inferential analyses, were employed to elucidate key trends and associations.
Results: The analysis included data from 500 patients diagnosed with MOH. The majority of patients were female (68.5%) with a mean age of 42 years (SD = 10.3). Primary headache diagnoses, such as migraine (62%) and tension-type headache (28%), were common among MOH patients. The most frequently overused medications were nonsteroidal anti-inflammatory drugs (NSAIDs) (47%), followed by combination analgesics containing caffeine (23%) and triptans (18%). Statistical analysis revealed a significant association between the duration of medication overuse and headache frequency (p < 0.001), with longer overuse periods correlating with increased headache frequency and severity. Furthermore, patients with comorbid psychiatric disorders demonstrated poorer treatment outcomes compared to those without psychiatric comorbidity (p = 0.012).
Conclusion: Medication overuse headache represents a prevalent and challenging condition in headache medicine, particularly among individuals with pre-existing primary headache disorders. This study provides valuable insights into the demographic characteristics, medication usage patterns, and treatment outcomes of MOH patients. Early recognition and intervention, tailored treatment approaches, and addressing comorbid psychiatric conditions are essential strategies in managing MOH effectively and reducing its burden on patients and healthcare systems. Further research is warranted to explore optimal treatment strategies and long-term outcomes in this patient population.
P.19
Awareness, Knowledge, and Practice towards Medication Overuse Headache in Thailand: A University Hospital-Based Survey in Residency Training Programs
P Anukoolwittaya1,2,3,4,5, T Pongpitakmetha1,2,3,4,5,6, A Hiransuthikul1,7, S Thanprasertsuk1,2,3,4,5,8 and W Rattanawong1,5,9
1Chulalongkorn Headache and Orofacial Pain (CHOP) Service and Research Group, Division of Neurology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
2Division of Neurology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
3Cognitive Clinical and Computational Neuroscience (CCCN) Center of Excellence, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
4Chula Neuroscience Center, King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, Bangkok, Thailand
5Thai Headache Society, The Neurological Society of Thailand (NST), Bangkok, Thailand
6Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
7Department of Preventive Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
8Department of Physiology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
9Department of Medicine, Faculty of Medicine, King Mongkut’s Institute of Technology Ladkrabang, Bangkok, Thailand
Introductions: Medication overuse headache (MOH) is a chronic headache disorder categorized within secondary headaches according to the ICHD-3 classification. The overuses of these drugs worsen headaches in individuals with underlying headache disorder(s), usually migraine and/or tension-type headache. MOH significantly impacts patients’ lives, contributing to disability, and the burden of healthcare cost. MOH represents a significant challenge in patient care, with physicians playing a vital role in its prevention and management. Nonetheless, awareness, knowledge, and practices concerning MOH among physicians are often found to be inadequate.
Objectives: The primary objective is to explore awareness, knowledge, and practice about medication overuse headache (MOH) in various residency training programs, which commonly encountering the headache patients, including neurology, internal medicine, and family medicine. Our secondary goal is to evaluate factors, including specialty training programs, influencing participants’ awareness, knowledge, and practices concerning MOH.
Methods: A cross-sectional university-based hospital study was conducted to investigate awareness, knowledge, and practices related to MOH among resident doctors at King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, Bangkok, Thailand. Participants were surveyed using an internet-based questionnaire. Pearson's chi-squared test (X2) analyzed associations in categorical data.
Results: Out of 130 residents, 70 participated in the study. Baseline demographic data was shown in Table 1. 10% of residents were unaware that analgesics could exacerbate headaches, with this unawareness being especially notable in family medicine (31.8%) compared to other specialties (X2 = 16.97, p = 0.02) (Figure 1-1A). For the knowledge aspect, 11.4% of participants were uncertain about the classification of MOH. 31.4% and 44.3% of participants were unsure about the frequency of simple analgesic and migraine-specific drug use leading to MOH, respectively, with internal medicine and family medicine residents showing uncertainty (X2 = 6.41, p = 0.41 and X2 = 14.47, p = 0.025 respectively) (Figure 1-1B, 1-1C). Regarding the practice aspect, 58.6% of respondents never recommended headache diaries for patient follow-up. Neurology residents (n = 18, 75%) showed a significantly higher endorsement of headache diaries compared to other specialists (X² = 18.04, p < 0.01) (Figure 1-2A). 32.9% of respondents occasionally asked patients about headache frequency, 5.7% never inquired, while 61.4% of them always asked. Neurology residents (n = 22, 91.7%) significantly surpassed others in regularly exploring headache frequency (X² = 15.87, p = 0.003) (Figure 1-2B). The method of headache frequency assessment was summarized in Figure 1-2C, 1-2D, and 1-2E. Neurology residents (n = 15, 62.5%) significantly favored using headache diaries compared to other specialties (X² = 20.25, p < 0.001) (Figure 1-2C). Prescription habits for analgesic medications (Figure 1-3) revealed that 87.1% of respondents prescribed acetaminophen, 92.9% prescribed NSAIDs, 34.3% prescribed triptans, 10% prescribed ergots, and 22.9% prescribed opioids. Neurologists significantly prescribed triptans more than other specialists (X² = 14.95, p < 0.001) (Figure 1-3C). Internal medicine residents prescribed opioids more than other specialists (X² = 7.959, p = 0.019) (Figure 1-3E).
Conclusion: From our study, neurology residents performed better in many aspects compared with other specialty residents. This study shows the gap in awareness, knowledge, and practice of MOH, especially in non-neurology resident training programs. Continuing medical education with a multifaceted approach may be required to address the issues.


P.20
Manageable Environmental Factors Affect Treatment Response as much as Migraine Phenotype
B Piri Cinar1, O Iyilikci2, E Uluduz3, S Eyupoglu4, M Iskender5, D Uluduz6 and A Ozge7
1Samsun University, Samsun, Turkey
2Manisa Celal Bayar University, Manisa, Turkey
3Koc University, Istanbul, Turkey
4Brain 360 Holistic Approach Center, Istanbul, Turkey
5Kocaeli Special Institution, Kocaeli, Turkey
6Cerrahpasa University, Istanbul, Turkey
7Mersin University, Mersin, Turkey
Introduction: Migraines are a prevalent and debilitating neurological condition that can significantly impact a person's quality of life. While various genetic and environmental factors contribute to the development and chronification of migraines, the role of specific environmental factors in the chronification of this condition remains inadequately explored.
Objectives: This article aims to address this research gap by focusing on the impact of manageable and unmanageable factors on the chronicity of migraine.
Methods: Ethical approval was obtained for this cross-sectional-observational study (2023/466), and the study was registered in clinical trails (NCT06304675). Demographic characteristics of the patients were recorded on the demographic data form. Then, the patient's headache characteristics (duration, type, presence of aura, accompanying features, etc.) and the answers to the questions about possible triggers of migraine and environmental factors were recorded in the data form.
Results: In chronic migraine group reported oversleeping, stress as a trigger at a higher rate versus episodic migraine group. In the episodic migraine group, it was found that participants who have TV transmitters were significantly less likely to benefit from treatment, while in chronic migraine group, it was found that participants who have pets were significantly less likely to benefit from treatment.
Conclusion: In conclusion, this study sheds light on the intricate relationship between environmental factors, migraine phenotype, and treatment response. By employing comprehensive statistical methods and analyzing a rich dataset, we have gained valuable insights into the complexities of migraine management.
P.21
Study Design and Methodology of PRECLUDE: A Phase 3, Multicenter, Randomized, Double-blind, Placebo-Controlled Trial of OnabotulinumtoxinA for the Preventive Treatment of Episodic Migraine
J Ailani1, P Pozo-Rosich2, A Patel3, T Nguyen4
and L James4
1Georgetown University Hospital, Washington DC, USA
2Vall d’Hebron Hospital and Institute of Research, Barcelona, Spain
3Kansas Institute of Research, Overland Park, USA
4AbbVie, North Chicago, USA
Introduction: Episodic migraine (EM) is part of the migraine disease spectrum and at high frequency approaches similar disability levels associated with chronic migraine (CM). OnabotulinumtoxinA is currently indicated for CM prevention.
Objective: To describe the study design and methodology of the phase 3 study of onabotulinumtoxinA for the preventive treatment of episodic migraine (EM) in adults (NCT05028569).
Methods: PRECLUDE is a phase 3 multicenter, randomized, double-blind, placebo-controlled study of onabotulinumtoxinA in adults 18 to 65 years of age with a history of migraine meeting ICHD-3 diagnostic criteria for ≥12 months. Study participation includes a 4-week screening/baseline phase using an electronic diary (e-Diary). Participants with EM who meet entry criteria are randomized 1:1:1 to onabotulinumtoxinA dose A, onabotulinumtoxinA dose B, or placebo into the 24-week double-blind placebo-controlled phase. Those who complete this phase may continue to the 24-week open-label phase and receive onabotulinumtoxinA dose A at 12-week intervals for up to 2 treatment cycles.
Results: This study is targeting enrollment of 777 participants across ∼125 sites in North America, Europe, and Israel. The primary endpoint is change from baseline in the frequency of monthly migraine days over Months 5 and 6. Secondary efficacy endpoints include change from baseline in monthly headache days, responder status for 50% reduction in monthly migraine days, monthly acute headache medication days, AIM-D Physical Impairment domain score, and MSQ v2.1 Role Function-Restrictive domain score. Safety endpoints included monitoring adverse events, clinical laboratory testing, vital sign measurements, and Columbia-Suicide Severity Rating Scale scores. Efficacy assessments are based on information recorded by the participant in an e-Diary on headache duration, characteristics, symptoms, and acute headache medication use. Several patient-reported outcomes measures are also assessed.
Conclusions: PRECLUDE will evaluate the use of OnabotulinumtoxinA for the preventive treatment of EM.
P.22
Striking Two Nerves: A Delayed Diagnosis of Glossopharyngeal Neuralgia Presenting as Premature Ventricular Contractions
A Sellers1 and M Blaya1
1Memorial Healthcare System, Pembroke Pines, United States of America
Introduction: Glossopharyngeal neuralgia (GPN) is characterized by severe paroxysmal pain along the distribution of the glossopharyngeal nerve. While GPN primarily involves the glossopharyngeal nerve, the vagus nerve is closely related anatomically and functionally. Thus, rare cases of GPN caused by neurovascular compression with involvement of the vagus nerve can result in symptoms of cardiac irregularities. Several reported cases of GPN with cardiac syncope have been identified and managed with microvascular decompression; however, per our literature review there have been no reports of GPN presenting as premature ventricular contractions.
Objectives: This case report emphasizes the importance of considering GPN in patients with atypical, unexplained symptoms that involve vagal and/or glossopharyngeal nerve functions.
Methods: We present a case of a 33-year-old female physician with a history of polycystic ovarian syndrome, alopecia, and positive anti-thyroid antibodies who developed palpitations, chest discomfort, and dry cough in July of 2021. She was initially diagnosed with gastroesophageal reflux disease (GERD) and pericarditis, yet despite an invasive diagnostic process involving esophagogastroduodenoscopy (EGD) and subsequent medical treatment, her symptoms persisted. The patient then scheduled an appointment with Electrophysiology, who discovered a significant premature ventricular contraction (PVC) burden and frequent ventricular ectopy. She underwent PVC ablation in September of 2021; however, her symptoms persisted as the true underlying etiology remained unidentified and thus untreated.
Shortly after the onset of chest discomfort and palpitations, the patient also developed brief, episodic, excruciating pain localized to her posterior throat precipitated by swallowing. This pain progressed over time, evolving into a near-constant aching sensation. The patient was evaluated by an Ear, Nose, and Throat (ENT) specialist in October of 2021. She underwent flexible laryngoscopy and CT neck, which excluded ENT pathology including structural abnormalities. The patient was subsequently referred to Neurology for further evaluation.
In March of 2022, workup with magnetic resonance angiography (MRA) of the brain revealed a vascular loop, likely a branch of the anterior inferior cerebellar artery (AICA), in contact with the right glossopharyngeal nerve. This finding further confirmed the diagnosis of classical glossopharyngeal neuralgia, with suspected vascular compression of the glossopharyngeal and vagus nerves as the etiology of the plethora of symptoms she experienced over the past year. In June of 2022, Neurosurgery performed a microvascular decompression through a right-sided suboccipital approach for treatment.
Results: Following surgical procedure, the patient obtained repeat computed tomography (CT) of the brain which demonstrated stable postsurgical changes without apparent complication. In July of 2022, the patient’s Neurosurgical follow-up appointment revealed complete resolution of throat pain with no residual symptoms.
Conclusion: Our patient’s clinical journey highlights the importance of recognizing atypical presentations, in particular cardiac dysregulation, of GPN in order to minimize diagnostic delays and optimize patient care. This patient experienced a prolonged diagnostic process involving multiple medical specialties with extensive and often invasive diagnostic investigation before finally reaching the diagnosis of glossopharyngeal neuralgia and undergoing appropriate treatment; we aim to mitigate such delays in future patients by increasing awareness and education.
P.23
From pain to peace: Galcanezumab's Impact towards very low frequency episodic migraine in real-world patients
W Rattanawong1,2,8, A Hiransuthikul2,3, T Pongpitakmetha2,4,7,8, P Anukoolwittaya2,5,7,8 and S Thanprasertsuk2,6,7,8
1Faculty of Medicine, King Mongkut's Institute Of Technology Ladkrabang, Bangkok, Thailand
2Chulalongkorn Headache and Orofacial Pain (CHOP) Service and Research Group, Division of Neurology, Department of Medicine, King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, Bangkok, Thailand
3Department of Preventive Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
4Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
5Division of Neurology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
6Department of Physiology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
7Chula Neuroscience Center, King Chulalongkorn Memorial Hospital, Bangkok, Thailand
8Thai Headache Society, The Neurological Society of Thailand, Bangkok, Thailand
Introduction: Studies have shown that migraine patients with a higher frequency of headache days experience greater disease burden and disabilities. Current guidelines suggest that the effectiveness of a preventive medication is indicated by a reduction of more than 50% in headache days per month. However, cumulative studies suggest that this number does not elucidate the true needs of migraine patients. In contrast, achieving very low-frequency episodic migraine (VLFEM) is associated with a lower burden and greater success in discontinuing preventive medication without or minimal increase in migraine headache days.
Objective: To compare between migraine patients using galcanezumab with migraine patients using oral migraine preventive medication (OMPM) in achieving VLFEM at month 3 and 6.
Methods: We conducted a retrospective data collection of patients who attended the headache clinic at King Chulalongkorn Memorial Hospital from January 2019 to September 2023. The study included patients aged 18 years and older, diagnosed with episodic migraine (EM) and chronic migraine (CM) according to the International Classification of Headache Disorders, version 3 (ICHD-3), who had been using galcanezumab for at least 3 months.
Migraine classes were defined as followings: VLFEM, having 0-3 headache days per month; low-frequency episodic migraine (LFEM), having 4-7 headache days per month; high-frequency episodic migraine (HFEM), having 8-14 headache days per month; and CM, having ≥15 headache days per month. Kaplan-Meier plots were used to assess the cumulative incidence of patients who converted to VLFEM at months 3 and 6, and log-rank test was used to assess the differences between patients using OMPM and galcanezumab. The Sankey diagram was used to illustrate changes in migraine classes for each patient. A multivariate Cox regression model was used to evaluate the association between psychiatric comorbidities (depression, anxiety, and/or bipolar disorder) and the conversion to VLFEM.
Results: Among 62 patients included, 31 (50%) used galcanezumab and 31 (50%) used OMPM. The OMPM group consisted of tricyclic antidepressants (35%), beta-blockers (23%), pregabalin (19%) topiramate (10%), Serotonin and norepinephrine reuptake inhibitors (6%) and other medications (7%). Baseline characteristics are detailed in the Table. Kaplan-Meier analysis of the conversion rate to VLFEM showed that galcanezumab group had significantly higher rates of achieving VLFEM compared to OMPM group: 29.0% vs. 6.5% at month 1, 46.5% vs. 19.6% at month 3, 52.4% vs. 29.7% at month 6, and 72.8% vs. 44.5% at month 9 (p = 0.03). Subgroup analysis using Sankey diagram showed higher percentage of patients achieving VLFEM transitioned from HFEM compared to those transitioning from CM in both groups at month 3 (Figure). Specifically, for HFEM to VLFEM, the rates were 29% for OMPM and 66% for galcanezumab, while for CM to VLFEM, the rates were 0% for OMPM and 11% for galcanezumab. Using multiveriate Cox regression model, there was no significant association between psychiatric comorbidities and the achievement of VLFEM.
Conclusion: Galcanezumab shows a greater conversion rate in achieving VLFEM compared to OMPM. However, most patients achieving VLFEM were initially HFEM. This could lead to a shift in the early initiation of monoclonal CGRP treatments in the future.
Figure
Table
P.24
EFFECTIVENESS OF NEURAC TREATMENT METHOD IN PATIENTS WITH MIGRAINE ASSOCIATED WITH NECK PAIN
D Sotnikov, O Potapov and O Kmyta
1Sumy State University, Sumy, Ukraine
2Medical Center “Neuromed”, Sumy, Ukraine
Introduction: Most patients with migraine periodically have accompanying pain in the neck. There are still debates about the association between migraine and neck pain: differentiation from cervicogenic headache, which is a concomitant or trigger of migraine, or is it a manifestation of migraine attack?
Objectives: To establish options for the coexistence of neck pain with chronic migraine and to study the effectiveness of using the neurac treatment method with sling exercises on the course of migraine.
Methods: 68 migraine patients who had neck pain aged 23 to 60 (average 33.4 ± 18.4) years were examined. The majority of patients were women – 53 (78%). Conditionally, patients were divided into two groups: 1st – neck pain was considered as a concomitant or one of the triggers of migraine attacks 39 (57.4%), 2nd – neck pain as a manifestation of chronic migraine 29 (42.6%).The first group included patients with an increase in migraine attacks after the appearance or growth of neck pain, worsening was provoked by long-term unusual static or dynamic load on the cervical spine, disappearance or reduction of headache after blockade of the large occipital nerve or facet joint C2, significant changes in X-ray or MRI examination (ante- or retrolisthesis, hernias between vertebral discs).
In both groups, the neurac treatment method with sling exercises was performed three times a week for 2 weeks.
Results: After a one-month course of neurac therapy, the number of days with headache decreased by 50% or more in the 1st group in 28 (41.2%) patients, in the 2nd - in 16 (23.6%). At the same time, the number of days with acute pain (more than 5 VAS points) decreased by 35.9% and 18.5%, and the number of days with inter-attack (background) pain – by 43.1% and 29.4%. Also, the average headache intensity decreased significantly - by 21.7% and 15.3%.
Conclusions: The effectiveness of neurac treatment method was demonstrated in both groups, however, in the group where neck pain was the trigger, the number of headache days and pain intensity decreased more significantly. Selected criteria for evaluating neck pain can be used to diagnose its origin.
P.25
Real-world effectiveness of erenumab in Japanese patients with migraine: A 6-month single-center observational study
S Kobayashi1, K Suzuki1, S Suzuki1, M Shioda1 and K Hirata1
1Dokkyo Medical University, Mibu, Shimotsuga, Japan
Background: Real-world evidence on the efficacy of erenumab in Asian migraine patients with various comorbidities and previous failure of multiple drug treatments is still limited.
Methods: We conducted a 6-month single-center cohort study of 45 patients with episodic or chronic migraine (CM) treated with erenumab. In this cohort, 60.0% were switching from other calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs), and 66.7% had experienced four or more prophylactic failures. The change in monthly migraine days (MMD) from baseline and the percentage of responders after treatment were calculated. Weekly migraine days (WMD) were obtained at baseline, months 1, 2, and 3, and compared between weeks 2 and 4.
Results: Thirty-six percent, 47%, and 63% of patients had a ≥ 30% response at 1, 3, and 6 months, respectively; the cumulative percentage of patients who had a ≥ 30% response at 6 months was 85%. Early responders (average ≥30% response at 1-3 months) accounted for 37.8%, 55.6%, and 25.9% of patients in the overall, CGRP mAb-naive, and CGRP mAb-switching groups, respectively. In the total, CGRP mAb-naive, and CGRP mAb-switching groups, 46.4%, 37.5%, and 58.8% of the non-early responders were late responders (averaging <30% response at 1-3 months and >30% response at 4-6 months), respectively. Mild side effects were observed in 5 patients (11.1%). Wearing-off (defined as an increase in WMDs ≥2 between weeks 2 and 4) was observed in 2.4% to 12.5% at months 1-3.
Conclusions: Erenumab was effective in the prophylactic treatment of migraine patients. At least 4-6 months would be preferable to evaluate efficacy in patients switched to erenumab from other CGRP mAbs.
P.26
Mood Disturbance and Migraine: Preliminary results from a Headache Database
U Ashraf1,2,3 and S Tomlinson1,3
1St Vincent's Hospital, Sydney, Australia
2University of New South Wales, Sydney, Australia
3University of Notre Dame Australia, Sydney, Australia
Introduction: Mood disorders are a common comorbidity in migraine patients. The relationship is thought to be bidirectional. Shared mechanisms between migraine and mood disorders have not been completely elucidated. The relationship between premonitory mood disturbance, mood disturbance during the migraine attack and a past medical history of mood disorders may provide further clarity regarding the possible biological underpinnings of these two comorbid conditions.
Objective: To investigate the relationship between premonitory mood disturbance, mood disturbance during the headache phase of migraine and medical background of mood disorder.
Methods: A retrospective cohort study was performed on patients from the Headache Clinic at St Vincent’s Hospital Sydney from February 2024 and collated onto a secure REDCAP database. Patients with migraine (ICHD-3 criteria) were included. Statistical significance was calculated using Fisher’s exact test.
Data was collected regarding mood disturbance during headaches, defined as irritability, anxiety or depressive symptoms during the headache phase and in the post-drome phase. Premonitory mood disturbance was categorised as irritability, anxiety or depressive symptoms with onset 24 hours to 1 hour before onset of headache. A background of mood disorder was based on a past medical history of a mood disorder on targeted history and review of clinical documentation.
Results: 58 patients with migraine had data on premonitory symptoms, past medical and psychiatric history recorded, and whether mood disturbance during the headache phase of their migraine. 43/58 (74%) had high frequency episodic migraine or chronic migraine (HFEM/CM) and 15/58 (26%) had episodic migraine (EM). 46/58 (79%) patients were women.
72% (42/58) experienced mood disturbance during headaches. 48% (28/58) patients had premonitory mood disturbance with 41% (24/58) patients having premonitory irritability, 21% (12/58) having premonitory anxiety and 10% (6/58) having premonitory depressive symptoms. 50% (29/58) patients had a current or previous diagnosis of a mood disorder. Table 1 shows the correlation between premonitory mood disturbance symptoms and headache-phase mood disturbance with background of mood disorder.
64% (18/29) patients with a background of mood disorder had premonitory symptoms of mood disturbance, compared to 33% (10/29) patients without a background of mood disorder (p = 0.065). 61% (17/29) patients with a background of mood disorder had premonitory irritability, compared to 23% (7/39) without a background of mood disorder (p = 0.001). 25% (7/29) patients with a background of mood disorder had premonitory anxiety, compared to 17% (5/29) patients without a background of mood disorder (p = 0.747). 14% (4/29) patients with a background of mood disorder had premonitory depressive symptoms, compared to 7% (2/29) patients without a background of mood disorder (p = 0.670).
Conclusion: Results confirm mood disturbance is common both during headache attacks and as a premonitory symptom. Patients with a background of mood disorders are more likely to have premonitory irritability. Premonitory mood disturbance, rather than mood disturbance during the headache phase, is associated with a background of mood disorder. Hence, targeted history of premonitory mood disturbance may be useful for screening for the presence of an underlying mood disorder.

P.27
Getting to grip with headache in schools
D Kernick1 and L Whitworth2
1National Health Service, Exeter, United Kingdom
2Ted Wragg Acadamy Trust, Exeter, United Kingdom
Introduction: 11% of children have migraine and 20-30% will experience tension type headache. The World Health Organisation puts headache disorders as third in the world in terms of disability in the under 25-year age group. Most young people will go on to experience migraine as an adult and early diagnosis and management may reduce this burden and prevent the transition to chronic migraine. Research we have undertaken shows that despite this high unmet need, less than 10% of people will seek help from their GP and when they do so, their needs are poorly addressed.
Objectives: Our objective is to reduce the burden of headache in a school setting.
Our aims are:
i). To describe the burden of headache in a school setting
ii). To develop a whole school toolkit to address this problem.
Methods: We measured headache frequency and its association with quality of life (PEDsQ4L, PedMidas) and in particular impact on school performance in 875 students age 11-15. We also explored a relationship of headache with hydration, eating breakfast and bullying.
We then developed a whole school toolkit to address the unmet need we had identified.
Based on a previous study, we estimated that for a 95% confidence level to identify a 10% + −2% population rate of our main variable of interest, (the percentage of subjects that had headache more frequently than once a week), we would need a sample size of 737 subjects.
Our data was not normally distributed and is presented in medians and interquartile ranges. We used Chi squared tests for categorical data and Spearman’s rank correlation (Rho) to test correlation between variables.
Results: 30% of students had problematic headache two or more times a week. There was a correlation of headache frequency with quality of life and in particular a significant impact on school functioning. Headache frequency was significantly correlated with missing breakfast, poor hydration and a history of bullying.
See Table in additional information.
We developed an intervention consisting of:
Info for staff about the project and raise the profile of the problem – video and written.
Addressing the personal headache needs of staff – self-help handbook for staff and video.
Students: assembly/tutor resource; lesson for PHSE year 7 and 11; written info and cartoon; signposting for mental health co-morbidity.
Parents: support material and video for parents of child identified with problematic headache. Letter they can take to their GP.
School first aiders – algorithm for headache presentation.
School nurses. Educational material.
Support material for GPs
School mental health team. Educational material to raise awareness as headache as a co-morbid problem.
Conclusion: Headache is an area of high unmet need associated with poor quality of life and school performance. Simple educational interventionssuch as we have developed delivered in a school setting are likely to have an impact upon the quality of life of children and their academic performance.
Table
P.28
Changes in family burden after the introduction of CGRP mAbs
K Murakata1, D Danno1, K Ota1, H Sugiyama1, Y Kashiwaya1, S Kikui1 and T Takeshima1
1Tominaga Hospital, Osaka, Japan
Migraine is a disease that can interfere with daily life, and it has been reported that the burden of illness includes a decrease in the patient's quality of life (QOL) and loss of labor. On the other hand, it has become clear that migraine affects not only social loss but also loss of time spent with the family, and it is a disease that places a heavy burden on the patient's family, such as forcing them to worry and endure.
Objective: We investigated changes in the burden on families after the introduction of human monoclonal antibody therapy targeting calcitonin gene-related peptides or their receptor (CGRP mAbs) and changes in the degree of burden on daily life in patients from the perspective of their families.
Methods: A questionnaire survey was conducted among the families of 32 patients with migraine (26 women and 6 men; mean age 44.2 ± 20.5 years) who were treated with CGRP mAbs in our hospital from October 2023 to December 2023.
Results: The average duration of illness in 32 patients was 22.8 ± 17.0 years, and all patients had migraine without aura, five patients (15.6%) had migraine with aura, 25 (78.1%) had chronic migraine, and 18 (56.3%) had medication overuse headache. The average treatment duration with CGRP mAbs was 16.8 ± 8.7 months, with 3 patients (12.5%) switching to another CGRP mAbs and 3 patients (12.5%) discontinuing the treatment. The breakdown of CGRP mAbs was as follows: galcanetumab (n = 11), fremanentumab (n = 18), and elenumab (n = 7). The average number of days with migraine attack and acute medication utilization were 23.9 ± 7.9 days and 14.6 ± 9.8 days respectively before the treatment, and those 10.2 ± 8.2 days and 5.7 ± 6.8 days after treatment. From the perspective of family members, 87.5% of the families reported that their condition had improved and 71.9% answered that the impact of the patient’s migraine on their family had improved.
Conclusions: The introduction of CGRP mAbs reduced the number of headache days and the number of days of acute treatment medication use in patients with migraine. Furthermore, in addition to the improvement of the patient's burden, as seen by the family, there was an improvement in the family burden. Since the number of cases in this survey was small, it is necessary to conduct a study with a larger cohort to validate these findings.
P.29
Efficacy and continuability of 675 mg fremanezumab administration over several years
S Yoshida1, N Imai1, M Keicho1, J Kamimura1, A Moriya1, N Yagi1, R Suzuki1, T Konishi1 and M Serizawa1
1Japanese Red Cross Shizuoka Hospital, Shizuoka, Japan
Introduction: Fremanezumab is a fully humanized monoclonal antibody that selectively targets calcitonin gene-related peptides (CGRPs). Subcutaneous injections of Fremanezumab at monthly and quarterly doses of 225 mg or 675 mg, respectively, have been approved for the prevention of migraine. Several studies have demonstrated the efficacy and tolerance of both dose schedules, finding that they significantly reduce the frequency and severity of headache attacks. However, data on the long-term adherence to these schedules in the real world are limited, especially regarding quarterly administration of 675 mg.
Objectives: To evaluate the efficacy and continuability of 675 mg fremanezumab administration over two years and analyze the reasons for discontinuation.
Methods: This was a single-center observational study. Among the patients attending our headache outpatient clinic, those aged 17–66 years in whom the 675 mg fremanezumab quarterly dose schedule was initiated from November 2021 to June 2022 were enrolled. Both chronic migraine (CM) and episodic migraine (EM) patients were enrolled in this study. The occurrence of adverse effects was evaluated in all cases, and the frequency and severity of headaches were recorded using a headache diary. The observation period terminated in May 10, 2024. Among the patients who were not receiving the 675 mg dose of fremanezumab at this point, the reason for cessation was investigated based on the follow-up medical records.
Results: Twenty-eight patients were enrolled, of whom 15 had CM and 13 had EM. One patient with CM was excluded due to withdrawal after the first injection. The mean length of the overall observation period was 15.6 months, with a standard deviation (SD) 9.8. One patient with CM developed injection site erythema after the first administration, but no other remarkable adverse events occurred. Of the 27 analyzed patients, the treatment was effective in 77.8% (n = 21; mean 18.8 months ± SD 8.6), while 22.2% of cases (n = 6; mean 4.5 months ± SD 3.6) showed insufficient effectiveness, resulting in medication discontinuation. Among the effective cases, 52.4% (n = 11; mean 25.2 months ± SD 2.2) have continued the 675 mg dose fremanezumab until now; treatment was discontinued due to sufficient recovery in 38.1% (n = 8; mean 12.1 months ± SD 8.1); 4.7% (n = 1) ceased treatment after pregnancy. Further, in 1 patient (4.7%), the drug was effective, but the administration was ceased because of injection-site erythema. Among the non-effective cases, 50% (n = 3) switched from fremanezumab to erenumab, 33.4% (n = 2) switched to galcanezumab, and the remaining 16.7% (n = 1) withdrew from follow-up. Of the three patients who switched from fremanezumab to erenumab, two still receive erenumab, while one switched from erenumab to fremanezumab at a monthly injection of 225 mg when erenumab became less effective. Of the two patients who switched from fremanezumab to galcanezumab, galcanezumab has been continued owing to its effectiveness.
Conclusion: This single-center, observational study confirmed that a 675 mg dose of fremanezumab effectively reduced the frequency of days of headache, further demonstrating that this administration may lead to cessation of the medication by recovery.
P.30
Calcitonin gene-related peptide monoclonal antibody may improve restless legs syndrome: implication from a patient with comorbid migraine
S Mukuto1, S Kobayashi1, S Suzuki1, T Shiina1, K Hirata1 and K Suzuki1
1Dokkyo Medical University, Shimotuga, Mibu, Kitakobayashi, Japan
Background: A significant association between migraine and restless legs syndrome (RLS) has been reported, and their coexistence is not uncommon. We report a patient with concomitant migraine and RLS who showed improvement of both migraine and RLS after treatment with galcanezumab, a calcitonin gene-related peptide (CGRP) monoclonal antibody.
Case presentation: A 47-year-old woman had been treated in our outpatient headache clinic for migraine without aura. The patient had RLS since childhood and had been treated with dopamine agonists and α2δ ligands. Over the past 2 months, the patient suffered from frequent migraine headaches and worsening RLS symptoms, despite ongoing treatment. Therefore, galcanezumab was started. After 1 month, the number of monthly headache days decreased from 20 to 4, and her score on the International RLS Study Group Rating Scale score improved from 38 to 10. Her photophobia, phonophobia and osmophobia were also markedly improved. The efficacy of galcanezumab for both migraine and RLS was sustained over 5 months.
Conclusion: Our findings suggest that CGRP monoclonal antibodies may have a beneficial effect on both migraine and RLS. However, additional clinical studies are needed to clarify how CGRP antagonism affects RLS.
P.31
New daily persistent dizziness: a case report
D Moreno Ajona1, J Moraleda2 and P Goadsby1
1NIHR King's Clinical Research Facility, & SLaM Biomedical Research Centre, The Wolfson Sensory, Pain and Regeneration Centre (SPaRC), Institute of Psychiatry, Psychology and Neuroscience (IoPPN), King's College London, London, United Kingdom
2Department of ENT, Queen Elizabeth Hospital, London, United Kingdom
Introduction: New daily persistent headache (NDPH) is characterised by an accurately described onset of a persistent headache. Secondary headaches should be ruled out including traumatic injury and CSF pressure disorders. The presence of migraine features in NDPH vary and different phenotypes or clusters have been proposed. On the other hand, persistent postural perceptual dizziness (PPPD) is another entity that typically presents with constant symptoms and where an initial vestibular insult is frequently identified. A high proportion of patients with PPPD have comorbid migraine. Likewise, vertigo has been described as a potent headache trigger. PPPD treatment entails vestibular rehabilitation, however, migraine patients often describe movement sensitivity.
Objectives: To describe the case of a twenty-eight-year-old female who was referred to the Headache clinic at Queen Elizabeth Hospital, London, UK.
Methods: She first experienced sporadic headaches around the age of 14. Her menarche was at age 13 and thought her headaches and menstruation could be linked. Her problem began 2 years before the consultation, on a particular day, when she was walking and started feeling like ‘being on a boat’. The only possible trigger that she could think of is that she was maybe more stressed because of being back in the office after the COVID-19 pandemic. Ever since then she described persistent dizziness, visual vertigo and a constant pressure-like headache. There were headache flare-ups 7 days a month. The pain then was described as squeezing, tight and localised on the left temple. There was bilateral photophobia, phonophobia, osmophobia, cranial allodynia and movement sensitivity. Cranial autonomic symptoms included bilateral facial pallor. She had bilateral tinnitus. Premonitory symptoms included mood changes, irritability, lethargy, yawning, neck stiffness, cognitive impairment and difficulty concentrating. Postdrome was characterized by feeling drained. Triggers for the flare-ups included stress, screens, overworking and alcohol. These would also worsen the dizziness. There was no postural component or worsening with Valsalva. The patient had tried prochlorperazine and betahistine as well as vestibular rehabilitation which did not help or were not tolerated. Simple analgesics were only partly efficacious. She was referred to the Joint Neurootology clinic (Neurology, ENT & Audiology). She underwent pure tone audiogram (PTA), tympanogram, video-head impulse test (v-HIT) and caloric testing.
Results: The PTA, tympanogram and v-HIT were unremarkable and the caloric test showed left side canal paresis (36% weaker). These findings were in line with a previous vestibular insult such as vestibular neuronitis. Given the presence of daily headache and migrainous features with prominent dizziness, flunarizine 5 mg ON was recommended for 4 months. At 2 months, following headache amelioration, vestibular rehabilitation was conducted and well-tolerated and 2 months later the patient became symptom free.
Conclusion: The diagnosis of NDPH, PPPD and vestibular migraine can sometimes be challenging given similar onset and common symptoms. Patients with prominent dizziness may benefit from a Joint Neurootology approach and vestibular tests may identify a potential cause for the onset. Vestibular migraine prevention prior to vestibular rehabilitation may prevent migraine movement sensitivity during therapy and improve outcomes.
P.32
Hypnic headache and dialysis: a dormant phenomenon?
G Pinho1 and R Oliveira2
1Hospital Da Luz, Lisboa, Lisbon, Portugal
2Barking, Havering and Redbridge University Hospitals NHS Trust, Romford, United Kingdom
Introduction: Hypnic headache is an exceptionally rare primary headache. Hypnic headache like presentation should prompt exclusion of secondary causes.
Objectives: To demonstrate potential triggering factors of a rare phenotype of primary headache.
Methods: Presentation and discussion of a real clinical case.
Results: A 70-year-old male with a history of end-stage chronic kidney disease, prostatic malignancy and remote smoking habits presented to the emergency department with a 10-day history of de novo headache. The headache was bifrontal and tension-type, occurred episodically and exclusively during sleep, both at night and nap time. It would wake him up from sleep, was of moderate severity, and would make the patient to get up and eat or walk around the house. It lasted between 30 and 120 minutes. There were not autonomic signs. Even though it appeared while he was asleep, he found lying awake safe and non-triggering. He had changed from alternate-day hemodialysis to a peritoneal dialytic technique ten days before developing the symptoms.
Physical and neurological exam were unremarkable, including peripheral pulses and craniofacial trigger point search. There were no mentation, visual acuity or optic disk changes, nor any other focal signs of nervous system involvement. The laboratory work-up showed increased inflammatory markers (CRP 5 mg/dL, ESR 76 mm), and the CT and MRI head with contrast discarded mass lesions, meningeal enhancement or signs of intracranial pressure changes, showing only mild microvascular white matter lesions. Doppler ultrasound of temporal arteries was normal. A trial of caffeine and paracetamol was attempted with a modest reduction in frequency and duration of the pain. He eventually developed fluid overload, with acute pulmonary oedema and aggravating inflammatory parameters, requiring diuretics and supportive care. All symptoms resolved after his renal replacement therapy was readjusted back to hemodialysis.
This case presents a nearly typical hypnic-type headache, with bouts of less than 4 hour-long nocturnal tension headache in an older male individual and partial response to caffeine. Where it fails diagnostic criteria is duration and correlation with hemodialysis, even though it might only constitute an eliciting factor and cerebral structural lesions were ruled out. Some studies suggest a potential role of hypothalamic degeneration in chronobiological rhythm and antinociceptive trigeminal tract pathway changes, leading to the occurrence of the “alarm-clock” events, and selective anterior hypothalamic atrophy and suprachiasmatic nuclei dysfunction as a pathophysiological mechanism, even though not nearly completely understood. Other papers also point to kidney dysfunction as a cause of decreased melatonin metabolism leading to more dull nocturnal surges and changes in circadian rhythm, REM/non-REM sleep cycles and pain modulation. In our patient, the confounding factor of fluid retention might have contributed to intracranial hypertension-dependent physiologic mechanisms, though both the history and imaging lacked some typical elements. A relation of cerebral oedema with anterior hypothalamic compression has been proposed.
Conclusion: This case highlights the potential roles of renal disease and fluid overload on hypnic-type headaches in patients in whom it is important to exclude secondary causes.
P.33
The influence of emotional behavior on pain self-efficacy during migraine attacks
F Pistoia1, F Guerra1, G Saporito1, J Ranieri1 and D Di Giacomo1
1University of L'Aquila, L'AQUILA, Italy
Introduction: Migraine is a disabling disease that affects both children and adults, influencing social relationships, work and productivity. Stress, emotional burden, anxiety feelings and catastrophizing thinking can trigger migraine attacks in vulnerable subjects.
Objectives: The aim of our study was to analyze the network of active negative emotions in patients with episodic migraine (EM) and to evaluate how psychological factors and behaviors interact with each other, potentially contributing to the worsening of migraine symptoms and disability.
Methods: Patients consecutively referring to the Headache Center of the S. Salvatore Hospital of L’Aquila, Italy in a 6-months period with a diagnosis of EM were screened for the inclusion in the study. Migraine diagnosis was performed by an experienced neurologist according to the International Classification of Headache Disorders (ICHD) criteria, 3rd edition. Inclusion criteria were: i) age >18 years, ii) diagnosis of EM with or without aura, and iii) availability to participate in the study and to sign the informed consent form. The exclusion criteria were a previous or current history of neurological or psychiatric disorders, dementia, intellectual disability, and an ongoing treatment with psychiatric drugs at the time of the study. Main clinical data for each patient. were collected including the number of monthly migraine headache days (MHDs) and the Migraine Disability Assessment Score Questionnaire (MIDAS) score. Patients also underwent a behavioral and emotional assessment through the following standardized psychological self-assessments tools: the Depression Anxiety Stress Scales 21 (DASS-21), the Pain Self-Efficacy Questionnaire (PSEQ), the Nepean Dysphoria Scale (NDS), the Difficulties in Emotion Regulation Scale- Short Form 18 (DERS), the Positive Mental Health Scale (PMH) questionnaire. A network analysis of negative emotions was performed to evaluate which emotional traits and relationships played a crucial role in pain coping and management.
Results: 60 outpatients aged 18-55 years (mean age 33.8; SD ±10.4) with a diagnosis of EM were included. Women (n = 50, mean age ± SD 33.8 ± 10.6) were more represented than men (n = 10 mean age ± SD 33.9 ± 9.6). Migraine without aura was the most common diagnosis (68.4%). The mean number of MHDs was 5.6 ± 1.8. On the MIDAS assessment, over half of the patients reported experiencing severe disability. The network analysis showed that negative emotions significantly influenced the ability of patients to cope with pain and maintain productivity during migraine attacks. Dysphoric variables (irritability, interpersonal resentment, and surrender) were correlated with difficulties in emotion regulation ability and with the capacity of engaging in goal-directed behaviors despite experiencing pain. The ability to regulate one's emotions and manage dysphoria were positively correlated with pain self-efficacy, whereas positive mental health was associated with individuals’ confidence in performing activities despite experiencing pain.
Conclusion: Negative emotions had a negative correlation with positive mental health and were linked to a lower capacity to carry out daily activities despite experiencing pain. This suggests that psychological interventions could improve mental health and potentially surpassing the effects of pharmacological interventions alone in migraine management. An integrated, patient-centered approach may represent an effective paradigm to reduce the burden of migraine, leading to a reduction in healthcare costs.
Figure

P.34
Ultrasound-Guided Dry Needling: Effects on Spinal Fluid Dynamics and Gut-Brain Axis Modulation in Migraine Patients with Central Sensitization
R Bubnov1 and M Spivak2
1Clinical Hospital ‘Pheophania’, Kyiv, Ukraine
2Zabolotny Institute of Microbiology and Virology, National Academy of Sciences of Ukraine, Kyiv, Ukraine
Introduction: The Gut-Brain Axis (GBA) plays a pivotal role in various conditions such as migraine, headache disorders. The multifactorial etiology involves myofascial pain, abnormal posture, and vascular dysregulation. While ophthalmic artery Doppler shows potential in conditions like migraine and stroke prevention, effective treatments targeting these mechanisms are still in exploration [1]. Neuromodulation techniques and US-guided trigger point interventions have shown efficacy, but their effects on ophthalmic artery Doppler and associated symptoms remain largely unexplored. Moreover, personalized probiotic administration, as a potential modulator of the GBA, may offer promising therapeutic avenues.
Aim and Objective: This study aims to investigate the effects of ultrasound-guided dry needling on spinal fluid dynamics and the modulation of the Gut-Brain Axis in patients with migraine, vertigo, and central sensitization symptoms, supplemented by personalized probiotic therapy.
Methods: Patients presenting with headache, vertigo, and central sensitization-related symptoms underwent US-guided dry needling targeting trigger points in suboccipital muscles. Precise needle placement was confirmed using ultrasound imaging, with a focus on muscles attached to the dura mater. Real-time monitoring, including M-mode visualization, captured pulsatile movements of dorsal and ventral roots at the C1-C2 level. Ophthalmic artery Doppler analysis was conducted pre- and post-intervention to assess changes in blood flow parameters. Additionally, personalized probiotic strains, including Lactobacillus and Bifidobacterium genera, were selectively administered at a dose of 10^9 CFU per day for ten days, based on individual symptoms. Mesenteric Doppler, kidney Doppler, blood flow resistive index in segmental arteries, and parameters related to visceral fat were also assessed.
Results: Ultrasound evaluation revealed significant alterations in pulsatile movements of dorsal and ventral roots within the spinal canal following dry needling, with a decrease in frequency from 250 to 80 per minute and an increase in amplitude from 0.07 mm to 0.18 mm. Doppler analysis demonstrated improved blood flow in retinal, ciliary, and ophthalmic arteries post-intervention. Furthermore, stabilization of parameters related to spinal fluid dynamics and normalization of mesenteric Doppler readings were observed following personalized probiotic administration.
Discussion: The observed changes in spinal fluid dynamics, indicated by alterations in pulsatile movements, suggest a potential link between ultrasound-guided dry needling and cerebrospinal fluid dynamics. The intervention likely influences myofascial structures attached to the dura mater, impacting the surrounding cerebrospinal fluid environment. Moreover, the supplemental personalized probiotic therapy appears to contribute to the modulation of the GBA, as evidenced by the normalization of mesenteric Doppler readings and improvements in eye symptoms.
Conclusion: Ultrasound-guided dry needling, supplemented by personalized probiotic therapy, emerges as a promising intervention for patients experiencing headaches, vertigo, and central sensitization. The ultrasound evaluation of spinal fluid dynamics emerges as a promising and potentially reliable marker for GBA modulation, particularly when tested in specific treatment modalities targeting both muscular and gut-related pathways.
References
1. Bubnov R and Spivak M. Ophthalmic artery Doppler as a test for gut-brain axis modulation: feasibility study. Endocrine Abstracts 2024; 99: EP599. DOI: 10.1530/endoabs.99.EP599
Image 1

P.35
Relationship of Glycemia and Headache Severity: Applying Statistical Methods in a case with Post-prandial Improvement
M Villar Martinez1 and P Goadsby2
1NIHR King's Clinical Research Facility, SLaM Biomedical Research Centre and Wolfson Sensory Pain and Regeneration, Institute of Psychiatry, Psychology and Neuroscience, London, UK
2Department of Neurology, University of California, Los Angeles, USA
Objective: To investigate a 53-year-old woman with a medical history of migraine, focusing on the potential association between her headache symptoms and metabolic factors, particularly glycaemia.
Methods: The patient underwent thorough investigations following the appearance of new headache attacks with a trigeminal-autonomic cephalalgia phenotype and post-prandial resolution. A a phyllodes tumour was identified, which has a potential secretion of insulin-like growth factor [1–4]. After tumour resection, the patient continued to experience headache with improvement post-meals. A linear regression analysis was conducted to explore the relationship between glycaemia and headache severity.
Results: The analysis revealed a significant relationship between glycaemia and headache severity, with a coefficient estimate of −1.0734 for glycaemia (p < 0.05). Notably, glycaemia exhibited a negative association with headache severity. The model, however, explained only a modest proportion of the variance (R2 = 0.06205), suggesting the presence of additional factors contributing to headache manifestation.
Conclusions: These findings suggest a potential link between glycaemia and headache symptoms in the context of the patient's medical history. While the exact mechanisms remain unclear, the observed association underscores the importance of considering metabolic factors in headache management. Statistical approaches could help in the differential diagnosis in the headache clinic
P.36
Sexual Dimorphism of CGRP Family of Receptors and Ligands in Rat Trigeminal Ganglion
A Maddahi1, J Edvinsson1 and L Edvinsson1
1Department of Clinical Sciences-Lund University, Lund, Sweden
Introduction: Calcitonin gene-related peptide (CGRP) has been shown to play a pivotal role in migraine pathophysiology. Recent studies have implicated other peptides within the calcitonin family in migraine pathogenesis. Previous research demonstrated abundant expression of CGRP and its receptors in the trigeminovascular system (TVS), particularly in the trigeminal ganglion (TG). Thus, the objective of the present study is to elucidate the distribution of other CGRP family peptides (adrenomedullin, amylin, and calcitonin) and their receptors (CTR, CLR, RAMP2, and RAMP3) in the TVS, while also investigating potential gender differences in their expression.
Methods: We meticulously dissected TGs and brains from both male and female adult rats. Protein and gene expression levels of CGRP, calcitonin, amylin, adrenomedullin, and their receptors were assessed through immunohistochemistry and real-time quantitative PCR. Additionally, the dura mater from male rats was isolated for further investigation of protein expression and fiber localization using immunohistochemistry.
Results: Immunoreactivity for adrenomedullin, amylin, CTR, RAMP1 and CLR were observed in the cytoplasm of TG neurons and satellite glial cells. Adrenomedullin and CTR protein expression were detected in Schwann cells surrounding fibers, and immunoreactive Aδ-fibers storing both adrenomedullin and CLR were identified. RAMP2 and RAMP3 immunoreactivities were observed in the nucleus of TG neurons and in satellite glial cells. Furthermore, RAMP1 and CLR (canonical CGRP receptor elements) were co-localized with CASPR in the nodes of Ranvier located in peripheral fibers. There were no significant differences in the number of adrenomedullin, amylin, CTR, CLR, RAMP2, and RAMP3 immunoreactive cells between males and females. Gene expression analysis revealed the presence of all genes in both male and female TG, except for CTR. Notably, CGRP mRNA levels in TG were significantly higher than those of other genes, and RAMP1 mRNA levels were significantly higher in female TG compared to male TG.
Conclusions: This study provides comprehensive insights into the distribution of CGRP family peptides and their receptors in the TVS, highlighting potential implications for migraine pathophysiology. Furthermore, our findings suggest interesting gender-specific differences in gene expression within the TG, warranting further investigation into their functional significance.
P.37
Real-World Evidence of Adding Atogepant to OnabotulinumtoxinA for Control of Chronic Migraine: A Retrospective Chart Review
A Blumenfeld1, L Mechtler2, L Cook3, C Rhyne4, B Jenkins5, O Hughes6, B Dabruzzo7, A Manack Adams7 and M Diamond8
1The Los Angeles and San Diego Headache Centers, San Diego, USA
2Dent Neurologic Institute, Buffalo, USA
3The Los Angeles Headache Center, Los Angeles, USA
4Norton Neuroscience Institute, Louisville, USA
5Neuroscience Group, Neenah, USA
6ICON plc, Blue Bell, USA
7AbbVie, North Chicago, USA
8Diamond Headache Clinic, Chicago, USA
Introduction: Combination use of atogepant and onabotulinumtoxinA has the potential to be more effective than either alone for the preventive treatment of CM.
Objective: To collect real-world data to evaluate the effectiveness, safety, and tolerability of adding atogepant to onabotulinumtoxinA as combination preventive treatment for chronic migraine (CM).
Methods: This retrospective, longitudinal, multi-center chart review included adults with CM receiving ≥2 consecutive onabotulinumtoxinA cycles before ≥3mo of onabotulinumtoxinA and atogepant combination treatment. Charts at first atogepant prescription (index date) and 2 onabotulinumtoxinA injection visits (∼3 and 6mo post-index) were reviewed for change from baseline in monthly headache days (MHDs), ≥ 50% reduction in MHDs, and rates and types of adverse events (AEs). Charts with CGRP agents for migraine prevention during baseline (∼3mo pre-index) were excluded.
Results: 31 charts met eligibility criteria (mean age 46.7 years, 94% female). Atogepant 60 mg and 30 mg were administered QD to 30 and 1 patients, respectively. Throughout the study, patients received a mean dose of 170U onabotulinumtoxinA. Pre-onabotulinumtoxinA, the mean MHD was 24.0d, reduced by a mean -8.15d (95%CI −11.44,−4.85; n = 25) after onabotulinumtoxinA pre-index (mean 3.97 yr). MHD additionally decreased by mean -4.53d [95%CI −7.44,−1.61] after ∼3mo of combination treatment (n = 31) and −8.75d total [95%CI −13.21, −4.29] after ∼6mo of combination treatment in patients with data available (n = 23). Nearly half of patients (n = 14/31) achieved ≥50% reduction in MHDs ∼3mo post-index. Overall, 95% CIs indicate that reductions from baseline were statistically significant. No new safety signals were identified when atogepant was added to onabotulinumtoxinA. The most commonly reported AEs (≥5%) were constipation and fatigue.
Conclusions: This real-world pilot study of patients with CM demonstrated clinically meaningful treatment benefit in the reduction of headache days with onabotulinumtoxinA alone and additive benefits with co-administration of atogepant. Safety results were consistent with the known safety profiles of onabotulinumtoxinA and atogepant.
P.38
Exploratory Efficacy Results from the TANDEM Trial: Safety, Tolerability, and Efficacy of Ubrogepant for the Acute Treatment of Migraine in Participants Taking Atogepant for the Preventive Treatment of Episodic Migraine
A Blumenfeld1, M He2, J Smith3, C Schlacher3, J Contreras-De Lama4 and L Davis5
1The Los Angeles Headache Center, Los Angeles, USA
2AbbVie, Madison, USA
3AbbVie, North Chicago, USA
4AbbVie, Irvine, USA
5Kolvita Family Medical Group, Mission Viejo, USA
Introduction: Ubrogepant is approved in the US for acute treatment of migraine in adults, with/without aura. Atogepant is approved in the US and EU for preventive migraine treatment in adults.
Objective: This exploratory analysis of the TANDEM trial evaluated efficacy of ubrogepant 100 mg PRN for the acute treatment of migraine in participants taking atogepant 60 mg QD for the preventive treatment of EM.
Methods: TANDEM, a phase 4, two-period, multicenter, open-label safety US study, enrolled adults with migraine, with or without aura, and <15 headache days per month across the 3 months. In Period 1(Weeks 1–12), participants were treated with atogepant 60 mg QD and their own acute migraine medication, excluding any gepant, for breakthrough migraine attacks. In Period 2(Weeks 13–24), participants continued atogepant 60 mg QD and were required to take ubrogepant 100 mg as needed (PRN) for breakthrough migraine attacks. In Period 2, a second ubrogepant dose, or the participants’ own acute medication, was allowed 2–24hrs after the initial ubrogepant dose. Safety was evaluated and treatment-emergent adverse events (TEAEs) were defined as AEs with an onset date ≥ date of the first dose of study treatment but <30 days after the last dose or Visit 8/Week 24. All efficacy endpoints in this study were exploratory and this analysis evaluated the efficacy of ubrogepant 100 mg PRN in Period 2. A structured Investigator Interviewer Questionnaire(IIQ) was used to assess ubrogepant dosing, pain freedom, and pain relief. Treatment optimization was assessed during Period 2 using the Migraine Treatment Optimization Questionniare-6(MTOQ-6). The IIQ and MTOQ-6 were completed at study (Week 16), (Week 20), and (Week 24) during Period 2. The MTOQ-6 consists of 6-items scored as never (1), rarely (2), less than half the time (3), or half the time or more (4). The total score is calculated by summing individual question scores, with higher scores indicating better acute treatment optimization (scores range 6–24). Sensitivity analyses were performed for the efficacy analyses to exclude any illogical responses to the IIQ
Results: For the efficacy analyses, Period 2 included 211 participants who were treated, had a baseline efficacy assessment, and had ≥1 postbaseline efficacy assessment (modified intent-to-treat [mITT] population 2). During Period 2, mean monthly ubrogepant use days over Weeks 13–24 was 2.13 days (SD, 1.86). Monthly and 12-week mean response rates for pain freedom and relief at 2hrs and sustained pain freedom and relief from 2–24hrs consistently exceeded 50% for breakthrough migraine attacks treated with ubrogepant during Period 2 (Table 1). Mean MTOQ-6 scores(SD) were 21.7(3.4), 22.2(2.9), and 22.4(2.8) during Weeks 16, 20, and 24, respectively. Sensitivity analyses performed after excluding illogical responses from the IIQ were consistent with prespecified analyses. The overall safety results were consistent with the known safety profile of atogepant and ubrogepant.
Conclusion: Ubrogepant-treated participants recalled high rates of pain freedom and relief, and high treatment optimization when used concomitantly with atogepant 60 mg QD. No new safety signals were identified.

LB.01
Efficacy Outcomes from a Phase 3, Randomised, Double-Blind, Placebo-Controlled Study of Fremanezumab for the Preventive Treatment of Episodic Migraine in Children and Adolescents
A Hershey1, C Szperka2, S Barash3, S Garnett3, J Bryson3, Y Kesler4, T Erez4, Y Carmeli Schwartz4, M Grozinski-Wolff3 and X Ning3
1Cincinnati Children’s Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, USA
2Children’s Hospital of Philadelphia and Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA
3Teva Branded Pharmaceutical Products R&D, Inc., West Chester, USA
4Teva Pharmaceutical Industries Ltd., Tel Aviv, Israel
Introduction: The anti-epileptic, topiramate, is currently the only treatment approved for migraine prevention in patients aged 12–17 years. Newer migraine-specific preventive treatments that target the calcitonin gene-related peptide (CGRP) pathway, such as fremanezumab, are approved for adults with chronic and episodic migraine (EM). However, there are limited data on the efficacy of CGRP pathway mAbs in children and adolescents.
Objectives: The SPACE study (NCT04458857) aims to evaluate the efficacy, safety and tolerability of fremanezumab for the preventive treatment of EM in children and adolescents. Here, we present efficacy outcomes from the SPACE study.
Methods: This multicentre, parallel-group, Phase 3 study consisted of a 4-week screening period and a 12-week double-blind period. Eligible participants were 6–17 years old, with a diagnosis of migraine (consistent with ICHD-3 criteria) for ≥6 months prior to screening and a history of ≤14 headache days per month in each of the 3 months prior to screening. Participants were randomised 1:1 to receive monthly fremanezumab subcutaneously (120 mg for <45 kg, 225 mg for ≥45 kg) or matched monthly placebo. The primary endpoint was the least-squares (LS) mean change from baseline in monthly average number of migraine days (MMD) during the 12 week double-blind period. Ranked secondary endpoints were the LS mean change from baseline in monthly headache days of at least moderate severity (MHD), the proportion of participants achieving ≥50% reduction in MMD, the LS mean change from baseline in days with acute medication use, and LS mean changes from baseline in Pediatric Migraine Disability (PedMIDAS) and Pediatric Quality of Life (PedsQL) scores at Week 12. A hierarchical testing procedure was implemented according to the predetermined sequence.
Results: In total, 237 participants were randomised and 234 (fremanezumab, n = 123 [120 mg, n = 36; 225 mg, n = 87]; placebo, n = 111) were included in the efficacy analysis. The LS mean change from baseline in MMD over 12 weeks was –2.5 for fremanezumab versus –1.4 for placebo (p = 0.0210), with a greater reduction in MMD observed with fremanezumab versus placebo as early as Week 4 (Figure 1). Over 12 weeks, the reduction in MHD of at least moderate severity was significantly greater with fremanezumab versus placebo (–2.6 vs –1.5; p = 0.0172), as was the proportion of participants achieving ≥50% reduction in MMD (47.2% vs 27.0%; p = 0.0016). The LS mean change from baseline in monthly average number of days with acute medication use was –2.1 for fremanezumab and –1.0 for placebo (p = 0.0016). A directional, but not statistically significant, improvement was observed in PedMIDAS score for fremanezumab versus placebo (–21.6 vs –15.3) at Week 12. No improvement was observed in PedsQL score for fremanezumab versus placebo (+5.7 vs +6.2) at Week 12.
Conclusions: In this 12-week study, fremanezumab demonstrated significantly superior efficacy over placebo in children and adolescents with EM, with results comparable to pivotal studies of fremanezumab in adults with EM. These findings add to the limited data on the efficacy of CGRP pathway mAbs in children and adolescents, and suggest fremanezumab may provide an effective preventive migraine treatment in this patient population.

LB.02
Real-world evidence of clinical and demographic characteristics in cluster headache
H Gosalia1, D Wei1,2 and P Goadsby1,2
1NIHR King’s Clinical Research Facility, & SLaM Biomedical Research Centre, The Wolfson Sensory, Pain and Regeneration Centre (SPaRC), Institute of Psychiatry, Psychology and Neuroscience (IoPPN), King’s College London, London, UK
2Department of Neurology, King’s College Hospital, London, United Kingdom
Introduction: Real-world data from patients facilitates a broader appreciation of the clinical features and demographic distribution of cluster headache. Synthesised into real world evidence. We may gain insights into differences between UK nations regarding cluster headache.
Objectives: To gather epidemiological, clinical and demographic data from a cluster headache questionnaire-based study involving a National Health Service (NHS)-based sample, from Scotland and South-Central England, in the UK.
Methods: A standardised questionnaire was administered to NHS home-oxygen patients across 14 Health Boards in Scotland, UK, covering 5,463,300 patients, with a sample size of 107 patients, at the time of analysis and 7 Clinical Commissioning Groups were involved in England, covering 4,581,933 with a sample size of 83. Cluster headache diagnosis was verified using the International Classification of Headache Disorders (ICHD-3).
Results: For the analysis, 83 patients were considered for the England region and 107 for the Scottish region. The median time to diagnosis was 2 (IQR: 10-1) months for Scotland and for England, 3 (IQR: 8-1) months. Neurologists most commonly made the diagnosis in both nations. In Scotland, 23% reported as current smokers compared to 37% in England. All patients in both nations reported the presence of at least one cranial autonomic symptom. The most prominent in both nations was lacrimation, 90% for England and 86% for Scotland. The median number of cranial autonomic symptoms reported was 6 (IQR: 6-3) for Scotland and 5 (IQR: 6-4) for England. For both cohorts, 92% reported migrainous symptoms. The most prominent was photophobia for both nations (61%). The most effective preventive treatment in both regions was verapamil and the most effective acute treatment was oxygen. In both regions, the top three preventives were verapamil, followed by lithium and then greater occipital nerve injection. Of episodic cluster headache (ECH) patients, 53% reported rebound headache with mean time 33 (SEM: 11) minutes after oxygen use in Scotland. Of chronic cluster headache (CCH) patients, 54% reported rebound headache with mean time 17 (SEM: 4) minutes in Scotland. For England, ECH rebound headache was reported by 64% with mean time 48 (SEM: 11) minutes and CCH rebound headache was 64% with mean time 29 (SEM: 8) minutes.
Conclusion: The real-world evidence highlights the current state of the clinical and demographic data in regions in the UK, with certain data analogous across the regions. Furthermore, real-world cluster headache data allows for a dataset to be built with direct knowledge from the patients, further developing novel research concepts.
LB.03
Triptan non-response in a London tertiary headache centre: what can we learn?
R-J Wilcha1 and P Goadsby1,2
1King's College London, United Kingdom
2University of California, CA, USA
Background: Triptans revolutionized the acute treatment of migraine, however, varied responses to triptans, owing to poor efficacy and tolerability, are reported. The definition of triptan non-response was recently standardized by the European Headache Federation (EHF). There is currently limited data available on the prevalence of triptan non-response.
Methods: We used clinic letters over a two-year duration to evaluate triptan response and triptan efficacy or tolerability failure, or both, in a London-based tertiary headache service.
Results: A total of 419 adult migraine patients (females: 83.8%, age: 46 ± 18 years, chronic migraine: 88.5%) were included in a service evaluation. In line with the EHF definitions, ‘triptan non-response’ was seen in 63.5% of patients (263/414), whilst 37.4% of patients (155/414) had failed at least two triptans (EHF ‘triptan resistant’) and 4.6% of patients (19/414) had failed at least three triptans, including a subcutaneous formulation (EHF ‘triptan refractory’). Advancing age (P < 0.001) and the presence of medication overuse (P = 0.006) increased the probability of triptan response, whilst an increased number of failed preventives (P < 0.001) and the use of CGRP monoclonal antibodies (P = 0.022) increased the probability of triptan non-response. The largest proportion of patients responded to eletriptan (49.5%), followed by nasal zolmitriptan (44.4%) and rizatriptan (35.7%).
Conclusion: Our findings highlight an alarming prevalence of triptan non-response among adult migraineurs receiving treatment in a London-based tertiary headache service. It is imperative for clinicians to explore methods to optimize acute medication efficacy, whether changing to a triptan with a superior response rate, advocating for early intervention or considering alternative acute medication classes, such as gepants or ditans.
LB.04
The Safety and Effectiveness of Dual Calcitonin Gene-Related Peptide (CGRP) Therapies for Migraine Treatment: A Focus on Small Molecule Antagonist and Ligand Monoclonal Combinations
H Lee1,2, A Cheung1,2, J Jahansooz1,2, E Weldon1,2, A Lee1,2, K Ishikawa1,2, N Little1, E Carrazana1,2 and K Liow1,2
1Headache & Facial Pain Center, Hawaii Pacific Neuroscience, Honolulu, United States
2John A. Burns School Of Medicine, University Of Hawaii, Honolulu, United States
Introduction: Single CGRP regimens may not improve migraine outcomes and could worsen symptoms in some patients. Combining small molecule antagonists (SMA) and ligand monoclonal antibodies (L-mAb) targets CGRP molecules and receptors, potentially providing increased synergistic relief. Our study aims to assess the effects of this dual-CGRP approach.
Objectives: To assess the effects of dual-CGRP therapy on patients with synergistic use of SMAs and L-mAbs.
Methods: A retrospective matched cohort study was conducted at a neurological care center in Hawaii, analyzing 90 chronic migraine patients aged ≥18 years treated with CGRP inhibitors (L-mAbs: fremanezumab, galcanezumab, eptinezumab; SMAs: ubrogepant, rimegepant, atogepant; or a combination). The study compared dual L-mAb and SMA CGRP treatments with mono-L-mAb or mono-SMA CGRP treatments, matched by age and sex. Variables included age, age at diagnosis, sex, onabotulinumtoxinA use, headache frequency, duration, severity, and associated symptoms before and three months post-treatment. Adverse events were recorded for the dual-treatment group at three-month follow-up. Statistical analyses were made using Wilcoxon, Kruskal-Wallis, and Fisher's exact tests, with significance set at < 0.05.
Results: Patients on dual-CGRP therapy had an average reduction of four headache days, with some experiencing up to 14 fewer days, while mono-CGRP patients experienced no change (p = 0.112). Headache severity was reduced by 20% for dual-CGRP patients and 10% for mono-CGRP patients (p = 0.039). Aura symptoms were significantly reduced in the dual-CGRP group, with 48% (13 patients) becoming aura-free compared to 20% in the mono-CGRP group (p = 0.004). Adverse events in the dual-CGRP group were mild, with three patients experiencing fatigue, drowsiness, or mild constipation. No patients discontinued treatment, and no serious adverse events were reported.
Conclusion: Dual-CGRP regimens may provide improved effectiveness for controlling migraine symptoms by significantly reducing headache severity and aura symptoms without significant adverse events.
LB.05
αCGRP and βCGRP are co-expressed in the trigeminal ganglia
T Rees1, M Garelja2, C Walker3 and D Hay2
1King's College London, United Kingdom
2The University of Otago, New Zealand
3The University of Auckland, New Zealand
Objective: Calcitonin gene-related peptide (CGRP) is a neuropeptide involved in pain transmission and migraine pathogenesis. CGRP has two major isoforms, αCGRP and βCGRP, which differ by three amino acids in humans and mice. αCGRP is highly expressed in the trigeminal ganglia (TG) and has a well-established role in pain sensitisation and migraine. In contrast, βCGRP expression is poorly defined and is often reported to be primarily expressed in the enteric nervous system, with limited relevance to migraine. Therefore, this study aimed to compare the relative distribution of αCGRP and βCGRP in the mouse TG.
Methods: Detection of the mouse CGRP isoforms by anti-CGRP antibodies was tested by dot blot. Wildtype (WT) and αCGRP knockout (KO) adult mouse TG (C57BL/6J background, WT 3M/1F, KO 4F) were immunostained for CGRP relative to neuronal markers (β tubulin III and NF200) and the calcitonin receptor (CTR). RNA-fluorescent in situ hybridisation (RNA-FISH) probes against αCGRP (Calca) and βCGRP (Calcb) mRNA were validated in transfected HEK293S cells. These probes were then used to examine isoform expression in WT adult mouse TG (C57BL/6J, 2F/3 M).
Results: All anti-CGRP antibodies tested detected both isoforms of CGRP. CGRP-like immunoreactivity was present in WT and αCGRP KO mouse TG in neuronal cell bodies, often colocalising with CTR. However, compared to the WT mice, CGRP immunoreactivity in the αCGRP KO TG was of a lower fluorescence intensity and lacked pearl-like fibre immunoreactivity. The RNA-FISH probes were specific to each isoform and indicated that αCGRP and βCGRP mRNA were often present in the same neuronal cell bodies, although some neuronal cell bodies only expressed one CGRP isoform.
Conclusions: βCGRP is expressed in mouse TG neurons, suggesting it plays a role in neuromodulation and nociception, alongside αCGRP. Both isoforms may be important for mediating CGRP's pathogenic activity in migraine.
LB.06
Stroke etiology and white matter hyperintensities in women with and without migraine
A Wilms1, N van der Weerd1, T van Harten1,2, K Linstra1,3, H van Os1, I de Boer1, M Kruit1, A MaassenVanDenBrink3, M Wermer1,4 and G Terwindt1
1Leiden University Medical Center, Leiden, Netherlands
2Massachusetts General Hospital, Boston, USA
3Erasmus University Medical Center, Rotterdam, Netherlands
4University Medical Center Groningen, Groningen,
Netherlands
Introduction: Women with migraine, especially those with migraine with aura, have a higher risk of white matter hyperintensities (WMH) and ischemic stroke. The coexistence of migraine, WMH and stroke, prompts inquiries into whether the stroke events in patients with migraine have a similar etiology as stroke events in patients without migraine. Moreover, it is unclear whether there is an additive effect on WMH volume in patients with a history of both migraine and ischemic stroke.
Objectives: We aimed to determine whether stroke etiology differs between women with and without migraine and whether migraine has additional impact on WMH volume in women with stroke.
Methods: Middle-aged women diagnosed with ischemic stroke, both with and without a history of migraine, as well as those with migraine with aura alone, were included in this cross-sectional study. Stroke etiology was categorized according to the TOAST criteria. Evaluation of WMH volume on 3D fluid-attenuated inversion recovery (FLAIR) images was conducted using our in-house developed semi-automated segmentation software in MeVisLab (version 3.4.1). Presence or absence of cerebellar WMH was scored. We used regression analysis to assess differences between groups, with adjustments for age, smoking status, and BMI.
Results: We included a total of 148 women, including those with migraine with aura without stroke (n = 38), stroke without migraine (n = 55), and stroke with migraine (n = 55). Patients with stroke more often had a history of smoking compared to patients with both stroke and migraine, and migraine only (74% vs. 46% and 41% respectively, p = 0.004). Women with both stroke and migraine more often had a stroke of undetermined origin than women with stroke alone (49% vs. 27%, p = 0.019). Total and periventricular WMH volumes were higher in women with stroke with migraine than in those with migraine only (0.63 mL vs. 0.46 mL, B -0.27 [−0.51 – −0.03], p = 0.030 and 0.55 mL vs. 0.42 mL, B −0.26 [−0.45 – −0.06], p = 0.012, respectively). No differences in deep WMH volume and presence of cerebellar WMH were found between the three groups. Crucially, there was no additional effect in WMH volume for women with a history of migraine and stroke compared to those with stroke alone.
Conclusion: Women with both stroke and migraine demonstrated a distinct stroke etiology from women with stroke without a migraine history, where smoking emerged as a more prevalent risk factor. There is no observed increase in WMH volume due to migraine in women with stroke. It is recommended that physicians inquire about migraine history, especially in non-smoking women with ischemic stroke.
Figure


LB.07
The effect of selective adenosine A3 receptor (A3AR) agonists in preclinical models of migraine-like periorbital hypersensitivity
R Torres-Granados1, P Sureda I Gibert1, S Michalski2, M Romero-Reyes1, D Salvemini2 and S Akerman1
1University of Maryland Baltimore, Baltimore, United States
2Saint Louis University, St. Louis, United States
Background: Despite the emergence of exciting new and effective migraine therapies there remains a need to identify novel targets for treatment that are safe, efficacious, and capture patient populations that gain little benefit from current treatments. This likely requires dissecting previously unidentified molecular mechanisms that may underpin migraine pathobiology. Recent preclinical studies in various chronic pain states have identified the adenosine A3 receptor (A3AR); Gαi-linked receptors expressed within neurons and glia related to spinal nociception. Their role in trigeminal nociceptive processing relevant to migraine and other headache disorders is not known.
Objective: To determine the efficacy of highly selective A3AR agonists in preclinical models of migraine-like periorbital hypersensitivity and to establish A3AR as a novel therapeutic target for migraine and related headache disorders.
Methods: We used male and female C57Bl/6 mice and two established approaches of persistent migraine-like periorbital hypersensitivity; chronic nitroglycerin (NTG, 10 mg/kg, IP, every other day for 9 days) and sumatriptan (medication) overuse (0.6 mg/kg, IP, every day for 11 days). We measured periorbital withdrawal thresholds in conscious mice by probing with calibrated von Frey filaments every 3-4 days until day 12, calculated using the UP-DOWN Reader (UDReader). Mice were treated with one of two highly selectively A3AR agonists, MRS5980 and CI-IB-MECA, using both a preventive protocol (dosing D1-D11) and a reversal protocol (dosing D7-D11) after hypersensitivity is established.
Results: In both male and female mice, MRS5980 (0.1, 0.3, and 1.0 mg/kg, IP, n = 8) dose-dependently prevented the development of NTG-mediated periorbital hypersensitivity, with the highest dose completely preventing its development (male, P = 0.946; female, P = 0.201). CI-IB-MECA (1 mg/kg, IP, n = 9–10) also prevented the development of migraine-like periorbital hypersensitivity and reversed established NTG-mediated hypersensitivity. In the medication overuse hypersensitivity assay, used as a surrogate of migraine, MRS5980 (1 mg/kg, n = 8) also prevented and reversed sumatriptan overuse-mediated periorbital hypersensitivity.
Conclusions: Together, these data provide preclinical support for A3AR agonism as a novel and promising approach for the treatment and prevention of migraine and related headache disorders, including medication overuse headache. This is based on using two independent preclinical approaches with two different classes of A3AR agonists. Further validation is necessary to dissect the therapeutic mechanism of action involved and the potential role of adenosine-A3AR signaling in migraine pathogenesis.
LB.P37
Impact of Migraine History and Discharge Diagnosis on Patient Journey and Treatment Approach in the Emergency Department
C Baugh1, C Leroue2, A Patel2, N Spence2, S Sweeney2, J Lilley3, J Bevilacqua3, X Zhang3, F Moehring-Moskal3 and J Brown2
1Department of Emergency Medicine, Brigham and Women’s Hospital, Boston, United States
2Pfizer Inc., New York City, United States
3Boston Strategic Partners, Inc., Boston, United States
Introduction: Migraine is a neurological disorder characterized by severe headache, often with nausea and vomiting, making it a common emergency department (ED) complaint. However, some individuals may be diagnosed with nonspecific headache, rather than migraine, due to subjectivity and variability among clinicians. A better understanding of care patterns and patient experiences, including those of people who receive a nonspecific diagnosis, may increase treatment success for migraine in the ED. Such real-world evidence on patient journey and medication utilization is lacking.
Objectives: The purpose of this study was to describe the ED journeys of people with migraine or headache not otherwise specified (NOS), both with and without established prior history of a migraine diagnosis.
Methods: This retrospective cohort study utilized Truveta electronic health records from member systems in the United States. We included people with a migraine or headache NOS primary ED discharge diagnosis, based on ICD-10-CM codes from index encounters between 06/01/2017 and 06/01/2022. All included individuals had data available for ≥12 months preceding and ≥6 months after the index encounter. The population was divided into 4 cohorts: those with a migraine diagnosis at index visit and history of migraine, defined by ICD-10-CM codes and prescriptions (“migraine with history”), migraine without prior established migraine history, headache NOS with migraine history (“headache with history”), and headache NOS without prior established migraine history. Baseline characteristics and healthcare resource use were assessed. Outcomes included ED length of stay, ED treatments, time to first treatment, and time from first treatment to disposition.
Results: Overall, 214,255 people were included. Most were female (76.6%) and White (56.9%); the mean age was 41.5 years. Over the 12-month lookback, people with a migraine history had a higher mean number of all-cause ED visits than those without (p < 0.001), regardless of index diagnosis (Table 1). Mean ED length of stay ranged from 5.3–5.8 hours across all cohorts. The mean time to first treatment (of selected acute treatments of interest) ranged from 3.1-3.8 hours. A majority received treatment, though those diagnosed with migraine were more likely to receive the selected acute treatments than those diagnosed with headache (migraine: 84.6% with, 80.5% without history; headache: 75.2% with, 64.4% without history; migraine vs. headache p < 0.001). More people with a migraine diagnosis (vs. headache) received non-steroidal anti-inflammatory drugs and antiemetics (both p < 0.001); more people with headache received acetaminophen, alone or in combination with other drugs (p < 0.001; Table 1). Migraine-specific medications were used in a small proportion of the population, and those with the highest usage rate were triptans (1.9% of the overall population).
Conclusions: These findings characterize ED journeys when people seek treatment for migraine or headache. People with pain characterized as headache, rather than migraine, may be less likely to receive treatment in the ED, regardless of prior history. Across all cohorts, ED length of stay was substantial, averaging ≥5 hours, and people often waited for pain relief, with a mean of >3 hours before receiving treatment.

LB.P38
A Study of Patient Satisfaction with a HEadache Interactive DIary Application (HEIDI) within a Secondary Headache Service
G Kennedy
1
1South Tyneside and Sunderland NHS Trust, Sunderland, United Kingdom
Introduction: Effective headache management relies on an accurate diagnosis and assessment of treatment responses based on headache diary information. A bespoke HEadache Interactive Diary (HEIDI) was developed with the unique function of providing real-time tabulated meaningful individual-based headache data in a simple user-defined format to support the clinical management of headache. Thus provides an overview of the number of headache and migraine days per month, medication days, GP and hospital visits and non-functional days in addition to any other quality of life function (HIT-6 score in this study). This is convenient for home-based treatments, collecting comparable and consistent data for audit purposes, as well as supporting allied health care practitioners to monitor headache conditions more accurately.
Objective: This study analysed the data from surveys collected from users of the HEadache Interactive DIary (HEIDI) App within Sunderland Royal Hospital Headache Service to evaluate rates of satisfaction compared to their usual headache diary method and discusses the potential role of electronic headache diaries in supporting Headache Services
Methods: A total of 70 participants were enrolled in the study, 54 (77.1%%) female, 4 Male (5.7%) and 12 (17.2%) who stated no gender. Mean age (n = 50) was 41.2 (SD 11.3) years with a range from 21 to 62 years. Baseline questionnaires were collected prior to the use of the HEIDI app in 63 users (90% response rate), and a repeat user survey was completed by 40 users (63% response rate) after a 6-month period of using the HEIDI app. Consistent diary entries over the six months were collected in 78% of responders and 76% of users were still using it 15 months later.
Results: There is a significant increase in overall user satisfaction associated with the HEIDI app by a factor of 1.63 from baseline (mean satisfaction 3.92 (SD = 1.18)) to end of the 6 month trial (mean satisfaction 6.40 (SD = 0.59)) with a large effect size t(29) = 9.76, p < .001, d = 1.78 [1.12–2.36], Figure 1. Key points are the very high ratings of the HEIDI app on quickness, ease of use, accessibility, usefulness and satisfaction (Figure 2). Well over 90% of respondents prefer the HEIDI app to previous diary methods, would choose to continue using it and would recommend it to others.
Conclusions: Headache diary mobile applications are a valuable tool for monitoring patients with headache conditions with high rates of patient user satisfaction over traditional paper headache diaries. Clinician access to bespoke individual headache data allows efficient remote monitoring and enables the service to be responsive to the patients’ needs in keeping with the NHS England Further Faster drive to improve efficiency of outpatient services. It also has implications for collection of comparable data on a larger scale which will be a powerful instrument in measuring headache treatment outcomes nationally or internationally


LB.P39
Longitudinal Analysis of a Nitroglycerin-Induced Mouse Migraine Model.
A Fantina-Woblistin1, L Breznik1, L Jauk1, R Rabl1, M Daurer1, T Löffler1 and M Prokesch1
1Scantox Neuro GmbH, Graz, Austria
Introduction: Migraine is one of the most common neurologic disorders affecting more than a billion people worldwide. However, the neurophysiological causes and thereby potential intervention avenues of migraine and its associated headache and neurological symptoms remain mostly unknown. These severely impairing symptoms and the lack of understanding emphasize the need for a fast turnaround model to study this condition and treatment options. The nitric oxide donor nitroglycerin (NTG) induces severe migraine-like attacks in mice and humans and was thus chosen to establish an inducible murine migraine model.
Objectives: Establish a robust NTG-induced model to enable treatment studies for migraine-like symptoms in mice. Define and validate behavioral, biochemical and histological readouts for longitudinal analysis of the condition.
Methods: 2-3 months old C57BL6 mice were injected with NTG every other day for 5 injections total (see figure). After the first, the fifth and after a week of wash-out period, behavioral tests were performed, and subsets of mice were sampled for biochemical and histological evaluation (see figure). Co-injection of the common anti-migraine compound sumatriptan was used as reference item. Mice were assessed for increased allodynia by grimace scale, grooming and hotplate test as well as light sensitivity in the light/dark box. Histologically and biochemically investigation was performed for c-fos, CGPR and inflammation markers.
Results: Mice tested after the initial injection or after repeated injection of NTG over multiple days showed a strong increase in the nociceptive response in the grimace scale analysis that could be alleviated by co-injection of sumatriptan, similarly to what has been observed in humans. No difference between groups was found after the wash-out period. Grooming, hot-plate and light-dark box testing did not show any differences between NTG- and vehicle-treated mice. Although biochemical and histological analysis is still ongoing, the first results indicate an increase in CGRP; c-fos, and IL-1beta signal in the medial prefrontal cortex of the brain.
Conclusion: These results affirm the NTG-induced migraine model as a valid and fast system to study migraine pathology in mice. The grimace scale proved to be a strong indicator of nociception in NTG-treated animals.
Figure

LB.P40
Nanotechnology in Headache Pathophysiology: Basic and Clinical Research on Liposomes and Nanoemulsions
T Kryeziu1, A Zajmi1 and M Basholli-Salihu1
1University Of Prishtina, Faculty Of Medicine, Prishtina, Kosovo
Introduction: The application of liposomes and nanoemulsions in headache research offers novel insights into the pathophysiology and treatment of migraine and cluster headaches. These nanoformulations could improve drug delivery, stability, and targeting, potentially transforming headache management.
Objectives: Review current research on liposome nanoemulsions in headache therapy.
Assess cytotoxicity and safety of these formulations.
Explore their effectiveness in delivering headache medications.
Methods: A comprehensive review of publications on liposomes and nanoemulsions in headache research was conducted, focusing on their preparation, characterization, cytotoxicity, and therapeutic efficacy.
Results: Studies demonstrate that liposome nanoemulsions enhance drug delivery and reduce cytotoxicity. Preclinical and clinical trials indicate improved therapeutic outcomes.
Conclusion: Liposome nanoemulsions hold promise for advancing headache treatment, offering enhanced delivery mechanisms and better safety profiles. Further research is needed to optimize these formulations for clinical use.
Conflict of Interest
The authors declare no conflicts of interest.
LB.P41
The Great Divide: Cluster Headache and Migraine Explained
A Zajmi1, T Kryeziu1, B Zajmi1 and E Muçaj1
1Faculty of Medicine, University of Prishtina, Prishtina, Kosovo
Introduction: Cluster headache and migraine are distinct primary headache disorders, each characterized by unique clinical features and underlying mechanisms. Understanding these differences is essential for effective diagnosis and management.
Objectives:
− Compare the clinical manifestations of cluster headache and migraine.
− Explore their distinct pathophysiological mechanisms.
− Evaluate current treatment strategies and their efficacy.
Materials and Methods: A comprehensive search of PubMed, MEDLINE, and Cochrane Library was conducted. Recent studies published, including systematic reviews, meta-analyses, case studies, and clinical trials, were analyzed.
Results: Cluster headaches present with severe unilateral pain and autonomic symptoms, while migraines involve pulsating headache with nausea and sensory sensitivity. Neuroscientific findings indicate distinct activation mechanisms for cluster headache—specifically involving the trigeminal-autonomic reflex—and migraine, which are associated with cortical spreading depression. Treatment options vary, including triptans and oxygen therapy for cluster headaches and triptans, CGRP antagonists, and lifestyle modifications for migraine.
Conclusion: Cluster headache and migraine exhibit different clinical features and pathophysiological mechanisms, necessitating tailored diagnostic and therapeutic approaches. It is imperative to explore potential biomarkers that could enhance disease categorization and facilitate targeted treatments for both cluster headaches and migraines. Further research is crucial to optimize management strategies and improve patient outcomes.
LB.P42
TMS-EEG reveals disrupted GABAergic and glutamatergic neurotransmission in Visual Snow Syndrome
V Santoro1,2, L Rocchi1,3, H Clark4, A Carobin1, I Premoli1, P Fong5,6, M Richardson1, P Goadsby2 and F Puledda2
1Department of Basic and Clinical Neuroscience, Institute of Psychiatry, Psychology and Neuroscience (IoPPN), King’s College London, London, United Kingdom
2Headache Group, Wolfson SPaRC, Institute of Psychiatry Psychology and Neuroscience (IoPPN), King’s College London, London, United Kingdom
3Department of Medical Sciences and Public Health, University of Cagliari, Cagliari, Italy
4Centre for Cognitive Neuroimaging, School of Psychology and Neuroscience, University of Glasgow, Glasgow, United Kingdom
5Division of Movement Disorders, Department of Neurology and Neuroscience Research Centre, Chang Gung Memorial Hospital at Linkou, Taoyuan City, Taiwan, ROC
6Medical School, College of Medicine, Chang Gung University, Taoyuan City, Taiwan, ROC
Introduction: Visual snow syndrome (VSS) is a condition characterised by persistent visual disturbances, particularly flickering dots across the visual field. Patients also report palinopsia, photophobia, and entoptic phenomena. The pathophysiology of VSS is associated with dysfunctional central visual processing, involving altered glutamatergic and GABAergic neurotransmission in the primary visual cortex V1 and motion area V5. Transcranial magnetic stimulation (TMS) combined with electroencephalography (EEG) over the primary motor cortex (M1) has widely been used to assess excitation/inhibition (E/I) balance.
Among the various peaks of the TMS-evoked EEG signals, the N45 peak reflects a balance of GABAAergic and glutamatergic neurotransmission, while P60 and N100 are modulated by glutamatergic and GABAB receptor-mediated neurotransmission, respectively.
Time-frequency decomposition of the TMS-EEG signal results in TMS-related spectral perturbations (TRSP). GABAA receptor-mediated inhibition is involved in the early increase of alpha TRSP, while GABAB receptor-mediated inhibition contributes to its late suppression. Both GABAA and GABAB receptor-mediated inhibition affect late beta TRSP suppression.
Objectives: Our aim in the present study is to investigate TMS-EEG biometrics as markers of cortical E/I balance in VSS.
Methods: TMS-evoked EEG potentials (TEPs) and TRSP were recorded in 10 patients with VSS (mean age = 35.9) and 10 healthy controls (mean age = 25.9). 150 TMS pulses at 90% of resting motor threshold were applied over left M1 during EEG recording, while 90% of the phosphene threshold was used for stimulation over left V1 and V5. Differences in TEPs and TRSP between patients and controls were analysed using multiple independent sample t-tests with a cluster-based permutation analysis for correction of multiple comparisons.
Results: VSS patients exhibited significantly higher suppression of late alpha and beta TRSP over M1 (270–800 ms; 210–440 ms) and early gamma TRSP increase over V1 (60–130 ms) compared to controls (p = 0.01; p = 0.01; p = 0.04). Other comparisons were not statistically significant (p > 0.05); however, trends towards increased N100 amplitude over M1 and reduced early TEP components over V5 were observed in VSS patients.
Conclusion: These results contribute to extend previous findings demonstrating altered excitation/inhibition balance in VSS. Higher alpha and beta TRSP suppression over M1, along with increased early gamma TRSP over V1 in patients, suggest impaired GABA receptor-mediated inhibition in this population. Additionally, the trend towards increased N100 amplitude over M1 and reduced early TEP components over V5 may indicate altered GABAergic and glutamatergic neurotransmission in these cortical areas.
LB.P43
The clinical features of migraine and their correlation with the thickness of the retinal nerve fibre layer
A Mishra1 and R Shukla1
1All India Institute Of India, Raebareli, India
Introduction: Unilateral, pulsating headaches that occur frequently are the hallmark of migraine. The decrease of blood flow and vascular narrowing that occur in the brain and eyes are known to be temporary, but long-term functional and structural alterations in these systems may be brought on by the chronic nature of migraine. It may cause changes in the thickness of the retinal nerve fibre layers (RNFL) and axonal loss. In order to determine if RNFL thickness and migraine clinical characteristics are associated, this study measured RNFL thickness, which offers a valuable indicator of the condition of the axons and the loss of ganglion cells in migraine patients.
Objective: The purpose of our study was to measure the RNFL thickness in migraine patients relative to age- and gender-matched controls, determine whether RNFL thickness varies in migraine patients with and without aura, and show whether these structural alterations are associated with migraine characteristics like duration and frequency of migraine episodes, and the degree of disability as determined by the MIDAS (Migraine Disability Assessment Scale).
Methods: A total of sixty migraine patients and sixty age- and gender-matched controls were enlisted. In addition to a thorough neurological and ophthalmological examination, RNFL was measured using spectral-domain optical coherence tomography (SD-OCT).
Results: There were non-statistically significant differences in RNFL thickness between migraine patients and controls in all quadrants of the retina on both sides (p-value >0.05). Additionally, there was no statistically significant difference in RNFL thickness between migraine patients with aura and those without (p-value >0.05) in any of the retinal quadrants on either side. The length of migraine attacks was found to be significantly correlated with both the superior RNFL thickness in both eyes and the inferior RNFL in the right eye. Additionally, there was a significant association (p < 0.05) between the length of the headache episode and the superior retina's RNFL thickness.
Conclusion: Our main finding was that, in contrast to controls, RNFL thickness did not significantly alter in migraine patients; however, RNFL thickness was significantly associated with the length of migraine sickness.
LB.P44
Use of Rimegepant 75 mg for the Acute Treatment of Migraine is Associated with a Reduction in Monthly Migraine Days: A Pooled Analysis of 2 Open-label
S Yu1, T Fullerton2, G Pixton2, Y Zou3, Q Zhong3 and H Zhu3
1PLA General Hospital, Beijing, China
2Pfizer Inc, Groton, United States
3Pfizer (China) Research and Development, China
Introduction: Rimegepant, a calcitonin gene-related peptide receptor antagonist, is indicated for acute and preventive treatment of migraine in adults.
Objective: This analysis examined whether long-term use of rimegepant for acute treatment of migraine may provide an additional preventive effect.
Methods: Data were pooled from 2 uncontrolled long-term open-label trials of rimegepant (NCT03266588, NCT05371652). Participants in this analysis had ≥6 monthly migraine days (MMDs) during a 30-day observation period (OP). Participants took oral rimegepant 75 mg as needed, up to once per day for up to 52 weeks, for acute treatment of migraine attacks of any severity. Adverse events (AEs) and change in the number of MMDs (relative to the OP) were summarized descriptively.
Results: Of 1288 treated participants, 68.7% reported an AE, 4.7% reported a severe AE, 2.9% reported a serious AE, and 2.4% reported an AE leading to rimegepant discontinuation. Upper respiratory tract infection (9.5%), nasopharyngitis (7.8%), and COVID-19 (7.6%) were reported by ≥5% of participants. Among 1269 participants included in the MMD analysis, the mean (SD) number of MMDs during the OP was 11.1 (4.3). The number of MMDs decreased, relative to the OP, over the course of 52-week treatment with rimegepant (Table). The mean (SD) change in MMDs was –2.0 (4.6) for the overall 52-week treatment period.
Conclusion: Long-term use of rimegepant 75 mg for acute treatment of migraine, up to once per day for up to 52 weeks, was well tolerated and may provide an additional preventive effect as evidenced in a reduction in MMDs. The observation that MMDs were reduced over time suggests that medication overuse headache is unlikely to be associated with rimegepant.

LB.P45
The effect of selective adenosine A3 receptor (A3AR) agonism on migraine-like dural-responsive trigeminocervical neurons
M Gamal-Eltrabily1, M Romero-Reyes1, D Salvemini2 and S Akerman1
1Department of Neural and Pain Sciences, School of Dentistry, University of Maryland Baltimore, Baltimore, United States
2Department of Pharmacological and Physiological Science, Saint Louis University, St Louis, United States
Introduction: Despite recent advances with new therapies, migraine management remains challenging for a large proportion of patients, with many showing weak or no response to the currently available pharmacological interventions. There is therefore significant interest in finding novel pharmacological targets for treatment. The adenosine A3 receptor (A3AR) is a Gi protein-coupled receptor that is widely expressed in the central nervous system and could represent a safe, novel option for targeted therapy. Previous preclinical studies have shown that A3AR agonism helps in alleviating various chronic pain states, via modulation of neuronal and glial activity. The possible role of A3AR in trigeminal-related nociception and migraine is unknown.
Objectives: To determine the effect of A3AR agonism on migraine-like trigeminal neuronal activity and establish the potential of A3AR as a novel target for the treatment of migraine and other related diseases.
Methods: Male and female Sprague Dawley rats were anesthetized, cannulated, and mounted on a stereotaxic device and maintained under anesthesia using propofol (20–30 mg/kg/hr.-IV infusion). Blood pressure, body temperature and expired CO2 were constantly monitored. In vivo electrophysiological extracellular recordings of trigeminocervical complex (TCC) neurons at the C1 level were performed, measuring ongoing spontaneous activity, and responses to cutaneous innocuous (brushing) and noxious (pinching) stimulation of receptive fields within the ophthalmic trigeminal division (V1), as well as to stimulation of the intracranial dural vasculature. Under these conditions, we tested the effect of intravenous (IV) administration of the selective A3AR agonist, Cl-IB-MECA (1 mg/kg), naratriptan (3 mg/kg; positive control), or saline (vehicle control) on these neuronal outcomes, over 180 minutes.
Results: Cl-IB-MECA and naratriptan significantly decreased TCC neuronal responses to dural electrical stimulation (both A-delta and C fibers responses) (p < 0.0001, n = 8 each) and ongoing spontaneous firing (p < 0.0001), when compared to vehicle group. Their inhibitory effect on TCC neurons was observed starting from 15 minutes following IV administration and lasted for the 180-min recording period without recovery. No statistical significance was observed when comparing Cl-IB-MECA with naratriptan groups (p < 0.72). Neither CI-IB-MECA nor naratriptan affected responses to cutaneous stimulation, however, Cl-IB-MECA did cause a decrease in blood pressure.
Conclusions: These data provide preclinical support that A3AR agonism modulates dural-responsive trigeminocervical neurons, inhibiting neuronal activity, and may therefore have a potential role in migraine-related mechanisms. It also provides strong support for A3AR as a novel target for therapeutic development. Cl-IB-MECA did cause changes in blood pressure that we believe relate to non-specific binding at A1 and A2A adenosine receptors. Future studies will use a new generation of highly selective A3AR agonists, which should confirm the efficacy of A3AR as a potentially novel target in migraine management, without these off-target effects.
LB.P46
Comparing Candesartan and Vitamin E for Prophylactic Treatment in Episodic Migraine Patients
A Oosterlee1, B Van der Arend, E Van Zwet, N Pelzer and G Terwindt
1Leiden University Medical Center, Leiden, The Netherlands
Introduction: Candesartan is recommended as a first-line prophylactic migraine treatment in both national and international guidelines. Small cross-over trials show it is superior to placebo and non-inferior to propranolol. Its low cost, minimal side effects, and few drug interactions make it a highly attractive first-line option.
Objectives: To investigate the efficacy of candesartan compared to vitamin E as prophylactic treatment in patients with episodic migraine.
Methods: This cohort study gathered electronic headache diary data from individuals with episodic migraine (EM) at the Leiden Headache Center. We specifically compared female patients with EM who were prescribed either candesartan or vitamin E. Our validated electronic diary features a validated algorithm capable of distinguishing between monthly migraine days (MMD) and monthly headache days (MHD). The baseline period was defined as the 28 days preceding the start of treatment. Primary outcome was the 50% responder rate for reduction in MMD from baseline to the last 28-day period with the highest achieved dosage of candesartan (≥4 mg daily) or vitamin E (400 IU daily). Secondary outcomes included change in MMD, MHD, and monthly acute medication days (MAMD). Groups were adjusted for baseline differences using propensity score matching, with each patient receiving a score based on age, MMD and MAMD, and subsequently matched 3:1 (candesartan to vitamin E). Chi-square test was used for the primary outcome, t-tests were used for secondary outcomes.
Results: After propensity score matching, 183 subjects were identified in the candesartan group and 61 in the vitamin E group. The mean age was 46.17 ± 11.66 years in the candesartan group and 43.44 ± 8.44 years in the vitamin E group. At baseline, the groups were comparable for MMD (5.89 ± 2.38 vs. 5.20 ± 2.77), MHD (9.65 ± 4.31 vs. 8.16 ± 3.69), and MAMD (5.57 ± 3.27 vs. 5.77 ± 3.37). Overall, 29.5% of patients in the candesartan group and 31.1% in the vitamin E group had a ≥ 50% response (OR = 1.1; 95% CI: 0.6–2.0). No differences were found between candesartan and vitamin E in the mean reduction of MMD (0.83 ± 3.46 vs. 0.66 ± 3.08, p = 0.73), MHD (1.25 ± 4.23 vs. 0.74 ± 3.31, p = 0.39), and MAMD (0.31 ± 4.18 vs. 0.44 ± 2.90, p = 0.82).
Conclusion: Both candesartan and vitamin E treatments achieved comparable 50% responder rates, similar to CGRP-Mabs treatments in clinical trials, indicating significant efficacy.
LB.P47
Three-month improvements in quality of life with fremanezumab in a real-world survey of an Irish chronic migraine patient cohort
E O'Sullivan2, M Ruttledge3, D Dhiraj4 and M O'Byrne1
1Teva Pharmaceuticals Ireland, Swords, Ireland
2Department of Neurology, Cork University Hospital, Cork, Ireland
3Department of Neurology, Beaumont Hospital, Dublin, Ireland
4Teva UK Limited, Castleford, United Kingdom
Introduction: Migraine is a neurological disease that can significantly affect quality of life (QoL). Fremanezumab is a calcitonin gene-related peptide (CGRP) pathway targeting monoclonal antibody for the prevention of migraine in adults. In Ireland, fremanezumab is reimbursed by the national health service for adult patients with chronic migraine who have failed three or more conventional prophylactic treatments. There is currently no real-world data for Ireland showing the impact of fremanezumab on QoL outcomes.
Objectives: This survey aimed to evaluate short-term QoL outcomes in patients with chronic migraine treated with fremanezumab in the Republic of Ireland.
Methods: This survey was conducted face-to-face by specialist nurses as an addition to the fremanezumab patient support programme (PSP). Each patient starting fremanezumab received two nurse visits: at treatment initiation for injection training (Visit 1), and a follow-up three months later (Visit 2). Patients prescribed fremanezumab through the Health Service Executive [HSE] managed access protocol < map > were eligible. Exclusion criteria were: treated with any CGRP pathway monoclonal antibody within the preceding six months; receiving fremanezumab for the treatment of a condition other than migraine; aged <18 or >70 years; or current pregnancy. Eligible patients who consented to participate completed a survey prior to receiving fremanezumab (Visit 1; QoL and demographics) and at three months post-initiation (Visit 2; QoL and PSP evaluation). QoL assessment used the Migraine-Specific Quality of Life Questionnaire (MSQ, v2.1; raw domain scores linearly converted and scaled to 0-100 scale, 100 indicating full functionality). Only descriptive statistics were preplanned. Additional post hoc statistical comparisons were conducted using Wilcoxon signed-rank test (Kolmogorov-Smirnov analysis indicated data were not normally distributed).
Results: 124 patients were recruited and underwent Baseline assessment; 119 had a three-month assessment, with five patients (4.0%) lost to follow-up. All 124 (100%) were initiated on monthly fremanezumab, with one patient transferred to quarterly dosing by 3-month follow-up. Baseline demographics, time since diagnosis, frequency of acute medication usage and number of prior preventive failures are presented in the Table. These show that the patient group had longstanding migraine, a high number of prior preventive failures and frequent usage of acute medication at Baseline. Results of MSQ median domain scores for Baseline versus three-month follow-up (Figure) were: Role Function – Restrictive (RFR) 28.57 (Baseline) vs 65.71 (three-month); Role Function – Preventive (RFP) 50.00 vs 80.00; and Emotional Function (EF) 20.00 vs 73.33. Across all MSQ domains, a substantial improvement in median score was seen from Baseline to follow-up. These differences from Baseline to follow-up exceeded the minimally clinically important differences across all domains, demonstrating meaningful improvement for patients. Statistical analysis showed that across all three domains, 3-month MSQ scores were significantly higher than Baseline (p < 0.001).
Conclusion: Treatment with fremanezumab led to a meaningful improvement in QoL in the real-world setting, for patients with chronic migraine in Ireland in only three months. This provides further supportive evidence for fremanezumab in a cohort of patients that are representative of the most challenging to treat at a headache/migraine clinic.


LB.P48
Safety Outcomes from a Phase 3, Randomised, Double-Blind, Placebo-Controlled Study of Fremanezumab for the Preventive Treatment of Episodic Migraine in Children and Adolescents
A Hershey1, C Szperka2, S Barash3, S Garnett3, J Bryson3, Y Kesler4, T Erez4, Y Carmeli Schwartz4, M Grozinski-Wolff3 and X Ning3
1Cincinnati Children’s Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, USA
2Children’s Hospital of Philadelphia and Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA
3Teva Branded Pharmaceutical Products R&D, Inc., West Chester, USA
4Teva Pharmaceutical Industries Ltd., Tel Aviv, Israel
Introduction: There are limited well-tolerated preventive migraine treatments approved for children and adolescents. Monoclonal antibodies (mAbs) that target the calcitonin gene related peptide (CGRP) or its receptor are approved for the preventive treatment of migraine in adults. The efficacy, safety and tolerability of fremanezumab, a humanised mAb targeting CGRP, have been demonstrated in multiple Phase 3 randomised controlled trials (RCTs) in various adult populations. However, there are currently limited data on the safety of CGRP pathway mAbs in children and adolescents.
Objectives: The SPACE study (NCT04458857) aimed to evaluate the efficacy, safety and tolerability of fremanezumab in children and adolescents with episodic migraine (EM). Here we present the safety outcomes from the SPACE study.
Methods: This multicentre, parallel-group, Phase 3 study consisted of a 4-week screening period and a 12-week double-blind period. Eligible participants were aged 6–17 years, with a diagnosis of migraine (consistent with ICHD-3 criteria) ≥ 6 months prior to screening and a history of ≤14 headache days per month in each of the 3 months prior to screening. Participants were randomised 1:1 to receive monthly fremanezumab subcutaneously (120 mg for <45 kg, 225 mg for ≥45 kg) or matched monthly placebo. The primary endpoint was the least-squares (LS) mean change from baseline in monthly average number of migraine days (MMD) during the 12 week double-blind period. Safety and tolerability were assessed through adverse event (AE) reporting, clinical laboratory test results and electrocardiogram findings.
Results: In total, 237 participants were randomised and 235 were available for analysis and allocated to fremanezumab (n = 123 [120 mg, n = 36; 225 mg, n = 87]) or placebo (n = 112) treatment groups. In total, 97% of participants in the fremanezumab group and 95% in the placebo group completed the 12-week double blind period. The proportion of participants reporting any AE was generally consistent across treatment groups (Table 1). Injection site reactions were the most common AEs reported more frequently with fremanezumab compared with placebo. The proportion of participants with serious AEs and AEs leading to discontinuation were low, and no deaths were reported. In addition, the primary endpoint of LS mean change from baseline in MMD over 12 weeks was –2.5 for fremanezumab versus –1.4 for placebo (p = 0.0210).
Conclusions: The safety and tolerability profile of fremanezumab in children and adolescents with EM was consistent with previous RCTs in adults, with no new emerging safety signals observed. These findings suggest fremanezumab provides an effective and well-tolerated preventive migraine treatment option in this patient population.

LB.P49
From Botulinum Neurotoxin to Breakthrough: Microvascular Decompression Resolves Severe Hemifacial Spasm
K Gaston1, J Sidhu1 and P Shah1
1Larkin Community Hospital, Miami, United States
Introduction: Hemifacial spasm (HFS) is a neuromuscular disorder characterized by involuntary unilateral contractions of facial muscles. Botulinum neurotoxin (Botulinum) injections are frequently employed as a symptomatic treatment, though long-term use presents concerns regarding efficacy and adverse effects. This case report discusses the clinical progression, complications, and eventual successful surgical intervention in a patient with HFS.
Objectives: To evaluate the limitations of prolonged Botulinum treatment in HFS management and to demonstrate the efficacy of microvascular decompression (MVD) as a definitive therapeutic approach.
Methods: A 53-year-old female with a history of hypertension presented in 2018 with left eye twitching. Initial treatment with 20 units of Botulinum resulted in symptomatic relief lasting 3-4 months. Over time, escalating doses up to 80 units led to adverse effects, including left facial flaccid paralysis and intermittent winking of the left eye. An MRI revealed periventricular plaques, raising suspicion for multiple sclerosis, which was later ruled out. Despite the exclusion of multiple sclerosis, the patient experienced worsening symptoms, including platysma twitching, dysphagia, and chronic intermittent retinal migraines significantly impacting her quality of life. She developed lower self-esteem, avoided photographs, and withdrew from public speaking engagements due to ridicule from colleagues. Following referral to a neurosurgeon, MVD was performed to alleviate the compression of cranial nerves VII, VIII, and IX by the anterior inferior cerebellar artery (AICA) and posterior inferior cerebellar artery (PICA) with Teflon insertion.
Results: The MVD procedure resulted in complete resolution of the patient’s HFS symptoms. Postoperatively, the patient reported significant improvements in quality of life, with no recurrence of facial twitching, dysphagia, or retinal migraines. This successful outcome emphasizes the importance of timely surgical intervention in cases where conservative treatments are inadequate.
Conclusion: This case highlights the limitations of long-term Botulinum therapy for HFS and the effectiveness of MVD in resolving severe, refractory symptoms. Early and accurate diagnosis, combined with prompt surgical referral, is crucial for optimal patient outcomes. Enhanced awareness among healthcare providers regarding alternative treatment modalities can significantly improve patient care and quality of life.

Author Index
Key
EP. = Electronic Poster
MO. = Mini Oral Presentation
O. = Oral Presentation
P.= Poster, M
LB.= Late-Breaking Presentation
A
Aaseth, K P.04
Abagnale, C E P.45, MO.06
Abraham, L E P.15, EP.18, EP.20
Afridi, S E P.05, EP.06
Ahern, A E P.05, EP.06
Ahmed, F E P.23, MO.08, MO.11, P.07, P.09
Ailani, J E P.15, EP.33, MO.12, P.12, P.21
Akbarkhodjaeva, Z P.11, P.18
Akcicek, H E P.32
Akerman, S E P.38, EP.39, LB.07, LB.P45
Ali, A E P.03, EP.21, EP.37
Alim-Marvasti, A E P.08
Allena, M MO.03
Al-Mahdi Al-Karagholi, M E P.04
Amarasena, P E P.43, EP.44, MO.09, O.08
Ambrosini, A E P.04
Amin, F E P.24
Antoniazzi, A MO.03
Anukoolwittaya, P P.02, P.19, P.23
Aoun, M P.15
Arkuszewski, M P.15
Ashina, M E P.07, EP.32, EP.33, E P.34, MO.07, P.13, O.09
Ashina, S E P.31, EP.34
Ashraf, U E P.40, EP.46, P.26
Atkinson, J E P.18
Avino, G E P.16, P.06
Awad, S E P.33
Ayton, S MO.12
B
Babaei, M E P.47
Babanrao Pisal, C P.15
Barash, S E P.30, EP.36, LB.01, LB.P48
Barbanti, P E P.29
Barlow, S E P.20
Bartole, L P.17
Basholli-Salihu, M LB.P40
Baugh, C LB.P37
Beier, D E P.24
Benedek-Segal, M E P.30, EP.36
Bernard, J MO.08
Bevilacqua, J LB.P37
Bhatia, A E P.26
Bierrum, W E P.08
Bighiani, F MO.03
Bjørk, M O.05
Bjorvatn, B E P.02
Blaya, M P.22
Blumenfeld, A E P.35, P.38
Boissonade, F E P.12
Boneva, N MO.01
Boscain, F E P.16
Bosch, A MO.05
Boserup, L E P.33
Botfield, H E P.11
Braca, S E P.13, EP.28, O.04
Brandt, R MO.02
Breznik, L LB.P39
Broadhurst, S P.08, P.10
Broide, R O.02
Brown, J E P.15, EP.20, LB.P37
Bryson, J E P.30, EP.36, LB.01, LB.P48
Bubnov, R P.34
Burgalassi, A E P.16, P.06
C
Caetano, G O.03
Cammarota, F MO.03
Capote, M P.01
Caramia, F MO.06
Carmeli Schwartz, Y EP.36, LB.01, LB.P48, EP.30
Carmine Belin, A EP.01
Carobin, A LB.P42
Caronna, E O.09
Carr, K E P.31
Carrazana, E LB.04
Casillo, F EP.45, MO.06
Cattaruzza, T P.17
Cerghet, M EP.21
Cetta, I EP.49, MO.13
Cevoli, S EP.16, P.06
Chan, A EP.14
Chan, X P.03
Chandratheva, A EP.08
Charles, A MO.01
Chaudhry, B EP.24
Chehrenama, M EP.26, EP.27
Chen, G EP.30, EP.36
Cheung, A LB.04
Cho, S EP.31, EP.34
Church, E EP.11
Cirillo, J EP.15
Clark, H LB. P42
Collings, S EP.05, EP.06
Colombo, B EP.49, MO.13
Contreras-De Lama, J P.38
Cook, L P.37
Coppola, G EP.16, EP.45, MO.06, P.06
Corrado, M EP.16, MO.03, P.06
Cowan, R EP.47
Coyle, L E P.09
Craig, J EP.03
Crawford, M P.03
Cretella, G EP.13, EP.28, O.04
Cullum, C EP.24
D
da Silva Lima, G EP.26, EP.27
Dabruzzo, B EP.31, P.37
Dahan, A P.14
Dai, F EP.20
Dalla Volta, G EP.16, P.06
Danelakis, A O.05
Danno, D P.28
Daurer, M LB.P39
Davis, L P.38
de Abreu Ferreira, R EP.34
de Boer, I LB.06
de Brún, C EP.18
De Felice, M EP.12
De Icco, R EP.16, MO.03, P.06
De Matteis, E EP.16, P.06
De Santis, F P.06, EP.16
De Simone, R EP.13, EP.28 O.04
Deb, M P.10
Delahaye, L P.05, P.12
Delahaye, L P.13
Delrosario, H EP.23, MO.11, P.07, P.09
Demartini, C MO.03
DeSouza, D EP.47
Dethabrew, A EP.08
Dhiraj, D LB.P47
Di Giacomo, D P.33
Di Lorenzo, C MO.06
Di Lorenzo, G EP.45
Di Piero, V MO.06
Di Renzo, A MO.06
Diamond, M P.37
Do, T EP.24
Dodick, D EP.26, EP.27
Dolezil, D EP.27, P.15
Dorman, P EP.32
Dorsey, S EP.23, MO.11, P.07, P.09
Duan, M MO.12
Duncan, C EP.09
E
Edvinsson, J EP.01, P.36
Edvinsson, L EP.01, P.36
Elhadd, K P.03
Erez, T LB.01, LB.P48
Espie, C P.03
Esteves, I O.03
Ettrup, A EP.33, MO.01
Eyupoglu, S EP.10, P.20
F
Fantina-Woblistin, A LB.P39
Fasano, C EP.16, P.06
Figueiredo, P O.03
Filippi, M EP.49, MO.13
Flannery, S EP.09
Fleming, L P.03
Florea, I MO.07
Fominykh, M EP.04
Fong, P LB.P42
Fountaine, R EP.14, EP.17
Fouto, A O.03
Francavilla, M MO.03
Fronczek, R MO.02, MO.05
Fullerton, T LB.P44
G
G. Nunes, R O.03
Galic, M EP.29
Gamal-Eltrabily, M LB.P45
Gandhi, P EP.31, MO.12
Garascia, G P.17
Garces, K P.01
Garelja, M LB.05
Garnett, S LB.01, LB.P48
Gaston, K LB.P49
Genovese, F EP.49, MO.13
Ghadiri-sani, M P.03, P.08, P.10
Giannini, C EP.13, EP.28, O.04
Giles, D O.05
Gil-Gouveia, R EP.27, O.03, P.15
Gilli, S EP.45
Giuliani, G MO.06
Goadsby,P EP.31, EP.43, EP.44, LB.03, LB.P42, MO.04, MO.09, O.08, P.05, P.31, P.35, O.09, MO.01, LB.02
Gobbi, C EP.04
Gonzalez-martinez, A MO.04
Gormal, R O.02
Gorrie, G P.03
Gosalia, H LB.02, MO.04
Gowman, H EP.05, EP.06
Granato, A EP.16, P.06, P.17
Grech, O EP.11
Greco, R MO.03
Greenwood, A P.03
Greenwood, F MO.09
Grillo, V MO.03
Grøntveit Winnberg, I EP.04
Grozinski-Wolff, M LB.01, LB.P48
Guerra, F P.33
Guerrieri, S MO.13
Gupta, M P.01
H
Ha, H P.05, P.12, P.13
Hagen, K O.05
Haider, S EP.08
Hall, J EP.12
Hamilton, K EP.37
Han, X EP.19
Hancock, L EP.20
Hansen, J EP.07
Hauberg, D EP.07
Hay, D LB.05
He, M EP.31, EP.34, P.38
Henry, A P.03
Hershey, A LB.01, LB.P48
Hiele, E MO.10
Hill, L EP.11
Hiransuthikul, A P.02, P.19, P.23
Hirata, K P.25, P.30
Holland, P O.01
Holle-Lee, D EP.31, EP.34
Horniblow, R EP.11
Hougaard, A EP.04
Hughes, O P.37
Hygge Blakeman, K EP.15, EP.20
I
Iannone, L EP.16, P.06
Imai, N EP.41, P.29
Irimia, P O.09
Ishikawa, K LB.04
Iskender, M P.20
Iyilikci, O P.20
J
Jackson, J EP.20
Jahansooz, J LB.04
James, L P.21
Jantzen, F EP.24
Jauk, L L B.P39
Jenkins, A E P.15, EP.18
Jenkins, B P.37
Jennysdotter Olofsgård, F EP.01
Jensen, R MO.01
Josiassen, M MO.01
K
Kamimura, J P.29
Kandapara, S P.08
Karsan, N EP.43, EP.44, MO.04, O.08
Kashiwaya, Y P.28
Katsarava, Z P.05
Keicho, M P.29
Kennedy, G LB.P38
Kernick, D P.27
Kesler, Y LB.01, LB.P48
Kessler, Y EP.36
Khalil, M EP.23, P.09
Khalil, M MO.11
Khan, R EP.23, MO.08, MO.11, P.07, P.09
Khodaie, M MO.07
Khodavirdi, A EP.26
Kikui, S P.28
KItamura, E EP.41
Kmyta, O P.24
Kobayashi, S P.25, P.30
Kokturk, P EP.32
Konishi, T P.29
Kristoffersen, E EP.02, P.04
Kruit, M LB.06
Kryeziu, T LB.P40, LB.P41
Kulkarni, D EP.50
Kumelj, T O.05
L
Lam, J P.05, P.12, P.13
Langseth, H O.05
Lanteri-Minet, M EP.27, P.05, P.12, P.13
Lastarria Perez, C EP.43, EP.44, O.08
Laverick, J P.03
Law, S EP.05, EP.06
Lee, A LB.04
Lee, H LB.04
Lee, X EP.33
Leroue, C LB.P37
Leroux, E P.05
Lewis, M EP.15
Lilley, J LB.P37
Linander, C MO.01
Linstra, K LB.06
Liow, K LB.04
Lipton, R EP.17, EP.29, EP.33, MO.12
Little, N LB.04
Liu, Y P.05, P.12, P.13
Liu, Z EP.27
Löf, E MO.07
Löffler, T LB.P39
Lombardo, T P.17
Lønberg, U EP.07
Lucas, C EP.27
Lunder, O P.04
M
Ma, L EP.19
Maassen van den Brink, A EP.25, LB.06, O.09
Macarimban, R EP.08
Maddahi, A P.36
Mahmood, S EP.21
Mampreso, E EP.16, P.06
Manack Adams, A P.37
Manganotti, P P.17
Martin, B P.03
Matharu, M O.05, P.12
Mathew, P EP.37
May, A EP.42, EP.48
Mazzotta, E MO.03
Mechtler, L P.37
Mehnert, J EP.48
Messina, R EP.49, MO.13
Meunier, F O.02
Michalski, S LB.07
Miele, A EP.28
Mikol, D EP.27
MIRDJURAEV, E EP.22
Mishra, A LB.P43
Mitsikostas, D EP.29, EP.32, O.09
Moehring-Moskal, F LB.P37
Mohammad Amin, F EP.32
Mollan, S EP.11
Monteith, T P.01
Moraleda, J P.31
Moreno Ajona, D P.31
Moriya, A EP.41, P.29
Morrison, I P.03
Muçaj, E LB.P41
Mugo, C EP.11
Mukuto, S P.30
Munday, V O.01
Murakata, K P.28
Music, R EP.09
N
Naber, W MO.02
Nachev, P O.05
Nagaraj, K EP.43, EP.44, MO.04, O.08
Nelson, M O.02
Nežádal, T EP.32
Nguyen, T P.21
Ning, X EP.30, EP.32, EP.36, LB.01, LB.P48
Nofar, J EP.37
Nørgaard, I EP.24
Nyholt, D O.05
O
O'Byrne, M LB.P47
Oliveira, R P.32
Ololade, S EP.43, EP.44, O.08
Olsen, M EP.25
Oosterlee, A LB.P46
Ornello, R EP.16, P.06
Ortega, M EP.29
O'Sullivan, E LB.P47
Ota, K P.28
Ozdemir Gultekin, T EP.10
Ozge, A EP.10, P.20
P
Paemeleire, K P.15
Pagani, E EP.49
Pallesen, S EP.02
Patel, A EP.05, EP.06, LB.P37, P.21
Patwardhan, K EP.50
Pavão Martins, I EP.32
Pavlovic, J EP.17
Pawinski, R EP.05, EP.06, EP.14
Pelzer, N LB.P46
Peng, K EP.42, EP.48
Perdigão, A O.03
Peres, M P.13
Perrotta, A EP.04
Pfleeger, K EP.34
Phu Do, T EP.04
Phul, R MO.07
Piasecka-Stryczynska, K EP.27
Piella, E EP.16, P.06
Pinho, G P.32
Piri Cinar, B P.20
Pistoia, F EP.16, P.06, P.33
Pixton, G EP.14, EP.17, LB.P44
Pongpitakmetha, T P.02, P.19, P.23
Porcaro, C EP.45
Potapov, O P.24
Powell, L EP.18
Požlep, G P.16
Pozo-Rosich, P EP.32, O.09, P.05, P.12, P.13, P.15, P.21
Prabhakar, P EP.43, EP.44, O.08
Premoli, I LB.P42
Prokesch, M LB.P39
Puledda, F LB.P42
R
Rabl, R LB.P39
Rainero, I EP.16, P.06
Rakhimbaeva, G P.18
Ramirez Campos, V EP.29, EP.32
Ran, C EP.01
Ranieri, J P.33
Rao, R EP.26
Rattanawong, W P.02, P.19, P.23
Rees, T LB.05
Rhyne, C P.37
Richardson, M LB.P42
Rocca, M EP.49
Rocchi, L LB.P42
Rogula, B EP.18
Romero-Reyes, M EP.38, EP.39, LB.07, LB.P45
Romozzi, M EP.16, P.06
Rosenzweig, I O.01
Roth-Ben Arie, Z EP.29, EP.30, EP.36
Ruiz De La Torre, E O.09
Ruiz-Tagle, A O.03
Russo, A EP.16, P.06
Russo, C EP.13, EP.28, O.04
Ruttledge, M LB.P47
S
Sacco, S P.06
Sahin, G EP.32
Saleem, A EP.03
Salinas Abarca, A EP.38, EP.39
Sallowm, Y EP.21
Salvemini, D EP.39, LB.07, LB.P45
Sances, G MO.03
Sanjanwala, B EP.47
Santoro, V LB.P42
Saporito, G P.33
Schankin, C EP.32
Schlacher, C P.38
Schultz, L EP.21
Sebastianelli, G EP.16, EP.45, MO.06, P.06
See, I EP.08
Sellers, A P.22
Semel, D EP.17
Serizawa, M P.29
Shadmanova, L EP.22
Shah, P LB.P49
Shiina, T P.30
Shioda, M P.25
Shirazi, A EP.08
Shukla, R LB.P43
Sidhu, J LB.P49
Sihabdeen, S EP.04
Simister, R EP.08
Sinclair, A EP.11
Singh, J EP.03
Smith, J EP.31, EP.34, P.38
Snellman, J P.15
Snoer, A MO.01
Sondergaard, B O.02
Soontrapa, P EP.43, EP.44, O.08
Sotnikov, D P.24
Spence, N LB.P37
Spencer, J EP.08
Sperling, B EP.33, MO.01
Spivak, M P.34
Sridhar, J EP.47
Stark, R P.13
Steinberg, A EP.01
Steiner, T EP.07
Stepien, A P.15
Stornaiuolo, A EP.13, EP.28, O.04
Straghan, E EP.14
Stubberud, A O.05
Stude, P P.15
Study group, I MO.13
Styles, K EP.09
Sugiyama, H P.28
Sumelahti, M EP.32
Sureda I Gibert, P LB.07
Suzuki, K P.25, P.30
Suzuki, R P.29
Suzuki, S P.25, P.30
Sweeney, S LB.P37
Syed, P O.02
Szabó, G EP.26, EP.27
Szklener, S EP.26
Szperka, C LB.01, LB.P48
T
Takeshima, T P.28
Talukder, S P.10
Tassorelli, C EP.16, EP.26, EP.31, EP.32, EP.34, MO.01, MO.03, P.06, P.12
Tepper, S EP.17, EP.27
Tepper, S MO.01
Terwindt, G EP.25, LB.06, LB.P46, MO.02, MO.10, O.09, P.14,
Thakerar, S MO.08
Thanprasertsuk, S P.02, P.19, P.23
Thieleke, A EP.42
Thijs, R MO.05
Tomlinson, S EP.40, EP.46, P.26
Torres-Granados, R EP.38, LB.07
Trimboli, M EP.16, P.06
Tronvik, E EP.04, O.05
Trugman, J EP.34
Tucker, E P.05, P.12, P.13
TURAKULOVA, D EP.22
U
Uluduz, D EP.10, P.20
Uluduz, E EP.10, P.20
Umashankar, K MO.12
V
Vaghi, G EP.16, MO.03, P.06
Valente, M EP.16, P.06
Van der Arend, B EP.25, LB.P46. MO.10
van der Weerd, N LB.06
van Harten, T LB.06
van Kemenade, E MO.02
van Os, H LB.06
van Tilborg, P MO.02, MO.05
Van Veelen, N MO.10
van Velzen, M P.14
van Welie, F EP.25, P.14
Van Zwet, E LB.P46, MO.10
Vandenbussche, N EP.44, O.08
Veledar, E P.01
Versijpt, J EP.25
Vetvik, K P.04
Viana, M EP.04
Villar Martinez, M P.35
Vollono, C EP.16, P.06
W
Waage, S EP.02
Walker, C LB.05
Watson, D EP.09
Wei, D LB.02, MO.04
Weldon, E LB.04
Wermer, M LB.06
Whitton, W EP.20
Whitworth, L P.27
Whoriskey, S P.03
Wilcha, R-J LB.03, EP.43, EP.44, O.08
Williams, A MO.08
Wilms, A LB.06
Wilson, L MO.12
Winsvold, B O.05
Wisløff, T P.04
Wood, R EP.05, EP.06
Y
Yagi, N P.29
Yiu, G EP.30, EP.36
Yoshida, S P.29
Younis, S EP.24
Yu, S EP.17, EP.19, EP.30, EP.36, LB.P44
Z
Zajmi, A LB.P41
Zajmi, A LB.P40
Zajmi, B LB.P41
Zaletel, M P.16
Zanaboni, A MO.03
Zanandrea, L EP.49, MO.13
Zecca, C EP.04
Zhang, X LB.P37
Zhong, Q EP.19, LB.P44
Zhu, H LB.P44
Zhu, Y EP.26
Zou, Y EP.17, LB.P44

