
Abstract
Background
To synthesize the available epidemiologic data on short-lasting unilateral neuralgiform headache attacks (SUNHA). This, in turn, might inform diagnostic work-up and clinical decision-making.
Methods
EMBASE and PubMed were searched for observational studies reporting on the prevalence or relative frequency of SUNHA or its individual clinical features. Two investigators independently conducted title and abstract screening, full-text review, data extraction, and risk of bias assessment, and random-effects meta-analyses were performed to estimate the prevalence or relative frequency of SUNHA and its individual clinical features.
Results
Fifteen clinic-based studies met our eligibility criteria. Of these, five studies reported estimates on the relative frequency of SUNHA among adults evaluated for headache or facial pain, yielding a pooled relative frequency as 0.32% (95% confidence interval = 0.17–0.62; I2 = 89.9%). Most often, SUNHA presented as episodic, side-locked stabbing headache of severe pain intensity, predominantly affecting the ophthalmic and/or maxillary branch of the trigeminal nerve. The most common cranial autonomic features were lacrimation, conjunctival injection, rhinorrhea and nasal congestion.
Conclusions
SUNHA is a rare headache disorder with distinct clinical features. However, our findings must be interpreted with caution as a result of between-study heterogeneity and lack of population-based studies, underscoring the need for further epidemiologic research.
Introduction
Trigeminal autonomic cephalalgias (TACs) are characterized by unilateral headache and cranial autonomic features ipsilateral to the pain (1). Among them, short-lasting unilateral neuralgiform headache attacks (SUNHA) represent rare and enigmatic disease entities (1). Their clinical manifestation involves recurrent attacks of unilateral headache accompanied by cranial autonomic features, such as conjunctival injection and lacrimation (i.e. tearing) (1). The attacks last seconds to minutes and occur as a single stab, a series of stabs or in a saw-tooth pattern at least once daily, and manifest in an either episodic or chronic headache pattern (1). Despite the profound impact, SUNHA attacks remains among the least understood TACs.
From a research standpoint, efforts to map the epidemiologic patterns and clinical features of SUNHA have been limited because of its low prevalence, a challenge common to other TACs (2,3). The notable exception within this group is cluster headache, which has been more extensively studied (4). Consequently, much of our current understanding of SUNHA remains based on case reports and small observational studies. This limitation not only impedes a comprehensive disease understanding, but also hinders disease recognition and the development of evidence-based management strategies. Therefore, a synthesis of the available evidence on the epidemiology and clinical features is warranted to guide clinical practices and outline directions for future research.
In this systematic review and meta-analysis, we aimed to estimate the prevalence of SUNHA in the adult general population and its relative frequency among adult patients evaluated for headache or facial pain in clinical settings. We also assessed clinical symptoms and signs in those with SUNHA, quantifying the relative frequency or pooled mean of each distinct feature.
Methods
A research protocol was developed for this systematic review and meta-analysis (PROSPERO identifier: CRD42024512228). The protocol adhered with the reporting guidelines for Meta-analysis of Observational Studies in Epidemiology (MOOSE) (5).
Classification
The International Classification of Headache Disorders (ICHD) has evolved over the years (1,6–8), providing diagnostic criteria for various headache disorders and facial pain. The ICHD-2, published in 2004 (7), formally recognized short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) as a distinct entity within the TAC category. However, short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) still awaited formal recognition, with proposed diagnostic criteria listed in the ICHD-2 Appendix.
The subsequent ICHD-3β edition, published in 2013 (8), formally introduced SUNA into the classification and provided refinements to the diagnostic criteria for SUNCT. Both disorders were classified as subtypes of SUNHA within the TAC category. The ICHD-3, published in 2018 (1), further refined the diagnostic criteria for SUNHA, offering more detail on attack frequency, duration, location, pain characteristics and the specific cranial autonomic features required for diagnosis.
Terminology
To achieve clarity and precision in our reporting, we adopt specific terms that reflect the nature and source of the data analyzed. When describing observational data derived from population-based studies, we use the term “prevalence”. This term is chosen to accurately describe the proportion of cases with SUNHA in the adult general population. Conversely, when we refer to observational data derived from clinic-based studies, we use the term “relative frequency”. This term denotes the proportion of cases with SUNHA among adult patients evaluated for headache or facial pain in clinical settings.
Search strategy
A systematic search was performed in the PubMed and EMBASE databases for observational studies reporting on SUNHA in adults. The search was carried out without language restrictions, from 1 January 2004 to 1 March 2024. The search string for EMBASE was as follows: “SUNCT*.mp. OR SUNA*.mp. OR SUNHA*.mp. OR trigeminal autonomic cephalalgias*.mp.”. For PubMed, we used the search string: “SUNCT”[all fields] OR “SUNA”[all fields] OR “SUNHA”[all fields] OR “trigeminal autonomic cephalalgia”[all fields]” This search string was used in combination with the MeSH terms: SUNCT Syndrome”[MeSH], “Trigeminal Autonomic Cephalalgias”[MeSH]”. In addition to this, we hand-searched the reference lists of included observational studies, as well as relevant systematic and narrative reviews. We also contacted the corresponding authors of the relevant investigations to supplement incomplete reports.
Selection criteria
The full list of eligibility criteria is outlined in Table 1. We included observational studies, either population- or clinic-based, reporting original data on the prevalence or relative frequency of SUNHA or its clinical features in adults (≥18 years of age). We permitted inclusion of studies with participants <18 years of age, contingent upon the participants’ mean ± SD age affirming a predominant adult population. We also required that participants had to have a diagnosis in adherence with either ICHD-2, ICHD-3β or ICHD-3 (1,7,8). Moreover, for studies reporting on the prevalence or relative frequency of distinct clinical features, we required a minimum sample size of five participants.
Inclusion and exclusion criteria.

ICHD = International Classification of Headache Disorders; SUNHA = short-lasting unilateral neuralgiform headache attacks.
Study selection and data extraction
Two investigators (JGL and MJH) independently screened titles and abstracts, performed full-text reviews, and identified articles eligible for inclusion. Any disagreements were resolved through consensus or referral to a third investigator (WKK, RHC or HMA). A standardized data extraction form was used to collect the following information from studies that were eligible for inclusion: study author, year of publication, study design, country, inclusion criteria, exclusion criteria, ICHD criteria used to diagnose SUNHA, the total number of participants and the number of patients with SUNHA. From these patients, the following additional data were extracted: age at onset, sex, periodicity, chronicity, the laterality, location, intensity, character, duration, frequency and triggering of attacks. The relative frequency of restlessness/agitation and cranial autonomic features, including lacrimation, conjunctival injection, rhinorrhea, nasal congestion, facial sweating, ptosis, miosis and eyelid edema, was also extracted, as well as migraine-related features such as phonophobia, photophobia, nausea and vomiting.
Quality assessment
To assess the methodological quality and determine the extent of bias in design, conduct, and analysis, two investigators (JGL and MJH) independently screened eligible studies using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Studies Reporting Prevalence Data (9). This instrument contains nine questions, each of which has the standardized options: “yes”, “no”, “unclear” and “not applicable”. Studies were categorized according to the percentage of answers with “yes” as high risk (≤49%), moderate risk (50–69%) or low risk of bias (≥70%).
Data synthesis and analysis
The primary outcomes were the estimated pooled prevalence of SUNHA in the adult general population and the pooled relative frequency among adult patients evaluated for headache or facial pain in clinical settings. The secondary outcome was the individual prevalence, relative frequency or pooled mean of SUNCT and SUNA and their demographic and clinical features in eligible population- or clinic-based studies. The results were extracted using a pre-defined data extraction form and, if two or more studies reported relevant data, a random-effects meta-analysis was conducted using a random intercept logistic regression model on log-transformed data. To calculate between-study variance, the maximum likelihood method was used, whereas the normal approximation method was used to calculate confidence intervals. A between-study heterogeneity of ≥75%, using the I2 statistic, was interpreted as considerable heterogeneity. Meta-regression was performed to explore causes of heterogeneity if 10 or more studies reported on the same outcome (10). All statistical analyses were performed with the R, version 4.2.0 (R Foundation, Vienna, Austria) using the “meta” and “metafor” packages.
Results
From 1883 records identified, 121 articles were retrieved for full-text review. Of these, 15 unique studies were eligible for inclusion and provided data for at least one meta-analysis (Figure 1) (11–25). In two studies (19,20), individual patient data were accessible and certain patients were excluded for not meeting our eligibility criteria, leading to data extraction from the qualified subset. An additional four articles were considered possibly relevant, requiring further clarification to ascertain their eligibility (26–29). Attempts were made to contact the respective authors for additional information; however, all of them either did not respond or declined our request, necessitating the exclusion of these studies. Of note, no population-based studies met the eligibility criteria, meaning that all reported findings are derived from clinic-based studies of adults who were evaluated for headache or facial pain.

Literature search flow diagram.
Table 2 presents the characteristics of the included studies. Notably, nine clinic-based studies reported on the relative frequency of SUNHA (11–19), some of whom also reported on its clinical features (18,19). The remaining clinic-based studies reported exclusively on the individual clinical features of SUNHA (20–25). In terms of design, seven of 15 studies were retrospective (15–19,21,22), two were cross-sectional (11,23) and six were prospective (12–14,20,24,25). All included studies were carried out in either secondary (n = 5) or tertiary care units (n = 10). The secondary care units were all neurologic clinics (13,14,16,20,21), whereas the tertiary care units were primarily headache clinics (11,12,15,17–19,22–25). The risk of bias assessment revealed that six included studies had a high risk (11,12,16–18,20), whereas nine had a moderate risk (13–15,19,21–25), as shown in the supplementary material, Tables S1 and S2.
Characteristics of clinic-based, observational studies reporting on SUNHA in adult patients.
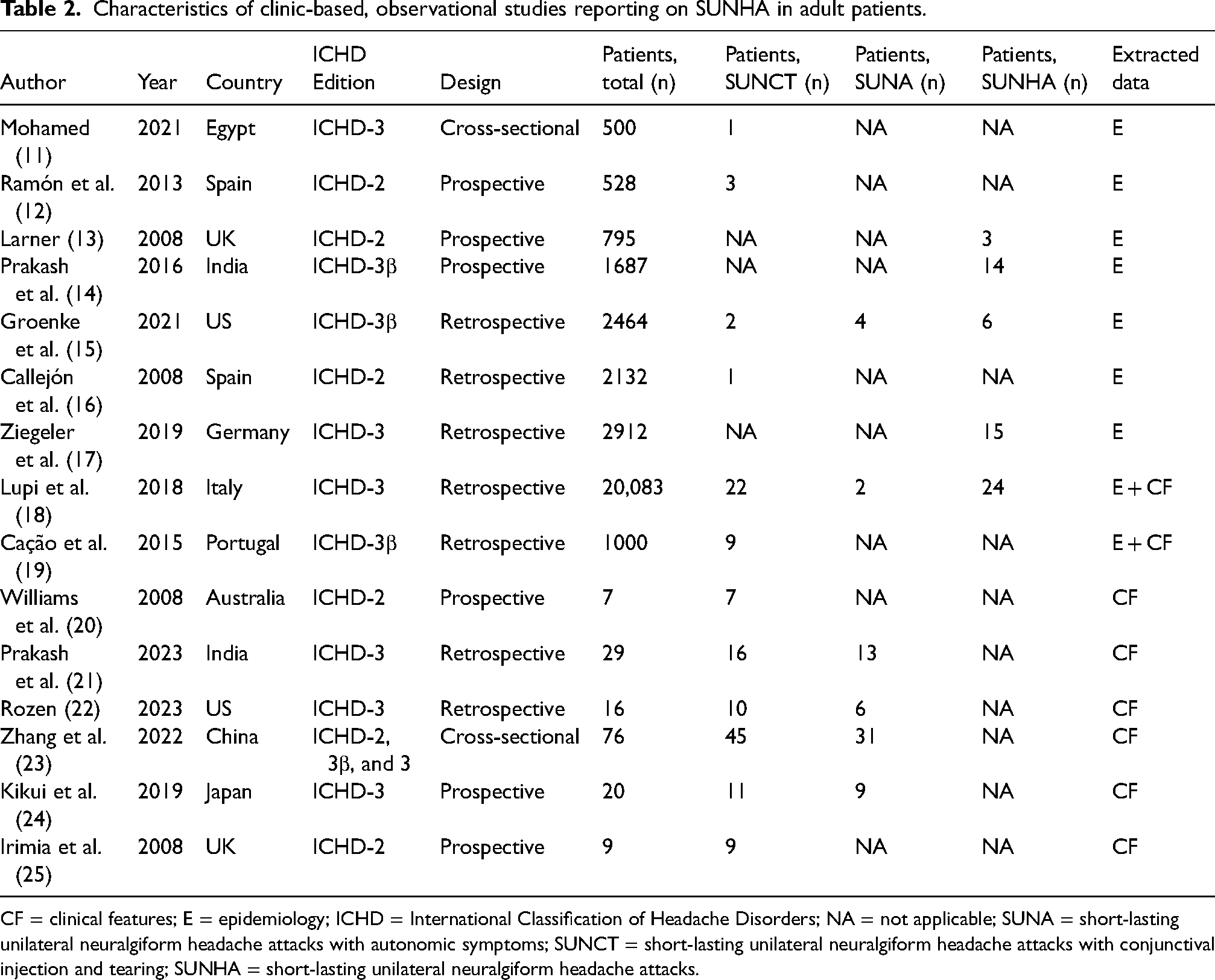
CF = clinical features; E = epidemiology; ICHD = International Classification of Headache Disorders; NA = not applicable; SUNA = short-lasting unilateral neuralgiform headache attacks with autonomic symptoms; SUNCT = short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNHA = short-lasting unilateral neuralgiform headache attacks.
The relative frequency of SUNHA
Five clinic-based studies, comprising 27,941 participants, reported on the relative frequency of SUNHA, identifying 62 cases (13–15,17,18). A random-effects meta-analysis estimated the pooled relative frequency as 0.32% (95% confidence interval (CI) = 0.17–0.62; I2 = 89.9%) (Figure 2a). The corresponding pooled relative frequency of SUNCT was estimated as 0.18% (95% CI = 0.07–0.45; I2 = 85.9%) (Figure 2b) based on data from six studies (11,12,15,16,18,19). Furthermore, the pooled relative frequency of SUNA was estimated as 0.04% (95% CI = 0.01–0.27; I2 = 90.4%) (Figure 2c) based on data from two studies (15,18).

(a) pooled relative frequency of SUNHA in observational, clinic-based studies of adult patients with headache or facial pain. (b) Pooled relative frequency of SUNCT in observational, clinic-based studies of adult patients with headache or facial pain. (c) Pooled relative frequency of SUNA in observational, clinic-based studies of adult patients with headache or facial pain. CI = confidence interval; SA = SUNA; ss = SUNHA; SU = SUNCT.
Age of onset and sex
Data on age at onset and sex were available in 98 patients with SUNCT from six studies (19–24) and from 59 patients with SUNA from four studies (21–24). The pooled mean age at onset was 46 years (95% CI = 39–54; I2 = 79%) for SUNCT and 42 years (95% CI = 39–45; I2 = 0%) for SUNA. Moreover, females accounted for 51% of the SUNCT cases (95% CI = 41–61; I2 = 0%) and 58% of the SUNA cases (95% CI = 45–70; I2 = 10%).
Periodicity and chronicity
Five studies involving 65 patients with SUNCT and three studies with 24 patients with SUNA reported on the presence of episodic versus chronic headache (18,20,21,24,25). The findings revealed that 86% of patients with SUNCT (95% CI = 25–99; I2 = 63.5%) and 68% of patients with SUNA (95% CI = 6–99; I2 = 0%) experienced episodic headache. None of the included studies reported on the frequency or duration of bouts.
Laterality and location of attacks
Almost all attacks were reported to be side-locked in both patients with SUNCT (98%, 95% CI = 92–99, I2 = 0%) and those with SUNA (94%, 95% CI = 84–98, I2 = 0%). These estimates were derived from six studies on SUNCT, comprising 97 patients, and three studies on SUNA, involving 53 patients. The specific location of these attacks was documented in a subset of included studies but varied considerably in reporting (19,21,23). To provide a comprehensive overview, the largest study was selected to present the data, comprising 45 patients with SUNCT and 31 patients with SUNA (23). The pain was most often localized to the ophthalmic (64%) and maxillary (60%) branches of the trigeminal nerve, whereas pain localized to the mandibular branch (4%) or within the C2–C3 dermatomes (29%) was less common. In patients with SUNA, 84% experienced pain localized to the ophthalmic branch, 32% in the maxillary branch, 6% in the mandibular branch and 35% within the C2–C3 dermatomes.
Pain intensity and pattern
Three studies, comprising 70 patients, reported on the usual pain intensity of SUNCT attacks (19,21,23), revealing that 89% (95% CI = 79–94; I2 = 0%) experienced pain of severe intensity, whereas 11% (95% CI = 6–21; I2 = 0%) reported pain of moderate intensity. Similarly, two studies, comprising 44 patients, provided data on the usual pain intensity of SUNA attacks (21,23), revealing that pain was of severe intensity in 84% (95% CI = 70–92; I2 = 0%) and of moderate intensity in 14% (95% CI = 6–27; I2 = 0%). Moreover, two studies comprising 23 patients with SUNCT (20,21) and one study involving 13 patients with SUNA (21) reported information on the patterns of pain during attacks. In patients with SUNCT, 54% (95% CI = 6–95; I2 = 87.6%) experienced episodes with single stabs, 70% (95% CI = 48–85; I2 = 0%) reported attacks with repetitive stabs and 26% (95% CI = 12–47; I2 = 0%) described a saw-tooth pattern. In patients with SUNA, all had experienced attacks with single stabs, 77% described repetitive stabs and 23% reported a saw-tooth pattern.
Duration and frequency
Two studies on SUNCT, comprising 20 patients (19,24), reported on the attack duration, yielding a pooled duration of 68 s (95% CI = 10–126; I2 = 82.5%). For SUNA, data were available from one clinic-based study, involving nine patients, in which the mean attack duration was reported to be 96 seconds (24). The same study also detailed the attack frequency in both disorders: 11 patients with SUNCT experienced an average of 75 daily attacks, whereas nine patients with SUNA had an average of 19 daily attacks.
Trigger factors
Several studies reported various factors that can trigger attacks in patients with SUNCT or SUNA (21,23,24). Notably, common triggers of migraine (e.g. bright lights, strong odors, alcohol) were rarely reported by patients with SUNCT or SUNA (21,23). The most prevalent trigger was cutaneous or intraoral stimulation, affecting 64% of SUNCT patients (95% CI = 53–73; I2 = 0%) and 47% of SUNA patients (95% CI = 34–60; I2 = 0%). Further details on different trigger factors are provided in the supplementary material, Table S3. In addition, two studies highlighted the presence of a refractory period after a triggered attack (23,24), which was observed in 9% of SUNCT patients (95% CI = 3–23; I2 = 37.8%) and 10% of SUNA patients (95% CI = 3–32; I2 = 0%).
Cranial autonomic features and restlessness/agitation
Data from five studies comprising 91 patients with SUNCT (19,21–24) and four studies involving 59 patients with SUNA (21–24) provided data on cranial autonomic features. Given that lacrimation and conjunctival injection are diagnostic requirements for SUNCT, these symptoms were necessarily present in all SUNCT cases. In patients with SUNA, lacrimation was reported by 73% (95% CI = 37–93; I2 = 81.3%), whereas conjunctival injection was described by 19% (95% CI = 7–43; I2 = 65.1%). Additional common cranial autonomic features are detailed in Table 3. Furthermore, a sense of restlessness/agitation was experienced by 59% (95% CI = 20–89; I2 = 67.9%) of patients with SUNCT (n = 80) and by 43% (95% CI = 26–62; I2 = 39.4%) of patients with SUNA (n = 50).
Cranial autonomic features in adult patients with SUNHA.

Because lacrimation and conjunctival injection are part of the SUNCT criteria, all SUNCT patients experienced both features. CI = confidence interval; I2 = measure of heterogeneity; NA = not applicable; SUNA = short-lasting unilateral neuralgiform headache attacks with autonomic symptoms; SUNCT = short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNHA = short-lasting unilateral neuralgiform headache attacks.
Migraine-related accompanying symptoms
The presence of ≥1 migraine-related associated symptom was reported by 29% (95% CI = 13–54; I2 = 51%) of patients with SUNCT and 47% (95% CI = 24–71; I2 = 35%) of patients with SUNA. Three studies reported on the presence of phonophobia and photophobia among patients with SUNCT (23–25), whereas two studies did so for patients with SUNA (23,24). The pooled relative frequency of phonophobia was 22% (95% CI = 13–33; I2 = 0%) in patients with SUNCT and 18% (95% CI = 9–32; I2 = 0%) in those with SUNA. For photophobia, the corresponding estimates were 15% (95% CI = 3–56; I2 = 70.7%) in SUNCT and 10% (95%, CI = 4–24; I2 = 0%) in SUNA. Moreover, one study reported data on the presence of nausea (23), which was noted during attacks in 24% of patients with SUNCT (n = 45) and 13% of patients with SUNA (n = 31). The same study also described that vomiting occurred in 13% of patients with SUNCT and 6% of patients with SUNA.
Discussion
To our knowledge, this is the first systematic review and meta-analysis on the epidemiology and clinical features of SUNHA. The pooled relative frequency was estimated as 0.32% among adults evaluated for headache or facial pain in clinical settings. The corresponding pooled relative frequencies were 0.18% for SUNCT and 0.04% for SUNA. The prevalence of SUNHA in the adult general population could not be estimated because none of the identified population-based studies investigating this met our eligibility criteria.
From a clinical standpoint, SUNCT and SUNA share considerable similarities. Both disorders commonly manifest in the fifth decade of life and exhibit an approximately equal sex distribution, with a slight female predominance in patients with SUNA. The headache pattern is most often episodic, with the pain being side-locked and of severe intensity. Furthermore, the pain is often of stabbing quality and is usually localized to the ophthalmic and maxillary branches of the trigeminal nerve in both disorders. In addition, attacks in both SUNCT and SUNA can frequently be triggered, with only a minority of patients reporting a refractory period after attacks. Of interest, ICHD-3 distinguishes between the two disorders exclusively based on the required presence of lacrimation and conjunctival injection in SUNCT (1), whereas patients with SUNA can experience either or neither of these symptoms. Recent findings from an open-label trial suggest that the treatment response to specific anticonvulsants is similar among patients diagnosed with either disorder (30). Thus, it is prudent for the next International Headache Classification Committee to unify SUNCT and SUNA into a single diagnostic entity (i.e. SUNHA).
Differential diagnoses
Trigeminal neuralgia constitutes the main differential diagnosis to SUNHA and has an estimated one -year prevalence of 0.5–1% (31). The clinical presentation of trigeminal neuralgia is characterized by recurrent attacks of severe pain within the distribution of one or more divisions of the trigeminal nerve. These unilateral attacks, triggered by innocuous stimuli, last up to two minutes, usually involves the maxillary and/or mandibular divisions, and mild cranial autonomic features are present in some patients (1,32–34). The clinical parallels between SUNHA and trigeminal neuralgia raise questions regarding their classification as distinct entities. Our findings, however, suggest that some differences do exist. For example, about one-third of patients with SUNHA experience pain outside of the trigeminal distribution. Furthermore, SUNHA attacks are often localized to the ophthalmic division of the trigeminal nerve, and not all patients report triggered attacks. However, spontaneous attacks have also been described in trigeminal neuralgia (33) and patients with involvement of the ophthalmic division often exhibit more pronounced cranial autonomic features (33). Moreover, lacrimation and conjunctival injection are more prevalent among patients with trigeminal neuralgia affecting the ophthalmic division (35). By contrast, symptoms such as facial swelling and excessive salivation tend to occur more frequently when the maxillary and/or mandibular divisions are involved (35). These insights suggest that SUNHA and trigeminal neuralgia are part of the same pathophysiologic continuum, in that the more prominent presence of cranial autonomic features in SUNHA and the presence of both lacrimation and conjunctival injection in SUNCT might, in part, be attributable to the predominant involvement of the ophthalmic division. Given these overlaps, future studies are encouraged to investigate whether SUNHA and trigeminal neuralgia are indeed variants of the same disorder, blurring the lines between what we currently classify as distinct disorders.
Less common differential diagnoses to SUNHA include migraine and TACs, such as cluster headache, paroxysmal hemicrania and hemicrania continua (1). It is worth noting that cranial autonomic features are present in all TACs and might also manifest in some people with migraine (1). A critical distinction lies in the much shorter duration of SUNHA attacks compared to those associated with migraine, cluster headache and hemicrania continua (1). The attack duration can, however, be somewhat similar in patients with paroxysmal hemicrania (1). The distinguishing feature is then the diagnostic requirement of an absolute response to treatment with indomethacin in paroxysmal hemicrania (1).
Methodological considerations and limitations
The present study has several limitations, warranting a cautious interpretation of our results. First and foremost, no population-based data were available to establish the prevalence of SUNHA in the adult general population. Of note, a recent nationwide registry study estimated the one-year prevalence of SUNHA as 1.2 per 100.000 among adults in the general population (36). However, this estimate did not adhere to the ICHD criteria for SUNHA. Instead, the study identified SUNHA cases using the ICD-10 code G44.8, required individuals to have received at least two lamotrigine prescriptions (totaling ≥200 tablets) and excluded those with the epilepsy reimbursement code G40. Our analyses were thus limited to observational data from clinic-based studies, in which adults with headache or facial pain were evaluated. We also noted that the relative frequencies tended to be lower in studies from secondary care units (13,14,16,20,21) compared to tertiary care units (11,12,15,17–19,22–25), limiting the generalizability of our results. Additionally, all included studies had a moderate or high risk of bias (see supplementary material, Tables S1 and S2).
Further limitations to this study include the considerable between-study heterogeneity observed for most calculated estimates, often with higher rates of heterogeneity among patients with SUNCT as opposed to SUNA. It was not possible to identify the cause(s) for this heterogeneity using meta-regression because of the limited number of studies included. However, we speculate that some between-study heterogeneity can, in part, be attributed to the differences in clinical settings among secondary and tertiary units, which might be a result of differences in referral patterns and the availability of specialized staff. Furthermore, publication bias might also influence our estimates because the likelihood of positive studies being published is greater. Also, the evolution of the ICHD criteria might be a contributing factor to some between-study heterogeneity because ICHD-3 is less restrictive in terms of attack frequency and duration, as well as reported cranial autonomic features (1,7,8). However, no discernable pattern was observed between the relative frequency of SUNHA and any specific edition of the ICHD. Another cause of between-study heterogeneity might stem from the method used for data collection; nine of 15 included studies had a cross-sectional or retrospective design. This introduces recall bias and increases the risk of both inaccurate and incomplete reporting. Also, the use of direct questions or predefined lists of clinical features might further exacerbate these issues. Finally, a possible limitation of our meta-analysis is not expanding the search criteria to include observational studies on trigeminal neuralgia, which might have captured a larger pool of potential SUNHA cases. However, accurate differentiation between SUNCT/SUNA and trigeminal neuralgia remains a diagnostic challenge. Future research focused on refining diagnostic criteria and improving the accuracy of distinguishing between these disorders would be valuable.
Future directions
Our findings underscore major gaps in the current understanding of SUNHA. Here, it is also important to acknowledge the limitations arising from inter-study heterogeneity and the absence of population-based data. Although our results cannot be considered generalizable to the entire SUNHA population, they offer a valuable starting point by synthesizing data from available clinic-based studies. Furthermore, our risk of bias assessment provides a roadmap for improving the design, conduct and reporting of future studies, which, in turn, can minimize heterogeneity and generate more accurate epidemiologic estimates. A particular need is thus determining the prevalence and clinical features of SUNHA in a population-based sample. In this context, establishing consensus guidelines on research practices will be important to obtain reliable estimates. We recommend that future studies clearly report inclusion and exclusion criteria and use a prospective study design. Furthermore, it is critical that future studies differentiate between patient cases adhering with the ICHD criteria and those who do not. This will minimize confusion and facilitate more robust comparisons across available studies. Future research should also consider investigating the presence or absence of potential cyclical patterns, such as monthly, seasonal and equinoctial/solstitial variations, in SUNHA attacks. In addition, it would be interesting to examine possible differences in SUNHA pain characteristics, including factors such as intensity, duration and trigeminal branch involvement. Moreover, we suggest classifying SUNHA as a single diagnostic entity without subdividing it into SUNCT and SUNA The differences between SUNCT and SUNA are marginal and do not, in our opinion, merit being classified as separate diagnostic entities. One small clinic-based study hinted at a possible higher attack frequency in patients with SUNCT compared to those with SUNA (24). However, larger studies are needed to confirm this difference and ascertain whether attack frequency is a distinguishing factor between these disorders. This information will help inform decisions regarding a possible unification of SUNCT and SUNA into a single diagnostic entity. In addition to this, more epidemiologic research is needed to ascertain the similarities and differences between SUNHA and trigeminal neuralgia because their clinical features overlap remarkably as well.
Conclusions
Our findings must be interpreted with caution because of methodologic issues and limitations in the included clinic-based studies. There is a pressing need for further research to delve into the epidemiology and clinical characteristics of SUNHA. However, our meta-analyses indicate that SUNHA is present in approximately 0.32% of patients evaluated for headache or facial pain. The most frequent clinical presentation for both SUNCT and SUNA was side-locked, episodic headache attacks of severe pain intensity, manifesting as single or repetitive stabs localized to the ophthalmic or maxillary branches of the trigeminal nerve. Furthermore, given the lack of notable differences between SUNCT and SUNA, we propose considering SUNHA as a single diagnostic entity.
Clinical implications
The relative frequency of SUNHA among adults evaluated for headache or facial pain was estimated as 0.32% (95% CI = 0.17–0.62; I2 = 89.9%). The most frequent clinical features were episodic, side-locked, stabbing headaches of severe pain intensity, affecting the ophthalmic and/or maxillary branch of the trigeminal nerve. Further research on this topic is warranted, as our results must be interpreted with caution due to between-study heterogeneity.
Supplemental Material
sj-docx-1-cep-10.1177_03331024241271976 - Supplemental material for Epidemiology and clinical features of short-lasting unilateral neuralgiform headache attacks: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cep-10.1177_03331024241271976 for Epidemiology and clinical features of short-lasting unilateral neuralgiform headache attacks: A systematic review and meta-analysis by Johanne Gry Larsen, Mikkel Johannes Henningsen, William Kristian Karlsson, Rune Häckert Christensen, Haidar Muhsen Al-Khazali, Faisal Mohammad Amin and Håkan Ashina in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024241271976 - Supplemental material for Epidemiology and clinical features of short-lasting unilateral neuralgiform headache attacks: A systematic review and meta-analysis
Supplemental material, sj-docx-2-cep-10.1177_03331024241271976 for Epidemiology and clinical features of short-lasting unilateral neuralgiform headache attacks: A systematic review and meta-analysis by Johanne Gry Larsen, Mikkel Johannes Henningsen, William Kristian Karlsson, Rune Häckert Christensen, Haidar Muhsen Al-Khazali, Faisal Mohammad Amin and Håkan Ashina in Cephalalgia
Supplemental Material
sj-docx-3-cep-10.1177_03331024241271976 - Supplemental material for Epidemiology and clinical features of short-lasting unilateral neuralgiform headache attacks: A systematic review and meta-analysis
Supplemental material, sj-docx-3-cep-10.1177_03331024241271976 for Epidemiology and clinical features of short-lasting unilateral neuralgiform headache attacks: A systematic review and meta-analysis by Johanne Gry Larsen, Mikkel Johannes Henningsen, William Kristian Karlsson, Rune Häckert Christensen, Haidar Muhsen Al-Khazali, Faisal Mohammad Amin and Håkan Ashina in Cephalalgia
Footnotes
Author contributions
FMA and HA were responsible for the study concept and design. JGL, MJH and WKK were responsible for the acquisition of data. JGL, MJH, WKK and RHC were responsible for the analysis and interpretation of data. JGL was responsible for drafting the manuscript. JGL, MJH, WKK, RHC, HMA, FMA and HA were responsible for the revising the manuscript for intellectual content. JGL, MJH, WKK, RHC, HMA, FMA and HA were responsible for final approval of the completed manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: JGL and MJH have no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; and no other relationships or activities that could appear to have influenced the submitted work. HMA and WKK reports personal fees from Pfizer, outside of the submitted work. RHC reports receiving travel funding from the Augustinus Foundation, outside of the submitted work. FMA has received personal fees from Pfizer, Teva, Lundbeck, Novartis and Eli Lilly, outside of the submitted work. HA reports personal fees from Lundbeck and Teva, outside of the submitted work.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.