
Abstract
Background
The current International Classification of Headache Disorders, 3rd edition (ICHD-3) diagnostic criteria for cardiac cephalalgia were established according to previous case reports and the opinion of experts. We aimed to assess the ICHD-3 diagnostic criteria for cardiac cephalalgia.
Methods
We conducted a series of cases study and evaluated these criteria in 54 patients with cardiac cephalalgia. Next, we assessed whether the ICHD-3 diagnostic criteria B, C and D for migraine without aura were fulfilled by these patients.
Results
ICHD-3 criteria A, B, C1, C2 and D for cardiac cephalalgia were met by 100% of patients, whereas criterion C3 was fulfilled by 81.5%. The least frequently fulfilled sub-criterion was C3b (accompanied by nausea) (18.5%). Moreover, we found that ICHD-3 criteria B, C and D for migraine without aura were met by a low proportion of patients: 11.1%, 46.3% and 25.9%, respectively, and no patient fulfilled the three criteria simultaneously.
Conclusion
Based on our results, we propose revised diagnostic criteria for cardiac cephalalgia. We suggest removing criterion C3 and C4. We also suggest removing the word “migraine-like” from its description.
Introduction
Cardiac cephalalgia is a secondary headache that occurs during an episode of myocardial ischemia. It was first described in 1997 (1) and subsequently introduced in the 2nd edition of the International Classification of Headache Disorders (2). The International Classification of Headache Disorders, 3rd edition (ICHD-3) diagnostic criteria for cardiac cephalalgia were established according to previous case reports and the opinion of experts (Table 1) (3).
ICHD-3 diagnostic criteria for cardiac cephalalgia 3 .

Some studies have suggested that current diagnostic criteria might not be adequate, mainly criterion C, which describes headache characteristics (4,5). Xu et al. (4) found that sub-criterion C3b (accompanied by nausea) was the least frequently met criterion (36.6% of cases) and proposed that accompanying cardiac symptoms (chest pain, chest tightness and sweating) should be included in the diagnostic criteria. A recent literature review that evaluated the ICHD-3 diagnostic criteria based on 88 cases of cardiac cephalalgia showed that sub-criterion C3b was fulfilled only by 31.8% and suggested removing it (5). Furthermore, cardiac cephalalgia is described in the ICHD-3 as a migraine-like headache. However, it is possible that this definition is not correct because throbbing quality was present only in 13.8% of previous case reports (5), with unilateral headache in 12.1%, and the absence of photo and phonophobia is a criterion of cardiac cephalalgia (sub-criterion C3b), but at least one of them is present in 18.5% of cases (6).
Given this situation and based on our very large representative prospectively evaluated material, the present study aimed to evaluate ICHD-3 diagnostic criteria for cardiac cephalalgia and assess whether the diagnostic criteria B, C, and D for migraine without aura from the ICHD-3 are fulfilled by patients with cardiac cephalalgia. In addition, the study proposed evidence-based diagnostic criteria for this entity.
Methods
Study design
We conducted a series of cases study of 54 patients with cardiac cephalalgia identified in a prospective study of consecutive patients admitted to the Cardiology Service at Hospital Clínico Universitario Lozano Blesa in Zaragoza, Spain, with suspected acute coronary syndrome (ACS) from January 2021 and January 2022 (6). A complete description of material and methods has been given elsewhere (6).
We assessed the occurrence of headache at ACS onset. All participants were evaluated during a face-to-face interview performed by a trained research team and using a standardized semi-structured case report form. The interview was performed during the first 24 h after admission to reduce recall bias.
For the evaluation of the ICHD-3 diagnostic criteria for cardiac cephalalgia, the percentage of patients with cardiac cephalalgia who met each of the diagnostic criteria was analysed.
Sub-criterion C2a (headache has significantly worsened in parallel with worsening of the myocardial ischemia) was not assessed because we considered that the only way to confirm this criterion would be to observe simultaneous worsening of headache and myocardial ischemia; for example, during a stress test. The population included in our study did not usually undergo this diagnostic test because they were mostly patients with myocardial infarction or unstable angina. Criterion C4 (headache is relieved by nitroglycerine or derivatives of it) was not evaluated because many patients in our study received different medical and/or interventional treatments almost simultaneously at the emergency room or even sometimes in the pre-hospital setting. For this reason, given the difficulty of discerning if headache improved with nitrates or if the improvement was caused by another drug or procedure, we decided to evaluate only sub-criterion C2b (headache has significantly improved or resolved in parallel with improvement in or resolution of the myocardial ischemia).
For the evaluation of the ICHD-3 criteria B, C and D for migraine without aura, we recorded the number of patients with cardiac cephalalgia that fulfilled each criterion and the number of patients who met all three criteria at the same time.
Patient consent and registration
The study was approved by the Regional Research Ethics Committee of Aragon (CEICA) with the reference number PI20/524. All participants provided their written informed consent before taking part into the study.
Results
In total, 538 patients were screened for eligibility and 100 patients met exclusion criteria. From 438 patients with suspected ACS included in the study, we found 381 patients with demonstrated myocardial ischemia. Among them, we identified 54 patients with cardiac cephalalgia. Some 77.8% of patients were male (n = 42) and the mean ± SD age was 62.2 ± 10.8 years. In relation to ACS symptoms onset, headache started simultaneously in most patients (n = 47; 87%), headache started before in six patients (11.1%) and headache started 10 min after in one patient. In all patients who presented headache before ACS symptoms, headache started within the previous 1 h (median 15 min before; interquartile range = 18.7–48.7 min). Headache was completely resolved in all patients. Table 2 summarizes the headache characteristics.
Headache characteristics in patients with cardiac cephalalgia. 6

NRS, numerical rating scale; IQR, interquartile range.
Evaluation of ICHD-3 criteria for cardiac cephalalgia
All patients fulfilled ICHD-3 diagnostic criteria. All patients with cardiac cephalalgia met criteria A (any headache fulfilling criterion C) and B (acute myocardial ischemia has been demonstrated).
Regarding criterion C, which is the criterion that establishes causality, all patients met criterion C1 (headache has developed in temporal relation to the onset of acute myocardial ischemia).
As for criterion C2, all patients met sub-criterion C2b (headache has significantly improved or resolved in parallel with improvement in or resolution of the myocardial ischemia). However, in the present study, we did not assess whether patients fulfilled sub-criterion C2a for the reasons explained above.
In relation to criterion C3, 44 patients (81.5%) met this criterion. Forty-seven patients (87%) fulfilled sub-criterion C3a (moderate to severe intensity), 10 patients (18.5%) fulfilled sub-criterion C3b (accompanied by nausea), 44 patients (81.5%) met sub-criterion C3c (not accompanied by photophobia or phonophobia) and 17 patients (31.5%) met sub-criterion C3d (aggravated by exertion). As mentioned above, criterion C4 was not evaluated.
Finally, all patients met criterion D (not attributable to another ICHD-3 diagnosis). Table 3 shows the number and percentage of patients with cardiac cephalalgia who met each one of the ICHD-3 diagnostic criteria.
Patients with cardiac cephalalgia that met ICHD-3 the diagnostic criteria for cardiac cephalalgia.

Evaluation of ICHD-3 criteria B, C and D for migraine without aura
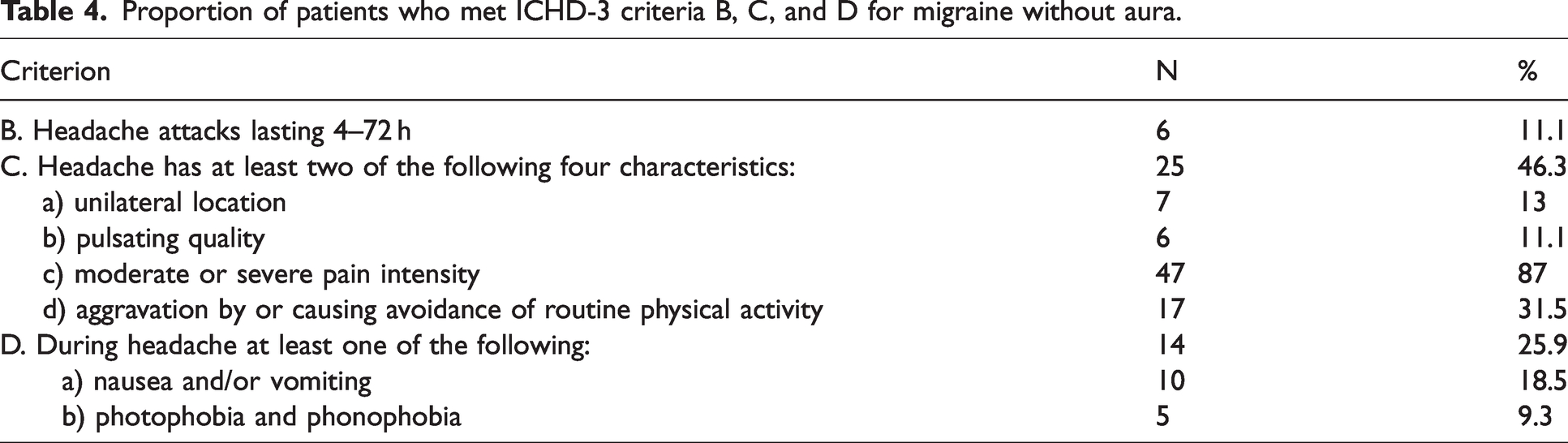
Only six patients (11.1%) fulfilled criterion B (headache attacks lasting 4–72 h). With regard to criterion C, which describes the clinical characteristics of headache, seven patients (13%) fulfilled sub-criterion Ca (unilateral location), six (11.1%) fulfilled sub-criterion Cb (pulsating quality), 47 (87%) fulfilled sub-criterion Cc (moderate or severe pain intensity) and 17 (31.5%) fulfilled sub-criterion Cd (aggravation by or causing avoidance of routine physical activity). In total, 25 patients (46,3%) had at least two of these headache characteristics and met criterion C.
Regarding criterion D, 14 patients (25,9%) presented at least one of the following accompanying symptoms: 10 patients (18.5%) fulfilled sub-criterion Da (nausea and/or vomiting) and five (9.3%) fulfilled sub-criterion Db (photophobia and phonophobia). No patient met all three criteria B, C and D for migraine without aura simultaneously (Table 4).
Proportion of patients who met ICHD-3 criteria B, C, and D for migraine without aura.
Discussion
The main finding of the present study is that criteria A, B, C1, C2 and D were met by 100% of patients, whereas criterion C3 was fulfilled by 81.5%. The least frequently fulfilled sub-criterion was C3b (accompanied by nausea). Moreover, we found that criteria B, C and D for migraine without aura were met by a low proportion of patients (11.1%, 46.3% and 25.9%, respectively) and no patient fulfilled the three criteria.
ICHD-3 criteria for cardiac cephalalgia
All patients from our study met ICHD-3 criteria A, B, C1, C2 and D for cardiac cephalalgia.
The most frequently fulfilled C3 sub-criteria were C3a and C3c. 87% of the patients presented moderate-severe intensity (sub-criterion C3a) and, in 81.5% of the cases, headache was not accompanied by photophobia or phonophobia (sub-criterion C3c). These data are similar to those reported in the study by Xu et al. (4) in which these criteria were met by 80% of patients. However, when reviewing the total number of cases reported to date, these criteria were met in a lower percentage of patients, 75% and 55.7%, respectively (5). Nevertheless, the data from the literature review should be interpreted with caution because, in a large part of the case reports, headache characteristics were not described in detail (5).
Sub-criteria C3b (headache accompanied by nausea) and C3d (aggravation by exertion) were met in a low percentage of patients, 18.5% and 31.5%, respectively. The low frequency of nausea as an accompanying symptom of cardiac cephalalgia was also described in the observational study (36.6%) (4) and in previous case reports (31.8%) (5).
Aggravation by exertion was less frequent in the present study than in the study by Xu et al. (4) and, in prior case reports (5), 100% and 55.7% respectively. This lower percentage could be because the present study only included hospitalized patients who therefore presented more severe ischemic pathology and could not have been exposed to physical activity because of their clinical situation.
Furthermore, we observed that ICHD-3 criteria B, C and D for migraine without aura were each met by only a small percentage of patients and that no patient met all three criteria at the same time. Taking this into consideration, it seems that the description of cardiac cephalalgia as a migraine-like headache is not adequate.
New diagnostic criteria proposal
In line with the results of the study by Xu et al. (4), criteria A, B and D were fulfilled by 100% of patients. In our opinion, these criteria should remain unchanged.
Regarding criterion C, our results showed that sub-criteria C1 and C2b were met by all patients and should remain. However, our results showed that, in most cases (87%), headache and ACS symptoms started simultaneously and, in all patients except one (98,1%), headache started within 1 h before ACS symptoms. For this reason, we think that it is important to specify in criterion C1 that headache develops in close temporal relation to the onset of acute myocardial ischemia.
Even though sub-criterion C2a was not analysed in the present study, we think that it should remain in the diagnostic criteria because it can be relevant in patients with stable angina or during stress test.
In relation to criterion C3, studies have shown that headache characteristics in patients with cardiac cephalalgia are very variable (4–6) and the compliance rate of some of the sub-criteria, especially C3b and C3d, is low. For this reason and to simplify the diagnostic criteria, we suggest that criterion C3 should be removed.
As for criterion C4, although we did not analyse it, previous studies have shown that all patients who reported the use of nitrates presented headache relief (4,5). Given that some patients might not take nitrates or that different therapies such us intravenous fibrinolysis or coronary revascularization might be applied, we think that this criterion should be deleted because it does not contribute as an addition to criteria C1 and C2. Table 5 shows our proposal for the modification of cardiac cephalalgia diagnostic criteria.
Proposal for the modification of cardiac cephalalgia diagnostic criteria.

Finally, we suggest removing the word “migraine-like” from the description of cardiac cephalalgia given that the characteristics of headache in these patients do not usually comply with migraine.
Strengths and limitations
The present study evaluated current diagnostic criteria in the largest cohort of patients with cardiac cephalalgia to date. We were not able to assess some of the criteria (C2a and 4) but that was found to be unnecessary. Furthermore, we only included patients with myocardial ischemia who required admission and we did not analyse patients with stable angina who are managed in the outpatient setting. For this reason, we adapted our proposal to also include this group of patients.
Conclusions
We evaluated ICHD-3 diagnostic criteria for cardiac cephalalgia in the largest cohort of patients with this entity to date. Criteria A, B, C1, C2 and D for cardiac cephalalgia were met by all patients, whereas criterion C3 was fulfilled by 81.5%, and the least frequently met sub-criterion was C3b (accompanied by nausea). Furthermore, criteria B, C, and D for migraine without aura were met by a low proportion of patients and no patient fulfilled the three criteria simultaneously.
To improve ICHD-3 diagnostic criteria for cardiac cephalalgia, we propose removing criterion C3 and C4. We also suggest removing the word “migraine-like” from its description.
Clinical implications
ICHD-3 criteria A, B, C1, C2 and D for cardiac cephalalgia were met by all patients. 81.5% of patients met criterion C3 and the percentage of patients who fulfilled C3 sub-criteria was variable. To improve current ICHD-3 diagnostic criteria for cardiac cephalalgia, we suggest removing criterion C3 and C4. We also suggest removing the word “migraine-like” from the description of cardiac cephalalgia given that the characteristics of headache in these patients do not usually comply with migraine.
Footnotes
Data availability
De-identified participant data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there are no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
The Regional Research Ethics Committee of Aragon (CEICA) approved the study. The reference number is PI20/524. All participants provided written informed consent before taking part into the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.