
Abstract
Background
The present study aimed to assess the burden of neck pain in adults with migraine and tension-type headache (TTH), utilizing the Neck Disability Index (NDI) and Numeric Pain Rating Scale (NPRS).
Methods
A systematic literature search was conducted on PubMed and Embase to identify observational studies assessing NDI and NPRS in populations with migraine or TTH. The screening of articles was independently performed by two investigators (HMA and ZA). Pooled mean estimates were calculated through random-effects meta-analysis. The I2 statistic assessed between-study heterogeneity, and meta-regression further explored heterogeneity factors.
Results
Thirty-three clinic-based studies met the inclusion criteria. For participants with migraine, the pooled mean NDI score was 16.2 (95% confidence interval (CI) = 13.2–19.2, I2 = 99%). Additionally, the mean NDI was 5.5 (95% CI = 4.11–6.8, p < 0.001) scores higher in participants with chronic compared to episodic migraine. The pooled mean NDI score for participants with TTH was 13.7 (95% CI = 4.9–22.4, I2 = 99%). In addition, the meta-analysis revealed a mean NPRS score of 5.7 (95% CI = 5.1–6.2, I2 = 95%) across all participants with migraine.
Conclusions
This systematic review and meta-analysis shows a greater degree of neck pain-related disability in migraine compared to TTH. Nevertheless, the generalizability of these findings is constrained by methodological variations identified in the current literature.
This is a visual representation of the abstract.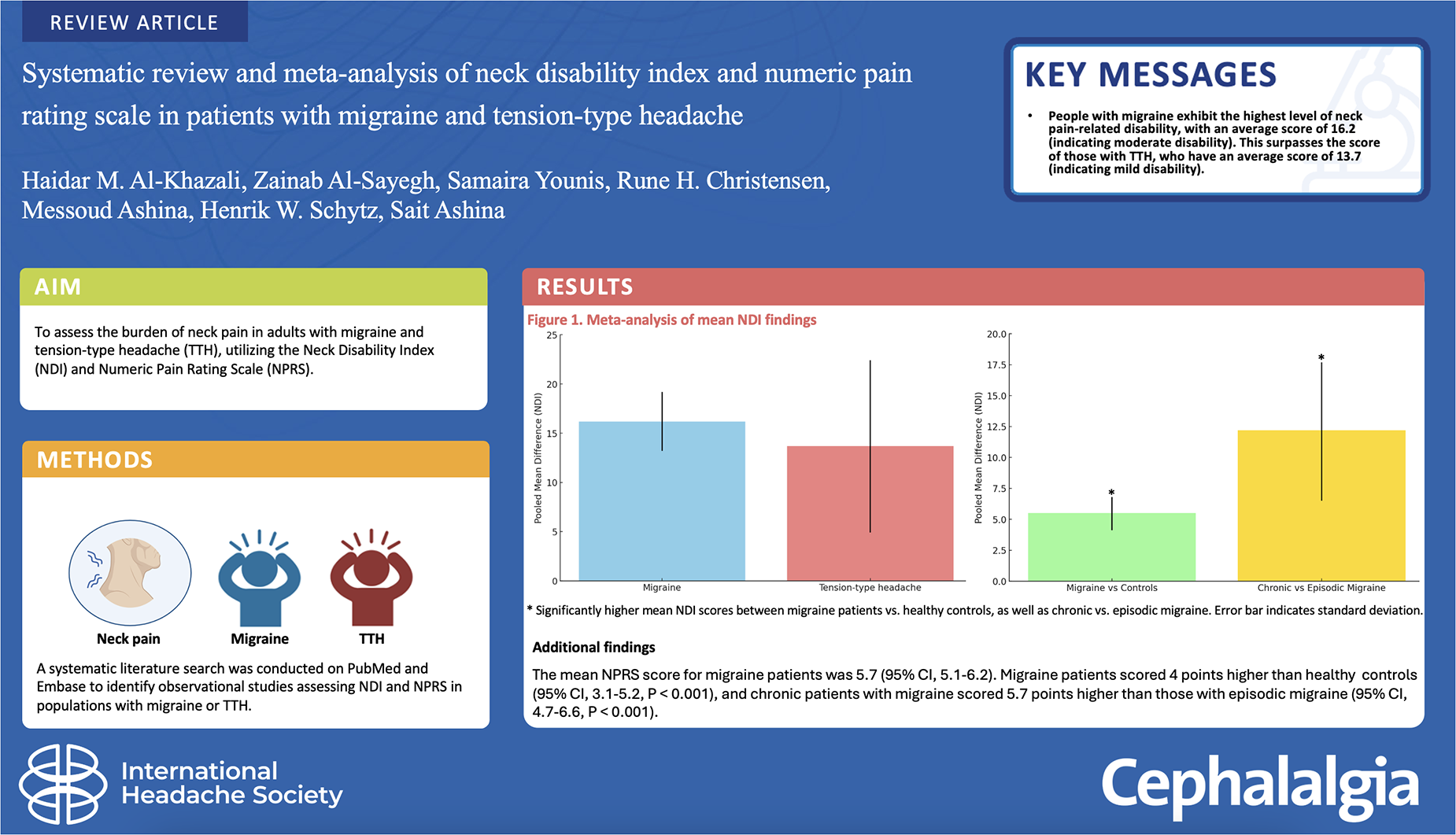
Keywords
Introduction
Neck pain has been found to be prevalent in individuals with both migraine and tension-type headache (TTH), yet the impact of neck pain in these conditions remains uncertain (1–6). Migraine and TTH are common primary headache disorders in the general population, and both are associated with significant burden and socioeconomic impact (7–9). Up to 80% of individuals afflicted by migraine report the presence of neck pain in association with their migraine attacks (1,10). The coexistence of neck pain is a maker of less favorable treatment responses and an unfavorable prognostic outlook for migraine (11–13). Moreover, cervical dysfunction might potentially trigger migraine attacks, leading to decreased periods between attacks and the progression to chronic headache (14–16).
In the context of TTH, affected individuals exhibit reduced neck mobility compared to individuals without headache. The progression from episodic to chronic TTH has been associated with shortened muscle length and weakened neck extensor muscles (17–21). On average, individuals with TTH as their primary headache, exhibit lower pressure pain thresholds in the pericranial region than those with migraine, as evidenced by both clinical and population-based studies (22–24). Furthermore, pericranial tenderness, quantified by the total tenderness score, is significantly higher in individuals with TTH compared to migraine sufferers and individuals without headache (25).
Validated and reliable instruments, such as the Neck Disability Index (NDI) for self-reported disability related to neck pain (26,27) and the Numeric Pain Rating Scale (NPRS) for assessing subjective pain levels on an 11-point numerical scale (28,29), can provide insights into the extent of disability caused by neck pain in individuals with migraine and TTH. To elucidate the influence of concurrent neck pain on individuals with migraine or TTH, we conducted the first systematic review and meta-analysis, focusing on the NDI and NPRS, among adult populations experiencing these disorders. This meta-analysis aimed to determine the pooled means of NDI and NPRS in individuals with these two primary headaches. In addition, we critically examined methodological aspects of the existing studies and proposed recommendations for future studies.
Methods
Data sources
This review was carried out following the reporting guideline of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (30). The study protocol was pre-registered in PROSPERO, the International Prospective Register of Systematic Reviews, under the registration number CRD42021271644. A comprehensive search was executed on PubMed and Embase for articles related to NDI and NPRS in individuals diagnosed with either migraine or TTH. The search was conducted on 1 August 2023, with the following search string: (migraine OR migraineurs OR tension type headache) AND (neck pain OR neck muscle pain OR neck stiffness OR neck symptoms OR neck complaints).
Study selection and data extraction
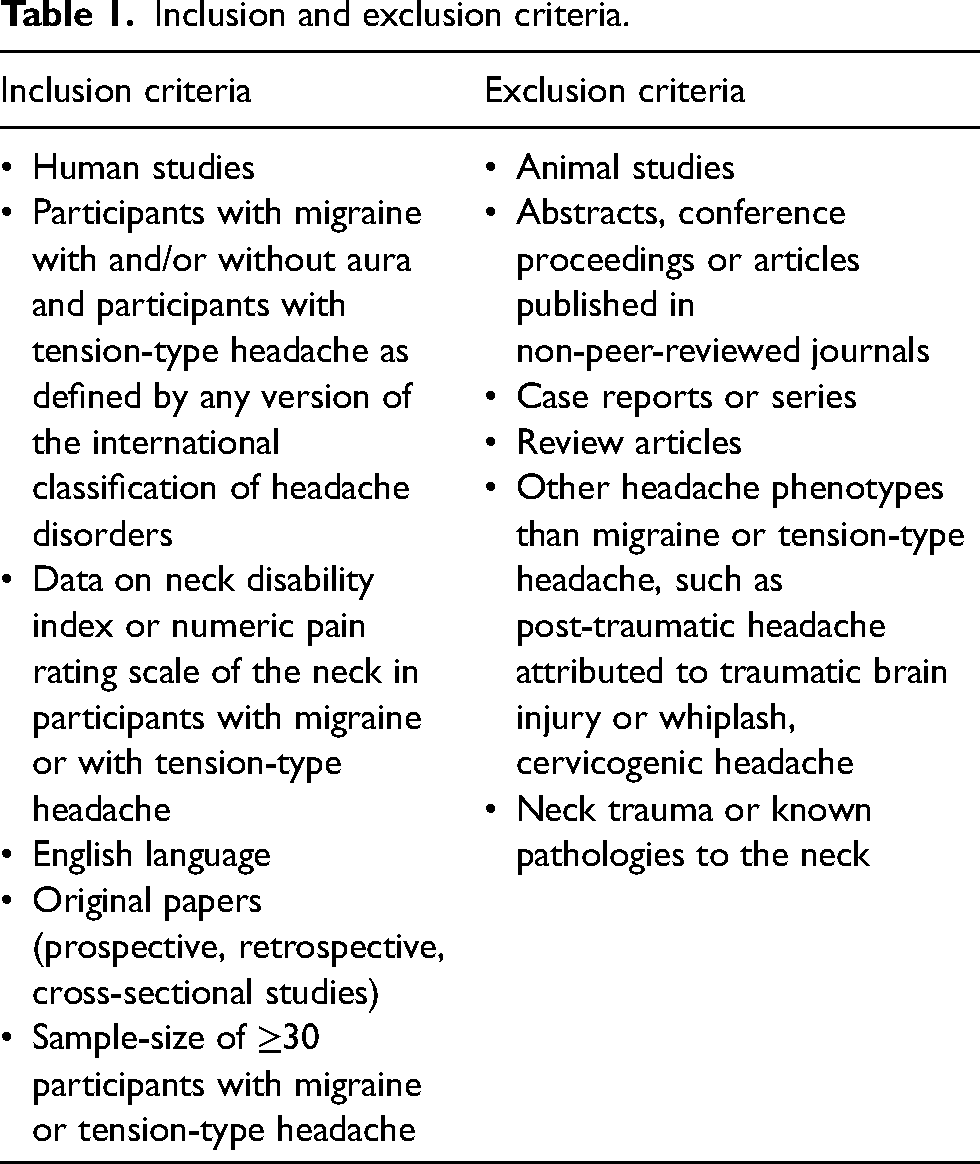
Two investigators (HMA and ZA) meticulously assessed all retrieved outcomes based on title and abstract. Full texts were procured for articles detailing patients diagnosed with either migraine or TTH and presumed to present pertinent neck pain data. Moreover, the reference lists of pertinent primary articles and reviews were also reviewed to identify any studies potentially overlooked in the primary selection process. Two investigators (HMA and ZA) independently evaluated full-text articles for eligibility, according to predefined criteria (Table 1). In cases of discrepancies, a third reviewer (SA) served as the final arbiter. From each article, HMA and ZA independently extracted information using a standardized summary form, encompassing details such as study design, gender distribution, age demographics, classification system employed for migraine and TTH, participant counts for each condition, the inclusion of healthy headache-free controls, and methodologies used for evaluating neck pain.
Inclusion and exclusion criteria.
Quality assessment
The quality assessment of all included studies was conducted independently by two evaluators (HMA and ZA), using the Joanna Briggs Institute (JBI) Critical Appraisal Tools designed for cross-sectional studies (31). In instances of discord, consensus was reached by the two evaluators (HMA and ZA), with potential intervention from a third evaluator (SY) if necessary. Full-text articles were reviewed for the following items: (i) clearly defined inclusion criteria; (ii) study subjects and setting; (iii) exposure measured validly/reliably; (iv) objective and standard criteria used for measurement of the condition; (v) confounding factors identified; (vi) strategies to deal with confounding factors; (vii) outcome measured validly/reliably; and (viii) use of appropriate statistical analysis. Responses to each item were categorized as “yes”, “no”, “unclear” or “not applicable.” Each study was attributed a quality assessment rating of “High”, “Moderate” or “Low.” A score of ≥ 7 was deemed as high quality, whereas scores ranging from 4 to 6 were considered moderate, and scores below 4 were designated as low quality.
Neck pain definition
In the current review, the definition of neck pain included instances where it coexisted or was associated with migraine or TTH. This approach was necessitated by the divergent definitions of neck pain across the array of studies under consideration.
Neck disability Index
NDI is a questionnaire consisting of 10 items designed to evaluate self-assessed disability in individuals with neck pain (26,27). The questionnaire covers 10 items in a range of aspects, including pain intensity, personal care, lifting, reading, headache, concentration, work, driving, sleeping and engaging in recreational activities. Each of these items in the questionnaire is rated on a scale from 0 to 5, where higher values signify increased disability, with a maximum cumulative score of 50 (26,27). The NDI score can be categorized as follows: 0–4 points denotes no disability, 5–14 points indicates mild disability, 15–24 points corresponds to moderate disability, 25–34 points signifies severe disability and a score of ≥ 35 points indicates complete disability (26,27). NDI is validated for use as both a continuous scoring and a categorical grading (26,27).
Numeric pain rating scale
The NPRS is used to quantify pain intensity through an 11-point numeric continuum (28,29). Individuals are prompted to assess their pain levels within a range from 0 (indicating an absence of pain) to 10 (representing the most extreme imaginable pain) (28,29).
Data synthesis and analysis
We conducted a descriptive meta-analysis of eligible clinical-based studies. Our primary outcomes included analyzing differences in NDI and NPRS means between individuals with migraine, TTH, and healthy headache-free controls, as well as between individuals with chronic and episodic migraine. Pooled means of NDI and NPRS were calculated by pooling study-specific estimates using random effect meta-analyses, which accommodated the heterogeneity across studies, with weighting based on the inverse variance method and estimation of parameters using the restricted maximum likelihood method. Secondary outcomes of significance included determining the pooled mean NDI scores in individuals with migraine and TTH. For subgroupings containing three or more study cohorts, a meta-analysis was conducted. The I2 statistic was used to assess inter-study heterogeneity. To evaluate potential publication bias in the included studies, both visual inspection of a funnel plot depicting SE against proportion effect size and Egger’s test were used, considering significance at p ≤ 0.05. All statistical analyses were executed utilizing Comprehensive Meta-Analysis software, version 3.0 (https://meta-analysis.com) and R, version 4.1.0 (R Foundation, Vienna, Austria) using the “meta” and “metafor” packages.
Results
In total, 3157 unique search hits were identified through the database search (Figure 1). No additional hits were found during a manual search of the reference lists from the included publications. One hundred and eight articles were retrieved and subjected to full assessment. There was substantial agreement among investigators (kappa = 0.8) for studies selected through title and abstract screening. Thirty-three eligible articles, published between 2010 and 2023, evaluated neck pain using NDI and NPRS in individuals with migraine and TTH (14,32–63). These 33 articles contributed data for both qualitative and quantitative synthesis (14,32–63). The data were exclusively obtained from clinic-based approaches because no population-based study utilized NDI or NPRS for assessing neck pain in headache populations.

Flow diagram. NDI = neck disability index; NPRS = numeric pain rating scale.
Study and participant characteristics
Data collection was prospective in all studies except for one study (53), and adherence to The International Classification of Headache Disorders (ICHD) criteria (64) was maintained across all studies. Among the 33 studies, 11 incorporated both male and female participants (32,38,40–42,44,45,51,60,62,63), whereas 13 incorporated a healthy headache-free control group (14,32,40,43–45,47,50,54,56,57,59,63). Specifically, seven studies compared the mean NDI data between migraine participants and non-headache controls (32,40,43–45,47,50), two studies compared the mean NDI data between TTH participants and healthy headache-free controls (50,63), and eight studies compared the mean NPRS data between migraine participants and healthy headache-free controls (14,32,43,44,54,56,57,59).
Only one study included both headache phenotypes and healthy headache-free controls (50). In this context, the chronic TTH group exhibited a higher NDI (mean score: 20.4 ± 8.1) compared to the chronic migraine group (mean score: 18.7 ± 9.0) and healthy headache-free controls (mean score: 1.6 ± 1.7) (50). Two studies included participants with migraine with aura (38,46), with one of them finding no difference in mean NDI between migraine participants with and without aura (t = −0.32, p = 0.250) (38). Few studies explored the factors associated with NDI or NPRS and neck impairment among headache groups. A positive association between the frequency of migraine attacks and NDI scores was observed in some studies (35,41), and neck pain-related disability was linked to an increased risk of developing chronic migraine (41). Lastly, one study identified a negative correlation between neck muscle strength and NDI for flexion, extension, and lateral flexion of the neck in women with migraine (37).
Migraine
Neck disability Index outcomes
We included 25 clinic-based studies that utilized NDI to evaluate neck pain in individuals with migraine. Among these, seven studies (involving a total of 578 migraine participants) reported the relative frequency of NDI severity categories, including none, mild, moderate and severe (33–37,39,45). A meta-analysis was conducted to determine the pooled relative frequency of these categories, yielding the following results: no NDI was reported by 23.0% (95% confidence interval (CI) = 18–30, I2 = 65%), mild NDI was reported by 45.3% (95% CI = 40–51, I2 = 41%), moderate NDI was reported by 25.0% (95% CI = 21–28, I2 = 9%) and severe NDI was reported by 6.7% (95% CI = 4–11, I2 = 46%).
Seventeen studies, encompassing 1389 migraine participants, provided reports on mean NDI values (32,37,38,40–53). The pooled mean NDI value for participants with migraine was calculated to be 16.2 (95% CI = 13.2–19.2, I2 = 99%) (Figure 2 and Table 2), which is indicative of moderate disability. A comparative analysis of mean NDI scores was conducted between participants with migraine (n = 474) and healthy headache-free controls (n = 271) in seven studies (32,40,43–45,47,50). The results indicated that the mean NDI was 12.1 (95% CI = 6.5–17.7, p < 0.001) scores higher among individuals with migraine compared to healthy headache-free controls (Figure 3; see also the supplementary material, Table S1). Six studies included both episodic (n = 371) and chronic (n = 185) participants with migraine (32,40,41,43,47,51). Within these studies, the mean NDI score was found to be highest among chronic migraine participants. The pooled data demonstrated that the mean NDI was 5.5 (95% CI = 4.11–6.8, p < 0.001) points higher among participants with chronic compared to episodic migraine (Figure 4; see also the supplementary material, Table S2).

Mean NDI scores in migraine. CI = confidence interval; MRAW = raw difference in means; NDI = neck disability index; No = number; SD = standard deviation. Pooled analysis of NDI scores in individuals with migraine.

Mean NDI scores among individuals with migraine and non-headache controls. CI = confidence interval; HC = non-headache controls; MD = mean difference; NDI = neck disability index; No = number; SD = standard deviation. Pooled analysis of NDI scores in individuals with migraine.

Mean NDI scores among individuals with episodic and chronic migraine. CI = confidence interval; CM = chronic migraine; EM = episodic migraine; MD = mean difference; NDI = neck disability index; No = number; SD = standard deviation. Pooled analysis of NDI scores in individuals with migraine.
Mean values of Neck Disability Index (NDI) in participants with migraine.

CM = chronic migraine; EM = episodic migraine; I2 = inconsistency; ICHD = International Classification of Headache Disorders; Migraine = not specified if migraine was episodic or chronic.
Numeric pain rating scale for neck pain outcomes
We incorporated 14 clinic-based studies utilizing the NPRS to assess the severity of neck pain in migraine participants (n = 948) (14,36,37,43–45,47,53,54,56–60). The meta-analysis yielded a mean NPRS score of 5.7 (95% CI = 5.1–6.2, I2 = 95%) across all studies (Table 3). In eight studies, a comparison of NRPS scores was conducted between participants with migraine and healthy headache-free controls (14,36,43,44,47,56,57,59). The pooled data indicated a 4 point higher mean NPRS score among individuals with migraine compared to healthy headache-free controls (4.1 (95% CI = 3.1–5.2, p < 0.001) (see supplementary material, Table S3). Additionally, seven studies explored the differences in NPRS scores between participants with episodic (n = 271) and chronic (n = 182) migraine (14,36,43,47,56,57,59). The meta-analysis revealed that the mean NRPS was 5.7 (95% CI = 4.7–6.6, p < 0.001) points higher in chronic compared to episodic participants with migraine (see supplementary material, Table S4).
Mean values of Numeric Pain Rating Scale (NPRS) in participants with migraine.

CM = chronic migraine; EM = episodic migraine; I2 = inconsistency; ICHD = International Classification of Headache Disorders; Migraine = not specified if migraine was episodic or chronic.
Tension-type headache
Neck disability Index outcomes
We included four clinic-based studies employing NDI to assess neck impairment in participants with TTH (n = 210) (50,61–63). The pooled data revealed a mean NDI score of 13.7 (95% CI = 4.9–22.4, I2 = 99%) (Table 4), suggesting mild disability. Among these studies, two included healthy headache-free controls (50,63). In one observational study involving 31 participants with chronic TTH and 31 healthy headache-free controls, the mean NDI scores were 20.4 ± 8.1 for those with chronic TTH and 1.6 ± 1.7 for healthy headache-free controls (50). Another study included TTH group with both episodic and chronic TTH, along with healthy headache-free controls, and reported the highest NDI scores in the TTH group (mean NDI: 7.1 ± 4.4 vs. 2.0 ± 2.7) (63). Notably, none of the studies investigated differences in NDI between participants with episodic and chronic TTH. Owing to the scarcity of studies (fewer than 3), we refrained from conducting a meta-analysis on the comparison between TTH and healthy headache-free controls, as well as between episodic and chronic TTH.
Mean values of Neck Disability Index (NDI) in participants with tension-type headache.

CI = confidence interval; ICHD = International Classification of Headache Disorders; CTTH = chronic tension-type headache; ETTH = episodic tension-type headache; I2 = Inconsistency; TTH = Not specified if tension-type headache was episodic or chronic.
Numeric pain rating scale of neck pain outcomes
Two studies utilized NPRS to evaluate neck pain intensity in participants with TTH (n = 103) (62,63). Meta-analysis was not conducted for NPRS in these studies due to the limited number of available studies. Both studies included participants with both episodic and chronic TTH. The mean NPRS scores among TTH participants were reported as 2.6 ± 1.9 in one study (62) and 3.1 ± 1.7 in the other study (63). None of these studies investigated differences in NPRS between participants with episodic and chronic TTH or compared to healthy headache-free controls.
Study assessment
The evaluation of each study incorporated in this analysis utilized the JBI assessment criteria for cross-sectional studies. Notably, none of the studies were rated as low quality, with eight studies being classified as moderate quality (36,47,53,56–58,62,63). The remaining 25 studies demonstrated high quality (14,22,32–36,48–50,53,56,59,60), as outlined in the supplemental material (Table S5).
Discussion
To our knowledge, this is the first systematic review and meta-analysis comparing NDI and NPRS scores among individuals with migraine and TTH. Our findings indicate that individuals with migraine demonstrate the highest level of neck pain-related disability, with a mean score of 16.2 (signifying moderate disability), surpassing those with TTH, with a mean sore of 13.7 (indicative of mild disability). This observation highlights the substantial contribution of neck discomfort to the overall disability experienced by individuals with migraine and, to a lesser extent, those with TTH.
We found that the mean NDI score was approximately 12 points higher in participants with migraine compared to healthy headache-free controls. Although a formal meta-analysis comparing individuals with TTH and healthy headache-free controls was not performed, we observed tendency of higher NDI scores among individuals with TTH (NDI score 7.1 ± 4.4 to 20.4 ± 8.1) compared to healthy headache-free controls (NDI score 1.6 ± 1.7 to 2.0 ± 2.7). Moreover, we found an association between neck pain-related disability and the frequency of migraine attacks. When restricting the NDI analysis to participants with episodic and chronic migraine, the pooled results indicated an approximately 5 point higher NDI score in the chronic migraine group. This study affirms that individuals with chronic migraine are more likely to suffer from neck pain-related disability than those with episodic migraine.
Neck pain and headache linkage
The pathophysiological mechanisms underlying relationship of migraine, TTH and neck pain can be explained by the proposed role of the trigeminocervical complex (16). This complex receives nociceptive inputs from the trigeminal nerves and upper cervical roots (65–67). This hypothesis is substantiated by various lines of evidence. Nociceptive input from pericranial muscles and the dura mater can activate the trigeminocervical complex (65–67). Specifically, sensory neurons of the dorsal root ganglion at C1–C3 have been observed to traverse the bony canal and large foramens of the skull to innervate pericranial muscles and the dura (68–71). This connection suggests that stimulation of posterior dural nociceptors intracranially may precipitate the onset of both headache and neck pain, whereas the occurrence of neck pain following the onset of headache might be attributed to central sensitization (25,68,72). Hence, this convergence impute implies that neck pain has the potential to stimulate central trigeminal pathways in a manner analogous to peripheral trigeminal input (73), and neck pain may decrease the pain threshold via both peripheral and central mechanisms in individuals experiencing migraine and TTH (74). Furthermore, cervical musculoskeletal impairments may interact with both migraine and TTH via the trigeminocervical complex (16). Nociception from cervical musculoskeletal impairments could possibly intensify symptoms during these headache episodes or trigger them by promoting trigeminocervical sensitization, which activates central pathways. Finally, both central and peripheral theories have been proposed to explain the neck pain headache linkage (75). For example, in the context of neck pain and migraine, higher headache frequency and a greater presence of premonitory symptoms are suggested to be driven by a central mechanism, whereas reduced active cervical range of motion and increased cervical hyperalgesia are thought to be driven by a peripheral mechanism (75).
Methodological considerations
Formulating definitive conclusions from our results is challenging because of the substantial heterogeneity observed across the studies (I2 = 99%) and their general methodological limitations. These limitations could arise from many factors summarized below. First, none of the studies utilized a neck pain diary for assessing neck pain. Second, only 11 out of the 33 included studies featured both genders, with a notable preponderance of female participants in these studies (32,38,40–42,44,45,51,60,62,63), It is noteworthy that being female has been reported to be associated with an increased risk of cutaneous allodynia in patients with migraine (76,77). A recently published cross-sectional study supported this observation by revealing a higher prevalence of cutaneous allodynia, a fourfold increased risk of severe cutaneous allodynia and an elevated prevalence of self-reported neck pain in females with migraine compared to males with migraine (39). This methodological issue may potentially also contribute an overestimation of our results, given lower thresholds for reporting neck pain in women. Third, the co-occurrence of TTH in individuals with migraine was not explored, potentially leading to underreported TTH data which could affect the neck pain scores. It is improbable that none of the studies featured episodic migraine participants with TTH, given their common cooccurrence (64). Moreover, it is conceivable that certain participants diagnosed with migraine and TTH may also have an undiagnosed comorbid cervicogenic headache disorder, given the association between cervical pathology and cervicogenic headache (78). Fourth, a lack of consensus on a clear definition of neck pain is evident in the literature. Although Liang et al. (51) provided a definition in their study, specifying neck pain as “any pain from the suboccipital region to the cervicothoracic junction and had to be either current or present within the past month”, this definition lacks specificity because it does not include reasonable cut-off scores for neck pain intensity or required days with neck pain. Thus, participants reporting a single day with mild neck pain within the past month, which might be considered within the normal range, would be included by this broad definition. Fifth, information pertaining to NDI and NPRS for neck pain most often relied on self-reported measures. However, in other studies, these assessments were determined through a clinical interview and subsequent examination, potentially introducing variability in data collection methods, and increasing the risk of heterogeneity among studies. Sixth, despite NDI being a recognized tool for assessing neck pain, it possesses certain limitations. NDI it is not specific to neck pain because it includes items addressing sleep disorders and headache. Therefore, in individuals experiencing both neck pain and migraine or TTH, isolating the specific influence of each condition on the total NDI score becomes challenging. Moreover, in disorders with variable and heterogenous presentations such as migraine and TTH, patient self-report of NDI and NPRS scores may vary within and outside the headache phase of an attack. Seventh, the NPRS as a screening tool can be insufficient for capturing neck pain disability, but it is currently one of the few available assessments for neck pain. Lastly, our systematic review did not identify any eligible population-based studies examining NDI and NPRS in migraine or TTH populations. By contrast, all included studies were clinic-based, enrolling participants from headache clinics. This approach limits the generalizability of our findings because clinic-based populations may represent more severe cases compared to the general population.
Clinical implications and future directions
The present systematic review and meta-analysis highlight that individuals with migraine exhibit the highest NDI and NPRS outcomes, followed by those with TTH and healthy headache-free controls. Although our findings require careful interpretation, they have substantial importance. Implementation of NDI and NPRS in clinical settings to assess neck pain severity and disability in patients with primary headache such as migraine and TTH may be beneficial. Moreover, both current clinical practice and prospective research would benefit from using a neck-headache diary to explore the temporal relationship between neck pain onset and headache episodes, enhancing our understanding of neck discomfort in migraine and TTH contexts.
Future research should address the methodological limitations outlined herein. Population-based studies incorporating NDI and NPRS are imperative to offer broader insights into neck pain disability among individuals with migraine and TTH. In addition, more refined prospective studies are needed to provide better estimations of NDI and NPRS before, during and after headache episodes. These recommendations will help elucidate potential fluctuations in neck pain intensity throughout the premonitory, migraine, and postdromal phases of a migraine attack.
The potential co-occurrence of TTH in migraine cases warrants investigation because its oversight may skew reported data. It would also be interesting for future studies to perform subgroup analyses between individuals with a history of overlapping chronic pain syndromes (e.g. fibromyalgia) and migraine/TTH.
Establishing an international consensus on a standardized definition of neck pain is vital for both research and clinical purposes. Such standardization will significantly reduce heterogeneity across studies, facilitating more accurate comparative analyses. In addition, a systematic approach to recording study-level characteristics is crucial. Potentially, the establishment of such a consensus might help identify headache treatments with concomitant effects on neck pain, or treatments that might be especially beneficial to patients with a cervical component contributing to their headaches.
Finally, several potential pain sources may originate in the cervical region. Rigorous examinations, including advanced imaging techniques and occasional diagnostic blocks guided by imaging, are essential for the most accurate diagnosis of the origin of neck pain. Employing these methods could help determine whether neck pain is merely coincidental with migraine and TTH, or if it is indeed an integral component of the primary headache process. However, the implementation of these evaluation methods may be challenging for headache specialists. Alternatively, individuals with neck pain could be referred to physiotherapists who are expert in headache disorder assessment and management. It is worth mentioning that manual assessment has proved similar diagnostic accuracy as radiological interventions (79). Therefore, multidisciplinary collaboration between physicians and physiotherapists could be a cost-effective and more accessible solution.
In conclusion, although our systematic review and meta-analysis suggests that the NDI and NPRS of neck pain are valuable for health professionals, it is important to acknowledge their limitations. Addressing these methodological challenges in future research is essential to advance our understanding of the progression and interrelation of neck pain and headache disorders.
Our systematic review and meta-analysis reveal that individuals with migraine exhibit the highest level of neck pain-related disability, with an average score of 16.2 (indicating moderate disability). This surpasses the score of those with tension-type headache (TTH), who have an average score of 13.7 (indicating mild disability). Individuals with migraine also reported more intense neck pain compared to those healthy individuals without headache and those with TTH. This highlights the significant impact of neck discomfort on the overall disability experienced by people with migraine and, to a lesser extent, by those with TTH. We only found one cross-sectional study comprising individuals with migraine, individuals with TTH and healthy individuals. The pooled results of this meta-analysis align with that comparative cross-sectional study It is important for healthcare providers to use the NDI and NPRS in their clinical work to understand how much neck pain affects individuals with migraine and TTH. These tools can help assess the impact of neck pain and provide information about how treatments are working.
Supplemental Material
sj-docx-1-cep-10.1177_03331024241274266 - Supplemental material for Systematic review and meta-analysis of Neck Disability Index and Numeric Pain Rating Scale in patients with migraine and tension-type headache
Supplemental material, sj-docx-1-cep-10.1177_03331024241274266 for Systematic review and meta-analysis of Neck Disability Index and Numeric Pain Rating Scale in patients with migraine and tension-type headache by Haidar M. Al-Khazali, Zainab Al-Sayegh, Samaira Younis, Rune H. Christensen, Messoud Ashina, Henrik W. Schytz and Sait Ashina in Cephalalgia
Footnotes
Author contributions
HMA and SA conceived and designed (including search strategies) the review. HMA and ZA performed the literature search. HMA wrote the first and subsequent drafts of the manuscript. SY, HWS, ZA, RHC, MA and SA participated in critical revisions and the writing of the article. All authors hread approved the final version of the manuscript submitted for publication.
Data availability
Upon reasonable request, the corresponding author will provide the necessary data and materials to interested researchers for the purpose of academic scrutiny, reproducibility and further scientific investigation.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HMA reports personal fees from Pfizer and Lundbeck, outside of the submitted work. HS reports receiving personal fees from AbbVie, Teva, Lundbeck, Novartis and Eli Lilly outside of the submitted work. MA reports receiving personal fees from AbbVie, Amgen, Astra Zeneca, Eli Lilly, GlaxoSmithKline, Lundbeck, Novartis, Pfizer and Teva Pharmaceuticals outside of the submitted work. MA also serves as an associate editor of Cephalalgia, The Journal of Headache and Pain and Brain. SA has received honoraria for consulting from Allergan/AbbVie, Eli Lilly, Impel NeuroPharma, Linpharma, Lundbeck, Pfizer, Satsuma, Teva and Theranica. SA is an Associate Editor for Neurology Reviews, BMC Neurology and Frontiers in Neurology; serves on the Advisory Board for Journal of Headache and Pain; and is a member of Education Committee of the International Headache Society. The other authors declare that they have no conflicts of interest.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.